Thyroid Nodule. N. Rojanapithayakorn P. Prasarttong-Osoth
|
|
|
- Randolph Curtis
- 5 years ago
- Views:
Transcription

1 Thyroid Nodule N. Rojanapithayakorn P. Prasarttong-Osoth

2 A Brief History of the Thyroid



3 A Brief History of the Thyroid Fabricius Wharton Von Haller


4 A Brief History of the Thyroid Kendall Enrico Fermi



5 A Brief History of the Thyroid Hiroshima,1945 Chernobyl,1986

6 History of Thyroid Surgery


7 History of Thyroid Surgery Billroth


8 History of Thyroid Surgery Kocher
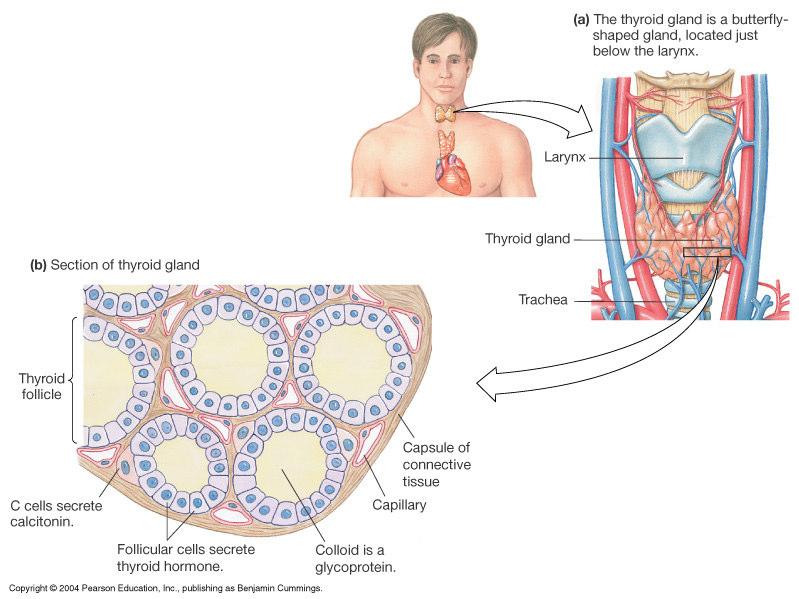
9 Embryology
10 Anatomy
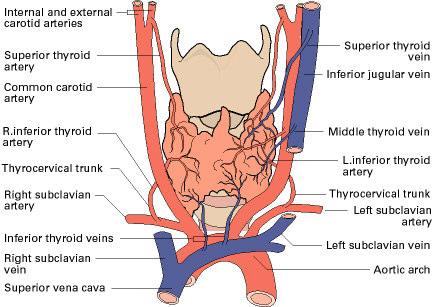
11 Anatomy


