Functional Pituitary Adenomas. Fawn M. Wolf, MD 2/2/2018
|
|
|
- Egbert Gallagher
- 6 years ago
- Views:
Transcription
1 Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018
2 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas
3 Hyperprolactinemia Clinically apparent prolactinomas: 5-50/100,000 Hypogonadism Prolactin inhibits gonadotropin release Full spectrum of severity Leads to bone loss (trabecular) Galactorrhea
4 Causes of Hyperprolactinemia Physiology: pregnancy, lactation, chest wall stimulation, intercourse Medications: dopamine antagonists, estrogen, opiates, marijuana Pituitary: prolactinoma, non-prolactinoma pituitary disease Renal failure (PRL not cleared by dialysis) Primary hypothyroidism (elevated TRH; may be accompanied by pituitary hyperplasia)
5 Diagnosis of Prolactinomas Serum draw, any time of day Avoid chest wall stimulation, sexual intercourse, intense exercise for 24 hours prior Serial dilution of serum samples eliminates the hook effect; consider when a large adenoma is accompanied by a mildly elevated prolactin >500 mcg/l diagnostic for macroprolactinoma mcg/l likely macroprolactinoma, but occasionally risperidone and metoclopramide can cause PRLs in the 200s mcg/l: prolactinoma vs non-tumor causes <95 mcg/l: microprolactinoma, non-functioning adenoma, or nontumor causes Macroadenomas leading to stalk inhibition as the cause of hyperprolactinemia typically lead to PRLs < 95 mcg/l
6 Drug Induced Hyperprolactinemia Usually associated with PRL mcg/l, occasionally into 200s with metoclopramide, risperidone, phenothiazines Prolactin should normalize within 3 days of holding the suspicious medication Obtain MRI if drug cannot be held or if onset of hyperprolactinemia does not coincide with therapy initiation 40-90% of patients on typical anti-psychotics will have hyperprolactinemia May be symptomatic (galactorrhea, hypogonadism, bone loss) If symptomatic, consider switch to alternative therapy or administration of replacement estrogen/testosterone
7 Prolactinomas: Treatment Dopamine agonists are mainstay of therapy Cabergoline is first line Side effects: headache, nausea, light-headedness Normalization of prolactin in 80-99% of patients Resolution of hypogonadism in majority of patients Tumor shrinkage in 80-90% patients Bromocriptine is second line More of the same side effects Cost is similar Lower efficacy for outcomes Consider surgery for rapid visual loss
8 Microprolactinomas Rarely progress to macroprolactinomas Asymptomatic: no treatment necessary If symptomatic: Females desiring pregnancy or males: cabergoline Females not desiring pregnancy: cabergoline OR combined oral contraceptive
9 Acromegaly Rare: annual incidence of six per million people Mean age at diagnosis years If GH rises prior to epiphyseal growth plate fusion, then this leads to pituitary gigantism Vast majority of cases are due to excess GH secretion from a pituitary adenoma Insidious onset: in hindsight, symptoms begin on average 12 years prior to diagnosis
10 Acromegaly: Clinical Features Clinical features due to excess of both GH and IGF-1 Overgrowth of many tissues: connective tissue, cartilage, bone, skin, visceral organs Cardiovascular disease and sleep apnea Metabolic disorders Colon neoplasia
11 Acromegaly: Clinical Features Soft tissue: hands, feet (ring/shoe size), tongue (macroglossia), nerve impingements (carpal tunnel), pharynx/larynx (sleep apnea in 50-70%) Bone: coarse facial features, enlarged jaw (macronathia), teeth spread apart, dental malocclusions, increase in BMD Skin: skin thickens (difficult venipuncture), skin tags, excessive sweating, hirsutism Joints: hypertrophic arthropathy Viscera: thyroid (goiter +/- nodules)
12 Acromegaly: Clinical Features Cardiovascular: HTN, LVH, diastolic dysfunction Metabolic: insulin resistance, DM2, hypertriglyceridemia Colon neoplasms: questionable increase in rates of colon cancer, but definite increase in colonic polyps as well as death from colon cancer Mortality: overall standard mortality ratio of 1.72, down to 1.09 following biochemical cure
13 When to Suspect Acromegaly Combination of DM2, sleep apnea, arthritis/tendonitis, especially if BMI is normal or in the absence of a FH of DM2 New dental malocclusions Heat intolerance, sweating Hand/foot swelling

14 When to Suspect Acromegaly Combination of DM2, sleep apnea, arthritis/tendonitis, especially if BMI is normal or in the absence of a FH of DM2 New dental malocclusions Heat intolerance, sweating Hand/foot swelling


15 75 yo white female with prior HTN, pre-dm, noted to have facial features of acromegaly During a hospitalization for diverticulitis. IGF-1 760, GH 20, MRI showed 1.8cm sellar mass. Underwent transphenoidal resection with residual disease post-operatively, in remission Now on medical therapy (pegvisomant). 81 years young now and doing great!
