Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience. Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore
|
|
|
- Marshall Richardson
- 5 years ago
- Views:
Transcription

1 Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore


2



3


4 Queensland 2500 times the size of Singapore Same population as Singapore! Half the number of ENT $urgeons Over two thirds of ENT surgeons in Brisbane and Gold Coast Fastest growing state in Australia Home of Kevin Rudd!

5 Head and Neck Service at Princess Alexandra Hospital Second largest hospital in Queensland 727 beds Head and Neck unit sees 840 new cancer cases per year 5 visiting medical officers and 1 staff specialist
 Trigeminal nerve perineural spread of skin SCC")
6 Head and Neck Cancer in Queensland High rate of smoking and alcohol consumption Sun related skin cancers extremely common Half all parotidectomies done for malignant disease (SCC with lymph node) Trigeminal nerve perineural spread of skin SCC common

7 Supracricoid laryngectomy (SCL + CHP / CHEP) First described by Majer & Rieder in 1959 Rediscovered and modified by the French in 1974 Not widely reported in English literature until 1990s Preservation of the hyoid bone, cricoid cartilage and one cricoarytenoid unit Reconstruction CHP or CHEP
8 SCL Indications T2 lesions of the glottis or supraglottis (epiglottis) T3 lesions with vocal cord fixation, pre-epiglottic space invasion or minimal thyroid cartilage invasion (Patient motivation!) Contraindications Arytenoid fixation Infraglottic extension (10 mm anteriorly, 5 mm posteriorly) Significant pre-epiglottic space involvement Cricoid cartilage invasion Invasion outer perichondrium of thyroid cartilage Extralaryngeal extension Poor pulmonary function Severe reflux disease

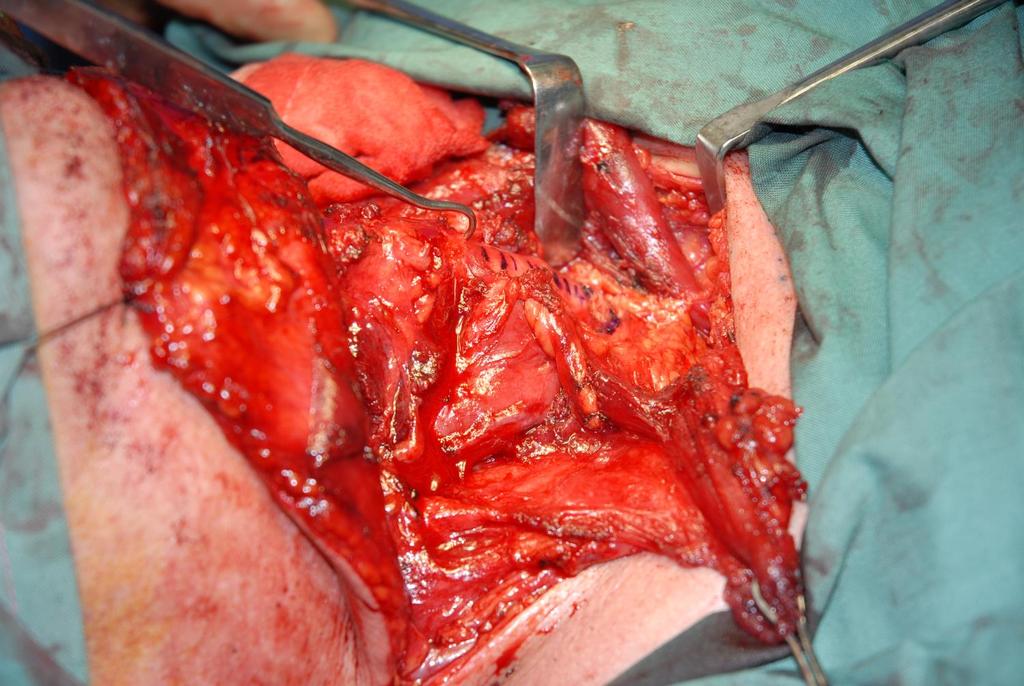
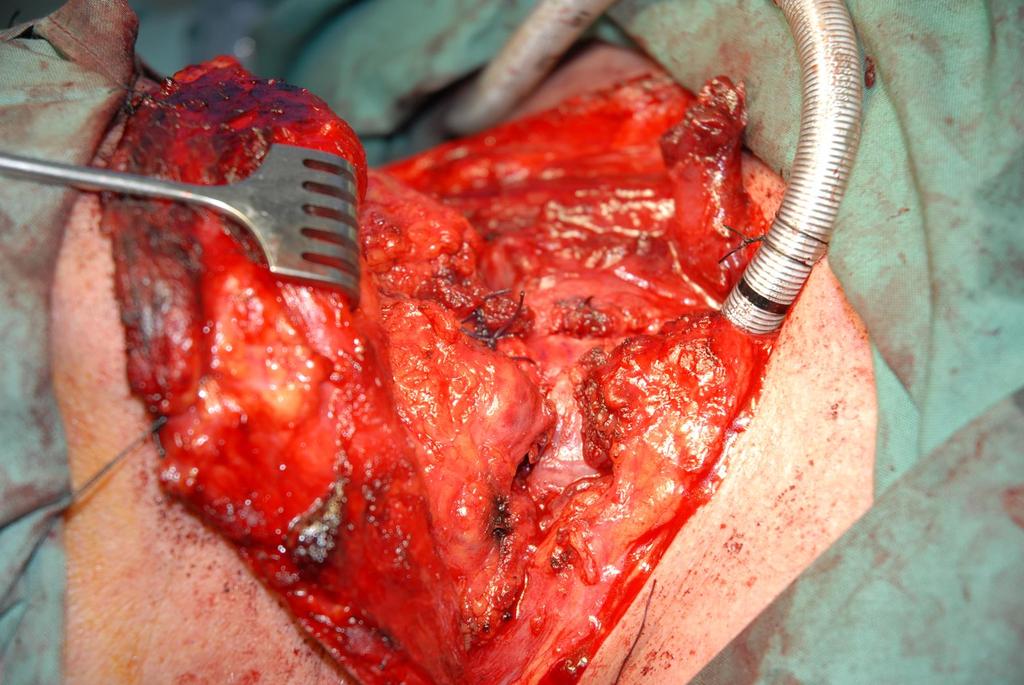
9 Surgical steps

10 Exposure Thyroidectomy incision extended as necessary for neck dissection Subplatysmal flaps elevated 1 cm beyond hyoid to sternal notch Sternohyoid divided superiorly and preserved Deep straps transected along upper and lower borders of the thyroid cartilage

11 Strap division
12 Exposure Laryngeal vessels are ligated preserving the superior laryngeal nerve Inferior pharyngeal constrictors and external thyroid cartilage perichondrium and transected, allowing the pyriform sinuses to be released as per laryngectomy Isthmus of the thyroid gland is divided and transfixed Trachea is freed to the carina by blunt dissection along the anterior wall Both recurrent laryngeal nerves are identified and preserved Cricothyroid joints are disarticulated
13 Exposure
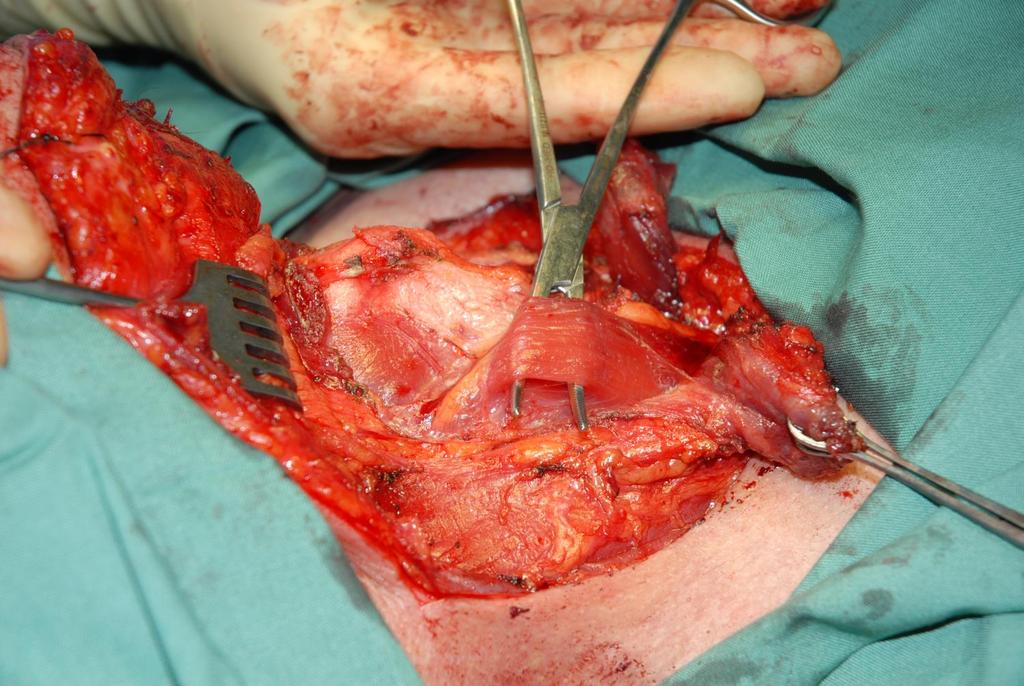
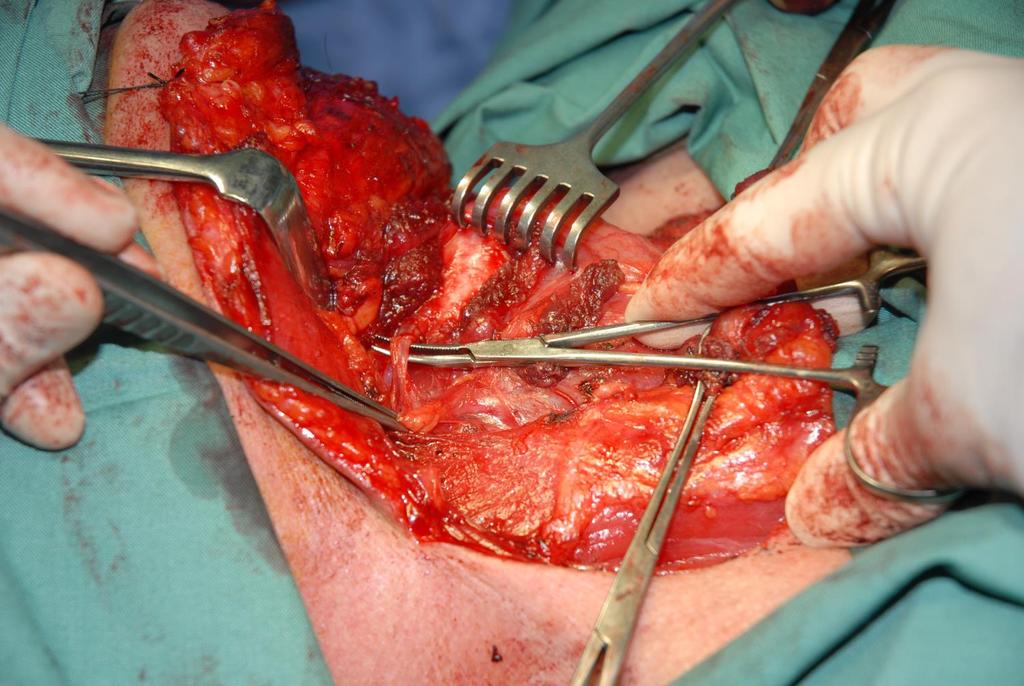
14 Resection Hyoid periosteum incised anteriorly and laterally Pre-epiglottic space dissected from posterior surface of hyoid Larynx entered superiorly through a transvallecular horizontal pharyngotomy, and inferiorly through cricothyroidotomy just above border of cricoid ETT removed then inserted via cricothyroidotomy Surgeon moves to head of bed for better visualisation Vertical pre-arytenoid incision is made with the scissor down to the cricothyroidotomy on the non-tumour bearing side
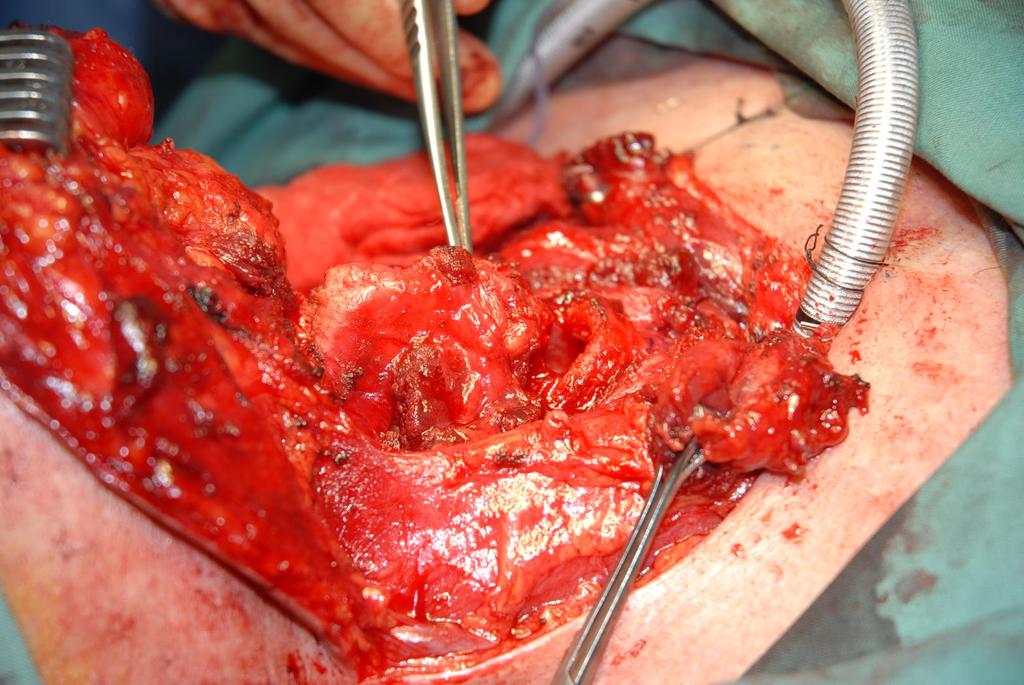
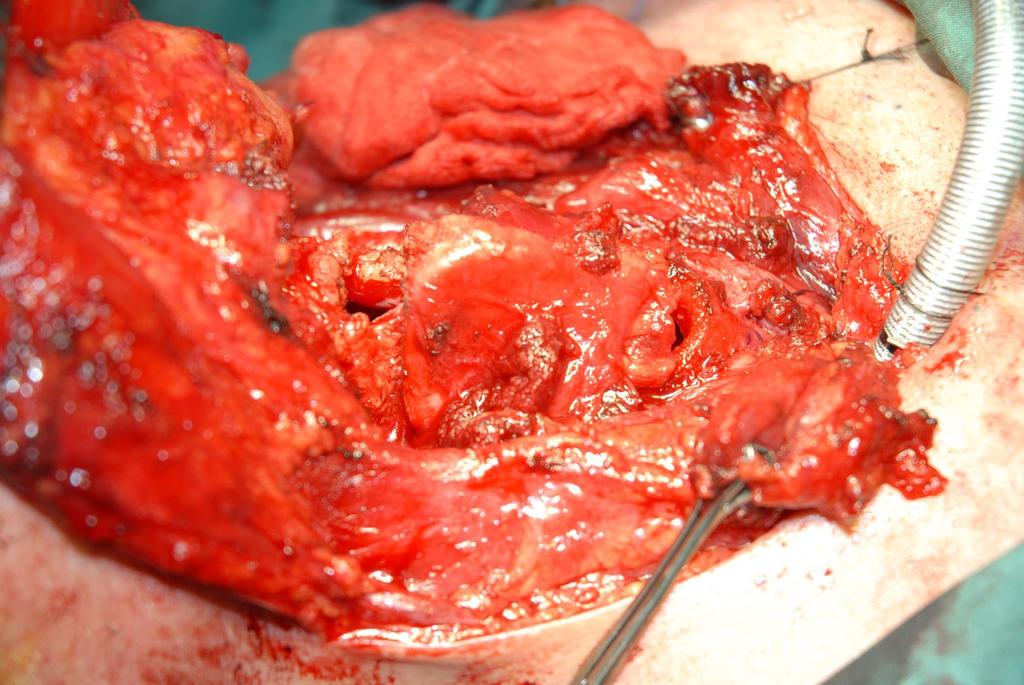
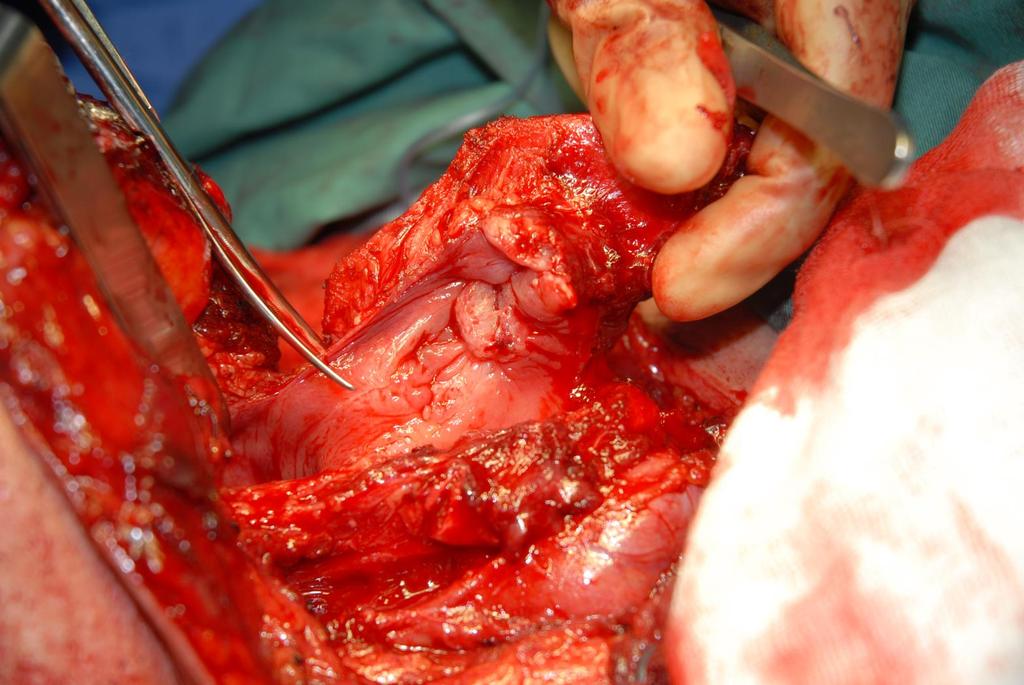
15 Resection
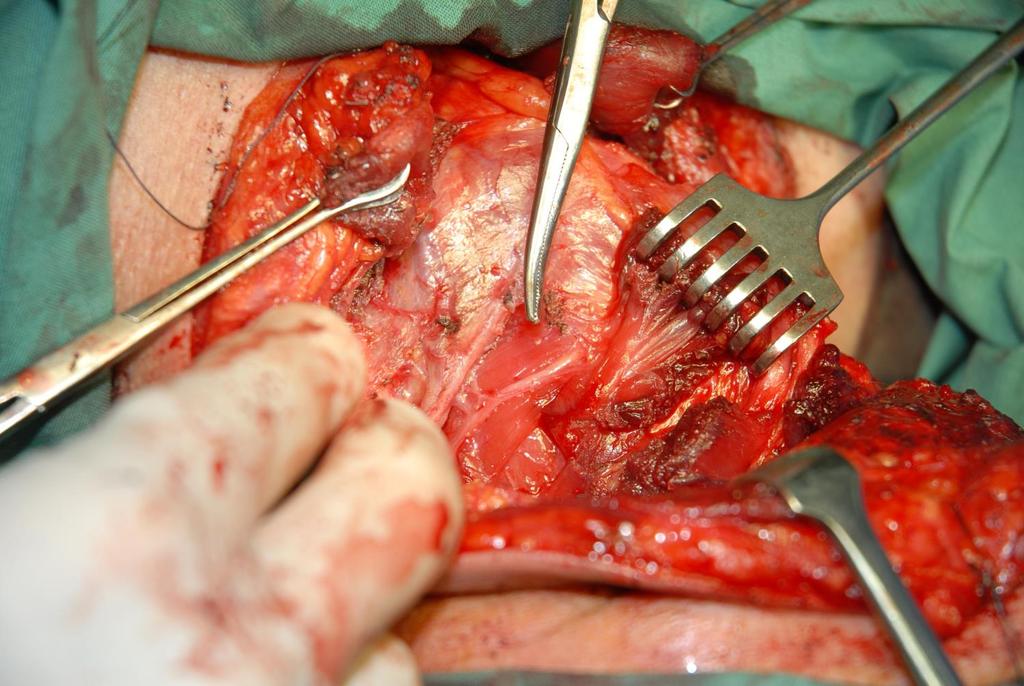
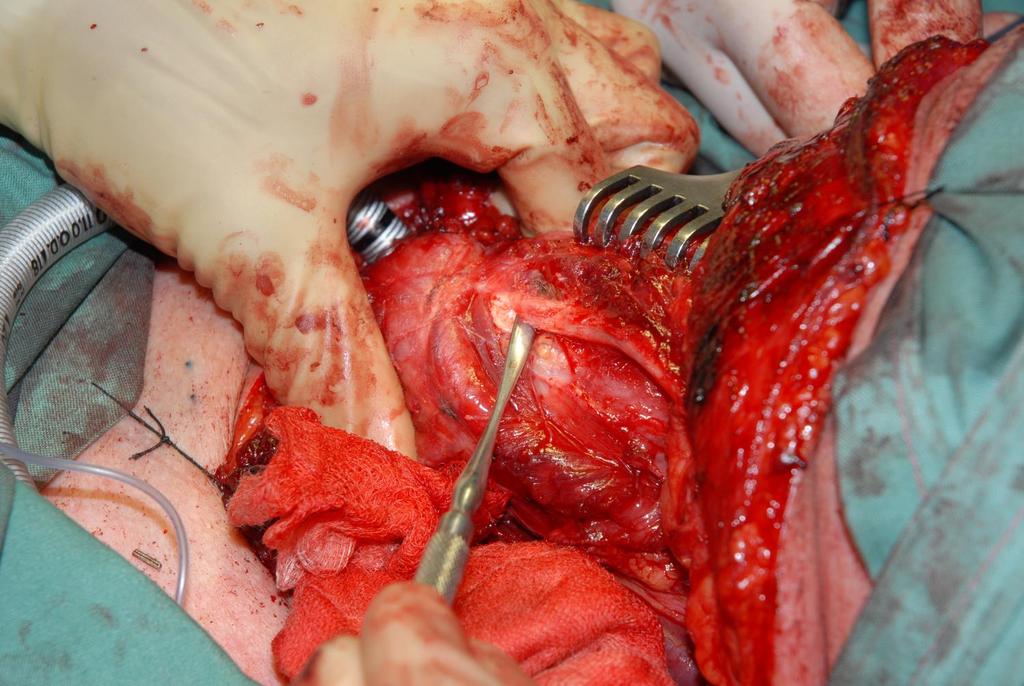
16 Resection Thyroid cartilage is then grasped and fractured along the midline, as if opening a book Excision of the tumour then proceeds under direct visualisation Excision of one arytenoid is possible
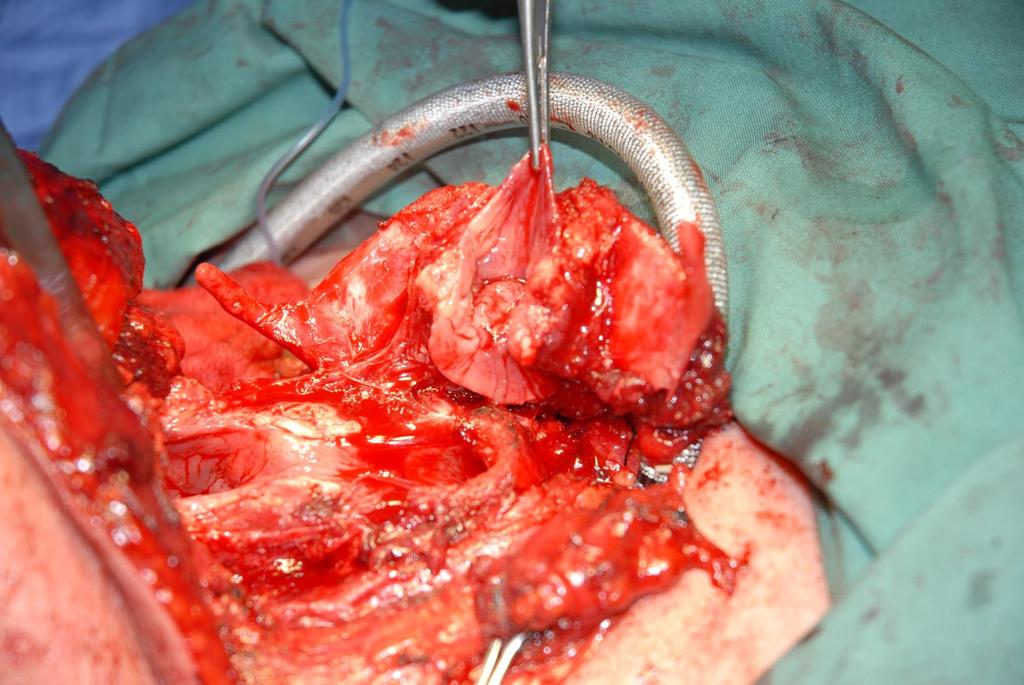

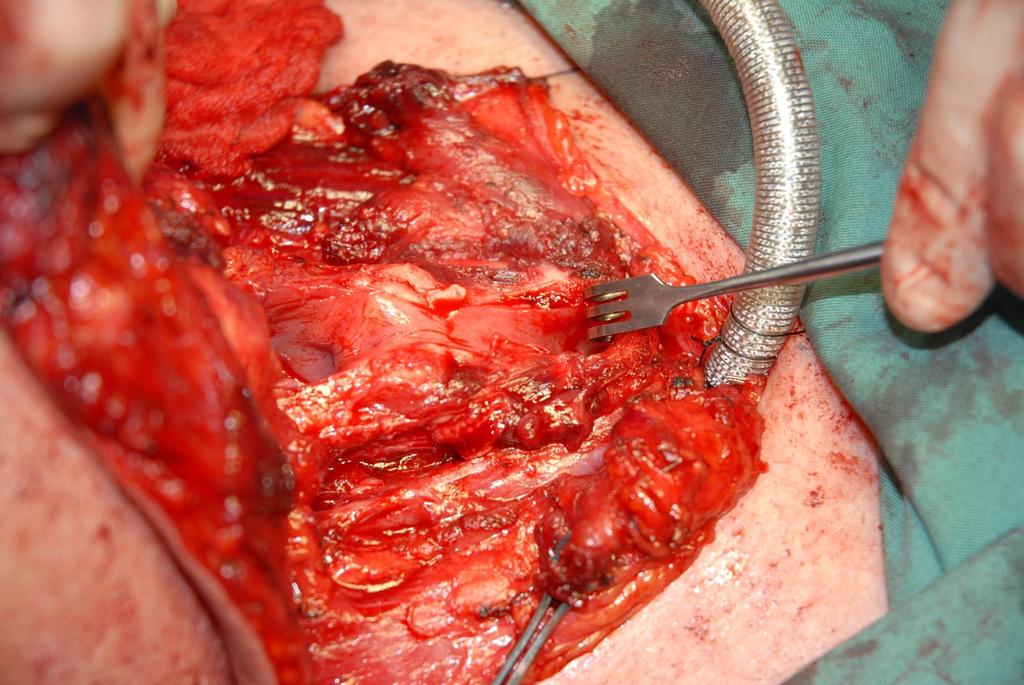
17 Resection
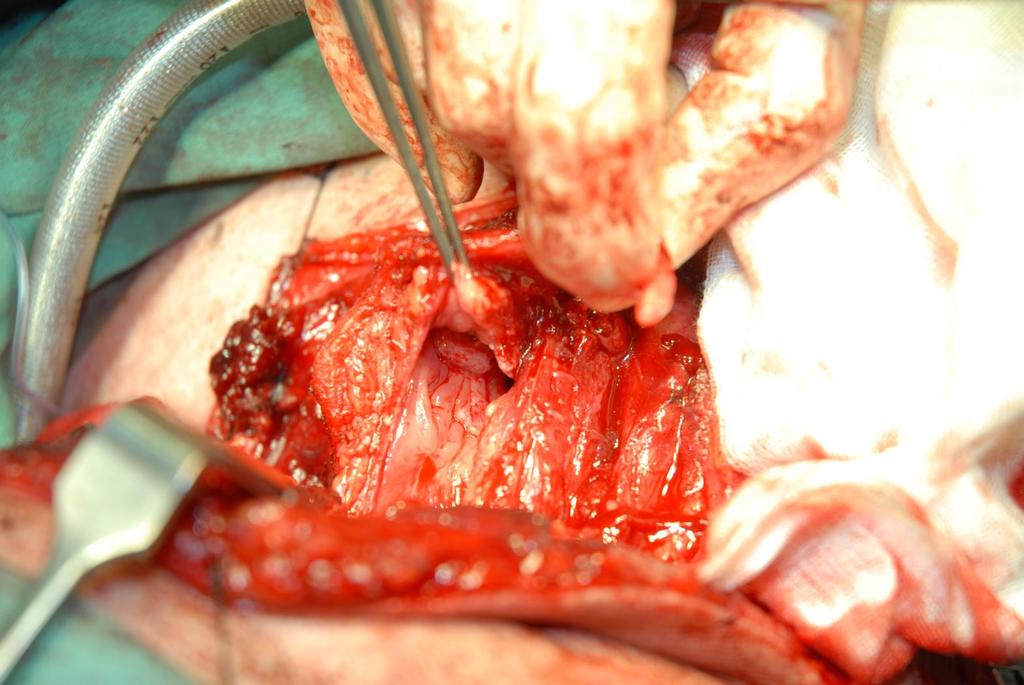
18 Reconstruction Nasogastric tube is best placed at this juncture Mucosa of the upper arytenoid is sutured close primarily with 4/0 vicryl Arytenoids are drawn forward and sutured to the posterolateral aspect of the cricoid with 2/0 vicryl sutures The cricohyoidopexy or cricohyoepiglottopexy is performed using three submucosal 0 prolene sutures around the hyoid and cricoid. The sutures should catch the root of the suprahyoid epiglottis if this structure has been preserved Tracheostomy is performed, allowing removal of the ETT Pexy sutures are tied whilst tension is applied by neighbouring sutures
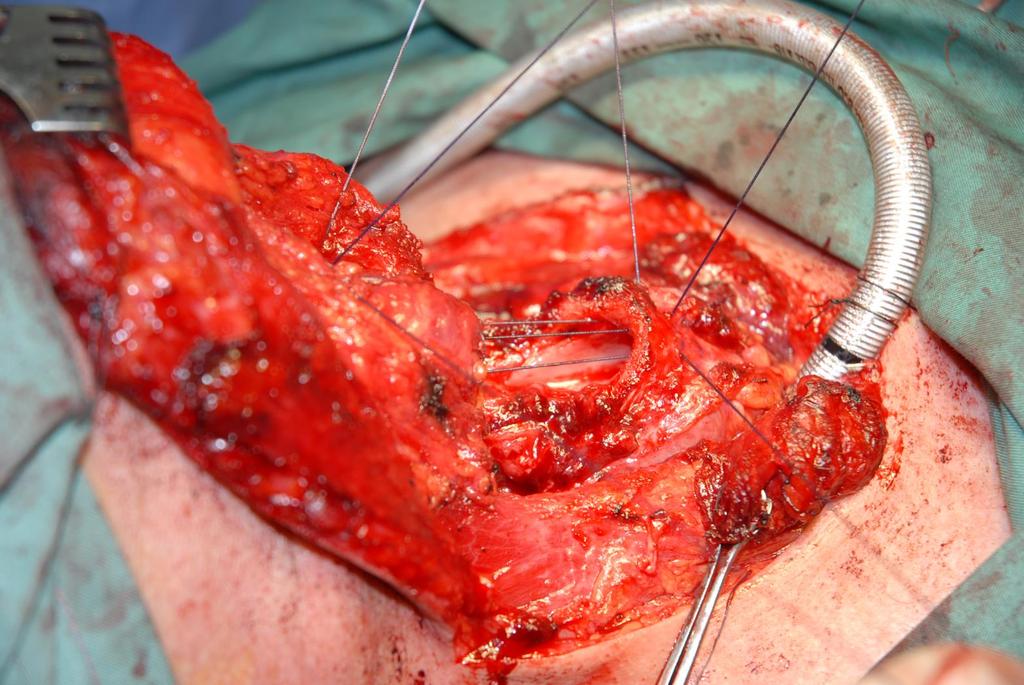
19 Reconstruction
20 Post-operative care Post-operative antibiotics for 7 days Long term anti-reflux medication Daily physiotherapy Decannulation is attempted when cuff deflation is tolerated and patients can cough Patients are taught supraglottic swallow by speech therapists PEG tube is considered in patients who are likely to need prolonged rehabilitation

21 Princess Alexandra Case Series (Retrospective chart review)
22 Patient details n = 19 Consecutive cases between Performed by 4 surgeons Age at diagnosis = 52.6 years 15 Male : 4 Female 6 treated for recurrent disease (2 post RT, 2 post laser, 2 post RT & laser) 13 treated primarily
23 Tumour characteristics Primary site: 14 glottic 5 supraglottic Stage preoperatively rt1b 2 T2 8 rt2 3 T3 5 rt3 1 Nodal status N0 14 N1 2 N2a 1 N2c 2
24 Operative details 13/19 had SCL-CHP 6/19 had SCL-CHEP 7/19 had one arytenoid resected 9/19 had simultaneous bilateral neck dissections 5/19 had unilateral neck dissections Pathology: 15/19 CLEAR 3/19 Positive 1/19 Close 1/19 Perineural Invasion 2/19 Lymphovascular invasion Median depth: 5.5 mm
25 Outcomes Median length of stay = 18 days Median days to decannulation = 8.5 days Median days to complete enteral feeding = 165 days 4/19 patients received adjuvant RT Complications: 3/19 wound infections, 2/19 chest infections, 1 significant aspiration, 1 post-op haematoma 2 patients had local recurrence; 1 significant aspiration had salvage surgery: 2 had total laryngectomy 1 required pharyngolaryngectomy Median FU: 15 months 17/19 Alive free of disease 1/19 Dead from disease 1/19 Dead from other causes
26 Trends from PA case series Salvage SCL and resection of one arytenoid associated with more complications and delayed PEG removal, but not longer decannulation No difference in overall survival in group treated primarily and group treated for salvage Salvage SCL following RT (4/19) All alive and free of disease at 84 months But 2/4 required completion laryngectomy Positive margins predicts local recurrence
27 Literature Review
28 Case series of previously untreated cases of early stage disease Series n Decannulation (days) Enteral feeding (days) Median FU (months) Diseasespecific survival Comment Laccourreye, Laennec Hospital, Paris, (Only in 74.6%) % Neo-adj 3 cycles of Cis/5FU chemo, 17/68 Adj RT to neck La Sapienza University Rome, in 97.2% (CHEP); 30 in 90% (CHP) 15 (CHEP); 28 (CHP) % Adj RT in 10; Uni & Multivariate analysis RT for T1 T2 glottis Mendenhall WM (2001) T1a T1b T2a T2b 5 year disease specific survival 98% 98% 95% 90% 5 year local control with laryngeal preservation 95% 95% 82% 76%
29 Case series of previously untreated advanced disease (T3 / T4) Series n Length of stay Decannulation (days) Enteral feeding (days) Medi an FU (mont hs) Diseasespecific survival Comment Laccourreye, Laennec Hospital, Paris, 1998 Brazilian National Cancer Inst, N/A N/A N/A % (Local control 91.7%) % (Local control 94.7%) Neo-adj 3 cycles of Cis/5FU chemo, 17/60 Adj RT 14/43 had adjuvant RT; 10 cases excluded due to poor FU RTOG Headline figure of 88% larynx preservation at 2 years and reduction of laryngectomy by 43% But, 23% poor swallow, 3% can t swallow and 36% 5 year disease-free survival in the concurrent chemoradiotherapy group
30 Comparable case series Series n Primary: Salvage Johns Hopkins, 2007 Lausanne, Switzerland, 2000 Stay (days) Decannulation (days) Enteral feeding (days) Median FU (months) Diseasespecific survival 24 14: % 69 54: % Brisbane 19 13: %
31 SCL after radiation failure? Supracricoid Partial Laryngectomies after radiation failure: A multi-institutional series Pellini R et. al. Head Neck 2008; 30: Multicentred Italian retrospective study 78 men, mean age 59.6 years Stage I and II disease initially Gy RT. No chemo Median disease-free interval between RT and salvage surgery = 16 months 62 SCL-CHEP 16 SCL-CHP 41/78 had one arytenoid resected 21/78 had simultaneous neck dissections 15 unilateral, 6 bilateral Disease-free survival = 95.5% at 3 and 5 years Overall survival = 85.2% at 3 years; 81.8% at 5 years All but 2 decannulated, all but 2 returned to enteral feeding
32 Conclusions SCL is an oncologically sound operation It has a role in selected untreated cases and in the salvage setting It is an option that should always be considered when contemplating total laryngectomy It may enhance quality of life without jeopardising survival rates. Further research in this area is necessary Unlike laser microsurgery, it requires minimal equipment and is easier to master

33
Alexander C Vlantis. Total Laryngectomy 57
 07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY VERTICAL PARTIAL LARYNGECTOMY Management of small tumours involving the true vocal folds can be contentious. Tumour control is achieved
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY VERTICAL PARTIAL LARYNGECTOMY Management of small tumours involving the true vocal folds can be contentious. Tumour control is achieved
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
Organ preservation in laryngeal cancer
 Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
A220: Larynx cancer tissues. (formalin fixed)
") A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
Thyroidectomy. Siu Kwan Ng. Modified Radical Neck Dissection Type II 47
