Hyperparathyroidism. When to Suspect, How to Diagnose, When and How to Intervene. Johanna A. Pallotta, MD, FACP, FACE
|
|
|
- Claude Murphy
- 6 years ago
- Views:
Transcription
1 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE
2 Potential conflicts of interest: None Johanna A. Pallotta, MD
3 Outline Definition of hyperparathyroidism (Primary, Secondary, Tertiary) Primary Hyperparathyroidism Changing presentation of primary hyperparathyroidism Clinical manifestations of primary hyperparathyroidism Indications for surgery Localization techniques for primary hyperparathyroidism Surgical techniques for primary hyperparathyroidism Management for ongoing hyperparathyroidism


 Gut 1 alpha")


4 Calcium Homeostasis Calcium Vitamin D Bicarbonate + Bone CALCIUM + + Parathyroid Hormone (PTH) Gut 1 alpha Hydroxylase + Liver Skin/Gut 1,25-Dihydroxy Vitamin D Kidney 25-Hydroxy Vitamin D 25-alpha Hydroxylase Vitamin D
5 Hypercalcemia Hyperparathyroidism When to Suspect Routine labs (asymptomatic patients) Bone density changes Nephrolithiasis Other causes of hypercalcemia: Malignancy, granulomatous disease, vitamin intoxication (A,D), medications (lithium, thiazides, calcium, theophylline), hyperthyroidism, immobilization Elevated PTH in the setting of hypercalcemia = hyperparathyroidism
6 1 0 Hyperparathyroidism 80-85% caused by a single adenoma 15 20% caused by 4-gland hyperplasia or double adenomas 0.5 2% caused by parathyroid carcinoma Treatment is surgical removal of enlarged, hypercellular gland(s)
7 1 0 Hyperparathyroidism 1. Establish diagnosis 2. Review indications for surgery 3. Localize abnormal gland(s) 4. Operate Keep in this order!

8 Captain Martell First patient diagnosed with hyperparathyroidism 1918


9 Bone Disease in Hyperparathyroidism


10 Berson and Yalow

11 Changing Presentation of Primary HPT Silverberg et al. Am J Med 1990;89:327
12 1 0 Hyperparathyroidism Clinical Manifestations Asymptomatic Kidney stones Polyuria Depression Memory loss Fatigue Constipation Osteoporosis Calciphylaxis Hypercalcemic crisis Musculoskeletal pain Peptic ulcers Pancreatitis Brown tumors
13 1 0 Hyperparathyroidism Diagnosis Elevated calcium and PTH levels Note normocalcemic hyperparathyroidism Low phosphorous level 24 hour urine calcium level Normal or elevated FHH (24 hour level < 100 mg) Low Ca/Cr ratio Genetic testing available Vitamin D levels
14 FHH Familial hypocalcuric hypercalcemia Gene mutation for the CaSR AD with high penetrance Mildly elevated serum Ca and PTH Low urinary calcium excretion (<100 mg/day) Calculate Ca/Cr clearance ratio Ca/Cr Clearance = <0.01
15 Indications for Parathyroid Surgery in Asymptomatic HPT New Guidelines Serum calcium > 1 mg/dl above normal Low bone density (T score < -2.5 L. spine, total hip, femoral neck, distal 1/3 radius) Vertebral fracture on films (x-ray, CT, MRI, VFA) Decreased renal fxn GFR < 60 ml/min 24 h urine Ca > 400 mg, stones (x-ray, U/S, CT), increased stone risk on biochemical analysis Age < 50 Bilezikian et al. Guidelines for the Management of Asymptomatic Primary Hyperparathyroidism: Summary Statement from the 4 th International Workshop. JCEM 2014.
16 Bilezikian et al. JCEM. October 2014
17 Indications for Parathyroid Surgery Other Things to Consider Neuropsychiatric symptoms and QOL Bone density and fracture risk Data confirms improvement s/p surgery Cardiovascular disease and survival Age and operative risk
18 Changes in Bone Density Over Time in Patients Who Undergo Observation Versus Surgery Silverberg et al JCEM 94:351.
19 Normocalcemic Hyperparathyroidism 62 yo female Ca 10.3, ionized 1.30 [normal range: ] PTH 85 Bone density femoral neck -2.2, spine -2.6 U/S: Heterogeneous thyroid c/w Hashimoto's. No obvious parathyroid adenoma. Small hypoechoic lesion right lower pole mildly suspicious for an enlarged parathyroid gland Sestamibi scan negative Does this patient have HPT? Is surgery likely to have a positive impact? Is a neck exploration warranted?
20 37 patients Average age 58 (range 32 to 78) Calcium 9.4 +/- 0.1 (SEM), PTH 93 +/-5 7 patients (19%) became hypercalcemic, all within three years Some persistently normocalcemic patients developed evidence for progressive hyperparathyroid disease
21 Normocalcemic hyperparathyroidism Considerations at the initial presentation.. Exclude all possible causes of secondary hyperparathyroidism. Take a detailed history, including h/o fragility fractures, recurrent nephrolithiasis and use of thiazides or lithium Laboratory studies: 25-OH vitamin D level renal function urine calcium excretion serum phosphorus
22 Prevalence of Normocalcemic Hyperparathyroidism Cusano et al., Journal of Clin Dens 2013

23 Relation between vitamin D and PTH Singhellakis et al. Hormones 2011
24 Ongoing Care of Hyperparathyroidism
25 If No Indication For Surgery How to Follow? Bilezikian et al. JCEM. October 2014
26 Management of Patients with Ongoing Hyperparathyroidism Continue to follow patient closely Hydration and exercise Calcium (1000 to 1200 mg/day) Don t cut out all calcium from the diet. Vitamin D - keep level >30 ng/ml ( IU/day) Avoid drugs that increase Ca (eg. Lithium, Thiazides)
27 Medications to Control Ca, PTH and Preserve Bone Density Calcitonin for acute hypercalcemia Bisphosphonates Zoledronic acid and pamidronate (IV, for acute Rx) Alendronate and risedronate (oral, for long term Rx) Cinacalcet Inhibits PTH secretion and drops Ca level No effect on BMD Increases urinary calcium excretion


28 Cinacalcet Effects on Calcium and PTH Peacock et al JCEM Jan;96(1):E9-18.

29 Parathyroid Locations Kronenberg H. Williams Textbook of Endocrinology, 11 th Edition.
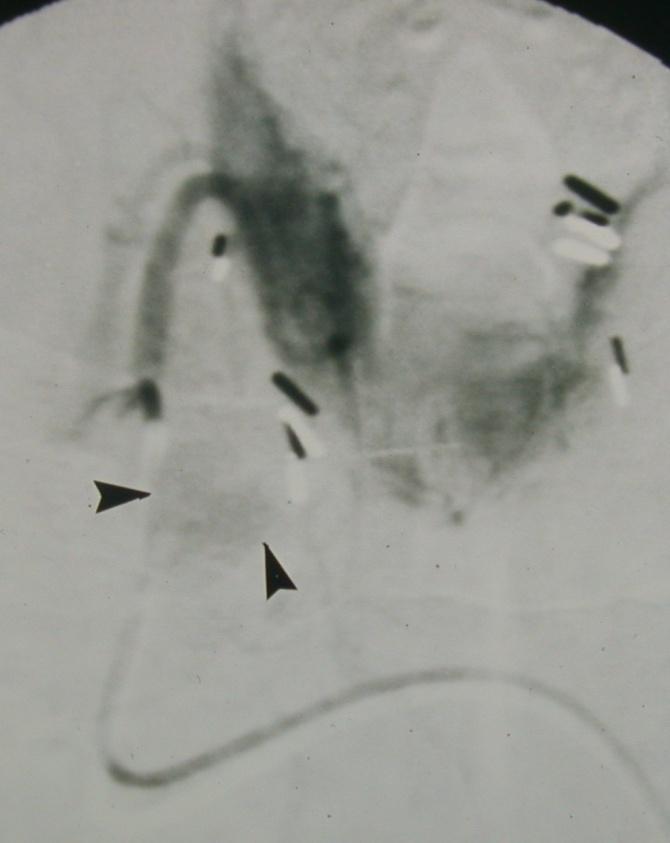