12 Superior laryngeal N. Recurrent laryngeal N.

13 Anatomy Lymphatic drainage Level 6 Level 4,3 Level 5
14 Histology
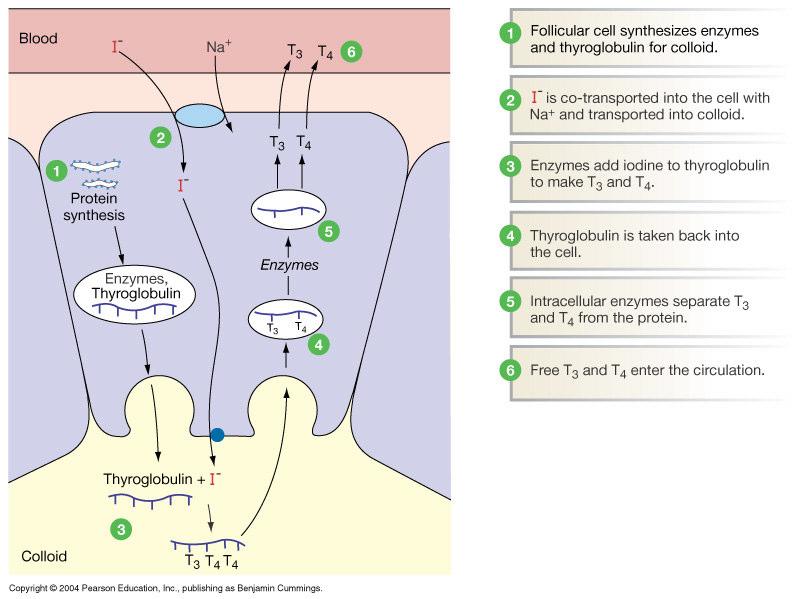
15 Physiology
16 Physiology
17 Thyroid hormone T4-80 ug/d d produced by the thyroid gland T ug/d;80% by peripheral conversion T % bound & T399.0% albumin & pre-albumin Half-life: T4 5-7 days T3 1 day 99.0% bound to TBG,
18 Epidemiology Nodule Framingham study : ages Women 6.4 % Men 1.5 % Mayo study : autopsy series ( no thyroid hx ) 21% had 1 nodules by direct palpation Overall, fewer than 5% of nodules are malignant
19 Benign Thyroid Nodules Colloid nodule Cyst Simple cyst Mixed cystic-solid Thyroid adenoma Non functional or hypofunctional Autonomous Thyroiditis Infection Granulomatous disease Abscess Developmental Unilateral lobe agenesis Cystic hygroma Dermoid
20 Colloid nodules Enlarged follicles containing abundant colloid and benign follicular cells Circumscribed, no fibrous capsule Related to iodine deficiency Endemic area : more than 10 % of children aged 6-12
21 Thyroid Cysts % of all thyroid nodules Simple cysts, hemorrhagic colloid nodules, or cystic parathyroid tumors 30 % are hemorrhagic adenomas 15 % are necrotic papillary cancers Often yield insufficient numbers of cells for Dx
22 Follicular Adenomas Monoclonal tumors arising from follicular epithelium Single lesions with well-developed fibrous capsules Uniform histologic structure distinct from the normal surrounding thyroid
23 Follicular Adenomas Histologic classification Normofollicular (simple) Macrofollicular Microfollicular (fetal) Trabecular and solid (embryonal) Oxyphilic cell type (Hürtle cell)
24 Multinodular goiter Most often caused by iodine deficiency More autonomous with increasing age Should focus on the dominant nodule or nodules that have a different consistency
25 Toxic nodular goiter (Plummer s s disease) Toxic adenoma / Toxic multinodular goiter Autonomously functioning thyroid nodule hypersecreting T3 and T4 Almost never malignant
26 Hashimoto s Thyroiditis Females yrs. Painless diffuse goiter Lab studies Hypothyroidism Anti TPO antibodies (90%) Anti Thyroglobulin antibodies (20-50%) Acute Hyperthyroidism (5%)
27 Subacute Thyroiditis (De Quervain's thyroiditis) Most common cause of painful thyroiditis Often follows a URI FNA : granulomatous change Course Pain and thyrotoxicosis (3-6 6 weeks) Asymptomatic euthyroidism Hypothyroid period (weeks to months) Recovery (complete in 95% after months)
28 Malignant Thyroid Nodules Well-Differentiated Thyroid Carcinomas Papillary carcinoma Follicular variant Tall cell Diffuse sclerosing Encapsulated Follicular carcinoma Overtly invasive Minimally invasive Hurthle cell carcinoma Anaplastic carcinoma Giant cell Small cell Medullary Carcinoma Miscellaneous Sarcoma Lymphoma Squamous cell carcinoma Mucoepidermoid carcinoma Clear cell tumors Pasma cell tumors Metastatic
29 Papillary Carcinoma 60-80% of all thyroid malignancies Mean age of 35 years 80% survive at 10 years Lymph node involvement is common Major route of metastasis is lymphatic 46%-90% of patients have lymph node involvement
30 Papillary Carcinoma Pathology Gross often multi-focal unencapsulated Histology Follicular variant/tall cell/columnar cell/diffuse sclerosing/encapsulated Psammoma bodies Orphan Annie cells
31 Follicular Carcinoma 20% of all thyroid malignancies Mean age of 39 years 60% survive to 10 years Metastasis : angioinvasion and hematogenous 15% - distant metastases to bone and lung Lymphatic involvement is seen in 13%
32 Follicular Carcinoma Pathology Gross - encapsulated, solitary Histology very well-differentiated vascular and capsular invasion FNA and frozen section cannot accurately distinquish between benign and malignant
33 Hurthle Cell Carcinoma Variant of follicular carcinoma 4-10% of all thyroid malignancies Lymphatic spread seen in 30% of patients Distant metastases to bone and lung is seen in 15% at the time of presentation
34 Hurthle Cell Carcinoma Pathology large, polygonal, eosinophilic follicular cells abundant granular cytoplasm and numerous mitochondria vascular and capsular invasion
35 Medullary Thyroid Carcinoma 10% of all thyroid malignancies Arises from the parafollicular cell or C-cells ( from neural crest cells of the branchial arches ) secrete calcitonin RET proto-oncogene oncogene (chromosome 10)
36 Medullary Thyroid Carcinoma Developes in 4 clinical settings: Sporadic MTC Familial MTC MEN IIa MEN IIb AD
37
38 Anaplastic Carcinoma 1-10% 10% of all thyroid malignancies Mean age of 60 years Highly lethal Median survival <8 months 53% have previous benign thyroid disease 47% have previous history of WDTC
39 Anaplastic Carcinoma Pathology Classified as large cell or small cell Large cell is more common and has a worse prognosis Histology - sheets of very poorly differentiated cells