 06 Thyroidectomy Siu Kwan Ng Modified Radical Neck Dissection Type II 47 Thyroidectomy STEP 1. EXPOSING THE THYROID GLAND The collar incision Figure 1 (curvilinear skin crease incision) is made at 1.5-2
06 Thyroidectomy Siu Kwan Ng Modified Radical Neck Dissection Type II 47 Thyroidectomy STEP 1. EXPOSING THE THYROID GLAND The collar incision Figure 1 (curvilinear skin crease incision) is made at 1.5-2
Treatment for Supraglottic Ca History: : Total Laryngectomy y was routine until early 50 s, when XRT was developed Ogura and Som developed the one-sta
 Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
T1/T2 LARYNX CANCER. Click to edit Master Presentation Date. Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery
 ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic space
 Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Anatomy of the Airway
 Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
SUPRACRICOID LARYNGECTOMY
 CC-BY-NC 3.0 SUPRCRICOID LRYNGECTOMY lejandro Castro & Javier Gavilán Supracricoid laryngectomy consists of en bloc resection of both vocal cords, the paraglottic spaces and the thyroid cartilage (Figure
CC-BY-NC 3.0 SUPRCRICOID LRYNGECTOMY lejandro Castro & Javier Gavilán Supracricoid laryngectomy consists of en bloc resection of both vocal cords, the paraglottic spaces and the thyroid cartilage (Figure
Supracricoid partial laryngectomy (SCPL) was first
 was first") Original Research Head and Neck Surgery Supracricoid Partial Laryngectomy: Analyses of Oncologic and Functional Outcomes Otolaryngology Head and Neck Surgery 147(6) 1093 1098 Ó American Academy of Otolaryngology
Original Research Head and Neck Surgery Supracricoid Partial Laryngectomy: Analyses of Oncologic and Functional Outcomes Otolaryngology Head and Neck Surgery 147(6) 1093 1098 Ó American Academy of Otolaryngology
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
12 Larynx. I - Cartilages. Learning Objectives
 12 Larynx Learning Objectives By the end of this topic you should be able to: Identify the cartilages, membranes, muscles and nerves of the larynx. Describe the attachments of the larynx to other structures
12 Larynx Learning Objectives By the end of this topic you should be able to: Identify the cartilages, membranes, muscles and nerves of the larynx. Describe the attachments of the larynx to other structures
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer. American Society of Clinical Oncology Clinical Practice Guideline
 Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Original Article Analysis of surgical methods and their long-term effect on laryngeal carcinoma
 Int J Clin Exp Med 2016;9(2):4491-4496 www.ijcem.com /ISSN:1940-5901/IJCEM0013482 Original Article Analysis of surgical methods and their long-term effect on laryngeal carcinoma Hong-Bing Liu *, Chun-Ping
Int J Clin Exp Med 2016;9(2):4491-4496 www.ijcem.com /ISSN:1940-5901/IJCEM0013482 Original Article Analysis of surgical methods and their long-term effect on laryngeal carcinoma Hong-Bing Liu *, Chun-Ping
Larynx. Rudimentary. Behind the posterior surface : -stylopharyngeus - salpingopharyngeus -platopharyngeus
 Larynx The larynx is an organ that provides a protective sphincter at the inlet of the air passages and is responsible for voice production. It extends from C3-C6: *Posterior: the pharynx *Lateral: the