30 Failed Parathyroid Exploration 41 yo woman presents after failed parathyroid exploration During first pregnancy, developed intractable kidney stones and noted to be hypercalcemic (10.3) PTH 143, Ph 2.7, 25OHD 29 At 28 weeks, she underwent parathyroid exploration During surgery: 2 glands were removed, a total thyroidectomy was done along with a cervical thymectomy without obvious parathyroid adenoma
31 Failed Parathyroid Exploration Pathology of glands removed was normal Referred to us Non-invasive studies including sestamibi and U/S were negative Vein catheterization was done


32 Venous Sampling
33 Selective Venous Sampling for Patient VW 09/29/ :25 #1 RT SUPERIOR 71* #2 LOW RT SUPERIOR 82* #3 ORIGIN RIGHT VERTEBRAL 70* #4 LEFT VERTEBRAL 94* #5 LEFT SUPERIOR 83* # 6 LOW LEFT SUPERIOR 82* #7 LEFT INTERNAL MAMMARY 81* #8 THYMIC 67* #9 THYMIC >5000* #10 COMMON INFERIOR TRUNK 260* #11 LEFT SIDE LEFT INOMINATE 83* #12 MID LEFT INOMINATE 80* #13 RT SIDE LEFT INOMINATE 470* #14 RT INOMINATE 165* #15 SVC 207*




34 Right internal mammary artery 2 3 Final images after ablation 6 1 Parathyroid adenoma Subselective catheterization Parathyroid adenoma Coils V.W. Parathyroid ablation 4 5 Persistent staining Adenoma prior to starting ablation Adenoma after contrast ablation-note swelling





35 Selective left inferior thyroid Superselective injection Coils following ablation Mediastinal adenoma Post angiography Post injection of Hyperosmolar contrast Selective arteriography and ablation


36 1. 2a. 2b. 3. Arterial phase Tissue phase Arteriogram
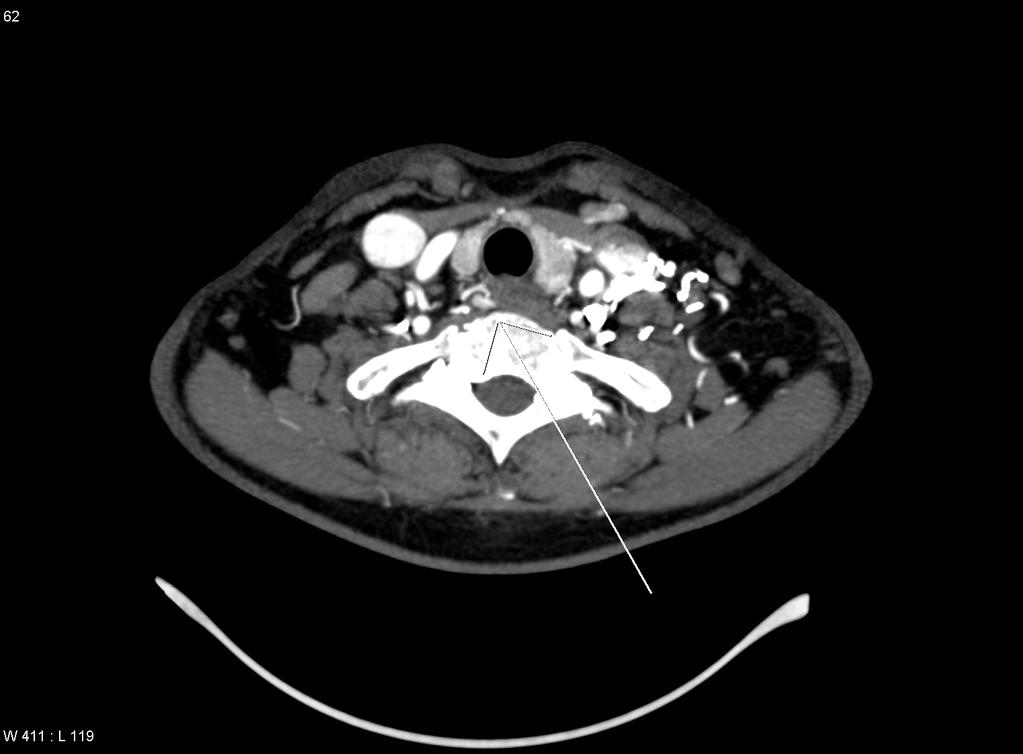
37 Case # 3 M.T. 63 yo female Dx with primary HPT Neck exploration March 2006 Pre-op sestamibi right lower gland Enlarged right lower gland removed Pathology hypercellular Identified 3 normal glands iopth remained elevated
38 Post-operative labs Calcium PTH 142 Case # 3 M.T. 63 yo female Bone density osteoporosis Symptoms Extreme fatigue, bone/joint pain
39 Case # 3 M.T. 63 yo female Sestamibi and U/S negative Venous sampling c/w right sided lesion
40 Patient M.T. 63 yo female What next?
41

42
43 Case # 3 M.T. 63 yo female Focused exploration Parathyroid adenoma TE groove at the level of the thoracic inlet Blood supply arising superiorly Likely descended right upper gland Intraoperative PTH 215 to 9 Post-operative labs Ca 9.5, PTH 26
44 Take Home Points Parathyroid disease is a biochemical diagnosis Imaging should be reserved for when you are planning on taking the patient to surgery U/S, sestamibi, and 4D-CT scan are the first line imaging modalities to locate a parathyroid adenoma Only experienced parathyroid surgeons should be used
45 Take Home Points Patients who require only medical follow up need close observation Difficult cases require referral for more sophisticated diagnostic studies Don t rush patients to surgery if unsure of diagnosis or indications If you don t know what to do, don t do anything -Robert Loeb, MD
46 Acknowledgements Long-standing collaborators: Dr. Barry Sacks Dr. Harvey Eisenberg Endocrine Fellows Patients
47 Question 1 Chose the answer that includes, in all 3 listed, indications for surgery in primary HPT, as outlined in the recent consensus conference: A. Osteoporosis, hypercalcuria, calcium > 11 B. Osteoporosis, age < 50, calcium > 12 C. Osteopenia, kidney stones, musculoskeletal pain
48 Question 2 The best laboratory data supporting the diagnosis of primary HPT is: A. calcium, PTH, albumin, phosphorous B. calcium, albumin, PTH, phosphorous, 24-hour urine calcium, vitamin D C. calcium, albumin, phosphorous, vitamin D
49 Question 3 Treatment recommendation for normocalcemic hyperparathyroidism: A. Cinecalcet and bisphosphonates B. Surgical exploration C. Close monitoring for progression of disease and complications
50 Question for Panel The patient has a high calcium level and hyperparathyroidism, and you suggest that they take 1000mg of calcium daily, preferably in their diet. When they question your recommendation based on their high calcium level, how do you answer them?
Potential conflicts of interest: None
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
Clinical Approach to Hypercalcemia For the Primary Care Provider
 Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones
 Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Parathyroid Imaging. A Guide to Parathyroid Surgery
 Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Hypercalcemia & Parathyroid Disorders. W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology
 Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Parathyroid Disease Scenarios for the Practicing Clinician. Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix
 Parathyroid Disease Scenarios for the Practicing Clinician Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix Clinical Scenario-1 73 year man (BK) with hypercalcemia
Parathyroid Disease Scenarios for the Practicing Clinician Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix Clinical Scenario-1 73 year man (BK) with hypercalcemia
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Primary Hyperparathyroidism
 Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Hypercalcemia. Brian Rose, M.D. Bozeman Health June 6, 2018
 Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Hypercalcemia. Hypercalcemia: When to Worry, When to Treat! Mineral Metabolism : A Short Course
 Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
4/20/2015. The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy. Learning Objectives
 Testing During Surgical Parathyroidectomy. Learning Objectives") The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
Calcium and Parathyroid Disorders
 Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Since the advent of multichannel serum chemistry
 ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy
 "Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
Minimally invasive parathyroidectomy
 Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
International Journal of Biological & Medical Research. An Uncommon Case of Persistent Hypercalcaemia following Parathyroid Surgery
 Int J Biol Med Res.2015;6(4):5336-5340 Int J Biol Med Res www.biomedscidirect.com Volume 6, Issue 2, April 2015 Contents lists available at BioMedSciDirect Publications International Journal of Biological
Int J Biol Med Res.2015;6(4):5336-5340 Int J Biol Med Res www.biomedscidirect.com Volume 6, Issue 2, April 2015 Contents lists available at BioMedSciDirect Publications International Journal of Biological
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
HYPERCALCAEMIA 101 FOR THE INTERNIST
 HYPERCALCAEMIA 101 FOR THE INTERNIST Dr Chionh Siok Bee Dept of Medicine, National University Hospital siok_bee_chionh@nuhs.edu.sg Medicine Review Course 18/09/2011 Outline of Talk Definition of hypercalcaemia
HYPERCALCAEMIA 101 FOR THE INTERNIST Dr Chionh Siok Bee Dept of Medicine, National University Hospital siok_bee_chionh@nuhs.edu.sg Medicine Review Course 18/09/2011 Outline of Talk Definition of hypercalcaemia
Disclosure. Primary Hyperparathyroidism 4 th IW. Topic Outline. Calcium, Vitamin D, PTH Disorders. I have nothing to disclose related to this topic
 Disclosure Calcium, Vitamin D, PTH Disorders Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF I have nothing to disclose related to this topic Topic Outline Calcium/Vitamin
Disclosure Calcium, Vitamin D, PTH Disorders Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF I have nothing to disclose related to this topic Topic Outline Calcium/Vitamin
Diagnosis and Treatment of Primary Hyperparathyroidism. Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic
 Diagnosis and Treatment of Primary Hyperparathyroidism Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Disclosure Nothing to Disclose Primary HPT Autonomous secretion of
Diagnosis and Treatment of Primary Hyperparathyroidism Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Disclosure Nothing to Disclose Primary HPT Autonomous secretion of
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
UPDATES ON PRIMARY HYPERPARATHYROIDISM. Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY
 UPDATES ON PRIMARY HYPERPARATHYROIDISM Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY Disclosures Speaker (Honorarium): Shire Off-label use of estrogen, raloxifene
UPDATES ON PRIMARY HYPERPARATHYROIDISM Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY Disclosures Speaker (Honorarium): Shire Off-label use of estrogen, raloxifene
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Parathyroid surgery at Massachusetts General Hospital: Information for patients and families
 Parathyroid surgery at Massachusetts General Hospital: Information for patients and families We are pleased that you have chosen Massachusetts General Hospital to receive treatment for your parathyroid
Parathyroid surgery at Massachusetts General Hospital: Information for patients and families We are pleased that you have chosen Massachusetts General Hospital to receive treatment for your parathyroid
Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease
 Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease Mira Milas MD, FACS Professor of Surgery Director of Endocrine Surgery No conflicts of interest or financial
Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease Mira Milas MD, FACS Professor of Surgery Director of Endocrine Surgery No conflicts of interest or financial
Disclosure. Topic Outline. Calcium, Vitamin D, PTH Disorders. PTH/Calcium-Normal Physiology. I have nothing to disclose
 Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Calcium Nephrolithiasis and Bone Health. Noah S. Schenkman, MD
 Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Cases in Endocrinology
 Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
David Bruyette, DVM, DACVIM
 VCAwestlaspecialty.com David Bruyette, DVM, DACVIM Disorders of calcium metabolism are common endocrine disorders in both dogs and cats. In this article we present a logical diagnostic approach to patients
VCAwestlaspecialty.com David Bruyette, DVM, DACVIM Disorders of calcium metabolism are common endocrine disorders in both dogs and cats. In this article we present a logical diagnostic approach to patients
When the level of calcium in the blood falls too low, the parathyroid glands secrete just enough PTH to restore the blood calcium level.
 Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Calcium Conundrums. California Chapter AACE. September 2015
 Calcium Conundrums California Chapter AACE September 2015 Michael W. Yeh, MD Chief, Section of Endocrine Surgery Associate Professor of Surgery and Medicine David Geffen School of Medicine at UCLA www.endocrinesurgery.ucla.edu
Calcium Conundrums California Chapter AACE September 2015 Michael W. Yeh, MD Chief, Section of Endocrine Surgery Associate Professor of Surgery and Medicine David Geffen School of Medicine at UCLA www.endocrinesurgery.ucla.edu
Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012.
 Levels Shireen Fatemi, M.D. April, 2012.") Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012 Disclosures I have no financial relationships with commercial interests,
Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012 Disclosures I have no financial relationships with commercial interests,
The parathyroid glands participate in the regulation
 41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
Challenges in the Management of Primary HPTH. Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH
 Challenges in the Management of Primary HPTH Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH Case Presentation 1 This a case of a 41-year-old gentleman who is referred to Endocrinology clinic for low BMD,
Challenges in the Management of Primary HPTH Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH Case Presentation 1 This a case of a 41-year-old gentleman who is referred to Endocrinology clinic for low BMD,
Hyperparathyroidism (primary): diagnosis, assessment and initial management
: diagnosis, assessment and initial management") National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
Outline. Parathyroid Localization Studies. Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center
 Parathyroid Localization Studies Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center Outline Clinical Context of Primary Hyperparathyroidism Ultrasound, Sestamibi, and Other
Parathyroid Localization Studies Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center Outline Clinical Context of Primary Hyperparathyroidism Ultrasound, Sestamibi, and Other
2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT)
") 2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT) Scott M. Wilhelm, MD, FACS Associate Professor and Section Head Endocrine Surgery University Hospitals-Cleveland
2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT) Scott M. Wilhelm, MD, FACS Associate Professor and Section Head Endocrine Surgery University Hospitals-Cleveland
Calcium metabolism and the Parathyroid Glands. Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands
 Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Case study Group 2 presentation
 Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
Summary Statement from a Workshop on Asymptomatic Primary Hyperparathyroidism: A Perspective for the 21st Century
 Summary Statement from a Workshop on Asymptomatic Primary Hyperparathyroidism: A Perspective for the 21st Century John P. Bilezikian, John T. Potts, Jr., Ghada El-Hajj Fuleihan, Michael Kleerekoper, Robert
Summary Statement from a Workshop on Asymptomatic Primary Hyperparathyroidism: A Perspective for the 21st Century John P. Bilezikian, John T. Potts, Jr., Ghada El-Hajj Fuleihan, Michael Kleerekoper, Robert
301 S. Westfield Rd., Suite 250 Madison, WI See inside for information about our Endocrine Surgery Referral Program
 301 S. Westfield Rd., Suite 250 Madison, WI 53717 See inside for information about our Endocrine Surgery Referral Program December 2017 Dear Colleague, Thank you for referring your patient(s) to UW Health
301 S. Westfield Rd., Suite 250 Madison, WI 53717 See inside for information about our Endocrine Surgery Referral Program December 2017 Dear Colleague, Thank you for referring your patient(s) to UW Health
Hypercalcemia may be detected incidentally. Practice CMAJ. Primary hyperparathyroidism. Primer. Key points. The case. What causes hypercalcemia?
 CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
Primary hyperparathyroidism
 How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Pathophysiology Clinical features Investigations Management Prognosis Special cases Case study
How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Pathophysiology Clinical features Investigations Management Prognosis Special cases Case study
Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from the West?
 ecommons@aku Section of Urology Department of Surgery August 1999 Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from
ecommons@aku Section of Urology Department of Surgery August 1999 Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from
Iperparatiroidismo normocalcemico: vero o falso?
 Iperparatiroidismo normocalcemico: vero o falso? Bari, 7-10 novembre 2013 TERAPIA E FOLLOW-UP A. Piovesan SCDU Endocrinologia Oncologica AO Città della Salute e della Scienza Molinette Torino THE THIRD
Iperparatiroidismo normocalcemico: vero o falso? Bari, 7-10 novembre 2013 TERAPIA E FOLLOW-UP A. Piovesan SCDU Endocrinologia Oncologica AO Città della Salute e della Scienza Molinette Torino THE THIRD
Posttransplant Bone Disease. Budapest 2007
 Posttransplant Bone Disease Budapest 2007 Post-transplant bone disease 7 10 % of kidney transplanted patients develope a fracture. The risk is higher in postmenopausal female transplanted patients. Diabetic,
Posttransplant Bone Disease Budapest 2007 Post-transplant bone disease 7 10 % of kidney transplanted patients develope a fracture. The risk is higher in postmenopausal female transplanted patients. Diabetic,
Secondary and Familial Hyperparathyroidism
 Secondary and Familial Jeffrey F. Moley, M.D. Chief, Endocrine and Oncologic Surgery Section, Professor of Surgery Associate Director, The Alvin J. Siteman Cancer Center Occurs in setting of CRF Chronic
Secondary and Familial Jeffrey F. Moley, M.D. Chief, Endocrine and Oncologic Surgery Section, Professor of Surgery Associate Director, The Alvin J. Siteman Cancer Center Occurs in setting of CRF Chronic
Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand
 International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
Parathyroid Imaging What is best
 Parathyroid Imaging What is best Mike Avison Bradford Why me? I m honoured to be asked to present this. There is no killer paper or text which clearly proves the best methodology. Bradford has performed
Parathyroid Imaging What is best Mike Avison Bradford Why me? I m honoured to be asked to present this. There is no killer paper or text which clearly proves the best methodology. Bradford has performed
Normocalcemic Primary Hyperparathyroidism: A Comparison with the Hypercalcemic Form in a Tertiary Referral Population
 Pierreux Jan, Bravenboer Bert. Normocalcemic Primary Hyperparathyroidism: A Horm Metab Res 2018; 00: 00 00 Normocalcemic Primary Hyperparathyroidism: A Comparison with the Hypercalcemic Form in a Tertiary
Pierreux Jan, Bravenboer Bert. Normocalcemic Primary Hyperparathyroidism: A Horm Metab Res 2018; 00: 00 00 Normocalcemic Primary Hyperparathyroidism: A Comparison with the Hypercalcemic Form in a Tertiary
Parathyroidectomy. Surgery for Parathyroid Problems
 Parathyroidectomy Surgery for Parathyroid Problems Why You Need Parathyroid Surgery Has your doctor just recommended that you have parathyroid surgery? If so, you likely have many questions. What are the
Parathyroidectomy Surgery for Parathyroid Problems Why You Need Parathyroid Surgery Has your doctor just recommended that you have parathyroid surgery? If so, you likely have many questions. What are the
Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma
 ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP
 Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP Endocrine in 25 Minutes Joshua S. Coren, D.O., MBA, FACOFP Vice Chair and Associate Professor, Family Medicine Rowan University School
Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP Endocrine in 25 Minutes Joshua S. Coren, D.O., MBA, FACOFP Vice Chair and Associate Professor, Family Medicine Rowan University School
Osteoporosis Treatment Overview. Colton Larson RFUMS October 26, 2018
 Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Endocrine Surgery When to Refer and What We Do
 Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Supplementary Online Content
 Supplementary Online Content Wilhelm SM, Wang TS, Ruan DT, et al. The American Association of Endocrine Surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg. Published
Supplementary Online Content Wilhelm SM, Wang TS, Ruan DT, et al. The American Association of Endocrine Surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg. Published
80 year old female with parathyroid mass and refractory hypercalcemia. Endorama September 24 th, 2015 Rajesh Jain
 80 year old female with parathyroid mass and refractory hypercalcemia Endorama September 24 th, 2015 Rajesh Jain HPI 80 F with pulmonary hypertension, rheumatic mitral stenosis, atrial fibrillation on
80 year old female with parathyroid mass and refractory hypercalcemia Endorama September 24 th, 2015 Rajesh Jain HPI 80 F with pulmonary hypertension, rheumatic mitral stenosis, atrial fibrillation on
New 2010 Osteoporosis Guidelines: What you and your health provider need to know QUESTIONS&ANSWERS
 New 2010 Osteoporosis Guidelines: What you and your health provider need to know QUESTIONS&ANSWERS Wednesday, December 1, 2010 1:00 p.m. to 2:00 p.m. ET 1. I m 55 years old. I ve been taking Fosavance
New 2010 Osteoporosis Guidelines: What you and your health provider need to know QUESTIONS&ANSWERS Wednesday, December 1, 2010 1:00 p.m. to 2:00 p.m. ET 1. I m 55 years old. I ve been taking Fosavance
Ca, Mg metabolism, bone diseases. Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary
 Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
PRIMARY HYPERPARATHYROIDISM WITH RICKETS. KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College
 PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
Clinical biochemistry of calcium and vitamin D
 Clinical biochemistry of calcium and vitamin D Dr Andrew Day Consultant in Clinical Biochemistry and Metabolic Medicine University Hospitals Bristol NHS Trust e-mail: andrew.day@uhbristol.nhs.uk A 48-year
Clinical biochemistry of calcium and vitamin D Dr Andrew Day Consultant in Clinical Biochemistry and Metabolic Medicine University Hospitals Bristol NHS Trust e-mail: andrew.day@uhbristol.nhs.uk A 48-year
Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease?
 Ann Surg Oncol (2011) 18:3437 3442 DOI 10.1245/s10434-011-1744-x ORIGINAL ARTICLE ENDOCRINE TUMORS Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease? Amanda L. Amin, MD, Tracy S.
Ann Surg Oncol (2011) 18:3437 3442 DOI 10.1245/s10434-011-1744-x ORIGINAL ARTICLE ENDOCRINE TUMORS Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease? Amanda L. Amin, MD, Tracy S.
Primary hyperparathyroidism (PHPT) CE/CME. Barbara Austin, MSN, ARNP, FNP-BC
 CE/CME. Barbara Austin, MSN, ARNP, FNP-BC") Primary Hyperparathyroidism A Case-based Review Primary hyperparathyroidism (PHPT) is most often detected as hypercalcemia in an asymptomatic patient during routine blood work. Knowing the appropriate
Primary Hyperparathyroidism A Case-based Review Primary hyperparathyroidism (PHPT) is most often detected as hypercalcemia in an asymptomatic patient during routine blood work. Knowing the appropriate
Agents that Affect Bone & Mineral Homeostasis
 Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Talking to patients with osteoporosis about initiating therapy
 Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Awaisheh. Mousa Al-Abbadi. Abdullah Alaraj. 1 Page
 f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus
 Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus The Harvard community has made this article openly available. Please
Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus The Harvard community has made this article openly available. Please
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Biopsy needle, thyroid gland, 74 technique, Bone hunger syndrome, 23
 The following figures were reproduced by permission, courtesy of the Mayo Clinic: Figures 2-7, 2-l4a, 2-l5a, 2-l5c, 2-l6a, 2-l8a, 3-l5a, 3-21a The following figure was slightly modified and reproduced
The following figures were reproduced by permission, courtesy of the Mayo Clinic: Figures 2-7, 2-l4a, 2-l5a, 2-l5c, 2-l6a, 2-l8a, 3-l5a, 3-21a The following figure was slightly modified and reproduced
HPI joint pain/arthritis serum calcium 11.5 PTH 147pg/ml
 HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
Current Management of Metastatic Bone Disease
 Current Management of Metastatic Bone Disease Evaluation and Medical Management Dr. Sara Rask Head, Medical Oncology Simcoe Muskoka Regional Cancer Centre www.rvh.on.ca Objectives 1. Outline an initial
