9/6/2016 DISCLOSURES. None to disclose. The Present WHERE WE ARE NOW?
|
|
|
- Reginald Horn
- 5 years ago
- Views:
Transcription
1 9/6/2016 SESSION #3000 CHANGING PARADIGMS IN THE DIAGNOSIS OF ENCAPSULATED FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA DELIBERATIONS, DISCUSSIONS AND CONTROVERSIES. Virginia A. LiVolsi, Raja R. Seethala & Zubair W. Baloch. DISCLOSURES None to disclose WHERE WE ARE NOW? The Present 1
 - Selection of Thyroid Nodules for Sampling US Features Maximal Diameter, cm FNA Requested % Respondents Meets 2015 ATA Criteria for FNA Hypoechoic with microcalcifications 0.7 67.")
2 9/6/2016 Fig. 1 Thyroid Nodule Management Paradigm Otolaryngologic Clinics of North America , DOI: ( /j.otc ) - Selection of Thyroid Nodules for Sampling US Features Maximal Diameter, cm FNA Requested % Respondents Meets 2015 ATA Criteria for FNA Hypoechoic with microcalcifications No Solid, isoechoic No Complex cystic No Solid, hypoechoic Yes Spongiform No Pure cyst No Thyroid FNA Bethesda Classification Scheme The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC): Implied Risk of Malignancy and Recommended Clinical Management Diagnostic Category Non-diagnostic or Unsatisfactory Risk of Malignancy (%) Usual Management Repeat FNA with ultrasound guidance Benign 0-3% Clinical follow-up Atypia of Undetermined Significance or Follicular Lesion of Undetermined Significance (AUS/FLUS) ~ 5-15% Repeat FNA Follicular Neoplasm or Suspicious for a Follicular Neoplasm (Specify if Hurthle type or Oncocytic) 15-30% Surgical lobectomy Suspicious for Malignancy 60-75% Near-total thyroidectomy or surgical lobectomy Malignant 97-99% Near-total thyroidectomy 2




3 9/6/2016 Monotonous cells, Microfollicles, Nuclear overlapping & Crowding Colloid Watery Susp Malig Malignant Nuclear Atypia Benign AUS/FLUS Foll Neop Susp Malig Malignant Follicular Cells Colloid Watery Nuclear Atypia Benign AUS/FLUS Foll Neop Susp Malig Malignant Follicular Cells Management of patients found to have an indeterminate or malignant result on initial FNA Published in: Henry B. Burch; Kenneth D. Burman; David S. Cooper; James V. Hennessey; Nicole O. Vietor; The Journal of Clinical Endocrinology & Metabolism 2016, 101,
4 9/6/2016 Growing Body of Literature Showing Inconsistencies in Surgical Pathology Diagnosis of Thyroid Cancer Among Experts Encapsulated Follicular Variant The Cytology Gold Standard is not so Gold Follow up Clinicopathologic Studies Showing Over diagnosis and Overtreatment of Thyroid Carcinoma PTC. Concept of Low and High Risk Disease TBSRTC Clinical and Radiology Guidelines American & European Thyroid Association American College of Radiology American Society of Radiologist in Ultrasound Molecular Profiling of Thyroid Tumors Molecular Diagnosis of Thyroid Nodules Diagnostic Tests with high Negative and Positive Predictive Value Encapsulated / Well Demarcated Follicular Patterned Lesions Follicular Adenoma Non Invasive NIFTP Well Demarcated Solid and cystic Usually mixed follicular growth pattern Isolated papillae comprising <1% of tumor mass Nuclear Features of PTC Absent Nuclear Features of PTC Present Follicular Carcinoma Invasive (Tumor Capsule & Vascular Invasion) FVPTC Invasive (Tumor Capsule & Vascular Invasion) POTENTIAL Ethical issues ISSUES & WITH Legal NIFTP implications DIAGNOSIS Should we reclassify cases diagnosed in the past as Encapsulated FVPTC to NIFTP? NO Standard of care Past vs. Present 4



5 9/6/2016 Potential Issues with NIFTP Diagnosis Cytopathology Diagnosis Based on Nuclear Morphology Increase in the number of False Positive diagnosis? 1. NIFTP is a Surgical Disease 2. Diagnosis based upon application of strict diagnostic criteria **Noninvasive nature has to be documented based on adequate sampling of tumor periphery and capsule Potential Issues with NIFTP Diagnosis Cytopathology Diagnosis Increase in the number of False Positive diagnosis? Too early to tell Most Encapsulated FVPTC are Classified as: Follicular Neoplasm / Suspicious for Follicular Neoplasm Or Suspicious for Papillary Carcinoma Cytology Dx: Suspicious for PTC, Surg Path NIFTP 5
 *Adequate sampling of entire tumor capsule is required to establish this diagnosis Changes in the Implied Risk of Malignancy for TBSRTC Categories AUS/FLUS Suspicious for Follicular")
 Institutional Data Showing TBSRTC Diagnostic Categories, Surgical Follow-Up, Risk Of Malignancy With and Without Cases of Non-Invasive Follicular Variant of Papillary")
6 9/6/2016 Cytology Dx: Follicular Neoplasm, Gene Expression Classifier Suspicious, Surg Path NIFTP New Terminology Recommendation Non invasive follicular thyroid neoplasm with papillary like nuclear features (NIFTP) *Adequate sampling of entire tumor capsule is required to establish this diagnosis Changes in the Implied Risk of Malignancy for TBSRTC Categories AUS/FLUS Suspicious for Follicular Neoplasm Suspicious for Malignancy 50% decrease (Strickland et al. Thyroid 2015 & Faquin et al. Cancer Cytopathology 2015) Institutional Data Showing TBSRTC Diagnostic Categories, Surgical Follow-Up, Risk Of Malignancy With and Without Cases of Non-Invasive Follicular Variant of Papillary Thyroid Carcinoma (NI-FVPTC) Faquin et al. Cancer Cytopathology 2015 Institution A Institution B Institution C Institution D Institution E TBSRTC Diagnoses ND Benign AUS/FLUS FN/SFN SM Malignant Surgical FU Benign Surgical FU Malignant Surgical FU No Surgery Total NI FVPTC Risk of Malignancy for all TBSRTC Categories ROM OROM 40.12% 48.89% 52.13% 44.26% 31.91% 14.32% 11.23% 19.67% 7.50% 7.58% ROM excluding NI FVPTC Cases 20.93% 30.56% 47.50% 36.30% 27.66% OROM excluding NI FVPTC Cases 7.47% 7.02% 17.92% 6.15% 6.57% % Decrease in Risk of Malignancyfor all TBSRTC Categories 18.33% 4.63% 7.96% ROM excluding NI FVPTC Cases 19.19% 4.26% OROM excluding NI FVPTC Cases 6.85% 4.21% 1.75% 1.35% 1.01% 6
 TBSRTC Diagnostic Categories ND Benign AUS/FLUS FN/SFN SM Malignant Total number of FNABs, n=6943 406 (5.8%) 4221 (60.8%) 1028 (14.8%) 463 (6.6%) 238 (3.4%) 587 (8.")


7 9/6/2016 Combined Institutional Data Showing TBSRTC Diagnostic Categories, Surgical Follow-Up, Risk Of Malignancy With and Without Cases of Non-Invasive Follicular Variant of Papillary Thyroid Carcinoma (NI-FVPTC) TBSRTC Diagnostic Categories ND Benign AUS/FLUS FN/SFN SM Malignant Total number of FNABs, n= (5.8%) 4221 (60.8%) 1028 (14.8%) 463 (6.6%) 238 (3.4%) 587 (8.4%) Surgical FU Benign Surgical FU, n= Malignant Surgical FU, n= Total PTC, n=756 Total NI FVPTC, n= Risk of Malignancy ROM 25.3% 9.3% 31.2% 33.2% 82.6% 99.1% OROM 4.4% 0.9% 12.0% 21.8% 62.1% 75.9% ROM excluding NI FVPTC Cases 23.9% 5.8% 17.6% 18.0% 59.2% 95.7% **p value OROM excluding NI FVPTC Cases 4.1% 0.5% 6.8% 11.8% 44.5% 73.4% **p Value % Decrease in Risk of Malignancy ROM excluding NI FVPTC Cases 1.4% 3.5% 13.6% 15.1% 23.4% 3.3% OROM excluding NI FVPTC Cases 0.2% 0.3% 5.2% 9.9% 17.6% 2.5% Cytologic Features and Molecular Alterations in a Cohort of 39 NFVPTCs and cptcs. Brooke E. Howitt et al. Am J Clin Pathol 2015;144: Copyright by the American Society for Clinical Pathology Maletta, F. et.al. Cytological features of non invasive follicular thyroid neoplasm withpapillary like nuclear features and their correlation with tumor histology. Hum Pathol

8 9/6/2016 Thyroid Nodule Management Paradigms Aka Personalized Approach Clinical Presentation + Ultrasound + FNA Diagnosis + Molecular Testing MOLECULAR TESTS vs. Clinical Application & Practice Sensitivity and specificity are characteristics of the test. The population does not affect the results. The relevant questions for the clinician and patient What is the chance that a person with a positive test truly has the disease? What is the chance that a person with a negative test result is disease free? Positive and negative predictive values are influenced by the prevalence of disease in the population being tested. 8
9 9/6/2016 Test: 90% sensitivity and 90% specificity Example 1: 20% of population has cancer PPV TP/all positive results= 18/26 = 69% NPV TN/all negative results=72/74 = 97% Example 2: 70% of population has cancer PPV TP/all positive results= 63/66 = 95% NPV TN/all negative results= 27/34 = 79% NPV Decreases as Cancer Prevalence Rises TEST A Sens 90% Spec 50% 100 TEST B Sens 60% Spec 95% NPV (%) Prevalence of Cancer (%) NPV & PPV for Afirma GEC for FLUS, FN based upon N Engl J Med :206 NPV NPV 94% 38% PPV Prevalence of malignancy NEJM paper PPV 9
 130 85(65%) 45(35%) (11 cases 24%) Integrated Genomic Characterization of Papillary Thyroid Carcinoma.")

10 9/6/2016 Afirma and NIFTP Follow up Study Suspicious by Afirma Nodules wsurgery Benign Malignant (NIFTP) Wong et al (Thyroid 2016) 63 41(65%) 22(35%) (14 cases 88%) Samulski et al (Diag Cytopath 2016) (65%) 45(35%) (11 cases 24%) Integrated Genomic Characterization of Papillary Thyroid Carcinoma. Cell (2014) Classic PTC Encapsulated FVPTC Foll Thyr CA Poorly Diff Thy Anapl Thyr CA Foll CA Adenoma MUTATIONS BRAF V600E BRAF K601E NRAS HRAS KRAS PTEN + ++ TSHR + ++ GNAS ++ GENE FUSIONS RET/PTC +++ PAX8/PPARG ALK fusions BRAF fusions + ETV6/NTRK3 ++ NTRK1 fusion ++ NexGen additions Using NexGen sequencing UPMC developed custom panel ThyroSeq ver2 TM Point mutations in 14 genes (BRAF, NRAS, KRAS, HRAS, AKT1, PTEN, TP53, TSHR, GNAS, CTNNB1, RET, PIK3CA, TERT, EIF1AX) 38 gene fusions (RET, PPAR, NTRK1, NTRK3k, ALK, THADA,BRAF) Therefore >60 genetic markers Nikiforov Cancer 2014;120:3627; Nikiforov Thyroid epub Sept
11 9/6/2016 THE FUTURE Conclusions Still Need More Data to Provide Opinions CONCLUSIONS? NIFTP Beneficial to patients Stricter set of exclusion criteria Grossing of encapsulated or well demarcated nodule Initial pathologic approach to diagnose and manage low-risk thyroid neoplasms. WHAT TO EXPECT TOO EARLY TO TELL NIFTP IS A SURGICAL DISEASE Change in the malignancy risk for Bethesda Classification categories especially suspicious for PTC 50-60%. Should the suspicious category be divided? Suspicious for malignancy & PTC? Change in the malignancy risk for AUS/FLUS & Follicular Neoplasm / Suspicious for Follicular Neoplasm 11
?")
12 9/6/2016 WHAT CRITERIA I SHOULD USE TO DIAGNOSE CONSISTENT WITH PTC? Before Opinions? Consider sampling issues, ultrasound features and disease presentation True papillae presence of fibrovascular core(s)? Diffuse rather than focal presence of major diagnostic nuclear features of PTC IF RENDERING A DIAGNOSIS OF SUSPICIOUS FOR PTC Suspicious for papillary thyroid carcinoma, see note. Note: The specimen shows a distinct population of atypical follicular cells with nuclear features suspicious but not diagnostic of papillary thyroid carcinoma. According to the published data 50-75% of thyroid FNA cases diagnosed as such are found to be malignant on surgical excision The histologic follow-up of thyroid FNA cases diagnosed as such can include one of the following entities: papillary thyroid carcinoma and non-invasive follicular tumor with papillary like nuclei (NIFTP). Molecular Analysis Which test Mutation and Translocation Panel 12

13 Virginia A. LiVolsi, MD Perelmann School of Medicine of the University of Pennsylvania I have consulted with Veracyte, Inc.
14 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE Prior to 1970s, the definition of Papillary vs Follicular Thyroid Carcinoma Rested on the predominant (>50%) pattern of the tumor at low power. Hence if tumor was mostly follicular in pattern, it was diagnosed as follicular carcinoma (AFIP FASCICLE 1969)
15 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE In 1960s, Dr. Stuart Lindsay defined the follicular variant of papillary carcinoma looking to the nuclei. The seminal paper in 1977 by Chen and Rosai described 7 cases of follicular variant of PTC based on nuclear features.
16 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE Cytopathologists liked this idea and the diagnosis of PTC could be made on FNA material The WHO (2004) defined PTC as a malignant tumor of the thyroid with a distinctive set of nuclear features. The WHO defined FTC as not having those nuclear features.


17
18
19 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE So in a span of two decades, pathologists changed their diagnostic emphasis from pattern to nuclear cytology. Papillary carcinoma whether it had papillae or how many it had was recognized by its nuclei and even if the entire tumor was follicular in pattern, if the nuclei were present it was a papillary carcinoma.
20 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE This had important clinical relevance Papillary carcinoma tended to show lymphatic spread (both in the gland and into lymph nodes) and was often multifocal; Whereas follicular carcinoma was unifocal and hardly ever spread to nodes; if it spread it went hematogenously to distant sites.
21 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE The follicular variant was therefore expected to behave as a papillary carcinoma. And some of them did!

