Management of unknown primary with neck node metastasis: Current evidence
|
|
|
- Maurice Holmes
- 6 years ago
- Views:
Transcription


1 Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad
2 Introduction- Approach to Topic What is MUO different terminologies How to diagnose How to treat Review of literature Take home message

3 Different terminologies CUP: Carcinoma of unknown primary PUO: Primary of unknown origin MUO: Metastases of unknown origin UKP: Unknown primary
4
5 Unknown primary A lymph node in the neck with malignant pathology without any obvious primary mucosal origin. Head and neck unknown primaries are generally squamous cell carcinomas Incidence: 5 % of head and neck cancers

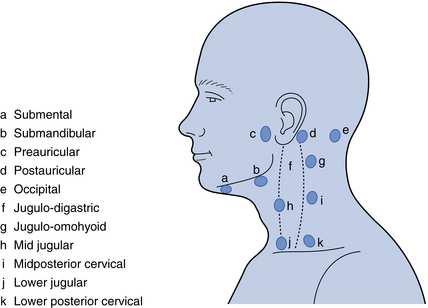
6 Levels of the Neck
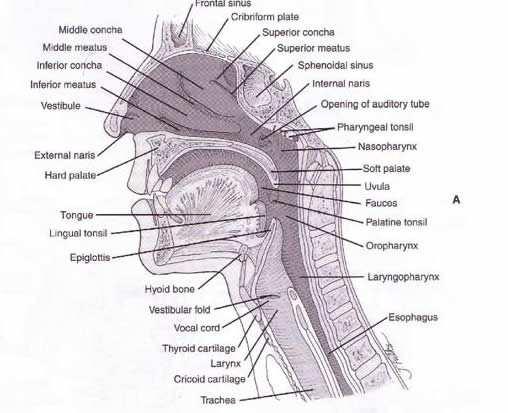
7 Levels of the Neck Level I - This includes the submental and submandibular lymph nodes. The submental triangle (sublevel IA) is bounded by the anterior belly of the digastric muscles (laterally) and the hyoid (inferiorly). The submandibular triangle (sublevel IB) is bounded by the body of the mandible (superiorly), the stylohyoid (posteriorly), and the anterior belly of the digastric (anteriorly). Level II - This includes lymph nodes of the upper jugular group and is divided into sublevels IIA and IIB. Level II is bounded by the inferior border of the hyoid (inferiorly), the base of skull (superiorly), the stylohyoid muscle (anteriorly) and the posterior border of the SCM (posteriorly). Sublevel IIA nodes lie anterior to the SAN. Sublevel IIB nodes lie posterior to the SAN. Level III - This includes lymph nodes of the middle jugular group. This level is bounded by the inferior border of the hyoid (superiorly) and the inferior border of the cricoid (inferiorly), the posterior border of the sternohyoid (anteriorly) and the posterior border of the SCM (posteriorly). Level IV - This includes lymph nodes of the lower jugular group. This level is bounded by the inferior border of the cricoid (superiorly), the clavicle / sternal notch (inferiorly), the posterior border of the sternohyoid (anteriorly) and the posterior border of the SCM (posteriorly). Level V - This includes posterior compartment lymph nodes. This compartment is bounded by the clavicle (inferiorly), the anterior border of the trapezius (posteriorly), the posterior border of the SCM (anteriorly). It is divided into sublevels VA (lying above a transverse plane marking the inferior border of the anterior cricoid arch) and VB (below the aforementioned plane). Level VI - This includes the anterior compartment lymph nodes. This compartment is bounded by the common carotid arteries (laterally), the hyoid (superiorly), the suprasternal notch (inferiorly).
8 3-5% of presentation,55-65 years 80-85% are tonsil and base of tongue Most commonly level II F/B III whereas I, IV and V are less frequent. Unilateral more common and B/L 10% Metastases in upper neck is mostly from head and neck SCC, PD ( Exception Adenocarcinoma - thyroid, parathyroid and parotid) From lower neck below clavicles other than from head and neck - Adenoca
9 Clinical Presentation Patients generally present with a painless, solitary neck mass, most often discovered by the patient. Masses are usually at least 3-5 cm Patients have usually gone through at least one course of antibiotics Benign masses are also often solitary and painless
10 Differential diagnosis Benign Developmental (i.e., thyroglossal duct cyst, branchial cleft cysts or inclusion cysts) Inflammatory (i.e., lymphadenitis, benign reactive hyperplasia, infected sebaceous cyst) Benign Neoplasms (i.e., lipoma, fibroma, hemangioma, neurofibroma, parathyroid adenoma or goiter)
11 Differential diagnosis Malignant Metastatic carcinoma, sarcoma or melanoma Lymphoma, Leukemia Carotid body tumor Primary major salivary gland tumor Thyroid cancer Parathyroid cancer Histiocytosis Carcinoid
12 Relationship of Node Location to Likely Disease Nodes at certain levels more likely certain primaries Upper neck nodes are the most likely to be head and neck cancer Subdigastric node may be virtually any head and neck primary, or a non-hodgkin s lymphoma Submandibular node suggests oral cavity, lip, nasal vestibule or salivary gland primary Submental nodes are uncommon
13 Relationship of Node Location to Likely Disease Mid Neck Likely primaries include larynx, hypopharynx, and less commonly esophagus, disease below clavicles or lymphoma Lower Neck and Supraclavicular Nodes Most often metastatic from chest or abdomen, possible esophagus or lymphoma. Parotid lymph nodes Parotid lymph nodes are more likely skin cancer than from a primary parotid tumor

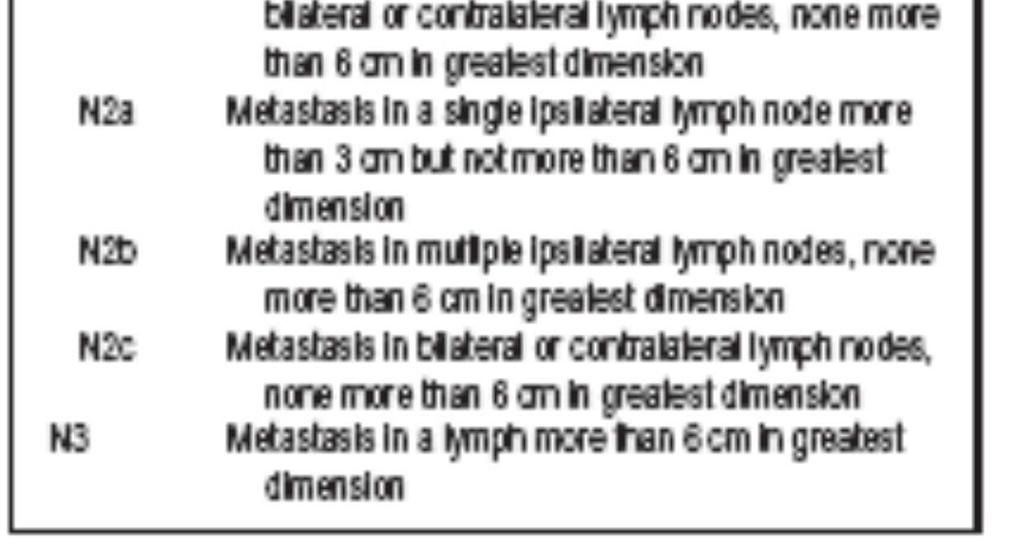
14 AJCC Nodal Staging
15 Diagnosis Physical exam Soft, rubbery nodules suggest lymphoma and leukemia Hard, fixed masses suggest carcinoma Indirect examination of oral cavity and oropharynx with mirror and/or fiberoptic endoscopy
16 Diagnosis Imaging CT followed by an MRI if inconclusive If there is still no imaging data for a primary, a PET may be ordered In a meta-analysis of 16 studies looking at the role of PET in 302 patients with cervical node metastases where a primary has yet to be discovered through the work up, 25% of primaries are identified through PET. Previously unrecognized regional or distant metastases were identified in 27% of patients Rusthoven, KE, Koshy, M, Paulino, AC, The role of fluorodeoxyglucose PET in cervical lymph node metastases from an unknown primary tumor. Cancer 2004; 101:2461
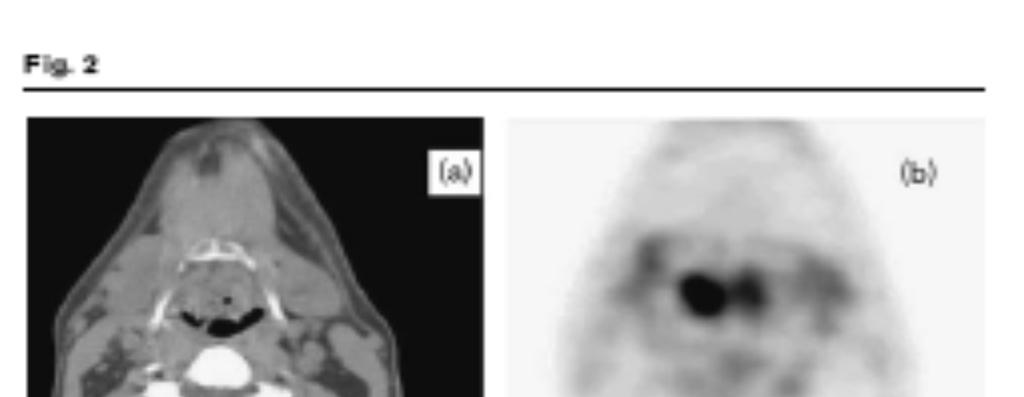
17
18 Diagnosis Fine needle biopsy of LN Incisional or excisional biopsy before definitive treatment neck recurrence distant metastasis wound necrosis
19 SCC and UD- EBV and p16 EBV in situ hybridization Nasopharyngeal malignancy SCC Polymerase chain reaction Oropharyngeal malignancy Treat accordingly
20 Diagnosis Staging surgical endoscopy panendoscopy (triple endoscopy) direct laryngoscopy to evaluate oropharynx, larynx and hypopharynx, nasopharyngoscopy and upper esophagoscopy
21 Diagnosis Screening Tonsillectomy If a primary site has not been discovered by this point, an ipsilateral screening tonsillectomy may be performed This is of greatest benefit in patients with subdigastric, submandibular or midjugulocarotid lymph nodes In a study of 87 patients with unknown primaries, 26% were discovered to have a tonsillar primary after tonsillectomy Lapeyre, M, Malissard, L, Peiffert, D et al. Cervical lymph node metastasis from an unknown primary: Is a tonsillectomy necessary? Int J Radiat Oncol Biol Phys; 39: 291 Literature for bilateral tonsillectomy not convincing (no chance of missing contralateral tonsil and greater symmetry on PE after B/L tonsillectomy
22 Treatment Treat as aggressive disease Treat based on staging N1- neck dissection OR radiation N2, N3- combined neck dissection AND radiation
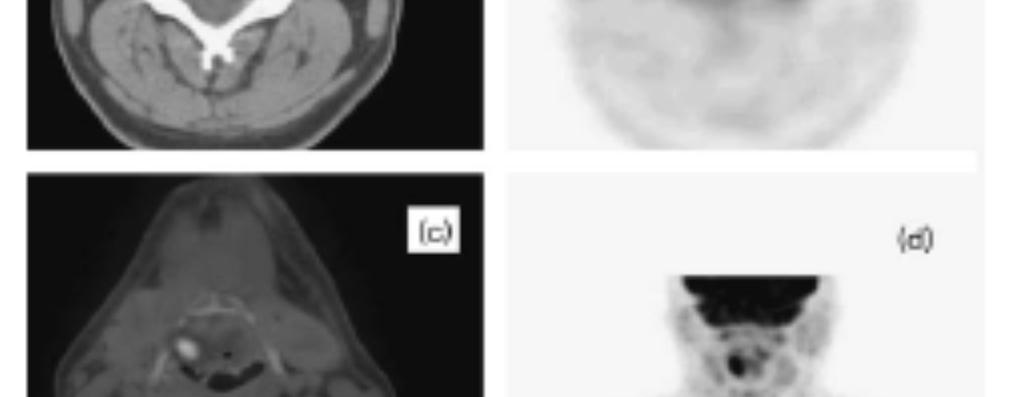
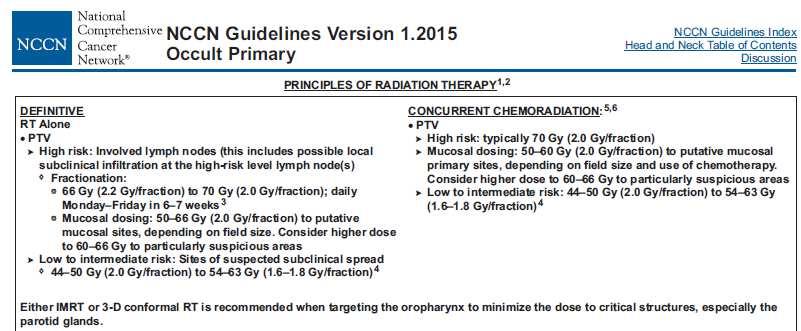
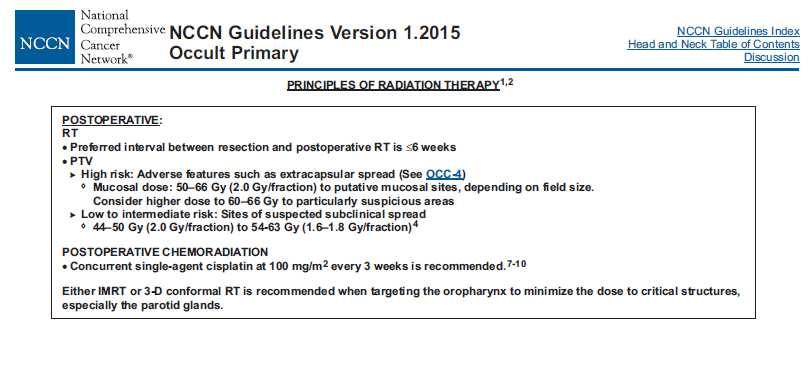
23 Basic guidelines


24
25 Poorly Differentiated Most frequent site is pharynx especially NP RT to neck and Waldeyer s ring including NP Neck dissection for residual Adenocarcinoma Node at level I-III could be salivary gland tumor Excision biopsy indicated and if clinical and pathological cannot find primary then consensus on neck dissection (I-V) including parotidectomy if indicated followed by RT
26
27
28
29
30
31
32 IMRT Part of the purpose of using IMRT is to decrease dose to the parotid, in order to decrease the grade of xerostomia and improve dose homogeneity Bhide, S et al. Intensity modulated radiotherapy improves target coverage and parotid gland sparing when delivering total mucosal irradiation in patients with squamous cell carcinoma of head and neck of unknown primary site. 2007; 32(3): Can also keep dose off of the larynx
33 Radiation Ipsilateral neck vs. bilateral neck, Bilateral favored Some studies show increase risk of neck disease or emergence of primary with ipsilateral treatment compared to bilateral without overall survival being affected Alternate studies show extensive radiation of mucosa and bilateral neck improve survival compared to ipsilateral neck radiation Study of 352 patients with squamous cell or undifferentiated cancer of the cervical lymph nodes with no evident primary, the patients who received ipsilateral neck radiation compared to those receiving bilateral had a 1.9 relative risk of recurrence in the head and neck and lower 5 year disease free survival Grau, C Johansen, LV, Jakobsen, J et al. Cervical lymph node metastases from unknown primary tumours. Results from a national survey by the Danish Society for Head and Neck Oncology. Radiother Oncol 2000;55:121.

34 Largest experience with primary RT Danish Society of Head and Neck Oncology over a 20 year period
35 Radiation by Node location Upper nodes Naso-, oro- and hypopharynx and supraglottic larynx. Oral cavity not included Junctional or lateral retropharyngeal node Naso- and oropharynx Submandibular- solitary node Neck only because of the major morbidity of irradiating the entire oral cavity Midjugular Oro-, hypopharynx and supraglottic larynx Supraclavicular Large portal to include apex of axilla
 associated with 1 0 below the clavicles e.g.")
36 Metastatic Cervical LNs Cervical node metastases of squamous cell carcinoma from occult primary constitute about 2-5% of all patients with CUP Mets in upper & mid neck attributed to H&N cancers Lower neck (SCF) associated with 1 0 below the clavicles e.g. lung or GI tract
37 Results Emergence rate of primary is 25% Medial nodal recurrence rate 35% 5 year overall survival rate 66% Estimated actuarial risk of emergence of head and neck primary after extensive irradiaton reaches 20% at 10 years. Median time to occurrence of subsequent primaries is about 21 months
38 Complications of Radiation Therapy Most common complication is xerostomia (dry mouth due to decreased saliva production) Fatigue Mucositis Altered taste sensations Red and irritated skin Occasional nausea Esophageal stricture
39 Chemotherapy Platinum-based chemotherapy in combination with radiation recommended for N3 patients by European Society of Medical Oncology (ESMO) Consider concurrent chemo/rt with supraclavicular LN or undifferentiated tumors, though no strong data to support Chemo/ RT is an option for palliation, unresectable local disease, distant metastatic spread
40 Follow up TFT should be monitored if the patient received radiation to the lower neck since upto 30% of patients may develop subclinical or overt radiation induced hypothyroidism Clinical and fibrescopic check every two months in the first year, every four months for second an third every year then every six months. PET once a year, additional examination at discretion
41 Recurrence Comparing subsequent mucosal primary lesions in patients with unknown primaries to head and neck cancer with a known primary site shows the incidence of a subsequent mucosal recurrence was similar for both groups.