16 Acromegaly: Diagnosis Biochemical diagnosis, not a clinical diagnosis Screening IGF-1 Nearly always elevated in patients with acromegaly Few physiologic causes of high IGF-1: puberty and pregnancy Many causes of low IGF-1: hypothyroidism, malnutrition, uncontrolled DM, liver/kidney failure, oral estrogen use Confirmation: 75g oral glucose tolerance. At 2 hours, GH < 1 ng/ml rules out acromegaly. Pituitary MRI for localization
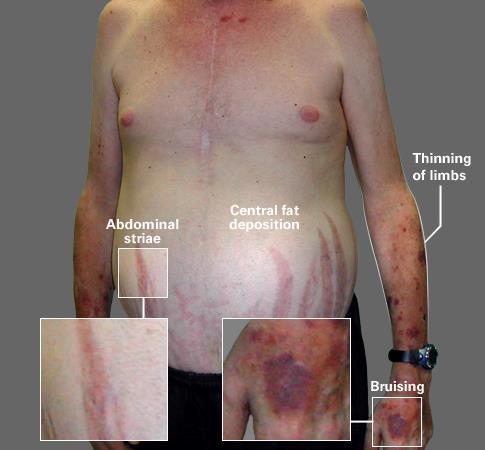
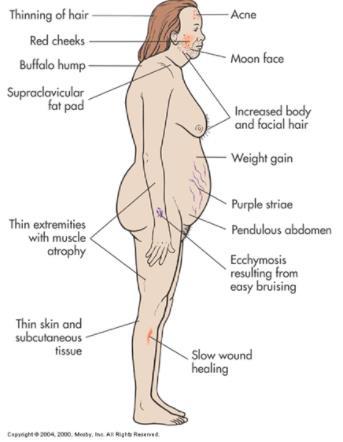
17 Clinical Features of Cushing s Syndrome
18
19
20 Real World Cushing s 34 yo female with 18 months of weight gain (30 lbs), fatigue, depression. Restricted to 1000 calories/day, worked with a physical trainer, developed proximal weakness noted by her trainer. Progressed to the point that she had to use her arms to pull herself up stairs. 46 yo female with hypothyroidism, stable on levothyroxine for years, with residual complaints of fatigue, difficulty losing weight. 2-3 year period of worsening overall stamina, anxiety, further weight gain normal UFC and elevated ONDST. Went home to Equador for a year further decline in health, mood, energy. UFC now elevated, salivary cortisols elevated and ONDST abnormal. 2.8mm pituitary adenoma, underwent TSS with surgical cure


21 Real World Cushing s 74 yo white female undergoes MRI for headaches, found to have a 1.2cm pituitary mass not seen in Stable HTN, new dx pre-dm. Definite truncal obesity, thin arms/legs noted on exam; notes everyone in my family looks like this, but then after further discussion does note that her body habitus has shifted significantly over the prior mos. Some fatigue, decline in stamina. Abnormal ONDST, underwent TSS 12/17 with path confirming an ACTH producing adenoma.
22 When to Consider Cushing s Syndrome Rapid weight gain with proximal weakness Patients with unusual features for age (HTN, osteoporosis) Patients with multiple and progressive features Adrenal adenomas
23 Diagnosis of Cushing s Syndrome 24h urine free cortisol (UFC)- 2 samples Late night salivary cortisols- 2 samples 1mg overnight dexamethasone suppression test (ONDST) Do not use: 8 am cortisol Imaging prior to biochemical diagnosis
24 Diagnosis of Cushing s Syndrome For all: rule out any exogenous glucocorticoid use (oral, injected, inhaled, topical) 24 hour UFC May miss mild cases Avoid if CrCl < 60ml/min (falsely low values) Salivary cortisol 1-2 hours after normal bedtime; do not use if pt does not have regular sleep/wake cycle 1mg ONDST Avoid with seizure meds, oral estrogen
25 Diagnosis of Cushing s Syndrome Start with 1 or 2 tests, depending on pre test probability based on history/exam If all tests are negative, Cushing s Syndrome is less likely but not impossible If symptoms progress in the next months-years, then re-evaluation is warranted
26 Take Home Points Prolactinomas are very common All pituitary adenomas, cases of amenorrhea/oligomenorrhea deserve a PRL screen Many causes of hyperprolactinemia other than prolactinomas Cushing s syndrome and acromegaly much less common, but probably under-diagnosed Consider Cushing s for rapidly progressive symptoms Even if initial Cushing's tests are normal or equivocal, ask patients to follow up if symptoms progress
27 References 2008 J Clin Endocrinol Metab 93(5):1526. The Diagnosis of Cushing s Syndrome: An Endocrine Society Clinical Practice Guideline 2011 J Clin Endocrinol Metab 96(2): 273. Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline 2014 J Clin Endocrinol Metab 99(11): Acromegaly: An Endocrine Society Clinical Practice Guideline
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly
 Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly Dr. Peter Igaz MD PhD DSc 2nd Department of Medicine Semmelweis University Fields of Endocrinology Diseases
Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly Dr. Peter Igaz MD PhD DSc 2nd Department of Medicine Semmelweis University Fields of Endocrinology Diseases
Neuroendocrine Disorders in Women
 Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
Pituitary Tumors and Incidentalomas. Bijan Ahrari, MD, FACE, ECNU Palm Medical Group
 Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY
 JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
Professor Ian Holdaway. Endocrinologist Auckland District Health Board
 Professor Ian Holdaway Endocrinologist Auckland District Health Board A land of milk and giants hormonesecreting pituitary tumours I M Holdaway, Endocrinologist, Auckland Acromegaly Prolactinomas Cushing
Professor Ian Holdaway Endocrinologist Auckland District Health Board A land of milk and giants hormonesecreting pituitary tumours I M Holdaway, Endocrinologist, Auckland Acromegaly Prolactinomas Cushing
High and Low GH: an update of diagnosis and management of GH disorders
 High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
Treating a Growing Problem: A Closer Look at Acromegaly. Lisa Nachtigall, MD (Moderator) Nicholas Tritos, MD, DSc Brooke Swearingen, MD
 Nicholas Tritos, MD, DSc Brooke Swearingen, MD") Treating a Growing Problem: A Closer Look at Acromegaly Lisa Nachtigall, MD (Moderator) Nicholas Tritos, MD, DSc Brooke Swearingen, MD Goal Address key challenges faced by physicians who treat acromegaly
Treating a Growing Problem: A Closer Look at Acromegaly Lisa Nachtigall, MD (Moderator) Nicholas Tritos, MD, DSc Brooke Swearingen, MD Goal Address key challenges faced by physicians who treat acromegaly
Pituitary Disorders Suranut Charoensri, MD
 Pituitary Disorders Suranut Charoensri, MD Division of Endocrinology and Metabolism Department of Medicine Faculty of Medicine, Khon Kaen University Anatomical Landmarks Nat Rev Endocrinol 2014;10:423-435
Pituitary Disorders Suranut Charoensri, MD Division of Endocrinology and Metabolism Department of Medicine Faculty of Medicine, Khon Kaen University Anatomical Landmarks Nat Rev Endocrinol 2014;10:423-435
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Hyperprolactinemia: N hidshi i MD. Nahid Shirazian MD. Internist, Endocrinologist
 Diagnosis and Treatment of Hyperprolactinemia: p N hidshi i MD Nahid Shirazian MD. Internist, Endocrinologist An Endocrine Society Clinical Practice Guideline (J Clin Endocrinol Metab 96: 273 288, 2011)
Diagnosis and Treatment of Hyperprolactinemia: p N hidshi i MD Nahid Shirazian MD. Internist, Endocrinologist An Endocrine Society Clinical Practice Guideline (J Clin Endocrinol Metab 96: 273 288, 2011)
Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male
: female / male") 1. Patient personal details Institute code: Physician code: Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male 2. Changes in acromegaly-specific medical
1. Patient personal details Institute code: Physician code: Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male 2. Changes in acromegaly-specific medical
Pituitary for the General Practitioner. Marilyn Lee Consultant physician and endocrinologist
 Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Metoclopramide Domperidone. HYPER- PROLACTINAEMIA: the true and the false problems
 Modern management of Hyperprolactinaemia Didier DEWAILLY, M.D. Department of Endocrine Gynaecology and Reproductive Medicine, Hôpital Jeanne de Flandre, C.H.R.U., 59037 Lille, France 1 Metoclopramide Domperidone
Modern management of Hyperprolactinaemia Didier DEWAILLY, M.D. Department of Endocrine Gynaecology and Reproductive Medicine, Hôpital Jeanne de Flandre, C.H.R.U., 59037 Lille, France 1 Metoclopramide Domperidone
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs
 Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
(3) Pituitary tumours
 Pituitary tumours") Hypopituitarism Diabetes Insipidus Pituitary tumours (2) Dr T Kemp - Endocrinology and Metabolism Unit - Steve Biko Academic Hospital (3) Pituitary tumours Pituitary microadenoma - intrasellar adenoma
Hypopituitarism Diabetes Insipidus Pituitary tumours (2) Dr T Kemp - Endocrinology and Metabolism Unit - Steve Biko Academic Hospital (3) Pituitary tumours Pituitary microadenoma - intrasellar adenoma
Sharon maslovitz Lis Maternity Hospital
 Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Medical background Healthy until 24yo
Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Medical background Healthy until 24yo
Mechanism of hyperprolactinemia
 Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
UW MEDICINE PATIENT EDUCATION. Acromegaly Symptoms and treatments. What is acromegaly? DRAFT. What are the symptoms? How is it diagnosed?
 UW MEDICINE PATIENT EDUCATION Acromegaly Symptoms and treatments This handout explains a health condition called acromegaly. It describes tests that are used to diagnose the condition and gives basic instructions
UW MEDICINE PATIENT EDUCATION Acromegaly Symptoms and treatments This handout explains a health condition called acromegaly. It describes tests that are used to diagnose the condition and gives basic instructions
GLMS CME- Cell Group 5 10 April Greenlane Medical Specialists Pui-Ling Chan Endocrinologist
 GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
Challenging Pituitary Cases. Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine
 Challenging Pituitary Cases Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine 1 34 yo male has incidental finding of large macroadenoma, with prolactin
Challenging Pituitary Cases Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine 1 34 yo male has incidental finding of large macroadenoma, with prolactin
HYPOTHALAMO PITUITARY GONADAL AXIS
 HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Pituitary Disease Resident Tutorial 2017
 Pituitary Disease Resident Tutorial 2017 Sarat Sunthornyothin MD Division of Endocrinology and Metabolism King Chulalongkorn Memorial Hospital Pituitary Anatomy hypophyseal portal system direct arterial
Pituitary Disease Resident Tutorial 2017 Sarat Sunthornyothin MD Division of Endocrinology and Metabolism King Chulalongkorn Memorial Hospital Pituitary Anatomy hypophyseal portal system direct arterial
Diseases of pituitary gland
 Diseases of pituitary gland A brief introduction Anterior lobe = adenohypophysis Posterior lobe = neurohypophysis The production of most pituitary hormones is controlled in large part by positively and
Diseases of pituitary gland A brief introduction Anterior lobe = adenohypophysis Posterior lobe = neurohypophysis The production of most pituitary hormones is controlled in large part by positively and
Clinical presentations of endocrine diseases
 Section I Chapter 1 Clinical approaches Clinical presentations of endocrine diseases Karen Gomez-Hernandez and Shereen Ezzat Endocrinology is a fascinating field that covers a wide range of diseases with
Section I Chapter 1 Clinical approaches Clinical presentations of endocrine diseases Karen Gomez-Hernandez and Shereen Ezzat Endocrinology is a fascinating field that covers a wide range of diseases with
Pathology of pituitary gland. By: Shifaa Qa qa
 Pathology of pituitary gland By: Shifaa Qa qa Sella turcica Adenohypophysis (80%): - epithelial cells - acidophil, basophil, chromophobe - Somatotrophs, Mammosomatotrophs, Corticotrophs, Thyrotrophs, Gonadotrophs
Pathology of pituitary gland By: Shifaa Qa qa Sella turcica Adenohypophysis (80%): - epithelial cells - acidophil, basophil, chromophobe - Somatotrophs, Mammosomatotrophs, Corticotrophs, Thyrotrophs, Gonadotrophs
Cortisol levels. Naturally produced by the adrenal Cortisol
 1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
Endocrine part two. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP
 Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP Endocrine in 25 Minutes Joshua S. Coren, D.O., MBA, FACOFP Vice Chair and Associate Professor, Family Medicine Rowan University School
Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP Endocrine in 25 Minutes Joshua S. Coren, D.O., MBA, FACOFP Vice Chair and Associate Professor, Family Medicine Rowan University School
Differential Diagnosis of Cushing s Syndrome
 Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Acromegaly: a challenging condition to diagnose and manage. C. L. Chik, MD, PhD, FRCPC University of Alberta, Edmonton
 Acromegaly: a challenging condition to diagnose and manage C. L. Chik, MD, PhD, FRCPC University of Alberta, Edmonton Acromegaly: a challenging condition to diagnose and manage? Objectives: n Know the
Acromegaly: a challenging condition to diagnose and manage C. L. Chik, MD, PhD, FRCPC University of Alberta, Edmonton Acromegaly: a challenging condition to diagnose and manage? Objectives: n Know the
Endocrine Pharmacology
 Endocrine Pharmacology 17-2-2013 DRUGS AFFECTING THE ENDOCRINE SYSTEM The endocrine system is the system of glands, each of which secretes a type of hormone directly into the bloodstream to regulate the
Endocrine Pharmacology 17-2-2013 DRUGS AFFECTING THE ENDOCRINE SYSTEM The endocrine system is the system of glands, each of which secretes a type of hormone directly into the bloodstream to regulate the
THE ANTERIOR PITUITARY. Embryology cont. Embryology of the pituitary BY MISPA ZUH HS09A179. Embryology cont. THE PITUIYARY GLAND Anatomy:
 THE ANTERIOR PITUITARY BY MISPA ZUH HS09A179 Embryology of the pituitary The pituitary is formed early in embryonic life from the fusion of the Rathke s pouch (anterior) and the diencephalon ( posterior)
THE ANTERIOR PITUITARY BY MISPA ZUH HS09A179 Embryology of the pituitary The pituitary is formed early in embryonic life from the fusion of the Rathke s pouch (anterior) and the diencephalon ( posterior)
No cases of precocious puberty were reported during clinical trials of risperidone in, cases of precocious puberty have been
 levels than adults. The growth hormone elevations reported for the 12 patients with growth hormone excess were modest and well below levels reported in children with gigantism. 7,8 None of the patients
levels than adults. The growth hormone elevations reported for the 12 patients with growth hormone excess were modest and well below levels reported in children with gigantism. 7,8 None of the patients
Endocrine Topic Review. Sethanant Sethakarun, MD
 Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Reproductive Health and Pituitary Disease
 Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
CYSTIC PROLACTINOMA: A SURGICAL DISEASE?
 AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
ABNORMAL PITUITARY FUNCTION
 Overview ABNORMAL PITUITARY FUNCTION Specialist Portfolio Seminar Katie Jones Sandwell and West Birmingham Hospitals NHS Trust Anterior pituitary overview Posterior pituitary overview Pituitary dysfunction
Overview ABNORMAL PITUITARY FUNCTION Specialist Portfolio Seminar Katie Jones Sandwell and West Birmingham Hospitals NHS Trust Anterior pituitary overview Posterior pituitary overview Pituitary dysfunction
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Pituitary gland Pituitary fossa Mass: 5 gms DIMENSIONS 7mm (Ht) 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum
 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum") Pituitary gland Pituitary fossa Mass: 5 gms DIMENSIONS 7mm (Ht) 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum Cell type hormone Clinical syndrome Tumor type Somatotroph Growth
Pituitary gland Pituitary fossa Mass: 5 gms DIMENSIONS 7mm (Ht) 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum Cell type hormone Clinical syndrome Tumor type Somatotroph Growth
Hormones by location
 Endocrine System Hormones by location Pineal Gland: Melatonin Feeling of sleepiness Hypothalamus: Hormones that stimulate or inhibit pituitary Temp., hunger, parenting attachment, thirst Pituitary Gland:
Endocrine System Hormones by location Pineal Gland: Melatonin Feeling of sleepiness Hypothalamus: Hormones that stimulate or inhibit pituitary Temp., hunger, parenting attachment, thirst Pituitary Gland:
Clinical Policy: Pasireotide (Signifor LAR) Reference Number: CP.PHAR.332 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PHAR.332 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Signifor LAR) Reference Number: CP.PHAR.332 Effective Date: 03.01.17 Last Review Date: 11.17 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the
Clinical Policy: (Signifor LAR) Reference Number: CP.PHAR.332 Effective Date: 03.01.17 Last Review Date: 11.17 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the
Hypothalamus & Pituitary Gland
 Hypothalamus & Pituitary Gland Hypothalamus and Pituitary Gland The hypothalamus and pituitary gland form a unit that exerts control over the function of several endocrine glands (thyroid, adrenals, and
Hypothalamus & Pituitary Gland Hypothalamus and Pituitary Gland The hypothalamus and pituitary gland form a unit that exerts control over the function of several endocrine glands (thyroid, adrenals, and
Pituitary gland diseases
 Pituitary gland diseases Pituitary Gland Weight 600 mg Is located within the sella turcica Anatomically and functionally distinct anterior and posterior lobes Pituitary Development The pituitary originate
Pituitary gland diseases Pituitary Gland Weight 600 mg Is located within the sella turcica Anatomically and functionally distinct anterior and posterior lobes Pituitary Development The pituitary originate
Hyperprolactinemia in A 15-Year-Old Girl with Primary Amenorrhea
 Clin Pediatr Endocrinol 1996; 5(2), 61-66 Copyright (C) 1996 by The Japanese Society for Pediatric Endocrinology Hyperprolactinemia in A 15-Year-Old Girl with Primary Amenorrhea Toshihisa Okada, Soroku
Clin Pediatr Endocrinol 1996; 5(2), 61-66 Copyright (C) 1996 by The Japanese Society for Pediatric Endocrinology Hyperprolactinemia in A 15-Year-Old Girl with Primary Amenorrhea Toshihisa Okada, Soroku
Growth Hormone, Somatostatin, and Prolactin 1 & 2 Mohammed Y. Kalimi, Ph.D.
 Growth Hormone, Somatostatin, and Prolactin 1 & 2 Mohammed Y. Kalimi, Ph.D. I. Growth Hormone (somatotropin): Growth hormone (GH) is a 191 amino acid single chain polypeptide (MW 22,000 daltons). Growth
Growth Hormone, Somatostatin, and Prolactin 1 & 2 Mohammed Y. Kalimi, Ph.D. I. Growth Hormone (somatotropin): Growth hormone (GH) is a 191 amino acid single chain polypeptide (MW 22,000 daltons). Growth
October 13, Surgical Nuances to Managing Cushing s Disease. Cortisol Regulation. Cushing s Syndrome Excess Cortisol. Sandeep Kunwar, M.D.
 Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
62-year-old woman with severe headache. Celeste Thomas November 1, 2012
 62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution?
 Case Reports in Radiology Volume 2015, Article ID 268974, 5 pages http://dx.doi.org/10.1155/2015/268974 Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution? Devon
Case Reports in Radiology Volume 2015, Article ID 268974, 5 pages http://dx.doi.org/10.1155/2015/268974 Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution? Devon
Pharmacology of Hypothalamic Hormones
 Pharmacology of Hypothalamic Hormones Pharmacology of Hypothalamic Hormones The neuroendocrine system, which is controlled by the pituitary and hypothalamus, coordinates body functions by transmitting
Pharmacology of Hypothalamic Hormones Pharmacology of Hypothalamic Hormones The neuroendocrine system, which is controlled by the pituitary and hypothalamus, coordinates body functions by transmitting
NANOS Patient Brochure
 NANOS Patient Brochure Pituitary Tumor Copyright 2015. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
NANOS Patient Brochure Pituitary Tumor Copyright 2015. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
Ch 8: Endocrine Physiology
 Ch 8: Endocrine Physiology Objectives 1. Review endocrine glands of body. 2. Understand how hypothalamus controls endocrine system & sympathetic epinephrine response. 3. Learn anterior pituitary hormones
Ch 8: Endocrine Physiology Objectives 1. Review endocrine glands of body. 2. Understand how hypothalamus controls endocrine system & sympathetic epinephrine response. 3. Learn anterior pituitary hormones
Sharon maslovitz Lis Maternity Hospital
 Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Conditions that may cause episodic headaches:
Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Conditions that may cause episodic headaches:
Hypothalamus & pituitary gland
 Hypothalamus & pituitary gland Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel: 88208292 Outline Hypothalamus Relationship between the hypothalamus
Hypothalamus & pituitary gland Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel: 88208292 Outline Hypothalamus Relationship between the hypothalamus
Hyperprolactinemia. Justin Moore, MD
 Hyperprolactinemia Justin Moore, MD Biography.com The Miraculous Lactation of St. Bernard Bernard prayed before a statue of the Madonna, asking her, "Show yourself a mother" ("Monstra te esse Matrem").
Hyperprolactinemia Justin Moore, MD Biography.com The Miraculous Lactation of St. Bernard Bernard prayed before a statue of the Madonna, asking her, "Show yourself a mother" ("Monstra te esse Matrem").
Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide)
") Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide) INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of
Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide) INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of
Pathophysiology of Pituitary Gland Disorders. PHCL 415 Hadeel Alkofide May 2010
 Pathophysiology of Pituitary Gland Disorders PHCL 415 Hadeel Alkofide May 2010 1 Learning Objectives Understand the physiology of pituitary gland Understand acromegaly & describe its clinical features
Pathophysiology of Pituitary Gland Disorders PHCL 415 Hadeel Alkofide May 2010 1 Learning Objectives Understand the physiology of pituitary gland Understand acromegaly & describe its clinical features
TREATMENT OF CUSHING S DISEASE
 TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
Disclosures. BMS, Ferring research grant funding NovoNordisk scientific advisory board Chiasma clinical trial investigator
 Pituitary Disorders Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes, and Hypertension Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures BMS, Ferring
Pituitary Disorders Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes, and Hypertension Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures BMS, Ferring
A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease
 A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease Z Hussein, MRCP*, B Tress**, P G Cohnan, FRACP***... 'Department of Medicine, Hospital Putrajaya, Putrajaya, Presint 7, 62250
A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease Z Hussein, MRCP*, B Tress**, P G Cohnan, FRACP***... 'Department of Medicine, Hospital Putrajaya, Putrajaya, Presint 7, 62250
Management of incidental pituitary microadenomas: a cost-effectiveness analysis King J T, Justice A C, Aron D C
 Management of incidental pituitary microadenomas: a cost-effectiveness analysis King J T, Justice A C, Aron D C Record Status This is a critical abstract of an economic evaluation that meets the criteria
Management of incidental pituitary microadenomas: a cost-effectiveness analysis King J T, Justice A C, Aron D C Record Status This is a critical abstract of an economic evaluation that meets the criteria
What we will cover. Evaluation of the Child with Suspected Pituitary Disease. ituitary
 Evaluation of the Child with Suspected Pituitary Disease Craig Alter, MD University of Pennsylvania Children s Hospital of Philadelphia What we will cover * What laboratory tests to order * MRI: common
Evaluation of the Child with Suspected Pituitary Disease Craig Alter, MD University of Pennsylvania Children s Hospital of Philadelphia What we will cover * What laboratory tests to order * MRI: common
Brain Tumors. Andrew J. Fabiano, MD FAANS. Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine
 Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Brain and Spine Tumors
 Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
Cushing s Syndrome. Diagnosis. GuidelineCentral.com. Key Points. Diagnosis
 Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
Testosterone Therapy in Men with Hypogonadism
 Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
DIMENSIONS 1 cm in diameter 0.5 to 1 gm in weight. LOCATION Sella turcica A bony cavity. DIVISIONS Anterior lobe Posterior lobe Pars intermedia
 DIMENSIONS 1 cm in diameter 0.5 to 1 gm in weight LOCATION Sella turcica A bony cavity DIVISIONS Anterior lobe Posterior lobe Pars intermedia body temperature autonomic nervous system emotional and food
DIMENSIONS 1 cm in diameter 0.5 to 1 gm in weight LOCATION Sella turcica A bony cavity DIVISIONS Anterior lobe Posterior lobe Pars intermedia body temperature autonomic nervous system emotional and food
Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary Tumor Apoplexy
 Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 817603, 4 pages http://dx.doi.org/10.1155/2013/817603 Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary
Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 817603, 4 pages http://dx.doi.org/10.1155/2013/817603 Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary
Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline
 Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline Shlomo Melmed, Felipe F. Casanueva, Andrew R. Hoffman, David L. Kleinberg, Victor M. Montori, Janet A. Schlechte
Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline Shlomo Melmed, Felipe F. Casanueva, Andrew R. Hoffman, David L. Kleinberg, Victor M. Montori, Janet A. Schlechte
The most current assessment of this problem can be found in the Apex note dated
 Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
Clinical Policy: Pasireotide (Signifor LAR) Reference Number: CP.PHAR.332
 Reference Number: CP.PHAR.332") Clinical Policy: (Signifor LAR) Reference Number: CP.PHAR.332 Effective Date: 03/17 Last Review Date: 02/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Signifor LAR) Reference Number: CP.PHAR.332 Effective Date: 03/17 Last Review Date: 02/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important
12/27/2013. Kristen Cain, MD FACOG Reproductive Medicine Institute Sanford Health, Fargo ND
 Kristen Cain, MD FACOG Reproductive Medicine Institute Sanford Health, Fargo ND 7% of all women 18-45 Obesity 1/3 of all US women Incidence of PCOS is increasing with increase obesity Obesity Irregular
Kristen Cain, MD FACOG Reproductive Medicine Institute Sanford Health, Fargo ND 7% of all women 18-45 Obesity 1/3 of all US women Incidence of PCOS is increasing with increase obesity Obesity Irregular
14 Girl with Cushing s Disease: An Update. Kristen Dillard, MD Endorama October 17, 2013
 14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
Managing Acromegaly: Review of Two Cases
 Managing Acromegaly: Review of Two Cases INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of patients with acromegaly who have
Managing Acromegaly: Review of Two Cases INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of patients with acromegaly who have
Imaging pituitary gland tumors
 November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
Endocrine Testing. Alice Y.Y. Cheng, MD, FRCP October 14, 2015
 Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC
 10 th Annual Canadian Endocrine Update 3 rd Canadian Endocrine Review Course Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC 10 th Annual Canadian Endocrine Update Dr.
10 th Annual Canadian Endocrine Update 3 rd Canadian Endocrine Review Course Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC 10 th Annual Canadian Endocrine Update Dr.
Acromegaly: Management of the Patient Who Has Failed Surgery
 Acromegaly: Management of the Patient Who Has Failed Surgery Minnesota/Midwest Chapter of the American Association of Clinical Endocrinologists 8 th Annual Meeting October 14, 2017 Mark E. Molitch, M.D.
Acromegaly: Management of the Patient Who Has Failed Surgery Minnesota/Midwest Chapter of the American Association of Clinical Endocrinologists 8 th Annual Meeting October 14, 2017 Mark E. Molitch, M.D.
CUSHING SYNDROME Dr. Muhammad Sarfraz
 Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Pasireotide Long-Acting Repeatable (Signifor) for acromegaly first and second line
 for acromegaly first and second line") Pasireotide Long-Acting Repeatable (Signifor) for acromegaly first and second line December 2010 This technology summary is based on information available at the time of research and a limited literature
Pasireotide Long-Acting Repeatable (Signifor) for acromegaly first and second line December 2010 This technology summary is based on information available at the time of research and a limited literature
Endocrine System. Overview Hormones Endocrine Organs
 Endocrine System Overview Hormones Endocrine Organs Endocrine vs. Exocrine Gland Secretes hormones sweat & saliva Ductless gland has ducts Injects tissue duct is filled Chemistry of Hormones & Physiology
Endocrine System Overview Hormones Endocrine Organs Endocrine vs. Exocrine Gland Secretes hormones sweat & saliva Ductless gland has ducts Injects tissue duct is filled Chemistry of Hormones & Physiology
I. Provide patient care that is compassionate, appropriate and effective for the prevention and treatment of endocrinologic disorders.
 Endocrinology Curriculum Goal Endocrinology is the diagnosis and care of disorders of the endocrine system. The principal endocrine problems handled by the general internist include goiter, thyroid nodules,
Endocrinology Curriculum Goal Endocrinology is the diagnosis and care of disorders of the endocrine system. The principal endocrine problems handled by the general internist include goiter, thyroid nodules,
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018
 Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
Indications for Surgical Removal of Adrenal Glands
 The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
Endocrine system pathology
 Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Imaging The Turkish Saddle. Russell Goodman, HMS III Dr. Gillian Lieberman
 Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
Urgent and Emergent Pituitary Conditions
 Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
Pituitary adenomas and menopause
 Pituitary adenomas and menopause Iulia Potorac Service d Endocrinologie Université de Liège CHU Liège RESULTATS Clinical case 1-38-year-old patient referred for exploration of premature ovarian failure
Pituitary adenomas and menopause Iulia Potorac Service d Endocrinologie Université de Liège CHU Liège RESULTATS Clinical case 1-38-year-old patient referred for exploration of premature ovarian failure
Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction
 Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction Mohammad Talha Rauf, MD Internal Medicine Resident PGY3 Dania AbuShanab, MD Julie Samantray,
Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction Mohammad Talha Rauf, MD Internal Medicine Resident PGY3 Dania AbuShanab, MD Julie Samantray,
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form