Larynx The larynx is an organ that provides a protective sphincter at the inlet of the air passages and is responsible for voice production. It extends from C3-C6: *Posterior: the pharynx *Lateral: the
Surgical Management of Subglottic Stenosis
 Surgical Management of Subglottic Stenosis Cameron D. Wright, MD ubglottic stenosis is usually due to either endotracheal S tube ischemic necrosis or idiopathic larygotracheal stenosis. The ischemic area
Surgical Management of Subglottic Stenosis Cameron D. Wright, MD ubglottic stenosis is usually due to either endotracheal S tube ischemic necrosis or idiopathic larygotracheal stenosis. The ischemic area
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient
 Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
FUNCTIONAL ANALYSIS OF SWALLOWING OUTCOMES AFTER SUPRACRICOID PARTIAL LARYNGECTOMY
 ORIGINAL ARTICLE FUNCTIONAL ANALYSIS OF SWALLOWING OUTCOMES AFTER SUPRACRICOID PARTIAL LARYNGECTOMY Jan S. Lewin, PhD, Katherine A. Hutcheson, MS, Denise A. Barringer, MS, Annette H. May, MA, Dianna B.
ORIGINAL ARTICLE FUNCTIONAL ANALYSIS OF SWALLOWING OUTCOMES AFTER SUPRACRICOID PARTIAL LARYNGECTOMY Jan S. Lewin, PhD, Katherine A. Hutcheson, MS, Denise A. Barringer, MS, Annette H. May, MA, Dianna B.
Adenoid Cystic Carcinoma Minor Salivary Gland Origin
 Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
Mohammed AlEssa MBBS,FRCSC Consultant Otolaryngology,Head & Neck Surgery King Saud University- medical city National guard health affairs KAMC
 Mohammed AlEssa MBBS,FRCSC Consultant Otolaryngology,Head & Neck Surgery King Saud University- medical city National guard health affairs KAMC 1.7% of all cancer in male in KSA ** Laryngeal cancer affects
Mohammed AlEssa MBBS,FRCSC Consultant Otolaryngology,Head & Neck Surgery King Saud University- medical city National guard health affairs KAMC 1.7% of all cancer in male in KSA ** Laryngeal cancer affects
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Please refer back to the slides as these are extra notes only. Slide 2 -The Larynx is a Box of cartilage.
 [ANATOMY #3] 1 بسم رلاهللا Please refer back to the slides as these are extra notes only. Slide 2 -The Larynx is a Box of cartilage. -The lower border of c6 is the lower border of cricoid cartilage. -The
[ANATOMY #3] 1 بسم رلاهللا Please refer back to the slides as these are extra notes only. Slide 2 -The Larynx is a Box of cartilage. -The lower border of c6 is the lower border of cricoid cartilage. -The
TRACHEOSTOMY. Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion
 TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
L ARYNX S TAGING F ORM
 CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Conservation Laryngeal Surgeries
 Conservation Laryngeal Surgeries The principles of management of the laryngeal cancer have evolved over the recent past with emphasis on organ preservation. These developments have paralleled technological
Conservation Laryngeal Surgeries The principles of management of the laryngeal cancer have evolved over the recent past with emphasis on organ preservation. These developments have paralleled technological
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
Larynx - cartilaginous structure holding the vocal folds which protrude into airstream