40 Thyroid Mets Breast Lung Renal GI Melanoma
41 Evaluation
42 History Age & Gender 4x more prevalent in women than in men among pts with nodules, rate of carcinoma 2x as high in men as in women (8% vs. 4%) higher rate of cancer in extreme age group ( < 20, > 60 yrs )
43 History Hyper- / Hypo- thyroidism Rapid change in size With pain may indicate hemorrhage into nodule Without pain may be bad sign
44 History Exposure to Radiation childhood : large thymus, acne, enlarged tonsils, cervical adenitis, sinusitis, malignancies 30%-50% chance to be malignant Mostly papillary carcinoma
45 Family history Medullary Thyroid Carcinoma Gardner Syndrome (familial adenomatous polyposis) Cowden Syndrome Mucocutaneous hamartomas, keratoses,fibrocystic breast changes & GI polyps Other thyroid carcinoma
46 History History suggestive of malignancy: Age < 20 or > 60 years Male sex Exposure to ionizing radiation Familly history of thyroid cancer Progressive enlargement Hoarseness Dysphagia, Dyspnea
47 Physical Examination Sign of hyperthyroidism Multinodular vs. Solitary nodule multinodular 4.7% chance of malignancy solitary nodule 4.1% chance of malignancy Indirect or fiberoptic laryngoscopy Cervical lymphadenopathy Pemberton s sign
48 Physical Examination Physical findings suggestive of malignancy: Cervical lymphadenopathy Vocal cord paralysis Very firm nodule Rapid tumor growth Fixation to adjacent structures
49 Investigation
50 Serum Testing TSH first-line serum test Identifies subclinical thyrotoxicosis T4, T3 Thyroglobulin Post-treatment treatment good to detect recurrence Calcitonin only in cases of medullary Antibodies Hashimoto s RET proto-oncogene oncogene

51 Plain Films
52 Ultrasonography Thyroid vs. non-thyroid Solitary nodule vs. multinodular goiter Cystic vs. solid Localization for FNA or injection Serial exam of nodule size LN enlargement and calcifications Noninvasive and inexpensive
53 Ultrasonography Findings suggestive of malignancy: Presence of halo Irregular border Presence of cystic components Presence of calcifications Heterogeneous echo pattern Extrathyroidal extension No findings are definitive
54 Ultrasonography When to use Ultrasonography..? Evaluation of a thyroid nodule: when a nodule is difficult to palpate or is deep- seated screening : familial thyroid cancer, childhood cervical irradiation Long term follow-up
55 Technetium 99m Thyroid scan cost-effective, readily available short half-life life trapped but not organified by the thyroid Radioactive iodine radioactive iodine (I-131, I-125, I I-123) I trapped and organified can determine functionality of a thyroid nodule
56 Thyroid scan When to use thyroid scanning..? Thyroid nodule with suppressed TSH Large MNG, esp. with substernal extension In search of ectopic thyroid tissue Immediately postop for localization of residual cancer or thyroid tissue Follow-up for tumor recurrence or metastasis



