Intimate partner violence: prevalence, risk factors and attitude of men and women in Jimma Zone, Ethiopia
|
|
|
- Calvin Boyd
- 6 years ago
- Views:
Transcription
1 Intimate partner violence: prevalence, risk factors and attitude of men and women in Jimma Zone, Ethiopia MUSSIE KASSA GEBREMEDIHN A study protocol in partial fulfillment for the masters of public health Advisors MARIA EMMELIN (PhD) Professor ULF HÖGBERG EPIDEMIOLOGY AND PUBLIC HEALTH DEPARTMENT OF PUBLIC HEALTH AND CLINICAL MEDICINE UMEÅ UNIVERSITY JUNE 2006
2 ABSTRACT Domestic violence is a major health problem and issue of gross human right violation. Its` magnitude and impacts on health were documented by studies from different corners of the world. The most recent figure from WHO has shown the state of the women in different countries including Ethiopia. In Ethiopia, seven out ten women are suffering from the consequences of partner violence. Having this fact on the ground, the achievement of the millennium development goals and ensuring sustainable development to alleviate poverty seem impractical. So the urgent need of addressing the issue should start with better understanding of its nature. So far most researches conducted worldwide address the women as a study subject. Similarly in Ethiopia study also including men is non-existing. Therefore, this thesis is geared towards filling this knowledge gap. A community based cross sectional study will be conducted to determine the prevalence, risk factors and attitudes of men and women towards intimate partner violence in Jimma zone, Ethiopia individuals in each men and women study group will be studied. For the purpose of comparison the same enrolment criteria will be used as the WHO multicountry study on domestic violence. Men and women study subjects will be selected from different non-overlapping districts. To ensure the safety and psychological well being of the respondents and the research team, the WHO ethical and safety recommendation will be strictly followed. The Amharic version of the WHO domestic violence questionnaire will be used to study women subjects. The instrument is already translated to Amharic and adapted to the country setting by the country research team. Based on the same instrument, the men questionnaire will be developed. In the process of transforming the instrument, qualitative research will be conducted to gain better understanding of norms and attitudes on intimate partner violence and how men respond to questions related to violence. In both questionnaires only relevant sections of the WHO questionnaire will be included. To ensure the quality of data various measures will be taken at different levels of the study. Data will be entered and analysed by using SPSS version 11.0 statistical packages. Multivariate analysis will be employed to identify risk factors. ii
3 Based on the study results appropriate recommendations will be forwarded and every effort will be made to reach policy makers with the result. iii
4 Acknowledgement I would like to express my heart felt gratitude to my supervisor Maria Emmelin for her patience and guidance with the writing up of this thesis. I really appreciate your comments and critical thinking. I am also grateful to professor Ulf who helped me a lot at the time when my main supervisor got sick. This protocol wouldn t have been finalized with out his kindly help. I would like to thank all the staff of the department of epidemiology and public health, Umeå University, for your help and for sharing the wisdom of knowledge during my stay in Umeå. Special thanks to Karin Johansson and Birgitta Åstrom. You made me feel at home starting from the first day in Umeå. No words to express my gratitude to my family and fiancé. Your love and care kept me warm in those chilly winter days. Last but not least I would like to extend my special thanks to the Swedish government and people for offering me a free education. I have seen calm and very helpful people in the other end the world. TACK. iv
5 Table of contents Abstract...i Table of contents...ii List of figures..iv 1 Introduction Aims of the thesis Over all aim Specific aims..2 3 Background International agreements on women rights and domestic violence Ethiopia-country profile Women issue in the national agenda..5 4 Review of current knowledge on intimate partner violence Search criteria Definition of terms Magnitude of the problem Causes of intimate partner violence Impact of intimate partner violence on health Physical health Reproductive health Mental health Attitude towards violence 15 5 Study Protocol Rationale of the study Objectives of the study General objectives Specific objectives Methods and materials Study area Study design..18 v
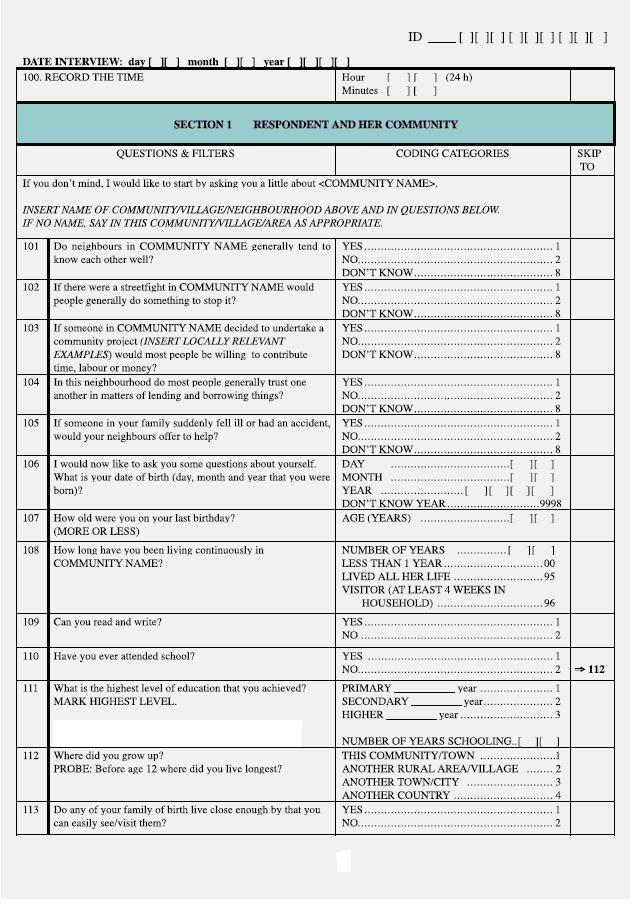
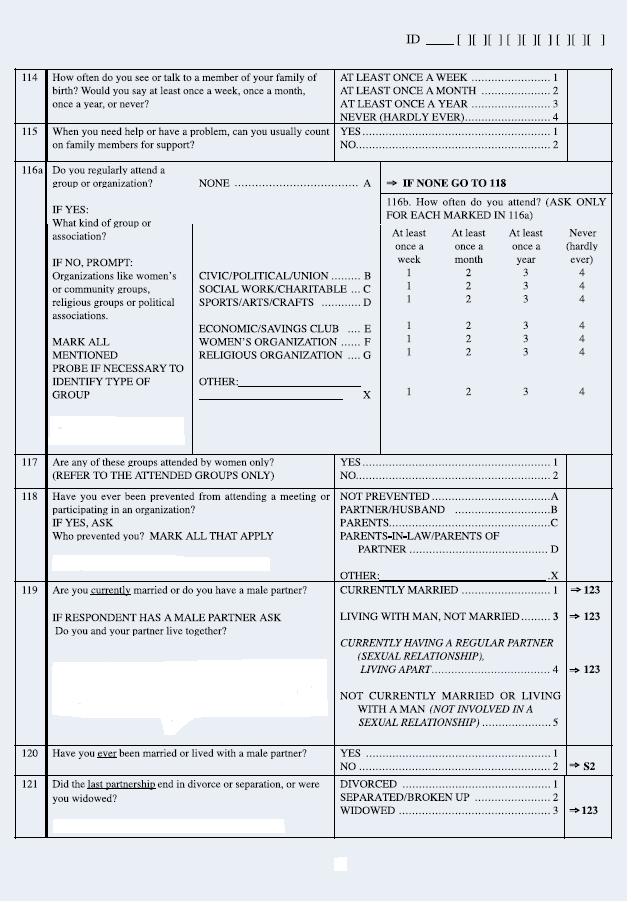
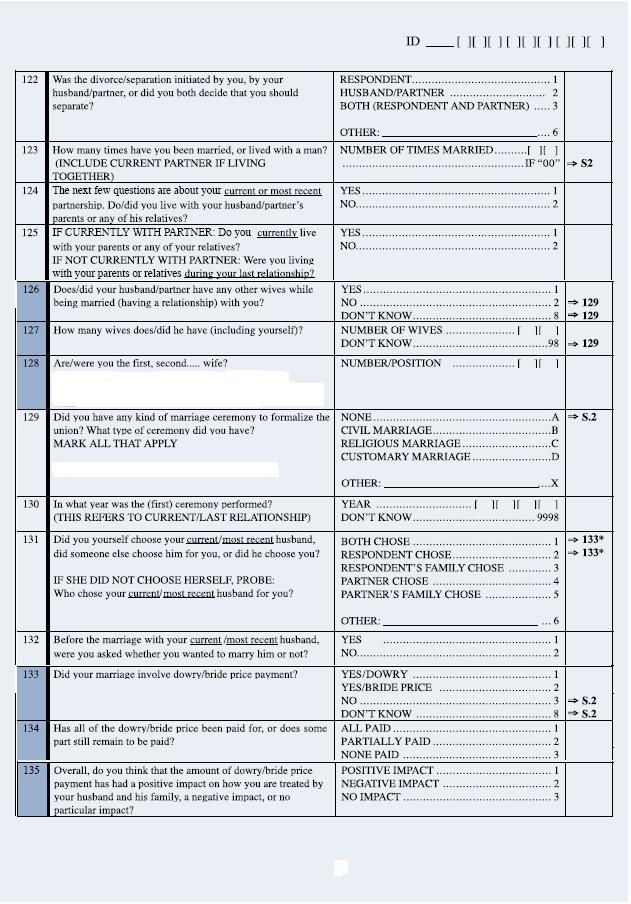
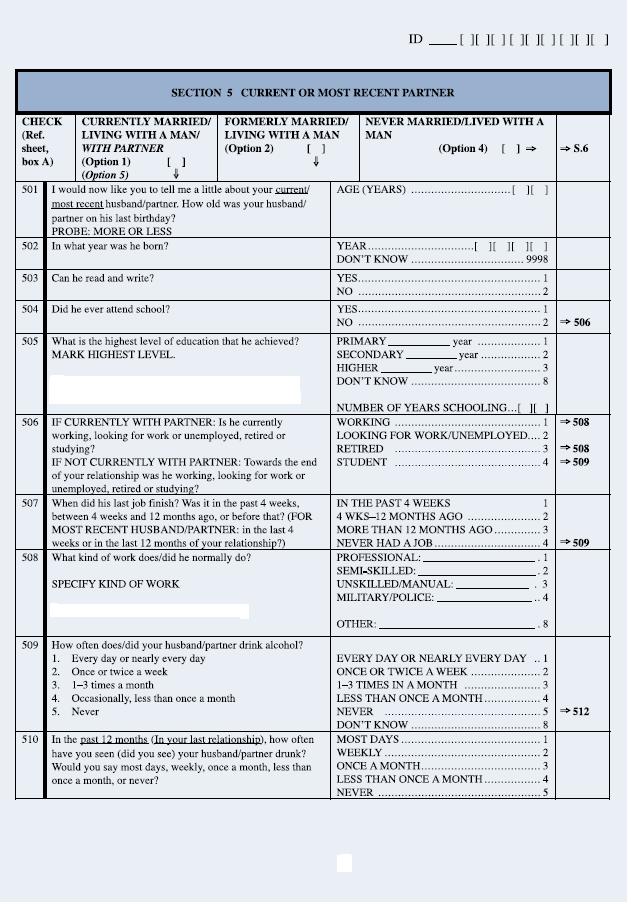
6 5.3.3 Study instrument Study population Sample size Sampling Data collection Data quality control Data analysis Ethical considerations References Annex...32 Women questionnaire vi
7 List of figures Figure 1. Regional map of Ethiopia 4 Figure 2.Violence and abuse against women over time..8 Figure 3.Percentage of women who experienced violence by intimate partner among ever- partnered women aged years, Ethiopia 10 Figure 4. An ecological frame work for understanding gender basedviolence 13 Figure 5. Map of Oromia National regional state, Ethiopia Figure 6.Diagrammatic representation of the steps of the sampling procedure...23 vii
8 1. Introduction Domestic violence, also known as partner abuse, spouse abuse or battering, occurs when one person uses force to inflict injury, emotional, sexual or physical harm upon another person they have, or had, a relationship with. Victims can be of any age, race, or gender (ACEP, 2003). Even though study results from the developed world emphasize also on the abusive role of women against their male partners, women are more frequently targets of both physical and sexual assault, not only by strangers, but also by partners and acquaintances (Linda et al, 1996). The devastating consequences of domestic violence extend well beyond compromising the health state of the victim to affect the family and the society as a whole. According to the World Bank (1993), violence against women is as serious a cause of death and incapacity among women of reproductive age as cancer, and a greater cause of ill-health than traffic accidents and malaria combined. Apart from its significance as a public health problem, domestic violence is one of the most pervasive of human rights violations, dignity, self-worth, and the right to enjoy fundamental freedom. Recognition of violence as a health and human right issue was underscored and strengthened by agreements and declarations at key international conferences (WHO, 2005). The fourth world conference on women in Beijing identified the lack of adequate information on prevalence, nature, causes and consequences of violence globally as a serious obstacle to the development of effective strategy to combat violence. The platform for action adopted at the conference encouraged governments, research institution, as well as non governmental and other organizations to promote research to bridge the knowledge gap in this area (UN, 1995). 1
9 2. Aims of the thesis 2.1 Over all aims The overall aim of this thesis is to prepare a protocol study to investigate the prevalence, risk factors and attitudes of men and women towards intimate partner violence in Jimma zone, Ethiopia. 2.2 Specific aims To review literature on intimate partner violence To develop a study protocol to investigate the prevalence, risk factors and attitude of men and women towards intimate partner violence 3. Background 3.1 International agreements on women s right and violence "Violence against women is perhaps the most shameful human rights violation. It knows no boundaries of geography, culture or wealth. As long as it continues, we cannot claim to be making real progress towards equality, development, and peace." Kofi Annan, United Nations Secretary-General Male dominance and female subordination was considered as a natural law for centuries but after the Second World War, in 1948, with the establishment of the UN, the organization adopts the universal declaration of human rights, the first international instrument to refer specifically to human rights and to the equal rights of men and women. The Declaration proclaims the entitlement of everyone to equality before the law and to the enjoyment of human rights and fundamental freedom without distinction of any kind and proceeds to include sex among the grounds of such impermissible distinction (UN, 2006a). In the 1950 s and 60`s the basic human rights to ``life, liberty and security were reinforced and refined by other conventions. As well the UN adopted various treaties that 2
10 protect and promote the rights of women in areas in which the UN considered such rights to be particularly vulnerable. But the approach to deal with the issue was fragmentary, as they failed to deal with discrimination against women in a comprehensive way (UN, 2006a and WHO, 2001a). Recognizing this, in 1979, the United Nations General Assembly adopted the Convention on the Elimination of All Forms of Discrimination Against Women, which defines what constitutes discrimination against women and frames an agenda for action to end such discrimination (UN, 2006b). Later on, in 1993, the UN approved the Declaration on the Elimination of Violence Against Women, the first international human-rights document to address exclusively the issue of violence against women (UN, 1993). Further endorsement of the central role of violence in compromising women s rights and women s health was provided by the programmes and platforms for action of the World Conference on Human Rights in Vienna in 1993, the International Conference on Population and Development in Cairo in 1994, the World Summit for Social Development in Copenhagen in 1995 and the Fourth World Conference on Women in Beijing in 1995(WHO, 2001a). In the last two decades, international women s right activists have shown substantial progress in creating awareness as to the scale of the problem (HRW, 2005). However, violence against women remains highly prevalent, pervasive, systematic and even sanctioned especially in the developing world. Today s world is no safer than it was two decades ago. The key challenge that remains is to move from awareness that is a human right violation and a crime, to making it socially unacceptable and counter to community norms (UNIFEM, 2005). 3.2 Ethiopia-Country profile Ethiopia is a country situated in the Horn of Africa (fig 1). It is bordered by Eritrea to the north, Djibouti to the northeast, Somalia to the east, Kenya to the south, and Sudan to the 3
.")
11 west. The total surface area of the country is 1.14 million sq. kilometers making it the tenth largest African country by land area. Ethiopia is the third most populous country in Africa following Nigeria and Egypt (Almanacs, 2006). According to the Ethiopian central statistical agency (2005) the population is estimated to be around 75million in July, Out of this, 62.1 million (84%) people live in rural area while the remaining 12.9 million (16%) people reside in urban areas. The population grows at a rate of 2.9 % annually putting the country in the list of countries with high population density. The majority of Ethiopians are Orthodox Christians and Muslims by religion. Ethiopia is comprised of nine national regional states (NRS) and two chartered cities (Fig 4). The regions further divided into 62 zones, 580 woredas (districts) and 1500 kebeles- the smallest administrative unit (UNDP-ET, 2006). Figure1. Regional Map of Ethiopia Source: Almanacs
12 Ethiopia's poverty-stricken economy is based on agriculture, accounting for half of GDP, 60% of exports, and 80% of total employment. The agricultural sector suffers from frequent droughts and poor cultivation practices. Although Ethiopia has shown a progressive economic development in the last decade, it remains to be one of the poorest countries in the world where around half of the population lives below the poverty line (CIA, 2005). Given the lack of access and control over resources and many discriminatory customs, women comprise the majority of those living in absolute poverty. 3.3 Women issues in the national agenda Before 1974 women s organized activities were run by nongovernmental bodies such as the Ethiopian officer s wives association and the Ethiopian female students associations. However, these associations didn t reach out to the rural areas where the majority women live. After the revolution in 1974, the revolutionary Ethiopian women s association (REWA) was established by proclamation. As part of the national basic education campaign, REWA succeeded in improving the literacy state of women. However, REWA has dissolved with the fall of the Marxist government leaving most of the Ethiopian women problems untouched (World Bank, 1998). The Federal Democratic Republic of Ethiopia government started its commitment to the advancement of women by setting up the women s affairs office with in the prime minister office which recently transformed to a minister of women affairs. Ethiopia adopted a national women s policy in The policy aims to institutionalize the political, economical and social rights of women by creating an appropriate structure in government offices and institutions. Gender differentials persist at all levels in the country. This is mainly a result of gender based division of labor and lack of access and control over resources compounded by the existence of different kinds of laws, national as well as a variety of customary and religious ones. Customary laws are entrenched at the grass root level in the society. The family arbitration system used for settling inter-household dispute is conducted mainly by 5
13 older men who want to maintain the subordinate position of women (UN 2003). Overall this has created a fertile ground to gender based violence. To mitigate the adverse social, cultural and political environment and empower women, the Ethiopian government has taken a number of measures. More recently, the penal code has been revised so as to make punishment for abduction, rape and sexual assault more severe. 4. Review of current knowledge on intimate partner violence 4.1 Search criteria The studies and other materials used in reviewing the current knowledge on domestic violence were identified by searching from pubmed and the WHO web sites. The search were made in four categories; prevalence, causes, impacts and attitudes to domestic violence. Special emphasis was given to studies including men. Since studies on men are scant, a twenty years search from was made. After scrutinizing the abstracts, the most relevant articles were selected. In the prevalence, causes and impacts category 15 articles and reviews were identified, while in the attitude part 6 articles were found. Only 3 studies including men as study subjects were found and included in this review. Being an important international document, the WHO study is cited in each parts of the review. 4.2 Definition of terms Research into violence against women is increasing, but there are no widely agreed definitions of the different forms of such violence that could be used to standardize research findings (Watts and Zimmerman 2002). According to the United Nations (1993), violence against women is defined as: Any act of gender-based violence that results in, or is likely to result in, physical, sexual or psychological harm or suffering to women, including threats of such acts, 6

14 coercion or arbitrary deprivations of liberty, whether occurring in public or private life. The term violence against women includes a range of abuses towards women, extending from sex selective abortion to elderly abuse. In figure 2, the authors (Watts and Zimmerman 2002) have summarized forms of violence by different perpetrators across the age span of a woman. More importantly they have illustrated that the risk of violence for women begins in utero and extends indefinitely in their life. Figure2.Violence and abuse against women over time Source: Watts and Zimmerman
15 One of the most common forms of violence against women is that performed by a husband or intimate male partner. It is often a cycle of abuse that includes acts of; physical aggression such as slapping, beating, arm twisting, stabbing, stabbing, strangling, burning, choking, kicking, threats with an object or weapon, and murder; sexual abuse such as coerced sex through threats intimidation or physical force, forcing unwanted sexual acts or forcing sex with others; psychological abuse which includes behavior that is intended to intimidate and persecute, and takes the form of threats of abuse, confinement to the home, surveillance, destruction of objects, isolation, verbal aggression and humiliation and economic abuse which includes acts such as the denial of funds, refusal to contribute financially, controlling access to health care, employment, etc. The terms domestic violence and intimate partner violence are often used interchangeably. In this paper, the terms are also used synonymously to describe physical, sexual or psychological abuse directed against a woman by her male partner. 4.3 Magnitude of the problem Violence pervades the lives of many people around the world, and touches all of us in some way. To many people, staying out of harm's way is a matter of locking doors and windows and avoiding dangerous places. To others, escape is not possible. The threat of violence is behind those doors, well hidden from public view Gro Harlem Brundtland, (WHO, 2002) Violence against women and girls is a global epidemic that kills, tortures, maimsphysically, psychologically, sexually, and economically. Women in different social contexts can be affected and victims can be of any age, race, ethnicity, education, and socioeconomic status (Heise, 1999). Reports from different parts of the world present widely ranging estimates of its prevalence. Differences in definitions, age groups included in studies and utilization of different methodologies poses difficulty to generate internationally comparable data on violence (Watts and Zimmerman, 2002). In nearly 50 population-based studies from around the world, 10% to over 50% of women report being hit or otherwise physically harmed by an intimate male partner at some point in their lives (Heise and Ellsberg, 8

16 1999). Even if these studies disclosed alarming figures, they are most likely significantly underestimating the prevalence of domestic violence as discussing violence continues to be a taboo subject in most societies (WHO, 2001c). More recently the World Health Organization Multi-Country Study on Women s Health and Domestic Violence, a ground breaking study, reveals a horrifying picture. The study analyses data collected in house hold surveys from women in 15 sites in 10 geographically, culturally, and economically diverse countries. The study confirms that violence by intimate partners, rather than by other perpetrators, is a dominant form of violence against women. For ever partnered women, the life time prevalence of physical or sexual violence, or both, by an intimate partner ranged from 15% to 75% in different sites. Across all countries between 20% and 75% of women had experienced one or more acts of emotional abuse. The study also showed that 71% of ever partnered women in Ethiopia suffered from sexual or physical violence, or both, over their life time (fig3). Around one third of these women had experienced severe forms of violence (WHO, 2005). Figure 3.Percentage of women who experienced violence by intimate partner, among ever- partnered women aged years, Butajira, Ethiopia Source: WHO country fact sheet
17 4.4 Causes of intimate partner violence The causes of intimate partner violence have been a subject of debate for decades and the issue remains to be settled. Different theoretical frameworks drawn by social scientists fail to provide a comprehensive explanation for the occurrence of intimate partner violence. Understanding its social causation has been hampered by the fact that most research has been done in the developed world and has been based on information obtained from women accessing sources of help. However, during the last decade, several well designed population based studies of domestic violence against women emerged from the developing countries (Jewkes, 2002a). Early research focused primarily on individual risk factors among men and women that predicted either victimization or perpetration of violence. In a review of 52 studies, Hotaling and Sugarman(1986) have shown lack of empirical support to a number of hypotheses. In this review the authors identified 97 potential correlates for husband to wife violence. The variables were assessed according to whether they were consistent risk markers, inconsistent markers, consistent non risk markers, or whether there was insufficient data to reach a conclusion. For women, the only characteristics that was consistently associated with the risk of being a victim of partner abuse as an adult was whether they had witnessed family violence as a child. All other potential risk factor, including women s age, race, education, alcohol, and drug use, occupation and income were either inconsistent or consistently non significant. However, several characteristics were found that consistently predicted physically violent behavior among men, including witnessing violence as a child, or experiencing violence as a child, educational level, income, alcohol use, violence towards children and partner sexual abuse. Furthermore, it was observed that characteristics associated with either a husband offender or the couple have greater utility for assessing the risk of husband to wife violence than characteristics of the wife victim. 10
18 In another comprehensive review of literature reports in United States, Wilt and Olson (1996) documented risk correlates to domestic violence. The variables they identified included younger age, divorced women, low socioeconomic status as measured by income and occupation. However, other studies have failed to elaborate consistent associations between socio-demographic characteristics and violence. Since the 1970 s causes of partner abuse have been addressed from the angle of various theoretical models. Among the most common have been the intraindividual theories focusing on cognitive, personality and pathological psychology that predispose individual to violence; social psychological theory viewing violence as socially learnt behavior that transmit from one generation to the next; and social cultural theories viewing violence as a consequence of global structural change (Valladares, 2005). The intergeneration transmission of violence is demonstrated by studies from different parts of the world. A study from northern India showed that men raised in violent homes were likely to believe in husband s right to control their wives as well they were found to be more abusive as compared to those men raised in non- violent homes (Martin etal, 2002). More recently researchers have used an ecological model to understand the multifaceted nature of intimate partner violence. First introduced in the late 1970 s, this ecological model was initially applied to child abuse and subsequently to youth violence. The model explores the relationship between individual and contextual factors and considers violence as the product of multiple levels of influence on behavior. As shown in fig. 4, the model is composed of four concentric circles (WHO, 2002). The inner circle factors focus on characteristics of the individual that increase the likelihood of being abused as a child or witnessing marital violence in the home, having absent or rejecting father, being male, low educational attainment, substance abuse and prior history of aggression. The second circle explores responsible factors of abuse within the proximal social relationships of women. This level includes factors such as male control over wealth and decision making in the family and marital conflict. The third circle (community) includes poverty and unemployment, social isolation of women and male participation in delinquent peer association. The fourth and final circle of the ecological model examines 11

19 the larger societal factors that influence the occurrence of violence. Included here are those factors that create an acceptable climate for violence, reduce inhibition against violence, norms and laws granting men control over female behavior and ideas of masculinity linked to dominance and aggression (WHO, 2002 and Jewkes et al,2002b). The ecological approach emphasizes the multiple natures of violence etiology rather than a single cause. So by summing up individual level risk factors with findings of cross cultural studies, it contributes to understanding why some societies and some individuals are more violent (Heise et al, 1999). Source: WHO fact sheet 2001 Figure 4. Ecological frame work for understanding gender based violence 4.5 Impact of intimate partner violence on health Domestic violence has been linked to many serious health problems, both immediate and long term. These include physical health problems, such as injury, chronic pain 12
20 syndrome, and gastrointestinal disorders, and a range of mental health problems, including anxiety and depression. Violence also undermines health by increasing a variety of negative behaviors, such as smoking, alcohol and drug abuse. Because most early studies on abuse and health involved woman seeking medical treatment, their finding could have over stated the relationship between violence and poor health. But links between victimization and ill health have been confirmed in recent studies among more representative groups (Heise et al,1999) Physical health Violence is a major cause of injury to women ranging from relatively minor cuts and bruises to permanent disability and death (Heise et al, 1999).The WHO multi-country study found that 19% to 55% physically abused women sustain injury from the abuse at some point in their life and among this over 20% of ever injured women reported that they had been injured many times (WHO, 2005). Injury, however, is not the most common physical outcome of partner abuse (WHO, 2002). More commonly abused women have significantly more than average self reported gastrointestinal symptoms and diagnosed functional gastrointestinal disorders associated with chronic stress. These disorders may begin during an acutely violent and thus stressful relationship. The consequent functional damage to the bowel can last longer than the violent relationship (Campbell, 2002). Similarly women with abuse history, particularly those with severe abuse, were much more likely to report somatic symptoms related to panic (e.g. palpitation, numbness, shortness of breath), musculoskeletal disorders (e.g. head ache, muscle ache), skin disturbance (e.g. rash) and respiratory illness (e.g. stuffy nose) (Leserman and Li, 1998). In its extreme form violence can be fatal. Worldwide, an estimated 40% to over 70% of homicides of women are committed by intimate partners, often in the context of abusive relationships. By contrast, only a small percentage of men murdered are killed by their female partners, and in such cases the women often are defending themselves or retaliating against abusive men (Heise et al, 1999) 13
21 4.5.2 Reproductive health Partner violence limits the women s right to reproductive decisions. The sexual coercion or male control affects the woman choice regarding conception, frequently leading to unplanned unwanted pregnancies (Valladares, 2005). Researchers have long assumed that the stress of having many children increases the risk of violence, but recent data from Nicaragua suggests that the relationship may be the opposite. In Nicaragua, the onset of violence largely precedes having many children (80% of violence beginning within the first 4 years of marriage), suggesting that violence may be a risk factor for having many children (WHO, 2002) The association between intimate partner violence and gynecologic problems have documented by several researches. Different symptoms and conditions include sexually transmitted diseases, vaginal bleeding or infection, fibroids, decreased sexual desire, genital irritation, pain on intercourse, chronic pelvic pain and urinary tract infections. The possible mechanisms of increased risk of gynecologic disorders include the shame and stress reported with forced sex manifesting as especially high levels of stress and depression known to depress the immune system; vaginal, anal, and urethral trauma from forced sex leading to increased transmission of microorganisms through direct route into the blood steam or backflow of bacteria in the urethra; sex on partners and having sex with other partners (Campbell, 2002). Furthermore, men who are violent towards their partners are also more likely to have multiple sexual partners potentially putting women in violent relationship at an increased risk of HIV or STI (Dunkle, 2004 and WHO, 2005). Partner violence during pregnancy is not uncommon. When it happens, it is detrimental to the mother, fetus or both. The WHO study on violence showed that abused pregnant women were less likely to attend antenatal and post natal care (WHO, 2005); suffer from pregnancy complications, poor weight gain and pregnancy out come including miscarriage and low birth weight (Valladeras, 2005). Similarly, evidence from a meta- 14
22 analysis of 14 published studies from North America and Europe showed a weak but significant association between abuse during pregnancy and low birth weight (Campbell, 2002) Mental health A growing body of research evidence is revealing that sharing her life with an abusive partner can have a profound impact on woman s mental health. Battered women are more likely to suffer from depression, anxiety, psychosomatic symptoms, eating problems, and sexual dysfunction (WHO, 2001 and WHO, 2002). Among women aged 15 to 49 in Ethiopia, for example, abused women were more likely to have had any form of depressive disorder with or without dysthemia in the last 12 months than women who were not victims of physical or sexual violence(gossaye et al, 2003). Similarly the WHO (2005) study reported significantly higher levels of emotional distress and suicidal ideation or attempted suicide among abused women as compared to women who had never experienced partner violence. 4.6 Attitudes towards violence Domestic violence is a complex issue to research as the extent and forms of its occurrence remain largely hidden and there is a great degree of social acceptance of the issue. Research from different cultural settings has demonstrated partner violence as widely accepted and justified, and perceived by both women and men as normal in married life. Studies have inquired into the justification of wife-beating under a variety of circumstances, ranging from disobedience and disrespect to in-laws, to infidelity and alcohol abuse. Among the most persistent circumstances in which violence is justified by women are those related to perceptions of non-performance of domestic duties or noncompliance with expectations (WHO, 2005 and Jejeebhoy, 1998) Findings from studies of men s attitudes suggest that men justify wife-beating for similar reasons. In a study from Cape Town, South Africa, violent men justify wife beating if she refuses sex or she challenges the male control over the relationship (Abrahams et al, 15
23 2004). In another study from India, men agreed that violence is justified if the wife is sexually unfaithful (79 per cent), disrespectful to family elders (77 per cent) and disrespectful to the husband (75 per cent). In short, evidence points to the fact that men and women justify and accept violence for various reasons that are embedded in existing social norms (Nata et al, 2002). In a cross-sectional study in Uganda Abraham et al (2003) interviewed men and women regarding their views to the circumstances in which violence against female partner would be justified. They recognized that the proportion of the respondents who justify beating varied with respect to each behavior in question. In addition, a relatively higher proportion of women tend to agree for each attitude question. For instance, 70% of men and 90% of women believed that beating was justifiable for one or more of the situations cited. The study also noted a higher tendency of younger men and women towards attitudes condoning domestic violence. For example, 66% of men and 73% women under 25 years age viewed beating of the female partner as justifiable for one or more reasons (other than infidelity).however, 43% men and 55% of women aged above 35 years believe in one or more reason. Qualitative research from various settings has also suggested that rates of violence by an intimate partner may be higher in settings where the behavior is normative, and where women and men believe that marriage grants men unconditional sexual access to their wives. The WHO study showed that the overall acceptance that wife-beating is justified in some situation was significantly greater among women who had ever experienced physical or sexual partner violence, or both, than among women who had never experienced violence (WHO, 2005). Similarly a study from Butajira, central Ethiopia, documented that women who had experienced physical or sexual partner violence were more likely than non-abused women to believe that a man would be justified in hitting his wife (Gossaye et al, 2003). However, the mechanism how attitudes towards wife-beating may influence women s experiences of violence at an individual level is not clear. It may be that women learn to accept or rationalize violence in circumstances where they themselves are victims, or that women are at greater risk of violence in communities 16
24 where a substantial proportion of individuals subscribe to the acceptability of violence (WHO, 2005). 5. Study Protocol 5.1 Rationale of the study Effective intervention on violence requires a full understanding of its nature. Until recently, most research on violence has been from the developed nations and has been institution based which may be less relevant in the context of the developing world. Researching domestic violence is relatively a new area for the developing world and it is at the stage of description. Studies in different settings have shown wide ranging figures of its magnitude between countries and groups in the same cultural setting, suggesting for possible risk and protective factors. The few available studies in Ethiopia have focused on the magnitude of the problem. Furthermore, these studies have focused entirely on women. Recognizing that most cases of intimate partner violence are perpetrated by men and taking in to account the key role of men s behavior in domestic violence, a study focusing including also men s experiences can provide a better understanding of the causes and attitudes which may be amenable to change. Moreover the World Health Organization on its report on the multi-country study on domestic violence underlined the need of research on causes of violence against women in different cultures and in different circumstances. 5.2 Objectives of the study General objectives To determine the prevalence, risk factors and attitude towards domestic violence among ever partnered women and men in Jimma zone, Ethiopia Specific objectives To determine the prevalence of intimate partner violence, potential risk factors and prevailing atttitudes as reported by women 17


25 To explore norms, attitudes and experiencies among men towards intimate partner violence and estimate of extent of IPV 5.3 Methods and materials Study area The study will be conducted in Jimma zone, Ethiopia. Jimma zone is one of the 12 zones of Oromiya region- the biggest region in Ethiopia. It is composed of Jimma town and 13 districts around Jimma town. The total population of the Jimma zone is estimated to be 2.7 million. Of this 90% live in rural area while the remaining 10% lives in urban setting. Jimma Figure5. Map of Oromia National regional state, Ethiopia Source: Google images Jimma town has been the capital city of Kaffa which is known as the botanical homeland of coffee. As the name coffee is derived from the word "Kaffa" after the discovery of coffee in this region. Jimma is located 335 km south west of the Ethiopian capital, Addis Ababa. Currently the town is serving as a political and economical centre of the jimma zone. Each district in the Jimma zone has one urban centre and several rural kebeles Study design A community based cross sectional study will be conducted. A cross-sectional study is a descriptive study in which events are measured at a point in time. In researching violence, cross sectional study provides information about 18
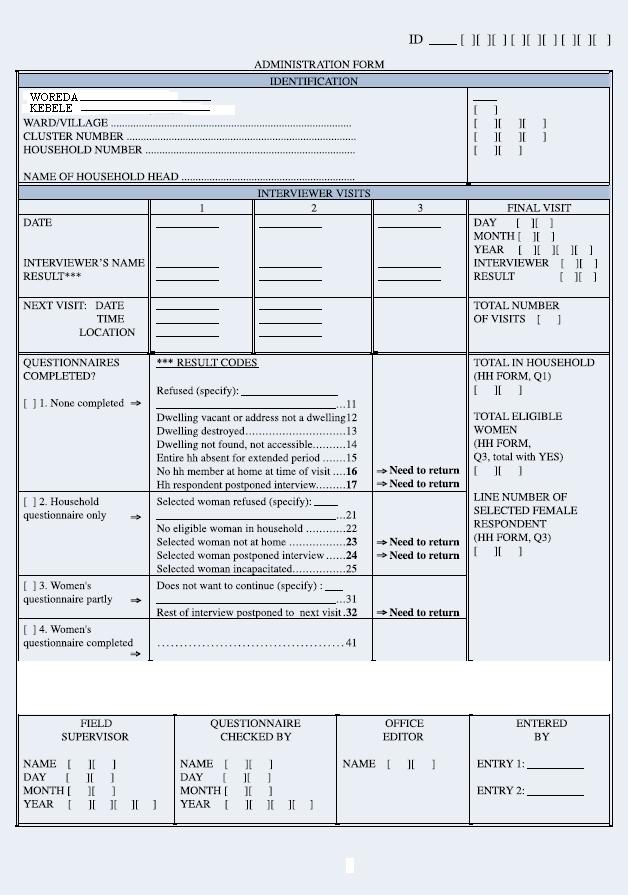
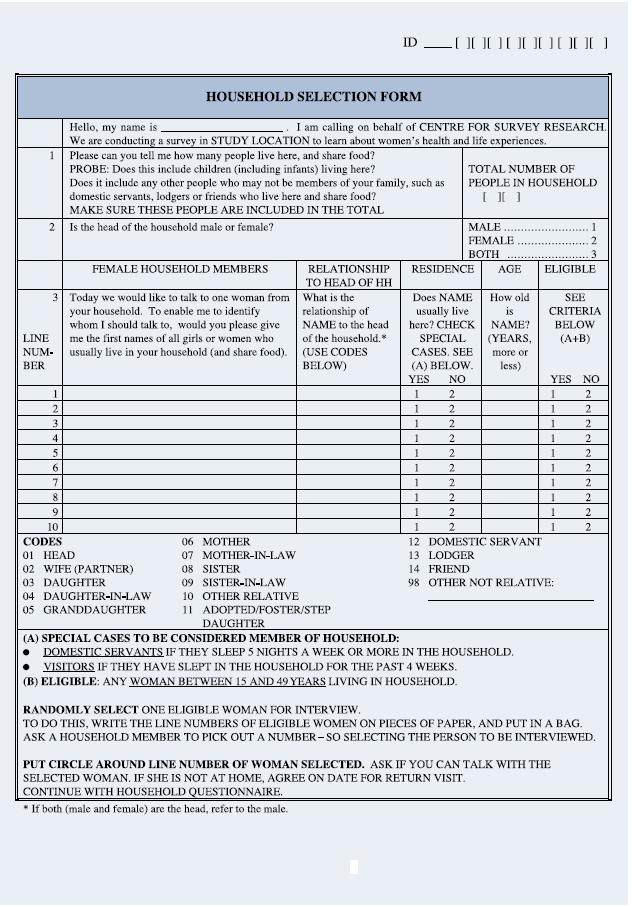
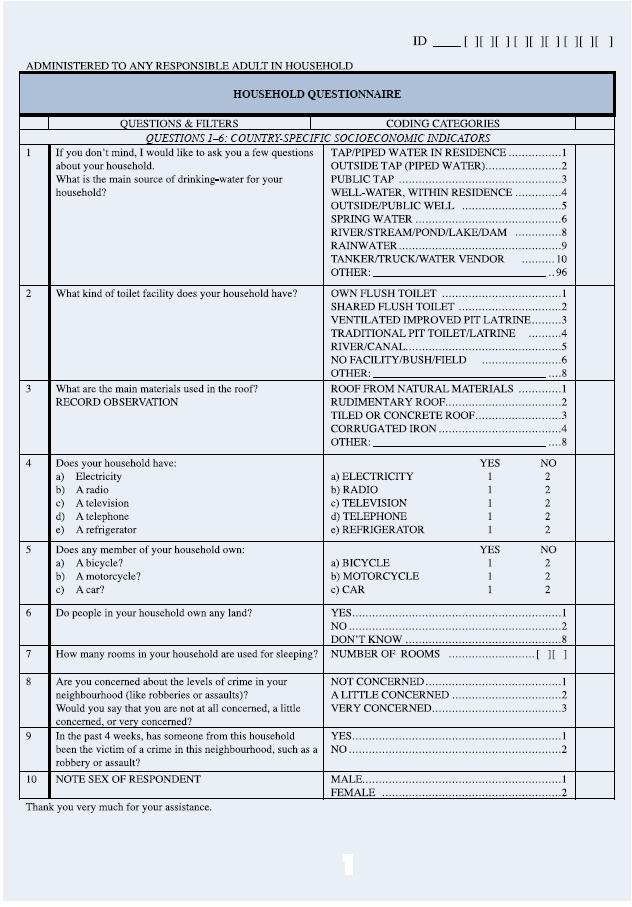
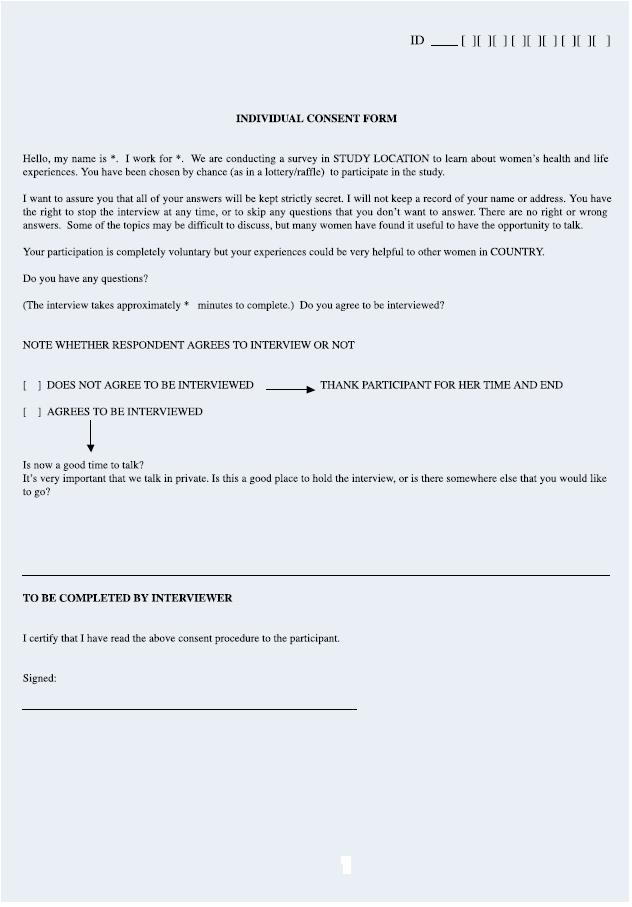
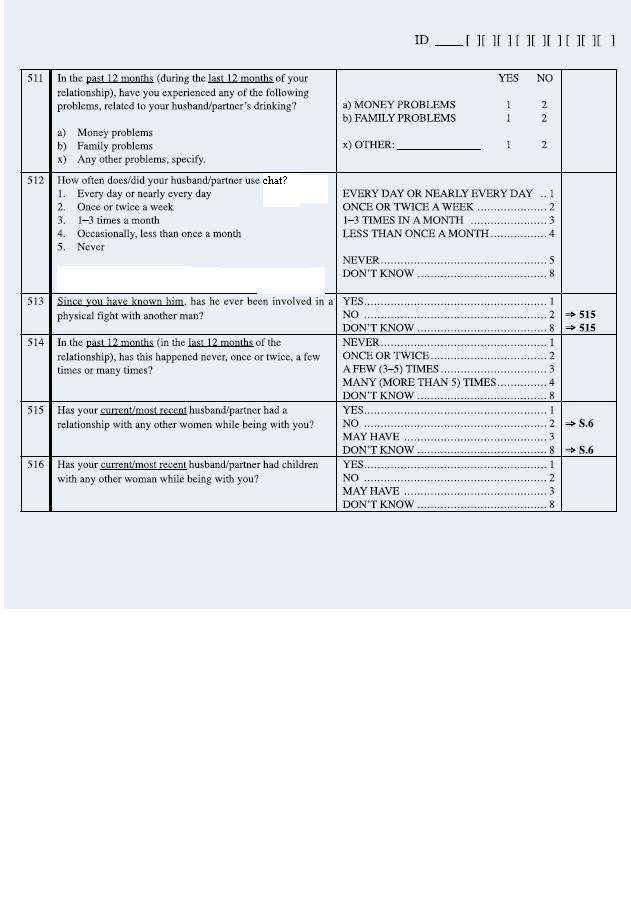
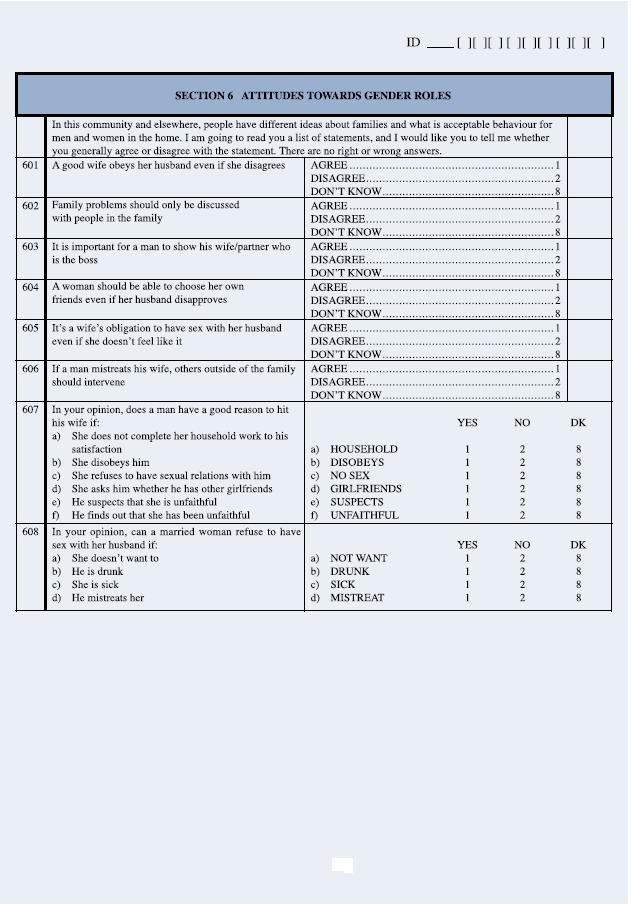
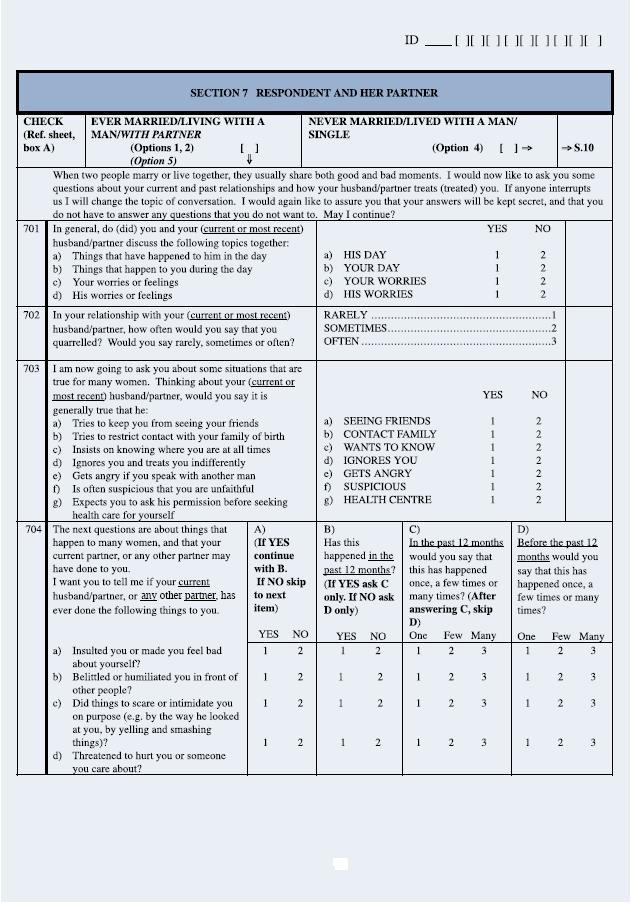
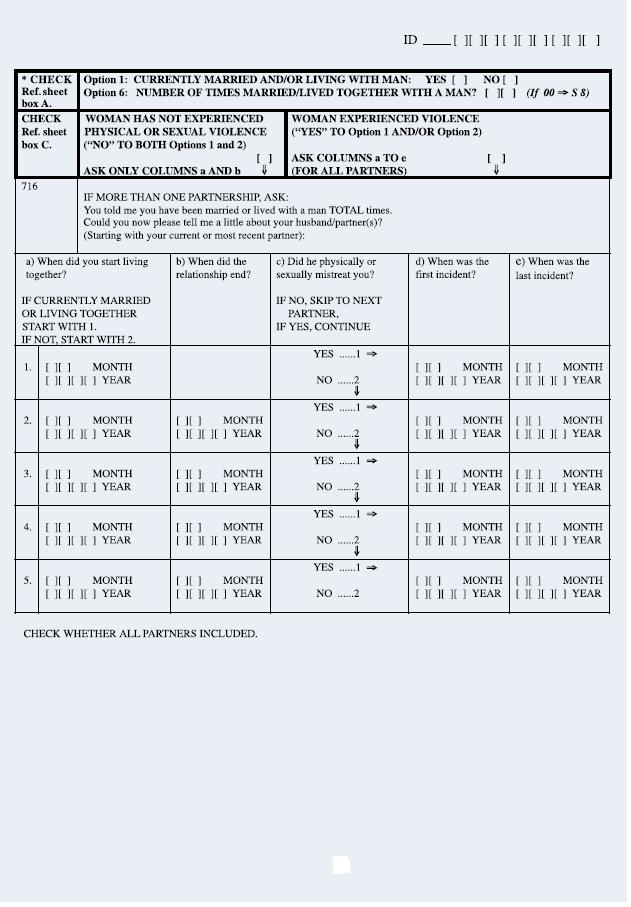
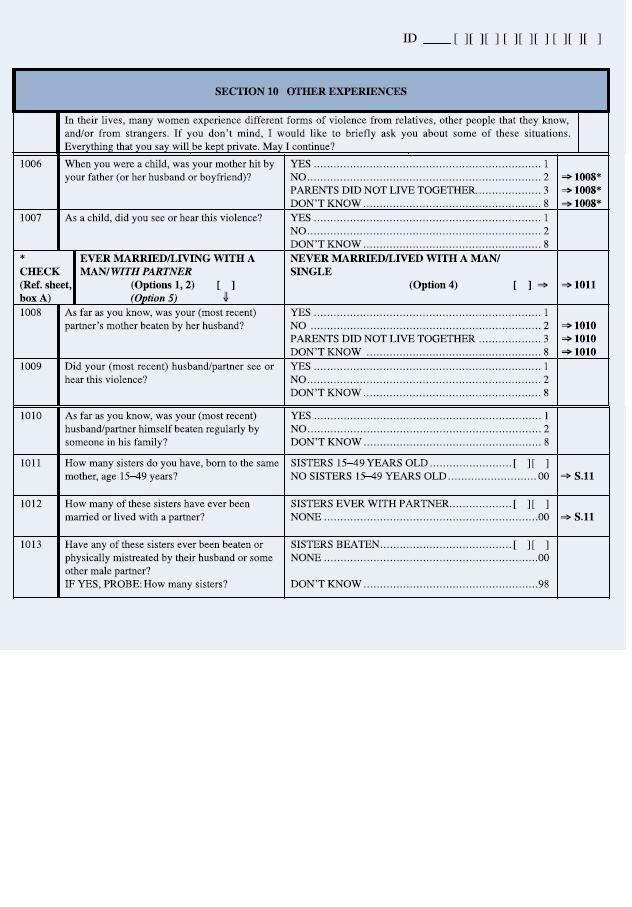
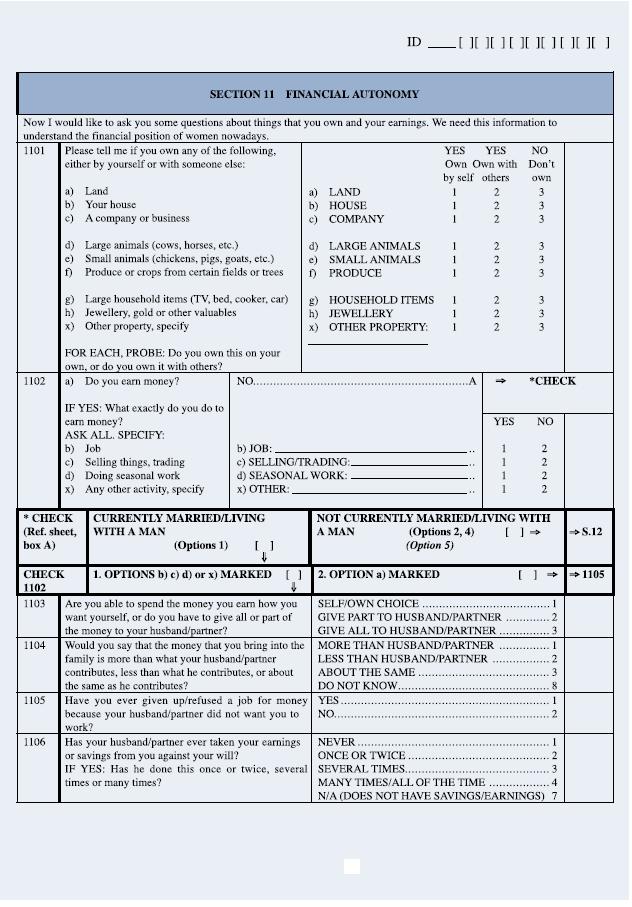
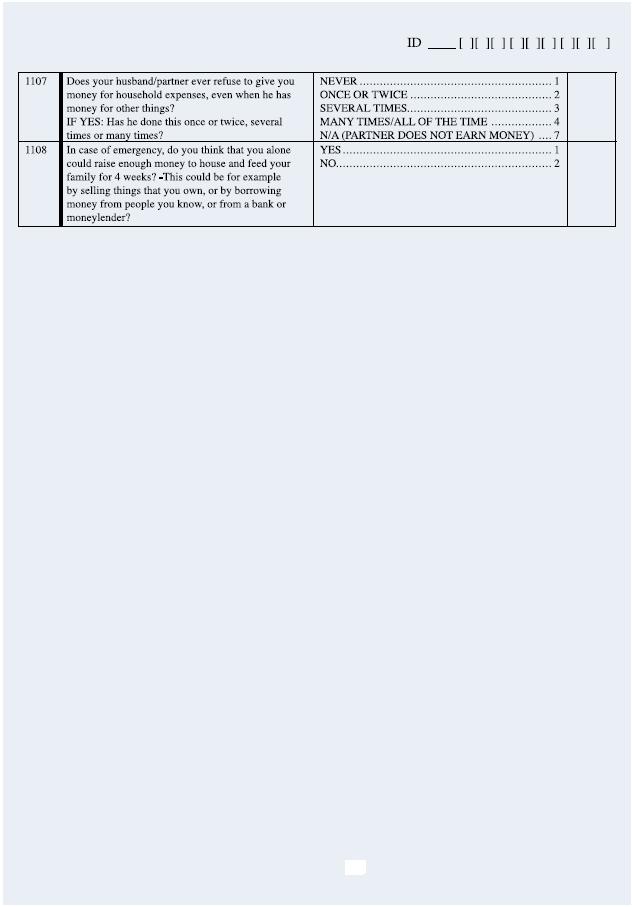
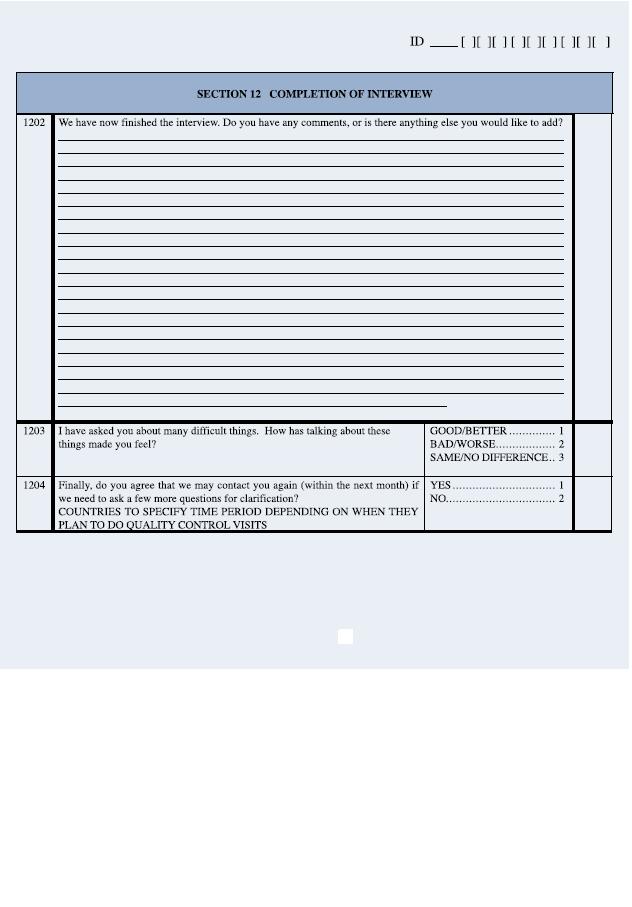
26 prevalence, Characteristics, and attitudes of men and women towards violence. However, in studies focusing on risk factor assessment cross sectional study may not be the most appropriate design since it is difficult to determine the temporal relation ship of causes and effects (Ellsberg and Heise, 2005). For this study, cross sectional study design is chosen after taking the objectives of the study and feasibility of other options into account Study instrument The Amharic version of the WHO domestic violence questionnaire will be used. The WHO questionnaire created for the purpose of the multi country study on women s health and domestic violence against women. The 9.9 version of the questionnaire consists of an administration form, household selection form, household questionnaire, women s questionnaire and reference sheet. The women questionnaire composed of an individual consent form and twelve parts including questions regarding the respondent and her community, her general and reproductive health, her financial autonomy, her children, her partner, her Attitudes towards gender roles, her experiences of partner and nonpartner violence, and the impact of violence on her life. The instrument is already translated to Amharic and adapted to the country setting by the country research team. However, the questions included in this instrument are wider than the objective of this study to be addressed. Therefore, in this study all the forms, the household questionnaire, part of the women s questionnaire and the reference sheet will be used. The parts of the women questionnaire which are relevant to the study include questions regarding the respondent and her community, her partner, her Attitudes towards gender roles, her experiences of partner violence. The Amharic version of the WHO domestic violence instrument will be used as a base to develop the men questionnaire. This instrument was a product of long process of discussion and consultation, and developed for the purpose of addressing women respondents. Its use in studying men subjects has never been tested. So maximum effort will be exerted to ascertain the highest validity and reliability of the instrument. 19
27 In the process of transforming the instrument, qualitative survey by using in-depth interview with key informants as health staff, teachers, community leaders, lawyers, policemen, and focus group discussion, with a convenient sample rural and urban men, young and middle aged, will be conducted. The purpose of semi-structured interviews will be to gain better understanding of norms and attitudes on intimate partner violence and how men respond to questions related to violence. All themes addressed in the WHOquestionnaire will be raised in the formative qualitative research. The structure of the interviews will reflect the forms of information to be collected during the actual data collection. In addition, focus group discussion on convenient sample will be used explore local perception and language regarding domestic violence. The parts of the questionnaire which are relevant to the study are all the forms, the household questionnaire, and part of the reference sheet and women s questionnaire. For the purpose of this study major modification will be applied to the women questionnaire. Parts of the women questionnaire which are extensively used in developing the men questionnaire include questions regarding the respondent and her community, her partner, her Attitudes towards gender roles, her experiences of partner violence. Although most of the questions in the modified questionnaire originated from the specified sections, a number of questions also included from the other (excluded) parts of the women questionnaire. Furthermore, new questions, for instance, respondents use of chat were also included. No preliminary questionnaire for the men can be elaborated before analysis of the keyinformant interview and focus group discussion. Furthermore, after having a first version it will be tested in a small sample with continous revision. Before having a final version for men the questionnaire will be tested on 5% of the sample. This will be used to explore the clarity, acceptability and other issues related to questions Study population 20
28 For the purpose of comparison, study subjects will be enrolled by using the criteria as in the WHO study (WHO, 2005). Ever partnered women and men aged that fulfil at least one of the following eligibility criteria will be included in the study: normally lives in the household a domestic servant and sleep for five nights a week or more in the household a visitor and has slept in the household for at least the past four weeks ever partnered`` women/men defined as individuals who are or have been married or in a common law relationship Sample size Sample size calculated by using the following formula Z 2. p. (1-p) N = * D d 2 Two thousands seven hundred seventy four (2774) individuals from each population will be enrolled in the study. The following assumptions are used to calculate sample size for both populations. Proportion on men perpetrating violence against their female partner (P) = % degree of precision Z α/2 = 1.96 Margin of error (d) =3% 30% non response rate will be used in order to make up for losses to the sample as a result of households without eligible individual, refusals to participate, or incomplete interviews. 21
29 Design effect =2 Design effect measures the increase in standard error of the estimate due to the sampling design. It is given by the equation D= 1+ (b-1) rho Where; rho is a measure of variability between clusters as compared to the variation with in clusters and b denotes the number of items to be studied in each cluster. When the intra cluster correlation of the study out-come is not known, the design effect is usually assumed to be Sampling For ethical and safety reasons the two samples will be taken from non overlapping separate districts. To accomplish this, the men sample will be selected first then the women sample will be selected after excluding those districts and kebeles from which the men samples are selected. Male population A sample of the men population will be selected by using multistage sampling (Fig.6). First the zone will be stratified into urban and rural settings. The rural setting will include all the districts while the urban setting include jimma town. Samples will be proportionally allocated according to the distribution of the population in urban and rural settings i.e. the composition of the study population have a 9:1 rural- urban ratio. Selection of rural subjects Out of the13 districts in rural jimma, 3 districts will be selected by random sampling with probabilities proportional to the size. From the selected 3 districts, a sample of 27 kebeles will be chosen (9 kebeles from each district) by using simple random sampling. Thereafter collecting the list of owners of houses from each kebele administrative offices; households will be selected by simple random sampling using the list of owners of the houses as a sampling frame. Once the house holds identified, lottery method will be employed to select one man from each house hold (in case of more than one eligible man in single house hold). Selection of urban subjects 22
30 Jimma town is composed of 21 kebeles. Among these 3 kebeles will be selected by using random sampling with probability proportional to the size of the kebele. Then systematic random sampling will be employed to select house holds; the sampling frame here will be the house number that can be obtained from the respective kebele offices. Individuals from each house holds will be selected by using the same methods and eligibility criteria as in the rural case. Women population Multistage sampling will be employed to sample of the women population (Fig.6). The sampling procedure started by excluding those districts and kebeles from which the male subjects are selected. The remaining districts and kebeles will be stratified into urban and rural setting. The rural setting will include the ten districts while all kebeles in jimma town except the three will be included as urban setting. Samples will be proportionally allocated according to the distribution of the population in urban and rural settings i.e. the composition of the study population have a 9:1 rural- urban ratio. Selection of rural subjects Three districts out of ten will be selected by random sampling with probabilities proportional to the size. From the selected 3 districts, a sample of 27 kebeles will be chosen (9 kebeles from each district) using simple random sampling. Thereafter collecting the list of owners of houses from each kebele administrative offices; households will be selected by simple random sampling using the list of owners of the houses as a sampling frame. In households with more than one eligible woman, a single respondent will be selected randomly for interview by using lottery method. Selection of urban subjects Three kebeles out of 18 will be selected by using random sampling with probability proportional to the size of the kebele. Then systematic random sampling will be employed to select households; the sampling frame here will be the house number that can be obtained from the respective kebele offices. Individuals from each house holds will be selected by using the same methods and eligibility criteria as in the rural case. 23
31 5.3.7 Data collection Women population Female high school graduates who are fluent in the local languages will be recruited. As Ellsberg and Heise (2005) described, rate of disclosure depends on characteristics of the interviewer, so greater care will be taken in the selection process. Interviewer characteristics-age, marital status, ability to engage with people of different back ground in an empathetic and non-judgmental manner, emotional maturity, skill at building rapport and ability to deal with sensitive issues will be considered in the recruitment. Training will be given on the following areas o Gender discrimination/ inequality o Basic introduction to domestic violence o Sensitivity of the issue o The aim of the study o Interviewing technique and using the questionnaire Female supervisors will be recruited among the trainees based on their activity during the training and experience in data collection, and will be trained on how to supervise. Male population Male high school graduates who are fluent in the local languages will be selected. Selection and training interviewers will follow similar procedure as in the case of the female data collectors. 24
32 Jimma zones Rural Urban 13 woredas 10 woredas Jimma Town 18 kebele s 3 woredas 3 woredas 27 kebeles 3 kebeles 3 kebele s 27 kebeles 2497 households 2497 househo lds 277 households 277 house holds 2497 individuals 2497 individu als 277 individuals 277 indivi duals Female Male Fig 6.Diagrammatic representation of the steps of the sampling 25
33 5.3.8 Data quality control To ensure the quality of data various measures will be taken at different levels of the study. During data collection each interviewer will be closely supervised and monitored by using performance indicators such as response rate, number of completed interviews and rate of identification of physical violence. The supervisors randomly check, with out warning, some of the house holds. Questionnaires will be checked for completeness and consistency by data collectors and supervisors every day; questionnaires with incomplete information or any error will be returned to the field for correction. Double data entry and automatic control to detect mismatch will be employed Data analysis Data will be entered and analysed by using SPSS version 11.0 statistical packages. Multivariate analysis will be employed to identify risk factors Ethical considerations Researching violence implies dealing with sensitive issue. If adequate precautions are not taken, the safety and psychological well being of both the respondents and the research team can be put in jeopardy (WHO, 2001b). By disclosing violence experiences a woman may be exposed to retaliation by her abusive partner. Furthermore, the interview may remind the respondent of her painful and frightening experiences, and this in itself can be distressing if she does not have a supportive social environment. Similarly the researcher may also be placed at risk of physical harm by abusive partners and of psychological harm by listening to painful events of abused women (Heise & Ellsberg, 2005). To address the ethical and safety issues in domestic violence research, the World Health Organization has published guideline (WHO, 2001b). Based on this guideline, the following ethical and safety measures will be followed. The survey will not be introduced to the household and wider community as a survey of violence. Instead, at this level the study will be framed as a study on 26
34 women s and men s health and life experiences. However, the woman herself will be fully informed about the nature of the questions. Before initiating the interview informed consent will be obtained. At this stage the sensitivity of the research topic and confidentiality of the responses will be raised and discussed. Interviews will be conducted only in a private setting. The participant will be allowed to reschedule (or relocate) the interview to a time (or place) that may be more safe or convenient for her. Only one woman per household should be interviewed about his experiences of domestic violence. During the course of the interview, the interviewer will introduce any section enquiring about violence carefully, forewarning the respondent about the nature of the questions and giving her the opportunity to either stop the interview, or not to answer these questions. Interviewers will be trained to terminate or change the subject of discussion if an interview is interrupted by anyone including children. As a possible strategy, a short diversionary questionnaire on a less sensitive topic concerning women s health will be developed to assist with this. The interviewer can then forewarn the respondent that she will start to discuss this other topic if an interview is interrupted, and if needed, turn to the diversionary questionnaire. To ensure safety of the interviewers, a trusted male escort (selected by the kebele office) will be assigned to accompany the interviewer team. All interviewers will receive strict instructions about the importance of maintaining confidentiality during their training. To make it firm, no interviewers will conduct interviews in their own community. No names will be written on questionnaires. Instead, unique codes will be used to distinguish questionnaires. Identifiers used to link a questionnaire with the household location or respondent will be kept separately from the questionnaires, and upon completion of the research, destroyed. To reduce the possible distress caused to the participants by the research questions, interviewers will be trained on how to forward questions in supportive 27
35 and non-judgmental manner. In addition, care will be taken to ensure that the language of the questionnaire will not be interpreted as being judgmental, blaming or stigmatizing. Those women or men identified as in need of help will be referred to the nearby health facility and Jimma university hospital 28
36 References Abrahams, N., Jewkes, R., Hoffman, M., Laubsher, R., Sexual violence against intimate partners in Cape Town: prevalence and risk factors reported by men. Bull World Health Organ; 82(5), Almanacs, 2006.Ethiopia: country profile. Available at; (Accessed April 2006) American College of Emergency Physicians,2003. Domestic violence. Dallas,ACEP. Available from: (Accessed Feb. 2006) Campbell, J.C., Health consequences of intimate partner violence. The Lancet; 359(9314), CIA, 2005.The world fact book. Central Intelligence Agency. Available from: (Accessed Feb 2006) CSA, National statistics. Addis Ababa, Central Statistical Agency. Available from: (Accessed Feb 2006) Dunkle, KL., Jewkes, RK., Brown, HC., Gray, GE., McIntryre, JA., Harlow, SD., 2004.Gender-based violence, relationship power, and risk of HIV infection in women attending antenatal clinics in South Africa. The Lancet; 363(9419), Ellsberg, M., Heise, L.,2005.Researching violence against women: a practical guide for researchers and activists. Washington DC; WHO, PATH. Gossaye Y., Deyessa N., Berhane Y., Ellsberg M., Emmelin M., Ashenafi M., Alem A., Negash A., Kebede D., Kullgren G., Hogberg U., Women s Health and Life Events Study in Rural Ethiopia. Ethiopian Journal of Health Development; 17. Heise, L., Ellsberg, M., Gottemoeller, M., Ending violence aginst women. Population reports Series L, No. 11. Baltimore, Johns Hopkins University School of Public Health. Hotaling, G.T., Sugarman, D.B., An analysis of risk markers in husband to wife violence: the current state of knowledge. Violence victims; 1(2), HRW, Women s rights. New York, Human Rights Watch. Available from: (Accessed Jan 2006) Jejeebhoy,S.,1998. Associations between wife-beating and fetal and infant death: impressions from a survey in rural India. Stud Fam Plann;29(3):
37 Jewkes, R., Intimate partner violence: causes and prevention. The lancet; 359 (9315), Leserman, J., LI, Z.,et al., Selected symptoms with sexual and physical abuse history among female patients with gastrointestinal disorders: the impact on subsequent health care visits. Psychol med; 28(2): Linda, E., Saltzman, Johnson, D., 1996.CDC s family and intimate violence prevention team: basing programs on sciences. Journal of American Medical Women s association,50(3), Martin, S., Moracco, K., Garro, J., Tsui, O., Kupper, L., Chase, L., Campbell,J., 2002.Domestic violence across generations: findings from northern India. International Journal of Epidemiology;31: Michael A.K., Tom L., et al., Domestic violence in rural Uganda: evidence from a community-based study. Bull World Health Organ.; 81(1):53-60 Nata,D., Madhabika,N., Keera A., Links between masculinity and violence:aggregate analysis. Washigton D.C.:International Center for Research on Women. UN, Declaration on elimination of violence against women. New York: United Nation UN Beijing declaration and platform for action. New York: United Nations division for the advancement of Women. Available from: (Accessed April 2006) UN, Ethiopia National Action Plan. Women watch. Available from: (Accessed Feb 2006) UN, 2006a. Short history of CEDAW convention. New York. United Nations Department of Public Information. Available from: (Accessed Jan 2006) UN, 2006b. Convention on the Elimination of All Forms of Discrimination Against Women. New York: United Nations Division for the Advancement of Women Department of Economic and Social Affairs. Available from: (accessed march 2006) UNDP-ET, Poverty reduction. Addis Ababa,United Nation Development Programme in Ethiopia. Available from: (Accessed Feb 2006) 30
38 UNIFEM, 2005.Violence against women around the world. New York, United Nation Development Fund for Women. Available from: (Accessed Jan 2006) Valladares, E., Partner violence during pregnancy psychological factors and child outcome in Nicaragua. Ph D Thesis. Umeå University. Watts, C., Zimmerman, C., Violence against women: global scope and magnitude. The Lancet; 359(9313), WHO, 1991.World health statistics; epidemiological and statistical methods for rapid health assessment. Geneva; WHO WHO, 2001a.Violence against women. Fact sheet; 239 WHO, 2001b. Putting women first: ethical and safety recommendations for research on domestic violence against women. Geneva: WHO WHO, 2001c. Women s health: west pacifi region. Geneva:WHO WHO, World report on violence and health. Geneva: WHO WHO, WHO multi-country study on women s health and domestic violence against women: Initial results on prevalence, health outcomes and women s responses. Geneva: WHO Wilt, S.,Olson, S., Prevalence of domestic violence in the United states. Journal of American Medical Women s association;51 (3), World Bank, World Development Report: Investing in Health. New York, Oxford University Press. World Bank, 1998.Implementing the Ethiopian Policy for Women : Institutional and Regulatory Issue. Washington DC, World Bank. file/az/women-1.htm 31

39 ANNEX Women questionnaire 32
40 33
41 34
42 35
43 36

44 37
45 38
46 39
47 40
48 41
49 42
50 43
51 44
52 45
53 46

54 47
55 48
56 49
57 50
58 51
59 52
60 53
VIOLENCE PREVENTION ALLIANCE TERMS OF REFERENCE
 VIOLENCE PREVENTION ALLIANCE TERMS OF REFERENCE Background Each year, around 520,000 people die as a result of interpersonal violence, which includes child maltreatment, youth violence, intimate partner
VIOLENCE PREVENTION ALLIANCE TERMS OF REFERENCE Background Each year, around 520,000 people die as a result of interpersonal violence, which includes child maltreatment, youth violence, intimate partner
Follow-up to the Second World Assembly on Ageing Inputs to the Secretary-General s report, pursuant to GA resolution 65/182
 Follow-up to the Second World Assembly on Ageing Inputs to the Secretary-General s report, pursuant to GA resolution 65/182 The resolution clearly draws attention to the need to address the gender dimensions
Follow-up to the Second World Assembly on Ageing Inputs to the Secretary-General s report, pursuant to GA resolution 65/182 The resolution clearly draws attention to the need to address the gender dimensions
WOMEN: MEETING THE CHALLENGES OF HIV/AIDS
 WOMEN: MEETING THE CHALLENGES OF HIV/AIDS gender equality and the empowerment of women are fundamental elements in the reduction of the vulnerability of women and girls to HIV/AIDS Article 14, Declaration
WOMEN: MEETING THE CHALLENGES OF HIV/AIDS gender equality and the empowerment of women are fundamental elements in the reduction of the vulnerability of women and girls to HIV/AIDS Article 14, Declaration
Economic and Social Council
 United Nations E/CN.6/2010/L.6 Economic and Social Council Distr.: Limited 9 March 2010 Original: English ADOPTED 12 March 2010 ADVANCE UNEDITED VERSION Commission on the Status of Women Fifty-fourth session
United Nations E/CN.6/2010/L.6 Economic and Social Council Distr.: Limited 9 March 2010 Original: English ADOPTED 12 March 2010 ADVANCE UNEDITED VERSION Commission on the Status of Women Fifty-fourth session
STATEMENT BY ADVOCATE DOCTOR MASHABANE DEPUTY PERMANENT REPRESENTATIVE OF THE REPUBLIC OF SOUTH AFRICA
 PERMANENT MISSION OF SOUTH AFRICA TO THE UNITED NATIONS 333 EAST 38TH STREET 9TH FLOOR NEW YORK, NY 10016 Tel: (212) 213-5583 Fax: (212) 692-2498 E-mail: pmun@southafrica-newyork.net STATEMENT BY ADVOCATE
PERMANENT MISSION OF SOUTH AFRICA TO THE UNITED NATIONS 333 EAST 38TH STREET 9TH FLOOR NEW YORK, NY 10016 Tel: (212) 213-5583 Fax: (212) 692-2498 E-mail: pmun@southafrica-newyork.net STATEMENT BY ADVOCATE
Resolution adopted by the General Assembly on 18 December [on the report of the Third Committee (A/69/481)]
![Resolution adopted by the General Assembly on 18 December [on the report of the Third Committee (A/69/481)]](/thumbs/89/97498920.jpg "Resolution adopted by the General Assembly on 18 December [on the report of the Third Committee (A/69/481)]") United Nations A/RES/69/150 General Assembly Distr.: General 17 February 2015 Sixty-ninth session Agenda item 27 (a) Resolution adopted by the General Assembly on 18 December 2014 [on the report of the
United Nations A/RES/69/150 General Assembly Distr.: General 17 February 2015 Sixty-ninth session Agenda item 27 (a) Resolution adopted by the General Assembly on 18 December 2014 [on the report of the
gender and violence 2 The incidence of violence varies dramatically by place and over time.
 gender and violence Everyone has the right to life, liberty, and the security of person (Article 3, UDHR, 1948; Articles 6.1 and 9.1, ICCPR, 1966). No one shall be subjected to... cruel, inhuman or degrading
gender and violence Everyone has the right to life, liberty, and the security of person (Article 3, UDHR, 1948; Articles 6.1 and 9.1, ICCPR, 1966). No one shall be subjected to... cruel, inhuman or degrading
Violence against Women Surveys Practice, Implementation and Decision-Making
 Violence against Women Surveys Practice, Implementation and Decision-Making Sabine Ravestijn Urban safety expert, Safer Cities Project: Port Moresby (UN-HABITAT) Port Moresby, Papua, New Guinea Summary
Violence against Women Surveys Practice, Implementation and Decision-Making Sabine Ravestijn Urban safety expert, Safer Cities Project: Port Moresby (UN-HABITAT) Port Moresby, Papua, New Guinea Summary
Key gender equality issues to be reflected in the post-2015 development framework
 13 March 2013 Original: English Commission on the Status of Women Fifty-seventh session 4-15 March 2013 Agenda item 3 (b) Follow-up to the Fourth World Conference on Women and to the twenty-third special
13 March 2013 Original: English Commission on the Status of Women Fifty-seventh session 4-15 March 2013 Agenda item 3 (b) Follow-up to the Fourth World Conference on Women and to the twenty-third special
60TH SESSION OF THE UNITED NATIONS COMMISSION ON HUMAN RIGHTS
 Statement Check against delivery 60TH SESSION OF THE UNITED NATIONS COMMISSION ON HUMAN RIGHTS Agenda item 10: Economic, social and cultural rights Geneva, 30 March 2004 First and foremost since the Joint
Statement Check against delivery 60TH SESSION OF THE UNITED NATIONS COMMISSION ON HUMAN RIGHTS Agenda item 10: Economic, social and cultural rights Geneva, 30 March 2004 First and foremost since the Joint
GENDER & HIV/AIDS. Empower Women, Halt HIV/AIDS. MAP with Statistics of Infected Women Worldwide
 Empower Women, Halt HIV/AIDS GENDER & HIV/AIDS While HIV/AIDS is a health issue, the epidemic is a gender issue. Statistics prove that both the spread and impact of HIV/AIDS are not random. HIV/AIDS disproportionately
Empower Women, Halt HIV/AIDS GENDER & HIV/AIDS While HIV/AIDS is a health issue, the epidemic is a gender issue. Statistics prove that both the spread and impact of HIV/AIDS are not random. HIV/AIDS disproportionately
FP Conference, Speke Resort and Conference Center, Munyonyo, Uganda. Getu Degu Alene (PhD) University of Gondar, Gondar, Ethiopia
 University of Gondar, Gondar, Ethiopia") Estimation of the total fertility rates and proximate determinants of fertility in North and South Gondar zones, Northwest Ethiopia : An application of the Bongaarts model Getu Degu Alene (PhD) University
Estimation of the total fertility rates and proximate determinants of fertility in North and South Gondar zones, Northwest Ethiopia : An application of the Bongaarts model Getu Degu Alene (PhD) University
Donne e addiction: La prospettiva di genere nella medicina delle dipendenze AULSS 9 Treviso 7 ottobre 2016
 Donne e addiction: La prospettiva di genere nella medicina delle dipendenze AULSS 9 Treviso 7 ottobre 2016 Alessandra Liquori O Neil Programme Officer liquori@unicri.it www.unicri.it SUSTAINABLE DEVELOPMENT
Donne e addiction: La prospettiva di genere nella medicina delle dipendenze AULSS 9 Treviso 7 ottobre 2016 Alessandra Liquori O Neil Programme Officer liquori@unicri.it www.unicri.it SUSTAINABLE DEVELOPMENT
BURKINA FASO SOCIAL INSTITUTIONS AND GENDER INDEX (BURKINA FASO-SIGI) Social Institutions & Gender Index
 Social Institutions & Gender Index") BURKINA FASO SOCIAL INSTITUTIONS AND GENDER INDEX (BURKINA FASO-SIGI) Social Institutions & Gender Index With the support of the Austrian Development Cooperation and in partnership with the Burkina Faso
BURKINA FASO SOCIAL INSTITUTIONS AND GENDER INDEX (BURKINA FASO-SIGI) Social Institutions & Gender Index With the support of the Austrian Development Cooperation and in partnership with the Burkina Faso
The Tragic Reality of Violence:
 The Tragic Reality of Violence: Has Violence Against Women Impeded Progress in s? Ali Caless & Erlina Chia At a Glance: Up to 71% of women are targeted in their lifetime Endless links to other issues Gaining
The Tragic Reality of Violence: Has Violence Against Women Impeded Progress in s? Ali Caless & Erlina Chia At a Glance: Up to 71% of women are targeted in their lifetime Endless links to other issues Gaining
SELECTED FACTORS LEADING TO THE TRANSMISSION OF FEMALE GENITAL MUTILATION ACROSS GENERATIONS: QUANTITATIVE ANALYSIS FOR SIX AFRICAN COUNTRIES
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized ENDING VIOLENCE AGAINST WOMEN AND GIRLS SELECTED FACTORS LEADING TO THE TRANSMISSION
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized ENDING VIOLENCE AGAINST WOMEN AND GIRLS SELECTED FACTORS LEADING TO THE TRANSMISSION
Commission on the Status of Women Fifty-fourth session New York, 1-12 March 2010 INTERACTIVE EXPERT PANEL
 United Nations Nations Unies Commission on the Status of Women Fifty-fourth session New York, 1-12 March 2010 INTERACTIVE EXPERT PANEL Regional Perspectives in Progress Achieved and Remaining Gaps and
United Nations Nations Unies Commission on the Status of Women Fifty-fourth session New York, 1-12 March 2010 INTERACTIVE EXPERT PANEL Regional Perspectives in Progress Achieved and Remaining Gaps and
About human nature...
 About human nature... Violence Assistant Professor Ivana Kolčić, MD, PhD ikolcic@mefst.hr Definition Epidemiology of violence - definition In the first Report on violence and health in 1996,
About human nature... Violence Assistant Professor Ivana Kolčić, MD, PhD ikolcic@mefst.hr Definition Epidemiology of violence - definition In the first Report on violence and health in 1996,
THE ENDING VIOLENCE AGAINST WOMEN AND GIRLS (EVAWG) CHALLENGE CALL FOR INNOVATIONS
 CHALLENGE CALL FOR INNOVATIONS") THE ENDING VIOLENCE AGAINST WOMEN AND GIRLS (EVAWG) CHALLENGE CALL FOR INNOVATIONS Background In partnership with UN Women, Resilient Africa Network (RAN) is implementing a project on equipping communities
THE ENDING VIOLENCE AGAINST WOMEN AND GIRLS (EVAWG) CHALLENGE CALL FOR INNOVATIONS Background In partnership with UN Women, Resilient Africa Network (RAN) is implementing a project on equipping communities
Summary of the National Plan of Action to End Violence Against Women and Children in Zanzibar
 Summary of the National Plan of Action to End Violence Against Women and Children in Zanzibar 2017 2022 Ministry of Labour, Empowerment, Elders, Youth, Women and Children (MLEEYWC) 1 Summary of the National
Summary of the National Plan of Action to End Violence Against Women and Children in Zanzibar 2017 2022 Ministry of Labour, Empowerment, Elders, Youth, Women and Children (MLEEYWC) 1 Summary of the National
Gender in Nigeria. Data from the 2013 Nigeria Demographic and Health Survey (NDHS)
") Gender in Nigeria Data from the 2013 Nigeria Demographic and Health Survey (NDHS) This report summarizes the gender-related findings of the 2013 Nigeria Demographic and Health Survey (NDHS), implemented
Gender in Nigeria Data from the 2013 Nigeria Demographic and Health Survey (NDHS) This report summarizes the gender-related findings of the 2013 Nigeria Demographic and Health Survey (NDHS), implemented
The elimination and prevention of all forms of violence against women and girls. Draft agreed conclusions
 Commission on the Status of Women 57 th session 4 15 March 2013 The elimination and prevention of all forms of violence against women and girls Draft agreed conclusions 1. The Commission on the Status
Commission on the Status of Women 57 th session 4 15 March 2013 The elimination and prevention of all forms of violence against women and girls Draft agreed conclusions 1. The Commission on the Status
Sexual Violence Research Agenda
 Sexual Violence Research Agenda To strengthen our understanding of rape and sexual violence, and ultimately prevent it, we need to ensure that the research undertaken is both priority driven and carried
Sexual Violence Research Agenda To strengthen our understanding of rape and sexual violence, and ultimately prevent it, we need to ensure that the research undertaken is both priority driven and carried
List of issues and questions with regard to the consideration of periodic reports
 United Nations Convention on the Elimination of All Forms of Discrimination against Women CEDAW/C/BFA/Q/6 Distr.: General 6 April 2010 Original: English Committee on the Elimination of Discrimination against
United Nations Convention on the Elimination of All Forms of Discrimination against Women CEDAW/C/BFA/Q/6 Distr.: General 6 April 2010 Original: English Committee on the Elimination of Discrimination against
Science Journal of Public Health
 Science Journal of Public Health 2014; 2(6): 507-512 Published online October 30, 2014 (http://www.sciencepublishinggroup.com/j/sjph) doi: 10.11648/j.sjph.20140206.11 ISSN: 2328-7942 (Print); ISSN: 2328-7950
Science Journal of Public Health 2014; 2(6): 507-512 Published online October 30, 2014 (http://www.sciencepublishinggroup.com/j/sjph) doi: 10.11648/j.sjph.20140206.11 ISSN: 2328-7942 (Print); ISSN: 2328-7950
Resolution adopted by the Human Rights Council on 30 September /18. Preventable maternal mortality and morbidity and human rights
 United Nations General Assembly Distr.: General 10 October 2016 A/HRC/RES/33/18 Original: English Human Rights Council Thirty-third session Agenda item 3 Resolution adopted by the Human Rights Council
United Nations General Assembly Distr.: General 10 October 2016 A/HRC/RES/33/18 Original: English Human Rights Council Thirty-third session Agenda item 3 Resolution adopted by the Human Rights Council
DRAFT: Sexual and Reproductive Rights and Health the Post-2015 Development Agenda
 DRAFT: Sexual and Reproductive Rights and Health the Post-2015 Development Agenda This draft working paper considers sexual and reproductive health and rights in the context of the post- 2015 framework.
DRAFT: Sexual and Reproductive Rights and Health the Post-2015 Development Agenda This draft working paper considers sexual and reproductive health and rights in the context of the post- 2015 framework.
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 United Nations DP/FPA/CPD/BRA/5 Executive Board of the United Nations Development Programme, the United Nations Population Fund the United Nations Office for Project Services Distr.: General 26 September
United Nations DP/FPA/CPD/BRA/5 Executive Board of the United Nations Development Programme, the United Nations Population Fund the United Nations Office for Project Services Distr.: General 26 September
24 th session. Kazakhstan
 24 th session Kazakhstan 68. The Committee considered the initial report of Kazakhstan (CEDAW/C/KAZ/1) at its 490th, 491st and 497th meetings, on 18 and 23 January 2001 (see CEDAW/C/SR.490, 491 and 497).
24 th session Kazakhstan 68. The Committee considered the initial report of Kazakhstan (CEDAW/C/KAZ/1) at its 490th, 491st and 497th meetings, on 18 and 23 January 2001 (see CEDAW/C/SR.490, 491 and 497).
A user s perspective on key gaps in gender statistics and gender analysis *
 UNITED NATIONS SECRETARIAT ESA/STAT/AC.122/10 Department of Economic and Social Affairs December 2006 Statistics Division English only Inter-Agency and Expert Group Meeting on the Development of Gender
UNITED NATIONS SECRETARIAT ESA/STAT/AC.122/10 Department of Economic and Social Affairs December 2006 Statistics Division English only Inter-Agency and Expert Group Meeting on the Development of Gender
ADVANCE UNEDITED E/CN.6/2008/L.5/REV.1. Women, the girl child and HIV/AIDS * *
 E/CN.6/2008/L.5/REV.1 ADVANCE UNEDITED Women, the girl child and HIV/AIDS The Commission on the Status of Women, Reaffirming the Beijing Declaration 1 and Platform for Action, 2 the outcome documents of
E/CN.6/2008/L.5/REV.1 ADVANCE UNEDITED Women, the girl child and HIV/AIDS The Commission on the Status of Women, Reaffirming the Beijing Declaration 1 and Platform for Action, 2 the outcome documents of
Eliminating Violence Against Women
 Eliminating Violence Against Women Topic Background One of the most common forms of gender-based violence (GBV) is against women. Physical, sexual, and psychological violence threaten women s health and
Eliminating Violence Against Women Topic Background One of the most common forms of gender-based violence (GBV) is against women. Physical, sexual, and psychological violence threaten women s health and
The Policy and Legal Framework Protecting the Rights of Women and Girls in Ethiopia & Reducing their Vulnerability to HIV/AIDS. An Advocacy Toolkit
 1 The Policy and Legal Framework Protecting the Rights of Women and Girls in Ethiopia & Reducing their Vulnerability to HIV/AIDS An Advocacy Toolkit 2 Women and Girls and HIV/AIDS: the Global Context HIV/AIDS
1 The Policy and Legal Framework Protecting the Rights of Women and Girls in Ethiopia & Reducing their Vulnerability to HIV/AIDS An Advocacy Toolkit 2 Women and Girls and HIV/AIDS: the Global Context HIV/AIDS
Standards for Sexuality Education in Europe: Frequently asked questions
 Standards for Sexuality Education in Europe: Frequently asked questions 1. What is holistic sexuality education? From a global perspective, sexuality education programmes can basically be grouped into
Standards for Sexuality Education in Europe: Frequently asked questions 1. What is holistic sexuality education? From a global perspective, sexuality education programmes can basically be grouped into
Statement of Patrizia DiGiovanni, Representative a.i. On the occasion of the National Launch of the AU- Ending Child Marriage Campaign
 Statement of Patrizia DiGiovanni, Representative a.i. On the occasion of the National Launch of the AU- Ending Child Marriage Campaign African Union Commission 25 November 2014, 09:00 Excellency Minister
Statement of Patrizia DiGiovanni, Representative a.i. On the occasion of the National Launch of the AU- Ending Child Marriage Campaign African Union Commission 25 November 2014, 09:00 Excellency Minister
IFMSA Policy Statement Ending AIDS by 2030
 IFMSA Policy Statement Ending AIDS by 2030 Proposed by IFMSA Team of Officials Puebla, Mexico, August 2016 Summary IFMSA currently acknowledges the HIV epidemic as a major threat, which needs to be tackled
IFMSA Policy Statement Ending AIDS by 2030 Proposed by IFMSA Team of Officials Puebla, Mexico, August 2016 Summary IFMSA currently acknowledges the HIV epidemic as a major threat, which needs to be tackled
Adult Perpetrators. Chapter 10
 Adult Perpetrators Chapter 10 INTRODUCTION Since 1993, the rate of nonfatal intimate partner violence has declined. Decline due to: Improved services for battered women Criminalization of intimate partner
Adult Perpetrators Chapter 10 INTRODUCTION Since 1993, the rate of nonfatal intimate partner violence has declined. Decline due to: Improved services for battered women Criminalization of intimate partner
CHAPTER 3: METHODOLOGY
 CHAPTER 3: METHODOLOGY 3.1 Introduction This study is a secondary data analysis of the 1998 South African Demographic and Health Survey (SADHS) data set of women and households. According to the SADHS
CHAPTER 3: METHODOLOGY 3.1 Introduction This study is a secondary data analysis of the 1998 South African Demographic and Health Survey (SADHS) data set of women and households. According to the SADHS
SEXUAL AND REPRODUCTIVE HEALTH RIGHTS OF WOMEN LIVING WITH HIV IN SOUTH AFRICA
 SEXUAL AND REPRODUCTIVE HEALTH RIGHTS OF WOMEN LIVING WITH HIV IN SOUTH AFRICA Sexuality, Poverty and Law Alexandra Muller and Hayley MacGregor January 2014 The IDS programme on Strengthening Evidence-based
SEXUAL AND REPRODUCTIVE HEALTH RIGHTS OF WOMEN LIVING WITH HIV IN SOUTH AFRICA Sexuality, Poverty and Law Alexandra Muller and Hayley MacGregor January 2014 The IDS programme on Strengthening Evidence-based
ON THE STATUS OF THE GIRL
 ON THE STATUS OF THE GIRL CHILD IN EAST AFRICA ON GENDER INEQUALITIES IN EDUCATION IN EAST AFRICA 1 BY THE EAST AFRICAN SUB-REGIONAL SUPPORT INITIATIVE FOR THE ADVANCEMENT OF WOMEN (EASSI) TOWARDS AN EAST
ON THE STATUS OF THE GIRL CHILD IN EAST AFRICA ON GENDER INEQUALITIES IN EDUCATION IN EAST AFRICA 1 BY THE EAST AFRICAN SUB-REGIONAL SUPPORT INITIATIVE FOR THE ADVANCEMENT OF WOMEN (EASSI) TOWARDS AN EAST
Executive Board of the United Nations Development Programme and of the United Nations Population Fund
 United Nations DP/FPA/CPD/TGO/5 Executive Board of the United Nations Development Programme and of the United Nations Population Fund Distr.: General 12 October 2007 Original: English UNITED NATIONS POPULATION
United Nations DP/FPA/CPD/TGO/5 Executive Board of the United Nations Development Programme and of the United Nations Population Fund Distr.: General 12 October 2007 Original: English UNITED NATIONS POPULATION
KAMPALA DECLARATION ON WOMEN AND THE SUSTAINABLE DEVELOPMENT GOALS IN EAST AND HORN OF AFRICA, OCTOBER 2016
 KAMPALA DECLARATION ON WOMEN AND THE SUSTAINABLE DEVELOPMENT GOALS IN EAST AND HORN OF AFRICA, OCTOBER 2016 Key message: Prioritise Investment in Women and Girls in the Eastern African Sub- Region and
KAMPALA DECLARATION ON WOMEN AND THE SUSTAINABLE DEVELOPMENT GOALS IN EAST AND HORN OF AFRICA, OCTOBER 2016 Key message: Prioritise Investment in Women and Girls in the Eastern African Sub- Region and
Violence against women and girls in LAC and recent health system mandates
 Violence against women and girls in LAC and recent health system mandates ALESSANDRA GUEDES Regional Advisor, Family Violence PAHO/WHO, Washington, DC December 5, 2016 Outline of the presentation Violence
Violence against women and girls in LAC and recent health system mandates ALESSANDRA GUEDES Regional Advisor, Family Violence PAHO/WHO, Washington, DC December 5, 2016 Outline of the presentation Violence
1
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 1 Surety bonds or other instruments issued by non-bank Financial Institutions are least preferred by UNDP. Unless stated otherwise, they shall be considered unacceptable
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 1 Surety bonds or other instruments issued by non-bank Financial Institutions are least preferred by UNDP. Unless stated otherwise, they shall be considered unacceptable
STATEMENT BY HON. NAKADAMA RUKIA ISANGA MINISTER FOR GENDER, LABOUR AND SOCIAL DEVELOPMENT OF THE REPUBLIC OF UGANDA UNITED NATIONS, NEWYORK
 STATEMENT BY HON. NAKADAMA RUKIA ISANGA MINISTER FOR GENDER, LABOUR AND SOCIAL DEVELOPMENT OF THE REPUBLIC OF UGANDA AT THE 59 TH SESSION OF THE COMMISSION ON THE STATUS OF WOMEN UNITED NATIONS, NEWYORK
STATEMENT BY HON. NAKADAMA RUKIA ISANGA MINISTER FOR GENDER, LABOUR AND SOCIAL DEVELOPMENT OF THE REPUBLIC OF UGANDA AT THE 59 TH SESSION OF THE COMMISSION ON THE STATUS OF WOMEN UNITED NATIONS, NEWYORK
SUSTAINABLE DEVELOPMENT GOALS
 SUSTAINABLE DEVELOPMENT GOALS (SDGs) ETHIOPIA FACT SHEET JULY 2017 Federal Democratic Republic of Ethiopia Central Statistical Agency (CSA) Demographics Indicator Source Value Total population 2017 Projection
SUSTAINABLE DEVELOPMENT GOALS (SDGs) ETHIOPIA FACT SHEET JULY 2017 Federal Democratic Republic of Ethiopia Central Statistical Agency (CSA) Demographics Indicator Source Value Total population 2017 Projection
Visionary Development Goal on Sexual and Reproductive Health & Rights
 Visionary Development Goal on Sexual and Reproductive Health & Rights Sexual and reproductive health and rights (SRHR) are inter-linked to all key development agendas and are central to human health and
Visionary Development Goal on Sexual and Reproductive Health & Rights Sexual and reproductive health and rights (SRHR) are inter-linked to all key development agendas and are central to human health and
OBSTETRIC FISTULA. Introduction WHEN CHILDBIRTH HARMS: 1 Updated with technical feedback December 2012
 WHEN CHILDBIRTH HARMS: OBSTETRIC FISTULA Updated with technical feedback December 2012 Introduction Obstetric fistula is a preventable and in most cases, treatable childbirth injury that leaves women incontinent,
WHEN CHILDBIRTH HARMS: OBSTETRIC FISTULA Updated with technical feedback December 2012 Introduction Obstetric fistula is a preventable and in most cases, treatable childbirth injury that leaves women incontinent,
Convention on the Elimination of All Forms of Discrimination against Women
 United Nations CEDAW/C/MOZ/Q/2 Convention on the Elimination of All Forms of Discrimination against Women Distr.: General 5 October 2006 Original: English Committee on the Elimination of Discrimination
United Nations CEDAW/C/MOZ/Q/2 Convention on the Elimination of All Forms of Discrimination against Women Distr.: General 5 October 2006 Original: English Committee on the Elimination of Discrimination
Progress in Human Reproduction Research. UNDP/UNFPA/WHO/World Bank. (1) Who s Work in Reproductive Health: The Role of the Special Program
 Who s Work in Reproductive Health: The Role of the Special Program") UNDP/UNFPA/WHO/World Bank Special Programme of Research, Developemnt and Research Training in Human Reproductive (HRP). WHO's work in reproductive health: the role of the Special Programme. Progress in
UNDP/UNFPA/WHO/World Bank Special Programme of Research, Developemnt and Research Training in Human Reproductive (HRP). WHO's work in reproductive health: the role of the Special Programme. Progress in
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 12 July 2011 Original:
United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 12 July 2011 Original:
Information, Education, and Health Needs of Youth with Special Needs in Sub-Saharan Africa for Achieving Millennium Development Goals
 EUROPEAN ACADEMIC RESEARCH, VOL. I, ISSUE 6/ SEPEMBER 2013 ISSN 2286-4822, www.euacademic.org IMPACT FACTOR: 0.485 (GIF) Information, Education, and Health Needs of Youth with Special Needs in Sub-Saharan
EUROPEAN ACADEMIC RESEARCH, VOL. I, ISSUE 6/ SEPEMBER 2013 ISSN 2286-4822, www.euacademic.org IMPACT FACTOR: 0.485 (GIF) Information, Education, and Health Needs of Youth with Special Needs in Sub-Saharan
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 Executive Board of the Development Programme, the Population Fund and the United Nations Office for Project Services Distr.: General 31 July 2014 Original: English Second regular session 2014 2 to 5 September
Executive Board of the Development Programme, the Population Fund and the United Nations Office for Project Services Distr.: General 31 July 2014 Original: English Second regular session 2014 2 to 5 September
XI. MISSING LINKS: GENDER EQUALITY, THE MDGS, AND THE INTERNATIONAL CONFERENCE ON POPULATION AND DEVELOPMENT
 XI. MISSING LINKS: GENDER EQUALITY, THE MDGS, AND THE INTERNATIONAL CONFERENCE ON POPULATION AND DEVELOPMENT Hilary Anderson United Nations International Research and Training Institute for the Advancement
XI. MISSING LINKS: GENDER EQUALITY, THE MDGS, AND THE INTERNATIONAL CONFERENCE ON POPULATION AND DEVELOPMENT Hilary Anderson United Nations International Research and Training Institute for the Advancement
Preventing and responding to violence against women Dr Avni Amin Department of Reproductive Health and Research, World Health Organization
 Preventing and responding to violence against women Dr Avni Amin Department of Reproductive Health and Research, World Health Organization Training course in adolescent sexual and reproductive health 2018
Preventing and responding to violence against women Dr Avni Amin Department of Reproductive Health and Research, World Health Organization Training course in adolescent sexual and reproductive health 2018
American Journal of Health Research
 American Journal of Health Research 2014; 2(4): 113-117 Published online July 30, 2014 (http://www.sciencepublishinggroup.com/j/ajhr) doi: 10.11648/j.ajhr.20140204.12 ISSN: 2330-8788 (Print); ISSN: 2330-8796
American Journal of Health Research 2014; 2(4): 113-117 Published online July 30, 2014 (http://www.sciencepublishinggroup.com/j/ajhr) doi: 10.11648/j.ajhr.20140204.12 ISSN: 2330-8788 (Print); ISSN: 2330-8796
Gender Profile: Mozambique
 General Total male population under 15 (2014) (CIA, 2015): 5,627,116 Total female population under 15 (2014) (CIA, 2015): 5,566,260 Total male population over 15 (2014) (CIA, 2015): 6,416,394 Total female
General Total male population under 15 (2014) (CIA, 2015): 5,627,116 Total female population under 15 (2014) (CIA, 2015): 5,566,260 Total male population over 15 (2014) (CIA, 2015): 6,416,394 Total female
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 United Nations DP/FPA/CPD/JOR/8 Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 6 August
United Nations DP/FPA/CPD/JOR/8 Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 6 August
ASSESSMENT OF EFFECTIVE COVERAGE OF HIV PREVENTION OF PREGNANT MOTHER TO CHILD TRANSIMISSION SERVICES IN JIMMA ZONE, SOUTH WEST ETHIOPIA
 ORIGINAL ARTICLE Assessment of Effective Coverage of HIV Mohammed H. et al ASSESSMENT OF EFFECTIVE COVERAGE OF HIV PREVENTION OF PREGNANT MOTHER TO CHILD TRANSIMISSION SERVICES IN JIMMA ZONE, SOUTH WEST
ORIGINAL ARTICLE Assessment of Effective Coverage of HIV Mohammed H. et al ASSESSMENT OF EFFECTIVE COVERAGE OF HIV PREVENTION OF PREGNANT MOTHER TO CHILD TRANSIMISSION SERVICES IN JIMMA ZONE, SOUTH WEST
WOMEN S REPRODUCTIVE HEALTH AS A GENDER, DEVELOPMENT AND HUMAN RIGHTS ISSUE: REGAINING PERSPECTIVE
 WOMEN S REPRODUCTIVE HEALTH AS A GENDER, DEVELOPMENT AND HUMAN RIGHTS ISSUE: REGAINING PERSPECTIVE Monique V. Chireau, MD, MPH Assistant Professor, Division of Clinical and Epidemiologic Research Department
WOMEN S REPRODUCTIVE HEALTH AS A GENDER, DEVELOPMENT AND HUMAN RIGHTS ISSUE: REGAINING PERSPECTIVE Monique V. Chireau, MD, MPH Assistant Professor, Division of Clinical and Epidemiologic Research Department
The Millennium Development Goals Report. asdf. Gender Chart UNITED NATIONS. Photo: Quoc Nguyen/ UNDP Picture This
 The Millennium Development Goals Report Gender Chart asdf UNITED NATIONS Photo: Quoc Nguyen/ UNDP Picture This Goal Eradicate extreme poverty and hunger Women in sub- are more likely than men to live in
The Millennium Development Goals Report Gender Chart asdf UNITED NATIONS Photo: Quoc Nguyen/ UNDP Picture This Goal Eradicate extreme poverty and hunger Women in sub- are more likely than men to live in
Summary of findings, conclusions and areas for further research
 82 CHAPTER 10 1 The study has now also been completed in New Zealand. 2 The deviations from the standard protocol and questionnaire as implemented in Ethiopia, Japan, and Serbia and Montenegro, are specified
82 CHAPTER 10 1 The study has now also been completed in New Zealand. 2 The deviations from the standard protocol and questionnaire as implemented in Ethiopia, Japan, and Serbia and Montenegro, are specified
Intersections of Domestic Violence and Sexual Assault ext ext. 17
 Intersections of Domestic Violence and Sexual Assault Rose Luna, Deputy Director, TAASA Brad Teaff, Training Specialist rluna@taasa.org bteaff@taasa.org 512-474-7190 ext. 13 512-474-7190 ext. 17 Underlying
Intersections of Domestic Violence and Sexual Assault Rose Luna, Deputy Director, TAASA Brad Teaff, Training Specialist rluna@taasa.org bteaff@taasa.org 512-474-7190 ext. 13 512-474-7190 ext. 17 Underlying
Male s Attitude on Women s Empowerment and Men as Supportive Partners in Promotion of RCH : A Study Among Slum Dwellers in Andhra Pradesh, India.
 Male s Attitude on Women s Empowerment and Men as Supportive Partners in Promotion of RCH : A Study Among Slum Dwellers in Andhra Pradesh, India. By P. Vinayaga Murthy *& V.K. Ravindra Kumar* Introduction
Male s Attitude on Women s Empowerment and Men as Supportive Partners in Promotion of RCH : A Study Among Slum Dwellers in Andhra Pradesh, India. By P. Vinayaga Murthy *& V.K. Ravindra Kumar* Introduction
National Strategy and Action Plan on Gender Equality and Domestic Violence
 REPUBLIC OF ALBANIA OF LABOUR, SOCIAL AFFAIRS AND EQUAL OPPORTUNITIES Department of Equal Opportunities Policies National Strategy and Action Plan on Gender Equality and Domestic Violence Prepared : Valbona
REPUBLIC OF ALBANIA OF LABOUR, SOCIAL AFFAIRS AND EQUAL OPPORTUNITIES Department of Equal Opportunities Policies National Strategy and Action Plan on Gender Equality and Domestic Violence Prepared : Valbona
Elimination of Violence against Women in the Pacific Islands
 Elimination of Violence against Women in the Pacific Islands Recommendations from the 12 th Triennial Conference of Pacific Women and Fifth Pacific Women s Ministerial Meeting (Rarotonga, Cook Islands,
Elimination of Violence against Women in the Pacific Islands Recommendations from the 12 th Triennial Conference of Pacific Women and Fifth Pacific Women s Ministerial Meeting (Rarotonga, Cook Islands,
XV. THE ICPD AND MDGS: CLOSE LINKAGES. United Nations Population Fund (UNFPA)
") XV. THE ICPD AND MDGS: CLOSE LINKAGES United Nations Population Fund (UNFPA) A. INTRODUCTION A global consensus emerged at the Millennium Summit, where 189 world leaders adopted the Millennium Declaration
XV. THE ICPD AND MDGS: CLOSE LINKAGES United Nations Population Fund (UNFPA) A. INTRODUCTION A global consensus emerged at the Millennium Summit, where 189 world leaders adopted the Millennium Declaration
GENDER EQUALITY AND WOMEN EMPOWERMENT: KEY TO POVERTY REDUCTION, FOOD SECURITY AND SOCIAL WELFARE
 GENDER EQUALITY AND WOMEN EMPOWERMENT: KEY TO POVERTY REDUCTION, FOOD SECURITY AND SOCIAL WELFARE Women in Triticum Awards Ceremony 2013 BGRI Technical Workshop 19-22 August, New Delhi, India Agriculture
GENDER EQUALITY AND WOMEN EMPOWERMENT: KEY TO POVERTY REDUCTION, FOOD SECURITY AND SOCIAL WELFARE Women in Triticum Awards Ceremony 2013 BGRI Technical Workshop 19-22 August, New Delhi, India Agriculture
COUNTRY POLICIES AND STRATEGIES FOR COMBATING GBV. Policies/ Plans. Development Plan in the 10th National Economic and Social Development Plan
 Thailand COUNTRY POLICIES AND STRATEGIES FOR COMBATING GBV Legal framework! The Protection of Domestic Violence Victims Act B.E. 55 (7) was announced in the Royal Gazette on August 14, 7, and was enacted
Thailand COUNTRY POLICIES AND STRATEGIES FOR COMBATING GBV Legal framework! The Protection of Domestic Violence Victims Act B.E. 55 (7) was announced in the Royal Gazette on August 14, 7, and was enacted
Checklist for assessing the gender responsiveness of sexual and reproductive health policies. Pilot document for adaptation to national contexts
 Checklist for assessing the gender responsiveness of sexual and reproductive health policies Pilot document for adaptation to national contexts Address requests about publications of the WHO Regional Office
Checklist for assessing the gender responsiveness of sexual and reproductive health policies Pilot document for adaptation to national contexts Address requests about publications of the WHO Regional Office
Violence Against Women Statistics: Latest Guidelines and Data
 Violence Against Women Statistics: Latest Guidelines and Data 5 th Global Forum on Gender Statistics, 3-5 November 2014, Aguascalientes, Mexico Overview of Presentation Overview of Guidelines on producing
Violence Against Women Statistics: Latest Guidelines and Data 5 th Global Forum on Gender Statistics, 3-5 November 2014, Aguascalientes, Mexico Overview of Presentation Overview of Guidelines on producing
Dr. Padmini Murthy MD, MPH, MS, CHES Medical Women s International Association Webinar Feb
 Dr. Padmini Murthy MD, MPH, MS, CHES Medical Women s International Association Webinar Feb 1 2014 Learning Objectives 1.Discuss the link between women s health and factors influencing their health status
Dr. Padmini Murthy MD, MPH, MS, CHES Medical Women s International Association Webinar Feb 1 2014 Learning Objectives 1.Discuss the link between women s health and factors influencing their health status
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 15 April 2011 Original:
United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 15 April 2011 Original:
Study to assess determinants of domestic violence among women in urban slum of Mumbai
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 8, Issue 4 (Jul.- Aug. 2013), PP 18-22 Study to assess determinants of domestic violence among women
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 8, Issue 4 (Jul.- Aug. 2013), PP 18-22 Study to assess determinants of domestic violence among women
Demographics HD 300 Child Abuse & Neglect
 Demographics HD 300 Child & Neglect Unit 10 Sexual (Intra-Familial) Sexual abuse cuts across all socioeconomic levels. Offenders are usually male (97%). Victims are usually female (77%). 1 in 4 molested
Demographics HD 300 Child & Neglect Unit 10 Sexual (Intra-Familial) Sexual abuse cuts across all socioeconomic levels. Offenders are usually male (97%). Victims are usually female (77%). 1 in 4 molested
Aide Memoire. Distr.: GENERAL. E/ECA/CWD/7/inf.2 3 May 2011
 Distr.: GENERAL E/ECA/CWD/7/inf.2 3 May 2011 UNITED NATIONS ECONOMIC AND SOCIAL COUNCIL ECONOMIC COMMISSION FOR AFRICA African Centre for Gender and Social Development Original: ENGLISH Seventh Session
Distr.: GENERAL E/ECA/CWD/7/inf.2 3 May 2011 UNITED NATIONS ECONOMIC AND SOCIAL COUNCIL ECONOMIC COMMISSION FOR AFRICA African Centre for Gender and Social Development Original: ENGLISH Seventh Session
FAST FACTS. 100 TO 140 MILLION girls and women in the world have experienced female genital mutilation/ cutting.
 603 MILLION women live in countries where domestic violence is not yet considered a crime. Women and girls make up 80% of the estimated 800,000 people trafficked across national borders annually, with
603 MILLION women live in countries where domestic violence is not yet considered a crime. Women and girls make up 80% of the estimated 800,000 people trafficked across national borders annually, with
Challenges and opportunities in achieving gender equality and the empowerment of rural women and girls Draft agreed conclusions
 Commission on the Status of Women Sixty-second session 12 23 March 2018 Challenges and opportunities in achieving gender equality and the empowerment of rural women and girls Draft agreed conclusions 1.
Commission on the Status of Women Sixty-second session 12 23 March 2018 Challenges and opportunities in achieving gender equality and the empowerment of rural women and girls Draft agreed conclusions 1.
IMPLEMENTATION FRAMEWORK OF THE SOLEMN DECLARATION ON GENDER EQUALITY IN AFRICA
 AU/MIN/CONF/WG/3 (I) AFRICAN UNION UNION AFRICAINE UNIÃO AFRICANA IMPLEMENTATION FRAMEWORK OF THE SOLEMN DECLARATION ON GENDER EQUALITY IN AFRICA ADOPTED AT THE FIRST AFRICAN UNION CONFERENCE OF MINISTERS
AU/MIN/CONF/WG/3 (I) AFRICAN UNION UNION AFRICAINE UNIÃO AFRICANA IMPLEMENTATION FRAMEWORK OF THE SOLEMN DECLARATION ON GENDER EQUALITY IN AFRICA ADOPTED AT THE FIRST AFRICAN UNION CONFERENCE OF MINISTERS
II. Adolescent Fertility III. Sexual and Reproductive Health Service Integration
 Recommendations for Sexual and Reproductive Health and Rights Indicators for the Post-2015 Sustainable Development Goals Guttmacher Institute June 2015 As part of the post-2015 process to develop recommendations
Recommendations for Sexual and Reproductive Health and Rights Indicators for the Post-2015 Sustainable Development Goals Guttmacher Institute June 2015 As part of the post-2015 process to develop recommendations
RIGHTS INSITITUTE FOR SOCIAL EMPOWERMENT- RISE GENDER POLICY
 RIGHTS INSITITUTE FOR SOCIAL EMPOWERMENT- RISE GENDER POLICY JUNE, 2016 Contents 1. RATIONALE... 3 2.0. POLICY FRAMEWORK... 4 2.1. POLITICAL COMMITMENT/PRINCIPLES... 4 2.2. AREAS OF ACTION/PROGRAM GOALS...
RIGHTS INSITITUTE FOR SOCIAL EMPOWERMENT- RISE GENDER POLICY JUNE, 2016 Contents 1. RATIONALE... 3 2.0. POLICY FRAMEWORK... 4 2.1. POLITICAL COMMITMENT/PRINCIPLES... 4 2.2. AREAS OF ACTION/PROGRAM GOALS...
2016 United Nations Political Declaration on Ending AIDS sets world on the Fast-Track to end the epidemic by 2030
 S T A T E M E N T 2016 United Nations Political Declaration on Ending AIDS sets world on the Fast-Track to end the epidemic by 2030 World leaders commit to reach three goals and 20 new Fast-Track Targets
S T A T E M E N T 2016 United Nations Political Declaration on Ending AIDS sets world on the Fast-Track to end the epidemic by 2030 World leaders commit to reach three goals and 20 new Fast-Track Targets
Determinants of Modern Contraceptive Utilization among Women of the Reproductive Age Group in Dawuro Zone, SNNPR, Southern Ethiopia
 Determinants of Modern Contraceptive Utilization among Women of the Reproductive Age Group in Dawuro Zone, SNNPR, Southern Ethiopia Terefe Dodicho Wolaita Sodo University, College of health sciences and
Determinants of Modern Contraceptive Utilization among Women of the Reproductive Age Group in Dawuro Zone, SNNPR, Southern Ethiopia Terefe Dodicho Wolaita Sodo University, College of health sciences and
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 United Nations DP/FPA/CPD/LSO/6 Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 2 August
United Nations DP/FPA/CPD/LSO/6 Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 2 August
Accredi ted. hours. Accredi ted. Hours
 Women s Studies Center University of Jordan Study plan number r 2012 Study Plan for Women s Studies Masters Program Thesis Track First: general terms and conditions 1. This plan conforms to the valid regulations
Women s Studies Center University of Jordan Study plan number r 2012 Study Plan for Women s Studies Masters Program Thesis Track First: general terms and conditions 1. This plan conforms to the valid regulations
New Brunswick plan to prevent and respond to violence against Aboriginal women and girls
 New Brunswick plan to prevent and respond to violence against Aboriginal women and girls 2017-2021 New Brunswick s Plan to Prevent and Respond to Violence Against Aboriginal Women and Girls Published by:
New Brunswick plan to prevent and respond to violence against Aboriginal women and girls 2017-2021 New Brunswick s Plan to Prevent and Respond to Violence Against Aboriginal Women and Girls Published by:
Civil society participation in the WHO GBV Global Action plan development
 FEEDBACK FROM: Gladness Hemedi Munuo TAMWA Crisis Resolving Centre Coordinator Tanzania Media Women s Association (TAMWA) Facilitating the participation of civil society and experts working on SRH, gender
FEEDBACK FROM: Gladness Hemedi Munuo TAMWA Crisis Resolving Centre Coordinator Tanzania Media Women s Association (TAMWA) Facilitating the participation of civil society and experts working on SRH, gender
Model United Nations College of Charleston November 3-4, Human Rights Committee on Gender Based Violence, General Assembly of the United Nations
 Model United Nations College of Charleston November 3-4, 2017 Human Rights Committee on Gender Based Violence, General Assembly of the United Nations Draft Resolution for Committee Consideration and Recommendation
Model United Nations College of Charleston November 3-4, 2017 Human Rights Committee on Gender Based Violence, General Assembly of the United Nations Draft Resolution for Committee Consideration and Recommendation
Violence Prevention A Strategy for Reducing Health Inequalities
 Violence Prevention A Strategy for Reducing Health Inequalities Professor Mark A Bellis Centre for Public Health Liverpool John Moores University WHO Collaborating Centre for Violence Prevention Overview
Violence Prevention A Strategy for Reducing Health Inequalities Professor Mark A Bellis Centre for Public Health Liverpool John Moores University WHO Collaborating Centre for Violence Prevention Overview
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 29 September 2011 Original:
United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 29 September 2011 Original:
ON THE SITUATION OF AND RESPONSE TO HIV IN THE REGION TOWARDS UNIVERSAL ACCESS: ACHIEVEMENTS AND CHALLENGES AND REQUIRED ACTION
 In the Name of God, the Compassionate, the Merciful Address by DR HUSSEIN A. GEZAIRY REGIONAL DIRECTOR WHO EASTERN MEDITERRANEAN REGION to the CONFERENCE ON THE SITUATION OF AND RESPONSE TO HIV IN THE
In the Name of God, the Compassionate, the Merciful Address by DR HUSSEIN A. GEZAIRY REGIONAL DIRECTOR WHO EASTERN MEDITERRANEAN REGION to the CONFERENCE ON THE SITUATION OF AND RESPONSE TO HIV IN THE
Gender Country Profile
 Gender Country Profile Kenya By Erin MacDonald and Rosanne Wong Edited by Dania Sheldon Contents General... 1 Health... 2 Education... 2 Economic Activity... 3 Decision-Making... 3 Human Rights... 3 Gender
Gender Country Profile Kenya By Erin MacDonald and Rosanne Wong Edited by Dania Sheldon Contents General... 1 Health... 2 Education... 2 Economic Activity... 3 Decision-Making... 3 Human Rights... 3 Gender
Vision 2020 for Sexual and Reproductive Health and Rights
 Vision 2020 for Sexual and Reproductive Health and Rights Introduction In recent decades, the international development agenda has changed dramatically. Historic United Nations conferences and summits
Vision 2020 for Sexual and Reproductive Health and Rights Introduction In recent decades, the international development agenda has changed dramatically. Historic United Nations conferences and summits
Economic and Social Council
 United Nations Economic and Social Council Distr.: General 18 November 2014 Original: English Economic and Social Commission for Asia and the Pacific Asia-Pacific Intergovernmental Meeting on HIV and AIDS
United Nations Economic and Social Council Distr.: General 18 November 2014 Original: English Economic and Social Commission for Asia and the Pacific Asia-Pacific Intergovernmental Meeting on HIV and AIDS
Mary Ann Tarantula, Chairman Patricia Latona, Susan Westerberg, Staci Alziebler-Perkins
 ZONTA AND THE UNITED NATIONS In New York City: Mary Ann Tarantula, Chairman Patricia Latona, Susan Westerberg, Staci Alziebler-Perkins In Europe: Simone Ovart, Vice Chairman Geneva Regula Dannecker Eva-Maria
ZONTA AND THE UNITED NATIONS In New York City: Mary Ann Tarantula, Chairman Patricia Latona, Susan Westerberg, Staci Alziebler-Perkins In Europe: Simone Ovart, Vice Chairman Geneva Regula Dannecker Eva-Maria
Call for Research Proposals. School-Related Gender Based Violence in Lebanon
 Call for Research Proposals School-Related Gender Based Violence in Lebanon UNESCO Beirut 11 August 2010 INTRODUCTION Within the framework of the project Supporting Gender Equality in Education in Lebanon
Call for Research Proposals School-Related Gender Based Violence in Lebanon UNESCO Beirut 11 August 2010 INTRODUCTION Within the framework of the project Supporting Gender Equality in Education in Lebanon
MINISTRY OF WOMEN'S AND VETERANS' AFFAIRS
 HAG-057 MINISTRY OF WOMEN'S AND VETERANS' AFFAIRS THE NATIONAL POLICY FOR WOMEN, THE GIRL CHILD AND HIV/AIDS CAMBODIA NOVEMBER 1999 CONTENTS Contents 1 Introduction 2 Principles 3 The Status of Women,
HAG-057 MINISTRY OF WOMEN'S AND VETERANS' AFFAIRS THE NATIONAL POLICY FOR WOMEN, THE GIRL CHILD AND HIV/AIDS CAMBODIA NOVEMBER 1999 CONTENTS Contents 1 Introduction 2 Principles 3 The Status of Women,
A Comparative Analysis of Fertility Plateau In Egypt, Syria and Jordan: Policy Implications
 A Comparative Analysis of Fertility Plateau In Egypt, Syria and Jordan: Policy Implications Executive Summary by Hoda Rashad and Hassan Zaky Social Research Center The American University in Cairo March
A Comparative Analysis of Fertility Plateau In Egypt, Syria and Jordan: Policy Implications Executive Summary by Hoda Rashad and Hassan Zaky Social Research Center The American University in Cairo March
Demographic and Health Profile. Ethiopia. Nigeria. Population is currently 73 million, annual growth rate is 2.4%
 Adebola Adedimeji Demographic and Health Profile Nigeria Population is currently 150 million, annual growth rate is 2% Political structure- Federal Republic; 36 states, almost 800 local governments Multi-ethnic,
Adebola Adedimeji Demographic and Health Profile Nigeria Population is currently 150 million, annual growth rate is 2% Political structure- Federal Republic; 36 states, almost 800 local governments Multi-ethnic,