 1! Larynx - cartilaginous structure holding the vocal folds which protrude into airstream 2! Flow increase - like thumb over garden hose Pressure drop - narrower space forces pressure drop due to speed
1! Larynx - cartilaginous structure holding the vocal folds which protrude into airstream 2! Flow increase - like thumb over garden hose Pressure drop - narrower space forces pressure drop due to speed
MULTIDISCIPLINARY MGMT. OF INTERMEDIATE STAGE LARYNGEAL CANCER, ROBERT L. FERRIS, MD 1
 CANCER, ROBERT L. FERRIS, MD 1 Thank you Dr. Johnston, good morning. I m pleased to present the grand rounds for the University of Pittsburgh, the Division of Head and Neck Surgery, and the topic for this
CANCER, ROBERT L. FERRIS, MD 1 Thank you Dr. Johnston, good morning. I m pleased to present the grand rounds for the University of Pittsburgh, the Division of Head and Neck Surgery, and the topic for this
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Anatomy of Head of Neck Cancer
 Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA
 AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
The Larynx. Prof. Dr.Mohammed Hisham Al-Muhtaseb
 The Larynx Prof. Dr.Mohammed Hisham Al-Muhtaseb The Larynx Extends from the middle of C3 vertebra till the level of the lower border of C6 Continue as Trachea Above it opens into the laryngo-pharynx Suspended
The Larynx Prof. Dr.Mohammed Hisham Al-Muhtaseb The Larynx Extends from the middle of C3 vertebra till the level of the lower border of C6 Continue as Trachea Above it opens into the laryngo-pharynx Suspended
Aetiology. Poor tube management. Small cricoid (acquired on congenital) Reflux Poor general status. Size of tube (leak) Duration of intubation
 Reflux Poor general status. Size of tube (leak) Duration of intubation") Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Survey of Laryngeal Cancer at SBUH comparing 108 cases seen here from to the NCDB of 9,256 cases diagnosed nationwide in 2000
 Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
The management of advanced supraglottic and
 ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Structure and Nerve Supply of The Larynx
 Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical sciences Structure and Nerve Supply of The Larynx This presentation was originally prepared by: Dr. Kumar Notes were added by:
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical sciences Structure and Nerve Supply of The Larynx This presentation was originally prepared by: Dr. Kumar Notes were added by:
Information and support
 13 11 20 Information and support Surgery for head and neck cancer Last reviewed June 2012 Contents Types of surgeries Surgery for oral cancer Surgery for salivary gland cancer Surgery for pharyngeal cancer
13 11 20 Information and support Surgery for head and neck cancer Last reviewed June 2012 Contents Types of surgeries Surgery for oral cancer Surgery for salivary gland cancer Surgery for pharyngeal cancer
Head and neck cancer - patient information guide
 Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
FACULTY OF MEDICINE SIRIRAJ HOSPITAL
 Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
2. Guidelines for Reporting Head and Neck Tumours
 39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City.
 JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Esophagus Stomach 4/2/15
 Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis
 Otolaryngology Head and Neck Surgery (2006) 135, 318-322 ORIGINAL RESEARCH Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis Mark E. Boseley, MD, and Christopher
Otolaryngology Head and Neck Surgery (2006) 135, 318-322 ORIGINAL RESEARCH Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis Mark E. Boseley, MD, and Christopher
Ovid: Oxford Textbook of Endocrinology & Diabetes
 Página 1 de 6 Copyright 2002 Oxford University Press Wass, John A.H., Shalet, Stephen M., Gale, Edwin, Amiel, Stephanie A. Oxford Textbook of Endocrinology & Diabetes, 1st Edition Surgical procedure Part
Página 1 de 6 Copyright 2002 Oxford University Press Wass, John A.H., Shalet, Stephen M., Gale, Edwin, Amiel, Stephanie A. Oxford Textbook of Endocrinology & Diabetes, 1st Edition Surgical procedure Part
Tympanic Bulla Temporal Bone. Digastric Muscle. Masseter Muscle
 Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Hypopharynx and larynx anatomy
 Hypopharynx and larynx anatomy Poster No.: C-0786 Congress: ECR 2016 Type: Educational Exhibit Authors: A. I. Fernández Martín, N. Delgado Ronda, E. Dominguez 1 3 2 4 5 Franjo, M. Martínez Martínez-Losa,
Hypopharynx and larynx anatomy Poster No.: C-0786 Congress: ECR 2016 Type: Educational Exhibit Authors: A. I. Fernández Martín, N. Delgado Ronda, E. Dominguez 1 3 2 4 5 Franjo, M. Martínez Martínez-Losa,
1/14/2019 CRITICAL PATHWAYS IN HEAD AND NECK CANCER DISCLOSURES OBJECTIVES
 CRITICAL PATHWAYS IN HEAD AND NECK CANCER Caroline Nickel, MS CCC-SLP Baylor University Medical Center Dallas, Texas DISCLOSURES Caroline Nickel is employed by Baylor Institute for Rehabilitation. Caroline
CRITICAL PATHWAYS IN HEAD AND NECK CANCER Caroline Nickel, MS CCC-SLP Baylor University Medical Center Dallas, Texas DISCLOSURES Caroline Nickel is employed by Baylor Institute for Rehabilitation. Caroline
NAACCR Webinar Series 11/2/2017
 COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue
 Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives
THE SUBMENTAL ISLAND FLAP IN HEAD AND NECK RECONSTRUCTION
 THE SUBMENTAL ISLAND FLAP IN HEAD AND NECK RECONSTRUCTION Emre Vural, MD, James Y. Suen, MD Department of Otolaryngology-Head and Neck Surgery, University of Arkansas for Medical Sciences, 4301 West Markham,
THE SUBMENTAL ISLAND FLAP IN HEAD AND NECK RECONSTRUCTION Emre Vural, MD, James Y. Suen, MD Department of Otolaryngology-Head and Neck Surgery, University of Arkansas for Medical Sciences, 4301 West Markham,
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Cancer of the Oral Cavity
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)
Chirurgia conservativa. Vice Direttore Scientifico Direttore Divisione Testa e Collo Istituto Europeo di Oncologia
 Chirurgia conservativa Fausto Chiesa Mohssen Ansarin Vice Direttore Scientifico Direttore Divisione Testa e Collo Istituto Europeo di Oncologia Laryngeal Cancer: 51% of H&N cancer H&N Cancer 4.7% of all
Chirurgia conservativa Fausto Chiesa Mohssen Ansarin Vice Direttore Scientifico Direttore Divisione Testa e Collo Istituto Europeo di Oncologia Laryngeal Cancer: 51% of H&N cancer H&N Cancer 4.7% of all
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Chapter 115: Conservation Surgery of the Larynx. Gary L. Schechter. History of Conservation Surgery of the Larynx
 Chapter 115: Conservation Surgery of the Larynx Gary L. Schechter Preservation of function is a prime consideration in all aspects of head and neck surgery. Conservation surgery of the larynx deals specifically
Chapter 115: Conservation Surgery of the Larynx Gary L. Schechter Preservation of function is a prime consideration in all aspects of head and neck surgery. Conservation surgery of the larynx deals specifically
External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other
 Internal trauma (Endotracheal intubation, tracheostomy) Other") Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Thyroid and Parathyroid Glands
 Thyroid and Parathyroid Glands Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/ explanation Objectives: By the end of the lecture,
Thyroid and Parathyroid Glands Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/ explanation Objectives: By the end of the lecture,
INDICATIONS OF CRICOHYOIDOEPIGLOTTOPEXY VERSUS ANTERIOR FRONTAL LARYNGECTOMY: THE ROLE OF CONTRALATERAL VOCAL FOLD SPREAD
 ORIGINAL ARTICLE INDICATIONS OF CRICOHYOIDOEPIGLOTTOPEXY VERSUS ANTERIOR FRONTAL LARYNGECTOMY: THE ROLE OF CONTRALATERAL VOCAL FOLD SPREAD David Bakhos, MD, Emmanuel Lescanne, MD, PhD, Patrice Beutter,
ORIGINAL ARTICLE INDICATIONS OF CRICOHYOIDOEPIGLOTTOPEXY VERSUS ANTERIOR FRONTAL LARYNGECTOMY: THE ROLE OF CONTRALATERAL VOCAL FOLD SPREAD David Bakhos, MD, Emmanuel Lescanne, MD, PhD, Patrice Beutter,
Carcinoma of the larynx L 4. Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%.
 L 4 Carcinoma of the larynx Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%. Incidence: It is more common in males than females in ratio 5:1.
L 4 Carcinoma of the larynx Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%. Incidence: It is more common in males than females in ratio 5:1.
The following images were all acquired using a CTI Biograph
 Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Anterior triangle of neck
 Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
Lecture 01. The Thyroid & Parathyroid Glands. By: Dr Farooq Khan PMC Date: 12 th March. 2018
 Lecture 01 The Thyroid & Parathyroid Glands By: Dr Farooq Khan PMC Date: 12 th March. 2018 INTRODUCTION LAYERS OF THE NECK The neck has four major compartments or layer which are enclosed by an outer musculofascial
Lecture 01 The Thyroid & Parathyroid Glands By: Dr Farooq Khan PMC Date: 12 th March. 2018 INTRODUCTION LAYERS OF THE NECK The neck has four major compartments or layer which are enclosed by an outer musculofascial
Alexander C Vlantis. Selective Neck Dissection 33
 05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
Early Glottic Cancer
 Early Glottic Cancer Mark S. Courey, MD Professor, UCSF Department of OHNS Director, Division of Laryngology Definition High-grade grade dysplasia Carcinoma in situ Micro-invasive invasive carcinoma Invasive
Early Glottic Cancer Mark S. Courey, MD Professor, UCSF Department of OHNS Director, Division of Laryngology Definition High-grade grade dysplasia Carcinoma in situ Micro-invasive invasive carcinoma Invasive
Hyoid Bone. Lower Airway. Aspiration. Larynx. Cartilages of the Larynx. Larynx Tracheobronchial Tree (TB Tree) Trachea Bronchi Bronchioles
 Trachea Bronchi Bronchioles") Lower Airway Larynx Tracheobronchial Tree (TB Tree) Trachea Bronchi Bronchioles Respiratory Terminal Hyoid Bone Not part of the larynx. The Hyoid bone is an anchor for the anterior muscles of the neck
Lower Airway Larynx Tracheobronchial Tree (TB Tree) Trachea Bronchi Bronchioles Respiratory Terminal Hyoid Bone Not part of the larynx. The Hyoid bone is an anchor for the anterior muscles of the neck
Dr. Aruna kommineni 3 rd year PG Dept. Of E.N.T.