22
23 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE BUT, The fly in the ointment landed when pathologists noted some tumors which grew like follicular carcinoma (encapsulated, pushing invasion, vascular invasion) YET had nuclei of papillary carcinoma.

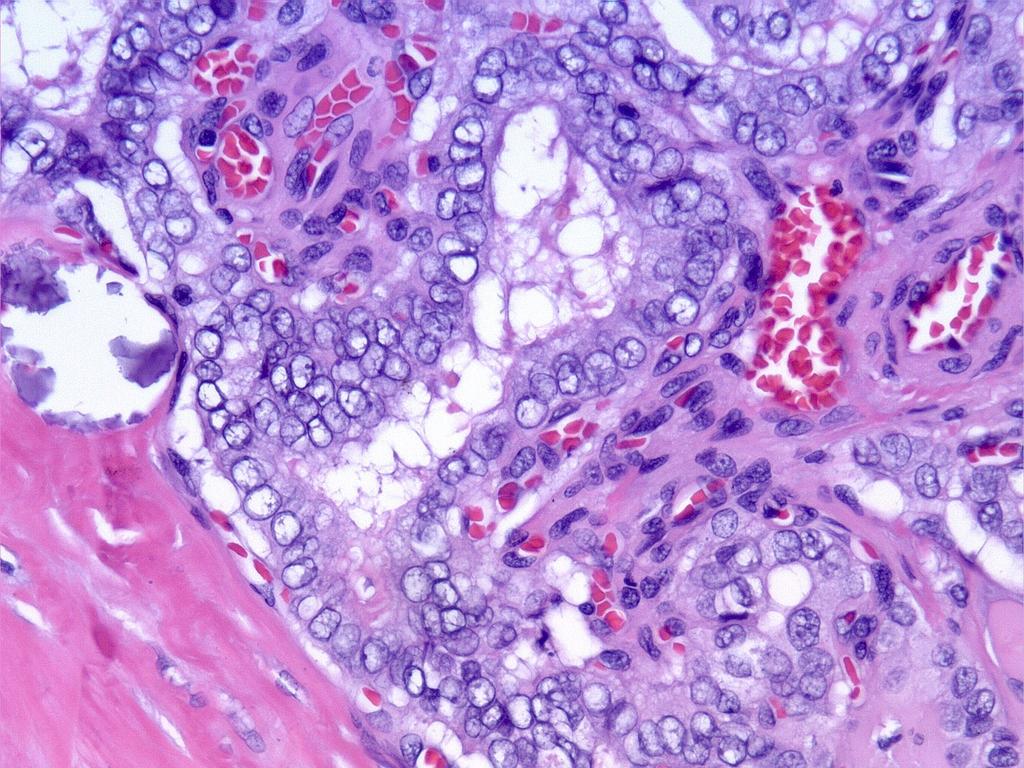
24 INVASION CAPSULE VASCULAR INVASION

25 CD 31 stain

26

27 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE In the first decade of the 21 st century, two major forms of follicular variant of papillary carcinoma were recognized: Infiltrative --behave like ordinary papillary carcinoma; Encapsulated less (??any) nodal mets, unifocality, more vascular invasion and probably distant mets.
28 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE Then things got interesting Subvariants of FVPTC Infiltrative Encapsulated with invasion Encapsulated without invasion Encapsulated with multifocal nuclear features Encapsulated with incomplete nuclear featues Microcarcinoma in an adenoma Diffuse follicular variant Macrofollicular variant
29 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE Could we make sense out of this? MAYBE molecular analysis could help. And it clarified some of the confusion The infiltrative FVPTC shared much with classic PTC The encapsulated FVPTC seemed to be more closely related to FTC/FA.
30 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE What could most pathologists do? Agree that if a tumor with a follicular pattern showed invasive growth infiltrative into the gland without capsule IT IS A CANCER. The subtype is often in dispute.

31

32
33 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE NONINVASIVE tumors. How common are they? This is difficult to determine since diagnostic criteria differ. It is estimated that about 45,000 or 50,000 cases are seen per year in North America.
34 FOLLICULAR VARIANT OF PTC: HISTORICAL PERSPECTIVE The main problem is the NONINVASIVE tumors. WHAT TO NAME THEM? HOW TO DEFINE THEM?
35 FOLLICULAR VARIANT OF PAPILLARY CARCINOMA ENCAPSULATED NONINVASIVE HISTORICAL CLUES Williams et al UMP Liu et al behave benign Kakudo et al not malignant OTHERS----suggested benign behavior.
36 SO THE IDEA TO EVALUATE THESE LESIONS IN AN ORDERLY SCIENTIFIC WAY
37 Changing Paradigms in the Diagnosis of Non-Invasive Follicular Variant of Papillary Thyroid Carcinoma: Deliberations, Discussions and Controversies ENTER NIFTP:DIAGNOSTIC AND MOLECULAR FEATURES Raja R. Seethala, M.D. University of Pittsburgh Medical Center I have no financial disclosures
38 NON-INVASIVE FOLLICULAR THYROID NEOPLASM WITH PAPILLARY LIKE NUCLEAR FEATURES (NIFTP) Inception Pathologic features of NIFTP Limitations and Challenges
39 The problem - Non invasive FVPTC Malignancy based on only nuclear features - subtle and subjective Treated like other well differentiated cancers Discordance between subtlety and perceived penalty for being incorrect
40 Indolent behavior to match the appearance Reference Follow-up Type and number of FVPTC cases Baloch Z, et al. Encapsulated Mod Pathol 2000 N=5 Liu J, et al. Cancer 2006 Widder S, et al. Surgery 2008 Piana S, et al. AJSP 2010 Liu Z, et al. Cancer science 2011 Median, 11.1 y Mean 8.75 y Mean 11.9 y Average 6.75 y Encapsulated N=61 Infiltrative N=17 Encapsulated N=26 Encapsulated N=66 Encapsulated\ N=30 Invasion Lymph node metastasis Recurrence/distant metastasis Tumor-related death 1 without invasion All 5-bone metastases 1- capsular invasion 3- vascular invasion Without invasion N=43 With invasion 3 (17%) 1/18 (6%) 0 N=18 11 (65%) 11 (65%) Without invasion N=26 Without invasion N=45 Without invasion N= Vivero M, et al. Thyroid 2013 Rosario PW, et al. Clinical endocrinology 2014 Median, 9.25 y Median 6 y Encapsulated N=27 Partially encapsulated/well circumscribed N=35 Without invasion N=14 With invasion N=13 Without invasion N= /30 Infiltrative N=9 7 (78%) Encapsulated Without invasion N=57 N=57 Howitt BE, et al. Histopathology 2015 Median 3 y Encapsulated N=79 Without invasion N = Ganly I, et al. Human Pathology 2015 Median 9.5 y Encapsulated N= 83 Without invasion N= 57 With invasion N= ~0.5% non invasive FVPTC have recurrence or metastasis (range of median f/u 3 to 11.9 years). Recurrent metastatic cases w/o invasion with extenuating circumstances (incomplete lesional capsule submission, incomplete excision)?overtreatment or overdiagnosis
41 Consensus group to address the problem 24 surgical pathologists, 2 endocrinologists, 1 surgeon, 1 molecular pathologist, 1 biostatistician, 1 psychiatrist, 1 patient Led by Dr. Yuri Nikiforov Review of 268 cases with f/u Numerous teleconferences and a face to face meeting in Boston 3/20-3/21/2015 Heated discussion regarding nomenclature shift
42 Summary of the Consensus Group Proceedings Inclusion and exclusion criteria were established for non-invasive FVPTC Nuclear scoring scheme was devised and validated 109 cases accepted as non-invasive FVPTC no adverse outcomes (median f/u 13 years) 101 cases designated as encapsulated/well demarcated FVPTC with invasion 12% with adverse outcome, 2% death Final consensus terminology Non Invasive Follicular Thyroid Neoplasm with Papillary Like Nuclear Features (NIFTP) Nomenclature Revision for Encapsulated Follicular Variant of Papillary Thyroid Carcinoma: A Paradigm Shift to Reduce Overtreatment of Indolent Tumors. Nikiforov YE et al., JAMA Oncol Apr 14. doi: /jamaoncol [Epub ahead of print]
43 Aftermath Accepted as an entity by upcoming WHO Will have its own provisional ICD-O3 histology code: 8349/1 CAP protocol modifications to accommodate NIFTP underway Endorsed by several organizations (though not yet ATA)
44 Diagnosis of NIFTP Abridged Anything that you would have called encapsulated/well demarcated/noninvasive FVPTC, now consider NIFTP BUT. You must be stricter in excluding invasion, other growth patterns, and morphologies Complete submission of tumor normal interface is no longer optional (get over it) NIFTP nuclear features are usually subtle, if it s too easy to find these, then you should worry about a more aggressive carcinoma.
45 Inclusion Criteria Border Non infiltrative Encapsulated Partly Encapsulated Well Demarcated Follicular Patterned Micro to macrofollicular/cystic Intercalation of microfollicles between macrofollicles Accentuation of cellularity at periphery Nuclear features of PTC Diffuse to heterogeneous (recommend a minimum of 30% of tumor) Typically not as obvious as classic/conventional PTC
46 Exclusion Criteria Invasion Encapsulated tumors tumoral capsular invasion Unencapsulated/well demarcated tumors infiltration of adjacent parenchyma Vascular, lymphatic invasion Perineural invasion, extrathyroidal extension Growth pattern Solid/trabecular/insular growth >30% True or well formed papillae >1% Aggressive morphologies (i.e. tall cell, columnar cell, hobnail) Distinctive morphologies (i.e. cribriform morular variant) Psammoma bodies High grade features Mitoses >3 per 10 hpf Tumor necrosis

 No P Follicular adenoma and/or adenomatoid")
47 ALGORITHM FOR DIAGNOSIS OF NIFTP Encapsulated or Well-demarcated Yes No N Infiltrative FVPTC Capsular and/or Lymphovascular invasion No >30% solid/insular/trabecular and/or >1% true papillary pattern and/or Psammoma bodies identified and/or Tall cell or columnar cell variants No Predominantly follicular pattern Yes Tumor necrosis and/or >3 mitoses/10 HPFs No Yes Yes No Yes O T N I F T EFVPTC or FC with invasion Solid PTC and/or Classical PTC and/or Tall cell or columnar cell variants Classical PTC encapsulated and/or Follicular adenoma Poorly differentiated tumor Nuclear features of papillary thyroid carcinoma (score 2 or 3) No P Follicular adenoma and/or adenomatoid nodule Yes NIFTP
48 Nuclear Features Still defining in NIFTP Main point of contention Poor to mediocre reproducibility and geographic variation
49 A scoring system capturing what you would do anyway Nuclear features Enlargement Elongation Overlap Grooves, Irregular nuclear contours Pseudoinclusions Glassy nuclei Margination of chromatin (and nucleoli) Clearing Restructuring Size and Shape (0-1 pt) Enlargement Elongation Overlap Membrane Irregularities (0-1 pt) Irregular nuclear contours Grooves Pseudoinclusions Chromatin Characteristics (0-1 pt) Glassy nuclei Margination of chromatin (and nucleoli) Clearing If combined score of 2 or 3: Nuclear features are adequate for NIFTP
")
")








50 Score 0 (insufficient) Score 1 (adequate) Size and Shape Enlargement Elongation Overlap Normalize to normal Careful here Membrane Irregularities Irregular nuclear contours Grooves Pseudoinclusions Chromatin Characteristics Glassy nuclei Margination of chromatin (and nucleoli) Clearing
51 Performance Characteristics with a Molecular Endpoint Test Set Sensitivity = 86.5% (82.7% %) Specificity = 80.8% (73.8% %) PPV = 92.2% (89.1% %) NPV = 69.8% (62.2% %) Classification Accuracy = 85.0% (82.8% %) Validation Set Sensitivity % (96.3% %) Specificity % (86.0% %) PPV % (87.1% %) NPV % (96.0% %) Classification Accuracy 94.3% (92.1% %)
52 Molecular alterations in NIFTP ~60% overall with clonal alterations (n=44 tested) ~80% cases classified as NIFTP (by mean score 2 or more) show clonal alterations 12/26 RAS +/- EIF1AX 7/26 PAX8/PPARG 5/26 THADA 1/26 ALK 1/26 BRAF K601E No BRAF V600E, RET/PTC in NIFTP Cases not considered NIFTP because of insufficient nuclear score were negative for mutation Integrated genomic characterization of papillary thyroid carcinoma. Cancer Genome Atlas Research Network. Cell Oct 23;159(3):676-90
53 FAQ about molecular phenotype Do you use molecular findings to diagnosis NIFTP? NO Does NIFTP have characteristic findings? YES RAS PAX8-PPARG THADA BRAF K601E What molecular alterations should make you doubt a NIFTP diagnosis? BRAF V600E Conventional Tall Cell spectrum RET/PTC CTNNB1 Cribriform Morular variant Multiple mutations TP53 Progression to poorly differentiated TERT
54 Gross Examination and Reporting Some things are the same, some are different
55 Grossing Entire tumor normal interface (no arguments) Mean NIFTP size ~3 cm = Usually <20 cassettes Stepwise submission acceptable if very large or grossly evident invasion Grossing need to map discrete lesions sampled more methodically
56 Sample Templated Gross The specimen is received fresh, labeled with the patient s name, initials [] and []. SPECIMEN TYPE: [total thyroidectomy] or [R/L subtotal thyroidectomy/lobectomy/lobectomy with isthmusectomy/other(specify] SPECIMEN INTEGRITY: [intact/disrupted/fragmented],[suture demarcating ] WEIGHT: [] grams OVERALL DIMENSIONS: [] x [] x [] cm right lobe: [] x [] x [] cm left lobe: [] x [] x [] cm isthmus: [] x [] x [] cm other(specify):[lymph nodes, parathyroid, skeletal muscle, skin] [] x [] x [] cm NUMBER OF DISCRETE LESIONS [] LESION #[]:* Location: [left/right/isthmus], [upper/middle/lower] Size: [] x [] x [] cm Border: [well demarcated +/- encapsulated, poorly defined] Capsular thickness: [](if >0.1 cm) Characteristics: [shape and color], [homogeneous/heterogeneous], [hemorrhagic/cystic/calcified] Distance to inked margin: [] cm SURROUNDING UNINVOLVED PARENCHYMA: []. OTHER FINDINGS: [] ADDITIONAL STUDIES/PROCEDURES: [] INK CODE: Black Thyroid capsule Green Isthmic/resection margin Red Area banked CASSETTE SUMMARY: *add up to 6 as needed.
57 Reporting: A work in progress AJCC stage no longer relevant Relevant parameters Size Laterality Margin status CAP Synoptic??? Likely an OPTIONAL limited dataset still important for possible population level data accumulation in registries
58 Limitations and Challenges A starting point not a final solution
59 This does not solve a more fundamental problem NIFTP does not solve the underlying problem of dumbing down neoplasia into binary categories in cancer care ATA 2015 Guidelines A spectrum not discrete groupings
60 Does not solve all diagnostic challenges of follicular patterned lesions Pros Cushion category between benign and overtly malignant Systematic approach to assess nuclear features Cons Nuclear features were scrutinized but other features (infiltration, vascular invasion, papillae, etc) were not Still lots of room for subjectivety Shift in the challenge and controversy Then Nuclear features Now Other features that were not well vetted
61 Specific issue: Mitoses Most problematic feature in UPMC experience Many follicular patterned neoplasms, benign and malignant may have increased mitotic counts Intent of NIFTP Not to scrutinize to find the absolute worst area Use this as a marker of high grade nuclear features not in isolation Recommendations 10 consecutive 40x fields Away from hemorrhage, cystic change (i.e. FNA tract) Only in cellular microfollicular patterned areas.
62 Other limitations Awkward name (?untranslatable in some languages) Retrospective nature, selection bias Absence of neck dissection to confirm pn0 Limited data on extreme long term follow-up (i.e. 30 years) Scale of hundreds of cases is not population level data
63 NIFTP has not been validated for.. Multiple tumors Small tumors (<1.0 cm) Heavily oncocytic tumors Scoring would fail since it is automatically 2 Molecular endpoints may not work as well Pediatric population
64 In Summary NIFTP has gained traction and has a position in the spectrum of follicular derived thyroid neoplasia Perhaps the first systematic response to the NIH directive from 2013 Histologic criteria are not novel, simply reframed to a new context Diagnosis, reporting, and clinical management are all evolving Start point not endpoint
Let s Make Sense of Present & Predict Future. In Light of Past 1/12/2016
 The New Diagnostic Paradigms in Thyroid Surgical Pathology and Affects on Reporting of Thyroid Fine Needle Aspiration Specimens Deliberations, Criticisms & Discussions Zubair W. Baloch, MD, PhD. Professor
The New Diagnostic Paradigms in Thyroid Surgical Pathology and Affects on Reporting of Thyroid Fine Needle Aspiration Specimens Deliberations, Criticisms & Discussions Zubair W. Baloch, MD, PhD. Professor
ACCME/Disclosures. Questions to Myself? 4/11/2016
 The New Diagnostic Paradigms in Thyroid Surgical Pathology and Affects on Reporting of Thyroid Fine-Needle Aspiration Specimens Deliberations, Criticisms & Discussions Zubair W. Baloch, MD, PhD. Professor
The New Diagnostic Paradigms in Thyroid Surgical Pathology and Affects on Reporting of Thyroid Fine-Needle Aspiration Specimens Deliberations, Criticisms & Discussions Zubair W. Baloch, MD, PhD. Professor
American Society of Cytopathology Companion Society Symposium Uses and Misuses of Ancillary Tests in Cytopathology
 American Society of Cytopathology Companion Society Symposium Uses and Misuses of Ancillary Tests in Cytopathology Zubair W. Baloch. MD, PhD. Professor of Pathology, UPENN Medical Center Perelman School
American Society of Cytopathology Companion Society Symposium Uses and Misuses of Ancillary Tests in Cytopathology Zubair W. Baloch. MD, PhD. Professor of Pathology, UPENN Medical Center Perelman School
Thyroid FNA: Diagnosis, Challenges and Solutions. Disclosures
 Thyroid FNA: Diagnosis, Challenges and Solutions Zubair W. Baloch, MD, PhD None Disclosures 1 Questions to Myself? Where We are Now? The Present 2 Reality Check There is More to How Thyroid Nodules are
Thyroid FNA: Diagnosis, Challenges and Solutions Zubair W. Baloch, MD, PhD None Disclosures 1 Questions to Myself? Where We are Now? The Present 2 Reality Check There is More to How Thyroid Nodules are
THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP
 THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP FOLLICULAR VARIANT OF PAPILLARY CARCINOMA HISTORICAL PERSPECTIVE FOLLICULAR VARIANT OF PAPILLARY CARCINOMA 1960 described by Dr. Stuart Lindsay
THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP FOLLICULAR VARIANT OF PAPILLARY CARCINOMA HISTORICAL PERSPECTIVE FOLLICULAR VARIANT OF PAPILLARY CARCINOMA 1960 described by Dr. Stuart Lindsay
An Alphabet Soup of Thyroid Neoplasms
 Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Dilemmas in Cytopathology and Histopathology
 Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
The Bethesda Indeterminate Categories: An Update to Diagnosis and Molecular Testing
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director, Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital The Bethesda Indeterminate Categories:
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director, Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital The Bethesda Indeterminate Categories:
NIFTP: Histopathology of a Cytological Monkey Wrench. B. Wehrli
 NIFTP: Histopathology of a Cytological Monkey Wrench B. Wehrli Non-Invasive Encapsulated Follicular Variant of Papillary Thyroid Carcinoma Before 2016 Non-Invasive Follicular Thyroid Neoplasm with Papillary-Like
NIFTP: Histopathology of a Cytological Monkey Wrench B. Wehrli Non-Invasive Encapsulated Follicular Variant of Papillary Thyroid Carcinoma Before 2016 Non-Invasive Follicular Thyroid Neoplasm with Papillary-Like
3/27/2017. Disclosure of Relevant Financial Relationships. Each year over 550,000 thyroid FNAs are performed in the U.S.!!! THYROID FNA: THE GOOD NEWS
 Disclosure of Relevant Financial Relationships William C. Faquin, MD, PhD Director, Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital Professor of Pathology Harvard Medical
Disclosure of Relevant Financial Relationships William C. Faquin, MD, PhD Director, Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital Professor of Pathology Harvard Medical
Follicular Derived Thyroid Tumors
 Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
New entities in thyroid pathology: update according to the WHO classification
 New entities in thyroid pathology: update according to the WHO classification R.R. de Krijger, Dept. of Pathology, University Medical Center and Princess Maxima Center, Utrecht, The Netherlands New issues
New entities in thyroid pathology: update according to the WHO classification R.R. de Krijger, Dept. of Pathology, University Medical Center and Princess Maxima Center, Utrecht, The Netherlands New issues
NIFTP Cytologic Aspects
 NIFTP Cytologic Aspects William C. Faquin, MD PhD Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Boston, MA USA So, what is the story about FVPTC
NIFTP Cytologic Aspects William C. Faquin, MD PhD Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Boston, MA USA So, what is the story about FVPTC
Building On The Best A Review and Update on Bethesda Thyroid 2017
 Building On The Best A Review and Update on Bethesda Thyroid 2017 Syed Z. Ali, MD, FRCPath, FIAC Professor of Pathology and Radiology The Johns Hopkins Hospital, Baltimore, Maryland USA TBSRTC Diagnostic
Building On The Best A Review and Update on Bethesda Thyroid 2017 Syed Z. Ali, MD, FRCPath, FIAC Professor of Pathology and Radiology The Johns Hopkins Hospital, Baltimore, Maryland USA TBSRTC Diagnostic
3/22/2017. Disclosure of Relevant Financial Relationships. Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC
 Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Disclosure
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Disclosure
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS
 Shamlal Mangray, MB, BS") Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Markers in Thyroid Nodule Evaluation. Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center
 Markers in Thyroid Nodule Evaluation Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center Disclosures Quest Diagnostics (consultant) UPMC/CBLPath
Markers in Thyroid Nodule Evaluation Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center Disclosures Quest Diagnostics (consultant) UPMC/CBLPath
ASC Companion Meeting at the 2017 USCAP: Ancillary Molecular Testing in "Indeterminate. Thyroid Nodules: How Far Have We Come?
 ASC Companion Meeting at the 2017 USCAP: Ancillary Molecular Testing in "Indeterminate Thyroid Nodules: How Far Have We Come? William C. Faquin, MD, PhD, Massachusetts General Hospital, Boston, MA The
ASC Companion Meeting at the 2017 USCAP: Ancillary Molecular Testing in "Indeterminate Thyroid Nodules: How Far Have We Come? William C. Faquin, MD, PhD, Massachusetts General Hospital, Boston, MA The
NIFTP addendum to the RCPath Dataset for thyroid cancer histopathology reports. June 2016
 NIFTP addendum to the RCPath Dataset for thyroid cancer histopathology reports June 2016 Authors: Dr Sarah J Johnson, Royal Victoria Infirmary, Newcastle upon Tyne Professor TJ Stephenson, Sheffield Teaching
NIFTP addendum to the RCPath Dataset for thyroid cancer histopathology reports June 2016 Authors: Dr Sarah J Johnson, Royal Victoria Infirmary, Newcastle upon Tyne Professor TJ Stephenson, Sheffield Teaching
Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease
 Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease Robert L. Ferris, MD, PhD Department of Otolaryngology/Head and Neck Surgery and Yuri E. Nikiforov, MD, PhD Division of
Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease Robert L. Ferris, MD, PhD Department of Otolaryngology/Head and Neck Surgery and Yuri E. Nikiforov, MD, PhD Division of
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
THYROID CYTOLOGY THYROID CYTOLOGY FINE-NEEDLE-ASPIRATION ANCILLARY TESTS IN THYROID FNA
 ANCILLARY TESTS IN THYROID FNA Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular Pathology Unit, IPATIMUP General-Secretary of the International
ANCILLARY TESTS IN THYROID FNA Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular Pathology Unit, IPATIMUP General-Secretary of the International
Molecular Testing for Indeterminate Thyroid Nodules. October 20, 2018
 Molecular Testing for Indeterminate Thyroid Nodules October 20, 2018 Patient 1: Left 1.0 cm AP x 1.6 cm transverse x 2.1 cm in length Well defined Isoechoic heterogeneous No calcification Grade 3 Vascularity
Molecular Testing for Indeterminate Thyroid Nodules October 20, 2018 Patient 1: Left 1.0 cm AP x 1.6 cm transverse x 2.1 cm in length Well defined Isoechoic heterogeneous No calcification Grade 3 Vascularity
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC
 Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Case Study
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Case Study
The Bethesda System for Reporting Thyroid Cytopathology, Laila Khazai 11/4/17
 The Bethesda System for Reporting Thyroid Cytopathology, 2017 Laila Khazai 11/4/17 In Summary No major changes for cytologists. The clinical team is faced with different risk of malignancies (ROM) associated
The Bethesda System for Reporting Thyroid Cytopathology, 2017 Laila Khazai 11/4/17 In Summary No major changes for cytologists. The clinical team is faced with different risk of malignancies (ROM) associated
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
CN 925/15 History. Microscopic Findings
 CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
Non-Invasive Follicular Thyroid Neoplasm with Papillary-like Nuclei (NIFTP)
") Papillary Thyroid Carcinoma: Follicular Variant Encapsulated Type Replaced by: Non-Invasive Follicular Thyroid Neoplasm with Papillary-like Nuclei (NIFTP) Lester D. R. Thompson www.lester-thompson.com
Papillary Thyroid Carcinoma: Follicular Variant Encapsulated Type Replaced by: Non-Invasive Follicular Thyroid Neoplasm with Papillary-like Nuclei (NIFTP) Lester D. R. Thompson www.lester-thompson.com
04/09/2018. Follicular Thyroid Tumors Updates in Classification & Practical Tips. Dissecting Indeterminants. In pursuit of the low grade malignancy
 Follicular Thyroid Tumors Updates in Classification & Practical Tips Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Follicular Thyroid Tumors Updates in Classification & Practical Tips Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
"Atypical": Criteria and
 "Atypical": Criteria and Controversies Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy CASE HISTORY In 2015, 45 y/o woman underwent
"Atypical": Criteria and Controversies Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy CASE HISTORY In 2015, 45 y/o woman underwent
What s an NIFTP? Keeping Up To Date in Thyroid 2018
 What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
Thyroid Nodules. No conflicts. Overview 5/16/2017. UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil
 Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
How to Handle Thyroid FNA
 How to Handle Thyroid FNA Maoxin Wu, MD, PhD Chief of Cytopathology Director of Fine Needle Aspiration (FNA) and Core Biopsy Services Clinical Professor, Department of Pathology Joint appointment, Department
How to Handle Thyroid FNA Maoxin Wu, MD, PhD Chief of Cytopathology Director of Fine Needle Aspiration (FNA) and Core Biopsy Services Clinical Professor, Department of Pathology Joint appointment, Department
The Frozen Section: Diagnostic Challenges and Pitfalls
 The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a single-institutional experience in Japan
 2017, 64 (12), 1149-1155 Original Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a single-institutional experience in Japan Mitsuyoshi Hirokawa 1), Miyoko Higuchi 2), Ayana
2017, 64 (12), 1149-1155 Original Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a single-institutional experience in Japan Mitsuyoshi Hirokawa 1), Miyoko Higuchi 2), Ayana
Thyroid Cytopathology: Weighing In The Bethesda System
 Thyroid Cytopathology: Weighing In The Bethesda System V8 Conflicts No financial consideration Bias Work in the Canadian environment where litigation is less Thyroid cytology is often referred in by small
Thyroid Cytopathology: Weighing In The Bethesda System V8 Conflicts No financial consideration Bias Work in the Canadian environment where litigation is less Thyroid cytology is often referred in by small
Thyroid follicular neoplasms in cytology. Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia
 Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events
 Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Kyle C. Strickland, MD, PhD; Brooke E. Howitt, MD; Justine A. Barletta, MD; Edmund S. Cibas, MD Jeffrey F. Krane, MD, PhD
 Suggesting the Cytologic Diagnosis of Noninvasive Follicular Thyroid Neoplasm With Papillary-Like Nuclear Features (NIFTP): A Retrospective Analysis of Atypical and Suspicious Nodules Kyle C. Strickland,
Suggesting the Cytologic Diagnosis of Noninvasive Follicular Thyroid Neoplasm With Papillary-Like Nuclear Features (NIFTP): A Retrospective Analysis of Atypical and Suspicious Nodules Kyle C. Strickland,
NCI Thyroid FNA State of the Science Conference. The Bethesda System For Reporting Thyroid Cytopathology
 The Bethesda System For Reporting Thyroid Cytopathology Towards a Uniform Terminology With Management Guidelines NCI Thyroid FNA State of the Science Conference Bethesda, MD October 22-23, 2007 154 registrants
The Bethesda System For Reporting Thyroid Cytopathology Towards a Uniform Terminology With Management Guidelines NCI Thyroid FNA State of the Science Conference Bethesda, MD October 22-23, 2007 154 registrants
Correspondence should be addressed to David N. Bimston; Received 23 January 2017; Accepted 20 March 2017; Published 13 April 2017
 Hindawi International Surgical Oncology Volume 2017, Article ID 4689465, 6 pages https://doi.org/10.1155/2017/4689465 Research Article Noninvasive Encapsulated Follicular Variant of Papillary Thyroid Cancer:
Hindawi International Surgical Oncology Volume 2017, Article ID 4689465, 6 pages https://doi.org/10.1155/2017/4689465 Research Article Noninvasive Encapsulated Follicular Variant of Papillary Thyroid Cancer:
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a review for pathologists
 2018 USCAP, Inc All rights reserved 0893-3952/18 $32.00 39 Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a review for pathologists Raja R Seethala, Zubair W Baloch, Justine
2018 USCAP, Inc All rights reserved 0893-3952/18 $32.00 39 Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a review for pathologists Raja R Seethala, Zubair W Baloch, Justine
Dr Catherine Woolnough, Hospital Scientist, Chemical Pathology, Royal Prince Alfred Hospital. NSW Health Pathology University of Sydney
 Dr Catherine Woolnough, Hospital Scientist, Chemical Pathology, Royal Prince Alfred Hospital NSW Health Pathology University of Sydney Thyroid Cancer TC incidence rates in NSW Several subtypes - Papillary
Dr Catherine Woolnough, Hospital Scientist, Chemical Pathology, Royal Prince Alfred Hospital NSW Health Pathology University of Sydney Thyroid Cancer TC incidence rates in NSW Several subtypes - Papillary
Case #1. Ed Stelow, MD University of Virginia
 Case #1 Ed Stelow, MD University of Virginia Imagine, If You Will It s 4:30 on Friday Last cytology case A thyroid FNA from outside that did not have any onsite interpretation It is from a 45-year old
Case #1 Ed Stelow, MD University of Virginia Imagine, If You Will It s 4:30 on Friday Last cytology case A thyroid FNA from outside that did not have any onsite interpretation It is from a 45-year old
Case #1 FNA of nodule in left lobe of thyroid in 67 y.o. woman
 Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
encapsulated thyroid nodule with a follicular architecture and some form of atypia. The problem is when to diagnose
 Histological Spectrum of Papillary Carcinoma of Thyroid A Two Years Study Gomathi Srinivasan 1, M. Vennila 2 1 Associate Professor Pathology, Government Medical College, Omandurar Estate, Chennai 600 002
Histological Spectrum of Papillary Carcinoma of Thyroid A Two Years Study Gomathi Srinivasan 1, M. Vennila 2 1 Associate Professor Pathology, Government Medical College, Omandurar Estate, Chennai 600 002
Improving the Long Term Management of Benign Thyroid Nodules
 25 th Annual Scientific AACE Clinical Congress Improving the Long Term Management of Benign Thyroid Nodules Stephanie L. Lee, MD, PhD Director, Thyroid Health Center Section of Endocrinology, Diabetes
25 th Annual Scientific AACE Clinical Congress Improving the Long Term Management of Benign Thyroid Nodules Stephanie L. Lee, MD, PhD Director, Thyroid Health Center Section of Endocrinology, Diabetes
Supplementary Online Content
 Supplementary Online Content Nikiforov YE, Seethala RR, Tallini G, et al. Nomenclature revision for encapsulated follicular variant of papillary thyroid carcinoma: a paradigm shift to reduce overtreatment
Supplementary Online Content Nikiforov YE, Seethala RR, Tallini G, et al. Nomenclature revision for encapsulated follicular variant of papillary thyroid carcinoma: a paradigm shift to reduce overtreatment
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration
 AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP)
") Page of Accepted Preprint first posted on September 0 as Manuscript ERC--0 Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) Pedro Weslley Rosario, M.D.; Gabriela Franco
Page of Accepted Preprint first posted on September 0 as Manuscript ERC--0 Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) Pedro Weslley Rosario, M.D.; Gabriela Franco
How to Use Molecular Genetic Studies in Endocrine Disease? (in the Management of Well- Differentiated Thyroid Cancer) No Conflicts to Declare
 No Conflicts to Declare") How to Use Molecular Genetic Studies in Endocrine Disease? (in the Management of Well- Differentiated Thyroid Cancer) No Conflicts to Declare Quan-Yang Duh Professor of Surgery University of California,
How to Use Molecular Genetic Studies in Endocrine Disease? (in the Management of Well- Differentiated Thyroid Cancer) No Conflicts to Declare Quan-Yang Duh Professor of Surgery University of California,
Thyroid Nodule Management
 Thyroid Nodule Management Shane O. LeBeau, MD Clinical Associate Professor of Medicine Clinical Lead, Endocrine Thyroid Unit Division of Endocrinology, Diabetes and Metabolism University of Pittsburgh
Thyroid Nodule Management Shane O. LeBeau, MD Clinical Associate Professor of Medicine Clinical Lead, Endocrine Thyroid Unit Division of Endocrinology, Diabetes and Metabolism University of Pittsburgh
Introduction 10/27/2011. Follicular Lesion/Atypia of Undetermined Significance
 Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
CLINICAL MEDICAL POLICY
 Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Molecular Markers for Fine Needle Aspirates of Thyroid Nodules MP-065-MD-DE Medical Management Provider Notice Date: 10/15/2018;
Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Molecular Markers for Fine Needle Aspirates of Thyroid Nodules MP-065-MD-DE Medical Management Provider Notice Date: 10/15/2018;
UPDATE ON THE Bethesda system for reporting thyroid cytology