Current Management of Metastatic Bone Disease Evaluation and Medical Management Dr. Sara Rask Head, Medical Oncology Simcoe Muskoka Regional Cancer Centre www.rvh.on.ca Objectives 1. Outline an initial
Guideline for the investigation and management of osteoporosis. for hospitals and General Practice
 Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Primary Hyperparathyroidism
 November 2002 Primary Hyperparathyroidism Lori Coburn, Harvard Medical School Year III Hyperparathyroidism An increase in parathyroid hormone (PTH) production Divided into Primary, Secondary and Tertiary
November 2002 Primary Hyperparathyroidism Lori Coburn, Harvard Medical School Year III Hyperparathyroidism An increase in parathyroid hormone (PTH) production Divided into Primary, Secondary and Tertiary
PARATHYROID IMAGING. James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center
 PARATHYROID IMAGING James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center NO DISCLOSURES Overview The hallmarks of the ideal test Benefits
PARATHYROID IMAGING James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center NO DISCLOSURES Overview The hallmarks of the ideal test Benefits
Acute renal failure and unknown cause hypercalcemia (case report)
") Acute renal failure and unknown cause hypercalcemia (case report) Clinic for hemodialysis CCU Sarajevo ... What is hypercalcemia??? ... What is hypercalcemia??? The definition of hypercalcemia is having
Acute renal failure and unknown cause hypercalcemia (case report) Clinic for hemodialysis CCU Sarajevo ... What is hypercalcemia??? ... What is hypercalcemia??? The definition of hypercalcemia is having
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
The mystery of the hidden parathyroid adenoma. Case #1. Imaging. Case of missed adenoma. Ultrasound false nega9ves. Case of missed adenoma 5/16/16
 The mystery of the hidden parathyroid adenoma AACE Annual Mee+ng 2016 Orlando, FL Case #1 Moderator: Panel: Jennifer L Mar+ MD FACS Endocrine Surgery NYC Azeez Farooki MD Endocrinology MSKCC Peter Sadow
The mystery of the hidden parathyroid adenoma AACE Annual Mee+ng 2016 Orlando, FL Case #1 Moderator: Panel: Jennifer L Mar+ MD FACS Endocrine Surgery NYC Azeez Farooki MD Endocrinology MSKCC Peter Sadow
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
76 year-old female presents with muscle cramps. Jess Hwang 12/6/12
 76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
ORIGINAL ARTICLE. Persistent Parathyroid Hormone Elevation Following Curative Parathyroidectomy for Primary Hyperparathyroidism
 Persistent Parathyroid Hormone Elevation Following Curative Parathyroidectomy for Primary Hyperparathyroidism Elizabeth A. Mittendorf, MD; Christopher R. McHenry, MD ORIGINAL ARTICLE Background: Persistent
Persistent Parathyroid Hormone Elevation Following Curative Parathyroidectomy for Primary Hyperparathyroidism Elizabeth A. Mittendorf, MD; Christopher R. McHenry, MD ORIGINAL ARTICLE Background: Persistent
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Aromatase Inhibitors & Osteoporosis
 Aromatase Inhibitors & Osteoporosis Miss Sarah Horn Consultant Oncoplastic Breast Surgeon April 2018 Aims Role of Aromatase Inhibitors (AI) in breast cancer treatment AI s effects on bone health Bone health
Aromatase Inhibitors & Osteoporosis Miss Sarah Horn Consultant Oncoplastic Breast Surgeon April 2018 Aims Role of Aromatase Inhibitors (AI) in breast cancer treatment AI s effects on bone health Bone health
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Bone Densitometry Pathway
 Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
News on the treatment of HPT
 News on the treatment of HPT G.C. Torre XIV Annual Conference of EES Tourin 25-27 November 2010 Epidemiology Prevalence: Sweeden = 4.3 /1000 Norway = 3/1000 Finland = 21/1000 USA = 1/1000 Italy = 5/1000
News on the treatment of HPT G.C. Torre XIV Annual Conference of EES Tourin 25-27 November 2010 Epidemiology Prevalence: Sweeden = 4.3 /1000 Norway = 3/1000 Finland = 21/1000 USA = 1/1000 Italy = 5/1000
Case. IRIM 2012: Calcium Cases. Case. Case. Distribution of Calcium. Question: What Test Would You Order Next?
 IRIM 2012: Calcium Cases Carolyn Becker MD Brigham and Women s Hospital Harvard Medical School Case A 65 yo man with multiple myeloma is admitted with pneumonia and sepsis. Exam: febrile, BP 80/60, P 120,
IRIM 2012: Calcium Cases Carolyn Becker MD Brigham and Women s Hospital Harvard Medical School Case A 65 yo man with multiple myeloma is admitted with pneumonia and sepsis. Exam: febrile, BP 80/60, P 120,