57 Thyroid scan Study : 4457 patients with nodules Cold 84% 15-25% cancer Warm 10% 9% cancer Hot 5.5% 1-44 % cancer
58 Other Imaging Modalities CT / MRI Evaluate local invasion Extension to substernal region Thyroid/non-thyroid nodule Recurrent or persistent thyroid tumor / scar Iodine contrast!
59 Fine-Needle Aspiration Biopsy Safe, efficacious, cost-effective Results comparable to large-needle biopsy, less complications Allow preop.. diagnosis and planning Sensitivity 70-98% Specificity %

60 Fine-Needle Aspiration Biopsy Technique: No gauge needle multiple passes ideally from periphery of lesion reaspirate after fluid drawn smeared and fixed in 95% alcohol
61 Fine-Needle Aspiration Biopsy Results Benign Malignant : papillary,medullary,anaplastic Suspicious/Indeterminate : follicular neoplasms, Hürthle cell neoplasms, papillary cancer, or lymphoma. Insufficient/Inadequate

 Epithelial cells in a")

62 (A) Benign epithelial cells, typical of a "colloid nodule". (B) Epithelial cells in a follicular arrangement (C) Epithelial cells in a pappilary formation from a papillary thyroid carcinoma. Nuclear grooves are also apparent.
63 Management
64
65 Management Benign Thyroid Nodule Thyroid suppressive therapy several reports - shrinkage of thyroid nodules clinically significant decrease in nodule volume in only 20% effect in larger nodules is probably smaller
66 Management Benign Thyroid Nodule Thyroid suppressive therapy Adverse Effects. decrease in bone density in postmenopausal women 3-fold increase in atrial fibrillation and increased mortality attributable to cardiovascular diseases
67 Management Benign Thyroid Nodule Thyroid suppressive therapy Should be avoided in patients with large thyroid nodules or long-standing goiters, TSH < 1µIU/mL postmenopausal women or men > 60 years patients with osteoporosis, cardiovascular disease, or systemic illnesses.
68 Management Benign Thyroid Nodule Surgical Indications. Compressive symptoms Suspicious malignancy Associated Hyperthyroidism. Cosmetic STN : Unilateral thyroid lobectomy MNG : Bilateral subtotal thyroidectomy
69 Management Benign Thyroid Nodule Radioiodine Therapy gradual decrease in thyroid volume radiation-induced thyroid dysfunction (hyperthyroidism in 5%, hypothyroidism in 20-30%) risk of induction of carcinoma alternative to surgery in elderly patients and those with cardiopulmonary disease
70 Management Benign Thyroid Nodule Percutaneous Ethanol Injection recurrent cystic nodules AFTN with a large fluid component before radioiodine treatment small AFTN with incomplete inhibition of the surrounding parenchyma should not be performed in solid, cold nodules, unless surgical treatment is contraindicated
71 Management Toxic nodular goiter overt hyperthyroidism:rx is always indicated subclinical hyperthyroidism : Rx in elderly patients and in younger ones who are at risk for cardiac disease or osteoporosis
72 Management Toxic nodular goiter Antithyroid-Drug Therapy hyperthyroidism is reversible, but always recurs after discontinued indicated before thyroid surgery before and sometimes after radioiodine treatment in elderly patients and those with other health problems
73 Management Toxic nodular goiter Surgery Uninodular : Lobectomy simple and effective recurrences after surgery are rare hypothyroidism develops in 10-20% recommended in children and adolescents; may be preferred in patients with large nodules
74 Management Toxic nodular goiter Surgery Multinodular :Bilateral subtotal thyroidectomy incidence of persistent and recurrent hyperthyroidism should be less than 10-20% widely varying rates of post-treatment hypothyroidism recommended in patients with large goiters
75 Management Toxic nodular goiter Radioiodine Therapy as effective as surgery more gradual than that after surgery hypothyroidism : less than 20% in most studies, in a large follow-up study, the risk of thyroid carcinoma was not increased attractive option for the majority of patients
76 Management Toxic nodular goiter Percutaneous Ethanol Injection alternative to radioiodine therapy and surgery for patients with uninodular goiter especially for patients with small nodules
77 Management Cystic Lesions Almost half such nodules disappear permanently after one or more aspirations Surgery : recurrence : usually >4 cm aspiration tends to yield bloody fluid but insufficient material for diagnosis Thyroxine therapy is ineffective
78 Management Hashimoto s Thyroiditis Thyroid suppression (levothyroxine( levothyroxine) Triiodothyronine (for myxedema coma) Surgery for compression or pain Subacute Thyroiditis NSAID s and salicylates. Oral steroids in severe cases Beta blockers for symptoms of hyperthyroidism
79 Management Suspicious Thyroid Nodule by FNA 20% are found to be malignant lesions Recommend surgical excision Lobectomy and isthmectomy Total thyroidectomy in : history of irradiation multiple thyroid nodules
80 Management Nondiagnostic Cytologic Specimen Usually results from a cystic nodule US-FNA directed is indicated 5% of thyroid nodules remain nondiagnostic. such nodules should be surgically excised
81 Management Indications for reaspiration Follow-up of benign nodule Enlarging nodule Recurrent cyst Thyroid nodule > 4 cm Initial nondiagnostic FNA biopsy No shrinkage of nodule after T4 therapy
82 Management Thyroid Nodules in Children Infections and developmental abnormalities are more common than in adults Incidence of cancer : 30% (14 61% ) FNA has not been used in very young children, surgery may be used to identify the cause
83 Management Thyroid incedentalomas Cancer < 5%, mostly papillary FNA in Familly history of thyroid cancer, childhood history of radiation U/S finding : size > 1.5 cm,hypoechoic, pattern, irregular margin,internal microcalcification
84 Management of thyroid cancer
85 Management Surgery is the definitive management of thyroid cancer, excluding most cases of ATC and lymphoma Types of operations: lobectomy with isthmectomy total thyroidectomy subtotal thyroidectomy
86 Management (WDTC) : Papillary and Follicular Lobectomy vs. Total thyroidectomy
87 Management (WDTC) : Papillary and Follicular Rationale for total thyroidectomy 30%-87.5% of PTC involve opposite lobe 7%-10% recurrence in the contralateral lobe Lower recurrence rates, some studies show increased survival Facilitates earlier detection & Rx for recurrent or metastatic carcinoma with iodine Potential to differentiate to ATC
88 Management (WDTC) : Papillary and Follicular Rationale for lobectomy Lower incidence of complications Hypoparathyroidism (1%-29%) Recurrent laryngeal nerve injury (1%-2%) Superior laryngeal nerve injury Long term prognosis is not improved by total thyroidectomy
89 Management (WDTC) : Papillary and Follicular Prognostic factors AMES (Lahey Clinic, Burlington, MA) AGES GAMES Grade (Mayo Clinic, Rochester, MN) (Memorial Sloan Kettering Cancer Center, NY) Age ( > 45 yrs ) Metastases of the tumor (other than Neck LN) Extent of primary tumor ( Extraglandular ) Size of tumor (> 4 cm)
90 Management (WDTC) : Papillary and Follicular Indications for total thyroidectomy Age < 15 y or > 45 yrs Radiation history Known distant metastases Bilateral nodularity Extrathyroidal extension Tumor > 4 cm in diameter Cervical lymph node metastases Aggressive variant
91 Management (WDTC) : Papillary and Follicular Managing lymphatic involvement If any cervical nodes are clinically palpable or identified by MR or CT imaging as being suspicious, a neck dissection should be done Elective neck dissections are not done
92 Management (WDTC) : Hurthle Cell Carcinoma Total thyroidectomy is recommended because: Lesions are often Multifocal They are more aggressive than WDTCs Most do not concentrate iodine
93 Management Medullary Carcinoma Recommended surgical management total thyroidectomy central lymph node dissection lateral jugular sampling Prophylactic thyroidectomy recommended age 2-62 If patient has MEN syndrome remove pheochromocytoma before thyroid surgery
94 Management Anaplastic Carcinoma Most have extensive extrathyroidal involvement at the time of diagnosis surgery is limited to biopsy and tracheostomy Radiotherapy and Chemotherapy

95 attention Thanks for your attention
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Evaluation and Management of Thyroid Nodules. Overview of Thyroid Nodules and Their Management. Thyroid Nodule detection: U/S versus Exam
 Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Goiter, Nodules and Tumors
 Goiter, Nodules and Tumors Howard J. Sachs, MD www.12daysinmarch.com Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Anaplastic Medullary MEN
Goiter, Nodules and Tumors Howard J. Sachs, MD www.12daysinmarch.com Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Anaplastic Medullary MEN
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
What you need to know about Thyroid Cancer
 What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
B Berry, J. 25 see also suspensory ligament of Berry biopsy see fine-needle aspiration biopsy (FNAB); open wedge biopsy
; open wedge biopsy") 174 Index Index Page numbers in italics refer to illustrations A abscess 80, 137 adenoma 61 parathyroid 18, 18 19, 62, 84 differential diagnosis 84, 84, 85, 85 thyroid 63 follicular 62, 63, 64 macrofollicular
174 Index Index Page numbers in italics refer to illustrations A abscess 80, 137 adenoma 61 parathyroid 18, 18 19, 62, 84 differential diagnosis 84, 84, 85, 85 thyroid 63 follicular 62, 63, 64 macrofollicular
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Chapter 14: Thyroid Cancer
 The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid Nodules. Hossein Gharib, MD, MACP, MACE
 Thyroid Nodules Hossein Gharib, MD, MACP, MACE Professor of Medicine Mayo Clinic College of Medicine President Elect, American College of Endocrinology University Course January 2008 CP1294362-1 Thyroid
Thyroid Nodules Hossein Gharib, MD, MACP, MACE Professor of Medicine Mayo Clinic College of Medicine President Elect, American College of Endocrinology University Course January 2008 CP1294362-1 Thyroid
PEDIATRIC THYROID MALIGNACY
 PEDIATRIC THYROID MALIGNACY Anthony Sheyn MD Assistant Professor of Otolaryngology Head and Neck Surgery University of Tennessee Health Science Center Thyroid nodules 20 per 1000 children nodules in children
PEDIATRIC THYROID MALIGNACY Anthony Sheyn MD Assistant Professor of Otolaryngology Head and Neck Surgery University of Tennessee Health Science Center Thyroid nodules 20 per 1000 children nodules in children
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Grave s autoimmune Graves and Hashimotos: antithyroglobulin and antimicrosomal antibodies T3 X 10d should decrease TSH 50%
 Vesalius SCALpel : Thyroid (see also: head and neck folios) Anatomic lingual thyroid most common ectopic location normal thyroid tissue patients may have no thyroid in neck manifest as teenager, may enlarge
Vesalius SCALpel : Thyroid (see also: head and neck folios) Anatomic lingual thyroid most common ectopic location normal thyroid tissue patients may have no thyroid in neck manifest as teenager, may enlarge
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY THE THYROID GLAND DM Dent INTRODUCTION Thyroid problems are commonly encountered in general practice. In most instances they will be minor ones of physiological
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY THE THYROID GLAND DM Dent INTRODUCTION Thyroid problems are commonly encountered in general practice. In most instances they will be minor ones of physiological
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Oh, I get it, the TSH goes up and down
 Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Thyroid Ultrasonography: clinical and radiological correlations
 Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal
Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
MTP: Thyroid Nodules
 Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
A rare case of solitary toxic nodule in a 3yr old female child a case report
 Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Thyroid carcinoma. Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec.
 Thyroid carcinoma Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec. Thyroid tumors PRIMARY TUMORS Tumors of the follicular epithelium : - Tumors of the follicular
Thyroid carcinoma Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec. Thyroid tumors PRIMARY TUMORS Tumors of the follicular epithelium : - Tumors of the follicular
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Thyroid Neoplasm. ORL-Head and neck Surgery 2014
 In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
Volume 2 Issue ISSN
 Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Thyroid and Parathyroid Surgery
 Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
An Alphabet Soup of Thyroid Neoplasms
 Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
The Frozen Section: Diagnostic Challenges and Pitfalls
 The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
Disclosures. Learning objectives. Case 1A. Autoimmune Thyroid Disease: Medical and Surgical Issues. I have nothing to disclose.
 Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
The Thyroid Gland. Chaitan K. Narsule, M.D.
 The Thyroid Gland Chaitan K. Narsule, M.D. The Thyroid Gland Thyreoides = shield shaped Goiter well-described in literature in 19th century Seaweed was medical treatment (iodine rich) The Thyroid Gland
The Thyroid Gland Chaitan K. Narsule, M.D. The Thyroid Gland Thyreoides = shield shaped Goiter well-described in literature in 19th century Seaweed was medical treatment (iodine rich) The Thyroid Gland
What is Thyroid Cancer? Here are four types of thyroid cancer:
 What is Thyroid Cancer? Thyroid cancer is a group of malignant tumors that originate from the thyroid gland. The thyroid is a gland in the front of the neck. The thyroid gland absorbs iodine from the bloodstream
What is Thyroid Cancer? Thyroid cancer is a group of malignant tumors that originate from the thyroid gland. The thyroid is a gland in the front of the neck. The thyroid gland absorbs iodine from the bloodstream
CN 925/15 History. Microscopic Findings
 CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
ASCP Competency Assessment
 ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
THYROID CANCER IN CHILDREN
 THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
Review Article Management of thyroid carcinoma Alauddin M, Joarder AH
 Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS. Dr. Pamela Hanson DO PGY3
 PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
 To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration
 AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY
 DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY DEVELOPMENT OF THYROID Concept of pharyngeal arch 3 rd week 4 th week Adults 7 th week HISTOGENESIS OF THYROID GLAND
DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY DEVELOPMENT OF THYROID Concept of pharyngeal arch 3 rd week 4 th week Adults 7 th week HISTOGENESIS OF THYROID GLAND
Michigan AACE: Case Presentation
 Michigan AACE: Case Presentation Marco De Santis D.O. Endocrinology Fellow McLaren Medical Center Macomb Background O 83 year old female with fatigue and TSH of 0.13 O Medical history T2DM, Osteoporosis,
Michigan AACE: Case Presentation Marco De Santis D.O. Endocrinology Fellow McLaren Medical Center Macomb Background O 83 year old female with fatigue and TSH of 0.13 O Medical history T2DM, Osteoporosis,
Well-differentiated Thyroid Cancer. Anton Sharapov, R4
 Well-differentiated Thyroid Cancer Anton Sharapov, R4 Outline Types of DTC Diagnosis of DTC Treatment options Extent of surgery Follow up cases A bit of history Theodore Kocher, Bern, Switzerland 1872,
Well-differentiated Thyroid Cancer Anton Sharapov, R4 Outline Types of DTC Diagnosis of DTC Treatment options Extent of surgery Follow up cases A bit of history Theodore Kocher, Bern, Switzerland 1872,
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Hyperthyroidism Diagnosis and Treatment. April Janet A. Schlechte, M.D.
 Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta
 Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Thyroid Diseases. Dr Rodney Itaki Lecturer Anatomical Pathology Discipline
 Thyroid Diseases Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology This is the normal appearance of thethyroid
Thyroid Diseases Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology This is the normal appearance of thethyroid
Cytology for the Endocrinologist. Nicole Massoll M.D
 Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Thyroid Cancer. With 51 Figures and 30 Tables. Springer
 H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
Shadow because the air
 Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Sonographic imaging of pediatric thyroid disorders in childhood. Experiences and report in 150 cases
 Sonographic imaging of pediatric thyroid disorders in childhood. Experiences and report in 150 cases M. Mearadji International Foundation for Pediatric Imaging Aid Sonographic technique. Use of high frequency
Sonographic imaging of pediatric thyroid disorders in childhood. Experiences and report in 150 cases M. Mearadji International Foundation for Pediatric Imaging Aid Sonographic technique. Use of high frequency
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
A descriptive study on solitary nodular goitre
 Original Research Article A descriptive study on solitary nodular goitre T. Chitra 1*, Dorai D. 1, Aarthy G. 2 1 Associate Professor, 2 Post Graduate Department of General Surgery, Govt. Stanley Medical
Original Research Article A descriptive study on solitary nodular goitre T. Chitra 1*, Dorai D. 1, Aarthy G. 2 1 Associate Professor, 2 Post Graduate Department of General Surgery, Govt. Stanley Medical
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
AACE/AME/ETA Guidelines
 AACE/AME/ETA Guidelines American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association Medical Guidelines for Clinical Practice for the Diagnosis
AACE/AME/ETA Guidelines American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association Medical Guidelines for Clinical Practice for the Diagnosis