42 Recurrence Location (primary site, new primary site, neck or distant), the histology, time since initial diagnosis and prior therapies. surgical management is favored for patients previously treated with radiotherapy, and likewise those previously having undergone surgery alone should be considered for radiotherapy (+/- chemotherapy). Some patients - for repeat radiotherapy even to high doses. Small localized recurrences may be managed surgically in some cases. Recurrence at the base of skull or other difficult-to-access locations can benefit from external consultation at centers equipped with gamma knife or SBRT technologies. Other options include palliative radiotherapy or best supportive care.
43 Prognosis The best indicator of prognosis is N stage at presentation Also, the presence of extracapsular extension is associated with a poorer prognosis Prognosis is similar between patients with a known vs. an unknown primary with the same nodal stage.
44 Future Research Phase III Randomized Study of Selective Irradiation Versus Extensive Irradiation in Patients With Cervical Lymph Node Metastases of Squamous Cell Carcinoma From an Unknown Primary- Opened 2002, now closed awaiting for results EORTC-24001, EORTC-22005, DAHANCA-EORTC-24001, CAN-NCIC-EORTC-24001, RTOG-EORTC-24001, NCT
45 TAKE HOME MESSAGE Depends on whether source is found during workup If primary site identified treat accordingly, ND followed by PORT to neck and mucosal sites Distinct advantages for different options Surgery/RT/CT+RT Mucosal irradiation decrease primary emergence but at cost Tailoring of therapy according to HPV, EBV, Nodal level, history prevent unwarranted toxicity



46


47 Although in politics you cover the known, in medicine you uncover the unknown
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Head & Neck Contouring
 Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Q&A. Fabulous Prizes. Collecting Cancer Data: Pharynx 12/6/12. NAACCR Webinar Series Collecting Cancer Data Pharynx
 Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
The following images were all acquired using a CTI Biograph
 Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Chapter 13: Mass in the Neck. Raymond P. Wood II:
 Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
CERVICAL LYMPH NODES
 CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
FACULTY OF MEDICINE SIRIRAJ HOSPITAL
 Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Since the first description of the radical neck dissection by George Crile almost a century
 ORIGINAL ARTICLE Neck Dissection Classification Update Revisions Proposed by the American Head and Neck Society and the American Academy of Otolaryngology Head and Neck Surgery K. Thomas Robbins, MD; Garry
ORIGINAL ARTICLE Neck Dissection Classification Update Revisions Proposed by the American Head and Neck Society and the American Academy of Otolaryngology Head and Neck Surgery K. Thomas Robbins, MD; Garry
Neck-2. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Practice teaching course on head and neck cancer management
 28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE LIFE THROUGH MEDICAL MEDICAL EDUCATION EDUCATION www.excemed.org
28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE LIFE THROUGH MEDICAL MEDICAL EDUCATION EDUCATION www.excemed.org
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
14. Mucosal Melanoma of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
Neck Dissection. Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)
, BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)") Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
10. HPV-Mediated (p16+) Oropharyngeal Cancer
 Oropharyngeal Cancer") 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Cervical Lymph Nodes
 Cervical Lymph Nodes Diana Gaitini, MD Unit of Ultrasound, Department of Medical Imaging Rambam Medical Center and Faculty of Medicine Technion, Israel Institute of Technology Haifa, Israel Learning Targets
Cervical Lymph Nodes Diana Gaitini, MD Unit of Ultrasound, Department of Medical Imaging Rambam Medical Center and Faculty of Medicine Technion, Israel Institute of Technology Haifa, Israel Learning Targets
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
Cancer of the Head and Neck and. HPV Infection. Andrew Urquhart MD, FACS Dept. Otolaryngology/Head and Neck Surgery Marshfield Clinic
 Cancer of the Head and Neck and HPV Infection Andrew Urquhart MD, FACS Dept. Otolaryngology/Head and Neck Surgery Marshfield Clinic Disclaimer I have no relevant financial relationships with the manufacturer(s)
Cancer of the Head and Neck and HPV Infection Andrew Urquhart MD, FACS Dept. Otolaryngology/Head and Neck Surgery Marshfield Clinic Disclaimer I have no relevant financial relationships with the manufacturer(s)
A Pathologist s Guide to Neck Dissection. Neck Dissections. Lymphatics of head and neck. Neck Dissections
 A Pathologist s Guide to Neck Dissection North American Society for Head and Neck Pathology Companion Meeting 2006 Sigrid Wayne, M.D. Department of Pathology University of Iowa The presence of cervical
A Pathologist s Guide to Neck Dissection North American Society for Head and Neck Pathology Companion Meeting 2006 Sigrid Wayne, M.D. Department of Pathology University of Iowa The presence of cervical
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Dr Nick McIvor. Dr John Chaplin. Head & Neck Surgeon Auckland City Hospital Auckland. Auckland Head & Neck Surgeon Gillies Hospital Auckland
 Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
NAACCR Webinar Series
 NAACCR 2009-2010 Webinar Series Collecting Cancer Data: Lip & Oral Cavity 8/5/2010 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes! NAACCR 2009/2010
NAACCR 2009-2010 Webinar Series Collecting Cancer Data: Lip & Oral Cavity 8/5/2010 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes! NAACCR 2009/2010
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
NAACCR Webinar Series 1
 Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Alexander C Vlantis. Selective Neck Dissection 33
 05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
Evaluation of Head and Neck Masses in Adults
 Evaluation of Head and Neck Masses in Adults Kristi Chang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery University of Iowa Hospitals and Clinics Annual Refresher Course for
Evaluation of Head and Neck Masses in Adults Kristi Chang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery University of Iowa Hospitals and Clinics Annual Refresher Course for
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
The Neck the lower margin of the mandible above the suprasternal notch and the upper border of the clavicle
 The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Oral cancer: Prognosis & Treatment. Dr. Hani Al Sheikh Radhi
 Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
LYMPHATIC DRAINAGE IN THE HEAD & NECK
 LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
Lecture 07. Lymphatic's of Head & Neck. By: Dr Farooq Amanullah Khan PMC
 Lecture 07 Lymphatic's of Head & Neck By: Dr Farooq Amanullah Khan PMC Dated: 28.11.2017 Lymphatic Vessels Of the 800 lymph nodes in the human body, 300 are in the Head & neck region. The lymphatic vessels
Lecture 07 Lymphatic's of Head & Neck By: Dr Farooq Amanullah Khan PMC Dated: 28.11.2017 Lymphatic Vessels Of the 800 lymph nodes in the human body, 300 are in the Head & neck region. The lymphatic vessels
Head and Neck Case Studies
 Head and Neck Case Studies John Chaplin & Nick McIvor www.headneck.co.nz Head and Neck lumps every lump must have a diagnosis Working diagnosis» +/- investigations Review» +/- investigations auckland head
Head and Neck Case Studies John Chaplin & Nick McIvor www.headneck.co.nz Head and Neck lumps every lump must have a diagnosis Working diagnosis» +/- investigations Review» +/- investigations auckland head
CLINICAL MEDICATION POLICY
 CLINICAL MEDICATION POLICY Policy Name: Opdivo (nivolumab) injection Policy Number: Approved By: Medical Management, Clinical Pharmacy Products: Highmark Health Options Application: All participating hospitals
CLINICAL MEDICATION POLICY Policy Name: Opdivo (nivolumab) injection Policy Number: Approved By: Medical Management, Clinical Pharmacy Products: Highmark Health Options Application: All participating hospitals
Volumi di trattamento del cavo orale
 SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD
 PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD Topics 1. Cervical lymphadenopathy 2. Lymphatic malformation 3. Thyroglossal duct cysts 4. Branchial cleft cysts 5. Thyroid masses CASE 1 Case 1 A 2
PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD Topics 1. Cervical lymphadenopathy 2. Lymphatic malformation 3. Thyroglossal duct cysts 4. Branchial cleft cysts 5. Thyroid masses CASE 1 Case 1 A 2
HPV and Head and Neck Cancer: What it means for you and your patients
 HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV
 DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018
 ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018 Dr. Victor Ho-Fun Lee MBBS, MD, FRCR, FHKCR, FHKAM (Radiology) Clinical Associate Professor Department of Clinical Oncology
ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018 Dr. Victor Ho-Fun Lee MBBS, MD, FRCR, FHKCR, FHKAM (Radiology) Clinical Associate Professor Department of Clinical Oncology
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Nasal Cavity CS Tumor Size (Revised: 02/03/2010)
") Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
Greater Baltimore Medical Center Sandra & Malcolm Berman Cancer Institute
 2008 ANNUAL REPORT Greater Baltimore Medical Center Sandra & Malcolm Berman Cancer Institute Cancer Registry Report The Cancer Data Management System/ Cancer Registry collects data on all types of cancer
2008 ANNUAL REPORT Greater Baltimore Medical Center Sandra & Malcolm Berman Cancer Institute Cancer Registry Report The Cancer Data Management System/ Cancer Registry collects data on all types of cancer
"The Space Between Us:" A Radiographic Review of Common and Uncommon Pathologic Findings within the Deep Spaces of the Neck
 "The Space Between Us:" A Radiographic Review of Common and Uncommon Pathologic Findings within the Deep Spaces of the Neck Poster No.: C-2457 Congress: ECR 2015 Type: Educational Exhibit Authors: A. K.
"The Space Between Us:" A Radiographic Review of Common and Uncommon Pathologic Findings within the Deep Spaces of the Neck Poster No.: C-2457 Congress: ECR 2015 Type: Educational Exhibit Authors: A. K.
Anterior triangle of neck
 Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
Clinical evaluation. Imaging Surgical treatment
 Parapharyngeal Space Khalid adhussain AL-Qahtani a MD,MSc,FRCS(c) Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular Reconstruction, ti and
Parapharyngeal Space Khalid adhussain AL-Qahtani a MD,MSc,FRCS(c) Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular Reconstruction, ti and
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
From GTV to CTV: A Critical Step Towards Cure. Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017
 From GTV to CTV: A Critical Step Towards Cure Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017 Head and Neck Cancer Model for Understanding CTV Expansion Radiation
From GTV to CTV: A Critical Step Towards Cure Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017 Head and Neck Cancer Model for Understanding CTV Expansion Radiation
The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide
 The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide Alba L. Reyes Ortiz, MD Elena Capilla, MD. Lina Cruz Hernández,
The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide Alba L. Reyes Ortiz, MD Elena Capilla, MD. Lina Cruz Hernández,
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Nasopharynx Cancer. 1 Feb Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar)
 Dr Peter Luk (Pathology Registrar)") Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
The many faces of extranodal lymphoma
 The many faces of extranodal lymphoma Frank Pameijer Departments of Radiology and Radiation Oncology University Medical Center Utrecht Special thanks to Ilona M Schmalfuss, MD University of Florida Gainesville,
The many faces of extranodal lymphoma Frank Pameijer Departments of Radiology and Radiation Oncology University Medical Center Utrecht Special thanks to Ilona M Schmalfuss, MD University of Florida Gainesville,
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
Advanced Anatomy of the Neck
 AACE 2018 Advanced Anatomy of the Neck Alex Tessnow, MD, MBA, FACE, ECNU University of Texas Southwestern Dallas, TX Content contributed by: H. Jack Baskin, Daniel Duick, Diana Dean, Robert A. Levine,
AACE 2018 Advanced Anatomy of the Neck Alex Tessnow, MD, MBA, FACE, ECNU University of Texas Southwestern Dallas, TX Content contributed by: H. Jack Baskin, Daniel Duick, Diana Dean, Robert A. Levine,
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY
 PATIENT CENTERED MEDICINE - 1 GOALS & OUTCOMES: PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY 1. To introduce the applied anatomy relevant for the examination of the head
PATIENT CENTERED MEDICINE - 1 GOALS & OUTCOMES: PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY 1. To introduce the applied anatomy relevant for the examination of the head
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
NAACCR Webinar Series 1. Instructors Q&A 10/6/2011. Collecting Cancer Data: Larynx Including Mucosal Melanoma of Larynx.
 NAACCR 2011 2012 Webinar Series Collecting Cancer Data: Larynx Instructors Shannon Vann, CTR Jim Hofferkamp, CTR 2 Q&A Please submit all questions concerning webinar content through the Q&A panel. 3 NAACCR
NAACCR 2011 2012 Webinar Series Collecting Cancer Data: Larynx Instructors Shannon Vann, CTR Jim Hofferkamp, CTR 2 Q&A Please submit all questions concerning webinar content through the Q&A panel. 3 NAACCR
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S.
 Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Refresher Course EAR TUMOR. Sasikarn Chamchod, MD Chulabhorn Hospital
 Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
Nasopharyngeal Carcinoma. Rusty Stevens, MD Christopher Rassekh, MD
 Nasopharyngeal Carcinoma Rusty Stevens, MD Christopher Rassekh, MD Introduction Rare in the US, more common in Asia High index of suspicion required for early diagnosis Nasopharyngeal malignancies SCCA
Nasopharyngeal Carcinoma Rusty Stevens, MD Christopher Rassekh, MD Introduction Rare in the US, more common in Asia High index of suspicion required for early diagnosis Nasopharyngeal malignancies SCCA
PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia)
") PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia) Dr. Miriam Joy C. Calaguas Dept. of Radiation Oncology St. Luke s Medical Center
PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia) Dr. Miriam Joy C. Calaguas Dept. of Radiation Oncology St. Luke s Medical Center
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
Ultrasound Interpretation of Non-Thyroid Neck Pathology
 Ultrasound Interpretation of Non-Thyroid Neck Pathology Kevin T. Brumund, M.D., F.A.C.S. Associate Professor of Surgery Head and Neck Surgery University of California, San Diego Health Sciences VA Medical
Ultrasound Interpretation of Non-Thyroid Neck Pathology Kevin T. Brumund, M.D., F.A.C.S. Associate Professor of Surgery Head and Neck Surgery University of California, San Diego Health Sciences VA Medical
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Head and Neck Case 1 PATIENT HISTORY
 Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Head and Neck Image 頭頸部放射影像學
 Head and Neck Image 頭頸部放射影像學 陳家媛 台北醫學大學 - 市立萬芳醫院 cychen@wanfang.gov.tw Normal Suprahyoid neck: the old way Nasopharynx Oropharynx Oral cavity Staging of SCC Spaces of Suprahyoid Neck: a New Way Deep
Head and Neck Image 頭頸部放射影像學 陳家媛 台北醫學大學 - 市立萬芳醫院 cychen@wanfang.gov.tw Normal Suprahyoid neck: the old way Nasopharynx Oropharynx Oral cavity Staging of SCC Spaces of Suprahyoid Neck: a New Way Deep
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Physician to Physician AJCC 8 th Edition. Head and Neck. Summary of Changes. AJCC Cancer Staging Manual, 7 th Ed. Head and Neck Chapters
 Physician to Physician Head and Neck William M. Lydiatt, MD Chair of Surgery Nebraska Methodist Hospital Clinical Professor of Surgery, Creighton University Validating science. Improving patient care.
Physician to Physician Head and Neck William M. Lydiatt, MD Chair of Surgery Nebraska Methodist Hospital Clinical Professor of Surgery, Creighton University Validating science. Improving patient care.
Over the past 18 years, numerous classifications have been proposed to distinguish
 ORGNAL ARTCLE An maging-based Classification for the Cervical Nodes Designed as an Adjunct to Recent Clinically Based Nodal Classifications Peter M. Som, MD; Hugh D. Curtin, MD; Anthony A. Mancuso, MD
ORGNAL ARTCLE An maging-based Classification for the Cervical Nodes Designed as an Adjunct to Recent Clinically Based Nodal Classifications Peter M. Som, MD; Hugh D. Curtin, MD; Anthony A. Mancuso, MD
See the latest estimates for new cases of salivary gland cancers in the US and what research is currently being done.
 About Salivary Gland Cancer Overview and Types If you have been diagnosed with salivary gland cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to
About Salivary Gland Cancer Overview and Types If you have been diagnosed with salivary gland cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to
6 th Reprint Handbook Pages AJCC 7 th Edition
 6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Chapter 9 Head and Neck Tumors
 1 Chapter 9 Head and Neck Tumors Peter Nthumba Introduction Lesions of any size in the head and neck may have a significant effect on cosmesis, speech, respiration, and alimentation and they can significantly
1 Chapter 9 Head and Neck Tumors Peter Nthumba Introduction Lesions of any size in the head and neck may have a significant effect on cosmesis, speech, respiration, and alimentation and they can significantly
Management of Salivary Gland Malignancies. No Disclosures or Conflicts of Interest. Anatomy 10/4/2013
 Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx
 Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Cancer of the upper aerodigestive tract: assessment and management in people aged 16 and over
 Cancer of the upper aerodigestive tract: assessment and management in people aged and over NICE guideline Draft for consultation, March 0 This guideline covers This guideline covers assessing and managing
Cancer of the upper aerodigestive tract: assessment and management in people aged and over NICE guideline Draft for consultation, March 0 This guideline covers This guideline covers assessing and managing
Hypopharynx. 1. Introduction. 1.1 General Information and Aetiology
 Hypopharynx 1. Introduction 1.1 General Information and Aetiology The human pharynx is the part of the throat situated between the nasal cavity and the esophagus and can be divided into three parts: the
Hypopharynx 1. Introduction 1.1 General Information and Aetiology The human pharynx is the part of the throat situated between the nasal cavity and the esophagus and can be divided into three parts: the
Esophagus Stomach 4/2/15
 Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Diseases of oral cavity
 Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
NAACCR Webinar Series 11/2/2017
 COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
3/12/2018. Head & Neck Cancer Review INTRODUCTION
 Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 4/30/2011 Radiology Quiz of the Week # 18 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 4/30/2011 Radiology Quiz of the Week # 18 Page 1 CLINICAL PRESENTATION AND RADIOLOGY