Case Presentation HPI. PMHx: HTN, BPH, psychiatric disorder, negative cardiac stress test 4/2010. Allergies: NKDA
|
|
|
- Ethel Stewart
- 5 years ago
- Views:
Transcription
1
2 Case Presentation HPI 62 year-old male presents with several episodes of anterior chest pain. Full cardiac evaluation was negative for ischemia. CT scan revealed a 4cm anterior mediastinal mass. Pt denies cough or respiratory issues. No weakness or diplopia. PMHx: HTN, BPH, psychiatric disorder, negative cardiac stress test 4/2010 Allergies: NKDA Meds: Lutensin, Atenolol, Norvasc, Fomax, Zyprexa, ASA 81 Shx: non-smoker
3 Case Presentation Physical Exam Afebrile, VSS Pupils equal and reactive, no ptosis No bruits, no lymphadenopathy S1S2, RRR Labs Hb/Hct: 13/39 Electrolytes- wnl Coags- wnl AChR-AB: negative Lungs clear bilaterally Soft abd NT/ND, no inguinal LN s

4 Chest Xray

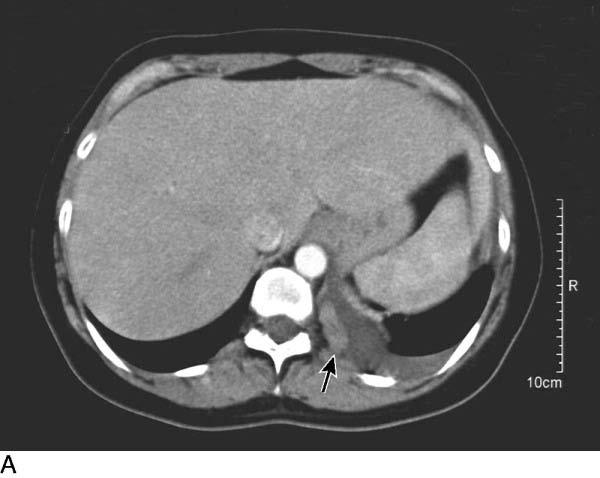
5 CT scan
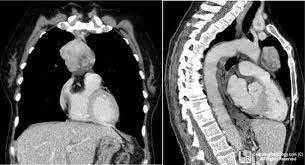
6 CT Scan
7 OR Procedure: Partial sternotomy, excision of thymic mass, partial pericardectomy, partial excision of innominate vein with patch reconstruction Pathology: Thymus- invasive squamous cell Ca of thymic origin Margins- all negative, except posterior (pericardial)- positive Positive lymphovascular invasion 2/9 LN positive for carcinoma T3, N1, Mx

8 Operative Procedure

9 Operative Procedure

10 Operative Procedure

11 Operative Procedure

12 Operative Procedure

13 Operative Procedure

14 Operative Procedure

15 Operative Procedure
16 Post-Operative Course Stable overnight stay in PACU on POD#0 Clears and OOB on POD#1 Chest tube output around 300 ml SSF Chest tubes removed on POD# 3 Discharged Home on POD#5

17 Mediastinum Midline region between the two lungs and their pleural coverings Occupied principally by heart, great vessels, trachea, bronchi, esophagus, and thymus Divided into Superior and Inferior (anterior, middle, and posterior)
18 Mediastinum Most common tumors of anterior superior mediastinum 4-T s- thymoma, terrible lymphoma, teratoma and thyroid lesions These represent more than 90% of all anterior mediastinal masses Posterior mediastinum DATES: Descending aorta, Azygous vein and hemiazygos vein, Thoracic duct, Esophagus, Sympathetic trunk/ganglia Thymoma is the most common mediastinal neoplasm in adults

19 Thymus A lymphoepithelial organ derived embryologically from 3 rd pair pharyngeal pouches that descend caudally and medially on the 7 th week of life By the 8 th week the gland has fused to form a four-lobed gland attached to the anterior pericardium Can be as cephalad as the hyoid bone or as far caudad as xiphoid process
20 Thymus Fully developed, it is a bilobed gland that sits in the anterior mediastinum It is separated from sternum by loose connective tissue, it lies anterior to pericardium and great vessels It can extend laterally to phrenic nerves and is partially covered by the pleural reflections It is in close contact to the left inomminate vein
21 Thymus Arterial supply Internal thoracic (mammary)- main Inferior thyroid Pericardiophrenic arteries Venous drainage From both lobes, veins ascend posteriorly into left brachiocephalic or rarely directly into SVC
22 Thymus Central lymphoid organ that transforms null lymphocytes into thymic or T-lymphocytes, which are responsible for cellular immunity Symptoms may arise from direct lesion compression or invasion, as well as from immunologic, hyperplastic or neoplastic manifestations
23 Thymoma Thymomas are epithelial tumors of the thymus 65% of thymomas are encapsulated (noninvasive) and 35% are invasive. Most common mediastinal neoplasm in adults, 40% of all anterior mediastinal masses Most pts between ages at diagnosis Indolent growth pattern, but malignant due to its potential for local invasion, pleural dissemination and systemic metastases 1/3 of pts with localized dz are symptomatic: cough or chest pain
24 Thymoma Locally advanced or disseminated dz may present with severe CP, SOB, phrenic n. paralysis, pleural effusions, and/or SVC syndrome MG- most common autoimmune disorder associated with thymomas-ocurring in 30-40% of pts; 10% of MG pts have thymomas Up to 30% of pts with thymoma present with other immune disorders- red cell aplasia and hypogammglobulinema
25 Diagnosis CT scan with IV contrast Defines size and relationship to intrathoracic structures Presence of droplet metastases- parietal pleural deposits that are unique to thymomas Differ from malignant nonseminomatous germ cell tumors Alpha feto protein (AFP) and B-HCG Thyroid lesions are contiguous with thyroid gland on CT scan; I-131 nuclear scans to confirm
26 Droplet Metastases
27 Diagnosis Two main DDx for anterior mediastinal mass Lymphoma and thymoma Thymomas- older pts, association with immune disorder, no constitutional symptoms and no lymphadenopathy Utility of PET scan for thymomas is being evaluated cannot differ between lymphoma and thymoma, but it can identify droplet metastases
28 Diagnosis En bloc thymectomy for clinically determined early-stage thymoma For larger lesions FNA-lacks sensitivity CT guided core bx - seeding Anterior mediastinostomy Cervical mediastinoscopy VATS ( seeding)
29 Staging WHO classification based on histology Morphology and lymphocyte-to-epithelial ratio Masaoka Anatomic classification Most accepted system on which management recommendations are based
30 Staging Masaoka Anatomic classification Stage I: Macroscopically and microscopically encapsulated Stage II A- microscopic transcapsular invasion B- macroscopic invasion into surrounding fat or grossly adherent but not through pleura or pericardium Stage III: Invasion into neighboring organs A- without invasion into great vessels B- with invasion of great vessels Stage IV A- pleural or pericardial dissemination B- lymphogenous or hematogenous metastasis
31 Pre-op Assessment Anterior mediastinal mass (thymoma) H&P, AchR-AB assay, MuSKR-AB, EMG studies, TFTs, PFTs, CXR, CT scan, and MRI Pre-op optimization is crucial, especially when thymectomy is being done for MG Use pyridostigmine and immunosuppressive agents to optimize strength and respiratory status Plasmapheresis or IVIG may help in pts with VC < 2L 22% of pts with pre-op respiratory insufficiency will require long-term mechanical ventialation
32 Pre-op Assessment Major risk is weakness of oropharyngeal/respiratory muscles, leading to aspiration, inability to cough and respiratory failure Anticholinesterases (pyridostigmine) should be discontinued around 8hrs prior to surgery If stopped to early- myasthenic crisis If overmedicated- cholinergic crisis
33 Treatment Stage I/II: Complete en bloc thymectomy, and removal of all surrounding fat with avoidance of phrenic n. or intrapleural spread Median sternotomy provides excellent exposure and access VATS- being done, long term follow up is needed to compare with open approaches
34 Treatment Difficult to establish a stage III before surgery Unilateral phrenic n. resection can be done Potentially operable stage III dz Induction chemotx- cisplatin based with response rates of %, and resectability rates bet 35-70% Post op radiation after stage III resection for local control Stage IVa: induction chemotx, assess resectability; if not resectable- chemoradiation; steroids and octreotride as 2 nd line

35 Thymoma Prognosis at 5 and 10 yrs Stage I : 95%, 85% Stage II: 80%, 75% Stage III: 40-60%, 20-30% Stage IV a: 0-40%
36 Thymic Carcinoma This tumor is a rare variant of thymic lesions and is histologically and biologically different from invasive or malignant thymoma; these are malignant at microscopic level Incidence: <1% of thymic malignancies, 5 year survival is 30-50% Thymic carcinomas tend to be very invasive and difficult to resect completely Even in the setting of complete resection, recurrence is common both locally and at distant sites Typically, these are young men (< age 50 years) with an otherwise excellent performance status
37 Thymic Carcinoma PET scan better due to higher proliferative potential in thymic carcinoma. Aggressive combined-modality approach (induction chemotherapy, resection, and postoperative chemoradiotherapy) should be employed While a good response to induction therapy and complete resection will provide a significant disease-free interval, long-term survival is still unlikely
38 Conclusion Goal of thymectomy should be complete removal of all thymic tissue MC indications: thymic neoplasm or MG Thymoma should be resected because of its risk for invasive spread or morbidity due to mass effects Even advanced tumors with local invasion of resectable structures such as the pericardium, superior vena cava, or innominate vessels should be considered for resection with reconstruction
39 Surgery is the cornerstone for thymic malignancies Complete resection is the most constant and significant prognostic factor for progression-free and overall survival Radiotherapy Although thymomas are regarded as being moderately radiosensitive, controversy exists about its role as adjuvant therapy Chemotherapy
40
41 Recommendations Stage I: Surgery to obtain microscopically complete resection Stage II-III (resectable): Surgery, post op RT controversial, but clearly recommended for incompletely resected tumors Increased Mediastinal recurrence-free survival from 0-79% vs 47% without adjuvant RT, No increase in overall survival
42 Recommendations Stage III-IV a (marginally resectable): Surgery and post-op radiation therapy, perioperative chemotherapy in incomplete resection (Level 2C evidence) Debulking surgery in debate, survival rates only 5-10% Stage III-IV a (initially unresectable) Upfront chemotherapy followed by surgery or radiation therapy depending on whether sufficient down-staging has been achieved. Stage IVB Chemotherapy is treatment of choice typically multiple agents.
43 Recommendations Local and Locoregional recurrences of thymoma Late recurrences 5-10 year are not uncommon In cases of recurrent thymoma, surgery remains the mainstay in therapy In nonresectable local recurrences, exclusive radiotherapy has been reported as an efficient treatment.
44 Key Points Tumors of the thymus represent a wide spectrum of diseases; Thymoma predominates Surgeon s role- knowledge of differential diagnoses, associated symptoms, palpable lymphadenopathy Pre-op management Surgery is the mainstay of therapy and obtaining complete resection is the most important prognostic factor Due to its rarity, further studies are warranted to evaluate and improve current therepeutic standards.
45 References Alavi A, Gupta N, Alberini JLPositron emission tomography imaging in nonmalignant thoracic disorders. Sem Nucl Med 2002; 22:293.and others Kelemen 3rd JJ, Naunheim KS: Minimally invasive approaches to mediastinal neoplasms. Sem Thorac Cardiovasc Surg 2000; 12:301. Kim ES, Putnam JB, Komaki R: Phase II study of a multidisciplinary approach with induction chemotherapy, followed by surgical resection, radiation therapy, and consolidation chemotherapy for unresectable malignant thymomas. Lung Cancer 2004; 44:369.and others Wright CD, Kessler KA: Surgical treatment of thymic tumors. Sem Thorac Cardiovasc Surg 2005; 17:20.
46
Thymic Tumors. Feiran Lou MD. MS. Kings County Hospital Department of Surgery
 Thymic Tumors Feiran Lou MD. MS. Kings County Hospital Department of Surgery Case HPI 53 yo man referred from OSH for anterior mediastinal mass. Initially presented with leg weakness and back pain for
Thymic Tumors Feiran Lou MD. MS. Kings County Hospital Department of Surgery Case HPI 53 yo man referred from OSH for anterior mediastinal mass. Initially presented with leg weakness and back pain for
Karoline Nowillo, MD. February 1, 2008
 Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
Michael C. Smith, M.D. August 25, 2016
 Michael C. Smith, M.D. August 25, 2016 23 year old female PMH: Obesity, Myasthenia Gravis PSH: Tracheostomy x 2 All: NKDA Meds: Pyridostigmine, Prednisone Taken to OR for VATS/Thymectomy Supine Position
Michael C. Smith, M.D. August 25, 2016 23 year old female PMH: Obesity, Myasthenia Gravis PSH: Tracheostomy x 2 All: NKDA Meds: Pyridostigmine, Prednisone Taken to OR for VATS/Thymectomy Supine Position
Myasthenia: Is Medical Therapy in the Grave? Katy Marino, PGY-5
 Myasthenia: Is Medical Therapy in the Grave? Katy Marino, PGY-5 Disclosures Outline History of Thymus Anatomy of Thymus Pathophysiology of Myasthenia Gravis Medical Management of Myasthenia Gravis Surgical
Myasthenia: Is Medical Therapy in the Grave? Katy Marino, PGY-5 Disclosures Outline History of Thymus Anatomy of Thymus Pathophysiology of Myasthenia Gravis Medical Management of Myasthenia Gravis Surgical
Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI
 XXI CONGRESSO NAZIONALE AIRO Genova, 19-22 novembre 2011 Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI PIERA NAVARRIA Unità Operativa di Radioterapia e Radiochirurgia Humanitas Cancer
XXI CONGRESSO NAZIONALE AIRO Genova, 19-22 novembre 2011 Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI PIERA NAVARRIA Unità Operativa di Radioterapia e Radiochirurgia Humanitas Cancer
Insights into Thymic Epithelial Tumors: Radiation Therapy
 Insights into Thymic Epithelial Tumors: Radiation Therapy Charles R. Thomas, MD Professor and Chairman, Department of Radiation Medicine Professor, Department of Medicine, Division of Hematology/Medical
Insights into Thymic Epithelial Tumors: Radiation Therapy Charles R. Thomas, MD Professor and Chairman, Department of Radiation Medicine Professor, Department of Medicine, Division of Hematology/Medical
ARRO Case Thymoma. Jordan Kharofa, MD Elizabeth Gore, MD Medical College of Wisconsin
 ARRO Case Thymoma Jordan Kharofa, MD Elizabeth Gore, MD Medical College of Wisconsin History HPI 54 yo male who presented to PCP with complaining subacute shortness of breath and chest pain. Pain increased
ARRO Case Thymoma Jordan Kharofa, MD Elizabeth Gore, MD Medical College of Wisconsin History HPI 54 yo male who presented to PCP with complaining subacute shortness of breath and chest pain. Pain increased
Standardized definitions and policies of minimally invasive thymoma resection
 Perspective Standardized definitions and policies of minimally invasive thymoma resection Alper Toker 1,2 1 Department of Thoracic Surgery, Istanbul Medical School, Istanbul University, Istanbul, Turkey;
Perspective Standardized definitions and policies of minimally invasive thymoma resection Alper Toker 1,2 1 Department of Thoracic Surgery, Istanbul Medical School, Istanbul University, Istanbul, Turkey;
DESCRIPTION: This is the part of the trunk, which is located between the root of the neck and the superior border of the abdominal region.
 1 THE THORACIC REGION DESCRIPTION: This is the part of the trunk, which is located between the root of the neck and the superior border of the abdominal region. SHAPE : T It has the shape of a truncated
1 THE THORACIC REGION DESCRIPTION: This is the part of the trunk, which is located between the root of the neck and the superior border of the abdominal region. SHAPE : T It has the shape of a truncated
Protocol for the Examination of Specimens From Patients With Thymic Tumors
 Protocol for the Examination of Specimens From Patients With Thymic Tumors Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Protocol for the Examination of Specimens From Patients With Thymic Tumors Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Sectional Anatomy Quiz II
 Sectional Anatomy II Rashid Hashmi Rural Clinical School, University of New South Wales, Wagga Wagga, New South Wales, Australia A R T I C L E I N F O Article type: Article history: Received: 3 Aug 2017
Sectional Anatomy II Rashid Hashmi Rural Clinical School, University of New South Wales, Wagga Wagga, New South Wales, Australia A R T I C L E I N F O Article type: Article history: Received: 3 Aug 2017
Right sided VATS thymectomy: current standards of extended thymectomy for myasthenia gravis
 Review Article on Videothoracoscopic Surgery Page 1 of 5 Right sided VATS thymectomy: current standards of extended thymectomy for myasthenia gravis Erkan Kaba 1, Tugba Cosgun 1, Kemal Ayalp 2, Mazen Rasmi
Review Article on Videothoracoscopic Surgery Page 1 of 5 Right sided VATS thymectomy: current standards of extended thymectomy for myasthenia gravis Erkan Kaba 1, Tugba Cosgun 1, Kemal Ayalp 2, Mazen Rasmi
Pathology of Mediastinal Tumors
 SAMO Meeting Lucerne 2009 Pathology of Mediastinal Tumors Alex Soltermann Most common lesions (adults) Clinical presentation 50% of the patients are asymptomatic, lesion discovered incidentally Symptoms
SAMO Meeting Lucerne 2009 Pathology of Mediastinal Tumors Alex Soltermann Most common lesions (adults) Clinical presentation 50% of the patients are asymptomatic, lesion discovered incidentally Symptoms
10/14/2018 Dr. Shatarat
 2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013
 Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
Anterior Mediastinal Masses: The 4 T s
 May 2001 Anterior Mediastinal Masses: The 4 T s Rachel Van Sambeek, Harvard Medical School, Year III 1 Mediastinal Compartments 3 arbitrary divisions that do not correlate with anatomic planes: Anterior
May 2001 Anterior Mediastinal Masses: The 4 T s Rachel Van Sambeek, Harvard Medical School, Year III 1 Mediastinal Compartments 3 arbitrary divisions that do not correlate with anatomic planes: Anterior
Role of Surgery in Management of Non Small Cell Lung Cancer. Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City
 Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Mediastinum and pericardium
 Mediastinum and pericardium Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The mediastinum: is the central compartment of the thoracic cavity surrounded by
Mediastinum and pericardium Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The mediastinum: is the central compartment of the thoracic cavity surrounded by
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Mediastinal Tumors: Imaging
 Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
Dr. Weyrich G07: Superior and Posterior Mediastina. Reading: 1. Gray s Anatomy for Students, chapter 3
 Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Basic Data. Sex:Male 31 years old Occupation: 搬家工人
 Basic Data Sex:Male 31 years old Occupation: 搬家工人 Chief Complaint Intermittent chest pain with shortness of breath for 2-3 months. Present Illness 4 months ago, he started having occasional chest pain
Basic Data Sex:Male 31 years old Occupation: 搬家工人 Chief Complaint Intermittent chest pain with shortness of breath for 2-3 months. Present Illness 4 months ago, he started having occasional chest pain
Identify the lines used in anatomical surface descriptions of the thorax. median line mid-axillary line mid-clavicular line
 L 14 A B O R A T O R Y Thorax THORACIC WALL Identify the lines used in anatomical surface descriptions of the thorax. median line mid-axillary line mid-clavicular line Identify the surface landmarks of
L 14 A B O R A T O R Y Thorax THORACIC WALL Identify the lines used in anatomical surface descriptions of the thorax. median line mid-axillary line mid-clavicular line Identify the surface landmarks of
Sectional Anatomy Quiz - III
 Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
Standard Definitions and Polices. Institutional Kit of Specialty-Specific Summary Sheets
 Standard Definitions and Polices Institutional Kit of Specialty-Specific Summary Sheets Introduction to Institutional Summary Kits of ITMIG Standard Definitions and Policies Thymic malignancies are relatively
Standard Definitions and Polices Institutional Kit of Specialty-Specific Summary Sheets Introduction to Institutional Summary Kits of ITMIG Standard Definitions and Policies Thymic malignancies are relatively
Educational Objectives. Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach.
 Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
CT Chest. Verification of an opacity seen on the straight chest X ray
 CT Chest Indications: To assess equivocal plain x-ray findings Staging of lung neoplasm Merastatic workup of extra thoraces malignancies Diagnosis of diffuse lung diseases with HRCT Assessment of bronchietasis
CT Chest Indications: To assess equivocal plain x-ray findings Staging of lung neoplasm Merastatic workup of extra thoraces malignancies Diagnosis of diffuse lung diseases with HRCT Assessment of bronchietasis
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Mediastinum It is a thick movable partition between the two pleural sacs & lungs. It contains all the structures which lie
 Dr Jamila EL medany OBJECTIVES At the end of the lecture, students should be able to: Define the Mediastinum. Differentiate between the divisions of the mediastinum. List the boundaries and contents of
Dr Jamila EL medany OBJECTIVES At the end of the lecture, students should be able to: Define the Mediastinum. Differentiate between the divisions of the mediastinum. List the boundaries and contents of
Right lung. -fissures:
 -Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
-Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Principles and Practice of Radiation Oncology. 4 th edition. Chapter 45. Mediastinum and Trachea
 Principles and Practice of Radiation Oncology 4 th edition Chapter 45 Mediastinum and Trachea Tony Y. Eng 1, Todd J. Scarbrough 2, Charles R. Thomas, Jr. 3 1 Associate Professor 3 Associate Professor and
Principles and Practice of Radiation Oncology 4 th edition Chapter 45 Mediastinum and Trachea Tony Y. Eng 1, Todd J. Scarbrough 2, Charles R. Thomas, Jr. 3 1 Associate Professor 3 Associate Professor and
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
Surgical Treatment of Complex Malignant Anterior Mediastinal Tumors Invading the Superior Vena Cava
 Ó 2006 by the Société Internationale de Chirurgie World J Surg (2006) 30: 162 170 Published Online: 20 January 2006 DOI: 10.1007/s00268-005-0009-x Surgical Treatment of Complex Malignant Anterior Mediastinal
Ó 2006 by the Société Internationale de Chirurgie World J Surg (2006) 30: 162 170 Published Online: 20 January 2006 DOI: 10.1007/s00268-005-0009-x Surgical Treatment of Complex Malignant Anterior Mediastinal
Thymic epithelial tumours: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up
 26 (Supplement 5): v40 v55, 2015 doi:10.1093/annonc/mdv277 Thymic epithelial tumours: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up N. Girard 1, E. Ruffini 2, A. Marx 3, C. Faivre-Finn
26 (Supplement 5): v40 v55, 2015 doi:10.1093/annonc/mdv277 Thymic epithelial tumours: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up N. Girard 1, E. Ruffini 2, A. Marx 3, C. Faivre-Finn
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Mediastinoscopy, Mediastinotomy And Thoracoscopy For Mediastinal Lesions. Alper Toker, MD
 Mediastinoscopy, Mediastinotomy And Thoracoscopy For Mediastinal Lesions Alper Toker, MD Istanbul University, Istanbul Medical School Department of Thoracic Surgery The mediastinum is a complex anatomic
Mediastinoscopy, Mediastinotomy And Thoracoscopy For Mediastinal Lesions Alper Toker, MD Istanbul University, Istanbul Medical School Department of Thoracic Surgery The mediastinum is a complex anatomic
The anterior mediastinum represents the second most
 Technique of Mediastinal Germ Cell Tumor Resection Kenneth A. Kesler, MD The anterior mediastinum represents the second most common site of germ cell tumor origin. Nonseminomatous germ cell cancers not
Technique of Mediastinal Germ Cell Tumor Resection Kenneth A. Kesler, MD The anterior mediastinum represents the second most common site of germ cell tumor origin. Nonseminomatous germ cell cancers not
T with myasthenia gravis (MG) [l-31. Thymothymectomy
 [l-31. Thymothymectomy") Recurrent Thymoma in Patients With Myasthenia Gravis Mikio Ohmi, MD, and Masahiro Ohuchi, MD Division of Thoracic and Cardiovascular Surgery, Sendai National Hospital, Sendai, Japan One hundred sixty-six
Recurrent Thymoma in Patients With Myasthenia Gravis Mikio Ohmi, MD, and Masahiro Ohuchi, MD Division of Thoracic and Cardiovascular Surgery, Sendai National Hospital, Sendai, Japan One hundred sixty-six
Anatomy Lecture 8. In the previous lecture we talked about the lungs, and their surface anatomy:
 Anatomy Lecture 8 In the previous lecture we talked about the lungs, and their surface anatomy: 1-Apex:it lies 1 inch above the medial third of clavicle. 2-Anterior border: it starts from apex to the midpoint
Anatomy Lecture 8 In the previous lecture we talked about the lungs, and their surface anatomy: 1-Apex:it lies 1 inch above the medial third of clavicle. 2-Anterior border: it starts from apex to the midpoint
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Chapter 5: Other mediastinal structures. The Large Arteries. The Aorta. Ascending aorta
 Chapter 5: Other mediastinal structures The Large Arteries The Aorta The aorta is the main arterial trunk of the systemic circulation and in the healthy state its wall contain a large amount of yellow
Chapter 5: Other mediastinal structures The Large Arteries The Aorta The aorta is the main arterial trunk of the systemic circulation and in the healthy state its wall contain a large amount of yellow
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
In the 1960s, thymomas were classified into two categories: Staging System of Thymoma MALIGNANCIES OF THE THYMUS. Akira Masaoka, MD, PhD S304
 MALIGNANCIES OF THE THYMUS Akira Masaoka, MD, PhD Introduction: Thirty years have gone by since the Masaoka staging system of thymoma was proposed in 1981. Although the Masaoka staging system has been
MALIGNANCIES OF THE THYMUS Akira Masaoka, MD, PhD Introduction: Thirty years have gone by since the Masaoka staging system of thymoma was proposed in 1981. Although the Masaoka staging system has been
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
MEDIASTINAL STAGING surgical pro
 MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI
 EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI Overview Introduction Diagnostic work up Treatment Group 1 Group 2 Group 3 Stage III lung cancer Historically was defined as locoregionally advanced
EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI Overview Introduction Diagnostic work up Treatment Group 1 Group 2 Group 3 Stage III lung cancer Historically was defined as locoregionally advanced
TNM classifications have been established for various
 Lymphogenous and Hematogenous Metastasis of Thymic Epithelial Tumors Kazuya Kondo, MD, PhD, and Yasumasa Monden, MD, PhD Department of Oncological and Regenerative Surgery, School of Medicine, University
Lymphogenous and Hematogenous Metastasis of Thymic Epithelial Tumors Kazuya Kondo, MD, PhD, and Yasumasa Monden, MD, PhD Department of Oncological and Regenerative Surgery, School of Medicine, University
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
THE DESCENDING THORACIC AORTA
 Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
Congenital Neck Masses C. Stefan Kénel-Pierre, MD
 Congenital Neck Masses C. Stefan Kénel-Pierre, MD SUNY-LICH Medical Center Department of Surgery Case Presentation xx year old male presents with sudden onset left lower neck swelling x 1 week Denies pain,
Congenital Neck Masses C. Stefan Kénel-Pierre, MD SUNY-LICH Medical Center Department of Surgery Case Presentation xx year old male presents with sudden onset left lower neck swelling x 1 week Denies pain,
LA TIMECTOMIA ROBOTICA
 LA TIMECTOMIA ROBOTICA Prof. Giuseppe Marulli UOC Chirurgia Toracica Università di Padova . The thymus presents a challenge to the surgeon not only as a structure that may be origin of benign and malignant
LA TIMECTOMIA ROBOTICA Prof. Giuseppe Marulli UOC Chirurgia Toracica Università di Padova . The thymus presents a challenge to the surgeon not only as a structure that may be origin of benign and malignant
Video-Mediastinoscopy Thoracoscopy (VATS)
") Surgical techniques Video-Mediastinoscopy Thoracoscopy (VATS) Gunda Leschber Department of Thoracic Surgery ELK Berlin Chest Hospital, Berlin, Germany Teaching Hospital of Charité Universitätsmedizin Berlin
Surgical techniques Video-Mediastinoscopy Thoracoscopy (VATS) Gunda Leschber Department of Thoracic Surgery ELK Berlin Chest Hospital, Berlin, Germany Teaching Hospital of Charité Universitätsmedizin Berlin
AMSER Case of the Month: January Mediastinal Mass
 AMSER Case of the Month: January 2019 Mediastinal Mass Paige Tannhauser, MS-4, Drexel University College of Medicine Dr. Matthew Hartman MD, Allegheny Health Network Dr. Jeffrey Mueller MD, Allegheny Health
AMSER Case of the Month: January 2019 Mediastinal Mass Paige Tannhauser, MS-4, Drexel University College of Medicine Dr. Matthew Hartman MD, Allegheny Health Network Dr. Jeffrey Mueller MD, Allegheny Health
Radiology- Pathology Conference 4/29/2012. Lymph Nodes. John McGrath
 Radiology- Pathology Conference 4/29/2012 Lymph Nodes John McGrath 1 Presentation material is for education purposes only. All rights reserved. 2012 URMC Radiology Page 1 of 24 Case 1: 51 year-old male
Radiology- Pathology Conference 4/29/2012 Lymph Nodes John McGrath 1 Presentation material is for education purposes only. All rights reserved. 2012 URMC Radiology Page 1 of 24 Case 1: 51 year-old male
The Itracacies of Staging Patients with Suspected Lung Cancer
 The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Thoracic wall including the diaphragm. Prof Oluwadiya KS
 The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
Case Report Two Invasive Thymomas Incidentally Found during Coronary Artery Bypass Graft Surgery
 Case Reports in Pathology Volume 2016, Article ID 1516521, 4 pages http://dx.doi.org/10.1155/2016/1516521 Case Report Two Invasive Thymomas Incidentally Found during Coronary Artery Bypass Graft Surgery
Case Reports in Pathology Volume 2016, Article ID 1516521, 4 pages http://dx.doi.org/10.1155/2016/1516521 Case Report Two Invasive Thymomas Incidentally Found during Coronary Artery Bypass Graft Surgery
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Lung & Pleura. The Topics :
 Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
Large veins of the thorax Brachiocephalic veins
 Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Leukaemia 35% Lymphoma 14%
 Distribution ib ti of Cancers in Children under 15 years Leukaemia 35% Lymphoma 14% Neuroblastoma 9% Other 5% Liver 1% Retinoblastoma 3% Bone and STS 15% CNS 20% Wilms' 8% 30-40% Mortality Germ Cell Tumours
Distribution ib ti of Cancers in Children under 15 years Leukaemia 35% Lymphoma 14% Neuroblastoma 9% Other 5% Liver 1% Retinoblastoma 3% Bone and STS 15% CNS 20% Wilms' 8% 30-40% Mortality Germ Cell Tumours
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
Revisit of Primary Malignant Neoplasms of the Trachea: Clinical Characteristics and Survival Analysis
 Jpn J Clin Oncol 1997;27(5)305 309 Revisit of Primary Malignant Neoplasms of the Trachea: Clinical Characteristics and Survival Analysis -, -, - - 1 Chest Department and 2 Section of Thoracic Surgery,
Jpn J Clin Oncol 1997;27(5)305 309 Revisit of Primary Malignant Neoplasms of the Trachea: Clinical Characteristics and Survival Analysis -, -, - - 1 Chest Department and 2 Section of Thoracic Surgery,
UCLA General Surgery Residency Program Rotation Educational Policy Goals and Objectives
 UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Surgical anatomy of thyroid and parathyroid glands
 Head & Neck Surgery Course Surgical anatomy of thyroid and parathyroid glands Dr Pierfrancesco PELLICCIA Pr Benjamin LALLEMANT Service ORL et CMF CHU de Nîmes CH de Arles Thyroid glands Dr Pierfrancesco
Head & Neck Surgery Course Surgical anatomy of thyroid and parathyroid glands Dr Pierfrancesco PELLICCIA Pr Benjamin LALLEMANT Service ORL et CMF CHU de Nîmes CH de Arles Thyroid glands Dr Pierfrancesco
Myasthenia Gravis. Mike Gilchrist 10/30/06
 Myasthenia Gravis Mike Gilchrist 10/30/06 Overview Background Pathogenesis Clinical Manifestations Diagnosis Treatment Associated Conditions Background Severe muscle disease Most common disorder of neuromuscular
Myasthenia Gravis Mike Gilchrist 10/30/06 Overview Background Pathogenesis Clinical Manifestations Diagnosis Treatment Associated Conditions Background Severe muscle disease Most common disorder of neuromuscular
slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments
 Done By : Rahmeh Alsukkar Date : 26 /10/2017 slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments Each segmental bronchus passes to a structurally
Done By : Rahmeh Alsukkar Date : 26 /10/2017 slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments Each segmental bronchus passes to a structurally
11/21/ M with LUL Mass Case Presentation / Round Table Discussion. Multiple-choice question What stage is this tumor?
 MS 62M with LUL Mass Case Presentation / Round Table Discussion Dr. Jasleen Kukreja and Johannes Kratz Department of Thoracic Surgery University of California, San Francisco 62M, presented to clinic 6/2009
MS 62M with LUL Mass Case Presentation / Round Table Discussion Dr. Jasleen Kukreja and Johannes Kratz Department of Thoracic Surgery University of California, San Francisco 62M, presented to clinic 6/2009
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Case Presentation. PMH: HTN, BPH, strabismus PSH: appendectomy Medications: norvasc, tamsulosin NKDA SH/FH: negative
 Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Clinical Usefulness of the WHO Histological Classification of Thymoma
 Original Article Clinical Usefulness of the WHO Histological Classification of Thymoma Satoshi Sonobe, MD, 1 Hideaki Miyamoto, MD, 1 Hiroshi Izumi, MD, 2 Bunsei Nobukawa, MD, 2 Toshiro Futagawa, MD, 1
Original Article Clinical Usefulness of the WHO Histological Classification of Thymoma Satoshi Sonobe, MD, 1 Hideaki Miyamoto, MD, 1 Hiroshi Izumi, MD, 2 Bunsei Nobukawa, MD, 2 Toshiro Futagawa, MD, 1
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Case presentation. Paul De Leyn, MD, PhD Thoracic Surgery University Hospitals Leuven Belgium
 Case presentation Paul De Leyn, MD, PhD Thoracic Surgery University Hospitals Leuven Belgium Perspectives in Lung Cancer Brussels 6-7 march 2009 LEUVEN LUNG CANCER GROUP Department of Thoracic Surgery
Case presentation Paul De Leyn, MD, PhD Thoracic Surgery University Hospitals Leuven Belgium Perspectives in Lung Cancer Brussels 6-7 march 2009 LEUVEN LUNG CANCER GROUP Department of Thoracic Surgery
D pects of the pathophysiology and treatment of thymomas
 CURRENT REVIEW Thymoma: Results of 241 Operated Cases Giuliano Maggi, MD, Caterina Casadio, MD, Antonio Cavallo, MD, Roberto Cianci, MD, Massimo Molinatti, MD, and Enrico Ruffini, MD Department of Thoracic
CURRENT REVIEW Thymoma: Results of 241 Operated Cases Giuliano Maggi, MD, Caterina Casadio, MD, Antonio Cavallo, MD, Roberto Cianci, MD, Massimo Molinatti, MD, and Enrico Ruffini, MD Department of Thoracic
Primary mediastinal tumours
 Primary mediastinal tumours Thorax (1974), 29, 475. YOUSF D. AL-NAAMAN, MOHAMAD S. AL-AN, and MUAYYAD M. AL-OMER Department of Thoracic and Cardiovascular Surgery, College of Medicine, University of Baghdad,
Primary mediastinal tumours Thorax (1974), 29, 475. YOUSF D. AL-NAAMAN, MOHAMAD S. AL-AN, and MUAYYAD M. AL-OMER Department of Thoracic and Cardiovascular Surgery, College of Medicine, University of Baghdad,
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
Video-assisted thoracoscopic microthymectomy
 Art of Operative Techniques Video-assisted thoracoscopic microthymectomy Joel Dunning Department of Thoracic Surgery, James Cook University Hospital, Middlesbrough, UK Correspondence to: Joel Dunning,
Art of Operative Techniques Video-assisted thoracoscopic microthymectomy Joel Dunning Department of Thoracic Surgery, James Cook University Hospital, Middlesbrough, UK Correspondence to: Joel Dunning,
Dana Alrafaiah. - Moayyad Al-Shafei. -Mohammad H. Al-Mohtaseb. 1 P a g e
 - 6 - Dana Alrafaiah - Moayyad Al-Shafei -Mohammad H. Al-Mohtaseb 1 P a g e Quick recap: Both lungs have an apex, base, mediastinal and costal surfaces, anterior and posterior borders. The right lung,
- 6 - Dana Alrafaiah - Moayyad Al-Shafei -Mohammad H. Al-Mohtaseb 1 P a g e Quick recap: Both lungs have an apex, base, mediastinal and costal surfaces, anterior and posterior borders. The right lung,
Tumors of the Thvmus and Thee
 Tumors of the Thvmus Thee Region: 111. Clinic&pathological Skdies on Teratornas Tumors of Germ Cell Type N. P. Bergh, M.D., P. Gatzinsky, M.D., S. Larsson, M.D., P. Lundin, M.D., B. Ridell, M.D. ABSTRACT
Tumors of the Thvmus Thee Region: 111. Clinic&pathological Skdies on Teratornas Tumors of Germ Cell Type N. P. Bergh, M.D., P. Gatzinsky, M.D., S. Larsson, M.D., P. Lundin, M.D., B. Ridell, M.D. ABSTRACT
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Resection of Thymic Carcinoma in a Patient with Thoracic Aortic Aneurysm
 Case Report Resection of Thymic Carcinoma in a Patient with Thoracic Aortic Aneurysm Makoto Nonaka, MD, 1 Mitsutaka Kadokura, MD, 1 Shigeru Yamamoto, MD, 1 Daisuke Kataoka, MD, 1 Atsushi Bito, MD, 1 Mitsuru
Case Report Resection of Thymic Carcinoma in a Patient with Thoracic Aortic Aneurysm Makoto Nonaka, MD, 1 Mitsutaka Kadokura, MD, 1 Shigeru Yamamoto, MD, 1 Daisuke Kataoka, MD, 1 Atsushi Bito, MD, 1 Mitsuru
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Superior and Posterior Mediastinum. Assoc. Prof. Jenny Hayes
 Superior and Posterior Mediastinum Assoc. Prof. Jenny Hayes WARNING This material has been provided to you pursuant to section 49 of the Copyright Act 1968 (the Act) for the purposes of research or study.
Superior and Posterior Mediastinum Assoc. Prof. Jenny Hayes WARNING This material has been provided to you pursuant to section 49 of the Copyright Act 1968 (the Act) for the purposes of research or study.
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
PLEURAE and PLEURAL RECESSES
 PLEURAE and PLEURAL RECESSES By Dr Farooq Aman Ullah Khan PMC 26 th April 2018 Introduction When sectioned transversely, it is apparent that the thoracic cavity is kidney shaped: a transversely ovoid space
PLEURAE and PLEURAL RECESSES By Dr Farooq Aman Ullah Khan PMC 26 th April 2018 Introduction When sectioned transversely, it is apparent that the thoracic cavity is kidney shaped: a transversely ovoid space
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment