BEST PAPERS OFF 2016 for Renal cancer & Bladder cancer
|
|
|
- Meghan Blake
- 6 years ago
- Views:
Transcription
1 BEST PAPERS OFF 2016 for Renal cancer & Bladder cancer ΙΩΑΝΝΗΣ ΒΑΡΚΑΡΑΚΗΣ ΑΝΑΠΛΗΡΩΤΗΣ ΚΑΘΗΓΗΤΗΣ ΟΥΡΟΛΟΓΙΑΣ ΕΘΝΙΚΟ & ΚΑΠΟΔΙΣΤΡΙΑΚΟ ΠΑΝΕΠΙΣΤΗΜΙΟ ΑΘΗΝΩΝ ΣΙΣΜΑΝΟΓΛΕΙΟ ΝΟΣΟΚΟΜΕΙΟ

2 ΔΕΝ ΕΧΩ ΣΥΓΚΡΟΥΣΗ ΣΥΜΦΕΡΟΝΤΩΝ
3

4 EAU guidelines recommend treatment in: large tumors women of child-bearing age follow-up or access to emergency care is inadequate A size threshold for treatment remains controversial, with previous recommendazons suggeszng 3 4 cm. The 4 cm threshold is based on a study by Oesterling et al based on 13 pt The true natural history may remain unknown because symptoma?c cases are more likely to be idenzfied and included in case series.
5 MATERIALS & METHODS Radiology record crawler system (Montage; Montage Healthcare Systems, Philadelphia, USA) 2741 pazents with renal AML. 447 pazents with 582 tumors with >3 abdominal imaging. FU: median 43 mo (range: mo)


 9% grew with rate >0.")
 had interven?")
6 RESULTS (10%) Tumors>4cm more likely Younger age TSC SymptomaZc intervenzon No difference in the average growth rate of lesions <4cm vs >4cm 91% did not grow or grew slowly (0.02cm/y) 9% grew with rate >0.25cm/y 93% were eleczve intervenzons 25/447(5.6%) had interven?on More frequently young age TSC SymptomaZc >4cm
7 RESULTS SYMPTOMS In 10% overall In 30% if AML>4cm Most common hematuria & pain Non TSC Pain > hematuria TSC Hematuria > Pain (p=0.16) Retroperitoneal bleeding Rare 0.4% Majority do not have prior Sx Can happen with RCC as well with same frequency Interven?on 5% SAE, RFA, mtor inhibitors, PNx
8 TAKE HOME MESSAGE Most sporadic AMLs are ASx do not grow or grow slowly regardless of inizal size. Pt with ASx or mildly Sx AMLs even if >4cm should be offered inizal AS Pt should be aware of small risk of progression especially in fast growing AMLs (>0.25cm/y)
 RFA outcomes associated with Tumor size Increased failure")
")
9 Uniform temperatures >60C required my not be reached (heat sink) RFA outcomes associated with Tumor size Increased failure rates Clear cell histology Degree of tumor enhancement (change HU from non-contrast to contrast enhanced arterial phase ) FAILURE?


10 MATERIALS & METHODS RESULTS ``` ` Sample? 158 pazents RFA ablazon Biopsy confirmed RCC in 81% 7% incomplete abla?on 93% (99 pt) RCC successful abla?on

11 RESULTS 5-year DFS P<0.01 <3cm 100% >3cm 69.2% P=0.24 <60HU 100% >60HU 92.4% P=0.27 Non-clear cell 100% Clear cell 92.5% Disease recurrence 5.4% (5 pt) Median follow up 30 mo
12 STUDY LIMITATIONS Retrospec?ve study. Limited number of pt. Standard protocol for contrast use in CT was used some varia?on is expected: Degree of enhancement within the tumor depends on 0ming amount of contrast used Part of tumor measured tumors are heterogeneous and degree of enhancement can vary.
13 TAKE HOME MESSAGE Tumors with contrast enhancement >60HU have higher incomplete abla?on a er RFA Contrast enhancement cannot predict DFS Tumor size >3cm remains a significant risk factor for DFS

14 Heterogeneous behavior of RCC lesions Low grade & stage indolent course High grade & stage risk of growth and systemic spread Residual tumor in the context of PSM mimics the primary lesion Lack of consensus for clinical relevance of a PSM acer PNx Variability in pathological characteriszcs in various studies Contemporary studies lack the sta?s?cal power High risk pazents with and without PSM PSM in high and low risk pazents
 2/3 in Low risk pt (71%) 1/3 in High risk pt (29%) Recurrence 5.")
15 A retrospec?ve mul?-ins?tu?onal review 1240 pt PNx (O/L/R) Median FU 33mo +sm 7.8% (97) 2/3 in Low risk pt (71%) 1/3 in High risk pt (29%) Recurrence 5.6% (69) Median Zme 19mo MATERIALS & METHODS PSM was unrelated to tumor size, stage, grade, histology, focality (all p > 0.05).
16 univariable -sm RESULTS +sm 61% 39% A +margin was associated with an increased risk of relapse on mulzvariable analysis (HR 2.08, 95% CI 1.09e 3.97, p. 0.03) but not with site of recurrence. increased risk of local as well as metasta?c relapse.
17 RESULTS Subgroups in which PSM was a predictor of recurrence Median Zme to recurrence was 19 months for high risk cases.
18 RESULTS 45% in 5 years a posi?ve surgical margin was significantly associated with a higher risk of recurrence in cases considered high risk (p < 0.001) but not low risk (p ).
19 STUDY LIMITATIONS Retrospec?ve nature Heterogeneity Surgical technique Pt seleczon Follow up Incomplete informa?on Nephrometry score Intraopera?ve biopsy Management of intraopera?ve biopsy Depth and magnitude of PSM Not powered for analysis of recurrence loca?on
20 TAKE HOME MESSAGE PSM associated with local and metasta?c tumor recurrence a er PN This relazonship observed specifically for tumors with high risk features RFS was similar among low risk features regardless of margin status In complex ct2 maybe RNx beger?

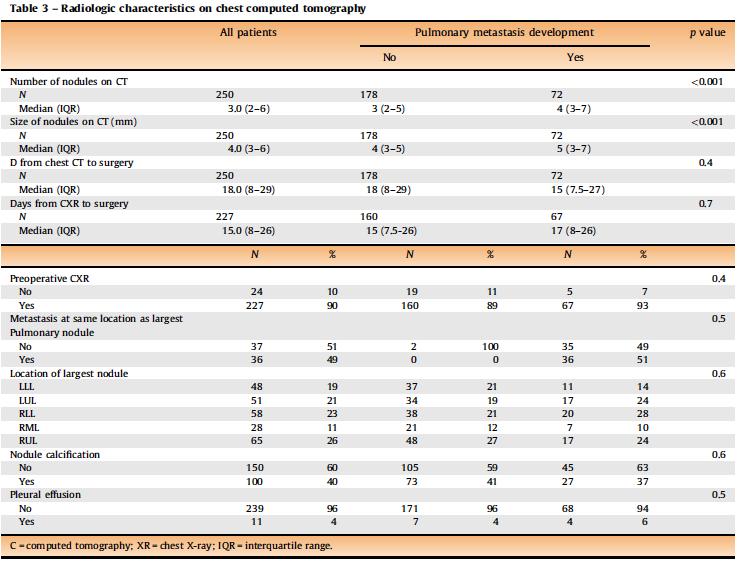
21 Most common site of metastasis in pt with RCC is the lung (45-75%) Indeterminate pulmonary nodules (IPN): 1mm-2cm round pulmonary opacity that may be benign or malignant Determine predictors of progression of an IPN to pulmonary metastasis in pt with localized or locally advanced RCC treated with nephrectomy.

22 MATERIALS & METHODS 251 pt with IPM in prop CT FU at least 3years (Q3-6mt CT or CXR) IPM <2cm Considered Pulmonary M when Increase of size Increase of number Histological diagnosis RESULTS IPN developed in M+ 29% (FU 35.3mo) IPN not develop in M+ 71% (FU 38mo)


23 RESULTS T N G LVI Sarc IVC pt3a
24 RESULTS



25 RESULTS 3y 65%


26 RESULTS 79%
27 Nomogram for LMFS Calibra?on plot of the predicted probability of 3y vs actual % of pt who survived 3y without LM
28 STUDY LIMITATIONS RetrospecZve study Single insztuzon SelecZon bias NOT standard preoperazve and postoperazve imaging strategy Heterogeneous treatment strategy a er diagnosis of pulmonary M may change DSS
29 TAKE HOME MESSAGE IPN have a higher probability of becoming M+ in pt with high T stage high N stage high Grade thrombi Presence of fat invasion Presence of LVI Presence of more and larger nodules in preop CT Although this knowledge will not change clinical management Beger risk stra?fica?on will change FU?ming and influence adjuvant TX strategies.
 PotenZally higher risk of Ureteral scarring/stricture UTUC recurrence (reflux?) Predic?")
30 Tumor in the IMPDU is unusual (finding of tumor in UO during TURBT) Complete TURBT (wide resec?on of the UO) PotenZally higher risk of Ureteral scarring/stricture UTUC recurrence (reflux?) Predic?ve factors for development of Ureteral scarring/stricture UTUC recurrence (reflux?)
31 MATERIALS & METHODS RetrospecZve analysis: 2,317 TURBT pt 112 pt with tumors of the IMPDU Complete TURBT with wide resec?on of UO Double-J catheter for 15d: extensive resec?on of the trigone macroscopic tumor remaining in the distal ureter All cases BCG FU U/S 1 mo a er. If hydro noted CTU 3 mt and Q6mt Stricture if intervenzon needed
32 RESULTS 4.83% (112pt) reseczon of UO Ta in 64% of cases T1 in 27.7% CIS in 17% 31% Double-J catheter (36 pt) Double J did not influence ureteral stenosis recurrent UTUC Distal ureteral stenosis in 11.6% at a median of 47 days UTUC developed in 15.2% (22mt FU) Distal ureter in 65.4% Invasive or high grade 59%-NUx

33 RESULTS Recurrent Tumor associa?on with Ureteral Stenosis and UTUC 42% were recurrent SS differences between primary and recurrent tumors with respect to the incidence of: ü symptoms at diagnosis (60% vs 26%, p <0.001), ü development of ureteral stenosis (4.6% vs 21.3%, p ) ü incidence of UTUC (4.6% vs 29.8%, p <0.001). Treatment of 13 pazents with ureteral stenosis: de-obstruczve TURBT in 6 (46%), ureteral reimplanta?on in 5 (38%) balloon dilazon in 2 (15%)
34 RESULTS UO stenosis UTUC univariate mulzvariate univariate mulzvariate Recurrent tumors Tumor Size>1.5cm T1 bladder & IMDU Cis IMDU
35 STUDY LIMITATIONS Retrospec?ve study Small number of pt with stenosis & UTUC recurrence Stent placement only when extended resec?on selec7on bias Not able to evaluate vesicoureteral reflux and therefore not possible to associate recurrent UTUC with reflux or primary mulzfocal disease
36 Tumor at the UO occurs with at 4.8% of TURBTs A er complete Resec?on of the UO a er a mean FU 56mo: Stenosis occurred at 11.6% UTUC occurred 15.2% On mul?variate analysis Tumor size >1.5cm and T1 stage were factors for stenosis T1 in the bladder and CIS in the IMPDU were factors for UTUC recurrence Double J stent did not influence the occurrence or not of stenosis TAKE HOME MESSAGE

37 Immediate RC is considered the gold standard a er BCG failure Salvage IVT in pazents who want to maintain their bladder Early RC a er BCG fails vs. delayed RC a er salvage IVT fails


38 MATERIALS & METHODS GROUP 1: Early RCx acer BCG failure GROUP 2: Late RCx acer salvage IVT T1 61 pt 56 pt cis Path report of last TURB before RCB
39 RESULTS Median?me from diagnosis prompzng for BCG to RCx 0.81years in group A 2.51 years in group B 1.7y retained their bladder more in group B Group B Underes?mated 37 pt NOT included Did not require RCx acer salvage IVT (for 5.7years)



40 RESULTS Predictors of upstaging LVI most strongly predicted muscle invasion 8 /10 pt with at least 1 TUR specimen with LVI progressed to pt2 or greater at RC
41 RESULTS OS 5y 80% CSS 5y 85% Median FU acer RCx Group A 4.68y Group B 5.14y A er RC bladder cancer recurred in 32 pazents, 15 in group 1 17 in group 2.
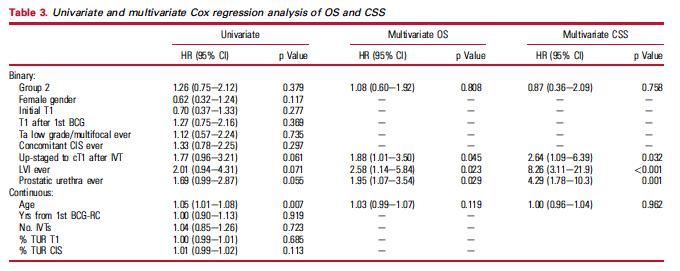

42 RESULTS Significant predictors of death
43 TAKE HOME MESSAGE Pa?ents that select to defer RCx and do further IVT a er they fail BCG, have similar OS and CSS while keeping their bladder for longer. Risk factors of poor prognosis in this popula?on include repezzve instances of ct1 and CIS, upstaging to ct1 prosta?c urethra involvement. LVI on any TUR specimen (very poor prognoszcator) (8/10 pt had MIBC at RC & 7/10 died of BC) 2 or more of these risk factors should prompt serious considerazon of abandoning further IVT in favor of RC..

44 Delay of RCx >12 weeks from diagnosis is associated with inferior survival (higher pt3-4, pn+) Determine the effect on survival of the?ming of radical cystectomy from the diagnosis of MIBC in pazents who received NAC
 2) intervals between diagnosis of MIBC and the inizazon of NAC and RCx; 3) Post-treatment and treatment clinical and pathological")
45 MATERIALS & METHODS CX + NAC JHH database Pa?ent Popula?on PaZent charts for 1) pretreatment characteris?cs (demographics, clinical stage, histology and previous IVT) 2) intervals between diagnosis of MIBC and the inizazon of NAC and RCx; 3) Post-treatment and treatment clinical and pathological characteriszcs. Study End Points Complete pathological response a er NAC (no tumor) Par?al pathological response a er NAC (no MIBC) Pathological response rate (%of pazents with CR & PR) Overall survival
46 RESULTS 201 pt NAC + extravesical Dx (35%) T3 28% T4 7% LND 9% 29% had variant histologies (squamous/ adenomatous/ micropapillary /sarcomatoid)
 51% pathological response rate Median OS 43.2 mo Be er OS age < 62 years (p. 0.")
47 RESULTS At cystectomy 22% complete pathological response (T0) 29% par?al pathological response (Tis/T1) 51% pathological response rate Median OS 43.2 mo Be er OS age < 62 years (p ) pure urothelial histology (p ) Worse OS < 3 cycles NAC extravesical /N+ disease (p ).

48 Dx 6wk NAC RESULTS 28wk 22wk 4GC-12wk 10wk RCx Associa?on of OS and Treatment Intervals P=0.36 P=0.8 P=0.38 None of the treatment intervals was significantly associated with OS
 Small sample GC predominantly used in this study (safety profile) Short FU Pt treated")
49 STUDY LIMITATIONS RetrospecZve Inherent selec?on bias (Young/caucasian pt) Small sample GC predominantly used in this study (safety profile) Short FU Pt treated with NAC who had progression or toxicity were not captured in this database
50 TAKE HOME MESSAGES There was a 51% pathological response rate (22% CR, 29% PR) NO associa?on between OS and?me between MIBC diagnosis and cystectomy in pazents with MIBC receiving NAC. Less than 3 cycles of NAC and extravesical and or pn+ Dx is associated with worse OS. However delays in treatment should not be legi?mized based on this study. In pa?ents not receiving NAC, prompt surgical intervenzon remains the standard of care.

 micturi?")
 higher quality of life scores.")
51 166 T1 HG randomised Low dose 40mg 8wk Standard dose 80mg Complete response rates low dose 79% standard dose 85% Low dose less fever (p = 0.001) micturi?on pain (p = 0.047) higher quality of life scores. No differences recurrence, Progression Overall survival



52 Comparing the short-term outcomes and complica?ons of monopolar and bipolar transurethral resec?on of non-muscle invasive bladder cancers: a prospec?ve, randomized, controlled study. Bolat D 1, Gunlusoy B 1, Degirmenci T 1, Ceylan Y 1, Polat S 1, Aydin E 1, Aydogdu O 1, Kozacioglu Z 1. Bipolar TURBT had significantly lower obturator jerk and bladder perfora?on than monopolar. B- TURBT is a reasonable treatment modality in pazents with NMIBC.
53 Ευχαριστώ

54 5% improvement in OS with NAC included only 4% with cn1-3 disease. Thus, NAC results may not necessarily extend to cn1-3. Clinical outcomes in pt with BCa & cn1-3 treated with induc?on chemotherapy followed by radical cystectomy are limited. In this study we assess pathological and survival outcomes
55 PATIENTS & METHODS Mul?-ins?tu?onal retrospeczve analysis (19 centers) PaZents with ct1-4an1-n3 urothelial carcinoma who received NAC followed by RCB. Lymph node status based on imaging criteria Chemotherapy regimens: MVAC GC other (not cisplazn) End points pathological response rates complete (pt0n0) par?al (pt1n0 or less) overall survival. factors prediczng outcomes
 had cn1-3 248/304 (82%) had pn0-3 RESULTS Chemo regimens GC 43% MVAC 42% Other")
 27% (pcr was only seen in pa7ents with cn1-n2).")
56 Number of pa?ents 304/1618 (19%) had cn /304 (82%) had pn0-3 RESULTS Chemo regimens GC 43% MVAC 42% Other 15% (median 4 cycles) Pathological Complete and Par?al Response pcr (pt0n0) 14.5% ppr (pt1n0 or less) 27% (pcr was only seen in pa7ents with cn1-n2). On mulzvariable analysis none of the selected variables were independent predictors of pcr or ppr pcr & ppr was similar with all chemo regimens
")
57 RESULTS Pathological Nodal Response. pcnr (pn0) 48% 56% of cn1 39% of cn2 39% of cn3 (p.0.03) OS improved in cn2-3 cases that became pn0 vs those remained pn+. Of pt0 bladder status pa7ents 38% were found to have posi7ve lymph nodes (pt0n+)




58 RESULTS P< mo 107mo 45mo 14mo Median OS for the enzre cohort was 23 mo 55% local recurrence or M+ disease (151 pt) Overall 50% pt died during FU (median of 10 mo) 88% of them died of bladder cancer 28% with pt0 23% with pn0 18% with pcr
 Remained NSS a er controlling for age, gender, T stage (p=0.")
 Number of nodes removed")
59 RESULTS OS longer for cn1 vs cn2-3 but NSS (p=0.23) Remained NSS a er controlling for age, gender, T stage (p=0.11) At the cutoff point of 15 lymph nodes removed OS was p=0.01 OS associated with pcr of nodes (pn0) Number of nodes removed (-)sm Cispla?n Tx (MVAC vs GC same)

60 RESULTS Pa?ents with Unknown Pathological Nodal status Median survival similar to the pn+ cohort worse than the pn0
61 RetrospecZve study No standardizazon of chemotherapy (dose, data on toxicity, morbidity and mortality) SelecZon bias in the choice of chemotherapy regimens. Some Pt with cn1-3 not proceed to RC (seleczon bias-favorable subset of cn1-3pt) Not centralized radiological and pathological review Not always biopsy confirmazon of nodal involvement Risk factors not included performance status medical comorbidizes, Hydronephrosis Cardiovascular status Renal funczon STUDY LIMITATIONS
62 Induc?on chemotherapy in N+ pazents associated with a clinically significant pathological response. Complete pathological nodal response can be achieved, even in pazents with cn2-3 disease, and this corresponds to improved survival. 48% of cn1-3 cases converted to pn0 down staging to pt0 occurred in 24% of cases 38% of pt0 had +N pcr (pt0no) only 14.5% In pazents with cn1-3 disease the best outcomes are seen in those Receiving cispla?n based chemo Same GC and MVAC Have nega?ve margins Complete nodal response at RC. TAKE HOME MESSAGES
63 Eur Urol Jan;69(1):60-9. doi: /j.eururo Epub 2015 Jul 23. EORTC Nomograms and Risk Groups for Predic?ng Recurrence, Progression, and Disease-specific and Overall Survival in Non-Muscle-invasive Stage Ta-T1 Urothelial Bladder Cancer Pa?ents Treated with 1-3 Years of Maintenance Bacillus Calmege- Guérin. Cambier S 1, Sylvester RJ 2, Colle e L 1, Gontero P 3, Brausi MA 4, van Andel G 5, Kirkels WJ 6, Silva FC 7, Oosterlinck W 8, Presco S 9, Kirkali Z 10, Powell PH 11, de Reijke TM 12, Turkeri L 13, Colle e S 1, Oddens J 14. Data for 1812 pazents were merged from two European OrganizaZon for Research and Treatment of Cancer randomized phase 3 trials in intermediate- and high-risk NMIBC. With a median follow-up of 7.4 yr, 762 pazents recurred; 173 progressed; and 520 died, 83 due to bladder cancer (BCa). StaZsZcally significant prognoszc factors idenzfied by mulzvariable analyses were prior recurrence rate and number of tumors for recurrence, and tumor stage and grade for progression and death due to BCa. T1G3 pazents do poorly, with 1- and 5-yr disease-progression rates of 11.4% and 19.8%, respeczvely, and 1- and 5-yr disease-specific death rates of 4.8% and 11.3%. LimitaZons include lack of repeat transurethral reseczon in high-risk pazents and exclusion of pazents with carcinoma in situ. NMIBC pazents treated with 1-3 yr of maintenance BCG have a heterogeneous prognosis. PaZents at high risk of recurrence and/or progression do poorly on currently recommended maintenance schedules. AlternaZve treatments are urgently required.
Early radical cystectomy in NMIBC Marko Babjuk
 Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Management of Locally Reccurent Renal Cell Carcinoma. Jose A. Karam, MD, FACS Assistant Professor Department of Urology
 Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer
 Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015
 Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Reviewing Immunotherapy for Bladder Carcinoma In Situ
 Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Treatment of Invasive Bladder Cancer in the Elderly and Frail Pa9ent
 Treatment of Invasive Bladder Cancer in the Elderly and Frail Pa9ent Jehonathan H Pinthus MD, Ph.D, FRCSC Associate Professor Department of Surgery/Urology McMaster University Life expectancy Current age
Treatment of Invasive Bladder Cancer in the Elderly and Frail Pa9ent Jehonathan H Pinthus MD, Ph.D, FRCSC Associate Professor Department of Surgery/Urology McMaster University Life expectancy Current age
Role and extension of lymph node dissection in kidney, bladder and prostate cancer. Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017
 Moderator: Dr A. Noujem 30 th March 2017") Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
Intravesical Therapy for Bladder Cancer
 Intravesical Therapy for Bladder Cancer Alexandre R. Zlotta, MD, PhD, FRCSC Professor, Department of Surgery (Urology), University of Toronto Director, Uro-Oncology, Mount Sinai Hospital Director, Uro-Oncology
Intravesical Therapy for Bladder Cancer Alexandre R. Zlotta, MD, PhD, FRCSC Professor, Department of Surgery (Urology), University of Toronto Director, Uro-Oncology, Mount Sinai Hospital Director, Uro-Oncology
NMIBC. Piotr Jarzemski. Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland
 NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
Controversies in the management of Non-muscle invasive bladder cancer
 Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC
 The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
Chemotherapy and Bladder Cancer. Blayne Welk UBC Urology Grand Rounds June 4, 2008
 Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer
 Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Current Findings on High Intensity Focused Ultrasound (HIFU) Thomas J Polascik, MD, FACS Professor of Surgery
 Thomas J Polascik, MD, FACS Professor of Surgery") Current Findings on High Intensity Focused Ultrasound (HIFU) Thomas J Polascik, MD, FACS Professor of Surgery Outline Whole gland abla6on selec6on and outcomes Focal abla6on - Eligibility and pa6ent selec6on
Current Findings on High Intensity Focused Ultrasound (HIFU) Thomas J Polascik, MD, FACS Professor of Surgery Outline Whole gland abla6on selec6on and outcomes Focal abla6on - Eligibility and pa6ent selec6on
UROTHELIAL CELL CANCER
 UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Lymphadenectomy in RCC: Yes, No, Clinical Trial?
 Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
ROBOTIC VS OPEN RADICAL CYSTECTOMY
 ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy?
 Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy? 80 patients LNU (n = 40) or ONU (n = 40) CSS (p = 0.2), BRFS (p = 0.86), MFS (p = 0.12) similar for the entire cohort Subgroups of pt3 UTUC
Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy? 80 patients LNU (n = 40) or ONU (n = 40) CSS (p = 0.2), BRFS (p = 0.86), MFS (p = 0.12) similar for the entire cohort Subgroups of pt3 UTUC
Management of High-Risk Non-Muscle Invasive Bladder Cancer. Seth P. Lerner, MD, FACS
 Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of
Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of
Oral Communications & Posters
 Carcinoma uroteliale: Current and future directions of treatment of Muscle-Invasive Bladder cancer/ Multimodality approach of bladder cancer Oral Communications & Posters CRISTINA MASINI Oncologia Medica
Carcinoma uroteliale: Current and future directions of treatment of Muscle-Invasive Bladder cancer/ Multimodality approach of bladder cancer Oral Communications & Posters CRISTINA MASINI Oncologia Medica
Non Muscle Invasive Bladder Cancer. Primary and Recurrent TCC 4/10/2010. Two major consequences: Strategies: High-Risk NMI TCC
 Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
WHAT IS THE ROLE OF ACTIVE SURVEILLANCE
 WHAT IS THE ROLE OF ACTIVE SURVEILLANCE IN THE CONTEXT OF RENAL ABLATION AND PARTIAL NEPHRECTOMY? Alessandro Volpe University of Eastern Piedmont Novara, Italy RCC INCIDENCE SEER DATABASE (1975-2006) RCC
WHAT IS THE ROLE OF ACTIVE SURVEILLANCE IN THE CONTEXT OF RENAL ABLATION AND PARTIAL NEPHRECTOMY? Alessandro Volpe University of Eastern Piedmont Novara, Italy RCC INCIDENCE SEER DATABASE (1975-2006) RCC
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Ode to a node Lymph node dissec3on in prostate and bladder cancer
 5/26/10 Ode to a node Lymph node dissec3on in prostate and bladder cancer Anthony Koupparis 1 Introduc3on prostate cancer PLND most accurate and reliable staging method for LNI Imaging techniques have
5/26/10 Ode to a node Lymph node dissec3on in prostate and bladder cancer Anthony Koupparis 1 Introduc3on prostate cancer PLND most accurate and reliable staging method for LNI Imaging techniques have
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
5/26/16: CT scan of the abdomen showed a multinodular liver disease highly suspicious for metastasis and hydronephrosis of the right kidney.
 Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
 30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer Center Contemporary Experience
 International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
T1HG Bladder Cancer What is the Best Therapy?
 T1HG Bladder Cancer What is the Best Therapy? Ashish M. Kamat, MD, MBBS, FACS Professor of Urology Director, Urologic Oncology Fellowship Guidelines for T1HG Bladder Cancer AUA Recommendation: BCG induction
T1HG Bladder Cancer What is the Best Therapy? Ashish M. Kamat, MD, MBBS, FACS Professor of Urology Director, Urologic Oncology Fellowship Guidelines for T1HG Bladder Cancer AUA Recommendation: BCG induction
Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer
 Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer Andrew J. Stephenson, MD, FRCSC, FACS Director, Urologic Oncology Associate Professor of Surgery Glickman Urological and Kidney
Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer Andrew J. Stephenson, MD, FRCSC, FACS Director, Urologic Oncology Associate Professor of Surgery Glickman Urological and Kidney
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists. Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
A patient with recurrent bladder cancer presents with the following history:
 MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
Disclosures. The Importance of Pathology? Pathologic, Morphologic and Clinical Features. Pathologic Reproducibility
 The Importance of Pathology? Seth P. Lerner, MD, FACS Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine Support for research Disclosures Photocure, Imalux,
The Importance of Pathology? Seth P. Lerner, MD, FACS Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine Support for research Disclosures Photocure, Imalux,
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
 A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
Issues in the Management of High Risk Superficial Bladder Cancer
 Issues in the Management of High Risk Superficial Bladder Cancer MICHAEL A.S. JEWETT DIVISION OF UROLOGY, DEPARTMENT OF SURGICAL ONCOLOGY, PRINCESS MARGARET HOSPITAL & THE UNIVERSITY OF TORONTO 1 Carcinoma
Issues in the Management of High Risk Superficial Bladder Cancer MICHAEL A.S. JEWETT DIVISION OF UROLOGY, DEPARTMENT OF SURGICAL ONCOLOGY, PRINCESS MARGARET HOSPITAL & THE UNIVERSITY OF TORONTO 1 Carcinoma
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Ureteroscopy Is Indicated in every patient with suspected Upper Tract Urothelial Tumor
 Ureteroscopy Is Indicated in every patient with suspected Upper Tract Urothelial Tumor Scott G. Hubosky, MD The Demetrius H. Bagley Jr., MD Associate Professor of Urology Director of Endourology Vice Chair
Ureteroscopy Is Indicated in every patient with suspected Upper Tract Urothelial Tumor Scott G. Hubosky, MD The Demetrius H. Bagley Jr., MD Associate Professor of Urology Director of Endourology Vice Chair
Neoadjuvant chemotherapy for bladder cancer: fighting between evidence 1 level and real life.
 THE INTERNATIONAL CONFERENCE PROGRESS IN URO-ONCOLOGY 5th Edition September, 25th 26th 2014 CLUJ-NAPOCA Neoadjuvant chemotherapy for bladder cancer: fighting between evidence 1 level and real life. Dr.
THE INTERNATIONAL CONFERENCE PROGRESS IN URO-ONCOLOGY 5th Edition September, 25th 26th 2014 CLUJ-NAPOCA Neoadjuvant chemotherapy for bladder cancer: fighting between evidence 1 level and real life. Dr.
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
Urinary Bladder Cancer
 Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Staging and Grading Last Updated Friday, 14 November 2008
 Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Critical Evaluation of Early Post-operative Single Instillation Therapy in NMIBC
 Critical Evaluation of Early Post-operative Single Instillation Therapy in NMIBC Levent N. Türkeri MD, PhD Professor of Urology Acıbadem University Faculty of Medicine Istanbul Conflict of Interest No
Critical Evaluation of Early Post-operative Single Instillation Therapy in NMIBC Levent N. Türkeri MD, PhD Professor of Urology Acıbadem University Faculty of Medicine Istanbul Conflict of Interest No
Contemporary management of high-grade T1 bladder cancer Arnulf Stenzl
 Contemporary management of high-grade T1 bladder cancer Arnulf Stenzl Dep. of Urology, Eberhard-Karls University, Tuebingen, Germany Treatment options in HG T1 BCa TUR-BT Primary and second resection (T0-status)
Contemporary management of high-grade T1 bladder cancer Arnulf Stenzl Dep. of Urology, Eberhard-Karls University, Tuebingen, Germany Treatment options in HG T1 BCa TUR-BT Primary and second resection (T0-status)
Original Article APMC-276
 Original Article APMC-276 The Clinical Value of Immediate Second Transurethral Resection in Patients with High Grade Non-Muscle Inasive Bladder Cancer (HG-NMIBC) Syed Saleem Abbas Jafri, Zafar Iqbal Khan
Original Article APMC-276 The Clinical Value of Immediate Second Transurethral Resection in Patients with High Grade Non-Muscle Inasive Bladder Cancer (HG-NMIBC) Syed Saleem Abbas Jafri, Zafar Iqbal Khan
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
BLADDER CANCER: PATIENT INFORMATION
 BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
Radical Cystectomy Often Too Late? Yes, But...
 european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
Old and New Radiation for Bladder and Upper Tract Cancers. Bridget Koontz Radiation Oncology Duke Cancer Institute
 Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC)
") Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 :$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
:$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
Bladder Case 1 SURGICAL PATHOLOGY REPORT. Procedure: Cystoscopy, transurethral resection of bladder tumor (TURBT)
") Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Complex case Presentations
 Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
Carcinoma of the Renal Pelvis and Ureter Histopathology
 Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Management options for high-risk, BCG-refractory NMIBC. Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center
 Management options for high-risk, BCG-refractory NMIBC Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center Bladder Cancer in U.S. 4 th most common cancer in men 9 th
Management options for high-risk, BCG-refractory NMIBC Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center Bladder Cancer in U.S. 4 th most common cancer in men 9 th
Surgeons Perspective: LN as a Draining Pattern. Jose A. Karam, MD, FACS Associate Professor Department of Urology
 Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Case 1. Receives induction BCG weekly x 6 without significant toxicity Next step should be:
 Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
Does the Use of Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers Improve Survival in Bladder Cancer?
 Does the Use of Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers Improve Survival in Bladder Cancer? Authors: Roderick Clark, 1 Kevin Wong, 2 Stacy Fan, 2 Joseph Chin, 1,3 Jonathan
Does the Use of Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers Improve Survival in Bladder Cancer? Authors: Roderick Clark, 1 Kevin Wong, 2 Stacy Fan, 2 Joseph Chin, 1,3 Jonathan
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
Clinical significance of immediate urine cytology after transurethral resection of bladder tumor in patients with non-muscle invasive bladder cancer
 International Journal of Urology (2011) 18, 439 443 doi: 10.1111/j.1442-2042.2011.02766.x Original Article: Clinical Investigationiju_2766 439..443 Clinical significance of immediate urine cytology after
International Journal of Urology (2011) 18, 439 443 doi: 10.1111/j.1442-2042.2011.02766.x Original Article: Clinical Investigationiju_2766 439..443 Clinical significance of immediate urine cytology after
 Case Presentation 58 year old male with recent history of hematuria, for which he underwent cystoscopy. A 1.5 cm papillary tumor was found in the left lateral wall of the bladder. Pictures of case Case
Case Presentation 58 year old male with recent history of hematuria, for which he underwent cystoscopy. A 1.5 cm papillary tumor was found in the left lateral wall of the bladder. Pictures of case Case
Renal Mass Biopsy: Needed Now More than Ever
 Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Options for first-line cisplatin-eligible patients
 The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
Indications For Partial
 Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic
 Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic renal cell carcinoma Wassim Kassouf, Leonardo L. Monteiro, Darrel E. Drachenberg, Adrian S. Fairey,
Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic renal cell carcinoma Wassim Kassouf, Leonardo L. Monteiro, Darrel E. Drachenberg, Adrian S. Fairey,
Lymph node dissection: how much is enough?
 1 Background Lymph node dissection: how much is enough? Eila C. Skinner, MD Professor of Clinical Urology USC Keck School of Medicine Radical cystectomy is the gold standard for the treatment of invasive
1 Background Lymph node dissection: how much is enough? Eila C. Skinner, MD Professor of Clinical Urology USC Keck School of Medicine Radical cystectomy is the gold standard for the treatment of invasive
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
BLADDER CANCER EPIDEMIOLOGY
 BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Why Do Axillary Dissection? Nodal Treatment and Survival NSABP B04. Revisiting Axillary Dissection for SN Positive Patients
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Vincenzo Ficarra. Direttore Clinica di Urologia Azienda Ospedaliera Universitaria di Udine
 Best Papers on Kidney Cancer Vincenzo Ficarra Direttore Clinica di Urologia Azienda Ospedaliera Universitaria di Udine Uro-oncological oncological topics Renal Tumor biopsy Positive Surgical Margins after
Best Papers on Kidney Cancer Vincenzo Ficarra Direttore Clinica di Urologia Azienda Ospedaliera Universitaria di Udine Uro-oncological oncological topics Renal Tumor biopsy Positive Surgical Margins after
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of intravesical microwave hyperthermia with intravesical chemotherapy for superficial
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of intravesical microwave hyperthermia with intravesical chemotherapy for superficial
Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer. Cheol Min Kang 2018/04/05
 Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Impact of adjuvant chemotherapy on patients with pathological Stage T3b and/or lymph node metastatic bladder cancer after radical cystectomy
 Japanese Journal of Clinical Oncology, 2015, 45(10) 963 967 doi: 10.1093/jjco/hyv098 Advance Access Publication Date: 29 July 2015 Original Article Original Article Impact of adjuvant chemotherapy on patients
Japanese Journal of Clinical Oncology, 2015, 45(10) 963 967 doi: 10.1093/jjco/hyv098 Advance Access Publication Date: 29 July 2015 Original Article Original Article Impact of adjuvant chemotherapy on patients
Risk Adapted Treatment of Non-muscle Invasive Bladder Cancer. Eila C. Skinner, MD
 Risk Adapted Treatment of Non-muscle Invasive Bladder Cancer Eila C. Skinner, MD Professor, Department of Urology Stanford University SWIU Winter Meeting January, 2015 Goals Minimize treatment for patients
Risk Adapted Treatment of Non-muscle Invasive Bladder Cancer Eila C. Skinner, MD Professor, Department of Urology Stanford University SWIU Winter Meeting January, 2015 Goals Minimize treatment for patients
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience. Paul Gellhaus Assistant Clinical Professor
 Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience Paul Gellhaus Assistant Clinical Professor Iowa??? none Disclosures Caveats Dr. Michael O Donnell
Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience Paul Gellhaus Assistant Clinical Professor Iowa??? none Disclosures Caveats Dr. Michael O Donnell
Debate: Adjuvant vs. Neoadjuvant Therapy for Urothelial Cancer
 Debate: Adjuvant vs. Neoadjuvant Therapy for Urothelial Cancer Kala Sridhar, MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital GU Medical Oncology Site Group Head Associate Professor, University
Debate: Adjuvant vs. Neoadjuvant Therapy for Urothelial Cancer Kala Sridhar, MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital GU Medical Oncology Site Group Head Associate Professor, University
September 10, Dear Dr. Clark,
 September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
Bladder Cancer in Primary Care. Dr Penny Kehagioglou Consultant Clinical Oncologist
 Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Pathologic Assessment of Invasion in TUR Specimens. A. Lopez-Beltran. T1 (ct1)
") Pathologic Assessment of Invasion in TUR Specimens A. Lopez-Beltran T1 (ct1) 1 Prognostic factors for progression/invasive disease Ta,T1,CIS- NMIBC :TNM 2017 ESSENTIAL: Grade T stage CIS Number of lesions
Pathologic Assessment of Invasion in TUR Specimens A. Lopez-Beltran T1 (ct1) 1 Prognostic factors for progression/invasive disease Ta,T1,CIS- NMIBC :TNM 2017 ESSENTIAL: Grade T stage CIS Number of lesions
Renal biopsy is mandatory for every small renal mass
 Renal biopsy is mandatory for every small renal mass Ben Challacombe Consultant Urologist The Urology Centre Guy s and St. Thomas Hospital NHS Foundation Trust Oncocytoma High Risk Partial converted to
Renal biopsy is mandatory for every small renal mass Ben Challacombe Consultant Urologist The Urology Centre Guy s and St. Thomas Hospital NHS Foundation Trust Oncocytoma High Risk Partial converted to
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Urothelial Tumors of the Upper Tract: Diagnosis and Management. Daniel Rapoport April 11, 2007 Urology Grand Rounds
 Urothelial Tumors of the Upper Tract: Diagnosis and Management Daniel Rapoport April 11, 2007 Urology Grand Rounds 1 Overview Background Epidemiology and risk factors Natural history and prognostic factors
Urothelial Tumors of the Upper Tract: Diagnosis and Management Daniel Rapoport April 11, 2007 Urology Grand Rounds 1 Overview Background Epidemiology and risk factors Natural history and prognostic factors
Intravesical Gemcitabine for High Risk, Nonmuscle Invasive Bladder Cancer after Bacillus Calmette-Guerin Treatment Failure
 Intravesical Gemcitabine for High Risk, Nonmuscle Invasive Bladder Cancer after Bacillus Calmette-Guerin Treatment Failure Itay A. Sternberg, Guido Dalbagni,* Ling Y. Chen, Sherri M. Donat, Bernard H.
Intravesical Gemcitabine for High Risk, Nonmuscle Invasive Bladder Cancer after Bacillus Calmette-Guerin Treatment Failure Itay A. Sternberg, Guido Dalbagni,* Ling Y. Chen, Sherri M. Donat, Bernard H.
models; Kaplan meier curves were also extrapolated for each cohort to compare disease specific and overall survival patterns.
 ; 21 Urological Oncology MUSCULARIS PROPRIA AND UPSTAGING OF ct1 BLADDER CANCER BADALATO ET AL. BJUI Does the presence of muscularis propria on transurethral resection of bladder tumour specimens affect
; 21 Urological Oncology MUSCULARIS PROPRIA AND UPSTAGING OF ct1 BLADDER CANCER BADALATO ET AL. BJUI Does the presence of muscularis propria on transurethral resection of bladder tumour specimens affect
ICUD 2011 Recommendations. Bladder Cancer
 ICUD 2011 Recommendations Bladder Cancer ICUD Bladder Cancer 2011 Chair Mark Soloway Co chair Henk van der Poel Committee Chairs A. Kamat/P. Hegarty M. Amin/V. Reuter P. Karakiewicz/S. Shariat B. Konety/W.
ICUD 2011 Recommendations Bladder Cancer ICUD Bladder Cancer 2011 Chair Mark Soloway Co chair Henk van der Poel Committee Chairs A. Kamat/P. Hegarty M. Amin/V. Reuter P. Karakiewicz/S. Shariat B. Konety/W.
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.
 Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone