Barrett esophagus. Bible class Inselspital
|
|
|
- Domenic Bates
- 5 years ago
- Views:
Transcription

1 Barrett esophagus Bible class Inselspital

2 Guidelines
3 Definition? BSG: ACG:

4 Definition? BSG: ACG:
5 What are the arguments for and against IM as prerequisite for the Dg?
6 What are the arguments for and against IM as prerequisite for the Dg? - Intestinal metaplasia is biologically more unstable Bhat S et al. Risk of malignant progression in Barrett's esophagus patients: results from a large population-based study.j Natl Cancer Inst Possible sampling error (false negativ Bx) Harrison R et al. Detection of intestinal metaplasia i Barrett s esophagus: an observational comparator study suggests the need for a minimum of eight biopsies. Am J Gastroenterol Evolution of IM over the time Gatenby PA et al. Relevance of the detection of intestinal metaplasia in non-dysplastic columnar-lined oesophagus. Scand J Gastroenterol 2008
7 What are the arguments for and against IM as prerequisite for the Dg? - < 50 of endoscopically resected OAC have IM Takubo K et al. Cardiac rather than intestinal-type background in endoscopic resection specimens of minute Barrett adenocarcinoma. Hum Pathol 2009.
8 What are the arguments for and against IM as prerequisite for the Dg? - < 50 of endoscopically resected OAC have IM Takubo K et al. Cardiac rather than intestinal-type background in endoscopic resection specimens of minute Barrett adenocarcinoma. Hum Pathol Is IM of the cardia of concern?
9 What are the arguments for and against IM as prerequisite for the Dg? - < 50 of endoscopically resected OAC have IM Takubo K et al. Cardiac rather than intestinal-type background in endoscopic resection specimens of minute Barrett adenocarcinoma. Hum Pathol Is IM of the cardia of concern? - No, 20% of people harbour IM Zaninotto G et al. Prevalence of intestinal metaplasia in the distal oesophagus, oesophagogastric junction and gastric cardia in symptomatic patients in north-east Italy. Dig Liver Dis 2001.
10 How is the distal esophageal and endoscopically defined?
11 How is the distal esophageal and endoscopically defined?
12 How is the distal esophageal and endoscopically defined? Is this a potential barrett esophagus?
13 How is the distal esophageal and endoscopically defined? Is this a potential barrett esophagus? No!
14 What describes the Prague Classification?
15 What describes the Prague Classification?
16 What should be further recorded?

17 What should be further recorded?
18 Biopsy protocol and importang aspects of sampling?
19 Biopsy protocol and importang aspects of sampling? - Targeted biopsies from visible lesions - 4 Quadrant biopsies every 2 cm - Optimize visualisation (Inspection of the OGJ by inversion if possible, careful flushing, acetic acid, starting distal and basal, inspection time!)
20 Screening/surveillance «Optimal» disease for a screening?
21 Screening/surveillance - «Optimal» disease for a screening? Disease with a high morbidity/mortality A early diagnosis leads to improved survival High prevalence of the disease in a certain population - High positive and negative predictive values of the test - Cost effective and well tolerated test/treatment
22 Screening Whats the prevalence of BE?
23 Screening Whats the prevalence of BE? -.5% 5% if GERD)
24 Screening Whats the prevalence of BE? -.5% 5% if GERD) What are the risk factors of BE?
25 Screening - Whats the prevalence of BE?.5% 5% if GERD) What are the risk factors of BE? Male gender, caucasian ethnicity Older age History of GERD Possible cigarette smoking Family history Abdominal adiposity
26 Is screening recommended?


27 Is screening recommended?
28 Surveillance Is there evidence I for surveillance?

29 Surveillance Is there evidence I for surveillance? - No, BOSS trial avaited
30 What are the most important arguments for the surveillance?
31 What are the most important arguments for the surveillance? - OAC has a very poor overall 5 year survival < 20% - OAC detected by screening have an earlier stage and better survival rate
32 What are the most important arguments for the surveillance? - OAC has a very poor overall 5 year survival < 20% - OAC detected by screening have an erlier stage and better survival rate Usefullness of surveillance proved?
33 What are the most important arguments for the surveillance? - OAC has a very poor overall 5 year survival < 20% - OAC detected by screening have an erlier stage and better survival rate Usefullness of surveillance proved? - No!
34 Why?
35 Why? - Lenght time bias:

36 - Lead time bias:
37 Is surveillance recommended?

38 Is surveillance recommended?
39 What s the incidence of OAC in BE?
40 What s the incidence of OAC in BE? %/year Bhat S et al. Risk of malignant progression in Barrett's esophagus patients: results from a large population-based study.j Natl Cancer Inst %/year Hvid-Jensen F et al. Incidence of adenocarcinoma among patients with Barrett s esophagus. N Engl J Med %/year Desai TK et al. Th e incidence of oesophageal adenocarcinoma in non-dysplastic Barrett's oesophagus: a meta-analysis. Gut 2012
41 What are the risk factors for malignant progression?
42 What are the risk factors for malignant progression? - Advancing age - Male gender - S oki g HR! - Length of Barrett esophagus - Ulcers, strictures and nodules! - Lack of PPI, NSAID/ASS, Statins
43 What are the risk factors for malignant progression? - Advancing age - Male gender - S oki g HR! - Length of Barrett esophagus - Ulcers, strictures and nodules! Metaanalysis of - Lack of PPI, NSAID/ASS, Statins cohort studies
44 Is chemoprevention indicated?
45 Is chemoprevention indicated? - AspECT trial awaited
46 Is chemoprevention indicated? - AspECT trial awaited Is fundoplicatio indicated?


47 Is chemoprevention indicated? - AspECT trial awaited Is fundoplicatio indicated?
48 What s the likelyhood to die from an Barrett unrelated cause in patients without dysplasia?
49 What s the likelyhood to die from an Barrett unrelated cause in patients without dysplasia? - > 90% Incarbone R et al. Outcome of esophageal adenocarcinoma detected during endoscopic biopsy surveillance for Barrett's esophagus. Surg Endosc 2002.
50 What s the likelyhood to die from an Barrett unrelated cause in patients without dysplasia? - > 90% Incarbone R et al. Outcome of esophageal adenocarcinoma detected during endoscopic biopsy surveillance for Barrett's esophagus. Surg Endosc What s the risk of progression of dysplasia?

51 What s the likelyhood to die from an Barrett unrelated cause in patients without dysplasia? - > 90% Incarbone R et al. Outcome of esophageal adenocarcinoma detected during endoscopic biopsy surveillance for Barrett's esophagus. Surg Endosc What s the risk of progression of dysplasia?
52 How is the surveillance proposed?
53 How is the surveillance proposed? ECOG score 0-2 (self care possible)
54 How is low grade dysplasia defined?

55 How is low grade dysplasia defined?
56 How is high grade dysplasia defined?

57 How is high grade dysplasia defined?
58 Is the interobserver agreement good for dysplasia?
59 Is the interobserver agreement good for dysplasia? - No, especially for low grad dysplasia
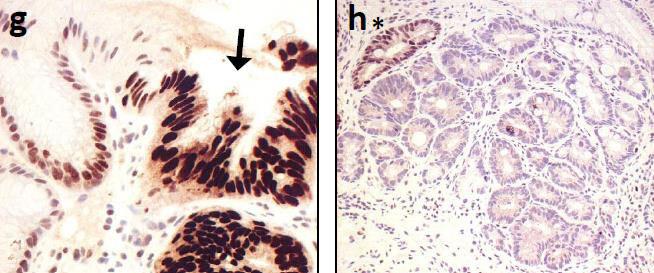
60 Is the interobserver agreement good for dysplasia? - No, especially for low grad dysplasia How it could be improved? - Immunostaining with p53
61 Is the interobserver agreement good for dysplasia? - No, especially for low grad dysplasia How it could be improved?
62 Is the interobserver agreement good for dysplasia? - No, especially for low grad dysplasia How it could be improved? - Immunostaining with p53
63
64
65 How should we manage dysplasia?
66 How should we manage dysplasia?
67 What about the SURF trial?
68 What about the SURF trial?