 UPDATE ON THE Bethesda system for reporting thyroid cytology Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy Present < Current State
UPDATE ON THE Bethesda system for reporting thyroid cytology Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy Present < Current State
Thyroid pathology Practical part
 Thyroid pathology Practical part My Algorithm After a good macroscopy and a microscopic overview of the lesion, I especially look at the capsule and the thyroid just above and just beneath the capsule.
Thyroid pathology Practical part My Algorithm After a good macroscopy and a microscopic overview of the lesion, I especially look at the capsule and the thyroid just above and just beneath the capsule.
Molecular Markers in Fine Needle Aspirates of the Thyroid
 Molecular Markers in Fine Needle Aspirates of the Thyroid Policy Number: 2.04.78 Last Review: 3/2014 Origination: 3/2013 Next Review: 3/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
Molecular Markers in Fine Needle Aspirates of the Thyroid Policy Number: 2.04.78 Last Review: 3/2014 Origination: 3/2013 Next Review: 3/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
Evening Specialty Conference: Cytopathology
 : Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
: Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Cytology for the Endocrinologist. Nicole Massoll M.D
 Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Medical Policy Manual. Topic: Molecular Markers in Fine Needle Aspirates of the Thyroid. Date of Origin: April 2013
 Medical Policy Manual Topic: Molecular Markers in Fine Needle Aspirates of the Thyroid Date of Origin: April 2013 Section: Genetic Testing Last Reviewed Date: April 2014 Policy No: 49 Effective Date: July
Medical Policy Manual Topic: Molecular Markers in Fine Needle Aspirates of the Thyroid Date of Origin: April 2013 Section: Genetic Testing Last Reviewed Date: April 2014 Policy No: 49 Effective Date: July
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Molecular Diagnostics in Thyroid Tumors
 USCAP 2011 Endocrine Pathology Society Companion Meeting Molecular Diagnostics in Thyroid Tumors Yuri E. Nikiforov, M.D., Ph.D. Department of Pathology University of Pittsburgh Medical Center Outline Overview
USCAP 2011 Endocrine Pathology Society Companion Meeting Molecular Diagnostics in Thyroid Tumors Yuri E. Nikiforov, M.D., Ph.D. Department of Pathology University of Pittsburgh Medical Center Outline Overview
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Section 2 Original Policy Date 2013 Last Review Status/Date September 1, 2014
 Policy Number 2.04.82 Molecular Markers in Fine Needle Aspirates of the Thyroid Medical Policy Section 2 Original Policy Date 2013 Last Review Status/Date September 1, 2014 Disclaimer Our medical policies
Policy Number 2.04.82 Molecular Markers in Fine Needle Aspirates of the Thyroid Medical Policy Section 2 Original Policy Date 2013 Last Review Status/Date September 1, 2014 Disclaimer Our medical policies
Fine-needle aspiration (FNA) cytology plays an important
 cytology plays an important") Update on Molecular Testing for Cytologically Indeterminate Thyroid Nodules Michiya Nishino, MD, PhD; Marina Nikiforova, MD Context. Approximately 15% to 30% of thyroid nodules that undergo fine-needle
Update on Molecular Testing for Cytologically Indeterminate Thyroid Nodules Michiya Nishino, MD, PhD; Marina Nikiforova, MD Context. Approximately 15% to 30% of thyroid nodules that undergo fine-needle
DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION
 Follicular-patterned thyroid lesions, WC Faquin 1 DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION William C. Faquin, M.D., Ph.D Department of Pathology, Massachusetts
Follicular-patterned thyroid lesions, WC Faquin 1 DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION William C. Faquin, M.D., Ph.D Department of Pathology, Massachusetts
The Korean Journal of Cytopathology 15(1) : 60-64, 2004
 : 60-64, 2004") 15 1 The Korean Journal of Cytopathology 15(1) : 60-64, 2004 : INTRODUCTION Papillary carcinoma of the thyroid gland has for long been traditionally diagnosed on the basis of the characteristic papillary
15 1 The Korean Journal of Cytopathology 15(1) : 60-64, 2004 : INTRODUCTION Papillary carcinoma of the thyroid gland has for long been traditionally diagnosed on the basis of the characteristic papillary
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases
 Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
 yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
Thyroid Cytopathology: What s New and What s Old That We Don t All Agree on?
 Thyroid Cytopathology: What s New and What s Old That We Don t All Agree on? RITU NAYAR, MD PROFESSOR & VICE CHAIR OF PATHOLOGY NORTHWESTERN UNIVERSITY FEINBERG SCHOOL OF MEDICINE DIRECTOR OF CYTOPATHOLOGY,
Thyroid Cytopathology: What s New and What s Old That We Don t All Agree on? RITU NAYAR, MD PROFESSOR & VICE CHAIR OF PATHOLOGY NORTHWESTERN UNIVERSITY FEINBERG SCHOOL OF MEDICINE DIRECTOR OF CYTOPATHOLOGY,
Molecular Markers in Fine Needle Aspirates of the Thyroid
 Medical Policy Manual Genetic Testing, Policy No. 49 Molecular Markers in Fine Needle Aspirates of the Thyroid Next Review: April 2019 Last Review: June 2018 Effective: July 1, 2018 IMPORTANT REMINDER
Medical Policy Manual Genetic Testing, Policy No. 49 Molecular Markers in Fine Needle Aspirates of the Thyroid Next Review: April 2019 Last Review: June 2018 Effective: July 1, 2018 IMPORTANT REMINDER
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Molecular Markers in Fine Needle Aspirates of the Thyroid Page 1 of 25 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Molecular Markers in Fine Needle Aspirates
Molecular Markers in Fine Needle Aspirates of the Thyroid Page 1 of 25 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Molecular Markers in Fine Needle Aspirates
Journal of Basic & Clinical Medicine
 Journal of Basic & Clinical Medicine http://www.sspublications.org/index.php/jbcm/index Cytomorphologic Features of Noninvasive Follicular Thyroid Neoplasm with Papillary-like Nuclear Features (NIFTP):
Journal of Basic & Clinical Medicine http://www.sspublications.org/index.php/jbcm/index Cytomorphologic Features of Noninvasive Follicular Thyroid Neoplasm with Papillary-like Nuclear Features (NIFTP):
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Overview of Indeterminate Cytology
 83 rd Annual Meeting American Thyroid Association Overview of Indeterminate Cytology Scott Boerner MD FRCPC Head Cytopathology, University Health Network University of Toronto DISCLOSURE Nothing to disclose
83 rd Annual Meeting American Thyroid Association Overview of Indeterminate Cytology Scott Boerner MD FRCPC Head Cytopathology, University Health Network University of Toronto DISCLOSURE Nothing to disclose
Thyroid master class. Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson
 Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Molecular markers in thyroid cancers
 Review Article DOI: 10.18203/issn.2456-3994.IntJMolImmunoOncol20172639 Molecular markers in thyroid cancers Alpa Nimesh Patel, Siddharth Singh Department of Internal Medicine, Pramukhswami Medical College,
Review Article DOI: 10.18203/issn.2456-3994.IntJMolImmunoOncol20172639 Molecular markers in thyroid cancers Alpa Nimesh Patel, Siddharth Singh Department of Internal Medicine, Pramukhswami Medical College,
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
Introduction: Ultrasound guided Fine Needle Aspiration: When and how
 International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
HEAD AND NECK ENDOCRINE SURGERY
 HEAD AND NECK ENDOCRINE SURGERY OCTOBER 22-23, 2010 THE MARK HOPKINS SAN FRANCISCO, CA THYROID FNA AND CYTOPATHOLOGY THEODORE R. MILLER, MD THE THYROID NODULE Prevalence of palpable nodule: Female ~ 6%
HEAD AND NECK ENDOCRINE SURGERY OCTOBER 22-23, 2010 THE MARK HOPKINS SAN FRANCISCO, CA THYROID FNA AND CYTOPATHOLOGY THEODORE R. MILLER, MD THE THYROID NODULE Prevalence of palpable nodule: Female ~ 6%