Lehigh Valley Physician Group
|
|
|
- Bathsheba Johns
- 5 years ago
- Views:
Transcription
1 Lehigh Valley Physician Group Welcome to LVPG Obstetrics and Gynecology We are pleased you have selected LVPG Obstetrics and Gynecology for your obstetrical / gynecological care. Meeting a new medical provider can cause anxiety for a patient. As such, we ask that you complete the attached forms and bring them with you to your initial visit. This will help our entire staff handle your experience more effectively. Please arrive 15 minutes prior to your appointment and be certain to bring your insurance card and co-payment, a photo ID, a list of your current medications including strength and dosage, and any required referral forms. In an effort to better serve our patients, our office has implemented an electronic medical record (EMR). This new system will make it easy for us to share information with you and members of your care team. Most importantly, this system will allow us to provide a safer, more efficient healthcare experience for you. Additionally, our office can accommodate those patients who utilize for scheduling appointments, prescription refills, or nonurgent medical questions. Please visit our website at LVHN.org/obgyn for additional information regarding our practice and providers. Thank you for giving us the opportunity to participate in your medical care. Our staff will strive to maintain your confidence in providing you with the ideal patient experience. Sincerely, The Patient Care Team of LVPG Obstetrics and Gynecology Revised:
2 LVPG Obstetrics and Gynecology PLEASE COMPLETE ALL QUESTIONS - PLEASE PRINT Today's Date Mark "X" if you are a previous patient MR# Patient Birth date Last Name First Name Middle Initial Address Street City State Zip Code Home Phone ( ) Work Phone ( ) Ext. Cell Phone ( ) Social Security # Circle: Single / Married / Divorced / Separated / Widowed / Student Spouse: Name SS# Birth date IF MINOR OR FULL TIME STUDENT Father's Name SS# Birth date Mother's Name SS# Birth date Patient's Employer (If minor or FT student, write Mother's) Company Address Occupation Spouse's Employer (If minor or FT student, write Father's) Company Address Occupation Phone ( ) Ext. Phone ( ) Ext. ALLERGIES Medication ALLERGIES - Other (Dust, pollen, pets, etc.) Family Doctor/PCP Phone ( ) 1. Primary Insurance CARD COPY. 2. Secondary Insurance CARD COPY. AUTHORIZATION: I, the undersigned patient OR parent / legal guardian of a minor patient, authorize LVPG Obstetrics and Gynecology to release any medical information necessary to process health insurance claim(s) for services rendered to me or to the minor patient. I hereby authorize direct payment by my health insurance plan(s) to LVPG Obstetrics and Gynecology for all medical services provided to me or to my dependent. (Signature of Patient or Parent / Legal Guardian) Form:
3 LVPG Obstetrics and Gynecology MEDICAL HISTORY FORM Please take a moment to complete this form to the best of your ability. You may leave questions blank for anything that you cannot answer. Thank you! Patient Name Date of Birth Date MR# PREGNANCY HISTORY: # of miscarriages # of ectopics # of abortions # of living children Year Delivery # Weeks Pregnant Vaginal C-section Vaginal C-section Vaginal C-section Vaginal C-section Baby s Gender Male Female Male Female Male Female Male Female Baby s Weight Complications PAST GYNECOLOGIC HISTORY: Age of first menses Frequency Duration Age of menopause Natural Surgical Induced by medication Sexually active: Yes No Partners: Male Female Both Age of first intercourse Number of lifetime sexual partners Current birth control method Sexually transmitted infections (e.g. chlamydia, gonorrhea, trichomoniasis, herpes, syphilis, HIV, genital warts, HPV): Abnormal Pap(s) Endometriosis Colposcopy LEEP Cone biopsy Fibroids MEDICAL HISTORY: List any significant medical problems you have now or have had in the past. High Blood Pressure Elevated Cholesterol Underactive thyroid Overactive thyroid Osteoporosis Osteopenia Migraines Blood clots (now or previous) Diabetes: Other: Controlled w/ diet Controlled w/ meds Controlled w/ Insulin PAST SURGICAL HISTORY: Hysterectomy: Abdominal Vaginal Laparoscopic Supracervical Reason: Fibroids Bleeding Prolapse Endometriosis Cancer: Type Cervical dysplasia/precancer Endometrial hyperplasia / precancer Other Ovaries removed: Left Right Both Breast Surgery: Biopsy Lumpectomy: Left Right Mastectomy: Left Right Reason: Benign Precancer Cancer Page 1 of 2
4 LVPG OBSTETRICS AND GYNECOLOGY MEDICAL HISTORY FORM Page 2 of 2 PAST SURGICAL HISTORY CONTINUED: List any other surgeries you have had. Please remember to include C-sections, tubal ligation, D&C or D&E, prolapse or incontinence surgery as well as non-gynecologic surgeries. MEDICATIONS: List any current medications, doses and instructions. (Attach a list if you are on several.) ALLERGIES: Medication / Food Reaction FAMILY HISTORY: List any medical problems that run in your family as well as the effected members. Condition Family member(s) Condition Family member(s) Breast cancer Diabetes Uterine cancer Colon cancer Ovarian cancer Other: High blood pressure Heart disease / attack Stroke Other SOCIAL HISTORY: Tobacco use: Never Quit Current: Number of packs per day Alcohol use: No Yes Average number of drinks per day Drug use: No Yes Substance VACCINATIONS: Please indicate if and when you received these vaccines: Gardasil (HPV vaccine): Date(s) Hepatitis B: Date(s) Pneumovax: Date Tetanus: Date Adacel/TDaP: Date Herpes Zoster (shingles): Date PREVENTATIVE SERVICES: Please indicate if and when you have had the following tests: Pap smear: Date Cholesterol blood work: Date Mammogram: Date DEXA scan (bone density): Date Colonoscopy: Date Sahara (bone density): Date Revised:
5 LVPG Obstetrics and Gynecology Exciting new patient videos! Emmi Programs: Interactive, online, health care education for our patients What are Emmi programs? They are a series of web-based, online, multimedia videos that educate patients and help them to take an active role in their care. How do patients receive Emmi programs? Your care provider will order an Emmi educational video that is specific to your gynecological or obstetrical care. You will receive secure s to your home address with the information you need to log into Emmi at your convenience, at any time, and view the educational programs ordered for you just like watching an online video! You can even type questions to a qualified Emmi nurse who is standing by for an interactive chat session. On the LVPG Medical Information Communication Preferences Form, please check the YES box and write your address on the line E- MAIL to receive provider-ordered online patient education programs so you can receive Emmi videos which your care provider feels are important to your care. We hope you enjoy Emmi programs, and we look forward to your feedback on the videos and to finding out if they are beneficial to you. Thank you
6 LVPG Medical Information Communication Preferences Patient MR# DOB / / As our patient, we may need to reach you when you are not in the practice. For your privacy, please indicate your preferred method for us to communicate confidential medical information, such as test or lab results, to you and/or others involved in your care. Please note that appointment reminder telephone calls may be left at the contact number(s) you list below. Please list your address to receive online health care educational programs ordered by your care provider. PLEASE INDICATE YOUR COMMUNICATION PREFERENCES BELOW: I give permission to leave medical information pertaining to me, my dependent or child, at the numbers listed below: Method Yes No Area Code, Phone #, Ext, Home telephone Answering Machine Work Phone Cell Phone for our Patient Portal secure registration to receive provider-ordered online patient education programs Pager Without specific permission, we will not release any medical information to anyone other than you. In some cases you may wish for another person to have access to your medical information. Please identify those individuals and their relationship to you (i.e. spouse, parent, son, daughter, partner etc.): Do not release medical information to anyone other than myself. I give permission to release medical information pertaining to me to the individuals listed below. Name Relationship (i.e. spouse, parent, son, daughter, etc.) Area Code, Phone # - Extension Comments I assume responsibility to inform the practice of changes in my phone number(s) or my preferences or to revoke this specific medical information authorization at any time. Signature of Patient or Patient s Legal Representative Date (Please Print Signer s Name) X:\LVPG Admin\Forms\LVPG Medical Information Communication Preferences January 19, 2013
7
8
Last Name First Name MI SS# DOB. Address. City State Zip. Best Phone# (home/ work/ cell) Alternate # (home/ work/ cell)
 Alternate # (home/ work/ cell)") 39 th and Market Street, Penn Presbyterian Medical Center, MOB 340 Philadelphia, PA 19104 215-662-9775 823 South 9 th Street, 1 st Floor Philadelphia, PA 19147 267-239-2725 Last Name First Name MI SS#
39 th and Market Street, Penn Presbyterian Medical Center, MOB 340 Philadelphia, PA 19104 215-662-9775 823 South 9 th Street, 1 st Floor Philadelphia, PA 19147 267-239-2725 Last Name First Name MI SS#
Patient Health Forms
 Patient Health Forms All forms MUST be completed and signed prior to seeing the Provider First: M: Last: Email Address: Home Address: Best Phone Number to Reach You: Last 4 of your social security #: Marital
Patient Health Forms All forms MUST be completed and signed prior to seeing the Provider First: M: Last: Email Address: Home Address: Best Phone Number to Reach You: Last 4 of your social security #: Marital
NOTICE TO OUR PATIENTS
 SMG Chestnut Street, SMG Elm Street, SMG Mancos Valley, Southwest Walk-In Care, Southwest School-Based Health Center, SMG Market Street, SMG Orthopedics, SMG Pulmonary and Sleep Medicine, SMG General Surgery,
SMG Chestnut Street, SMG Elm Street, SMG Mancos Valley, Southwest Walk-In Care, Southwest School-Based Health Center, SMG Market Street, SMG Orthopedics, SMG Pulmonary and Sleep Medicine, SMG General Surgery,
New Patient Paperwork
 Name (Last, First, M.I.): M F Email Address: Primary Phone: Race: Today's Date: DOB: Alternate Emergency Phone: Contact: American Indian/Alaska Native Asian African American Caucasian Nat Hawaiian/Pacific
Name (Last, First, M.I.): M F Email Address: Primary Phone: Race: Today's Date: DOB: Alternate Emergency Phone: Contact: American Indian/Alaska Native Asian African American Caucasian Nat Hawaiian/Pacific
Adult Health History
 Patient Name Date of Birth Adult Health History This form will assist us in obtaining a complete medical history and health record on you. By completing this ahead of time it will also simply your visit
Patient Name Date of Birth Adult Health History This form will assist us in obtaining a complete medical history and health record on you. By completing this ahead of time it will also simply your visit
Adult Health History for New Patient
 Adult Health History for New Patient Name: Birth Date: Today s Date: Preferred Pharmacy (name and location): Your answers on this form will help your health care provider get an accurate history of your
Adult Health History for New Patient Name: Birth Date: Today s Date: Preferred Pharmacy (name and location): Your answers on this form will help your health care provider get an accurate history of your
New Patient Medical History
 New Patient Medical History MR #: Initial Appointment Date: / / Name: Birth Date: / / Address: City: State: Zip: Best Phone # to reach you: ( ) Second contact #: ( ) Email Address: Occupation: Marital
New Patient Medical History MR #: Initial Appointment Date: / / Name: Birth Date: / / Address: City: State: Zip: Best Phone # to reach you: ( ) Second contact #: ( ) Email Address: Occupation: Marital
Breast implants Breast reduction surgery Breast biopsy Breast lumpectomy Chest reconstruction Other:
 New Patient Intake Form This form lets us get to know you and know how we can help. Not every question is important to everyone, but the more you can answer, the more we can help. If there is a question
New Patient Intake Form This form lets us get to know you and know how we can help. Not every question is important to everyone, but the more you can answer, the more we can help. If there is a question
EMERGENCY CONTACT INFORMATION: Name of contact: Address: Phone#: Relationship: May we release medical information to this person?
 ! Page 1 of 5 PATIENT INFORMATION: NAME (Nombre): DATE OF BIRTH (Fecha de Nacimiento): ADDRESS (Direccion): CITY (Ciudad): STATE(Estado): ZIP(Codigo Postal): TELEPHONE (HOME)(# Casa): CELL(# Celular):
! Page 1 of 5 PATIENT INFORMATION: NAME (Nombre): DATE OF BIRTH (Fecha de Nacimiento): ADDRESS (Direccion): CITY (Ciudad): STATE(Estado): ZIP(Codigo Postal): TELEPHONE (HOME)(# Casa): CELL(# Celular):
Welcome to About Women by Women
 Welcome to About Women by Women Today s Date New Patient Questionnaire Name: Birth Date: / / Home Phone: Address: Cell Phone: Work Phone: Occupation: Employer: Marital Status: Married Living w/ Partner
Welcome to About Women by Women Today s Date New Patient Questionnaire Name: Birth Date: / / Home Phone: Address: Cell Phone: Work Phone: Occupation: Employer: Marital Status: Married Living w/ Partner
Name : Date of Birth : Social Security #: Age: Address: City: State: Zip Code: Home Phone: Work Phone: Cell Phone: Address: May we leave a
 Name : Date of Birth : Social Security #: Age: Address: City: State: Zip Code: Home Phone: Work Phone: Cell Phone: Email Address: May we leave a message? Home Work Cell PLEASE DO NOT LEAVE A MESSAGE Marital
Name : Date of Birth : Social Security #: Age: Address: City: State: Zip Code: Home Phone: Work Phone: Cell Phone: Email Address: May we leave a message? Home Work Cell PLEASE DO NOT LEAVE A MESSAGE Marital
We look forward to seeing you. Please feel free to call us with any questions.
 1227 E. 9th Street Edmond, OK 73034 Phone: (405) 475-0100 Fax: (405) 475-9275 https://susandimickmd.com Welcome to Dr. Dimick s Office. We appreciate the opportunity to provide your health care needs.
1227 E. 9th Street Edmond, OK 73034 Phone: (405) 475-0100 Fax: (405) 475-9275 https://susandimickmd.com Welcome to Dr. Dimick s Office. We appreciate the opportunity to provide your health care needs.
Patient Registration Form
 Patient Registration Form Date: Last Name: First: Middle: Street Address City State Zip Home Phone: Work Phone: Mobile Phone: Date of Birth: Social Security: Sex: Male Female Martial Status: Single Married
Patient Registration Form Date: Last Name: First: Middle: Street Address City State Zip Home Phone: Work Phone: Mobile Phone: Date of Birth: Social Security: Sex: Male Female Martial Status: Single Married
743 Jefferson Avenue Suite 203 Scranton, Pennsylvania
 743 Jefferson Avenue Suite 203 Scranton, Pennsylvania 18510 570.344.9997 Name: DOB: / / Age: Address: City: State: Zip: Home Phone: Work Phone: Cell Phone: Reason for your visit today: Who referred you
743 Jefferson Avenue Suite 203 Scranton, Pennsylvania 18510 570.344.9997 Name: DOB: / / Age: Address: City: State: Zip: Home Phone: Work Phone: Cell Phone: Reason for your visit today: Who referred you
IN CASE OF AN EMERGENCY NOT LIVING WITH YOU
 GENERAL INFORMATION Name (as it appears on insur card) Address City State Zip Home phone Cell Email Marital status DOB SS# Employer Work # Parent name (if minor) IN CASE OF AN EMERGENCY NOT LIVING WITH
GENERAL INFORMATION Name (as it appears on insur card) Address City State Zip Home phone Cell Email Marital status DOB SS# Employer Work # Parent name (if minor) IN CASE OF AN EMERGENCY NOT LIVING WITH
Christine Chai, M.D. 901 Dover Drive, Suite 214 Newport Beach, CA 92660
 Christine Chai, M.D. 901 Dover Drive, Suite 214 Newport Beach, CA 92660 Patient Information: Birth Date: Age: Last Name: First: Middle: Address: City: Zip Code: Telephone#: Cell Phone#: Social Security
Christine Chai, M.D. 901 Dover Drive, Suite 214 Newport Beach, CA 92660 Patient Information: Birth Date: Age: Last Name: First: Middle: Address: City: Zip Code: Telephone#: Cell Phone#: Social Security
Please complete all pages of this form. Your physician will review the form with you during your appointment. Last Name: First Name: Middle Initial:
 Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
New Patient Intake Form
 501 Islington Street, Suite 2B Portsmouth, NH 03801 P: 603-610-8882 F: 603-463-0943 New Patient Intake Form Personal Information Today s Date Name Age DOB: Phone: H ( ) W ( ) Cell ( ) Preferred Home Work
501 Islington Street, Suite 2B Portsmouth, NH 03801 P: 603-610-8882 F: 603-463-0943 New Patient Intake Form Personal Information Today s Date Name Age DOB: Phone: H ( ) W ( ) Cell ( ) Preferred Home Work
Adult Health History for NEW Patients
 Adult Health History for NEW Patients Your answers on this form will help your health care provider get an accurate history of your medical concerns and conditions. If you are a current patient there is
Adult Health History for NEW Patients Your answers on this form will help your health care provider get an accurate history of your medical concerns and conditions. If you are a current patient there is
Dawn Frankwick, MD Patricia Rodrigues, MD Carol Salerno, MD Ali Lewis, MD Anita Tiwari, MD
 Dear New Patient: Thank you for selecting Meridian Women s Health as your medical provider. In order to provide the very best and most efficient care please complete the enclosed forms describing your
Dear New Patient: Thank you for selecting Meridian Women s Health as your medical provider. In order to provide the very best and most efficient care please complete the enclosed forms describing your
RESEARCH PARTICIPANT REGISTRATION FORM
 RESEARCH PARTICIPANT REGISTRATION FORM PATIENT: DOB: AGE: DATE: Last Name First Name M.I. ADDRESS: CITY: STATE: ZIP: HOME PHONE: WORK PHONE: MOBILE: SOCIAL SECURITY NUMBER # (Why are we asking for this?*):
RESEARCH PARTICIPANT REGISTRATION FORM PATIENT: DOB: AGE: DATE: Last Name First Name M.I. ADDRESS: CITY: STATE: ZIP: HOME PHONE: WORK PHONE: MOBILE: SOCIAL SECURITY NUMBER # (Why are we asking for this?*):
(FIRST) (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE:
 (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE:") PATIENT INFORMATION EMAIL: MARITAL STATUS: [ ]MARRIED [ ]SINGLE [ ]DIVORCED [ ]WIDOWED NAME: (FIRST) (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE: DOB: PHONE: [ ]Home [ ]Work [ ]Cell PHONE: [ ]Home [
PATIENT INFORMATION EMAIL: MARITAL STATUS: [ ]MARRIED [ ]SINGLE [ ]DIVORCED [ ]WIDOWED NAME: (FIRST) (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE: DOB: PHONE: [ ]Home [ ]Work [ ]Cell PHONE: [ ]Home [
University Gynecologic Oncology Associates
 University Gynecologic Oncology Associates Medical History Form Date: Name: Date of Birth: / / GYNE HISTORY Age of first period? If you no longer have periods, at what age did they stop? Are you pregnant
University Gynecologic Oncology Associates Medical History Form Date: Name: Date of Birth: / / GYNE HISTORY Age of first period? If you no longer have periods, at what age did they stop? Are you pregnant
NEW PATIENT HISTORY. Primary Care Physician Preferred Pharmacy Pharmacy address Phone. Reason for today s visit. Pregnancies abortions miscarriages
 NEW PATIENT HISTORY Name Date of Birth Today s date Primary Care Physician Preferred Pharmacy Pharmacy address Phone _ Reason for today s visit Date of last menstrual period OB HISTORY NUMBER NUMBER NUMBER
NEW PATIENT HISTORY Name Date of Birth Today s date Primary Care Physician Preferred Pharmacy Pharmacy address Phone _ Reason for today s visit Date of last menstrual period OB HISTORY NUMBER NUMBER NUMBER
Metro Acupuncture 6255 Barfield Road, Suite 175 Atlanta, GA
 Metro Acupuncture 6255 Barfield Road, Suite 175 Atlanta, GA 30328 404 255-8388 www.metroacupuncture.com Patient Information Last Name: First Name: Middle Initial: Street Address: City: State: Zip: Preferred
Metro Acupuncture 6255 Barfield Road, Suite 175 Atlanta, GA 30328 404 255-8388 www.metroacupuncture.com Patient Information Last Name: First Name: Middle Initial: Street Address: City: State: Zip: Preferred
Patient Profile Patient Name: DOB: Address: City: State: Zip: Spouse/Significant Other: Children's names and ages: Patient Employer: Address:
 Patient Profile Patient Name: DOB: Address: City: State: Zip: Phone# (H): (W): Other: Email: May Dr. Strong to leave medical information on your answering machine/voicemail? YES NO May Dr. Strong to send
Patient Profile Patient Name: DOB: Address: City: State: Zip: Phone# (H): (W): Other: Email: May Dr. Strong to leave medical information on your answering machine/voicemail? YES NO May Dr. Strong to send
Patient Name (First, Middle, Last) Height Weight. Ethnicity Race Language. Address. City State Zip. Home Phone Cell Phone. Work Phone Other Phone
 Height Weight. Ethnicity Race Language. Address. City State Zip. Home Phone Cell Phone. Work Phone Other Phone") Patient Name (First, Middle, Last) Height Weight Date of Birth Social Security # Gender Male Female Ethnicity Race Language Address City State Zip Home Phone Cell Phone Work Phone Other Phone Email Occupation
Patient Name (First, Middle, Last) Height Weight Date of Birth Social Security # Gender Male Female Ethnicity Race Language Address City State Zip Home Phone Cell Phone Work Phone Other Phone Email Occupation
PATIENT REGISTRATION
 PATIENT REGISTRATION "Please PRINT clearly and fill out form COMPLETELY and hand all insurance cards for copying ** First Name: Last Name: Middle Initial: Address: Apt #: City: State: Zip: Date of Birth:
PATIENT REGISTRATION "Please PRINT clearly and fill out form COMPLETELY and hand all insurance cards for copying ** First Name: Last Name: Middle Initial: Address: Apt #: City: State: Zip: Date of Birth:
Which physician are you scheduled to see? Scheduled Appointment Date: As a reminder: Please arrive minutes prior to your scheduled appointment.
 Which physician are you scheduled to see? Scheduled Appointment : As a reminder: Please arrive 15-20 minutes prior to your scheduled appointment. Please bring the following on the day of your scheduled
Which physician are you scheduled to see? Scheduled Appointment : As a reminder: Please arrive 15-20 minutes prior to your scheduled appointment. Please bring the following on the day of your scheduled
New Patient Form Welcome!
 New Patient Form Welcome! Last First Middle Initial DOB Address City ST ZIP Phone (H) (C) Email Occupation Employer Relationship Status S M W D Spouse s Name DOB Children s Names and Ages Have you had
New Patient Form Welcome! Last First Middle Initial DOB Address City ST ZIP Phone (H) (C) Email Occupation Employer Relationship Status S M W D Spouse s Name DOB Children s Names and Ages Have you had
New Patient History. Patient Name: Date of Birth: Reason for Today s Visit: Today s Date: Who is your Primary Care Physician (PCP)?
?") ew Patient History Patient ame: Date of Birth: Reason for Today s Visit: Today s Date: Who is your Primary Care Physician (PCP)? Review of Systems Please circle any concerning symptoms you are currently
ew Patient History Patient ame: Date of Birth: Reason for Today s Visit: Today s Date: Who is your Primary Care Physician (PCP)? Review of Systems Please circle any concerning symptoms you are currently
NEW PATIENT QUESTIONNAIRE
 NEW PATIENT QUESTIONNAIRE PLEASE PRINT Full name: Age: Preferred Contact number: Email address: Why are you here today? To establish primary care Annual exam Consultation from another doctor If consultation,
NEW PATIENT QUESTIONNAIRE PLEASE PRINT Full name: Age: Preferred Contact number: Email address: Why are you here today? To establish primary care Annual exam Consultation from another doctor If consultation,
Patient Information Form
 Patient Information Form Welcome to West Cancer Center We want to provide excellent service. The following information will allow us to accurately handle your billing and insurance. First Date Referring
Patient Information Form Welcome to West Cancer Center We want to provide excellent service. The following information will allow us to accurately handle your billing and insurance. First Date Referring
GYN PATIENT REGISTRATION
 GYN PATIENT REGISTRATION Note: This form may be completed manually or on your computer. To complete this form on the computer: 1.Type your answer in each field. 2. Save your work often on your computer
GYN PATIENT REGISTRATION Note: This form may be completed manually or on your computer. To complete this form on the computer: 1.Type your answer in each field. 2. Save your work often on your computer
Acknowledgement of receipt of notice of privacy practices
 Acknowledgement of receipt of notice of privacy practices NOTICE OF PRIVACY PRACTICES I acknowledge that I have received a Notice of Privacy Practices from Kettering Physician Network (dba Kettering Cancer
Acknowledgement of receipt of notice of privacy practices NOTICE OF PRIVACY PRACTICES I acknowledge that I have received a Notice of Privacy Practices from Kettering Physician Network (dba Kettering Cancer
Date: New Patient Form First Visit Date:
 Date: New Patient Form First Visit Date: **PATIENT INFORMATION** **PRIMARY INSURANCE** Name: Insurance Company: Street: Claim Address: Facility/Complex City/state/Zip: Group #: Town/State/Zip: Policy/
Date: New Patient Form First Visit Date: **PATIENT INFORMATION** **PRIMARY INSURANCE** Name: Insurance Company: Street: Claim Address: Facility/Complex City/state/Zip: Group #: Town/State/Zip: Policy/
PLEASE PRINT PLEASE CHECK THE BOX AFTER THE PHONE NUMBER THAT YOU WANT AS YOUR PREFERRED NUMBER
 NORTHERN VIRGINIA CENTER FOR ARTHRITIS PLEASE PRINT PATIENT REGISTRATION Patient s Name: DOB: Sex: Address: PLEASE CHECK THE BOX AFTER THE PHONE NUMBER THAT YOU WANT AS YOUR PREFERRED NUMBER Home#( ) [
NORTHERN VIRGINIA CENTER FOR ARTHRITIS PLEASE PRINT PATIENT REGISTRATION Patient s Name: DOB: Sex: Address: PLEASE CHECK THE BOX AFTER THE PHONE NUMBER THAT YOU WANT AS YOUR PREFERRED NUMBER Home#( ) [
Welcome to our Practice
 Welcome to our Practice The staff of Akron General Obstetrics & Gynecology is pleased that you have chosen us to provide your women s health care. Please know that your health is our primary concern and
Welcome to our Practice The staff of Akron General Obstetrics & Gynecology is pleased that you have chosen us to provide your women s health care. Please know that your health is our primary concern and
PATIENT REGISTRATION (Please Print)
") 14800 W. Mountain View Blvd., Suite 160 13090 N. 94 th Drive, Suite 101 Surprise, AZ 85374 Peoria, AZ 85381 (623) 584-3376 (623) 584-3376 Fax: (623) 584-3375 Fax: (623) 584-3375 PATIENT REGISTRATION (Please
14800 W. Mountain View Blvd., Suite 160 13090 N. 94 th Drive, Suite 101 Surprise, AZ 85374 Peoria, AZ 85381 (623) 584-3376 (623) 584-3376 Fax: (623) 584-3375 Fax: (623) 584-3375 PATIENT REGISTRATION (Please
Clinical Genetics Service
 Clinical Genetics Service Helping You and Your Family Reduce Your Risk Your appointment is at AM/PM North Office Location 7714 Conner Road Suite 107 Knoxville, TN 37849 West Office Location Tennova Turkey
Clinical Genetics Service Helping You and Your Family Reduce Your Risk Your appointment is at AM/PM North Office Location 7714 Conner Road Suite 107 Knoxville, TN 37849 West Office Location Tennova Turkey
Female Patient Questionnaire & History
 Female Patient Questionnaire & History Name: (Last) (First) (Middle) Today s Date: Home Phone: Cell Phone: Work: E-Mail Address: Primary Care Physician s Name: May we contact you via E-Mail? ( ) YES (
Female Patient Questionnaire & History Name: (Last) (First) (Middle) Today s Date: Home Phone: Cell Phone: Work: E-Mail Address: Primary Care Physician s Name: May we contact you via E-Mail? ( ) YES (
FAMILY MEDICINE New Patient Medical History Form
 FAMILY MEDICINE New Patient Medical History Form Personal History : Name: Date of Birth / / (mm/dd/yyyy) Age Occupation Birthplace (City&Country) Marital Status (check one): Single Married Divorced Separated
FAMILY MEDICINE New Patient Medical History Form Personal History : Name: Date of Birth / / (mm/dd/yyyy) Age Occupation Birthplace (City&Country) Marital Status (check one): Single Married Divorced Separated
Fertility Specialty Care
 Fertility Specialty Care PATIENT INFORMATION: Last Name First Name & Initial Address City State Zip Home Phone ( ) Cell Phone ( ) Date of Birth Social Security Number Marital Status: Married Single Ethnicity:
Fertility Specialty Care PATIENT INFORMATION: Last Name First Name & Initial Address City State Zip Home Phone ( ) Cell Phone ( ) Date of Birth Social Security Number Marital Status: Married Single Ethnicity:
Female Patient Questionnaire & History
 !! Female Patient Questionnaire & History Name: Today s Date: (Last) (First) (Middle) Date of Birth: Age: Weight: Occupation: Home Address: City: State: Zip: Home Phone: Cell Phone: Work: E-Mail Address:
!! Female Patient Questionnaire & History Name: Today s Date: (Last) (First) (Middle) Date of Birth: Age: Weight: Occupation: Home Address: City: State: Zip: Home Phone: Cell Phone: Work: E-Mail Address:
Primary Care Clinic Adult Patient Demographics
 Primary Care Clinic Adult Patient Demographics Patient s Name: Previous or Nickname: Sex: Male Female Social Security Number - - Date of Birth: Mailing Address: City State Zip Code Home Phone #: ( ) -
Primary Care Clinic Adult Patient Demographics Patient s Name: Previous or Nickname: Sex: Male Female Social Security Number - - Date of Birth: Mailing Address: City State Zip Code Home Phone #: ( ) -
Premier Internal Medicine of Alpharetta, PC
 Patient Information Date / / First Name Middle Initial Last Name Date of Birth / / Social Security # Gender Male Female Marital Status Single Married Separated Divorced Widowed Address Apt # City State
Patient Information Date / / First Name Middle Initial Last Name Date of Birth / / Social Security # Gender Male Female Marital Status Single Married Separated Divorced Widowed Address Apt # City State
Patient Information. Patient Name: DOB: Last First M.I. Home Address: City: State: Zip: Home Phn: Cell Phn: Alt. Phn: SSN:
 Dr. Alvin Huang, M.D., F.A.C.E. 1650 W. Rosedale St. Suite 301, Fort Worth TX 76104 (P) 817-259-4333 (F) 817-820-0303 Patient Information Patient Name: DOB: Last First M.I. Home Address: City:_ State:
Dr. Alvin Huang, M.D., F.A.C.E. 1650 W. Rosedale St. Suite 301, Fort Worth TX 76104 (P) 817-259-4333 (F) 817-820-0303 Patient Information Patient Name: DOB: Last First M.I. Home Address: City:_ State:
GIDEON G. LEWIS, M.D.
 GIDEON G. LEWIS, M.D. Date: LAST Name: FIRST Name: MIDDLE Initial: Address: City: State: Zip Code: Date of birth: / / Social Security #: - - Sex: M F Marital Status (Circle): Single Married Divorced Widowed
GIDEON G. LEWIS, M.D. Date: LAST Name: FIRST Name: MIDDLE Initial: Address: City: State: Zip Code: Date of birth: / / Social Security #: - - Sex: M F Marital Status (Circle): Single Married Divorced Widowed
Cheralyn Perkins, DPM David Scalzo, DPM Kathleen Hope, DPM Nicole Branning, DPM TODAY S DATE: / / LEGAL NAME: LAST FIRST MIDDLE
 PATIENT INFORMATION PATIENT INTAKE FORM BANGOR PODIATRY, LLC Cheralyn Perkins, DPM David Scalzo, DPM Kathleen Hope, DPM Nicole Branning, DPM TODAY S DATE: / / LEGAL NAME: LAST FIRST MIDDLE ADDRESS: STREET
PATIENT INFORMATION PATIENT INTAKE FORM BANGOR PODIATRY, LLC Cheralyn Perkins, DPM David Scalzo, DPM Kathleen Hope, DPM Nicole Branning, DPM TODAY S DATE: / / LEGAL NAME: LAST FIRST MIDDLE ADDRESS: STREET
Welcome to OBGYN Associates.
 Welcome to OBGYN Associates. We are happy you have chosen our practice for your specific medical needs. Please fill out the enclosed forms and bring them with you to your appointment. We do ask that you
Welcome to OBGYN Associates. We are happy you have chosen our practice for your specific medical needs. Please fill out the enclosed forms and bring them with you to your appointment. We do ask that you
City State Zip. Cell Phone. Other Phone. Gender Male Female Status Single Married Divorced Widowed. Height Weight EXERCISE Yes No Times per Week
 Patient Name (First Middle Last) Date of Birth Social Security # Address City State Zip Home Phone Work Phone Cell Phone Other Phone Email Place of Birth Occupation Retired Yes No Gender Male Female Status
Patient Name (First Middle Last) Date of Birth Social Security # Address City State Zip Home Phone Work Phone Cell Phone Other Phone Email Place of Birth Occupation Retired Yes No Gender Male Female Status
Women s Health Partners A Division of Signature Medical Group Kennerly Road, Suite 405 St. Louis, MO 63128
 Pamela Campbell, DO, FACOG Salina Green, MD, FACOG Jamie Joyce, MD, FACOG Madeline Giacalone, DO Kristin Wald, WHNP-BC Janice Eisleben, WHNP-BC Women s Health Partners A Division of Signature Medical Group
Pamela Campbell, DO, FACOG Salina Green, MD, FACOG Jamie Joyce, MD, FACOG Madeline Giacalone, DO Kristin Wald, WHNP-BC Janice Eisleben, WHNP-BC Women s Health Partners A Division of Signature Medical Group
Personal Data. Present Symptoms
 Chris A. Pate, MD 2280 Hwy 70 West, Suite B 265 Racine Drive, Suite 102 Goldsboro, NC 27530 Wilmington, NC 28403 (919) 988-9332 Fx(919) 581-0353 (910) 399-6661 Fx(910) 399-6667 Name Personal Data Address
Chris A. Pate, MD 2280 Hwy 70 West, Suite B 265 Racine Drive, Suite 102 Goldsboro, NC 27530 Wilmington, NC 28403 (919) 988-9332 Fx(919) 581-0353 (910) 399-6661 Fx(910) 399-6667 Name Personal Data Address
South Coast Medical Group Patient Registration
 Patient South Coast Medical Group Patient Registration TODAY S Date:_ Last name First name Initial _ Social Security Number Date of Birth / / Sex Male Female Street Address City State Zip _ Phone Home
Patient South Coast Medical Group Patient Registration TODAY S Date:_ Last name First name Initial _ Social Security Number Date of Birth / / Sex Male Female Street Address City State Zip _ Phone Home
WHEN WAS YOUR LAST TEST OR IMMUNIZATION? PLEASE LIST PAST ILLNESSES, OPERATIONS, HOSPITALIZATIONS YOU HAVE HAD: TYPE: DATE TYPE: DATE
 NAME: DATE: DOB: REFERRD BY: REASON FOR VISIT: ROUTINE PHYSICAL PROBLEM DESCRIBE PROBLEM: AGE: CHECK IF YOU HAD ANY OF THESE MEDICAL PROBLEMS IN THE PAST MAJOR ILLNESSES YES NO YES NO Anemia Hepatitis
NAME: DATE: DOB: REFERRD BY: REASON FOR VISIT: ROUTINE PHYSICAL PROBLEM DESCRIBE PROBLEM: AGE: CHECK IF YOU HAD ANY OF THESE MEDICAL PROBLEMS IN THE PAST MAJOR ILLNESSES YES NO YES NO Anemia Hepatitis
Dear Patient, Sincerely, South Texas Bone & Joint Physical Therapy & Rehabilitation Team
 Physical Therapy & Rehabilitation 601 Texan Trail, Suite 250 Corpus Christi, Texas 78411 Telephone: (361)854-0811 EXT 221 Fax: (361)561-0609 www.southtexasboneandjoint.com Dear Patient, South Texas Bone
Physical Therapy & Rehabilitation 601 Texan Trail, Suite 250 Corpus Christi, Texas 78411 Telephone: (361)854-0811 EXT 221 Fax: (361)561-0609 www.southtexasboneandjoint.com Dear Patient, South Texas Bone
Retinal Consultants of San Antonio PATIENT REGISTRATION
 PATIENT REGISTRATION Today s Date Referred by Patient Full Name Home Address City State Zip Code Home Phone Cell Phone E-mail address Date of Birth Preferred Method of Contact: Home Phone / Cell Phone
PATIENT REGISTRATION Today s Date Referred by Patient Full Name Home Address City State Zip Code Home Phone Cell Phone E-mail address Date of Birth Preferred Method of Contact: Home Phone / Cell Phone
INSURANCE DISCLAIMER
 INSURANCE DISCLAIMER Preventative medicine and bio- identical hormone replacement is a unique practice and is considered a form of alternative medicine. Even though the physicians and nurses are board
INSURANCE DISCLAIMER Preventative medicine and bio- identical hormone replacement is a unique practice and is considered a form of alternative medicine. Even though the physicians and nurses are board
TOMBALL REGIONAL INTERNAL MEDICINE ASSOCIATES Medical Complex Drive, Suite 6 Tomball, TX
 TOMBALL REGIONAL INTERNAL MEDICINE ASSOCIATES 13414 Medical Complex Drive, Suite 6 Tomball, TX 77375 281-516-0212 Welcome! We are glad that you have chosen Tomball Regional Internal Medicine Associates
TOMBALL REGIONAL INTERNAL MEDICINE ASSOCIATES 13414 Medical Complex Drive, Suite 6 Tomball, TX 77375 281-516-0212 Welcome! We are glad that you have chosen Tomball Regional Internal Medicine Associates
DONE! You can now close the browser.
 Visit My Doctor Online at kp.org/mydoctor. Prepare for your visit This form will help you prepare for your upcoming visit with your doctor. You can complete it on your computer (Mac or PC) and e-mail it
Visit My Doctor Online at kp.org/mydoctor. Prepare for your visit This form will help you prepare for your upcoming visit with your doctor. You can complete it on your computer (Mac or PC) and e-mail it
Female New Patient Package
 Female New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
Female New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
FOLSOM CARDIOLOGY. Registration Form. Office Use Only: Patient Acct #
 FOLSOM CARDIOLOGY Please complete forms in black ink only Registration Form Office Use Only: Patient Acct # Name: Date of Birth: Address: Street City State Zip Code Phone: Work: Cell: Marital Status: S
FOLSOM CARDIOLOGY Please complete forms in black ink only Registration Form Office Use Only: Patient Acct # Name: Date of Birth: Address: Street City State Zip Code Phone: Work: Cell: Marital Status: S
NEW PATIENT DATA SHEET Please complete as best you can. It is not necessary to have all information before speaking with a doctor. PATIENT INFORMATION
 NEW PATIENT DATA SHEET Please complete as best you can. It is not necessary to have all information before speaking with a doctor. PATIENT INFORMATION PATIENT NAME DOB AGE PARTNER NAME DOB AGE STREET CITY
NEW PATIENT DATA SHEET Please complete as best you can. It is not necessary to have all information before speaking with a doctor. PATIENT INFORMATION PATIENT NAME DOB AGE PARTNER NAME DOB AGE STREET CITY
COMPLAINTS (Briefly describe each complaint by order of severity): HAVE YOU EVER HAD FALLS, AUTO ACCIDENTS OR INJURIES?
: HAVE YOU EVER HAD FALLS, AUTO ACCIDENTS OR INJURIES?") CORAL REEF CHIROPRACTIC CENTER, PA NAME (Last, First, Middle Initial) HOME PHONE TODAY S DATE COMPLETE ADDRESS (Include City, State & Zip) CELL PHONE DATE OF BIRTH OCCUPATION EMPLOYER NAME EMAIL AGE SEX
CORAL REEF CHIROPRACTIC CENTER, PA NAME (Last, First, Middle Initial) HOME PHONE TODAY S DATE COMPLETE ADDRESS (Include City, State & Zip) CELL PHONE DATE OF BIRTH OCCUPATION EMPLOYER NAME EMAIL AGE SEX
Clinic Adult Patient Demographics
 Clinic Adult Patient Demographics Patient s Name: Previous or Nickname: Sex: Male Female Social Security Number - - Date of Birth: Mailing Address: City State Zip Code Home Phone #: ( ) - May we leave
Clinic Adult Patient Demographics Patient s Name: Previous or Nickname: Sex: Male Female Social Security Number - - Date of Birth: Mailing Address: City State Zip Code Home Phone #: ( ) - May we leave
Denise E. Bruner, M.D. & Associates, P.C.
 page 1 of 6 NAME:(LAST) (FIRST) (M.I.) DATE OF BIRTH: / / SEX: M / F AGE: MARITAL STATUS: (please circle ONE) S M W D MEDICATION ALLERGIES Address (street) (city) (state) (zip) Phone numbers home: work:
page 1 of 6 NAME:(LAST) (FIRST) (M.I.) DATE OF BIRTH: / / SEX: M / F AGE: MARITAL STATUS: (please circle ONE) S M W D MEDICATION ALLERGIES Address (street) (city) (state) (zip) Phone numbers home: work:
Female New Patient Package
 Female New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. In
Female New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. In
Inflammatory Bowel Disease Medical Exam Questionnaire
 Patient Name: MR: Date: Name DOB / / Age Marital Status Race Gender M / F Height Present Weight Usual Weight Insurance Managed Care Self referral Yes No Yes No Yes No Primary Care Physician Referring Physician
Patient Name: MR: Date: Name DOB / / Age Marital Status Race Gender M / F Height Present Weight Usual Weight Insurance Managed Care Self referral Yes No Yes No Yes No Primary Care Physician Referring Physician
Jeri Shuster, M.D., P.A.
 Please help us to help you by completing this health history form. We will review together at your first visit. Included is potentially relevant Ob-Gyn, Medical, Surgical, and pertinent family history.
Please help us to help you by completing this health history form. We will review together at your first visit. Included is potentially relevant Ob-Gyn, Medical, Surgical, and pertinent family history.
Patient Information. Insurance Information
 Thoracic Group, PA Hyperhidrosis Center at Thoracic Group PA Robert J. Caccavale, MD Jean-Philippe Bocage, MD (732) 247-3002 Patient Information Name: Date: Date of Birth: Social Security #: Street Address:
Thoracic Group, PA Hyperhidrosis Center at Thoracic Group PA Robert J. Caccavale, MD Jean-Philippe Bocage, MD (732) 247-3002 Patient Information Name: Date: Date of Birth: Social Security #: Street Address:
HEALTH HISTORY QUESTIONNAIRE. Family Risk Assessment Program
 HEALTH HISTORY QUESTIONNAIRE Family Risk Assessment Program Name DOB Current Age Address Home Phone Cell Phone Business Phone Best time to contact you Day Evening E-mail Address (Email will only be used
HEALTH HISTORY QUESTIONNAIRE Family Risk Assessment Program Name DOB Current Age Address Home Phone Cell Phone Business Phone Best time to contact you Day Evening E-mail Address (Email will only be used
PATIENT REGISTRATION FORM. Last Name: First Name: Initial: Address: City: State: Zip Code: Date of Birth: / / Social: - - address:
 TIMOTHY B. COLE, MD ALLISON TRAVIS, MD 7300 Eldorado Parkway, Ste 260, McKinney, TX 75070 Phone: 972-747-0440 / Fax: 972-747-0441 PATIENT REGISTRATION FORM Date: Last Name: First Name: Initial: Address:
TIMOTHY B. COLE, MD ALLISON TRAVIS, MD 7300 Eldorado Parkway, Ste 260, McKinney, TX 75070 Phone: 972-747-0440 / Fax: 972-747-0441 PATIENT REGISTRATION FORM Date: Last Name: First Name: Initial: Address:
Top Tier. Medical Breast Specialist, P.C.
 Karen S. Barbosa, D.O. Board Certified, Fellowship Trained Breast Surgeon Top Tier Medical Breast Specialist, P.C. 80 Maple Avenue Smithtown, NY 11787 Office: 631.870.8721 Fax: 631.870.8722 Office Visit
Karen S. Barbosa, D.O. Board Certified, Fellowship Trained Breast Surgeon Top Tier Medical Breast Specialist, P.C. 80 Maple Avenue Smithtown, NY 11787 Office: 631.870.8721 Fax: 631.870.8722 Office Visit
ALLERGIES. If yes, please list the food and non-medication (i.e. latex) allergies and type of reaction you had: MEDICATIONS
 allergies and type of reaction you had: MEDICATIONS") Name: Birthdate: What is your main health concern today? Do you currently use tobacco? YES NO Have in the past? YES NO Year Quit If yes, what kind of tobacco?_number of years: Amount of tobacco per day:
Name: Birthdate: What is your main health concern today? Do you currently use tobacco? YES NO Have in the past? YES NO Year Quit If yes, what kind of tobacco?_number of years: Amount of tobacco per day:
Initial Clinical History and Physical Form
 601 E FM 544, Suite 400, Murphy, TX, 75094 TEL: 972-442-4700 Initial Clinical History and Physical Form Patient Information Name: Age: of Birth: / / Sex: Male / Female Marital Status: Single Married Divorced
601 E FM 544, Suite 400, Murphy, TX, 75094 TEL: 972-442-4700 Initial Clinical History and Physical Form Patient Information Name: Age: of Birth: / / Sex: Male / Female Marital Status: Single Married Divorced
PATIENT INFORMATION. Name: First Name MI Last Name. Date of Birth: / / Sex: Male / Female / Declined SSN:
 PATIENT INFORMATION Name: First Name MI Last Name Date of Birth: / / Sex: Male / Female / Declined SSN: Race: Ethnicity: Hispanic/Latino Not Hispanic/Latino Declined Marital Status: Single Married Divorced/Separated
PATIENT INFORMATION Name: First Name MI Last Name Date of Birth: / / Sex: Male / Female / Declined SSN: Race: Ethnicity: Hispanic/Latino Not Hispanic/Latino Declined Marital Status: Single Married Divorced/Separated
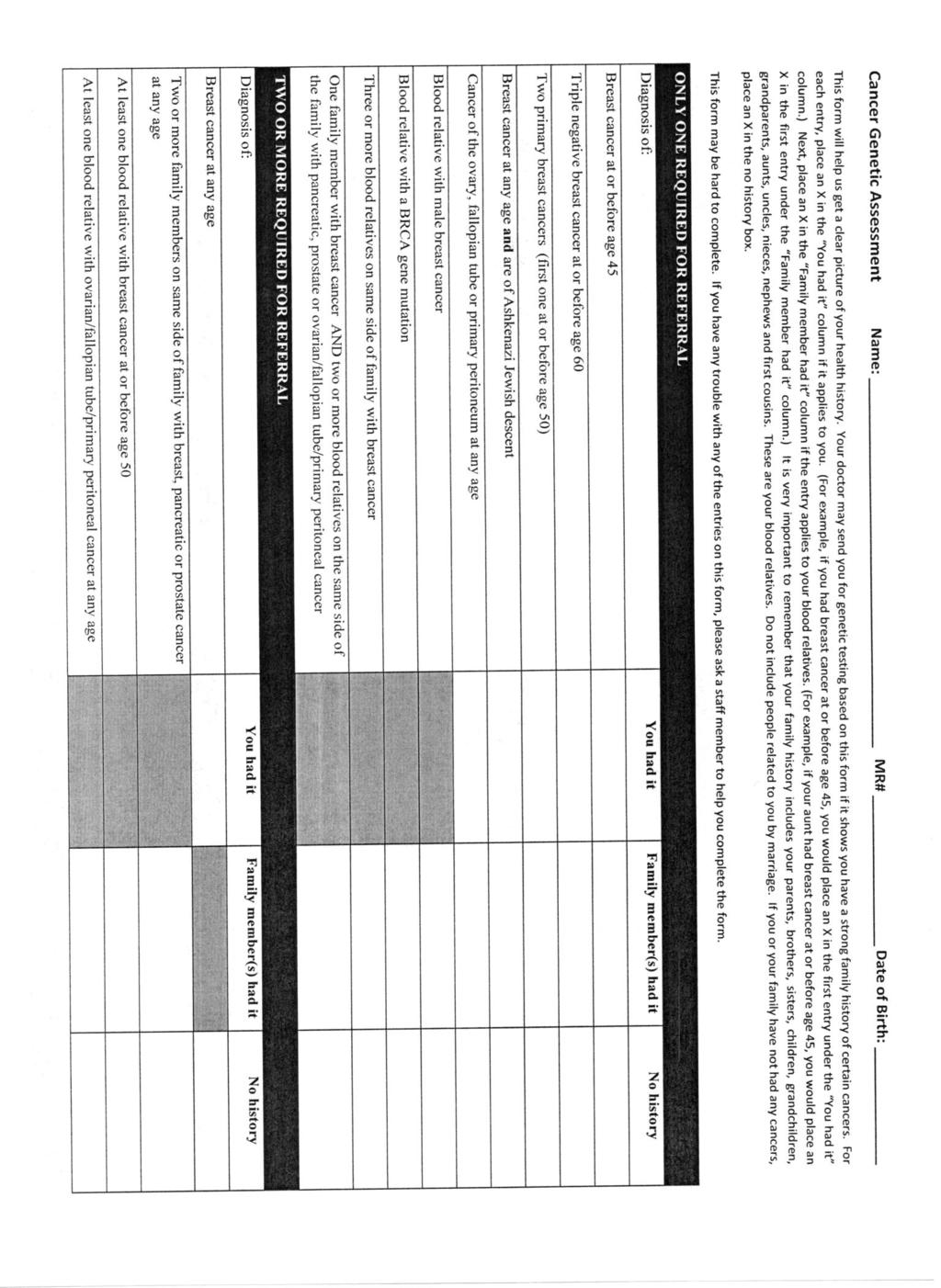
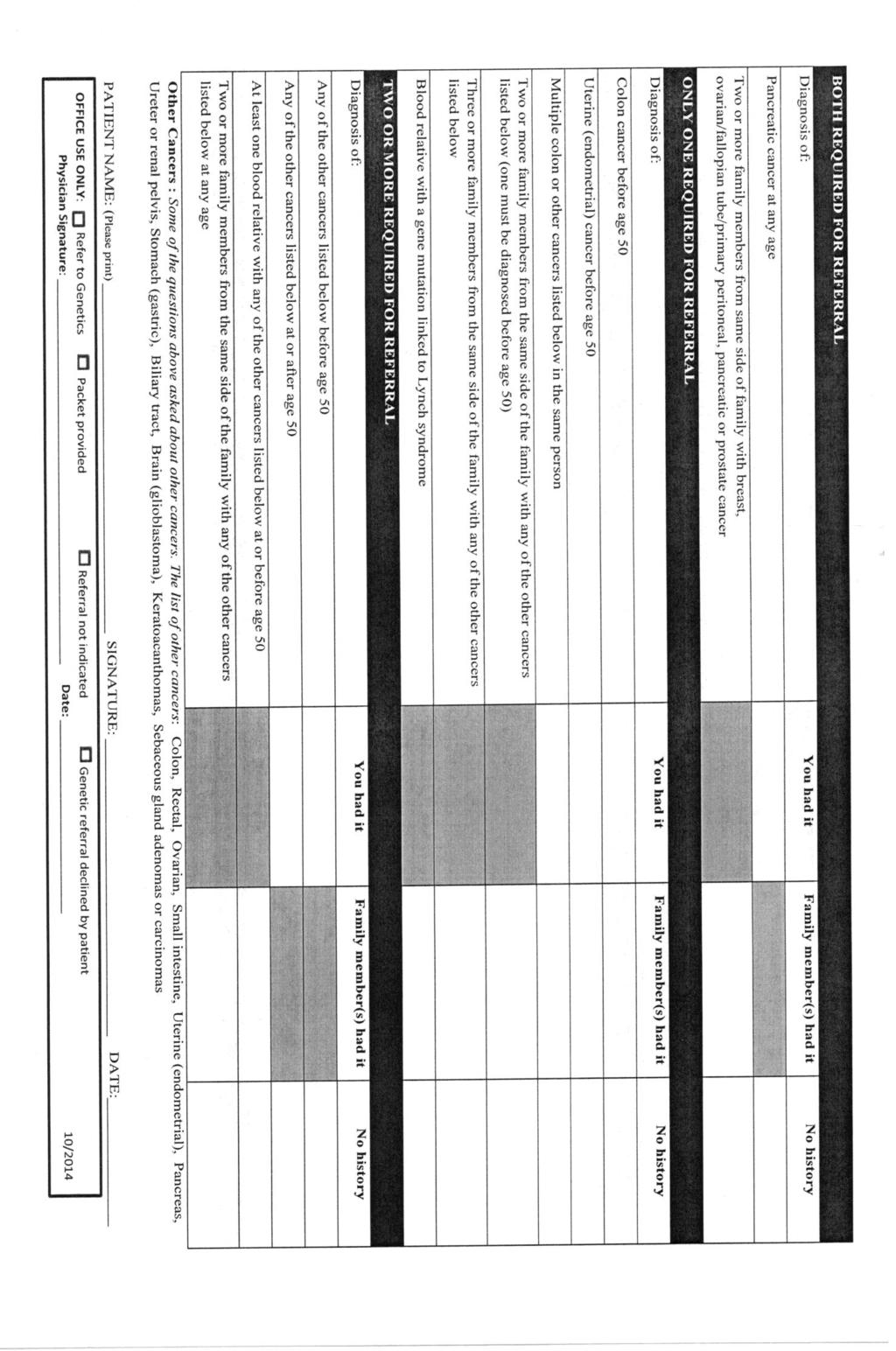
Genetic Risk Evaluation and Testing Program
 INSTRUCTIONS: Please complete this form to the best of your ability PRIOR to your appointment. Please remember to list ALL relatives, both living and deceased, regardless of if they have had cancer or
INSTRUCTIONS: Please complete this form to the best of your ability PRIOR to your appointment. Please remember to list ALL relatives, both living and deceased, regardless of if they have had cancer or
Blue Precision HMO Annual Health Assessment Form - Adult
 BCBSIL Subscriber ID: Name of Physician: Blue Precision HMO Annual Health Assessment Form - Adult Reason(s) for Visit: Date of Service: Medications: Name of Medication Dosage Frequency Comments Allergies:
BCBSIL Subscriber ID: Name of Physician: Blue Precision HMO Annual Health Assessment Form - Adult Reason(s) for Visit: Date of Service: Medications: Name of Medication Dosage Frequency Comments Allergies:
ADULT INFORMATION SHEET
 DATE: DOCTOR TIME ADULT INFORMATION SHEET FULL NAME NICKNAME: SEX: BIRTHDATE: AGE: SOCIAL SECURITY #: HOME PHONE #: CELL PHONE #: MAILING ADDRESS: STREET CITY: STATE: ZIP: PLACE OF EMPLOYMENT: E-MAIL ADDRESS:
DATE: DOCTOR TIME ADULT INFORMATION SHEET FULL NAME NICKNAME: SEX: BIRTHDATE: AGE: SOCIAL SECURITY #: HOME PHONE #: CELL PHONE #: MAILING ADDRESS: STREET CITY: STATE: ZIP: PLACE OF EMPLOYMENT: E-MAIL ADDRESS:
COMPREHENSIVE NEW PATIENT QUESTIONNAIRE
 What brings you in today? What do you prefer to be called (nickname)? Please list all of your medical conditions. 1. 5. 2. 6. 3. 7. 4. 8. What surgical or medical procedures have you had in the past? 1.
What brings you in today? What do you prefer to be called (nickname)? Please list all of your medical conditions. 1. 5. 2. 6. 3. 7. 4. 8. What surgical or medical procedures have you had in the past? 1.
Tel: (312) Women s Integrated Fax: (312) Pelvic Health Program. 1.0: Basic Information. Preferred Language:
 Women s Integrated Fax: (312) Pelvic Health Program. 1.0: Basic Information. Preferred Language:") Tel: (312) 694-7337 Women s Integrated Fax: (312) 695-0156 Pelvic Health Program 1.0: Basic Information Date of Birth: / / Age: Home Address: Preferred Language: English Spanish Other: Email address: Preferred
Tel: (312) 694-7337 Women s Integrated Fax: (312) 695-0156 Pelvic Health Program 1.0: Basic Information Date of Birth: / / Age: Home Address: Preferred Language: English Spanish Other: Email address: Preferred
Health History Questionnaire. Age Date of Birth Gender. Married Single Separated Divorced Widowed Partnership
 Health History Questionnaire Name Date Age Date of Birth Gender Married Single Separated Divorced Widowed Partnership Live with: Spouse Partner Parents Children Friends Alone Please complete these next
Health History Questionnaire Name Date Age Date of Birth Gender Married Single Separated Divorced Widowed Partnership Live with: Spouse Partner Parents Children Friends Alone Please complete these next
MGH Beacon Hill Primary Care New Patient Form
 MGH Beacon Hill Primary Care New Patient Form For Office Use Only Date Reviewed By Name Date of birth Medical History Please check all that apply. Alcoholism Angina or heart attack Anorexia/bulimia Arthritis
MGH Beacon Hill Primary Care New Patient Form For Office Use Only Date Reviewed By Name Date of birth Medical History Please check all that apply. Alcoholism Angina or heart attack Anorexia/bulimia Arthritis
Name: Today s Date: Address: State, Zip Code
 New Patient Health History Questionnaire Name: Today s Date: Address: City State, Zip Code Email Address: Date of Birth: Home Telephone #: Cell Number: Work Number: Emergency Contact name & number: Referred
New Patient Health History Questionnaire Name: Today s Date: Address: City State, Zip Code Email Address: Date of Birth: Home Telephone #: Cell Number: Work Number: Emergency Contact name & number: Referred
Female New Patient Package
 Female New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
Female New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
Patient Information: Date: Last Name: Street Address: City: SS #: First Name: Sex: M F Birthdate: Contact Information:
 Welcome to PHC Family Medicine! We know you have a choice and appreciate your choosing us to provide care to your family. Dr. Frankhouser will be asking about your concerns today, but so that we can learn
Welcome to PHC Family Medicine! We know you have a choice and appreciate your choosing us to provide care to your family. Dr. Frankhouser will be asking about your concerns today, but so that we can learn
Primary Care Demographic and Medical History Form
 Primary Care Demographic and Medical History Form PATIENT DEMOGRAPHIC INFORMATION: Patient Name: Date of Birth: / / Street Address: City: State: Zip: Home Phone #: Work #: Cell #: Email: Preferred Method
Primary Care Demographic and Medical History Form PATIENT DEMOGRAPHIC INFORMATION: Patient Name: Date of Birth: / / Street Address: City: State: Zip: Home Phone #: Work #: Cell #: Email: Preferred Method
Comprehensive Patient History Form
 Comprehensive Patient History Form Date: Name: D.O.B. Past Medical History: (check all that apply) Acid Reflux Cataracts Heart disease Migraines Alcohol or Drug Problem Colitis/Crohns Heart valve problems
Comprehensive Patient History Form Date: Name: D.O.B. Past Medical History: (check all that apply) Acid Reflux Cataracts Heart disease Migraines Alcohol or Drug Problem Colitis/Crohns Heart valve problems
Directions to Whole Woman Health - located in the NW Des Moines/Beaverdale area:
 Whole Woman Health Patient Registration Form Welcome New Patient! We are pleased you have chosen Whole Woman Health. Below is your registration form as well as Medical History and Assessment forms. Please
Whole Woman Health Patient Registration Form Welcome New Patient! We are pleased you have chosen Whole Woman Health. Below is your registration form as well as Medical History and Assessment forms. Please
311 North M.D. First Name. Race: Asian. White. Name. Phone: Coverage: made. Name Relationship
 Robert Antonelle, M.D. White Plains Gastroenterology 311 North Street, Suite 403 White Plains, NY 10605 Patient Demographics Patient s Last Name First Name Middle Initial SSN Date of Birth Age Gender F
Robert Antonelle, M.D. White Plains Gastroenterology 311 North Street, Suite 403 White Plains, NY 10605 Patient Demographics Patient s Last Name First Name Middle Initial SSN Date of Birth Age Gender F
Corinna Mosher, M.D. A Medical Corporation 415 E. Rolling Oaks Drive Suite #280 Thousand Oaks, CA (805) Fax (805)
 Fax (805)") Patient Registration: Corinna Mosher, M.D. A Medical Corporation 415 E. Rolling Oaks Drive Suite #280 Thousand Oaks, CA 91361 (805) 496-8522 Fax (805) 496-0469 Last Name: First Name: MI: Address: City:
Patient Registration: Corinna Mosher, M.D. A Medical Corporation 415 E. Rolling Oaks Drive Suite #280 Thousand Oaks, CA 91361 (805) 496-8522 Fax (805) 496-0469 Last Name: First Name: MI: Address: City:
Health Questionnaire
 Patient Name Date of Birth Thank you for choosing Southern Cancer Center for your care. To help us best prepare for your appointment, please complete this form and bring it to your appointment. If you
Patient Name Date of Birth Thank you for choosing Southern Cancer Center for your care. To help us best prepare for your appointment, please complete this form and bring it to your appointment. If you
Name Age DOB Sex M F Your relationship status: Single Married Life partner Widowed Address
 Today s Date Contact Information Name Age DOB Sex M F Your relationship status: Single Married Life partner Widowed Address Phone numbers and E-mail (please check numbers to call or leave a message) Home
Today s Date Contact Information Name Age DOB Sex M F Your relationship status: Single Married Life partner Widowed Address Phone numbers and E-mail (please check numbers to call or leave a message) Home
PATIENT HEALTH HISTORY
 Name DOB Sex Age Date MR# PLACE CHARGE TICKET LABEL IN THE DASHED SPACE OR COMPLETE THE ABOVE: PLEASE ANSWER EACH QUESTION AS CORRECTLY AS YOU CAN BY PLACING AN "X" IN APPROPRIATE BOX What is the reason
Name DOB Sex Age Date MR# PLACE CHARGE TICKET LABEL IN THE DASHED SPACE OR COMPLETE THE ABOVE: PLEASE ANSWER EACH QUESTION AS CORRECTLY AS YOU CAN BY PLACING AN "X" IN APPROPRIATE BOX What is the reason
New Patient History Form (Age 18 and over)
") New Patient History Form (Age 18 and over) Obstetrics & Gynecology Name Age Date first middle last Occupation Marital Status: c Single c Married c Divorced c Widowed Referred to our office by: What is
New Patient History Form (Age 18 and over) Obstetrics & Gynecology Name Age Date first middle last Occupation Marital Status: c Single c Married c Divorced c Widowed Referred to our office by: What is
Our office is located at 2030 Drew Street, Clearwater FL, We are on Drew Street, in between N.E Old Coachman Road and Hercules Avenue.
 Dear New Patient, Thank you for choosing Dennis M. Lox, M.D to participate in your healthcare. We realize that you could have chosen any other office, so we are honored that you have chosen us. While Dr.
Dear New Patient, Thank you for choosing Dennis M. Lox, M.D to participate in your healthcare. We realize that you could have chosen any other office, so we are honored that you have chosen us. While Dr.