Protap Mukherjee 1 Lopamudra Ray Saraswati 2
|
|
|
- Melina Dickerson
- 6 years ago
- Views:
Transcription
1 Women's Health, Family Planning and Accessibility to Health Care in Rural Madhya Pradesh in India: An Insight into the NRHM Program Indicators, Spatial Disparity and Health Planning Protap Mukherjee 1 Lopamudra Ray Saraswati 2 Introduction National Rural Health Mission: Vision and Goals The National Rural Health Mission ( ) seeks to provide effective healthcare to rural population throughout the country with special focus on 18 states, which have weak public health indicators and/or weak infrastructure. These 18 States are Arunachal Pradesh, Assam, Bihar, Chhattisgarh, Himachal Pradesh, Jharkhand, Jammu & Kashmir, Manipur, Mizoram, Meghalaya, Madhya Pradesh, Nagaland, Orissa, Rajasthan, Sikkim, Tripura, Uttaranchal and Uttar Pradesh. The Mission is an articulation of the commitment of the Government to raise public spending on Health from 0.9% of GDP to 2-3% of GDP. It has as its key components provision of a female health activist in each village; a village health plan prepared through a local team headed by the Health & Sanitation Committee of the Panchayat; strengthening of the rural hospital for effective curative care and made measurable and accountable to the community through Indian Public Health Standards (IPHS); and integration of vertical Health & Family Welfare Programmes and Funds for optimal utilization of funds and infrastructure and strengthening delivery of primary healthcare. It seeks to revitalize local health traditions and mainstream AYUSH into the public health system. It aims at effective integration of health concerns with determinants of health like sanitation & hygiene, nutrition, and safe drinking water through a District Plan for Health. It seeks decentralization of programmes for district management of health. It seeks to address the inter-state and inter-district disparities, especially among the 18 high focus States. It seeks to improve access of rural people, especially poor women and children, to equitable, affordable, accountable and effective primary healthcare. The Goals of the mission are: i) Reduction in Infant Mortality Rate (IMR) and Maternal Mortality Ratio (MMR), ii) Universal access to public health services such as Women s health, child health, water, sanitation & hygiene, immunization, and Nutrition, iii) Prevention and control of communicable and non-communicable diseases, including locally endemic diseases iv) Access to integrated comprehensive primary healthcare v) Population stabilization, gender and demographic balance, vi) Revitalize local health traditions and mainstream AYUSH and vii) Promotion of healthy life styles 1 Research Associate, National Population Stabilisation Fund, New Delhi, India pmukherjee25@gmail.com and 2 Research Associate, Invest India Market Solutions Private Limited, Noida, India, lopamudrars@gmail.com.
2 Madhya Pradesh Scenarios From the point of view of per capita income, literacy, urbanization, infrastructure facilities and other development indicators, Madhya Pradesh belongs to the category of less developed states of the country. Administratively, Madhya Pradesh has 61 districts with considerable variation between districts on almost all demographic, social, and economic indicators. Madhya Pradesh is a State with a considerable degree of regional diversity in terrain, culture, socio-economic conditions and status of women. In terms of Human Development Index (HDI), the state lags behind the country as a whole, with an index value of 37 out of 100 compared to 45 for the country (PPM, Govt. of MP, 2000). The current health status of mothers and children in the state needs considerable improvement. The infant mortality rate in 1997 has been estimated at 94 infant deaths per 1,000 live births, one of the highest rates in the country. The per cent of children aged months who have received any vaccine increased from 62 per cent in to 80 per cent in in rural areas and from 80 per cent to 94 per cent in urban areas. While immunization services have successfully reached more children than six years ago, the proportion of children receiving all required doses of all vaccines has not shown appreciable improvement. The proportion of pregnant women that obtained antenatal care (ANC) services increased from 52 per cent in to 62 per cent in Only 22 per cent of deliveries in Madhya Pradesh in were institutional deliveries; of these, two-thirds occurred in private health institutions. Trained personnel assisted less than one-third of total deliveries. Skilled personnel such as doctors, midwives and trained dais attended an additional 20 per cent of births at home. Over two-thirds of births in rural areas and about one-seventh of births in urban areas occur at home attended by traditional birth attendants, who are often untrained and work under unhygienic conditions. The maternal mortality rate in the state is the highest in the country with 498 mothers dying due to maternal causes per 100,000 live births (PPM, Govt. of MP, 2000). Madhya Pradesh ranks among the lowest in the country in terms of nearly all health related indicators. There is a need to bridge the gap between the State and the national averages on priority basis. In order to provide health care to all villages, there is a need to strengthen the health infrastructure in rural, tribal and slum areas. It is proposed to bring down the Infant Mortality rate (IMR) from 91 per thousand live births to 45, reduce Maternal Mortality Rate (MMR) to 2 per thousand lives birth, reduce the total fertility rate from 4 to 3 and reduce the child mortality rate to 90 during the plan period. Specific strategies would be evolved in the area where these are very high as compared to the state average. National Rural Health Mission is being seen as a vital link to government programmes on reducing maternal mortality. They will address the health needs of rural population particularly among the vulnerable sections and guide women to access the facilities for ante-natal care, institutional delivery, post-natal care and counselling on nutrition and family planning services. Objective In this paper, the focus is concentrated in some of the indicators of NRHM. The specific objectives are: 1. To study the level of maternal health in rural Madhya Pradesh 2. To examine the effects of accessibility on maternal health care and family planning among rural women in this state
3 3. To identify the spatial pattern of disparity in maternal health care and services, and to find out the more vulnerable districts in the state. Data For the present paper, the source of data is DLHS-RCH survey, Round-II, under Reproductive and Child Health Project. The survey was conducted in two phases in 2002 and DLHS-RCH collected information on various indicators related to maternal and child health. For the present study Household file, Woman file and Village file have been taken. Out of total sample of the Madhya Pradesh, only rural women have been selected which is accounted for 69 % of the total sampled population. Methodology For the present study bi-variate and multi variate analyses have been carried out by a set of different background variables. Simple percentages have been calculated to know the basic composition and characteristics of rural women in Madhya Pradesh as revealed by DLHS- RCH-II. A composite index (Accessibility Index) based on five indicators has been developed to represent the overall accessibility of rural women in terms of distance. The following variables have been taken for calculating Accessibility Index: i) Distance to BUS stand (in KM), ii) Distance to Railway station (in KM), iii) Distance of Sub centre from village, iv) Distance of PHC from village and v) Distance of CHC/RH from village. On the basis of the calculated values Accessibility Index has been divided into three categories: i) Good (5 to 8 km), ii) Moderate (8 to 12 km), and iii) Poor (more than 12 km). Composite index like Full ANC and Safe delivery also calculated for the rural women. Four dependent variables have been selected for the multi-variate analyses which are: full ANC, Safe delivery, aware of any modern family planning method and currently using any modern family planning method. To study the effect of different socio-economic and demographic predictors on these variables, logistic regression analyses were carried out. GIS based maps have been prepared to extract the better spatial interpretation. Results and Discussions Table 1: Characteristics of Rural Women in Madhya Pradesh From this table it is clear that rural Madhya Pradesh basically consists of married women of 20 to 24 years and 25 to 29 years of age groups (23 and 21 percent, respectively). The Hinduism (97 percent) has found to the main religion among the women in rural Madhya Pradesh. Among castes, other backward class (43 percent) shows the higher percentage. Findings also reveal that majority of women (41 percent) have marital duration more than 15 years and above. More than two-fifth (44 percent) of the rural women have two to three children. Finding shows that nearly three-fourth (71 percent) of rural women is illiterate. Even most of the husbands (38 percent) are illiterate. Sixty-nine percent women in rural Madhya Pradesh belongs lo low household s standard of living. Only 44 percent women are currently using any modern family planning method. The results also reveal that 34 percent rural women have access to the availability of any public health facity in the village and only 15 percent of the women have good accessibility to any public health facity.
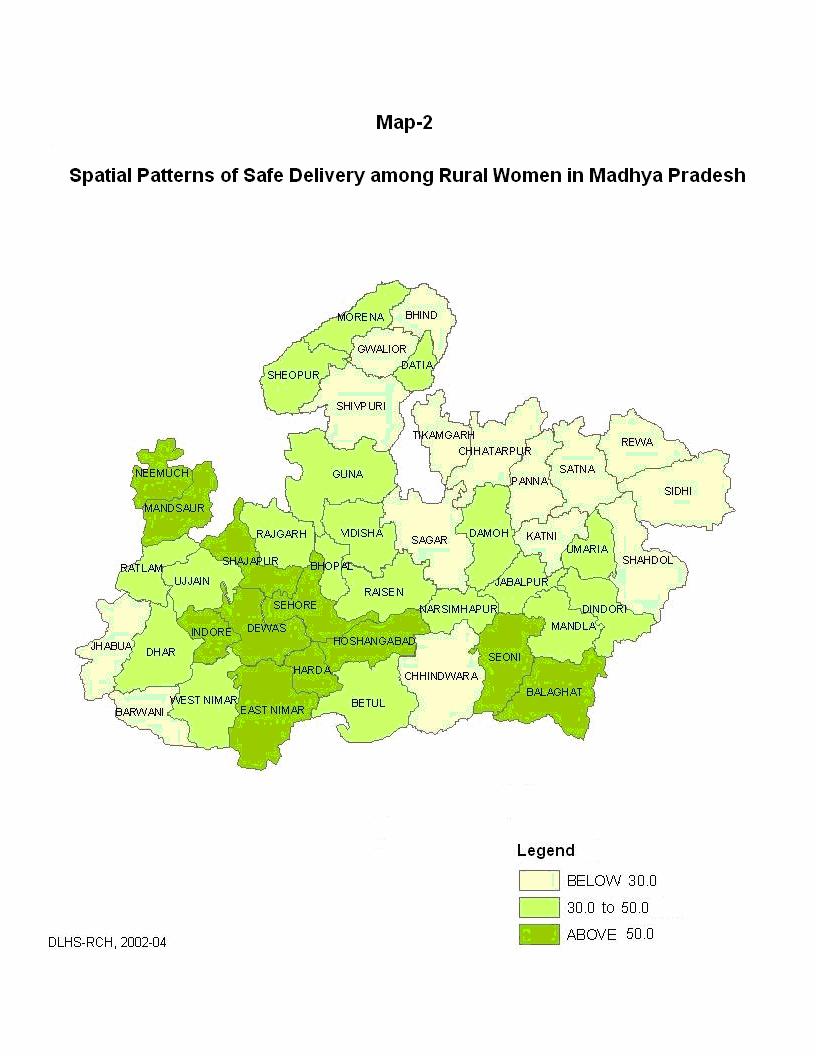
4 Table 2: Levels of Obstetric Care among Rural Women in Madhya Pradesh Any ANC: It has been found from the bi-variate analyses that the level of any ANC is higher among young currently married women, i.e. women of years of age (54 percent) and Muslim women (68 percent). Women from other caste (57 percent) have the highest percentage of any ANC. Women who have marital duration of less than 5 years and also have less than 2 children are more prone to take any ANC. Women and Husband s education and household standard of living index is positively associated with the any ANC. Accessibility also plays a positive role in obstetric care. Full ANC: though the level of full ANC is very lower among the rural women in Madhya Pradesh, it is to be found higher among women of years of age groups. The women belong to other religions and other castes are more prone to take full ANC. Like any ANC, full ANC also shows the same association regarding marital duration, education of women and husbands, SLI and levels of accessibility and availability of health facilities in the village. Safe Delivery: The results regarding safe delivery are also same like full ANC. It has positive association with women and husband s education, household s standard of living, knowledge of modern method of family planning, accessibility and availability of health facilities and negatively associated with women s age, marital duration and total children ever born. Safe delivery is found to be higher among Muslim women and women belong to other castes. Table 3: Knowledge and Use of Modern Method of Family Planning among Rural Women in Madhya Pradesh Knowledge of Modern Family Planning Method: The Bivariate analyses show that on an average; more than 95 percent rural women have knowledge about modern method of family planning. This knowledge is relatively higher among women of years of age (99 percent), women belonging to other castes (98 percent), women who married before 15 years and above (99 percent), women having more than three children (99 percent). Findings show that this knowledge also positively related with women and husband s education, household s standard of living, obstetric care and levels of accessibility and availability of health facilities. Use of Modern Family Planning Method: The study reveals that use of modern family planning method is steadily increasing with the increase in age and it reaches nearly 70 percent in the age group years. Women belong to other religions and other castes are found to use more this method in comparison to their other counterparts. Women and husband s education though do not show strong relationship with the use of current methods. Interestingly, it is found higher among illiterate women and husbands. Obstetric care, levels of accessibility and availability of health facilities have strong influences on the use of current family planning methods. Table 4 and Table 5, Map-1 and Map-2: Variation in the Spatial Pattern of the Different Indicators of Maternal Health Care among Rural Women in Madhya Pradesh There is a wide regional disparity in different maternal health and health care indicators in rural Madhya Pradesh. It has been found that the percentage of rural women having any ANC is lowest and highest respectively in Sidhi and Balaghat districts. Full ANC is lower among women of Shivpuri (0.4 percent) and it is highest in district Seoni. Map-1 shows that south-
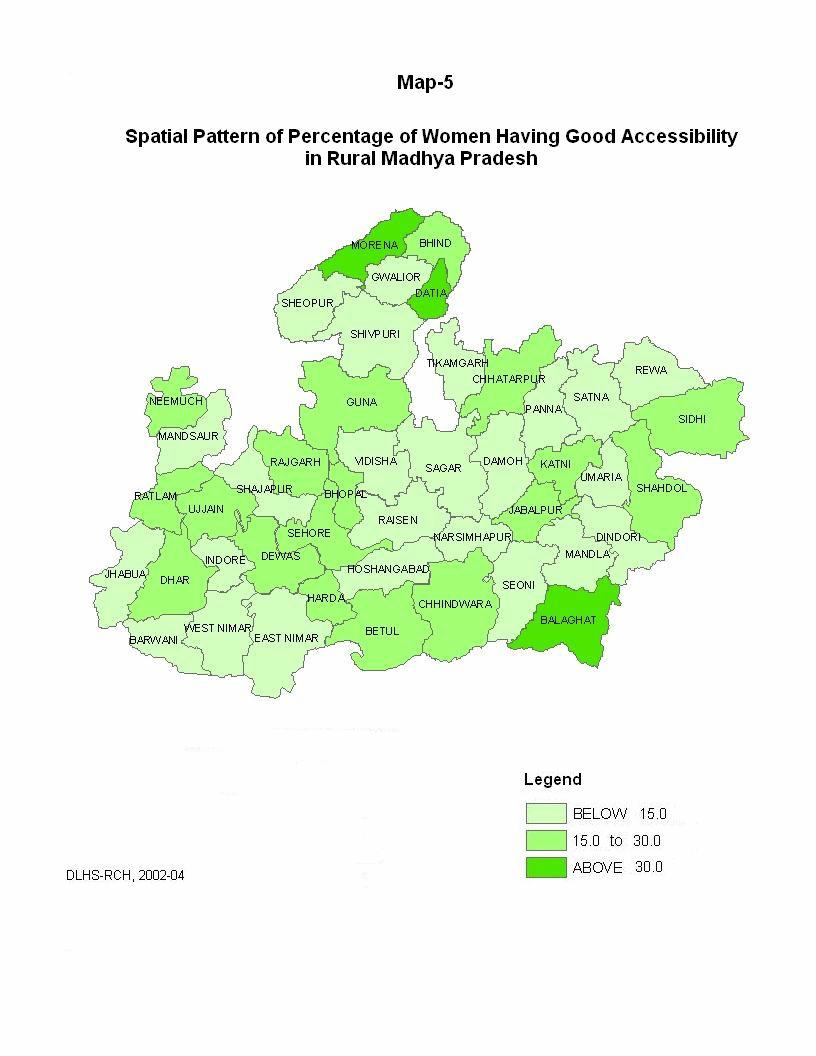
5 eastern region of the state show higher percentage of full ANC. The percentage of women having safe delivery is found to be lowest in Sidhi district (15 percent) where the highest safe delivery is found in Balaghat district (62 percent). It is observed from the Map-2 that northeastern region of the state is the poor performer regarding safe delivery. There is not much spatial variation regarding knowledge of modern family planning method as the average knowledge of the rural women for modern family planning method is 98 percent. Though the women from Sheopur have relatively less knowledge about it. The knowedge of family planning is better among women in districts like Dhar, Jabalpur, Katni, Neemuch etc. Table 6: Results of Multi-variate Analyses Full ANC: The calculated odds ratio show that women belonging to the age group years are two times more likely to take full ANC than the women belonging to years of age. This likelihood of taking full ANC is decreasing sharply after the age The Hindu women and women belonging to other castes are more prone to take full ANC. The odds ratio for women education show that as the education is increasing, the likelihood of getting full ANC is also increasing. The women belonging to high standard of living are 1.6 times more prone to take full ANC than women from poor standard of living. It has been found that women with moderate accessibility have the more chance to get full ANC. Safe Delivery: The odds ratios for the women s age show a negative relation with the probability of going for safe delivery in rural Madhya Pradesh. Muslim women are 1.7 times more willing to go for safe delivery than Hindu women. There are significant associations between marital duration, children ever born and women s education with safe delivery. Though the association is negative in case of marital duration, it is positively related with children ever born and women s education. The women from richer families have more chance for safe delivery and those women who have full ANC, are 2.3 times more likely to go for safe delivery. The findings show that women with good accessibility to public health facilities are more prone to have safe delivery in comparison to women with poor accessibility. Currently Using Any Modern Family Planning Method: The findings reveal that women s age is significantly associated with the currently use of modern family planning methods. The elder women are more likely to use modern methods in comparison to younger married women. Muslim women are less likely and women belonging to other religions are more like to use modern methods than Hindu women. Among all the caste/tribe categories, women from scheduled tribes are less prone to use modern methods. Marital duration and children ever born are also significantly associated with the use of modern methods. It is husband s education which shows higher likelihood to use modern method than women s education. Again poor women are less prone to use this method. Good accessibility increases the likelihood of using modern methods among the rural women in Madhya Pradesh. Table 7 and Map-3 to Map-5: Variation in the Spatial Pattern of the Accessibility of Rural Women in Madhya Pradesh Table 7 and Map-3 show that there is a wide disparity regarding spatial pattern of accessibility of rural women to any public health facility. The lowest accessibility is observed in Vidisha (20 percent) where as the highest accessibility is enjoyed by the women of Rewa.
6 The Map-5 shows that the more than 75 percent of women living in the eastern region of the state have accessibility to any public health facility. Regarding availability of any public health facility in the village, the performance of the southern part of the state is well as more than 40 percent of women living in this area are avail to any public health facility. The highest and least percentage of women enjoying health facility in the village is respectively from districts Datia and Shivpuri. Districts like Barwani and Damoh are the lowest performer regarding good accessibility (i.e. accessibility of any public health facility and public infrastructure is between 5 to 8 km). Good accessibility is more enjoyed by women in Datia district. Only one district in south-eastern part and two districts of northern part of the state show better good accessibility. It is observed from the map and table that most of the parts of the rural Madhya Pradesh have poor accessibility. Conclusion Majority of the rural women in Madhya Pradesh belongs to poor family. Their level of education is also poor. The level of basic obstetric care and knowledge of family planning is lower at the rural level. And this situation becomes worse with the wide regional disparity in health care indicators. Full ANC and safe delivery relates with age-groups, place of residence, education of women and standard of living index. Knowledge of modern method of family planning and its use also depends on these variables. NRHM seeks to improve accessibility to the public health facility among rural women. Findings justify this fact as the results show that good accessibility and availability of health facility are the good predictors for safe delivery and full ANC. Again full ANC and safe delivery may help women to learn more about modern family planning method and encourage them to use it. Apart from obstetric care, there is a strong need to give emphasis on the accessibility as it is directly related with the other associated factors. The findings give highlights on regional disparity in some of the indicators of NRHM and points out the vulnerable districts in terms of the performance. This identification may be helpful in selection of deprived areas and disadvantaged groups and also for policy implication.
7 References: Arora, Surg V Adm Punita Maternal Mortality-Indian Scenario. MJAPI 61: Bhat, P. N. Mari Maternal Mortality in India: An Update. Studies in Family Planning 33,3: Bhatia, Jagdish C. and John Cleland Determinants of Maternal Care in a Region of South India. Health Transition Review 5, Chandhiok, Nomita et al Determinants of antenatal care utilisation in rural areas of India : A cross sectional study from 28 districts. Journal of Gyneocology India 56,1: Chaurasia, Alok Ranjan. 2006: Obstetric Risk and Obstetric Care in Central India, Institute of Economic Growth, New Delhi Fathalla, Mahmoud The Long Road to Maternal Death. People,volume14,number3. Government of Madhya Pradesh, Madhya Pradesh - Summary of Salient Features of Tenth Plan ( ) Luthra, Rita. Safe motherhood: a matter of human rights and social justice. Maine, Deborah Why did Maternal Mortality Decline in Maltab? Studies in Family Planning 27,4: Maternal and Neonatal Health Focused Antenatal Care: Planning and Providing Care during Pregnancy. Programme Brief, March. McCarthy and Deborah Maine A Framework for Analyzing the Determinants of Maternal Mortality. Studies in Family Planning 23,1: Ministry of Health and Family Welfare: National Rural Health Mission: Mission Document ( ), Govt. of India RCH India Summary Report. IIPS, MoHFW, March. SID-SAN and Sirkat Gals Regional Conference on Maternal Health and Well-being in South Asia: Strategies for Meeting the Millennium Development Goals, 3-5 February. Stewart, Kathryn M., Cynthia K. Stanton, Mario Festin and Nora Jacobson Issues in Measuring Maternal Morbidity: Lessons from the Philippines Safe Motherhood Survey Project. Studies in Family Planning 27,1: UNFPA Indicators for Reducing Maternal Mortality. Tool Number 6: Programme Indicators, March. World Health Organisation (WHO) Beyond the Numbers: Reviewing the maternal deaths and complications to make pregnancy safer. Geneva:WHO.
8 Table 1: Characteristics of Rural Women in Madhya Pradesh Variables Percentage of Rural Women Women's Age Religion Hindu 96.5 Muslim 2.5 Others 0.9 Caste Scheduled Caste 16.4 Scheduled Tribe 23.8 Other Backward Class 42.5 Others 17.4 Marital Duration Less than 5 Years to 9 Years to 14 Years Years and above 40.5 Children ever Born Less than to 3 Children 44.2 More than Women's Education Non-literate 70.7 Primary 4.8 Middle 18.9 Secondary 3.2 Higher Secondary and above 2.4 Husbands' Education Non-literate 37.5 Primary 7.2 Middle 31.4 Secondary 11.4 Higher Secondary and above 12.5 Households' Standard of Living Index Low 69.2 Medium 23.5 High 7.3 Knowledge of Any Modern Family Planning Method No 2.4 Yes 97.6 Currently Using Any Modern Family Planning Method No 55.9 Yes 44.1 Accessibility Throughout the Year No 30.3 Yes 69.7 Availability of Public Health Facility in the Village No 65.6 Yes 34.4 Accessibility Index Good 14.9 Moderate 61.0 Poor 24.2 Total Women 26186
9 Table 2: Percent Distribution of Obstetric Care by Different Background Variables VARIABLES Any ANC Full ANC Safe Delivery Women's Age Religion Hindu Muslim Others Caste Scheduled Caste Scheduled Tribe Other Backward Class Others Marital Duration Less than 5 Years to 9 Years to 14 Years Years and above Children ever Born Less than to 3 Children More than Women's Education Non-literate Primary Middle Secondary Higher Secondary and above Husbands' Education Non-literate Primary Middle Secondary Higher Secondary and above Households' Standard of Living Index Low Medium High Knowledge of Any Modern Family Planning Method No Yes Currently Using Any Modern Family Planning Method No Yes Accessibility of Any Public Health Facility throughout the Year No Yes Availability of Public Health Facility in the Village No Yes Accessibility Index Good Moderate Poor Total Rural Women
10 Table 3: Percent distribution of awareness and use of modern family planning method by different background variables VARIABLES Knowledge of Any Modern Family Planning Method Currently Using Any Modern Family Planning Method Women's Age Religion Hindu Muslim Others Caste Scheduled Caste Scheduled Tribe Other Backward Class Others Marital Duration Less than 5 Years to 9 Years to 14 Years Years and above Children ever Born Less than to 3 Children More than Women's Education Non-literate Primary Middle Secondary Higher Secondary and above Husbands' Education Non-literate Primary Middle Secondary Higher Secondary and above Households' Standard of Living Index Low Medium High Full ANC No Yes Safe Delivery No Yes Accessibility of Any Public Health Facility throughout the Year No Yes Availability of Public Health Facility in the Village No Yes Accessibility Index Good Moderate Poor Total Rural Women
11 Table 4: Spatial Pattern of Percentage of Rural Women Suffering From Obstetric Morbidity and Has Access to Obstetric Care District Any Pregnancy Complication Any Delivery Complication Any Post Delivery Complication Any ANC Full ANC Safe Delivery Balaghat Barwani Betul Bhind Bhopal Chhatarpur Chhindwara Damoh Datia Dewas Dhar Dindori East Nimar Guna Gwalior Harda Hoshangabad Indore Jabalpur Jhabua Katni Mandla Mandsaur Morena Narsimhapur Neemuch Panna Raisen Rajgarh Ratlam Rewa Sagar Satna Sehore Seoni Shahdol Shajapur Sheopur Shivpuri Sidhi Tikamgarh Ujjain Umaria Vidisha West Nimar Rural MP
12 Table 5: Spatial Pattern of Percentage of Rural Women Having Awareness of Reproductive Morbidity and Modern Family Planning and Its Uses District Ever Heard of RTI/STI Ever Heard of HIV/AIDS Knowledge of Ane Modern Family Planning Method Currently Using Any Modern Family Planning Method Balaghat Barwani Betul Bhind Bhopal Chhatarpur Chhindwara Damoh Datia Dewas Dhar Dindori East Nimar Guna Gwalior Harda Hoshangabad Indore Jabalpur Jhabua Katni Mandla Mandsaur Morena Narsimhapur Neemuch Panna Raisen Rajgarh Ratlam Rewa Sagar Satna Sehore Seoni Shahdol Shajapur Sheopur Shivpuri Sidhi Tikamgarh Ujjain Umaria Vidisha West Nimar Rural MP
13 Table 6: Odds ratio for full ANC, safe delivery, and awareness and use of modern family planning method VARIABLES Full ANC Safe Delivery Women's Age R Knowledge of Any Modern Family Planning Method Currently Using Any Modern Family Planning Method * 1.926** ** ** ** ** 0.600* 4.110** * * 4.797** * 0.228** 0.459* 4.970** Religion Hindu R Muslim 0.616** 1.678** ** Others * Caste Scheduled Caste R Scheduled Tribe 1.011** * 0.953* Other Backward Class * Others 1.529* * 1.262* Marital Duration Less than 5 Years R 5 to 9 Years * to 14 Years ** 1.802* 1.820** 15 Years and above ** 3.846** 2.873** Children ever Born Less than 2 R 2 to 3 Children ** 2.274** 8.853** More than * 2.236** 2.256** 7.075** Women's Education Non-literate R Primary ** 1.189** 1.426** Middle 2.363** 1.246** 1.817* 1.379** Secondary 3.651** 1.394** 1.792** Higher Secondary and above 7.859** 1.800** 2.370* Husbands' Education Non-literate R Primary 0.098* * 1.528** Middle * 1.236* 1.435** Secondary * ** Higher Secondary and above ** Households' Standard of Living Index Low R Medium 1.169* 1.208** 2.117** 1.758** High 1.647** 1.879** 2.911** 2.411** Full ANC No R Yes ** Accessibility of Any Public Health Facility throughout the Year No R Yes * 1.531* 1.092* Availability of Public Health Facility in the Village No R Yes 1.526* 1.359** 1.325** 1.518* Accessibility Index Good R Moderate 1.065* 0.904** 0.355* 0.947* Poor 0.867* 0.801** 0.266* 0.822** Significant at ** 1% level, * 5 % level, R Reference Category
14 Table 7: Spatial Pattern of Percentage of Rural Women Having Accessibility to Public Health Facility District Accessibility to Any Public Health Facility Availability of Any Public Accessibility Index Health Facility in Village Good Moderate Poor Balaghat Barwani Betul Bhind Bhopal Chhatarpur Chhindwara Damoh Datia Dewas Dhar Dindori East Nimar Guna Gwalior Harda Hoshangabad Indore Jabalpur Jhabua Katni Mandla Mandsaur Morena Narsimhapur Neemuch Panna Raisen Rajgarh Ratlam Rewa Sagar Satna Sehore Seoni Shahdol Shajapur Sheopur Shivpuri Sidhi Tikamgarh Ujjain Umaria Vidisha West Nimar Rural MP
15
16
17
18
19
Utilization of Health Services and RCH Status in Madhya Pradesh: A District Level Analysis
 Utilization of Health Services and RCH Status in Madhya Pradesh: A District Level Analysis Ravendra K. Sharma, Rajiv Ranjan, Ashok Kumar, Arvind Pandey Abstract The study attempts to explore the pattern
Utilization of Health Services and RCH Status in Madhya Pradesh: A District Level Analysis Ravendra K. Sharma, Rajiv Ranjan, Ashok Kumar, Arvind Pandey Abstract The study attempts to explore the pattern
District Level Household and Facility Survey 2010
 District Level Household and Facility Survey - Madhya Pradesh International Institute for Population Sciences (Deemed University) Mumbai- Ministry of Health and Family Welfare New Delhi- Suggested citation:-
District Level Household and Facility Survey - Madhya Pradesh International Institute for Population Sciences (Deemed University) Mumbai- Ministry of Health and Family Welfare New Delhi- Suggested citation:-
CHARACTERISTICS OF SURVEY RESPONDENTS 3
 CHARACTERISTICS OF SURVEY RESPONDENTS 3 The health, nutrition, and demographic behaviours of women and men vary by their own characteristics, such as age, marital status, religion, and caste, as well as
CHARACTERISTICS OF SURVEY RESPONDENTS 3 The health, nutrition, and demographic behaviours of women and men vary by their own characteristics, such as age, marital status, religion, and caste, as well as
CHAPTER 5 FAMILY PLANNING
 CHAPTER 5 FAMILY PLANNING The National Family Welfare Programme in India has traditionally sought to promote responsible and planned parenthood through voluntary and free choice of family planning methods
CHAPTER 5 FAMILY PLANNING The National Family Welfare Programme in India has traditionally sought to promote responsible and planned parenthood through voluntary and free choice of family planning methods
Differentials in the Utilization of Antenatal Care Services in EAG states of India
 International Research Journal of Social Sciences ISSN 2319 3565 Differentials in the Utilization of Antenatal Care Services in EAG states of India Rakesh Kumar Singh 1 and Shraboni Patra 2 International
International Research Journal of Social Sciences ISSN 2319 3565 Differentials in the Utilization of Antenatal Care Services in EAG states of India Rakesh Kumar Singh 1 and Shraboni Patra 2 International
Fertility And Rch-Status In Madhya Pradesh: A District Level Analysis
 Trans.Inst.Indian Geographers ISSN 0970-9851 Fertility And Rch-Status In Madhya Pradesh: A District Level Analysis Kalyan Sundar Som and R. P. Mishra, Sagar, Madhya Pradesh Abstract Fertility is an important
Trans.Inst.Indian Geographers ISSN 0970-9851 Fertility And Rch-Status In Madhya Pradesh: A District Level Analysis Kalyan Sundar Som and R. P. Mishra, Sagar, Madhya Pradesh Abstract Fertility is an important
Women Empowerment and Maternal Health Care Utilisation in North-East India
 Journal of North East India Studies Vol. 4(2), Jul-Dec. 2014, pp. 69-80. Women Empowerment and Maternal Health Care Utilisation in North-East India Mousumi Gogoi Maternal health care services have always
Journal of North East India Studies Vol. 4(2), Jul-Dec. 2014, pp. 69-80. Women Empowerment and Maternal Health Care Utilisation in North-East India Mousumi Gogoi Maternal health care services have always
6.10. NUTRITIONAL STATUS OF TRIBAL POPULATION
 6.1. NUTRITIONAL STATUS OF TRIBAL POPULATION The tribal populations are is recognised as socially and economically vulnerable. Their lifestyles and food habits are different from that of their rural neighbours.
6.1. NUTRITIONAL STATUS OF TRIBAL POPULATION The tribal populations are is recognised as socially and economically vulnerable. Their lifestyles and food habits are different from that of their rural neighbours.
7.10. NUTRITIONAL STATUS OF TRIBAL POPULATION
 7.1. NUTRITIONAL STATUS OF TRIBAL POPULATION The tribal populations are is recognised as socially and economically vulnerable. Their lifestyles and food habits are different from that of their rural neighbours.
7.1. NUTRITIONAL STATUS OF TRIBAL POPULATION The tribal populations are is recognised as socially and economically vulnerable. Their lifestyles and food habits are different from that of their rural neighbours.
Does Empowerment of Women helps in use of Maternal Health Care Services in India: Evidences from North-East Region
 Does Empowerment of Women helps in use of Maternal Health Care Services in India: Evidences from North-East Region Introduction Near about 500,000 women die every year because of pregnancy related complications
Does Empowerment of Women helps in use of Maternal Health Care Services in India: Evidences from North-East Region Introduction Near about 500,000 women die every year because of pregnancy related complications
Reproductive Morbidity among Currently Married Women in EAG States: Evidence from the Reproductive and Child Health survey
 Reproductive Morbidity among Currently Married Women in EAG States: Evidence from the Reproductive and Child Health survey 2002-2004 Santosh Kumar Gupta 1, Rajiva Prasad 2 Introduction and Context India
Reproductive Morbidity among Currently Married Women in EAG States: Evidence from the Reproductive and Child Health survey 2002-2004 Santosh Kumar Gupta 1, Rajiva Prasad 2 Introduction and Context India
XXVI IUSSP International Population Conference in Marrakech, Morocco, 2009
 Paper Submitted in XXVI IUSSP International Population Conference in Marrakech, Morocco, 2009 Title Understanding the Factors Associated with Slow Progress in Childhood Immunisation in India Abhishek Kumar
Paper Submitted in XXVI IUSSP International Population Conference in Marrakech, Morocco, 2009 Title Understanding the Factors Associated with Slow Progress in Childhood Immunisation in India Abhishek Kumar
Factors Influencing Maternal Health Care Services Utilization in Northeast States, India: A Multilevel analysis
 American International Journal of Research in Humanities, Arts and Social Sciences Available online at http://www.iasir.net ISSN (Print): 2328-3734, ISSN (Online): 2328-3696, ISSN (CD-ROM): 2328-3688 AIJRHASS
American International Journal of Research in Humanities, Arts and Social Sciences Available online at http://www.iasir.net ISSN (Print): 2328-3734, ISSN (Online): 2328-3696, ISSN (CD-ROM): 2328-3688 AIJRHASS
TRENDS AND DIFFERENTIALS IN FERTILITY AND FAMILY PLANNING INDICATORS IN JHARKHAND
 Journal of Economic & Social Development, Vol. - XI, No. 1, June 2015 ISSN 0973-886X 129 TRENDS AND DIFFERENTIALS IN FERTILITY AND FAMILY PLANNING INDICATORS IN JHARKHAND Rajnee Kumari* Fertility and Family
Journal of Economic & Social Development, Vol. - XI, No. 1, June 2015 ISSN 0973-886X 129 TRENDS AND DIFFERENTIALS IN FERTILITY AND FAMILY PLANNING INDICATORS IN JHARKHAND Rajnee Kumari* Fertility and Family
Chapter V. Conclusion and Recommendation
 Chapter V Conclusion and Recommendation Chapter V SUMMARY AND CONCLUSIONS The present study entitled An Inter-State Study of Maternal and Child Healthcare in India. Maternal and child health is a productive
Chapter V Conclusion and Recommendation Chapter V SUMMARY AND CONCLUSIONS The present study entitled An Inter-State Study of Maternal and Child Healthcare in India. Maternal and child health is a productive
Determinants of Infertility and Treatment Seeking Behaviour among Currently Married Women in India. Ramesh Chellan India
 Determinants of Infertility and Treatment Seeking Behaviour among Currently Married Women in India Ramesh Chellan India Background Infertility is a worldwide problem affecting about 50 80 million couples
Determinants of Infertility and Treatment Seeking Behaviour among Currently Married Women in India Ramesh Chellan India Background Infertility is a worldwide problem affecting about 50 80 million couples
ISSN: (Online) RESEARCH REVIEW International Journal of Multidisciplinary
 RESEARCH REVIEW International Journal of Multidisciplinary") Volume-03 Issue-12 December -2018 ISSN: 2455-3085 (Online) www.rrjournals.com [UGC Listed Journal] Demographic Change and Urbanization in India with reference to Empowered Action Group (EAG) States: Some
Volume-03 Issue-12 December -2018 ISSN: 2455-3085 (Online) www.rrjournals.com [UGC Listed Journal] Demographic Change and Urbanization in India with reference to Empowered Action Group (EAG) States: Some
Awareness of Janani Shishu Suraksha Karyakram among women in Maharashtra, India
 Awareness of Janani Shishu Suraksha Karyakram among women in Maharashtra, India Vini Sivanandan, R. Nagrajan, Sanjevani Mulay, Arun Pisal, Akram Khan, A.P. Prasik, R. Pol and Vandana Shivnekar Gokhale
Awareness of Janani Shishu Suraksha Karyakram among women in Maharashtra, India Vini Sivanandan, R. Nagrajan, Sanjevani Mulay, Arun Pisal, Akram Khan, A.P. Prasik, R. Pol and Vandana Shivnekar Gokhale
NRHM Programmes and maternal and child health care service utilization: a study on Kannur District of Kerala
 NRHM Programmes and maternal and child health care service utilization: a study on Kannur District of Kerala Abstract M. Lijina M.Phil. Scholar, Department of Economics, Gandhigram Rural Institute-Deemed
NRHM Programmes and maternal and child health care service utilization: a study on Kannur District of Kerala Abstract M. Lijina M.Phil. Scholar, Department of Economics, Gandhigram Rural Institute-Deemed
NATIONAL HEALTH MISSION OF INDIA. Dr. Rajesh Kumar, MD PGIMER School of Public Health Chandigarh (India)
") NATIONAL HEALTH MISSION OF INDIA Dr. Rajesh Kumar, MD PGIMER School of Public Health Chandigarh (India) Outline Historical Milestones/Background National Health Mission (NHM) Impact of NHM? Challenges
NATIONAL HEALTH MISSION OF INDIA Dr. Rajesh Kumar, MD PGIMER School of Public Health Chandigarh (India) Outline Historical Milestones/Background National Health Mission (NHM) Impact of NHM? Challenges
Ageing in India: The Health Issues
 Malcolm Adiseshiah Mid-Year Review of the Indian Economy 2016-17 Ageing in India: The Health Issues Debasis Barik November 5, 2016 India International Centre, New Delhi Outline Background Population Ageing:
Malcolm Adiseshiah Mid-Year Review of the Indian Economy 2016-17 Ageing in India: The Health Issues Debasis Barik November 5, 2016 India International Centre, New Delhi Outline Background Population Ageing:
Knowledge of family planning and current use of contraceptive methods among currently married women in Uttar Pradesh, India
 International Journal of Community Medicine and Public Health Kerketta S et al. Int J Community Med Public Health. 2015 Nov;2(4):449-455 http://www.ijcmph.com pissn 2394-6032 eissn 2394-6040 Research Article
International Journal of Community Medicine and Public Health Kerketta S et al. Int J Community Med Public Health. 2015 Nov;2(4):449-455 http://www.ijcmph.com pissn 2394-6032 eissn 2394-6040 Research Article
EXTENDED ABSTRACT. Integration of Reproductive Health Service Utilization and Inclusive Development Programme in Uttar Pradesh, India
 INTEGRATION, REPRODUCTIVE HEALTH, INCLUSIVE DEVELPOMENT PROGRAMME IN INDIA 1 EXTENDED ABSTRACT Integration of Reproductive Health Service Utilization and Inclusive Development Programme in Uttar Pradesh,
INTEGRATION, REPRODUCTIVE HEALTH, INCLUSIVE DEVELPOMENT PROGRAMME IN INDIA 1 EXTENDED ABSTRACT Integration of Reproductive Health Service Utilization and Inclusive Development Programme in Uttar Pradesh,
HEALTH SYSTEM STRENGTHENING UNDER THE NATIONAL RURAL HEALTH MISSION (NRHM) IN INDIA
 IN INDIA") HEALTH SYSTEM STRENGTHENING UNDER THE NATIONAL RURAL HEALTH MISSION (NRHM) IN INDIA Anuradha Gupta Joint Secretary Govt. of India Over 1.1 billion population 35 States and Union Territories Federal system
HEALTH SYSTEM STRENGTHENING UNDER THE NATIONAL RURAL HEALTH MISSION (NRHM) IN INDIA Anuradha Gupta Joint Secretary Govt. of India Over 1.1 billion population 35 States and Union Territories Federal system
Assesment Of Janani Suraksha Yojana In Karimganj District: A Descriptive Study
 Assesment Of Janani Suraksha Yojana In Karimganj District: A Descriptive Study Rasida Begum Research Scholar, Department of Social Work, Assam University, Silchar, India Dr. G. Albin Joseph Assistant Professor,
Assesment Of Janani Suraksha Yojana In Karimganj District: A Descriptive Study Rasida Begum Research Scholar, Department of Social Work, Assam University, Silchar, India Dr. G. Albin Joseph Assistant Professor,
Methodology. 1 P a g e
 Extended Abstract Disparities in Social Development and Status of women: An analysis of India and its states Ranjana Kesarwani* *Doctoral Candidate, International Institute for Population Sciences, Mumbai-400088,
Extended Abstract Disparities in Social Development and Status of women: An analysis of India and its states Ranjana Kesarwani* *Doctoral Candidate, International Institute for Population Sciences, Mumbai-400088,
Trends and Differentials in Fertility and Family Planning Indicators of EAG States in India
 Trends and Differentials in Fertility and Family Planning Indicators of EAG States in India September 2012 Authors: Dr. R.K Srivastava, 1 Dr. Honey Tanwar, 1 Dr. Priyanka Singh, 1 and Dr. B.C Patro 1 1
Trends and Differentials in Fertility and Family Planning Indicators of EAG States in India September 2012 Authors: Dr. R.K Srivastava, 1 Dr. Honey Tanwar, 1 Dr. Priyanka Singh, 1 and Dr. B.C Patro 1 1
Does Lifestyle Matters in Prevalence of Tuberculosis: Evidence from India
 Does Lifestyle Matters in Prevalence of Tuberculosis: Evidence from India Santosh Kumar Gupta 1, Usha Ram 2 Introduction and Context Smoking, drinking and tobacco use continues to be the leading cause
Does Lifestyle Matters in Prevalence of Tuberculosis: Evidence from India Santosh Kumar Gupta 1, Usha Ram 2 Introduction and Context Smoking, drinking and tobacco use continues to be the leading cause
EFFECTS OF FEMALE S LITERACY ON MATERNAL HEALTH: AN EMPIRICAL STUDY OF JAMMU AND KASHMIR STATE
 EFFECTS OF FEMALE S LITERACY ON MATERNAL HEALTH: AN EMPIRICAL STUDY OF JAMMU AND KASHMIR STATE DR DEEPTI GUPTA Assistant Professor (Sociology) The Law School University of Jammu Jammu and Kashmir ABSTRACT
EFFECTS OF FEMALE S LITERACY ON MATERNAL HEALTH: AN EMPIRICAL STUDY OF JAMMU AND KASHMIR STATE DR DEEPTI GUPTA Assistant Professor (Sociology) The Law School University of Jammu Jammu and Kashmir ABSTRACT
World Bank Presentation
 World Bank Presentation India s urban poor Sonia Hammam, Richard L. Clifford June, 7 1 Key Messages development in India has been anti-poor Consumption poverty is lower in urban areas but it has declined
World Bank Presentation India s urban poor Sonia Hammam, Richard L. Clifford June, 7 1 Key Messages development in India has been anti-poor Consumption poverty is lower in urban areas but it has declined
SURAKSHA YOJANA, INSTITUTIONAL DELIVERIES AND MATERNAL MORTALITY: WHAT DOES THE EVIDENCE SAY?
 14 JANANI SURAKSHA YOJANA, INSTITUTIONAL DELIVERIES AND MATERNAL MORTALITY: WHAT DOES THE EVIDENCE SAY? Ambrish Dongre Despite tremendous medical advances, the instances of maternal and neonatal mortality
14 JANANI SURAKSHA YOJANA, INSTITUTIONAL DELIVERIES AND MATERNAL MORTALITY: WHAT DOES THE EVIDENCE SAY? Ambrish Dongre Despite tremendous medical advances, the instances of maternal and neonatal mortality
globally. Public health interventions to improve maternal and child health outcomes in India
 Summary 187 Summary India contributes to about 22% of all maternal deaths and to 20% of all under five deaths globally. Public health interventions to improve maternal and child health outcomes in India
Summary 187 Summary India contributes to about 22% of all maternal deaths and to 20% of all under five deaths globally. Public health interventions to improve maternal and child health outcomes in India
INVOLVEMENT OF MEN IN FAMILY PLANNNG: USE OF CONTRACEPTION BY MEN IN INDIA. Rima Ghosh
 INVOLVEMENT OF MEN IN FAMILY PLANNNG: USE OF CONTRACEPTION BY MEN IN INDIA. Rima Ghosh ABSTRACT: Men often play the dominant roles in decisions crucial to reproductive health of women. However, family
INVOLVEMENT OF MEN IN FAMILY PLANNNG: USE OF CONTRACEPTION BY MEN IN INDIA. Rima Ghosh ABSTRACT: Men often play the dominant roles in decisions crucial to reproductive health of women. However, family
7.2 VITAMIN A DEFICIENCY
 7.2 VITAMIN A DEFICIENCY Vitamin A is an important micronutrient for maintaining normal growth, regulating cellular proliferation and differentiation, controlling development, and maintaining visual and
7.2 VITAMIN A DEFICIENCY Vitamin A is an important micronutrient for maintaining normal growth, regulating cellular proliferation and differentiation, controlling development, and maintaining visual and
Contraceptive Use Dynamics in South Asia: The Way Forward
 Contraceptive Use Dynamics in South Asia: The Way Forward Authors Manas R. Pradhan 1, H. Reddy 2, N. Mishra 3, H. Nayak 4, Draft Paper for Presentation in the Poster Session 103 at the 27 th IUSSP Conference,
Contraceptive Use Dynamics in South Asia: The Way Forward Authors Manas R. Pradhan 1, H. Reddy 2, N. Mishra 3, H. Nayak 4, Draft Paper for Presentation in the Poster Session 103 at the 27 th IUSSP Conference,
Factors affecting maternal health care seeking behaviour in northeast states, India: evidence from district level household survey-4 ( )
") International Journal of Research in Medical Sciences Singh KJ et al. Int J Res Med Sci. 2016 Nov;4(11):4949-4956 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20163797
International Journal of Research in Medical Sciences Singh KJ et al. Int J Res Med Sci. 2016 Nov;4(11):4949-4956 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20163797
India's voice against AIDS. December 2012
 India's voice against AIDS December 2012 HIV Sentinel Surveillance 2010-11 A Technical Brief India's voice against AIDS December 2012 Contents Acronyms...4 Executive Summary...5 1. Introduction...8 Objectives
India's voice against AIDS December 2012 HIV Sentinel Surveillance 2010-11 A Technical Brief India's voice against AIDS December 2012 Contents Acronyms...4 Executive Summary...5 1. Introduction...8 Objectives
COUNTRY PROFILE ON UNIVERSAL ACCESS TO SEXUAL AND REPRODUCTIVE HEALTH SERVICES:
 PROFILE ON SEXUAL AND HEALTH SERVICES: 2 1. Country context India continues to be the second most populous country in the world with a population of 1210 million; 623.7 million males and 586.5 million
PROFILE ON SEXUAL AND HEALTH SERVICES: 2 1. Country context India continues to be the second most populous country in the world with a population of 1210 million; 623.7 million males and 586.5 million
Haryana-06 Delhi-07 Total disabled population Persons 455, , , ,886 13, ,454 Males 273, ,908 68, ,872 8, ,44
 INDIA-00 Jammu & Kashmir-01 Total disabled population Persons 21,906,769 16,388,382 5,518,387 302,670 229,718 72,952 Males 12,605,635 9,410,185 3,195,450 171,816 129,443 42,373 Females 9,301,134 6,978,197
INDIA-00 Jammu & Kashmir-01 Total disabled population Persons 21,906,769 16,388,382 5,518,387 302,670 229,718 72,952 Males 12,605,635 9,410,185 3,195,450 171,816 129,443 42,373 Females 9,301,134 6,978,197
Childlessness in India: Are we ready as developed countries
 Childlessness in India: Are we ready as developed countries Praween Agrawal Abstract India observe double burden of fertility childlessness along with high fertility, which brings close to a developed
Childlessness in India: Are we ready as developed countries Praween Agrawal Abstract India observe double burden of fertility childlessness along with high fertility, which brings close to a developed
Rural Healthcare Infrastructural Disparities in India: a Critical Analysis of Availability and Accessibility
 DOI: http://doi.org/10.15415/jmrh.2017.32011 Rural Healthcare Infrastructural Disparities in India: a Critical Analysis of Availability and MOHD TAQI 1 *, SWATI BIDHURI 2, SUSMITA SARKAR 3, WANI SUHAIL
DOI: http://doi.org/10.15415/jmrh.2017.32011 Rural Healthcare Infrastructural Disparities in India: a Critical Analysis of Availability and MOHD TAQI 1 *, SWATI BIDHURI 2, SUSMITA SARKAR 3, WANI SUHAIL
Full Length Research Article
 Available online at http://www.journalijdr.com International Journal of DEVELOPMENT RESEARCH ISSN: 2230-9926 International Journal of Development Research Vol. 06, Issue, 10, pp.9798-9803, October, 2016
Available online at http://www.journalijdr.com International Journal of DEVELOPMENT RESEARCH ISSN: 2230-9926 International Journal of Development Research Vol. 06, Issue, 10, pp.9798-9803, October, 2016
Sickle Cell Disease in Central India - Need for Micro Level Planning
 Sickle Cell Disease in Central India - Need for Micro Level Planning R.B. Gupta Abstract Haemoglobinopathies in form of sickle haemoglobin and β -thalassaemia are common in Central India and are important
Sickle Cell Disease in Central India - Need for Micro Level Planning R.B. Gupta Abstract Haemoglobinopathies in form of sickle haemoglobin and β -thalassaemia are common in Central India and are important
Maternal Health Care Services and Its Utilization in Bihar, India
 International Journal of Humanities and Social Science Invention ISSN (Online): 2319 7722, ISSN (Print): 2319 7714 Volume 4 Issue 1 ǁ January. 2015 ǁ PP.73-86 Maternal Health Care Services and Its Utilization
International Journal of Humanities and Social Science Invention ISSN (Online): 2319 7722, ISSN (Print): 2319 7714 Volume 4 Issue 1 ǁ January. 2015 ǁ PP.73-86 Maternal Health Care Services and Its Utilization
List of Licensed Blood Banks
 List of Licensed Blood Banks Government Blood Banks: Medical College level Blood Banks of Madhya Pradesh (05): S. No. District Blood Bank with complete address & location 1. Blood Bank, Hamidia Hospital
List of Licensed Blood Banks Government Blood Banks: Medical College level Blood Banks of Madhya Pradesh (05): S. No. District Blood Bank with complete address & location 1. Blood Bank, Hamidia Hospital
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 15 April 2011 Original:
United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 15 April 2011 Original:
Sexual Behaviour in Rural Northern India: An Insight
 Sexual Behaviour in Rural Northern India: An Insight Meren Longkumer* Dr S.K.Singh** Dr.H.Lhungdim,*** Introduction As we all know, sex is usually not an overt discussion in India, but the spread of HIV/AIDS
Sexual Behaviour in Rural Northern India: An Insight Meren Longkumer* Dr S.K.Singh** Dr.H.Lhungdim,*** Introduction As we all know, sex is usually not an overt discussion in India, but the spread of HIV/AIDS
IJCISS Vol.2 Issue-09, (September, 2015) ISSN: International Journal in Commerce, IT & Social Sciences (Impact Factor: 2.
 ISSN: International Journal in Commerce, IT & Social Sciences (Impact Factor: 2.") (Impact Factor: 2.446) Infant and Child Mortality in India: Levels, Trends and Determinants Naveen Sood Naveen Sood, Assistant Professor PG Department of Economics, DAV College, Jalandhar, Punjab ABSTRACT
(Impact Factor: 2.446) Infant and Child Mortality in India: Levels, Trends and Determinants Naveen Sood Naveen Sood, Assistant Professor PG Department of Economics, DAV College, Jalandhar, Punjab ABSTRACT
HUMAN DEVELOPMENT INDEX: STATUS IN TELANGANA
 Chapter6 HUMAN DEVELOPMENT INDEX: STATUS IN TELANGANA People are the real wealth of nations, and human development focuses on enlarging people s choices Human Development Report, 2015, UNDP. Human development
Chapter6 HUMAN DEVELOPMENT INDEX: STATUS IN TELANGANA People are the real wealth of nations, and human development focuses on enlarging people s choices Human Development Report, 2015, UNDP. Human development
FACT SHEET SIKKIM. District Level Household and DLHS - 3. International institute for population sciences (Deemed University) Mumbai
 Mumbai") 2007-2008 DLHS - 3 Ministry of Health and Family Welfare District Level Household and Facility survey FACT SHEET SIKKIM International institute for population sciences (Deemed University) Mumbai Introduction
2007-2008 DLHS - 3 Ministry of Health and Family Welfare District Level Household and Facility survey FACT SHEET SIKKIM International institute for population sciences (Deemed University) Mumbai Introduction
FACT SHEET DELHI. District Level Household and DLHS - 3. International institute for population sciences (Deemed University) Mumbai
 Mumbai") 2007-2008 DLHS - 3 Ministry of Health and Family Welfare District Level Household and Facility survey FACT SHEET DELHI International institute for population sciences (Deemed University) Mumbai Introduction
2007-2008 DLHS - 3 Ministry of Health and Family Welfare District Level Household and Facility survey FACT SHEET DELHI International institute for population sciences (Deemed University) Mumbai Introduction
Measuring Level and Pattern of Infertility and Childlessness in India
 Measuring Level and Pattern of Infertility and Childlessness in India Sujata Ganguly a, Sayeed Unisa b a PhD scholar, International Institute for Population Sciences, Mumbai, India. Emailsujataganguly2002@rediffmail.com
Measuring Level and Pattern of Infertility and Childlessness in India Sujata Ganguly a, Sayeed Unisa b a PhD scholar, International Institute for Population Sciences, Mumbai, India. Emailsujataganguly2002@rediffmail.com
CHAPTER TWO: TRENDS IN FAMILY PLANNING USE AND PUBLIC SECTOR OUTLAY IN INDIA
 CHAPTER TWO: TREDS I FAMILY PLAIG USE AD PUBLIC SECTOR OUTLAY I IDIA 2.1 Introduction: This chapter examines the trends in use of family planning methods, changes in use of family planning methods over
CHAPTER TWO: TREDS I FAMILY PLAIG USE AD PUBLIC SECTOR OUTLAY I IDIA 2.1 Introduction: This chapter examines the trends in use of family planning methods, changes in use of family planning methods over
Economic Inequalities in Maternal Health Care: Prenatal Care and Skilled Birth Attendance in India,
 Economic Inequalities in Maternal Health Care: Prenatal Care and Skilled Birth Attendance in India, 1992 2006 Praveen Kumar Pathak 1 *, Abhishek Singh 2, S. V. Subramanian 3 1 International Institute for
Economic Inequalities in Maternal Health Care: Prenatal Care and Skilled Birth Attendance in India, 1992 2006 Praveen Kumar Pathak 1 *, Abhishek Singh 2, S. V. Subramanian 3 1 International Institute for
DFID India VAW strategy
 DFID India VAW strategy 1. Catalysis 2. Analysis 3. Strategies Dr Peter Evans, Senior Governance Adviser, DFID India 1 1. Catalysis India s Domestic Violence Act (2005) (some) legal ambiguity cleared up
DFID India VAW strategy 1. Catalysis 2. Analysis 3. Strategies Dr Peter Evans, Senior Governance Adviser, DFID India 1 1. Catalysis India s Domestic Violence Act (2005) (some) legal ambiguity cleared up
Exploring the socioeconomic, demographic and behavioral correlates of gender disparities in HIV testing in India
 Exploring the socioeconomic, demographic and behavioral correlates of gender disparities in HIV testing in India Mayank Kumar Singh 1 S.K. Singh 2 Ravi Prakash 3 Abstract: The existence and rapid spread
Exploring the socioeconomic, demographic and behavioral correlates of gender disparities in HIV testing in India Mayank Kumar Singh 1 S.K. Singh 2 Ravi Prakash 3 Abstract: The existence and rapid spread
Rivu Basu 1, Abhishek Paul 2, Suresh Chandra Malick 2, Somdipta Bhattacharya
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 10 Ver. I (Oct. 2015), PP 37-42 www.iosrjournals.org Prevalence of Tobacco Use and Its Different
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 10 Ver. I (Oct. 2015), PP 37-42 www.iosrjournals.org Prevalence of Tobacco Use and Its Different
Chapter IV Interstate Analysis of Health Outcomes
 Chapter IV Interstate Analysis of Health Outcomes CHAPTER IV INTERSTATE ANALYSIS OF HEALTH OUTCOMES 4.1 Health Outcomes: Meaning and Importance It is well acknowledged by all that health is an integral
Chapter IV Interstate Analysis of Health Outcomes CHAPTER IV INTERSTATE ANALYSIS OF HEALTH OUTCOMES 4.1 Health Outcomes: Meaning and Importance It is well acknowledged by all that health is an integral
Tuberculosis-HIV epidemic situation and emerging challenges in North India
 NTI Bulletin 2015,51 /1&4, 1 7 Tuberculosis-HIV epidemic situation and emerging challenges in North India Rajesh Deshmukh 1,3, Raghu Ram Rao 2, Shah A 2,3, Sreenivas A Nair 3, R S Gupta 1, SD Khaparde
NTI Bulletin 2015,51 /1&4, 1 7 Tuberculosis-HIV epidemic situation and emerging challenges in North India Rajesh Deshmukh 1,3, Raghu Ram Rao 2, Shah A 2,3, Sreenivas A Nair 3, R S Gupta 1, SD Khaparde
The State of Reproductive Health Care in India
 The State of Reproductive Health Care in India Amlan Majumder Department of Economics Dinhata College P. O. Dinhata, DT. Cooch Behar PIN. 736 135, West Bengal, INDIA. Tel. +91-9232526777 Cell. +91-9832469667
The State of Reproductive Health Care in India Amlan Majumder Department of Economics Dinhata College P. O. Dinhata, DT. Cooch Behar PIN. 736 135, West Bengal, INDIA. Tel. +91-9232526777 Cell. +91-9832469667
The World Bank: Policies and Investments for Reproductive Health
 The World Bank: Policies and Investments for Reproductive Health Sadia A Chowdhury Coordinator, Reproductive and Child Health, The World Bank Bangkok, Dec 9, 2010 12/9/2010 2 Maternal Mortality Ratio (MMR):
The World Bank: Policies and Investments for Reproductive Health Sadia A Chowdhury Coordinator, Reproductive and Child Health, The World Bank Bangkok, Dec 9, 2010 12/9/2010 2 Maternal Mortality Ratio (MMR):
Schedule Caste Women and Family Planning In Karnataka-A Critical Analysis
 International Journal of Humanities and Social Science Invention ISSN (Online): 2319 7722, ISSN (Print): 2319 7714 Volume 1 Issue 1 December. 2012 PP.45-49 Schedule Caste Women and Family Planning In Karnataka-A
International Journal of Humanities and Social Science Invention ISSN (Online): 2319 7722, ISSN (Print): 2319 7714 Volume 1 Issue 1 December. 2012 PP.45-49 Schedule Caste Women and Family Planning In Karnataka-A
Sociodemographic profile of beneficiaries and comparative evaluation of ante natal care services under JSY at different health care delivery system
 Original Research Article DOI: 10.18231/2394-6776.2018.0021 Sociodemographic profile of beneficiaries and comparative evaluation of ante natal care services under JSY at different health care delivery
Original Research Article DOI: 10.18231/2394-6776.2018.0021 Sociodemographic profile of beneficiaries and comparative evaluation of ante natal care services under JSY at different health care delivery
India Factsheet: A Health Profile of Adolescents and Young Adults
 India Factsheet: A Health Profile of Adolescents and Young Adults Overview of Morbidity and Mortality With a population of 1.14 billion people, the more than 200 million youth aged 15-24 years represent
India Factsheet: A Health Profile of Adolescents and Young Adults Overview of Morbidity and Mortality With a population of 1.14 billion people, the more than 200 million youth aged 15-24 years represent
CHAPTER 5 FAMILY PLANNING
 CHAPTER 5 FAMILY PLANNING The National Family Welfare Programme in India has traditionally sought to promote responsible and planned parenthood through voluntary and free choice of family planning methods
CHAPTER 5 FAMILY PLANNING The National Family Welfare Programme in India has traditionally sought to promote responsible and planned parenthood through voluntary and free choice of family planning methods
A FOCUS ON CHILDREN ANDHRA PRADESH
 A FOCUS ON CHILDREN ANDHRA PRADESH TABLE OF CONTENT 1 Introduction... 2 1.1. Demography and income ---------------------------------------------3 2 Water & Sanitation... 6 2.1. Sanitation ---------------------------------------------------------------7
A FOCUS ON CHILDREN ANDHRA PRADESH TABLE OF CONTENT 1 Introduction... 2 1.1. Demography and income ---------------------------------------------3 2 Water & Sanitation... 6 2.1. Sanitation ---------------------------------------------------------------7
Ministry of Health and Family Welfare Government of India
 , Ministry of Health and Family Welfare Government of India District Level Household and Facility Survey under Reproductive and Child Health Project (DLHS-3) District Fact Sheet 27-8 Bihar Madhubani
, Ministry of Health and Family Welfare Government of India District Level Household and Facility Survey under Reproductive and Child Health Project (DLHS-3) District Fact Sheet 27-8 Bihar Madhubani
CHAPTER 5 FAMILY PLANNING
 CHAPTER 5 FAMILY PLANNING The National Family Welfare Programme in India has traditionally sought to promote responsible and planned parenthood through voluntary and free choice of family planning methods
CHAPTER 5 FAMILY PLANNING The National Family Welfare Programme in India has traditionally sought to promote responsible and planned parenthood through voluntary and free choice of family planning methods
CHAPTER II CONTRACEPTIVE USE
 CHAPTER II CONTRACEPTIVE USE In a major policy and programmatic shift in April 1996, India s National Family Welfare Programme was renamed the Reproductive and Child Health Programme. This programme enunciated
CHAPTER II CONTRACEPTIVE USE In a major policy and programmatic shift in April 1996, India s National Family Welfare Programme was renamed the Reproductive and Child Health Programme. This programme enunciated
Compiled By: Santosh Pal District Facilitator, Chhatarpur GOI UN Joint Programme on Convergence Disclaimer: It is a reference document only.
 Profile of Chhatarpur District Compiled By: Santosh Pal District Facilitator, Chhatarpur GOI UN Joint Programme on Convergence Disclaimer: It is a reference document only. BASIC INDICATORS S. No Indicator
Profile of Chhatarpur District Compiled By: Santosh Pal District Facilitator, Chhatarpur GOI UN Joint Programme on Convergence Disclaimer: It is a reference document only. BASIC INDICATORS S. No Indicator
MATERNAL HEALTH IN AFRICA
 MATERNAL HEALTH IN AFRICA This Fact Sheet was prepared in January 2013 for the Summit of CARMMA (Campaign on Accelerated Reduction of Maternal, New Born and Child Mortality in Africa) in Addis Ababa Where
MATERNAL HEALTH IN AFRICA This Fact Sheet was prepared in January 2013 for the Summit of CARMMA (Campaign on Accelerated Reduction of Maternal, New Born and Child Mortality in Africa) in Addis Ababa Where
District Fact Sheet - Guna
 District Fact Sheet - Guna Compiled By: - District Planning & Monitoring Unit, Guna D P M U Zila Panchayat, Guna Distr Profile on Guna Demographic and Economic 1 Population (million) 2011 1240938 72597565
District Fact Sheet - Guna Compiled By: - District Planning & Monitoring Unit, Guna D P M U Zila Panchayat, Guna Distr Profile on Guna Demographic and Economic 1 Population (million) 2011 1240938 72597565
Nishant R. Bhimani*, Pushti V. Vachhani, Girija P. Kartha. Department of Community Medicine, C. U. Shah Medical College, Surendranagar, Gujarat, India
 International Journal of Community Medicine and Public Health Bhimani NR et al. Int J Community Med Public Health. 2017 Apr;4(4):1289-1294 http://www.ijcmph.com pissn 2394-6032 eissn 2394-6040 Original
International Journal of Community Medicine and Public Health Bhimani NR et al. Int J Community Med Public Health. 2017 Apr;4(4):1289-1294 http://www.ijcmph.com pissn 2394-6032 eissn 2394-6040 Original
Balance Sheets 1. CHILD HEALTH... PAGE NUTRITION... PAGE WOMEN S HEALTH... PAGE WATER AND ENVIRONMENTAL SANITATION...
 Balance Sheets A summary of the goals, gains and unfinished business of the 1990-2000 decade as included in the Report of the Secretary-General, 'We the Children: End-decade review of the follow-up to
Balance Sheets A summary of the goals, gains and unfinished business of the 1990-2000 decade as included in the Report of the Secretary-General, 'We the Children: End-decade review of the follow-up to
Modelling the impact of poverty on contraceptive choices in. Indian states
 Int. Statistical Inst.: Proc. 58th World Statistical Congress, 2, Dublin (Session STS67) p.3649 Modelling the impact of poverty on contraceptive choices in Indian states Oliveira, Isabel Tiago ISCTE Lisbon
Int. Statistical Inst.: Proc. 58th World Statistical Congress, 2, Dublin (Session STS67) p.3649 Modelling the impact of poverty on contraceptive choices in Indian states Oliveira, Isabel Tiago ISCTE Lisbon
Situational Analysis of Equity in Access to Quality Health Care for Women and Children in Vietnam
 Situational Analysis of Equity in Access to Quality Health Care for Women and Children in Vietnam Presentation by Sarah Bales and Jim Knowles Ha Long Bay, 8 April 2008 Organization of the Presentation
Situational Analysis of Equity in Access to Quality Health Care for Women and Children in Vietnam Presentation by Sarah Bales and Jim Knowles Ha Long Bay, 8 April 2008 Organization of the Presentation
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 12 July 2011 Original:
United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 12 July 2011 Original:
INTRODUCTION BACKGROUND OF THE NATIONAL FAMILY HEALTH SURVEYS
 INTRODUCTION 1 1.1 BACKGROUND OF THE NATIONAL FAMILY HEALTH SURVEYS The National Family Health Surveys (NFHS) are nationwide surveys conducted with a representative sample of households throughout the
INTRODUCTION 1 1.1 BACKGROUND OF THE NATIONAL FAMILY HEALTH SURVEYS The National Family Health Surveys (NFHS) are nationwide surveys conducted with a representative sample of households throughout the
Utilization pattern and associated factors of maternal health care services in Haryana, India: a study based on district level household survey data
 International Journal of Reproduction, Contraception, Obstetrics and Gynecology Ray S et al. Int J Reprod Contracept Obstet Gynecol. 2018 Mar;7(3):1154-1163 www.ijrcog.org DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20180910
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Ray S et al. Int J Reprod Contracept Obstet Gynecol. 2018 Mar;7(3):1154-1163 www.ijrcog.org DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20180910
Meeting the MDGs in South East Asia: Lessons. Framework
 Meeting the MDGs in South East Asia: Lessons and Challenges from the MDG Acceleration Framework Biplove Choudhary Programme Specialist UNDP Asia Pacific Regional Centre 21 23 23 November 2012 UNCC, Bangkok,
Meeting the MDGs in South East Asia: Lessons and Challenges from the MDG Acceleration Framework Biplove Choudhary Programme Specialist UNDP Asia Pacific Regional Centre 21 23 23 November 2012 UNCC, Bangkok,
Briefing on Intensified Malaria Control Project-3 (IMCP-3)
") Briefing on Intensified Malaria Control Project-3 (IMCP-3) India CCM Induction and Orientation Workshop 3 rd -4 th December 2015 Directorate of National Vector Borne Diseases Control Programme, Delhi Plan
Briefing on Intensified Malaria Control Project-3 (IMCP-3) India CCM Induction and Orientation Workshop 3 rd -4 th December 2015 Directorate of National Vector Borne Diseases Control Programme, Delhi Plan
UTILIZATION OF MATERNAL HEALTH CARE SERVICES IN SOUTH INDIA. K. Navaneetham Centre for Development Studies Thiruvananthapuram, India
 1 UTILIZATION OF MATERNAL HEALTH CARE SERVICES IN SOUTH INDIA K. Navaneetham Centre for Development Studies Thiruvananthapuram, India Email: knava@eth.net & A. Dharmalingam Department of Sociology & Social
1 UTILIZATION OF MATERNAL HEALTH CARE SERVICES IN SOUTH INDIA K. Navaneetham Centre for Development Studies Thiruvananthapuram, India Email: knava@eth.net & A. Dharmalingam Department of Sociology & Social
A STUDY TO EVALUATE WORKING PROFILE OF ACCREDITED SOCIAL HEALTH ACTIVIST (ASHA) AND TO ASSESS THEIR KNOWLEDGE ABOUT INFANT HEALTH CARE
 AND TO ASSESS THEIR KNOWLEDGE ABOUT INFANT HEALTH CARE") IJCRR Vol 05 issue 12 Section: Healthcare Category: Research Received on: 23/05/13 Revised on: 14/06/13 Accepted on: 26/06/13 A STUDY TO EVALUATE WORKING PROFILE OF ACCREDITED SOCIAL HEALTH ACTIVIST (ASHA)
IJCRR Vol 05 issue 12 Section: Healthcare Category: Research Received on: 23/05/13 Revised on: 14/06/13 Accepted on: 26/06/13 A STUDY TO EVALUATE WORKING PROFILE OF ACCREDITED SOCIAL HEALTH ACTIVIST (ASHA)
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 12 July 2011 Original:
United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 12 July 2011 Original:
Interstate Disparity of Infant Mortality rates & Its Determinants in India: Evidence from Cross Sectional Data in
 IOSR Journal Of Humanities And Social Science (IOSR-JHSS) Volume 20, Issue 7, Ver. VII (July 2015), PP 130-136 e-issn: 2279-0837, p-issn: 2279-0845. www.iosrjournals.org Interstate Disparity of Infant
IOSR Journal Of Humanities And Social Science (IOSR-JHSS) Volume 20, Issue 7, Ver. VII (July 2015), PP 130-136 e-issn: 2279-0837, p-issn: 2279-0845. www.iosrjournals.org Interstate Disparity of Infant
Does Community Monitoring Improve Delivery of Maternal Health Services? Examining the Role of VHSC in Mayurbhanj District, Orissa
 Does Community Monitoring Improve Delivery of Maternal Health Services? Examining the Role of VHSC in Mayurbhanj District, Orissa 10 CHAPTER Jiban Krushna Behera,* Sudharani Acharya* and Sunita Singh**
Does Community Monitoring Improve Delivery of Maternal Health Services? Examining the Role of VHSC in Mayurbhanj District, Orissa 10 CHAPTER Jiban Krushna Behera,* Sudharani Acharya* and Sunita Singh**
Disparities in Social development and Status of women: An analysis of India and its States
 International Research Journal of Social Sciences ISSN 2319 3565 Disparities in Social development and Status of women: An analysis of India and its States Abstract Kesarwani Ranjana and Yadav Awdhesh
International Research Journal of Social Sciences ISSN 2319 3565 Disparities in Social development and Status of women: An analysis of India and its States Abstract Kesarwani Ranjana and Yadav Awdhesh
Executive Board of the United Nations Development Programme and of the United Nations Population Fund
 United Nations DP/FPA/CPD/ALB/2 Executive Board of the United Nations Development Programme and of the United Nations Population Fund Distr.: General 11 October 2005 Original: English UNITED NATIONS POPULATION
United Nations DP/FPA/CPD/ALB/2 Executive Board of the United Nations Development Programme and of the United Nations Population Fund Distr.: General 11 October 2005 Original: English UNITED NATIONS POPULATION
Maternal care utilization among adolescent mothers in Urban India: Evidence from DLHS-3
 Maternal care utilization among adolescent mothers in Urban India: Evidence from DLHS-3 Introduction Reducing maternal mortality remains an important challenge to global public health systems, particularly
Maternal care utilization among adolescent mothers in Urban India: Evidence from DLHS-3 Introduction Reducing maternal mortality remains an important challenge to global public health systems, particularly
India - National Family Health Survey
 Microdata Library India - National Family Health Survey 1998-1999 International Institute for Population Sciences (IIPS) - Ministry of Health and Family Welfare (MOHFW) Report generated on: June 16, 2017
Microdata Library India - National Family Health Survey 1998-1999 International Institute for Population Sciences (IIPS) - Ministry of Health and Family Welfare (MOHFW) Report generated on: June 16, 2017
GOVERNMENT OF INDIA MINISTRY OF HEALTH AND FAMILY WELFARE DEPARTMENT OF HEALTH AND FAMILY WELFARE
 GOVERNMENT OF INDIA MINISTRY OF HEALTH AND FAMILY WELFARE DEPARTMENT OF HEALTH AND FAMILY WELFARE 1103. SHRI J.J.T. NATTERJEE: SHRI KANWAR SINGH TANWAR: ADV. JOICE GEORGE: SHRI PANKAJ CHAUDHARY: LOK SABHA
GOVERNMENT OF INDIA MINISTRY OF HEALTH AND FAMILY WELFARE DEPARTMENT OF HEALTH AND FAMILY WELFARE 1103. SHRI J.J.T. NATTERJEE: SHRI KANWAR SINGH TANWAR: ADV. JOICE GEORGE: SHRI PANKAJ CHAUDHARY: LOK SABHA
Chapter 9 DEMOGRAPHIC DEVELOPMENT
 Chapter 9 DEMOGRAPHIC DEVELOPMENT INTRODUCTION This chapter deals with the overall demographic situation in Punjab. The scope is rather mixed consisting of demographic history since the state became a
Chapter 9 DEMOGRAPHIC DEVELOPMENT INTRODUCTION This chapter deals with the overall demographic situation in Punjab. The scope is rather mixed consisting of demographic history since the state became a
Inequalities in childhood immunization coverage in Ethiopia: Evidence from DHS 2011
 Inequalities in childhood immunization coverage in Ethiopia: Evidence from DHS 2011 Bezuhan Aemro, Yibeltal Tebekaw Abstract The main objective of the research is to examine inequalities in child immunization
Inequalities in childhood immunization coverage in Ethiopia: Evidence from DHS 2011 Bezuhan Aemro, Yibeltal Tebekaw Abstract The main objective of the research is to examine inequalities in child immunization
Management Information System for Health. Andhra Pradesh. A Case Study
 Management Information System for Health Andhra Pradesh A Case Study Shyama Nagarajan Rachna Sharma Shruti Tripathi November 4, 2016 HIS: Andhra Pradesh November 4, 2016 1 / 29 Motivation Evidence based
Management Information System for Health Andhra Pradesh A Case Study Shyama Nagarajan Rachna Sharma Shruti Tripathi November 4, 2016 HIS: Andhra Pradesh November 4, 2016 1 / 29 Motivation Evidence based
Contraceptive Use and Unmet Need for Family Planning among Tribal Women in India and Selected Hilly States
 Contraceptive Use and Unmet Need for Family Planning among Tribal Women in India and Selected Hilly States Abstract: The paper provides a comprehensive picture of knowledge and contraceptive use among
Contraceptive Use and Unmet Need for Family Planning among Tribal Women in India and Selected Hilly States Abstract: The paper provides a comprehensive picture of knowledge and contraceptive use among
District Level Household and Facility Survey under Reproductive and Child Health Project (DLHS-3)
") Ministry of Health and Family Welfare Government of India District Level Household and Facility Survey under Reproductive and Child Health Project (DLHS3) District Fact Sheet 278 Kerala Palakkad International
Ministry of Health and Family Welfare Government of India District Level Household and Facility Survey under Reproductive and Child Health Project (DLHS3) District Fact Sheet 278 Kerala Palakkad International
The determinants of use of postnatal care services for Mothers: does differential exists between urban and rural areas in Bangladesh?
 ISPUB.COM The Internet Journal of Epidemiology Volume 8 Number 1 The determinants of use of postnatal care services for Mothers: does differential exists between urban and rural areas in Bangladesh? M
ISPUB.COM The Internet Journal of Epidemiology Volume 8 Number 1 The determinants of use of postnatal care services for Mothers: does differential exists between urban and rural areas in Bangladesh? M
Ramesh Chellan. State Facilitator-Demographer, UNICEF-PHDMA, Planning and Coordination Department, Government of Odisha, Bhubaneswar, Odisha, India.
 South East Asia Journal Of Public Health ISSN: 2220-9476 ISSN: 2313-531X (Online) Factors associated with symptoms of reproductive tract infection/sexually transmitted infection and treatment seeking behavior
South East Asia Journal Of Public Health ISSN: 2220-9476 ISSN: 2313-531X (Online) Factors associated with symptoms of reproductive tract infection/sexually transmitted infection and treatment seeking behavior
Ballabgarh HDSS, India
 Ballabgarh HDSS, India Fig 1: Geographical map of Ballabgarh HDSS Ballabgarh is located in Faridabad district of State of Haryana in India and situated between 28 o 25' 16" North latitude and 77 o 18'
Ballabgarh HDSS, India Fig 1: Geographical map of Ballabgarh HDSS Ballabgarh is located in Faridabad district of State of Haryana in India and situated between 28 o 25' 16" North latitude and 77 o 18'
Executive Board of the United Nations Development Programme and of the United Nations Population Fund
 United Nations Executive Board of the United Nations Development Programme and of the United Nations Population Fund Distr.: General 9 April 2010 Original: English DP/FPA/DCP/PRK/5 Annual session 2010
United Nations Executive Board of the United Nations Development Programme and of the United Nations Population Fund Distr.: General 9 April 2010 Original: English DP/FPA/DCP/PRK/5 Annual session 2010