 Dr. Aruna kommineni 3 rd year PG Dept. Of E.N.T. Name : XXX Age: 35 yrs Sex : female Occupation : Agricultural labour Date of admission: 03/02/2017 Patient had presented to the OPD with complaints of hoarse
Dr. Aruna kommineni 3 rd year PG Dept. Of E.N.T. Name : XXX Age: 35 yrs Sex : female Occupation : Agricultural labour Date of admission: 03/02/2017 Patient had presented to the OPD with complaints of hoarse
Modified frontolateral partial laryngectomy operation: combined muscle-pedicle hyoid bone and thyrohyoid membrane flap in laryngeal reconstruction
 Cancer Biol Med 2013;10:103-109. doi: 10.7497/j.issn.2095-3941.2013.02.007 ORIGINAL ARTICLE Modified frontolateral partial laryngectomy operation: combined muscle-pedicle hyoid bone and thyrohyoid flap
Cancer Biol Med 2013;10:103-109. doi: 10.7497/j.issn.2095-3941.2013.02.007 ORIGINAL ARTICLE Modified frontolateral partial laryngectomy operation: combined muscle-pedicle hyoid bone and thyrohyoid flap
STEP 1 INCISION AND ELEVATION OF SKIN FLAP STEP 3 SEPARATE PAROTID GLAND FROM SCM STEP 2 IDENTIFICATON OF GREAT AURICULAR NERVE
 STEP 1 INCISION AND ELEVATION OF SKIN FLAP Create a modified Blair Figure 1 or facelift incision. Figure 2 Raise a superficial cervico-fascial flap between the Superficial Musculo Aponeurotic System (SMAS)
STEP 1 INCISION AND ELEVATION OF SKIN FLAP Create a modified Blair Figure 1 or facelift incision. Figure 2 Raise a superficial cervico-fascial flap between the Superficial Musculo Aponeurotic System (SMAS)
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no
 67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
1. Thyroxine (inactive form) also called T4 (90% of the secretion). 2. Triiodothyronine (active form) also called T3 (10% of the secretion).
 also called T4 (90% of the secretion). 2. Triiodothyronine (active form) also called T3 (10% of the secretion).") A Introduction The nomenclature of the thyroid gland comes from its close relation to the thyroid cartilage (the thyroid cartilage was named like this because thyroid means shield and it is shielding the
A Introduction The nomenclature of the thyroid gland comes from its close relation to the thyroid cartilage (the thyroid cartilage was named like this because thyroid means shield and it is shielding the
Transoral Laser Microsurgery in Carcinomas of the Oral Cavity, Pharynx, and Larynx
 The indications and approach using CO 2 laser surgery in carcinomas of the upper aerodigestive tract are reviewed. Lu Jian Jun. The Dulcimer, 2000. Oil on canvas, 36 48. Courtesy of Weinstein Gallery,
The indications and approach using CO 2 laser surgery in carcinomas of the upper aerodigestive tract are reviewed. Lu Jian Jun. The Dulcimer, 2000. Oil on canvas, 36 48. Courtesy of Weinstein Gallery,
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
(loco-regional disease)
") (loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
(loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
Respiratory System. Cambridge University Press Concise Anatomy for Anaesthesia Andreas G. Erdmann Excerpt More information
 Respiratory System 1 The mouth DESCRIPTION The mouth extends from the lips (anterior) to the isthmus of the fauces (posterior). There are two sections: Vestibule slit-like cavity between the cheeks/lips
Respiratory System 1 The mouth DESCRIPTION The mouth extends from the lips (anterior) to the isthmus of the fauces (posterior). There are two sections: Vestibule slit-like cavity between the cheeks/lips
Respiratory System. Clinical notes. Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz)
") Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz) Respiratory System The test of the respiratory system follows the general rules for written tests (see Continuous
Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz) Respiratory System The test of the respiratory system follows the general rules for written tests (see Continuous
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
CO 2 LASER SURGERY IN THE TREATMENT OF GLOTTIC CANCER
 CO 2 LASER SURGERY IN THE TREATMENT OF GLOTTIC CANCER Giovanni Motta, MD, 1 Erik Esposito, MD, 2 Sergio Motta, MD, 1 Gianpaolo Tartaro, MD, 3 Domenico Testa, MD 1 1 Institute of Otorhinolaryngology, Ateneo
CO 2 LASER SURGERY IN THE TREATMENT OF GLOTTIC CANCER Giovanni Motta, MD, 1 Erik Esposito, MD, 2 Sergio Motta, MD, 1 Gianpaolo Tartaro, MD, 3 Domenico Testa, MD 1 1 Institute of Otorhinolaryngology, Ateneo
Airway Anatomy. Soft palate. Hard palate. Nasopharynx. Tongue. Oropharynx. Hypopharynx. Thyroid cartilage
 Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
A retrospective review in the management of T3 laryngeal squamous cell carcinoma: an expanding indication for transoral laser microsurgery
 Butler et al. Journal of Otolaryngology - Head and Neck Surgery (2016) 45:34 DOI 10.1186/s40463-016-0147-1 ORIGINAL RESEARCH ARTICLE Open Access A retrospective review in the management of T3 laryngeal
Butler et al. Journal of Otolaryngology - Head and Neck Surgery (2016) 45:34 DOI 10.1186/s40463-016-0147-1 ORIGINAL RESEARCH ARTICLE Open Access A retrospective review in the management of T3 laryngeal
ORIGINAL ARTICLE. Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx
 ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
Assessing The Survival And Functional Outcomes Of Patients With Supraglottic Squamous Cell Carcinoma
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2014 Assessing The Survival And Functional Outcomes Of Patients
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2014 Assessing The Survival And Functional Outcomes Of Patients
Department of Otolaryngology, Kurume University School of Medicine, Kurume, Japan
 THE KURUME MEDICAL JOURNAL Vol. 16, No. 3, 1969 PATHOLOGICAL STUDIES RELATING TO NEOPLASMS OF THE HYPOPHARYNX AND THE CERVICAL ESOPHAGUS IKUICHIRO HIROTO, YASUSHI NOMURA, KUSUO SUEYOSHI, SHIGENOBU MITSUHASHI,
THE KURUME MEDICAL JOURNAL Vol. 16, No. 3, 1969 PATHOLOGICAL STUDIES RELATING TO NEOPLASMS OF THE HYPOPHARYNX AND THE CERVICAL ESOPHAGUS IKUICHIRO HIROTO, YASUSHI NOMURA, KUSUO SUEYOSHI, SHIGENOBU MITSUHASHI,
Respiratory System. Ling Shucai
 Respiratory System Ling Shucai General Description Ⅰ. Constituents: Respiratory tract Lungs Pleura and plural cavity Ⅱ. Function: exchange O 2 and CO 2 mainly Mediastinum Respiratory tract Upper respiratory
Respiratory System Ling Shucai General Description Ⅰ. Constituents: Respiratory tract Lungs Pleura and plural cavity Ⅱ. Function: exchange O 2 and CO 2 mainly Mediastinum Respiratory tract Upper respiratory