69 What about the SURF trial?
70 What are the therapeutic options with HGD?
71 What are the therapeutic options with HGD?
72 Risk of lymph node mestasis in T1?

73 Risk of lymph node mestasis in T1? - T1a: 0-10% - T1b SM1: conflicting data, if R0L0 an poor surgical candidate => endoscopic resection - T1b SM2-3: Risk up to 46% => Surgery
74 What should be done after curative endoscopic resection?
75 What should be done after curative endoscopic resection? - Eradication of BE (>80 have remaining dysplasia, 20% metachronous lesions in 2 years
76 What should be done after curative endoscopic resection? - Eradication of BE (>80 have remaining dysplasia, 20% metachronous lesions in 2 years) Is (PET)-CT indicated if early esophageal cancer is supposed?
77 What should be done after curative endoscopic resection? - Eradication of BE (>80 have remaining dysplasia, 20% metachronous lesions in 2 years) Is (PET)-CT indicated if early esophageal cancer is supposed? - No
78 What should be done after curative endoscopic resection? - Eradication of BE (>80 have remaining dysplasia, 20% metachronous lesions in 2 years) Is (PET)-CT indicated if early esophageal cancer is supposed? - No What about EUS?
79 What should be done after curative endoscopic resection? - Eradication of BE (>80 have remaining dysplasia, 20% metachronous lesions in 2 years) Is (PET)-CT indicated if early esophageal cancer is supposed? - No What about EUS? - Can be done, but frequent over- (15 25%) and understaging (4 12%) of T1 vrs T2

80
81 How should we follow up the patients?
82 How should we follow up the patients? - Every 3 month for 1 year, than yearly - Biopsies of the prior extend of BE (burried dysplasia!)

83 How should we follow up the patients? - Every 3 month for 1 year, than yearly - Biopsies of the prior extend of BE (burried dysplasia!)
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Endoscopic Management of Barrett s Esophagus
 Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
In 1998, the American College of Gastroenterology issued ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France
 Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France Barrett s esophagus (BE) is an acquired condition in which the normal squamous epithelium
Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France Barrett s esophagus (BE) is an acquired condition in which the normal squamous epithelium
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Relative risk of dysplasia for patients with intestinal metaplasia in the distal oesophagus and in the gastric cardia
 Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
Changes to the diagnosis and management of Barrett s Oesophagus
 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Accepted Manuscript. CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D
 Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
How to stage early BE cancer - EUS or endoscopic removal?
 How to stage early BE cancer - EUS or endoscopic removal? Presented by Bas Weusten Institution St. Antonius Hospital, Nieuwegein Academic Medical Center, Amsterdam case 56 y old female patient Lung transplant
How to stage early BE cancer - EUS or endoscopic removal? Presented by Bas Weusten Institution St. Antonius Hospital, Nieuwegein Academic Medical Center, Amsterdam case 56 y old female patient Lung transplant
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Everything Esophagus: Barrett s Esophagus. Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina
 Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Current Management of Low-Grade Dysplasia in Barrett Esophagus
 Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Burning Issues in the Esophagus
 Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Chapter 12: Training in Pathology. DDSEP Chapter 13: Question 19
 DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Chapter 2 Complications of Gastroesophageal Reflux Disease
 Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
What s New in the Management of Esophageal Disease
 What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease
 Original Article Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease From Military Hospital, Rawalpindi Obaid Ullah Khan, Abdul Rasheed Correspondence: Dr. Abdul
Original Article Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease From Military Hospital, Rawalpindi Obaid Ullah Khan, Abdul Rasheed Correspondence: Dr. Abdul
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
Original article INTRODUCTION
 Diseases of the Esophagus (2014), DOI: 10.1111/dote.12166 Original article A Barrett s esophagus registry of over 1000 patients from a specialist center highlights greater risk of progression than population-based
Diseases of the Esophagus (2014), DOI: 10.1111/dote.12166 Original article A Barrett s esophagus registry of over 1000 patients from a specialist center highlights greater risk of progression than population-based
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Henry Moon was one of the giants in academic pathology during my early years.
 Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
How to remove BE cancer: EMR or ESD? Expected outcome
 How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia
 ...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
RFA and Cyrotherapy for Esophageal Disease
 RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
Current status of gastric ESD in Korea. Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea
 Current status of gastric ESD in Korea Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea Contents Brief history of gastric ESD in Korea ESD/EMR for gastric adenoma
Current status of gastric ESD in Korea Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea Contents Brief history of gastric ESD in Korea ESD/EMR for gastric adenoma
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Barrett s Esophagus: Are We Making any Progress?
 3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
ESOPHAGEAL CANCER. Epidemiology 3/22/2017. Esophageal Carcinoma: subtypes. Esophageal Adenocarcinoma (EAC) Epidemiology.
 Epidemiology.") ESOPHAGEAL CANCER Disclosures Sushil Ahlawat, MD, FACP, FASGE, AGAF Associate Professor of Medicine Director of Endoscopy RUTGERS NJMS Nothing to disclose. Esophageal Carcinoma: subtypes Subtype Squamous
ESOPHAGEAL CANCER Disclosures Sushil Ahlawat, MD, FACP, FASGE, AGAF Associate Professor of Medicine Director of Endoscopy RUTGERS NJMS Nothing to disclose. Esophageal Carcinoma: subtypes Subtype Squamous
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
Is Radiofrequency Ablation Effective In Treating Barrett s Esophagus Patients with High-Grade Dysplasia?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 30 PRACTICE GUIDELINES nature publishing group CME ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
30 PRACTICE GUIDELINES nature publishing group CME ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process
 MEASURE TYPE: Process") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
Disclosures. Gastroesophageal Reflux Disease. Gastroesophageal Reflux Disease
 Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Adenocarcinoma of the distal esophagus is a recognized
 ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of the distal esophagus, gastroesophageal junction and gastric cardia?
 Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Ablation. See specific types, e.g., Thermal ablation Achalasia, 53 75 described, 53 features of, 53 management of past options, 54 POEM
Index Note: Page numbers of article titles are in boldface type. A Ablation. See specific types, e.g., Thermal ablation Achalasia, 53 75 described, 53 features of, 53 management of past options, 54 POEM
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
Barrett's Esophagus: Sorting Out the Controversy
 Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Disclosures. Gastric Intestinal Metaplasia and Early Gastric Cancer: Screening, Surveillance, and Endoscopic Therapy. ASGE Guidelines.
 Gastric Intestinal Metaplasia and Early Gastric Cancer: Screening, Surveillance, and Endoscopic Therapy Consultant for: Olympus Medtronic US Endoscopy Disclosures Joo Ha Hwang, MD, PhD Associate Professor
Gastric Intestinal Metaplasia and Early Gastric Cancer: Screening, Surveillance, and Endoscopic Therapy Consultant for: Olympus Medtronic US Endoscopy Disclosures Joo Ha Hwang, MD, PhD Associate Professor
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
From reflux to esophageal cancer. Josh Boys, MD TCV 2 nd year indentured servant
 From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus. Original Policy Date
 MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Table 2.9. Case control studies of helicobacter pylori infection and oesophageal adenocarcinoma
 Characteristics of Characteristics of controls Detection Chow et al (1998) 1993-1995 129 of newly diagnosed oesophageal/gastric cardia (OGC) adenocarcinoma. 224 population controls selected by random digit
Characteristics of Characteristics of controls Detection Chow et al (1998) 1993-1995 129 of newly diagnosed oesophageal/gastric cardia (OGC) adenocarcinoma. 224 population controls selected by random digit
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Oesophageal Disorders
 Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, by Am. Coll. of Gastroenterology ISSN /02/$22.00
 THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
Targeting care in Barrett s oesophagus
 HEPATO-GASTROENTEROLOGY Clinical Medicine 2014 Vol 14, No 6: s78 s83 Targeting care in Barrett s oesophagus Authors: Sebastian Zeki A and Rebecca C Fitzgerald B ABSTRACT Barretts oesophagus represents
HEPATO-GASTROENTEROLOGY Clinical Medicine 2014 Vol 14, No 6: s78 s83 Targeting care in Barrett s oesophagus Authors: Sebastian Zeki A and Rebecca C Fitzgerald B ABSTRACT Barretts oesophagus represents
The presence of intestinal-type goblet cells (ITGCs) in
 in") Goblet Cell Mimickers in Esophageal Biopsies Are Not Associated With an Increased Risk for Dysplasia Mamoun Younes, MD; Atilla Ertan, MD; Gulchin Ergun, MD; Ray Verm, MD; Margaret Bridges, MD; Karen Woods,
Goblet Cell Mimickers in Esophageal Biopsies Are Not Associated With an Increased Risk for Dysplasia Mamoun Younes, MD; Atilla Ertan, MD; Gulchin Ergun, MD; Ray Verm, MD; Margaret Bridges, MD; Karen Woods,
Barrett s Esophagus: State of the Art Management
 In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Disclosures. Heartburn and Barrett s Esophagus. Heartburn and Barrett s Esophagus. GERD is common in the U.S. None
 Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Vital staining and Barrett s esophagus
 Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
When to Refer for OGD and the Work Up of Upper GI Malignancies
 When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading?
 Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Endoscopic management of Barrett s esophagus:european Society of Gastrointestinal Endoscopy (ESGE) Position Statement
 Position Statement") Endoscopic management of Barrett s esophagus:european Society of Gastrointestinal Endoscopy (ESGE) Position Statement Authors Bas Weusten 1, 2,RafBisschops 3,EmanuelCoron 4,MárioDinis- Ribeiro 5,Jean-MarcDumonceau
Endoscopic management of Barrett s esophagus:european Society of Gastrointestinal Endoscopy (ESGE) Position Statement Authors Bas Weusten 1, 2,RafBisschops 3,EmanuelCoron 4,MárioDinis- Ribeiro 5,Jean-MarcDumonceau
Barrett s Esophagus: State of the Art. Food Getting Stuck
 Barrett s Esophagus: State of the Art Nicholas J. Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Food Getting Stuck 73-year-old retired Wilmington police
Barrett s Esophagus: State of the Art Nicholas J. Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Food Getting Stuck 73-year-old retired Wilmington police
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Health technology Endoscopic surveillance of Barrett's oesophagus to detect malignancy in an early and curable stage.
 Endoscopic surveillance of Barretts esophagus: a cost-effectiveness comparison with mammographic surveillance for breast cancer Streitz J M, Ellis F H, Tilden R L, Erickson R V Record Status This is a
Endoscopic surveillance of Barretts esophagus: a cost-effectiveness comparison with mammographic surveillance for breast cancer Streitz J M, Ellis F H, Tilden R L, Erickson R V Record Status This is a
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
CLINICAL EFFECTIVENESS
 Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Barrett s esophagus: lessons from recent clinical trials
 INVITED REVIEW Annals of Gastroenterology (2016) 29, 1-7 Barrett s esophagus: lessons from recent clinical trials Daniela Golger, Andreas Probst, Helmut Messmann Klinikum Augsburg, Germany Abstract Data
INVITED REVIEW Annals of Gastroenterology (2016) 29, 1-7 Barrett s esophagus: lessons from recent clinical trials Daniela Golger, Andreas Probst, Helmut Messmann Klinikum Augsburg, Germany Abstract Data
Barrett s Esophagus. lining of the lower esophagus that bears his name (i.e., Barrett's esophagus). We now
. We now") Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
ORIGINAL ARTICLE. Adenocarcinoma of the Esophagus With and Without Barrett Mucosa
 ORIGINAL ARTICLE Adenocarcinoma of the Esophagus With and Without Barrett Mucosa Michael S. Sabel, MD; Kate Pastore, MD; Hannah Toon, MD; Judy L. Smith, MD Hypothesis: Previous studies have demonstrated
ORIGINAL ARTICLE Adenocarcinoma of the Esophagus With and Without Barrett Mucosa Michael S. Sabel, MD; Kate Pastore, MD; Hannah Toon, MD; Judy L. Smith, MD Hypothesis: Previous studies have demonstrated