Abstract. n engl j med 363;9 nejm.org august 26,
|
|
|
- Kenneth Potter
- 5 years ago
- Views:
Transcription
1 The new england journal of medicine established in 1812 august 26, 2010 vol. 363 no. 9 Inhibition of Mutated, Activated BRAF in Metastatic Melanoma Keith T. Flaherty, M.D., Igor Puzanov, M.D., Kevin B. Kim, M.D., Antoni Ribas, M.D., Grant A. McArthur, M.B., B.S., Ph.D., Jeffrey A. Sosman, M.D., Peter J. O Dwyer, M.D., Richard J. Lee, M.D., Ph.D., Joseph F. Grippo, Ph.D., Keith Nolop, M.D., and Paul B. Chapman, M.D. Abstract Background The identification of somatic mutations in the gene encoding the serine threonine protein kinase B-RAF (BRAF) in the majority of melanomas offers an opportunity to test oncogene-targeted therapy for this disease. Methods We conducted a multicenter, phase 1, dose-escalation trial of PLX4032 (also known as RG7204), an orally available inhibitor of mutated BRAF, followed by an extension phase involving the maximum dose that could be administered without adverse effects (the recommended phase 2 dose). Patients received PLX4032 twice daily until they had disease progression. Pharmacokinetic analysis and tumor-response assessments were conducted in all patients. In selected patients, tumor biopsy was performed before and during treatment to validate BRAF inhibition. Results A total of 55 patients (49 of whom had melanoma) were enrolled in the dose-escalation phase, and 32 additional patients with metastatic melanoma who had BRAF with the V600E mutation were enrolled in the extension phase. The recommended phase 2 dose was 960 mg twice daily, with increases in the dose limited by grade 2 or 3 rash, fatigue, and arthralgia. In the dose-escalation cohort, among the 16 patients with melanoma whose tumors carried the V600E BRAF mutation and who were receiving 240 mg or more of PLX4032 twice daily, 10 had a partial response and 1 had a complete response. Among the 32 patients in the extension cohort, 24 had a partial response and 2 had a complete response. The estimated median progression-free survival among all patients was more than 7 months. From the Abramson Cancer Center of the University of Pennsylvania, Philadelphia (K.T.F., P.J.O.); Massachusetts General Hospital Cancer Center, Boston (K.T.F.); Vanderbilt University, Nashville (I.P., J.A.S.); the University of Texas M.D. Anderson Cancer Center, Houston (K.B.K.); UCLA, Los Angeles (A.R.); Peter MacCallum Cancer Centre, East Melbourne, VIC, Australia (G.A.M.); Roche Pharmaceuticals, Nutley, NJ (R.J.L., J.F.G.); Plexxikon, Berkeley, CA (K.N.); and Memorial Sloan- Kettering Cancer Center, New York (P.B.C.). Address reprint requests to Dr. Flaherty at Massachusetts General Hospital Cancer Center, 55 Fruit St., Yawkey 9E, Boston, MA 02114, or at kflaherty@partners.org. N Engl J Med 2010;363: Copyright 2010 Massachusetts Medical Society. Conclusions Treatment of metastatic melanoma with PLX4032 in patients with tumors that carry the V600E BRAF mutation resulted in complete or partial tumor regression in the majority of patients. (Funded by Plexxikon and Roche Pharmaceuticals.) n engl j med 363;9 nejm.org august 26,
2 The new england journal of medicine Metastatic melanoma is an aggressive disease for which there are few effective therapies. The two therapies approved by the Food and Drug Administration, high-dose interleukin-2 and dacarbazine, are each associated with response rates of only 10 to 20% and a small percentage of complete responses; neither is thought to improve overall survival. 1,2 In randomized trials, the median survival among patients treated with dacarbazine was less than 8 months. 3,4 A search for mutations in a component of the mitogen-activated protein (MAP) kinase pathway in a large panel of common cancers revealed that 40 to 60% of melanomas, and 7 to 8% of all cancers, carry an activating mutation in the gene encoding the serine threonine protein kinase B-RAF (BRAF) Ninety percent of reported BRAF mutations result in a substitution of glutamic acid for valine at amino acid 600 (the V600E mutation). This BRAF mutation constitutively activates BRAF and downstream signal transduction in the MAP kinase pathway. BRAF mutations are also found in 40 to 70% of papillary or anaplastic thyroid cancers 6-8,16-18 and in a small percentage of several other types of tumor. PLX4032 (Plexxikon; RG7204, Roche Pharmaceuticals) is a potent inhibitor of BRAF with the V600E mutation. Preclinical studies showed that PLX4032 and its analogue PLX4720 inhibit the kinase activity of BRAF with the V600E mutation at low nanomolar concentrations, abrogate signaling through the MAP kinase pathway, and block proliferation of cells carrying BRAF with the V600E mutation in vitro at high nanomolar concentrations. 17,18 Orally administered PLX4720 inhibits the growth and, at higher doses, induces the regression of human melanoma tumors transplanted into immunocompromised mice. None of these effects are observed in normal tissues or in tumor cells that lack a BRAF mutation. We conducted a trial of the use of PLX4032 in patients with metastatic cancer. The primary goals were to define the safety and pharmacokinetic characteristics of treatment with continuous, twice-daily administration of PLX4032, to determine the maximum dose that could be administered until adverse effects prevented further dose increases (i.e., the recommended phase 2 dose), and to determine the objective response rate, the duration of response, and the rate of progression among patients who had melanoma tumors with the V600E BRAF mutation and who were given the recommended phase 2 dose of PLX4032. Methods Study Design The study was sponsored by Plexxikon and Roche Pharmaceuticals, which provided the study drug. The study was designed by two academic authors and one industry author. All authors made the decision to submit the manuscript for publication. All authors analyzed the data, prepared the manuscript, and vouch for the completeness and accuracy of the data and analyses. The study was conducted in accordance with the protocol. Dose-Escalation Phase PLX4032 was initially in a crystalline formulation. In the dose-escalation phase of the study, which involved several consecutively enrolled groups of three to six patients, the first group received 200 mg of PLX4032 by mouth daily; subsequent groups received the drug at higher doses, according to a dose-escalation scheme. This formulation was found to have poor bioavailability (see the Results section), and enrollment for the dose-escalation phase was halted while the drug was reformulated as a highly bioavailable microprecipitated bulk powder, initially as a 40-mg capsule and subsequently as 80-mg and 120-mg capsules, as well as 240-mg tablets. Enrollment was resumed, with newly enrolled patients receiving the microprecipitated-bulk-powder formulation at a dose of 160 mg (two 80-mg capsules) twice daily, with subsequent escalation. Patients received continuous therapy with PLX4032 unless unacceptable side effects or disease progression occurred. Doses were not escalated unless the patients receiving the highest current dose had been observed for at least 4 weeks and dose-limiting side effects had been reported in fewer than a third. Dose escalation in a given patient was permitted if the safety and adverseeffect profile had been established for the next highest dose. The recommended phase 2 dose was defined as the highest dose at which no more than one of six patients had dose-limiting side effects. Extension Phase Once the recommended phase 2 dose had been identified, an extension cohort was treated at this 810 n engl j med 363;9 nejm.org august 26, 2010
3 Inhibition of Mutated, Activated BRAF dose. In this cohort, all patients had melanoma and a prospectively identified V600E BRAF mutation. The primary objective in the extension cohort was to determine the response rate. Secondary objectives were to define the toxicity and pharmacokinetics of PLX4032 more precisely and to obtain data on pharmacodynamic effects. Patients Eligibility criteria included the provision of written informed consent, an age of 18 years or older, solid tumors confirmed histologically that were refractory to standard therapy or for which standard or curative therapy did not exist, Eastern Cooperative Oncology Group performance status score of 0 (able to be fully active and carry out all predisease activities without restriction) or 1 (unable to perform physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, such as light housework or office work), 19 life expectancy of 3 months or longer, absence of known progressing or unstable brain metastases, and adequate hematologic, hepatic, and renal function. The dose-escalation phase of the trial was open to patients with any type of tumor, although patients who had melanomas with the V600E mutation in BRAF were overrepresented because of the selective activity of PLX4032 against such tumors in preclinical testing. For the extension cohort, eligibility was restricted to patients with melanomas harboring a V600E BRAF mutation, as ascertained by means of a polymerase-chainreaction assay (TaqMan, Applied Biosystems). This assay involves hybridizing a probe specific to the 1799T A substitution that results in the V600E BRAF mutation with DNA isolated from formalin-fixed, paraffin-embedded tumor tissue and determining the presence or absence of amplification after repeated chain-reaction cycles. 20 Study Assessments Safety evaluations were conducted at baseline, day 8, day 15, day 29, and every 4 weeks thereafter. These evaluations included a physical examination, electrocardiography, laboratory studies that included a complete blood count, clinical chemical testing, and urinalysis. Adverse events were graded according to the Common Terminology Criteria for Adverse Events (version 3.0) ( ctep.info.nih.gov/protocoldevelopment/electronic_ applications/docs/ctcaev3.pdf). During the trial, squamous-cell carcinoma, keratoacanthoma type, was observed in several patients (see the Results section). As a result, the protocol was amended to ensure that patients underwent dermatologic evaluations at baseline and every 2 months during the study; computed tomographic (CT) scans of the chest were analyzed for the appearance of new lesions suggestive of a primary cancer. CT studies were performed at 8-week intervals during therapy in all patients and at the end of the first 4 weeks of therapy in some patients. The findings were judged according to the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.0. A complete response was defined as the disappearance of all target lesions, and a partial response as a decrease by at least 30% in the sum of the largest diameter of each target lesion, relative to the corresponding sum at baseline. Progressive disease was defined as an increase by at least 20% in the sum of the largest diameter of each target lesion, relative to the smallest corresponding diameter recorded since the start of treatment, or the appearance of one or more new lesions. Stable disease was defined as the absence of shrinkage sufficient for a partial response and the absence of enlargement sufficient for progressive disease, relative to the corresponding sum at baseline. Progression-free survival was defined as the time from the first day of treatment to the first documentation of disease progression or death, whichever occurred first. Pharmacokinetic assessments were made on day 1 and day 15 of the first 4 weeks of therapy, and single plasma samples were obtained every 4 weeks during the study. Plasma samples were analyzed by means of high-performance liquid chromatography, with detection by means of mass spectroscopy. Patients in the dose-escalation phase who were receiving a dose greater than 160 mg twice daily and patients in the extension cohort underwent 18 F-fluorodeoxyglucose positron-emission tomography (FDG-PET) at baseline and on day 15 of the first 4 weeks of therapy. Selected patients underwent tumor biopsy before the start of therapy as well as on day 15. Biopsy specimens were immediately fixed in formalin for analysis of phosphorylated extracellular signal-regulated kinase (ERK), the protein cyclin D1, and the monoclonal antibody Ki-67 by means of immunohistochemistry. The sampled tumors were cutaneous or superficial lymph-node lesions; except in the case of n engl j med 363;9 nejm.org august 26,
4 The new england journal of medicine Table 1. Baseline Characteristics of the Patients, According to Study Cohort.* Characteristic Age yr Dose-Escalation Cohort (N = 55) Extension Cohort (N = 32) Median Range Sex no. (%) Male 34 (62) 19 (59) Female 21 (38) 13 (41) Tumor type no. (%) Melanoma 49 (89) 32 (100) Thyroid 3 (5) 0 Other 3 (5) 0 Extent of metastatic melanoma no. (%) Stage M1a 7 (14) 6 (19) Stage M1b 6 (12) 2 (6) Stage M1c 36 (73) 24 (75) LDH >ULN no. (%) 13 (41) ECOG performance status score no. (%) 0 28 (51) 15 (47) 1 27 (49) 17 (53) No. of previous chemotherapy regimens no. (%) 0 5 (10) 7 (22) 1 16 (33) 9 (28) 2 5 (10) 4 (12) 3 23 (47) 12 (38) * ECOG denotes Eastern Cooperative Oncology Group, LDH lactate dehydrogenase, and ULN upper limit of the normal range. The extent of metastatic melanoma is described as the American Joint Com mittee on Cancer stage. These data were not reported for the six patients in the dose-escalation cohort who did not have melanoma. The number of previous therapies was not reported for the six patients in the dose-escalation cohort who did not have melanoma. one patient, sequential biopsy specimens were not taken from the same lesion. Statistical Analysis For the primary end point of a partial or complete response in the extension cohort, we calculated that a sample of 32 patients would provide 95% confidence (α = 0.05), with 80% power (β = 0.20), that an observed response rate of 40% would be consistent with a true response rate of more than 10%, which was considered justification for further study. For this report, January 31, 2010, was the cutoff date for the safety and efficacy follow-up. Results Patients Fifty-five patients were enrolled in the dose-escalation phase of the study (see Fig. 2 in the Supplementary Appendix, available with the full text of this article at NEJM.org); 32 additional patients with metastatic melanoma that carried the V600E BRAF mutation were treated at the recommended phase 2 dose in the extension phase (Table 1). The majority of patients (49 of 55 [89%]) in the doseescalation cohort had metastatic melanoma; 3 of the remaining 6 patients had papillary thyroid cancer that carried the V600E BRAF mutation. Screening for the V600E BRAF mutations was not a requirement for study entry during the doseescalation phase, but throughout the trial, an increasing number of patients were prospectively identified as having the mutation (for a total of 16 of the 21 patients with melanoma who were enrolled in the groups receiving 240 mg twice daily to 1120 mg twice daily). The initial crystalline formulation of PLX4032 was found to have no dose-limiting side effects or antitumor activity at doses of 200 mg daily to 1600 mg twice daily in consecutively enrolled groups of patients. Since the serum levels detected were lower than the levels predicted in preclinical models to be effective, a microprecipitatedbulk-powder formulation with substantially higher bioavailability was developed and used for the remainder of the study; the lowest dose was 160 mg twice daily, and escalated doses were 240, 320 or 360, 720, and 1120 mg twice daily (Fig. 2 in the Supplementary Appendix). Patients who had been receiving the crystalline formulation were switched to the microprecipitated-bulkpowder formulation. The protocol allowed the dose to be reduced if side effects developed. Once the recommended phase 2 dose was established for the microprecipitated-bulk-powder formulation in the dose-escalation cohort, the extension cohort was enrolled. All patients in the extension cohort had melanoma carrying the V600E BRAF mutation (Table 1). Adverse Events During the latter part of the dose-escalation phase of the trial, when the microprecipitatedbulk-powder formulation of PLX4032 was used, dose-limiting toxic effects were not observed until a dose of 720 mg twice daily was given. At the next-highest dose given to one group of patients, 812 n engl j med 363;9 nejm.org august 26, 2010
5 Inhibition of Mutated, Activated BRAF Table 2. Drug-Related Adverse Events of Grade 2 or Higher Reported in More Than 5% of the 87 Study Patients, According to the Dose of PLX4032 Given Twice Daily.* Event Arthralgia Rash <240 mg (N = 30) 240 mg (N = 4) 320 or 360 mg (N = 8) 720 mg (N = 7) number (percent) 960 mg (N = 32) 1120 mg (N = 6) Total (N = 87) Grade (25) 2 (25) 0 10 (31) 1 (17) 14 (16) Grade (3) 1 (17) 2 (2) Grade 2 1 (3) (14) 7 (22) 1 (17) 10 (12) Grade (3) 3 (50) 4 (3) Squamous-cell carcinoma, keratoacanthoma type Grade Grade 3 1 (3) 2 (50) 3 (38) 0 10 (31) 2 (33) 18 (21) Nausea Grade 2 1 (3) 0 1 (11) 1 (14) 4 (12) 1 (17) 8 (9) Grade (3) 0 1 (1) Fatigue Grade (6) 1 (17) 3 (3) Grade (6) 2 (33) 4 (5) Photosensitivity reaction Grade (14) 4 (12) 1 (17) 6 (7) Grade (3) 0 1 (1) Palmar plantar dysesthesia Grade (6) 1 (17) 3 (3) Grade (6) 0 2 (2) Pruritus Grade (12) 0 4 (5) Grade (17) 1 (1) Lymphopenia Grade (25) 0 2 (6) 0 4 (5) Grade (17) 1 (1) * Adverse events were graded according to the Common Terminology Criteria for Adverse Events (version 3.0) ( ctep.info.nih.gov/protocoldevelopment/electronic_applications/docs/ctcaev3.pdf). Four patients had a grade 4 adverse event: two had elevated γ-glutamyltransferase levels, one had fatigue, and one had reversible pancytopenia of uncertain attribution mg twice daily, four of the six patients had dose-limiting side effects: three patients with grade 3 rash (two of whom also had grade 3 fatigue) and one patient with grade 3 arthralgia (Table 2). A dose of 960 mg twice daily was evaluated and determined to be tolerated in the first six patients given the dose, so it was established as the recommended phase 2 dose for the extension cohort. Those six patients were included as the first six patients in the extension cohort. In the extension cohort, 13 patients (41%) required a dose reduction during therapy (to 720 mg twice daily in 10 patients, to 600 mg twice daily in 1 patient, and to 480 mg twice daily in 2 patients). The most common PLX4032-related grade 2 or 3 side effects observed were arthralgia, rash, nausea, photosensitivity, fatigue, cutaneous squamous-cell carcinoma, pruritus, and palmar plantar dysesthe- n engl j med 363;9 nejm.org august 26,
6 The new england journal of medicine A Mean PLX4032 AUC 0 24 (µm hr) Twice-Daily Dose (mg) Figure 2 (facing page). Representative Findings of the Effect of PLX4032 at the Recommended Phase 2 Dose in Study Patients with Melanoma That Carried the V600E Mutation. The recommended phase 2 dose was 960 mg twice daily. Panel A (hematoxylin and eosin) shows immunohistochemical analyses of the expression of phosphorylated extracellular signal-regulated kinase (ERK), cyclin D1, and Ki-67 in tumor-biopsy specimens obtained at baseline and on day 15 of treatment. Panel B shows the uptake of 18 F-fluorodeoxyglucose (FDG) at baseline and on day 15 of treatment, as assessed by means of positron-emission tomography (PET). Panel C shows computed tomographic images of lesions (arrows) in lung, liver, and bone (with each pair of images shown for a different patient) at baseline and at 8 weeks. B Mean PLX4032 Concentration (µm) Hour Day 15 Day 1 Figure 1. Mean PLX4032 Concentrations over a 24-Hour Period. Data are shown for the microprecipitated-bulk-powder formulation. Panel A shows the mean area under the plasma concentration time curve (AUC 0 24), according to the twice-daily dose. Panel B shows the mean concentration after the administration of a single dose, on day 1, or multiple doses at the steady state, on day 15, at the recommended phase 2 dose of 960 mg twice daily. I bars indicate standard deviations. sia (Table 2). In total, 89% of all side effects were grade 1 or 2. Rashes were evenly distributed among the face or neck, trunk, and extremities. Eight patients in the dose-escalation cohort (15%) and 10 patients in the extension cohort (31%) had cutaneous squamous-cell carcinomas, with a total of 35 carcinomas. These were reviewed centrally, and all but one either were keratoacanthoma type or had features of a keratoacanthoma. The median time to the appearance of a cutaneous squamous-cell carcinoma was 8 weeks; the majority of the carcinomas were resected, and in no case did they lead to discontinuation of treatment. No squamous-cell carcinomas at other organ sites were observed during the study. Pharmacokinetics Pharmacokinetic analyses revealed that exposure increased with the dose throughout the range of doses of the microprecipitated-bulk-powder formulation that were administered, with exposure being proportional to dose for doses of 240 mg twice daily through 960 mg twice daily. At the recommended phase 2 dose, 960 mg twice daily, the mean (±SD) area under the plasma concentration time curve over a 24-hour period (AUC 0 24 ) was 1741±639 μm hour (Fig. 1A), and the mean maximum concentration at steady state was 86±32 μm (Fig. 1B). The mean PLX4032 level on day 15, after repeated dosing, was six to nine times the mean level on day 1, and its mean halflife was approximately 50 hours (range, 30 to 80). With the twice-daily dosing regimen, all patients were exposed to relatively constant daily levels of the drug at steady state. Pharmacodynamics Tumor-biopsy specimens that had been obtained at baseline and at day 15 were available for seven of the patients in the extension cohort who were receiving PLX4032 at the recommended phase 2 dose. Tumor levels of phosphorylated ERK, cyclin D1, and Ki-67 were markedly reduced at day 15 as compared with baseline in all specimens tested (Fig. 2A). This finding suggests that PLX n engl j med 363;9 nejm.org august 26, 2010



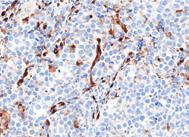









7 Inhibition of Mutated, Activated BRAF A Tumor Biopsy Phosphorylated ERK Cyclin D1 Ki-67 Baseline Day 15 B FDG-PET Baseline Day 15 C Computed Tomography Lung Liver Bone Baseline 8 Wk n engl j med 363;9 nejm.org august 26,
8 The new england journal of medicine inhibited the MAP kinase pathway, resulting in decreased cyclin D1 levels and decreased proliferation. In virtually all patients, a marked decrease in tumor uptake of FDG was noted at day 15 (Fig. 2B). Tumor Response Dose-Escalation Phase No responses were observed at doses of 160 mg twice daily of the microprecipitated-bulk-powder formulation or at any dose of the crystalline formulation. Of the patients receiving doses of 240 mg or more twice daily, 16 had melanoma with tumors that harbored the V600E BRAF mutation. Among these 16 patients, a partial or complete response was seen in the 1 patient receiving 240 mg twice daily, 2 of the 4 patients receiving 320 or 360 mg twice daily, 4 of the 6 patients receiving 720 mg twice daily, and 4 of the 5 patients receiving 1120 mg twice daily. The overall response rate was 69% (11 of 16 patients), with 10 partial responses and 1 complete response (Fig. 1A in the Supplementary Appendix). Responses were seen at all sites of metastatic disease, including the liver, small bowel, and bone (Fig. 2C). The duration of the response ranged from 2 to more than 18 months, with 4 patients still having a partial or complete response at the data cut-off date (Fig. 1B in the Supplementary Appendix). In addition to the patients with melanoma, the 3 patients with papillary thyroid cancer had a partial or complete response, with the response lasting 8 months in 1 patient (who was progression-free for 12 months) and stable disease lasting 11 and 13 months in each of the other 2 patients. A total of 5 patients with metastatic melanoma whose tumors did not have a BRAF mutation received doses of 240 mg or more twice daily. None had evidence of tumor regression during the study; 4 had progressive disease within the first 2 months of treatment. Extension Phase The extension cohort consisted solely of patients who had melanoma with the V600E BRAF mutation. All were treated at the recommended phase 2 dose of 960 mg twice daily. A total of 26 of the 32 patients had a response (81%), with a complete response in 2 patients and a partial response in 24 patients (Fig. 3A). Among patients with symptomatic metastatic disease, improvement of symptoms, such as a reduced need for narcotics for pain in 3 patients, was reported within 1 to 2 weeks. As in the dose-escalation cohort, we observed tumor responses in visceral organs and bone metastases as well as more typically responsive sites such as the lungs and lymph nodes. Responses were also routinely observed in patients with elevated lactate dehydrogenase levels (10 partial responses among the 13 patients) and in patients who had received more than one previous type of therapy (11 partial responses among the 16 patients). To date, 16 of the 32 patients are still in the study; the estimated median progression-free survival among these patients is more than 7 months, on the basis of a Kaplan Meier analysis. The estimated median overall survival has not been reached. Discussion Our trial shows that therapy targeting tumors containing activating V600E BRAF mutations can induce complete or partial tumor regression in patients. PLX4032 induced complete or partial tumor regression in 81% of patients who had melanoma with the V600E BRAF mutation. Responses were observed at all sites of disease, including the bone, liver, and small bowel. During the doseescalation phase of the trial, we also saw responses in patients who were receiving doses below the recommended phase 2 dose. These efficacy data are particularly encouraging in light of the high disease burden in most of our patients and the presence of symptomatic disease in many of them. Most side effects related to PLX4032 appeared to be proportional to the dose and exposure to the drug. Cutaneous side effects, fatigue, and arthralgia predominated. In the extension cohort, at the dose of 960 mg twice daily, approximately 40% of patients required a short- or long-term reduction in dose to 720 mg, 600 mg, or 480 mg twice daily, many for grade 2 side effects. Squamous-cell carcinoma, keratoacanthoma type, developed in a total of 10 of 32 patients (31%); we also observed squamous-cell carcinoma, keratoacanthoma type, in patients in the dose-escalation cohort. The characteristic rapid eruption of individual, dome-shaped, nonpigmented lesions and histologic findings were present in each case. Usually, squamous-cell carcinoma, keratoacanthoma type, are well-differentiated tumors with very low invasive potential and no metastatic potential; our data do not allow us to determine their behavior in patients receiving PLX4032. Recent data show that BRAF inhibitors can activate the MAP kinase pathway in cells that lack a BRAF 816 n engl j med 363;9 nejm.org august 26, 2010
9 Inhibition of Mutated, Activated BRAF A Best Overall Response % Change from Baseline Threshold for response according to RECIST Melanoma stage M1a Melanoma stage M1b Melanoma stage M1c 100 B Response over Time Melanoma stage M1a Melanoma stage M1b Melanoma stage M1c Time of partial or complete response Progressive disease Patient remaining in study Months Figure 3. Antitumor Response in Each of the 32 Patients in the Extension Cohort. All 32 patients had melanoma tumors that carried the V600E mutation of the v-raf murine sarcoma viral oncogene homologue B1 (BRAF). All were treated at the recommended phase 2 dose of 960 mg twice daily. Panel A shows the best overall response for each of the 32 patients, measured as the change from baseline in the sum of the largest diameter of each target lesion. Negative values indicate tumor shrinkage, and the dashed line indicates the threshold for a partial response according to Response Evaluation Criteria in Solid Tumors (RECIST) (i.e., shrinkage by 30%). Two patients had a complete response. Panel B shows the duration and characteristics of the responses in each patient. n engl j med 363;9 nejm.org august 26,
10 The new england journal of medicine mutation This activation may pertain to some of the side effects seen with PLX4032. Though the early response to PLX4032 seems to occur reliably, responsive tumors can develop resistance to treatment. Among the patients in the dose-escalation cohort who had a response to treatment, the duration of the response ranged from 2 to more than 18 months. The mechanism of secondary tumor resistance is not yet known. We also observed that in some patients with V600E BRAF mutations, the tumors showed resistance without evidence of an early response. The mechanism of this primary refractory state is currently under investigation. To date, we have not seen gatekeeper BRAF mutations in resistant tumors, although this issue requires more investigation. Sorafenib, which inhibits BRAF (both the wild type and the V600E mutant) and v-raf-1 murine leukemia viral oncogene homologue 1 (RAF1), has been studied in melanoma. In animal models of melanoma, sorafenib has not shown selective activity against tumors carrying BRAF mutations, and in clinical trials, sorafenib used either alone or in combination with chemotherapy has not had significant antimelanoma effects It is possible that the non-braf effects of sorafenib mediate side effects that limit the likelihood of achieving a drug concentration that is high enough to inhibit the V600E BRAF mutation. It is now clear that melanomas can be categorized by specific molecular changes that drive their proliferation. 28 The overriding hypothesis is that inhibition of the activated pathway in the individual tumor will lead to tumor regression. There is recent preliminary evidence that imatinib can induce regression in 33% of the small proportion of melanomas driven by mutations in KIT (the v-kit Hardy Zuckerman 4 feline sarcoma viral oncogene homologue). 29 In our study, PLX4032 induced responses in the vast majority of melanomas caused by BRAF mutations, which constitute 40 to 60% of all melanomas. We do not yet know whether treatment with PLX4032 will improve overall survival; an ongoing phase 3 trial (ClinicalTrials.gov number, NCT ) is addressing that question. Supported by Plexxikon and Roche Pharmaceuticals. Drs. Flaherty, Puzanov, Kim, Ribas, McArthur, Sosman, O Dwyer, and Chapman report the receipt by their institutions of grant support from Plexxikon to conduct this clinical trial; Drs. Flaherty, Puzanov, Kim, Ribas, Sosman, and Chapman report receiving consulting fees or reimbursement for travel expenses from Roche Pharmaceuticals; Dr. Sosman reports pending receipt of grant support from Roche Pharmaceuticals; Dr. O Dwyer reports receiving grant support from Plexxikon; Drs. Lee and Grippo report being employees of Roche Pharmaceuticals; and Dr. Nolop reports being an employee of Plexxikon, holding equity in the company, and receiving reimbursement for travel expenses from the company. No other potential conflict of interest relevant to this article was reported. Disclosure forms provided by the authors are available with the full text of this article at NEJM.org. We thank Drs. Katherine Nathanson and Xiaowei Xu (of the University of Pennsylvania) for leading the analysis of tumors for BRAF mutations and the immunohistochemical analysis of phosphorylated ERK and Ki-67 during the dose-escalation part of the study, Drs. Astrid Koehler and Michael Stumm (of Roche Pharmaceuticals) for leading these analyses during the extension part of the study, and Dr. Ruben Ayala (of Roche Pharmaceuticals) for the pharmacokinetic analysis. References 1. Comis RL. DTIC (NSC-45388) in malignant melanoma: a perspective. Cancer Treat Rep 1976;60: Atkins MB, Lotze MT, Dutcher JP, et al. High-dose recombinant interleukin 2 therapy for patients with metastatic melanoma: analysis of 270 patients treated between 1985 and J Clin Oncol 1999; 17: Middleton MR, Grob JJ, Aaronson N, et al. Randomized phase III study of temozolomide versus dacarbazine in the treatment of patients with advanced metastatic malignant melanoma. J Clin Oncol 2000;18: [Erratum, J Clin Oncol 2000;18:2351.] 4. Bedikian AY, Millward M, Pehamberger H, et al. Bcl-2 antisense (oblimersen sodium) plus dacarbazine in patients with advanced melanoma: the Oblimersen Melanoma Study Group. J Clin Oncol 2006; 24: Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature 2002;417: Nikiforova MN, Kimura ET, Gandhi M, et al. BRAF mutations in thyroid tumors are restricted to papillary carcinomas and anaplastic or poorly differentiated carcinomas arising from papillary carcinomas. J Clin Endocrinol Metab 2003;88: Fukushima T, Suzuki S, Mashiko M, et al. BRAF mutations in papillary carcinomas of the thyroid. Oncogene 2003;22: Cohen Y, Xing M, Mambo E, et al. BRAF mutation in papillary thyroid carcinoma. J Natl Cancer Inst 2003;95: Yuen ST, Davies H, Chan TL, et al. Similarity of the phenotypic patterns associated with BRAF and KRAS mutations in colorectal neoplasia. Cancer Res 2002; 62: Oliveira C, Pinto M, Duval A, et al. BRAF mutations characterize colon but not gastric cancer with mismatch repair deficiency. Oncogene 2003;22: Wang L, Cunningham JM, Winters JL, et al. BRAF mutations in colon cancer are not likely attributable to defective DNA mismatch repair. Cancer Res 2003;63: Tannapfel A, Sommerer F, Benicke M, et al. Mutations of the BRAF gene in cholangiocarcinoma but not in hepatocellular carcinoma. Gut 2003;52: Cho NY, Choi M, Kim BH, Cho YM, Moon KC, Kang GH. BRAF and KRAS mutations in prostatic adenocarcinoma. Int J Cancer 2006;119: Singer G, Oldt R III, Cohen Y, et al. Mutations in BRAF and KRAS characterize the development of low-grade ovarian serous carcinoma. J Natl Cancer Inst 2003;95: n engl j med 363;9 nejm.org august 26, 2010
11 Inhibition of Mutated, Activated BRAF 15. Honecker F, Wermann H, Mayer F, et al. Microsatellite instability, mismatch repair deficiency, and BRAF mutation in treatment-resistant germ cell tumors. J Clin Oncol 2009;27: Kimura ET, Nikiforova MN, Zhu Z, Knauf JA, Nikiforov YE, Fagin JA. High prevalence of BRAF mutations in thyroid cancer: genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma. Cancer Res 2003;63: Tsai J, Lee JT, Wang W, et al. Discovery of a selective inhibitor of oncogenic B-Raf kinase with potent antimelanoma activity. Proc Natl Acad Sci U S A 2008; 105: Sondergaard JN, Nazarian R, Wang Q, et al. Differential sensitivity of melanoma cell lines with BRAF V600E mutation to the specific Raf inhibitor PLX4032. J Transl Med 2010;8: Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 1982;5: Koch WH. Technology platforms for pharmacogenomic diagnostic assays. Nat Rev Drug Discov 2004;3: Heidorn SJ, Milagre C, Whittaker S, et al. Kinase-dead BRAF and oncogenic RAS cooperate to drive tumor progression through CRAF. Cell 2010;140: Poulikakos PI, Zhang C, Bollag G, Shokat KM, Rosen N. RAF inhibitors transactivate RAF dimers and ERK signalling in cells with wild-type BRAF. Nature 2010;464: Hatzivassiliou G, Song K, Yen I, et al. RAF inhibitors prime wild-type RAF to activate the MAPK pathway and enhance growth. Nature 2010;464: Wilhelm SM, Carter C, Tang L, et al. BAY exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res 2004; 64: Eisen T, Ahmad T, Flaherty KT, et al. Sorafenib in advanced melanoma: a phase II randomised discontinuation trial analysis. Br J Cancer 2006;95: McDermott DF, Sosman JA, Gonza- lez R, et al. Double-blind randomized phase II study of the combination of sorafenib and dacarbazine in patients with advanced melanoma: a report from the Study Group. J Clin Oncol 2008;26: Hauschild A, Agarwala SS, Trefzer U, et al. Results of a phase III, randomized, placebo-controlled study of sorafenib in combination with carboplatin and paclitaxel as second-line treatment in patients with unresectable stage III or stage IV melanoma. J Clin Oncol 2009;27: Curtin JA, Fridlyand J, Kageshita T, et al. Distinct sets of genetic alterations in melanoma. N Engl J Med 2005;353: Carvajal RD, Chapman PB, Wolchok JD, et al. A phase II study of imatinib mesylate (IM) for patients with advanced melanoma harboring somatic alterations of KIT. J Clin Oncol 2009;27:Suppl:15S. abstract. Copyright 2010 Massachusetts Medical Society. posting presentations at medical meetings on the internet Posting an audio recording of an oral presentation at a medical meeting on the Internet, with selected slides from the presentation, will not be considered prior publication. This will allow students and physicians who are unable to attend the meeting to hear the presentation and view the slides. If there are any questions about this policy, authors should feel free to call the Journal s Editorial Offices. n engl j med 363;9 nejm.org august 26,
Response and resistance to BRAF inhibitors in melanoma
 Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
BRAF Inhibitors in Metastatic disease. Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia
 Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
Improved Survival with Vemurafenib in Melanoma with BRAF V600E Mutation
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Improved Survival with Vemurafenib in Melanoma with BRAF V6E Mutation Paul B. Chapman, M.D., Axel Hauschild, M.D., Caroline Robert,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Improved Survival with Vemurafenib in Melanoma with BRAF V6E Mutation Paul B. Chapman, M.D., Axel Hauschild, M.D., Caroline Robert,
presentation session & clinical Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania
 Melanoma: highlights from the oral presentation session & clinical science symposium at ASCO 2009 Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania Abstracts to be discussed
Melanoma: highlights from the oral presentation session & clinical science symposium at ASCO 2009 Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania Abstracts to be discussed
Survival in BRAF V600 Mutant Advanced Melanoma Treated with Vemurafenib
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Survival in BRAF V600 Mutant Advanced Melanoma Treated with Vemurafenib Jeffrey A. Sosman, M.D., Kevin B. Kim, M.D., Lynn Schuchter,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Survival in BRAF V600 Mutant Advanced Melanoma Treated with Vemurafenib Jeffrey A. Sosman, M.D., Kevin B. Kim, M.D., Lynn Schuchter,
Normal RAS-RAF (MAPK) pathway signaling
 pathway signaling") BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
BRAF Gene Mutation Testing To Select Melanoma Patients for BRAF Inhibitor Targeted Therapy. Original Policy Date
 MP 2.04.66 BRAF Gene Mutation Testing To Select Melanoma Patients for BRAF Inhibitor Targeted Therapy Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date
MP 2.04.66 BRAF Gene Mutation Testing To Select Melanoma Patients for BRAF Inhibitor Targeted Therapy Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date
Corporate Medical Policy
 Corporate Medical Policy BRAF Gene Variant Testing to Select Melanoma or Glioma Patients File Name: Origination: Last CAP Review: Next CAP Review: Last Review: braf_gene_variant_testing_to_select_melanoma_or_glioma_patients_for_targeted_
Corporate Medical Policy BRAF Gene Variant Testing to Select Melanoma or Glioma Patients File Name: Origination: Last CAP Review: Next CAP Review: Last Review: braf_gene_variant_testing_to_select_melanoma_or_glioma_patients_for_targeted_
Corporate Medical Policy
 Corporate Medical Policy BRAF Gene Mutation Testing to Select Melanoma or Glioma Patients File Name: Origination: Last CAP Review: Next CAP Review: Last Review: braf_gene_mutation_testing_to_select_melanoma_or_glioma_patients_for_targeted_
Corporate Medical Policy BRAF Gene Mutation Testing to Select Melanoma or Glioma Patients File Name: Origination: Last CAP Review: Next CAP Review: Last Review: braf_gene_mutation_testing_to_select_melanoma_or_glioma_patients_for_targeted_
Case Report Long Term Survival and Continued Complete Response of Vemurafenib in a Metastatic Melanoma Patient with BRAF V600K Mutation
 Case Reports in Oncological Medicine Volume 2016, Article ID 2672671, 4 pages http://dx.doi.org/10.1155/2016/2672671 Case Report Long Term Survival and Continued Complete Response of Vemurafenib in a Metastatic
Case Reports in Oncological Medicine Volume 2016, Article ID 2672671, 4 pages http://dx.doi.org/10.1155/2016/2672671 Case Report Long Term Survival and Continued Complete Response of Vemurafenib in a Metastatic
Improved Survival with Vemurafenib in Melanoma with BRAF V600E Mutation
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Improved Survival with Vemurafenib in Melanoma with BRAF V6E Mutation Paul B. Chapman, M.D., Axel Hauschild, M.D., Caroline Robert,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Improved Survival with Vemurafenib in Melanoma with BRAF V6E Mutation Paul B. Chapman, M.D., Axel Hauschild, M.D., Caroline Robert,
Ipilimumab ASCO Data Review and Discussion Webcast. Monday, June 2, 2008
 Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Osimertinib Activity in Patients With Leptomeningeal Disease From Non-Small Cell Lung Cancer: Updated Results From the BLOOM Study
 Osimertinib Activity in Patients With Leptomeningeal Disease From Non-Small Cell Lung Cancer: Updated Results From the BLOOM Study Abstract 9002 Yang JC, Kim DW, Kim SW, Cho BC, Lee JS, Ye X, Yin X, Yang
Osimertinib Activity in Patients With Leptomeningeal Disease From Non-Small Cell Lung Cancer: Updated Results From the BLOOM Study Abstract 9002 Yang JC, Kim DW, Kim SW, Cho BC, Lee JS, Ye X, Yin X, Yang
Clinical Study Synopsis for Public Disclosure
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis - which is part of
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis - which is part of
Subject: Cobimetinib (Cotellic ) Tablet
 Tablet") 09-J2000-53 Original Effective Date: 03/15/16 Reviewed: 11/14/18 Revised: 12/15/18 Subject: Cobimetinib (Cotellic ) Tablet THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
09-J2000-53 Original Effective Date: 03/15/16 Reviewed: 11/14/18 Revised: 12/15/18 Subject: Cobimetinib (Cotellic ) Tablet THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Flaherty KT, Infante JR, Daud A, et al. Combined BRAF and MEK
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Flaherty KT, Infante JR, Daud A, et al. Combined BRAF and MEK
Cabozantinib for medullary thyroid cancer. February 2012
 Cabozantinib for medullary thyroid cancer February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive
Cabozantinib for medullary thyroid cancer February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive
Targeted Therapies in Melanoma
 Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Efficacy of larotrectinib in adolescents and young adults with TRK fusion cancer
 Efficacy of larotrectinib in adolescents and young adults with TRK fusion cancer Soledad Gallego, 1 Valentina Boni, 2 Ulrik Lassen, 3 Anna Farago, 4 Wafik El-Deiry, 5 David Hong, 6 Blanca López-Ibor, 2
Efficacy of larotrectinib in adolescents and young adults with TRK fusion cancer Soledad Gallego, 1 Valentina Boni, 2 Ulrik Lassen, 3 Anna Farago, 4 Wafik El-Deiry, 5 David Hong, 6 Blanca López-Ibor, 2
The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma
 and Binimetinib (MEK162) in Patients With Metastatic Melanoma") The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma Reinhard Dummer, 1 Keith Flaherty, 2 Richard Kefford, 3 Paolo A. Ascierto, 4 Laure Moutouh-de Parseval,
The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma Reinhard Dummer, 1 Keith Flaherty, 2 Richard Kefford, 3 Paolo A. Ascierto, 4 Laure Moutouh-de Parseval,
BRAF Inhibition in Melanoma
 BRAF Inhibition in Melanoma New York City, Mar 22-23, 2013 Bartosz Chmielowski, MD, PhD Assistant Clinical Professor University of California Los Angeles Disclosures Speaker Bureau: BMS, Genentech, Prometheus
BRAF Inhibition in Melanoma New York City, Mar 22-23, 2013 Bartosz Chmielowski, MD, PhD Assistant Clinical Professor University of California Los Angeles Disclosures Speaker Bureau: BMS, Genentech, Prometheus
vemurafenib 240mg film-coated tablet (Zelboraf ) SMC No. (792/12) Roche Products Ltd.
 SMC No. (792/12) Roche Products Ltd.") Resubmission vemurafenib 240mg film-coated tablet (Zelboraf ) SMC No. (792/12) Roche Products Ltd. 08 November 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Resubmission vemurafenib 240mg film-coated tablet (Zelboraf ) SMC No. (792/12) Roche Products Ltd. 08 November 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Identification of BRAF mutations in melanoma lesions with the Roche z480 instrument
 Identification of BRAF mutations in melanoma lesions with the Roche z480 instrument Márta Széll IAP, Siófok May 14, 2012 Multifactorial skin diseses: much more frequent then genodermatoses exhibit familial
Identification of BRAF mutations in melanoma lesions with the Roche z480 instrument Márta Széll IAP, Siófok May 14, 2012 Multifactorial skin diseses: much more frequent then genodermatoses exhibit familial
A View to the Future: The Development of Targeted Therapy for Melanoma. Michael Davies, M.D., Ph.D.
 A View to the Future: Science to Survivorship Symposium September 26, 2009 The Development of Targeted Therapy for Melanoma Michael Davies, M.D., Ph.D. Assistant Professor, Melanoma Medical Oncology How
A View to the Future: Science to Survivorship Symposium September 26, 2009 The Development of Targeted Therapy for Melanoma Michael Davies, M.D., Ph.D. Assistant Professor, Melanoma Medical Oncology How
EGFR Antibody. Necitumumab, LY , IMC-11F8. Drug Discovery Platform: Cancer Cell Signaling
 EGFR Antibody Necitumumab, LY3012211, IMC-11F8 Derived from Yarden Y and Shilo BZ 1 ; Schneider MR and Wolf E. 2 Drug Discovery Platform: Cancer Cell Signaling A Single-Arm, Multicenter, Open-Label, Phase
EGFR Antibody Necitumumab, LY3012211, IMC-11F8 Derived from Yarden Y and Shilo BZ 1 ; Schneider MR and Wolf E. 2 Drug Discovery Platform: Cancer Cell Signaling A Single-Arm, Multicenter, Open-Label, Phase
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only.
 The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
Presenter Disclosure Information
 Presenter Disclosure Information Tara C. Gangadhar, M.D. The following relationships exist related to this presentation: Research funding (Institution): Incyte Corporation and Merck & Co., Inc Preliminary
Presenter Disclosure Information Tara C. Gangadhar, M.D. The following relationships exist related to this presentation: Research funding (Institution): Incyte Corporation and Merck & Co., Inc Preliminary
Trial record 1 of 1 for:
 Find Studies About Studies Submit Studies Resources About Site Trial record 1 of 1 for: YO39523 Previous Study Return to List Next Study A Study of Atezolizumab Versus Placebo in Combination With Paclitaxel,
Find Studies About Studies Submit Studies Resources About Site Trial record 1 of 1 for: YO39523 Previous Study Return to List Next Study A Study of Atezolizumab Versus Placebo in Combination With Paclitaxel,
Rapid BRAF mutation detection in melanoma patients by immunohistochemistry
 http://dx.doi.org/10.17202/juso.2017.4.1 Journal of Universal Science Vol 4(1): 1-5, 2017 Rapid BRAF mutation detection in melanoma patients by immunohistochemistry László FÜLÖP 1, Katalin GÖTZER 1, Erzsébet
http://dx.doi.org/10.17202/juso.2017.4.1 Journal of Universal Science Vol 4(1): 1-5, 2017 Rapid BRAF mutation detection in melanoma patients by immunohistochemistry László FÜLÖP 1, Katalin GÖTZER 1, Erzsébet
Vemurafenib: a new treatment for BRAF-V600 mutated advanced melanoma
 Cancer Management and Research open access to scientific and medical research Open Access Full Text Article Vemurafenib: a new treatment for BRAF-V600 mutated advanced melanoma Review Rosalie Fisher James
Cancer Management and Research open access to scientific and medical research Open Access Full Text Article Vemurafenib: a new treatment for BRAF-V600 mutated advanced melanoma Review Rosalie Fisher James
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Conflict of Interest Disclosure
 "NRAS mutation status in advanced melanoma: how much does this really matter to prognosis and therapy?" John Jakob, MD, PhD Department of Melanoma Medical Oncology, The University of Texas M.D. Anderson
"NRAS mutation status in advanced melanoma: how much does this really matter to prognosis and therapy?" John Jakob, MD, PhD Department of Melanoma Medical Oncology, The University of Texas M.D. Anderson
Drug Discovery Platform: Cancer Cell Signaling. MET Inhibitor. Merestinib, LY Christensen JG, et al1; Eder JP, et al 2
 MET Inhibitor Drug Discovery Platform: Cancer Cell Signaling Christensen JG, et al1; Eder JP, et al 2 A Randomized, Double-Blind, Phase 2 Study of Ramucirumab or Merestinib or Placebo Plus and Gemcitabine
MET Inhibitor Drug Discovery Platform: Cancer Cell Signaling Christensen JG, et al1; Eder JP, et al 2 A Randomized, Double-Blind, Phase 2 Study of Ramucirumab or Merestinib or Placebo Plus and Gemcitabine
Clinical Significance of BRAF Gene Mutations in Patients with Non-small Cell Lung Cancer
 Clinical Significance of BRAF Gene Mutations in Patients with Non-small Cell Lung Cancer MASASHI KOBAYASHI 1, MAKOTO SONOBE 1, TSUYOSHI TAKAHASHI 1, AKIHIKO YOSHIZAWA 2, MASASHI ISHIKAWA 1, RYUTARO KIKUCHI
Clinical Significance of BRAF Gene Mutations in Patients with Non-small Cell Lung Cancer MASASHI KOBAYASHI 1, MAKOTO SONOBE 1, TSUYOSHI TAKAHASHI 1, AKIHIKO YOSHIZAWA 2, MASASHI ISHIKAWA 1, RYUTARO KIKUCHI
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
A Case Study: Ipilimumab in Pre-treated Metastatic Melanoma
 A Case Study: Ipilimumab in Pre-treated Metastatic Melanoma Tai-Tsang Chen, PhD Global Biometric Sciences, Bristol-Myers Squibb EFSPI Statistical Meeting on Evidence Synthesis Brussels, Belgium November
A Case Study: Ipilimumab in Pre-treated Metastatic Melanoma Tai-Tsang Chen, PhD Global Biometric Sciences, Bristol-Myers Squibb EFSPI Statistical Meeting on Evidence Synthesis Brussels, Belgium November
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
MET Inhibitor. Merestinib, LY Drug Discovery Platform: Cancer Cell Signaling. Derived from Christensen JG, et al 1 ; Eder JP, et al.
 MET Inhibitor Merestinib, LY2801653 Derived from Christensen JG, et al 1 ; Eder JP, et al. 2 Drug Discovery Platform: Cancer Cell Signaling A Randomized, Double-Blind, Phase 2 Study of Ramucirumab or Merestinib
MET Inhibitor Merestinib, LY2801653 Derived from Christensen JG, et al 1 ; Eder JP, et al. 2 Drug Discovery Platform: Cancer Cell Signaling A Randomized, Double-Blind, Phase 2 Study of Ramucirumab or Merestinib
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
CombiRT in Metastatic Melanoma Trial
 CombiRT in Metastatic Melanoma Trial An open-label, single-arm, phase I/II, multicenter study to evaluate the safety and efficacy of the combination of dabrafenib, trametinib and palliative radiotherapy
CombiRT in Metastatic Melanoma Trial An open-label, single-arm, phase I/II, multicenter study to evaluate the safety and efficacy of the combination of dabrafenib, trametinib and palliative radiotherapy
Phase II Cancer Trials: When and How
 Phase II Cancer Trials: When and How Course for New Investigators August 21-23, 2013 Acknowledgment Elizabeth Eisenhauer for some slides! Learning Objectives At the end of the session the participant should
Phase II Cancer Trials: When and How Course for New Investigators August 21-23, 2013 Acknowledgment Elizabeth Eisenhauer for some slides! Learning Objectives At the end of the session the participant should
University of California Los Angeles, Los Angeles, CA; 2. Department of Dermatology, University of Kiel, Kiel, Germany;
 Final Efficacy Results of A3671009, a Phase III Study of Tremelimumab vs Chemotherapy (Dacarbazine or Temozolomide) in First-line Patients With Unresectable Melanoma Antoni Ribas, 1 Axel Hauschild, 2 Richard
Final Efficacy Results of A3671009, a Phase III Study of Tremelimumab vs Chemotherapy (Dacarbazine or Temozolomide) in First-line Patients With Unresectable Melanoma Antoni Ribas, 1 Axel Hauschild, 2 Richard
Circulating Tumor DNA in GIST and its Implications on Treatment
 Circulating Tumor DNA in GIST and its Implications on Treatment October 2 nd 2017 Dr. Ciara Kelly Assistant Attending Physician Sarcoma Medical Oncology Service Objectives Background Liquid biopsy & ctdna
Circulating Tumor DNA in GIST and its Implications on Treatment October 2 nd 2017 Dr. Ciara Kelly Assistant Attending Physician Sarcoma Medical Oncology Service Objectives Background Liquid biopsy & ctdna
ClinicalTrials.gov Protocol and Results Registration System (PRS) Receipt Release Date: 09/30/2015. ClinicalTrials.gov ID: NCT
 Receipt Release Date: 09/30/2015. ClinicalTrials.gov ID: NCT") ClinicalTrials.gov Protocol and Results Registration System (PRS) Receipt Release Date: 09/30/2015 ClinicalTrials.gov ID: NCT01378962 Study Identification Unique Protocol ID: ML25514 Brief Title: A Study
ClinicalTrials.gov Protocol and Results Registration System (PRS) Receipt Release Date: 09/30/2015 ClinicalTrials.gov ID: NCT01378962 Study Identification Unique Protocol ID: ML25514 Brief Title: A Study
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
CHK1 Inhibitor. Prexasertib, LY MsOH H 2 O. Drug Discovery Platform: Cancer Cell Signaling
 CHK1 Inhibitor Prexasertib, LY2606368 MsOH H 2 O Derived from Garrett MD and Collins I 1 ; Thompson R and Eastman A. 2 Drug Discovery Platform: Cancer Cell Signaling A Phase 2 Study of LY2606368 in Patients
CHK1 Inhibitor Prexasertib, LY2606368 MsOH H 2 O Derived from Garrett MD and Collins I 1 ; Thompson R and Eastman A. 2 Drug Discovery Platform: Cancer Cell Signaling A Phase 2 Study of LY2606368 in Patients
NCCP Chemotherapy Regimen. Vemurafenib Monotherapy
 INDICATIONS FOR USE: Vemurafenib Monotherapy INDICATION ICD10 Regimen Code *Reimbursement Indicator Treatment of adult patients with BRAF V600 mutation-positive unresectable or metastatic melanoma. C43
INDICATIONS FOR USE: Vemurafenib Monotherapy INDICATION ICD10 Regimen Code *Reimbursement Indicator Treatment of adult patients with BRAF V600 mutation-positive unresectable or metastatic melanoma. C43
Phase II Cancer Trials: When and How
 Phase II Cancer Trials: When and How Course for New Investigators August 9-12, 2011 Learning Objectives At the end of the session the participant should be able to Define the objectives of screening vs.
Phase II Cancer Trials: When and How Course for New Investigators August 9-12, 2011 Learning Objectives At the end of the session the participant should be able to Define the objectives of screening vs.
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Clinical Activity and Safety of Anti-PD-1 (BMS , MDX-1106) in Patients with Advanced Non-Small-Cell Lung Cancer
 in Patients with Advanced Non-Small-Cell Lung Cancer") Clinical Activity and Safety of Anti-PD-1 (BMS-936558, MDX-1106) in Patients with Advanced Non-Small-Cell Lung Cancer J.R. Brahmer, 1 L. Horn, 2 S.J. Antonia, 3 D. Spigel, 4 L. Gandhi, 5 L.V. Sequist,
Clinical Activity and Safety of Anti-PD-1 (BMS-936558, MDX-1106) in Patients with Advanced Non-Small-Cell Lung Cancer J.R. Brahmer, 1 L. Horn, 2 S.J. Antonia, 3 D. Spigel, 4 L. Gandhi, 5 L.V. Sequist,
Bristol-Myers Squibb, Braine-l Alleud, Belgium; 12 MD Anderson Cancer Center, Houston, TX, USA
 3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
Initial Results from an Open-label, Doseescalation Phase I Study of the Oral BRAF Inhibitor LGX818 in BRAF V600 mutant Advanced Melanoma
 Initial Results from an Open-label, Doseescalation Phase I Study of the Oral BRAF Inhibitor LGX818 in BRAF V600 mutant Advanced Melanoma Reinhard Dummer, 1 Caroline Robert, 2 Marta Nyakas, 3 Grant McArthur,
Initial Results from an Open-label, Doseescalation Phase I Study of the Oral BRAF Inhibitor LGX818 in BRAF V600 mutant Advanced Melanoma Reinhard Dummer, 1 Caroline Robert, 2 Marta Nyakas, 3 Grant McArthur,
Corporate Medical Policy
 Corporate Medical Policy Molecular Analysis for Targeted Therapy for Non-Small Cell Lung File Name: Origination: Last CAP Review: Next CAP Review: Last Review: molecular_analysis_for_targeted_therapy_for_non_small_cell_lung_cancer
Corporate Medical Policy Molecular Analysis for Targeted Therapy for Non-Small Cell Lung File Name: Origination: Last CAP Review: Next CAP Review: Last Review: molecular_analysis_for_targeted_therapy_for_non_small_cell_lung_cancer
Study No Title : Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Impressive response to dual BRAF and MEK inhibition in patients with BRAF mutant intrahepatic cholangiocarcinoma 2 case reports and a brief review
 Case Report Impressive response to dual BRAF and MEK inhibition in patients with BRAF mutant intrahepatic cholangiocarcinoma 2 case reports and a brief review Viraj Lavingia 1, Marwan Fakih 2 1 Department
Case Report Impressive response to dual BRAF and MEK inhibition in patients with BRAF mutant intrahepatic cholangiocarcinoma 2 case reports and a brief review Viraj Lavingia 1, Marwan Fakih 2 1 Department
Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors
 Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors Allison Ackerman, MD, PhD 1 ; Oliver Klein, MD 2 ; David F. McDermott, MD 1 ; Wei Wang, PhD 3
Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors Allison Ackerman, MD, PhD 1 ; Oliver Klein, MD 2 ; David F. McDermott, MD 1 ; Wei Wang, PhD 3
Clinical Trials. Phase II Studies. Connective Tissue Oncology Society. Jon Trent, MD, PhD
 Clinical Trials Phase II Studies Jon Trent, MD, PhD Associate Professor Dept. of Sarcoma Medical Oncology The University of Texas, M. D. Anderson Cancer Center Connective Tissue Oncology Society GIST Overview
Clinical Trials Phase II Studies Jon Trent, MD, PhD Associate Professor Dept. of Sarcoma Medical Oncology The University of Texas, M. D. Anderson Cancer Center Connective Tissue Oncology Society GIST Overview
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-028 Study
 Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Clinical Policy: Nivolumab (Opdivo) Reference Number: CP.PHAR.121
 Reference Number: CP.PHAR.121") Clinical Policy: (Opdivo) Reference Number: CP.PHAR.121 Effective Date: 07/15 Last Review Date: 04/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: (Opdivo) Reference Number: CP.PHAR.121 Effective Date: 07/15 Last Review Date: 04/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
pan-canadian Oncology Drug Review Final Clinical Guidance Report Vemurafenib (Zelboraf) for Advanced Melanoma October 1, 2012
 for Advanced Melanoma October 1, 2012") pan-canadian Oncology Drug Review Final Clinical Guidance Report Vemurafenib (Zelboraf) for Advanced Melanoma October 1, 2012 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Vemurafenib (Zelboraf) for Advanced Melanoma October 1, 2012 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Locally Advanced and Metastatic Melanoma. Relevant disclosures 6/23/2018. What is the median survival of metastatic melanoma? Abel D.
 Locally Advanced and Metastatic Melanoma Abel D. Jarell, MD, FAAD Adjunct Dartmouth School of Medicine, Hanover, NH Northeast Dermatology Associates, Portsmouth, NH Relevant disclosures What is the median
Locally Advanced and Metastatic Melanoma Abel D. Jarell, MD, FAAD Adjunct Dartmouth School of Medicine, Hanover, NH Northeast Dermatology Associates, Portsmouth, NH Relevant disclosures What is the median
Update on new agents in Gastrointestinal Tumor (GIST)
") Update on new agents in Gastrointestinal Tumor (GIST) Albiruni R Abdul Razak Medical Oncology Sarcoma Site Lead Princess Margaret Cancer Centre/Mount Sinai Hospital 21 st October 2017 1 Disclosure Research
Update on new agents in Gastrointestinal Tumor (GIST) Albiruni R Abdul Razak Medical Oncology Sarcoma Site Lead Princess Margaret Cancer Centre/Mount Sinai Hospital 21 st October 2017 1 Disclosure Research
Prospective Case Series of Cutaneous Adverse Effects Associated With Dabrafenib and Trametinib
 670368CMSXXX10.1177/1203475416670368Journal of Cutaneous Medicine and SurgeryLacroix and Wang research-article2016 Original Article Prospective Case Series of Cutaneous Adverse Effects Associated With
670368CMSXXX10.1177/1203475416670368Journal of Cutaneous Medicine and SurgeryLacroix and Wang research-article2016 Original Article Prospective Case Series of Cutaneous Adverse Effects Associated With
BRAF Gene Mutation Testing to Select Melanoma Patients for BRAF Inhibitor Targeted Therapy
 Section: Medicine Effective Date: January 15, 2015 Subsection: Laboratory/Pathology Original Policy Date: March 9, 2012 Subject: BRAF Gene Mutation Testing to Select Melanoma Last Review Status/Date: December
Section: Medicine Effective Date: January 15, 2015 Subsection: Laboratory/Pathology Original Policy Date: March 9, 2012 Subject: BRAF Gene Mutation Testing to Select Melanoma Last Review Status/Date: December
Unmet Need Mucosal and Uveal Melanoma
 Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
Clinical Policy: Nivolumab (Opdivo) Reference Number: CP.PHAR.121 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PHAR.121 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Opdivo) Reference Number: CP.PHAR.121 Effective Date: 07.15 Last Review Date: 01.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Opdivo) Reference Number: CP.PHAR.121 Effective Date: 07.15 Last Review Date: 01.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic
 Dabrafenib for treating unresectable, advanced or metastatic") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic BRAF V600 mutation-positive melanoma mutation-positive melanoma
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic BRAF V600 mutation-positive melanoma mutation-positive melanoma
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only.
 The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
OUR EXPERIENCES WITH ERLOTINIB IN SECOND AND THIRD LINE TREATMENT PATIENTS WITH ADVANCED STAGE IIIB/ IV NON-SMALL CELL LUNG CANCER
 & OUR EXPERIENCES WITH ERLOTINIB IN SECOND AND THIRD LINE TREATMENT PATIENTS WITH ADVANCED STAGE IIIB/ IV NON-SMALL CELL LUNG CANCER Interim Data Report of TRUST study on patients from Bosnia and Herzegovina
& OUR EXPERIENCES WITH ERLOTINIB IN SECOND AND THIRD LINE TREATMENT PATIENTS WITH ADVANCED STAGE IIIB/ IV NON-SMALL CELL LUNG CANCER Interim Data Report of TRUST study on patients from Bosnia and Herzegovina
New Targeted Therapies in Melanoma
 Vemurafenib and ipilimumab have improved overall survival in patients with metastatic melanoma. Tenzin Norbu Lama. Returning Home (detail). New Targeted Therapies in Melanoma Ragini R. Kudchadkar, MD,
Vemurafenib and ipilimumab have improved overall survival in patients with metastatic melanoma. Tenzin Norbu Lama. Returning Home (detail). New Targeted Therapies in Melanoma Ragini R. Kudchadkar, MD,
Novel EGFR TKI Theliatinib: An Open Label, Dose Escalation Phase I Clinical Trial
 Novel EGFR TKI Theliatinib: An Open Label, Dose Escalation Phase I Clinical Trial 2014-309-00CH1 Presenter: Jifang Gong, Beijing Cancer Hospital Lin Shen 1, Li Zhang 2, Hongyun Zhao 2, Wenfeng Fang 2,
Novel EGFR TKI Theliatinib: An Open Label, Dose Escalation Phase I Clinical Trial 2014-309-00CH1 Presenter: Jifang Gong, Beijing Cancer Hospital Lin Shen 1, Li Zhang 2, Hongyun Zhao 2, Wenfeng Fang 2,
White paper Evaluation of BRAF (V600E) Mutation by Immunohistochemical Staining with anti-braf V600E (VE1) Antibody: A Comparison with Sanger
 Mutation by Immunohistochemical Staining with anti-braf V600E (VE1) Antibody: A Comparison with Sanger") White paper Evaluation of BRAF (V600E) Mutation by Immunohistochemical Staining with anti-braf V600E (VE1) Antibody: A Comparison with Sanger Sequencing 2 Evaluation of BRAF (V600E) Mutation by Immuno-histochemical
White paper Evaluation of BRAF (V600E) Mutation by Immunohistochemical Staining with anti-braf V600E (VE1) Antibody: A Comparison with Sanger Sequencing 2 Evaluation of BRAF (V600E) Mutation by Immuno-histochemical
ClinicalTrials.gov Identifier: NCT Adi Diab 1, Nizar Tannir 1, Daniel Cho
 Pivot-02: Preliminary safety, efficacy and biomarker results from dose escalation of the Phase 1/2 study of CD-122-biased agonist NKTR-214 plus nivolumab in patients with locally advanced/metastatic melanoma,
Pivot-02: Preliminary safety, efficacy and biomarker results from dose escalation of the Phase 1/2 study of CD-122-biased agonist NKTR-214 plus nivolumab in patients with locally advanced/metastatic melanoma,
Progression of RAS-Mutant Leukemia during RAF Inhibitor Treatment
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e brief report Progression of RAS-Mutant Leukemia during RAF Inhibitor Treatment Margaret K. Callahan, M.D., Ph.D., Raajit Rampal, M.D., Ph.D., James
T h e n e w e ngl a nd j o u r na l o f m e dic i n e brief report Progression of RAS-Mutant Leukemia during RAF Inhibitor Treatment Margaret K. Callahan, M.D., Ph.D., Raajit Rampal, M.D., Ph.D., James
BRAF Genetic Testing to Select Melanoma or Glioma Patients for Targeted Therapy
 Medical Policy Manual Genetic Testing, Policy No. 41 BRAF Genetic Testing to Select Melanoma or Glioma Patients for Targeted Therapy Next Review: August 2019 Last Review: July 2018 Effective: August 1,
Medical Policy Manual Genetic Testing, Policy No. 41 BRAF Genetic Testing to Select Melanoma or Glioma Patients for Targeted Therapy Next Review: August 2019 Last Review: July 2018 Effective: August 1,
BRAF Mutation Analysis
 Last Review Date: October 13, 2017 Number: MG.MM.LA.38aC Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: October 13, 2017 Number: MG.MM.LA.38aC Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Overall and Progression-Free Survival in Metastatic Melanoma: Analysis of a Single-Institution Database
 This review of a single-institution experience in treating metastatic melanoma examines the utility of different treatments and suggests guidelines for interpreting survival and disease-free survival in
This review of a single-institution experience in treating metastatic melanoma examines the utility of different treatments and suggests guidelines for interpreting survival and disease-free survival in
Neratinib in patients with HER2-mutant, metastatic cervical cancer: findings from the phase 2 SUMMIT basket trial
 Neratinib in patients with HER2-mutant, metastatic cervical cancer: findings from the phase 2 SUMMIT basket trial Anishka D Souza 1, Lynda D. Roman 1, Cristina Saura 2, Irene Braña 2, Geoffrey I. Shapiro
Neratinib in patients with HER2-mutant, metastatic cervical cancer: findings from the phase 2 SUMMIT basket trial Anishka D Souza 1, Lynda D. Roman 1, Cristina Saura 2, Irene Braña 2, Geoffrey I. Shapiro
n engl j med 367;2 nejm.org july 12,
 The new england journal of medicine established in 1812 july 12, 212 vol. 367 no. 2 Improved Survival with MEK Inhibition in BRAF-Mutated Melanoma Keith T. Flaherty, M.D., Caroline Robert, M.D., Ph.D.,
The new england journal of medicine established in 1812 july 12, 212 vol. 367 no. 2 Improved Survival with MEK Inhibition in BRAF-Mutated Melanoma Keith T. Flaherty, M.D., Caroline Robert, M.D., Ph.D.,
Product: Talimogene Laherparepvec Clinical Study Report: Date: 31 October 2018 Page 1
 Date: 31 October 2018 Page 1 2. SYNOPSIS Name of Sponsor: Amgen Inc., Thousand Oaks, CA, USA Name of Finished Product: Imlygic Name of Active Ingredient: Talimogene laherparepvec Title of Study: A Phase
Date: 31 October 2018 Page 1 2. SYNOPSIS Name of Sponsor: Amgen Inc., Thousand Oaks, CA, USA Name of Finished Product: Imlygic Name of Active Ingredient: Talimogene laherparepvec Title of Study: A Phase
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP
 Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
Supplementary Table 1: Summary of 33 Patients Treated with Abemaciclib in Dose Escalation
 Supplementary Table 1: Summary of 33 Patients Treated with Abemaciclib in Dose Escalation Cohort Dose and Frequency Age and Sex Tumor Type Number of Cycles Best Overall Response 4M Colorectal cancer -
Supplementary Table 1: Summary of 33 Patients Treated with Abemaciclib in Dose Escalation Cohort Dose and Frequency Age and Sex Tumor Type Number of Cycles Best Overall Response 4M Colorectal cancer -
Update on Genetic Testing for Melanoma
 Update on Genetic Testing for Melanoma Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania February 18, 2018 AAD
Update on Genetic Testing for Melanoma Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania February 18, 2018 AAD
TGFβR1 Kinase Inhibitor
 TGFβR1 Kinase Inhibitor Galunisertib, LY2157299 H 2 0 Derived from Prud homme GJ 1 ; Flavell RA, et al. 2 Drug Discovery Platform: Cancer Angiogenesis and Tumor Microenvironment/Immuno-Oncology A Phase
TGFβR1 Kinase Inhibitor Galunisertib, LY2157299 H 2 0 Derived from Prud homme GJ 1 ; Flavell RA, et al. 2 Drug Discovery Platform: Cancer Angiogenesis and Tumor Microenvironment/Immuno-Oncology A Phase
SUPPLEMENTARY INFORMATION
 doi:10.1038/nature23291 Supplementary discussion part 1 Our model suggests that, in tumours that express Class 3 BRAF mutants and activated RAS, both BRAF MUT /RAF WT heterodimers and WT RAF dimers are
doi:10.1038/nature23291 Supplementary discussion part 1 Our model suggests that, in tumours that express Class 3 BRAF mutants and activated RAS, both BRAF MUT /RAF WT heterodimers and WT RAF dimers are
Anaplastic Thyroid Cancer:
 1 Anaplastic Thyroid Cancer: A Doctor s Perspective for Patients and Families Living with the Disease By Maria E. Cabanillas, M.D., F.A.C.E. Associate Professor and Faculty Director of Clinical Research
1 Anaplastic Thyroid Cancer: A Doctor s Perspective for Patients and Families Living with the Disease By Maria E. Cabanillas, M.D., F.A.C.E. Associate Professor and Faculty Director of Clinical Research
Principal Investigator: Robert J. Jones, MD, Beatson Cancer Center, 1053 Great Western Road, Glasgow; United Kingdom
 SYNOPSIS Issue Date: 14 October 2010 Document No.: EDMS-ERI-13494974:2.0 Name of Sponsor/Company Name of Finished Product Name of Active Ingredient(s) Protocol No.: COU-AA-BE Cougar Biotechnology, Inc.
SYNOPSIS Issue Date: 14 October 2010 Document No.: EDMS-ERI-13494974:2.0 Name of Sponsor/Company Name of Finished Product Name of Active Ingredient(s) Protocol No.: COU-AA-BE Cougar Biotechnology, Inc.
References: Published Clinical Trials in Metastatic Melanoma
 References: Published Clinical Trials in Metastatic Melanoma Melanoma historical data summary While results from open-label, or uncontrolled, or small # center studies can vary enormously, results from
References: Published Clinical Trials in Metastatic Melanoma Melanoma historical data summary While results from open-label, or uncontrolled, or small # center studies can vary enormously, results from
Media Release. Basel, 29 September 2014
 Media Release Basel, 29 September 2014 Roche s investigational combination of cobimetinib plus Zelboraf (vemurafenib) provided significant benefit to people with advanced melanoma over Zelboraf alone Cobimetinib
Media Release Basel, 29 September 2014 Roche s investigational combination of cobimetinib plus Zelboraf (vemurafenib) provided significant benefit to people with advanced melanoma over Zelboraf alone Cobimetinib
MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES
 MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES Although response is not the primary endpoint of this trial, subjects with measurable disease will be assessed by standard criteria. For the purposes of this
MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES Although response is not the primary endpoint of this trial, subjects with measurable disease will be assessed by standard criteria. For the purposes of this
Qué hemos aprendido hasta hoy? What have we learned so far?
 Qué hemos aprendido hasta hoy? What have we learned so far? Luís Costa Hospital de Santa Maria & Instituto de Medicina Molecular Faculdade de Medicina de Lisboa Disclosures Research Grants: Amgen; Novartis;
Qué hemos aprendido hasta hoy? What have we learned so far? Luís Costa Hospital de Santa Maria & Instituto de Medicina Molecular Faculdade de Medicina de Lisboa Disclosures Research Grants: Amgen; Novartis;
Synopsis (C1034T02) CNTO 95 Module 5.3 Clinical Study Report C1034T02
 CNTO 95 Module 5.3 Clinical Study Report C1034T02") Module 5.3 Protocol: EudraCT No.: 2004-002130-18 Title of the study: A Phase 1/2, Multi-Center, Blinded, Randomized, Controlled Study of the Safety and Efficacy of the Human Monoclonal Antibody to Human
Module 5.3 Protocol: EudraCT No.: 2004-002130-18 Title of the study: A Phase 1/2, Multi-Center, Blinded, Randomized, Controlled Study of the Safety and Efficacy of the Human Monoclonal Antibody to Human
DCC-2618, a novel pan-kit and PDGFR
 DCC-2618, a novel pan-kit and PDGFRα Kinase switch control inhibitor demonstrates encouraging activity in patients (pts) with Gastrointestinal Stromal Tumors (GIST) N. Somaiah, A. Razak, M. Gordon, F.
DCC-2618, a novel pan-kit and PDGFRα Kinase switch control inhibitor demonstrates encouraging activity in patients (pts) with Gastrointestinal Stromal Tumors (GIST) N. Somaiah, A. Razak, M. Gordon, F.
Cancer Registry Report. Cancer Focus: Melanoma
 Cancer Registry Report Cancer Focus: Melanoma In 2005, nearly 60,000 patients were diagnosed with melanoma, resulting in about 7800 deaths Fortunately, melanoma is often diagnosed in an early stage when
Cancer Registry Report Cancer Focus: Melanoma In 2005, nearly 60,000 patients were diagnosed with melanoma, resulting in about 7800 deaths Fortunately, melanoma is often diagnosed in an early stage when
Technology appraisal guidance Published: 12 December 2012 nice.org.uk/guidance/ta269
 Vemurafenib for treating locally advanced or metastatic BRAF V600 mutation-positive malignant melanoma Technology appraisal guidance Published: 12 December 2012 nice.org.uk/guidance/ta269 NICE 2018. All
Vemurafenib for treating locally advanced or metastatic BRAF V600 mutation-positive malignant melanoma Technology appraisal guidance Published: 12 December 2012 nice.org.uk/guidance/ta269 NICE 2018. All
Clinical Policy: Cetuximab (Erbitux) Reference Number: PA.CP.PHAR.317
 Reference Number: PA.CP.PHAR.317") Clinical Policy: (Erbitux) Reference Number: PA.CP.PHAR.317 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that patients
Clinical Policy: (Erbitux) Reference Number: PA.CP.PHAR.317 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that patients
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Sponsor / Company: Sanofi Drug substance(s): SAR (iniparib)
: SAR (iniparib)") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):