Relationship between Selected Physical Characteristics and Functional Capacity in the Anterior Cruciate Ligament-Insufficient Athlete
|
|
|
- Stanley Sanders
- 5 years ago
- Views:
Transcription
1 Relationship between Selected Physical Characteristics and Functional Capacity in the Anterior Cruciate Ligament-Insufficient Athlete By: Scott M. Lephart, PhD, ATC *, David H. Perrin, PhD, ATC, Freddie H. Fu, MD, Joe H. Gieck, EdD, ATC, PT, Frank C. McCue III, MD **, and James J. Ingang, ATC, PT Lephart, S.M., Perrin, D.H., Fu, F., Gieck, J.H., McCue, F.C., & Irrgang, J.J. (1992). Relationship between selected physical characteristics and functional capacity in the anterior cruciate insufficient athlete. Journal of Orthopaedic and Sports Physical Therapy, 16, ***Note: Figures may be missing for this format of the document ***Note: Footnotes and endnotes indicated with parentheses Abstract: Traditionally, clinicians have utilized various physical characteristics as criteria to assess the functional status of anterior cruciate ligament (ACL)-insufficient athletes without validating the efficacy of such assessments. The primary purposes of this study were to determine the relationship between traditionally used physical characteristics and functional capacity of individuals with an ACL insufficiency and to compare functional results of two groups of ACLinsufficient athletes. Forty-one subjects were tested for strength and power on an isokinetic device, anthropometric characteristics, and function using three functional performance tests (FPT). Results revealed that conventional physical characteristics correlated poorly (r =.01 to r =.42) with the functional tests. Additionally, athletes who were able to return to preinjury levels of activity performed significantly (p < 0.05) better on the FPT than those who were unable to return to preinjury activities. Based on the results of this study, use of such traditional physical characteristics for predicting function in the ACL-insufficient athlete may be inappropriate, and the functional performance tests designed for this study appear to be the most valuable assessment of the athlete's functional capacity. Little research has examined the relationship between physical characteristics such as strength, joint laxity, range of motion, muscular girth, and functional capacity of the anterior cruciate ligament (ACL)-insufficient knee (4, 5, 10, 12). This dearth of literature has contributed to inconsistencies in both evaluation and rehabilitation, while adversely affecting the determination of the functional capacity of the athlete with an ACL insufficiency. Because incomplete data exist regarding the relationship between these physical characteristics and functional capacity, the efficacy of the various protocols currently employed for the management of the condition is * Director, Sports Medicine/Athletic Training; assistant professor of education; assistant professor of orthopaedic surgery; School of Medicine; University of Pittsburgh, Pittsburgh, PA Associate professor, Curry School of Education; director, Sports Medicine Research Lab and Graduate Athletic Training Education; University of Virginia, Charlottesville, VA Blue Cross and Blue Shield of Western Pennsylvania professor of orthopaedics team physician; University of Pittsburgh, Pittsburgh, PA Head athletic trainer; associate professor, Curry School of Education; University of Virginia, Charlottesville, VA ** Professor of orthopaedics; team physician; University of Virginia, Charlottesville, VA Director, Sports Medicine Institute, Presbyterian-University Hospital, University of Pittsburgh Medical Center, Pittsburgh, PA
2 uncertain. Moreover, without guidance from the literature, controversy regarding the variables that influence functional disability most has resulted in inconsistencies in management for the ACL-deficient athlete (1, 6. 7, 17, 18, 20-22, 24). Several factors confound a clear understanding of the relationship between function and strength, laxity, range of motion, and thigh girth. First, assessment of joint laxity has heretofore been limited to manual examinations having varying levels of accuracy and reliability. Second, documentation of muscular performance characteristics of the ACL-insufficient knee is limited. Finally, definitions of adequate "function" of the ACL-insufficient knee have been limited to patient self-assessment, using criteria that are subjective and often inappropriate due to their lack of sensitivity to the functional demands of an athlete (12, 16, 17, 22). Relative to subjects with ACL-deficient knees, the purposes of this study were to: 1) compare the involved and uninvolved knees using selected physical impairment variables; 2) determine the relationship between involved/uninvolved physical impairment deficit measures and five different functional tests; and 3) compare the functional test results between one group of athletes who were able to return to competition and another group of athletes who were not. METHODS Subjects Forty-one subjects (32 male, 9 female) participated in the study. Subjects were selected to participate in the study from the University of Pittsburgh Sports Medicine Program and the Sports Medicine Institute of Presbyterian University Hospital, Pittsburgh, PA. Criteria for subject selection included the following: 1) the injury had occurred within the previous months, 2) an orthopaedic surgeon had made assessment of a positive Lachman and pivot shift tests as described by Katz et al (10), and 3) the involved knee had to possess >5 mm of anterior knee joint laxity compared to the uninvolved knee as determined with a KT Additional criteria for participation in the study included absence of medial or lateral laxity, absence of surgery, completion of a consistent rehabilitation program, and attempt by the subject to return to preinjury levels of athletic activity. All subjects were in a subacute injury stage when tested. All subject testing occurred during a 1-week period, and only subjects meeting the aforementioned inclusion criteria were included in the study. The subjects' ages ranged from 16 to 32 years (mean = 22.7 yrs), and the mean postinjury time was 26.5 months. Twenty-one of the subjects reported that they had experienced a recurrent injury to the knee, while 29 subjects reported that they had returned to a preinjury level of activity. Subjects were subgrouped into a Return (N = 29) group if they indicated they had returned to preinjury levels of activity and an Unable to return (N = 12) group if they were unable to return to preinjury levels of activity Procedure Data collection for each subject occurred over a successive 2-day period; 1 day involved the measurement of the selected physical characteristics, and the next day an evaluation was made of functional performance. The variables measured included anterior knee joint laxity, quadriceps and hamstring muscle- group peak torque, torque acceleration energy, peak torque ratios of the quadriceps/hamstrings at 60 and 270 /sec, knee joint range of motion, and circumferential thigh
3 girth measurements. Function was assessed via the Iowa Athletic Knee Rating Scale (IAKS) (22) and three functional performance tests designed exclusively for this study. Measurement of Laxity Anterior knee laxity was measured using the instrumented knee joint arthrometer M EDmetric Arthrometer Model KT-1000 (MEDmetric Corporation, San Diego, CA). The purpose of this measurement was to quantitatively measure the anterior knee joint laxity of the ACLinsufficient knee. The test protocol described by Daniel et al was used for measurement of joint laxity (2). Laxity was measured under 20 lbs of anterior force. The KT-1000 has been reported to be 90% accurate for ACL diagnosis, with sufficiently high test-retest reliability (2, 23). Measurement of Muscular Strength and Power Quadriceps and hamstring muscle-group peak torque, torque acceleration energy (TAE), and reciprocal muscle group ratios were obtained with a Cybex II isokinetic dynamometer (Lumex, Inc., Ronkonkoma, NY) at speeds of 60 and 270 "/sec, respectively. The TAE is defined as the work performed in the first 1/8 second of muscle contraction (8) and has been shown to be highly related to traditional power measurements (11). The isokinetic device was calibrated prior to testing. Subjects were seated in the standard and upright positions and stabilized by securing straps at the mid-thigh, waist, and chest (3, 8). A dual-pad Cybex anti-shear device was employed to decrease the shearing or anterior translation of the tibia, which is associated with isokinetic knee extension in the ACL-insufficient knee (9). Each subject performed six trial repetitions (three submaximal and three maximal) at 60 and 270 /sec, followed by six maximal test repetitions. The order of testing was randomized with respect to involved and uninvolved limbs. Peak torque. TAE, and reciprocal muscle-group ratios were determined with a Cybex Data Reduction Computer (CDRC) (Lumex, Inc., Ronkonkoma, NY). Measurement of Thigh Circumference Thigh girth measurements of both extremities were obtained using a standard circumferential measurement tape while the subjects were nonweight bearing (14). Measurements of circumference were taken 4 and 9 in proximal to the medial joint line. The purpose of these thigh circumference measurements was to determine if any thigh muscular atrophy existed in the subject's involved extremity. Measurement of Knee Joint Range of Motion Active knee joint flexion and extension were assessed through standard goniometry (14). Both flexion and extension were measured with the subject in the prone position. Rating of Activity Status The IAKS was used to assess each subject's activity status (Table 1). The test consisted of two separate assessments totaling 100 points. A 60-point questionnaire was employed that explored subjective symptoms of pain, swelling, instability, giving way, and activity status. An objective orthopaedic examination was performed, and points were assigned (40 total) based on laxity, pain, swelling, and joint ROM (22).

4 The IAKS was devised to provide a stringent measurement of function (22). Therefore, the scale was sensitive to a wide variation of total scores determined by the degree of functional incapacity experienced by each subject. Even the slightest functional incapacity was detected because a perfect score of 100 could only be obtained if the athlete was functioning without any disability at a professional level (22). Measurement of Functional Performance The functional performance tests (FPT) were used to obtain an objective measurement of function by reproducing the activities required to perform common sports skills (12). The tests included a co- contraction semicircular maneuver, a carioca maneuver, and a shuttle run. The tests were designed to produce rotational forces at the knee, tibial subluxation, and acceleration and deceleration, respectively (12). Test- retest reliability values for these tests range from r =.92 to r =.96 (12). The cocontraction test (Figure 1) was performed by securing a Velcro belt around the athlete's waist. The belt was attached to a heavy 122 cm length of rubber tubing with an outer diameter of 2.54 cm (Rehab Tubing, Pro Orthopedic Devices, Inc., Tucson, AZ). The tubing was anchored to a metal loop that was secured on a wall 154 cm above the floor. A semicircle was painted on the floor, which had a radius of 244 cm from the metal loop. The subject stood facing the wall with the toes of his/her feet on the line. This stretched the tubing 122 cm beyond its recoil length. The cocontraction test required each subject to complete five wall-to-wall lengths of the 180 semicircle, with the tension applied to the overstretched rubber tubing. The subjects began the test on the right side of the semicircle and moved in a side-step or shuffle fashion to complete the five lengths (three lengths right-to-left, two lengths left-to-right) in the minimum amount of time possible.

5 The carioca test (Figure 2) required the subjects to move laterally with a cross-over step. The test was performed over two lengths of a 12m distance. The subject began moving from left to right and reversed direction following the first 12-m length, thus performing the test moving a total of 24.5 m in the minimum amount of time possible. The shuttle run test was performed by the athlete running four lengths of 6.1 m. Subjects ran 6.1m, touched a line on the floor with their foot, reversed direction, returned to the starting point, touched the line, and repeated the process. The complete test covered 24.4 m with three changes in direction. The criterion measurement for all three tests was elapsed time, which was measured using a handheld stop watch. Each subject performed three trials on all tests, and the fastest time was recorded as the score for each of the three tests. The sum of the best time on each test was the total FPT score. Analysis Analysis of the data included computation of mean values for laxity, strength, girth, and range of motion. To examine for statistically significant differences between involved and uninvolved measurements, the data were then analyzed using analysis of variance (ANOVA). To establish the relationship among physical characteristics and functional capacity, the data were next analyzed using a Pearson product moment correlation coefficient. The final purpose of the statistical analysis included determining if differences existed in the functional performance tests and IAKS between subjects who had returned to a preinjury level of competition and those who had been unable to return. Subjects were assigned to either a "Return" group or to an "Unable to return" group. A one- way ANOVA was then computed to determine significant differences on both the functional performance tests and the IAKS for the two groups.


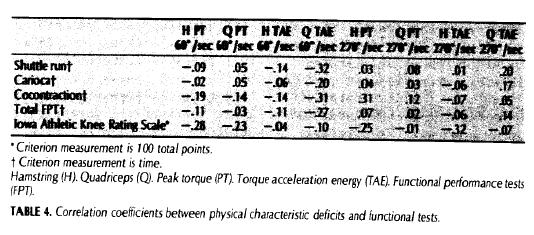
6 FIGURE 2. Carioca test. The athlete moves lateraly using an alternating cross-over step. RESULTS Bilateral comparisons for all isokinetic strength, joint laxity, circumferential, and range of motion measurements are presented in Table 2. The analyses revealed significant involved extremity deficits for several comparisons, including quadriceps extension and hamstring flexion peak torque (60 and 270 /sec). Involved extremity reciprocal muscle group peak torque ratios were significantly higher than uninvolved ratios at 60 /sec. Statistically significant differences were not found for TAE between involved and uninvolved sides during knee extension and flexion at either speed. Differences in anterior knee joint laxity were significant, with the involved extremity displaying greater laxity than the uninvolved extremity on passive anterior tibial displacement of 20 lbs. There was a lack of any strong correlation between the involved extremity physical characteristics and the functional tests (Table 3). The highest correlations were observed between the shuttle run test and several involved extremity measurements, including knee extension (quadriceps) peak torque at 60 (r = -.42, p <.05) and 270 "/sec (r = -.41, p <.05), knee extension TAE at 270 /sec (r = -.38, p <.05), and knee flexion (hamstrings) TAE at 270 /sec (r = -.34, p <.05). Other significant correlations were observed between involved extremity knee (hamstring) flexion TAE at 270 /sec and the shuttle run (r = -.42, p <.05), the cocontractions test (r = -.33, p <.05), and the total FPT (r = -.32, p <.05). Finally the IAKS correlated significantly with the total FPT (r = -.49). No significant correlations were observed between any of the functional tests and any of the bilateral deficits (Table 4).
. Table 5 reveals the differences between the Return and Unable to return groups for each functional measure.")

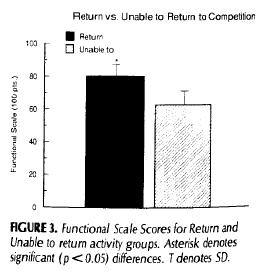
7 To examine for differences in function between those who were able to return to preinjury levels of activity and those who were not, subjects were assigned to one of two groups (Return, N = 29; Unable to return, N - = 12). Table 5 reveals the differences between the Return and Unable to return groups for each functional measure. The Return group scored significantly better on the IAKS and on all the functional performance tests. Figures 3 and 4 illustrate the group mean differences for the IAKS and the FPT between the Return and Unable to return groups. There were no significant differences observed between male and female subjects for the variables assessed. Of the nine females in the study, six were in the Return group while three were in the Unable to return group.

8
 and McDaniel and Dameron (13) both stated that deficits in strength must be overcome for successful return to preinjury levels of function.")
9 DISCUSSION The isokinetic peak torque deficits in the ACL-insufficient extremity during both knee extension and flexion at both testing speeds were consistent with the findings of Ti- bone et al (21). Furthermore, Giove et al (7) and McDaniel and Dameron (13) both stated that deficits in strength must be overcome for successful return to preinjury levels of function. As a result, many currently employed rehabilitation protocols focus on the attainment of bilateral strength equivalency as criteria for return to competition. Based on the peak torque deficits identified in this study, such rehabilitation objectives are reasonable. However, clinicians should realize that peak torque deficits are not necessarily related to an athlete's functional capacity. The data presented suggest that neither hamstring nor quadriceps peak torque deficits were highly related to functional performance. Therefore, bilateral peak torque measurements used exclusively as criteria for return to activity in the ACL-insufficient athlete are inadequate. More appropriately, the strength deficits should be addressed during rehabilitation but should not be used solely for the assessment of the athlete's functional level. Rather, the assessment of the athlete's functional level should also include functional tests specific to the athlete's sport. Although the anterior knee joint laxity was significantly higher on the involved knee in the subjects in this study, these deficits were not found to be related to the functional capacity of the athlete. This finding suggests that the capacity to dynamically compensate for the ACL insufficiency is not necessarily related to the amount of static laxity present in the knee. The subjects did not present significant differences between involved and uninvolved extremity range of motion measurements. Furthermore, there were no differences in thigh circumference measurements. Thus, thigh circumference deficits were not related to deficits in peak torque in these subjects, and the use of bilateral circumferential measurements as a criterion for assessing bilateral strength equivalence would be inappropriate in these subjects. Consistent with Walla et al, relatively poor relationships were observed between the selected physical characteristics and the functional measurements that were assessed (22). The poor relationship between the selected physical characteristics and function suggests that these variables
10 did not influence the functional capacity of subjects participating in this study. The role of the thigh musculature in dynamic stabilization of the knee has been suggested previously by Giove et al (7) and McDaniel and Dameron (13). However, the results of this investigation may suggest otherwise. On the other hand, the poor relationships observed in this study may be attributed to the manner in which the assessments of muscular characteristics have been obtained. Isokinetic testing occurs in an open kinetic chain system with muscular assessment from a nonweight-bearing state (15). It is suggested that the use of such instrumentation is inappropriate to assess the compensatory role of this musculature due to the inability to reproduce tibial-femoral translation when the athlete is not in a closed kinetic chain system or weight-bearing state. Furthermore. the assessment of muscular characteristics using an open kinetic chain isokinetic device in this study was limited to isokinetic concentric assessments only. The dynamic compensation of the ACLinsufficient knee occurs, presumably, with the musculature functioning isometrically and eccentrically, as well as concentrically. Therefore, in order to accurately assess the compensatory effects of the thigh musculature, development of an instrument that more closely simulates the activities in which the compensation occurs would seem indicated. Consistent with previous statements regarding the open kinetic chain isokinetic assessments, the Medmetric K-T 1000 instrumented arthrometry values were similarly obtained. Additionally, these assessments of static laxity were made with near complete muscular relaxation. The static laxity assessments provide a quantitative measure of the amount of anterior tibial-femoral translation but fail to assess the role of the secondary restraints. Furthermore, the role of the musculature in dynamically controlling tibial-femoral subluxation in the ACL-insufficient athlete remains in question. The mean quadriceps and hamstring reciprocal muscle group peak ratios for both the involved and uninvolved extremities were found to be consistent with previous studies that reported the ratios to range from 43 to 90% in normal nonathletic populations (16). Furthermore, the quadriceps and hamstring reciprocal muscle group peak torque ratios for both the involved and uninvolved sides were consistent with reports on normal football players averaging 54% at the test speed of 60 /sec and 66% at the test speed of 240 /sec (19). While little research exists regarding the reciprocal muscle-group peak torque ratios in the ACL-insufficient athlete, Giove et al stated that hamstring muscular strength equal to quadriceps strength of the involved extremity allowed athletes to return to higher levels of sport participation (7). The data presented here suggest that the quadriceps/hamstring reciprocal muscle group peak torque ratios were not highly related to the functional capacity of the subjects and, therefore, may have little influence on ability to return to activity. As stated previously, the true compensatory effects of the hamstring musculature are not assessed while the athlete is in a nonweight-bearing state. Therefore, the recommendations suggesting the development of a substantially high quadriceps/hamstring strength ratio cannot be discarded when the objective is dynamic control of anterior translation of the tibia in the ACL-insufficient athlete. The three FPT were intended to provide an objective instrument for the clinician to assess functional capacity in the ACL-insufficient athlete. The FPT attempted to simulate stresses about the knee commonly encountered during athletic participation. Thus, high levels of performance in these tests should be related to a return to preinjury levels of activity. The
11 results of this investigation substantiate this expectation. Subjects who returned successfully to athletic competition scored significantly higher on the FPT than those who were unable to return to preinjury levels of competition. Thus, it is suggested that the clinician implement these FPT in establishing criteria for return to competition. The FPT allow the clinician to objectively quantify performance while also visually assessing factors such as running gait, compensation. and apprehension. Questionnaires such as the IAKS have been designed to assess function of an athlete in a subjective manner. While the IAKS relies predominantly on a subjective assessment of function, it was nonetheless found to relate closely to actual functional capacity. Subjects who returned to preinjury levels of competition scored significantly higher on the IAKS than subjects who were unable to return. The IAKS was also highly related to the FPT. These findings suggest that an athlete's perception of functional capacity is an important component of the overall criteria for return to activity. There continues to be inconsistency in the prescription of therapeutic exercise for the athlete suffering from an ACL insufficiency. In addition to these discrepancies, inconsistency exists with regard to criteria for return to activity. McDaniel and Dameron suggest that dynamic muscular control is necessary for return to functional levels (13). Howerer, little research has established the efficacy of functional performance testing in the assessment of adequate dynamic muscular stability. Giove et al suggested that one criterion for return to activity is that the injured extremity hamstring strength he at least equal to the quadriceps muscle group strength (7). Somewhat similarly, Walla et al suggested that a "hamstring reflex" is necessary in order to function at high levels of activity (22). The recommendation of Walla et al seems reasonable, but this assessment is subjective in nature and occurs in an open kinetic chain, which does not assimilate the stresses placed on the knee while competing. This study suggests that the strengthening objectives of rehabilitation and the existing criteria used to return the athlete to competition are not necessarily synonymous. The objective of regaining normal thigh muscular strength, particularly of the hamstring muscle group, is a reasonable goal. Previous research has found these strength deficiencies in ACL-insufficient athletes. Furthermore, a fundamental understanding of the role of the hamstring musculature in controlling anterior tibial translation is clear. However, this study failed to establish a relationship between involved extremity peak torque deficits and functional capacity. CONCLUSION Based on the findings of this investigation it has been proposed that a combination of functional performance tests and an athlete sell assessment of readiness to return to competition be used as the criteria for return to activity. The 1AKS was found to be highly related to ability to return to preinjury levels of activity. The test included a number of assessments. such as subject signs and symptoms due to the insufficiency, perception of functional capacity, and an orthopaedic assessment of physical status. The combination of the IA KS and the FPT designed for this study seemed to hest represent an athlete's capacity to return to competition. As a result of the findings in this study. the use of peak torque. laxity, thigh circumference. and various other nonfunctional criteria are not recommended as the primary criteria in
12 determining an ACI-insufficient athlete's readiness to return to competition. Once normative values have been established for the functional performance tests and the IAKS specific to the various sports, the clinician will have resources available to objectively assess the functional capacity of the athlete utilizing tests that reproduce the stresses placed upon the knee which the ACL-insufficient athlete must compensate for during competition. REFERENCES 1. Andrews J: Diagnosis and treatment of the ACL deficient knee. Presented at Mid- Atlantic National Athletic Trainer's Annual Meeting, Greensboro, NC, Daniel D, Stone M, Sachs R, Lawrence M: Instrumented measurement of anterior knee laxity. Am J Sports Med 13: , Davies JD: A Compendium of Isokinetics in Clinical Usage, p 43. LaCrosse, WI: S & 5 Publishers, deandrade JR, Grant C, Dixon A: Joint distension and reilex muscle inhibition in the knee. I Bone J oint Surg 47A: Feagin JA. Curl W: Isolated tear of the anterior cruciate ligament: 5-year followup study: Am J Sports Med 4:95100, Fetto JA Marshall D: The natural history and diagnosis of anterior cruciate ligament insufficience. Clin Orthop 147:29-37, Giove MA, Miller SJ, Kent MA, Sanford TL, Garrick JG: Nonoperative treatment of the torn anterior cruciate ligament. I Bone loins Surg 65A: , Isolated Joint Testing & Exercise.Handbook for Using Cybex II, pp Ronkonkoma. NY: Lumex, Inc., Johnson D. Controlling antenor shear during isoktnetic knee extension exercise. I Orthop sports Phys Ther 4: Katz AA, Fingeroth R: The diagnostic accuracy of ruptures of the anterior cruciate ligament comparing the Lachman test, the anterior drawer sign, and the pivot shift test in acute and chronic knee injures. Am J Sports Med 14:8891, Lephart SM, Perrin DH, Manning IM, Gieck JH, McCue FC, Saliba EN: Torque acceleration energy as an alternative predictor of anaerobic power. Med Sci Sports Exerc 19 (Suppl): 559, Lephart SM, Perrin DH, Minger K, Fu FH: Functional performance tests for the anterior cruciate ligament insufficient athlete. J Athl Train 26:44-50, McDaniel W, Dameron T: Untreated ruptures of the anterior cruciate ligament. J Bone Joint Surg 62A: , Minor MA, Minor SD: Patient Evaluation Methods for the Health Profession, pp Reston: Reston Publishing Co., Inc., Norkin C, Levangie P: Joint Structure and Function: A Comprehensive Analysis, pp Philadelphia: F. A. Davis Co., Noyes LJ: Assessment of selected reports on the strength relationship of the knee musculature. J Orthop Sports Phys Ther 4:78-85, Noyes FR, Butler D, Grood ES: Clinical paradoxes of anterior cruciate instability and a new test to detect its instability. Orthop Trans 2:78, 1978
13 18. Noyes FR, Matthews DS, Mooar PA, Grood EA: The symptomatic anterior cruciate-deficient knee. Part II. J Bone Joint Surg 65A: , Schlinkman B: Norms of high school football players derived from Cybex data reduction computer. I Orthop Sports Phys Ther 5: , Slocum DB, Larson RL: Rotary instability of the knee. / Bone Joint Surg 50A: , Tibone JM, Antich MS, Fanton CS, Moynes DR, Perry Functional analysis of anterior cruciate ligament instability. Am J Sports Med 14: , Walla D, Albright I, McAuley E, Martin R, Eldridge V, El-Khoury G: Hamstring control and the unstable anterior cruciate ligament-deficient knee. Am I Sports Med 13:34-39, Weesner CL, Albohm MI, Ritter MA: Clinical usage and application of instrumented cruciate ligament assessment. J Athl Train 22:29-31, Youmans W: The so-called "isolated" anterior cruciate ligament syndrome: A report of 32 cases with some observation on treatment and its effect on result. Am J Sports Med 6:26-30, 1978
Validity of Data Extraction Techniques on the Kinetic Communicator (KinCom) Isokinetic Device
 Isokinetic Device") Validity of Data Extraction Techniques on the Kinetic Communicator (KinCom) Isokinetic Device By: Laurie L. Tis, PhD, AT,C * and David H. Perrin, PhD, AT,C Tis, L.L., & Perrin, D.H. (1993). Validity of
Validity of Data Extraction Techniques on the Kinetic Communicator (KinCom) Isokinetic Device By: Laurie L. Tis, PhD, AT,C * and David H. Perrin, PhD, AT,C Tis, L.L., & Perrin, D.H. (1993). Validity of
OMICS - 3rd Int. Conference & 2
 KNEE OBJECTIVE STABILITY AND ISOKINETIC THIGH MUSCLE STRENGTH AFTER ANTERIOR CRUCIATE LIGAMENT (ACL) RECONSTRUCTION: A Randomized Six-Month Follow-Up Study M. Sajovic Department of Orthopedics and Sports
KNEE OBJECTIVE STABILITY AND ISOKINETIC THIGH MUSCLE STRENGTH AFTER ANTERIOR CRUCIATE LIGAMENT (ACL) RECONSTRUCTION: A Randomized Six-Month Follow-Up Study M. Sajovic Department of Orthopedics and Sports
Clinical Use of the Johnson Anti-Shear Device: How and Why to Use It
 0196-6011 /86/0706-0304$02.00/0 THE JOURNAL OF ORTHOPAEDIC AND SPORTS PHYSICAL THERAPY Copyr~ght 8 1986 by The Orthopaedic and Sports Physical Therapy Sections of the American Physical Therapy Association
0196-6011 /86/0706-0304$02.00/0 THE JOURNAL OF ORTHOPAEDIC AND SPORTS PHYSICAL THERAPY Copyr~ght 8 1986 by The Orthopaedic and Sports Physical Therapy Sections of the American Physical Therapy Association
Effect of Preload and Range of Motion on Isokinetic Torque in Women
 Effect of Preload and Range of Motion on Isokinetic Torque in Women By: Laurie L. Tis, David H. Perrin, Arthur Weltman, Donald W. Ball, and Joe H. Gieck * Tis, L.L., Perrin, D.H., Weltman, A., Ball, D.W.,
Effect of Preload and Range of Motion on Isokinetic Torque in Women By: Laurie L. Tis, David H. Perrin, Arthur Weltman, Donald W. Ball, and Joe H. Gieck * Tis, L.L., Perrin, D.H., Weltman, A., Ball, D.W.,
Knee Movement Coordination Deficits. ICD-9-CM: Sprain of cruciate ligament of knee
 1 Knee Movement Coordination Deficits Anterior Cruciate Ligament ACL Tear ICD-9-CM: 844.2 Sprain of cruciate ligament of knee ACL Insufficiency ICD-9-CM: 717.83 Old disruption of anterior cruciate ligament
1 Knee Movement Coordination Deficits Anterior Cruciate Ligament ACL Tear ICD-9-CM: 844.2 Sprain of cruciate ligament of knee ACL Insufficiency ICD-9-CM: 717.83 Old disruption of anterior cruciate ligament
Athletics rehabilitation
 19 th July, ISBS2016 Applied Sessions Athletics rehabilitation Integrative Approaches for Successful Rehabilitation This session will be led by an orthopedic surgeon and an athletic trainer who are very
19 th July, ISBS2016 Applied Sessions Athletics rehabilitation Integrative Approaches for Successful Rehabilitation This session will be led by an orthopedic surgeon and an athletic trainer who are very
The Reliability of Four Different Methods. of Calculating Quadriceps Peak Torque Angle- Specific Torques at 30, 60, and 75
 The Reliability of Four Different Methods. of Calculating Quadriceps Peak Torque Angle- Specific Torques at 30, 60, and 75 By: Brent L. Arnold and David H. Perrin * Arnold, B.A., & Perrin, D.H. (1993).
The Reliability of Four Different Methods. of Calculating Quadriceps Peak Torque Angle- Specific Torques at 30, 60, and 75 By: Brent L. Arnold and David H. Perrin * Arnold, B.A., & Perrin, D.H. (1993).
Comparison of Weight-Bearing and Non-Weight-Bearing Conditions on Knee Joint Reposition Sense
 Comparison of Weight-Bearing and Non-Weight-Bearing Conditions on Knee Joint Reposition Sense By: Michael J. Higgins and David H. Perrin Higgins, M.J., Perrin, D.H. (1997). Comparison of weight bearing
Comparison of Weight-Bearing and Non-Weight-Bearing Conditions on Knee Joint Reposition Sense By: Michael J. Higgins and David H. Perrin Higgins, M.J., Perrin, D.H. (1997). Comparison of weight bearing
Comparison of Clinical and Dynamic Knee Function in Patients with Anterior Cruciate Ligament Deficiency
 0363-5465/103/3131-0068$02.00/0 THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 31, No. 1 2003 American Orthopaedic Society for Sports Medicine Comparison of Clinical and Dynamic Knee Function in Patients
0363-5465/103/3131-0068$02.00/0 THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 31, No. 1 2003 American Orthopaedic Society for Sports Medicine Comparison of Clinical and Dynamic Knee Function in Patients
Can Muscle Power Be Estimated From Thigh Bulk Measurements? A Preliminary Study
 Journal of Sport Rehabilitation, 1999, 8.50-59 O 1999 Human Kinetics Publishers, Inc. Can Muscle Power Be Estimated From Thigh Bulk Measurements? A Preliminary Study Eric Maylia, John A. Fairclough, Leonard
Journal of Sport Rehabilitation, 1999, 8.50-59 O 1999 Human Kinetics Publishers, Inc. Can Muscle Power Be Estimated From Thigh Bulk Measurements? A Preliminary Study Eric Maylia, John A. Fairclough, Leonard
Effect of cold treatment on the concentric and eccentric torque-velocity relationship of the quadriceps femoris
 Effect of cold treatment on the concentric and eccentric torque-velocity relationship of the quadriceps femoris By: Kerriann Catlaw *, Brent L. Arnold, and David H. Perrin Catlaw, K., Arnold, B.L., & Perrin,
Effect of cold treatment on the concentric and eccentric torque-velocity relationship of the quadriceps femoris By: Kerriann Catlaw *, Brent L. Arnold, and David H. Perrin Catlaw, K., Arnold, B.L., & Perrin,
Effect of ACL Reconstruction and Tibial Rotation on Anterior Knee Laxity
 Effect of ACL Reconstruction and Tibial Rotation on Anterior Knee Laxity By: Kevin M. Guskiewicz, PhD, ATC; David H. Perrin, PhD, ATC; David E. Martin, PhD, ATC; David M. Kahler, MD; Bruce M. Gansneder,
Effect of ACL Reconstruction and Tibial Rotation on Anterior Knee Laxity By: Kevin M. Guskiewicz, PhD, ATC; David H. Perrin, PhD, ATC; David E. Martin, PhD, ATC; David M. Kahler, MD; Bruce M. Gansneder,
When are athletes ready for return to sports??? Functional Testing for Return to Sports. Important Factors Involved in Return to Sport
 Functional Testing for Return to Sports Meg Jacobs PT Momentum Physical Therapy and Sports Rehab Mjacobs@wegetyouhealthy.com When are athletes ready for return to sports??? Post ACL reconstruction, average
Functional Testing for Return to Sports Meg Jacobs PT Momentum Physical Therapy and Sports Rehab Mjacobs@wegetyouhealthy.com When are athletes ready for return to sports??? Post ACL reconstruction, average
Comparison of N-K Table Offset Angles with the Human Knee Flexor Torque Curve
 Comparison of N-K Table Offset Angles with the Human Knee Flexor Torque Curve By: Daniel J. LaPlaca *, Douglas R. Keskula, Kristinn I. Heinrichs, and David H. Perrin LaPlaca, D.J., Keskula, D., Heinrichs,
Comparison of N-K Table Offset Angles with the Human Knee Flexor Torque Curve By: Daniel J. LaPlaca *, Douglas R. Keskula, Kristinn I. Heinrichs, and David H. Perrin LaPlaca, D.J., Keskula, D., Heinrichs,
Anterior Cruciate Ligament Hamstring Rehabilitation Protocol
 Anterior Cruciate Ligament Hamstring Rehabilitation Protocol 1 / 6 2 / 6 3 / 6 Anterior Cruciate Ligament Hamstring Rehabilitation Level of Evidence: Successful anterior cruciate ligament (ACL) reconstruction
Anterior Cruciate Ligament Hamstring Rehabilitation Protocol 1 / 6 2 / 6 3 / 6 Anterior Cruciate Ligament Hamstring Rehabilitation Level of Evidence: Successful anterior cruciate ligament (ACL) reconstruction
Reliability of Lower Extremity Functional Performance Tests
 Reliability of Lower Extremity Functional Performance Tests Lori A. Bolgla, PT' Douglas R. Keskula, Ph D, PT, ATC2 ports medicine clinicians commonly see athletes who have sustained a lower extremity injury
Reliability of Lower Extremity Functional Performance Tests Lori A. Bolgla, PT' Douglas R. Keskula, Ph D, PT, ATC2 ports medicine clinicians commonly see athletes who have sustained a lower extremity injury
Grant H Garcia, MD Sports and Shoulder Surgeon
 What to Expect from your Anterior Cruciate Ligament Reconstruction Surgery A Guide for Patients Grant H Garcia, MD Sports and Shoulder Surgeon Important Contact Information Grant Garcia, MD Wallingford:
What to Expect from your Anterior Cruciate Ligament Reconstruction Surgery A Guide for Patients Grant H Garcia, MD Sports and Shoulder Surgeon Important Contact Information Grant Garcia, MD Wallingford:
Anterior Cruciate Ligament Hamstring Rehabilitation Protocol
 Anterior Cruciate Ligament Hamstring Rehabilitation Protocol Focus on exercise quality avoid overstressing the donor area while it heals. Typically, isolated hamstring strengthening begins after the 6
Anterior Cruciate Ligament Hamstring Rehabilitation Protocol Focus on exercise quality avoid overstressing the donor area while it heals. Typically, isolated hamstring strengthening begins after the 6
ACL Rehabilitation and Return To Play
 ACL Rehabilitation and Return To Play Seth Gasser, MD Director of Sports Medicine Florida Orthopaedic Institute Introduction Return to Play: the point in recovery from an injury when a person is safely
ACL Rehabilitation and Return To Play Seth Gasser, MD Director of Sports Medicine Florida Orthopaedic Institute Introduction Return to Play: the point in recovery from an injury when a person is safely
ACL Athletic Career. ACL Rupture - Warning Features Intensive pain Immediate swelling Locking Feel a Pop Dead leg Cannot continue to play
 FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
ISOKINETIC TESTING AND DATA INTERPRETATION
 ISOKINETIC TESTING AND DATA INTERPRETATION PRINCIPLES OF ISOKINETIC The principle behind Isokinetic exercise and testing is that the lever arm moves at a preset fixed speed allowing for accommodating resistance
ISOKINETIC TESTING AND DATA INTERPRETATION PRINCIPLES OF ISOKINETIC The principle behind Isokinetic exercise and testing is that the lever arm moves at a preset fixed speed allowing for accommodating resistance
5/13/2016. ACL I Risk Factors AAP Position Statement. Anterior Cruciate Ligament Injuries: Diagnosis, Treatment and Prevention.
 ACL I Risk Factors AAP Position Statement Timothy E. Hewett, PhD 2016 Chicago Sports Medicine Symposium Chicago, Illinois August 5-7, 2016 2015 MFMER slide-1 Anterior Cruciate Ligament Injuries: Diagnosis,
ACL I Risk Factors AAP Position Statement Timothy E. Hewett, PhD 2016 Chicago Sports Medicine Symposium Chicago, Illinois August 5-7, 2016 2015 MFMER slide-1 Anterior Cruciate Ligament Injuries: Diagnosis,
Knee Injuries. PSK 4U Mr. S. Kelly North Grenville DHS. Medial Collateral Ligament Sprain
 Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
Rehabilitation of an ACL injury in a 29 year old male with closed kinetic chain exercises: A case study
 Abstract Objective: This paper will examine a rehabilitation program for a healthy 29 year old male who sustained an incomplete tear of the left ACL. Results: Following a 9 week treatment plan focusing
Abstract Objective: This paper will examine a rehabilitation program for a healthy 29 year old male who sustained an incomplete tear of the left ACL. Results: Following a 9 week treatment plan focusing
***Note: Figures may be missing for this format of the document ***Note: Footnotes and endnotes indicated with brackets
 Isokinetic Strength of the Trunk and Hip in Female Runners By: Laurie L. Tis, MEd, ATC *, David H. Perrin, PhD, ATC, David B. Snead, PhD, Arthur Weltman University of Virginia and Washington University
Isokinetic Strength of the Trunk and Hip in Female Runners By: Laurie L. Tis, MEd, ATC *, David H. Perrin, PhD, ATC, David B. Snead, PhD, Arthur Weltman University of Virginia and Washington University
Anterior Cruciate Ligament (ACL) Rehabilitation
 Rehabilitation") Thomas D. Rosenberg, M.D. Vernon J. Cooley, M.D. Anterior Cruciate Ligament (ACL) Rehabilitation Dear Enclosed you will find a copy of our Anterior Cruciate Ligament (ACL) Rehabilitation program and the
Thomas D. Rosenberg, M.D. Vernon J. Cooley, M.D. Anterior Cruciate Ligament (ACL) Rehabilitation Dear Enclosed you will find a copy of our Anterior Cruciate Ligament (ACL) Rehabilitation program and the
ACL AND PCL INJURIES OF THE KNEE JOINT
 ACL AND PCL INJURIES OF THE KNEE JOINT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery,
ACL AND PCL INJURIES OF THE KNEE JOINT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery,
Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction
 Reconstruction") Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These
Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These
DATA INTERPRETATION AND ANALYSIS
 DATA INTERPRETATION AND ANALYSIS Numerical and Curve Analysis Ref: Compendium of Isokinetics George Davies Report Parameters Peak Torque Highest muscular force output at any moment during a repetition.
DATA INTERPRETATION AND ANALYSIS Numerical and Curve Analysis Ref: Compendium of Isokinetics George Davies Report Parameters Peak Torque Highest muscular force output at any moment during a repetition.
Anterior Cruciate Ligament (ACL) Injuries
 Injuries") Anterior Cruciate Ligament (ACL) Injuries Mark L. Wood, MD The anterior cruciate ligament (ACL) is one of the most commonly injured ligaments of the knee. The incidence of ACL injuries is currently estimated
Anterior Cruciate Ligament (ACL) Injuries Mark L. Wood, MD The anterior cruciate ligament (ACL) is one of the most commonly injured ligaments of the knee. The incidence of ACL injuries is currently estimated
Medical Practice for Sports Injuries and Disorders of the Knee
 Sports-Related Injuries and Disorders Medical Practice for Sports Injuries and Disorders of the Knee JMAJ 48(1): 20 24, 2005 Hirotsugu MURATSU*, Masahiro KUROSAKA**, Tetsuji YAMAMOTO***, and Shinichi YOSHIDA****
Sports-Related Injuries and Disorders Medical Practice for Sports Injuries and Disorders of the Knee JMAJ 48(1): 20 24, 2005 Hirotsugu MURATSU*, Masahiro KUROSAKA**, Tetsuji YAMAMOTO***, and Shinichi YOSHIDA****
Analyses of Isokinetic and Closed Chain Movements for Hamstring Reciprocal Coactivation
 Journal of Sport Rehabilitation, 2007, 16, 319-325 2007 Human Kinetics, Inc. Analyses of Isokinetic and Closed Chain Movements for Hamstring Reciprocal Coactivation John P. Miller and Ronald V. Croce Context:
Journal of Sport Rehabilitation, 2007, 16, 319-325 2007 Human Kinetics, Inc. Analyses of Isokinetic and Closed Chain Movements for Hamstring Reciprocal Coactivation John P. Miller and Ronald V. Croce Context:
By: Thomas G. Benoit, MEd, ATC, David E. Martin, PhD, ATC, David H.Perrin, PhD, ATC *
 Hot and Cold Whirlpool Treatments and Knee Joint Laxity By: Thomas G. Benoit, MEd, ATC, David E. Martin, PhD, ATC, David H.Perrin, PhD, ATC * Benoit, T.G., Martin, D.E., & Perrin, D.H. (1996). Hot and
Hot and Cold Whirlpool Treatments and Knee Joint Laxity By: Thomas G. Benoit, MEd, ATC, David E. Martin, PhD, ATC, David H.Perrin, PhD, ATC * Benoit, T.G., Martin, D.E., & Perrin, D.H. (1996). Hot and
ACL RECONSTRUCTION SPORTS REHABILITATION. Written by Bart Sas, Qatar
 ACL RECONSTRUCTION PREDICTORS AND PROGNOSIS OF OUTCOME POST RECONSTRUCTION Written by Bart Sas, Qatar Injury to the anterior cruciate ligament (ACL) is arguably the most devastating injury that an athlete
ACL RECONSTRUCTION PREDICTORS AND PROGNOSIS OF OUTCOME POST RECONSTRUCTION Written by Bart Sas, Qatar Injury to the anterior cruciate ligament (ACL) is arguably the most devastating injury that an athlete
W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco
 Knee Pain And Injuries In Adults W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco Pain Control Overview Narcotics rarely necessary after 1 st 1-2
Knee Pain And Injuries In Adults W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco Pain Control Overview Narcotics rarely necessary after 1 st 1-2
Rehabilitation Guidelines for Patellar Tendon and Quadriceps Tendon Repair
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Patellar Tendon and Quadriceps Tendon Repair The knee consists of four bones that form three joints. The femur is the large bone in the thigh
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Patellar Tendon and Quadriceps Tendon Repair The knee consists of four bones that form three joints. The femur is the large bone in the thigh
Followup of the acute nonoperated isolated
 Followup of the acute nonoperated isolated anterior cruciate ligament tear* RICHARD J. HAWKINS, MD, FRCS(C), FACS, GARY W. MISAMORE, MD, AND THOMAS R. MERRITT, MD, FRCS(C) From the Division of Orthopaedics,
Followup of the acute nonoperated isolated anterior cruciate ligament tear* RICHARD J. HAWKINS, MD, FRCS(C), FACS, GARY W. MISAMORE, MD, AND THOMAS R. MERRITT, MD, FRCS(C) From the Division of Orthopaedics,
By: TEDDY W. WORRELL, MEd, PT, ATC, CRAID R. DENEGAR, PhD, ATC, SUSAN L. ARMSTRONG, MEd, ATC, and DAVID H. PERRIN, PhD, ATC
 Effect of Body Position on Hamstring Muscle Group Average Torque By: TEDDY W. WORRELL, MEd, PT, ATC, CRAID R. DENEGAR, PhD, ATC, SUSAN L. ARMSTRONG, MEd, ATC, and DAVID H. PERRIN, PhD, ATC Worrell, T.W.,
Effect of Body Position on Hamstring Muscle Group Average Torque By: TEDDY W. WORRELL, MEd, PT, ATC, CRAID R. DENEGAR, PhD, ATC, SUSAN L. ARMSTRONG, MEd, ATC, and DAVID H. PERRIN, PhD, ATC Worrell, T.W.,
The Relationship Between Grading and Instrumented Measurements of Anterior Knee Joint Laxity
 Journal of Sport Rehabilitation, 2008, 17, 60-67 2008 Human Kinetics, Inc. The Relationship Between Grading and Instrumented Measurements of Anterior Knee Joint Laxity Wendy L. Hurley, Craig Denegar, and
Journal of Sport Rehabilitation, 2008, 17, 60-67 2008 Human Kinetics, Inc. The Relationship Between Grading and Instrumented Measurements of Anterior Knee Joint Laxity Wendy L. Hurley, Craig Denegar, and
Intramachine and intermachine reproducibility of concentric performance: A study of the Con-Trex MJ and the Cybex Norm dynamometers
 Isokinetics and Exercise Science 12 (4) 91 97 91 IOS Press Intramachine and intermachine reproducibility of concentric performance: A study of the Con-Trex MJ and the Cybex Norm dynamometers C. Bardis
Isokinetics and Exercise Science 12 (4) 91 97 91 IOS Press Intramachine and intermachine reproducibility of concentric performance: A study of the Con-Trex MJ and the Cybex Norm dynamometers C. Bardis
Isokinetic Evaluation of Internal/External Tibial Rotation Strength After the Use of Hamstring Tendons for Anterior Cruciate Ligament Reconstruction
 Isokinetic Evaluation of Internal/External Tibial Rotation Strength After the Use of Hamstring Tendons for Anterior Cruciate Ligament Reconstruction Tanya Armour,* PhD, Lorie Forwell, MSc, PT, Robert Litchfield,
Isokinetic Evaluation of Internal/External Tibial Rotation Strength After the Use of Hamstring Tendons for Anterior Cruciate Ligament Reconstruction Tanya Armour,* PhD, Lorie Forwell, MSc, PT, Robert Litchfield,
Functional Gait Adaptations in Patients With Anterior Cruciate Ligament Deficiency Over Time
 CLINICAL ORTHOPAEDICS AND RELATED RESEARCH Number 348, pp 166-175 0 1998 Lippincott-Raven Publishers Functional Gait Adaptations in Patients With Anterior Cruciate Ligament Deficiency Over Time Gary Wexler,
CLINICAL ORTHOPAEDICS AND RELATED RESEARCH Number 348, pp 166-175 0 1998 Lippincott-Raven Publishers Functional Gait Adaptations in Patients With Anterior Cruciate Ligament Deficiency Over Time Gary Wexler,
TREATMENT GUIDELINES FOR GRADE 3 PCL TEAR
 GENERAL CONSIDERATIONS Posterior cruciate ligament (PCL) injuries occur less frequently than anterior cruciate ligament (ACL) injuries, but are much more common than previously thought. The PCL is usually
GENERAL CONSIDERATIONS Posterior cruciate ligament (PCL) injuries occur less frequently than anterior cruciate ligament (ACL) injuries, but are much more common than previously thought. The PCL is usually
ACLR AND MCL REPAIR CLINICAL PRACTICE GUIDELINE
 ACLR AND MCL REPAIR CLINICAL PRACTICE GUIDELINE Progression is time and criterion-based, dependent on soft tissue healing, patient demographics, and clinician evaluation. Contact Ohio State Sports Medicine
ACLR AND MCL REPAIR CLINICAL PRACTICE GUIDELINE Progression is time and criterion-based, dependent on soft tissue healing, patient demographics, and clinician evaluation. Contact Ohio State Sports Medicine
Post Operative Knee Rehab: Return to Play after ACLR
 Post Operative Knee Rehab: Return to Play after ACLR Fall Session 2016 Mary Lloyd Ireland, M.D. Associate Professor University of Kentucky Dept. of Orthopaedic Surgery & Sports Medicine, Lexington, KY
Post Operative Knee Rehab: Return to Play after ACLR Fall Session 2016 Mary Lloyd Ireland, M.D. Associate Professor University of Kentucky Dept. of Orthopaedic Surgery & Sports Medicine, Lexington, KY
Anterior Tibial Translation During Progressive Loading of the ACL-Deficient Knee During Weight-Bearing and Nonweight-Bearing Isometric Exercise
 Anterior Tibial Translation During Progressive Loading of the ACL-Deficient Knee During Weight-Bearing and Nonweight-Bearing Isometric Exercise H. john Yack, PhD, PT, 01' lias M. Riley, BS, ATC, PAC2 Terry
Anterior Tibial Translation During Progressive Loading of the ACL-Deficient Knee During Weight-Bearing and Nonweight-Bearing Isometric Exercise H. john Yack, PhD, PT, 01' lias M. Riley, BS, ATC, PAC2 Terry
Commonality of ACL Injuries and Prevention Methods in Women. Anterior cruciate ligament or ACL injuries have become more common in
 4/6/12 Period 2 Commonality of ACL Injuries and Prevention Methods in Women Anterior cruciate ligament or ACL injuries have become more common in the past decade than at any other time in our history.
4/6/12 Period 2 Commonality of ACL Injuries and Prevention Methods in Women Anterior cruciate ligament or ACL injuries have become more common in the past decade than at any other time in our history.
Current trends in ACL Rehab. James Kelley, MDS, PT
 Current trends in ACL Rehab James Kelley, MDS, PT Objectives Provide etiological information Discuss the criteria for having an ACL reconstruction Review the basic rehabilitation principles behind ACL
Current trends in ACL Rehab James Kelley, MDS, PT Objectives Provide etiological information Discuss the criteria for having an ACL reconstruction Review the basic rehabilitation principles behind ACL
A Discussion of Job Content Validation and Isokinetic Technology. Gary Soderberg, Ph.D., PT, FAPTA i March 2006
 A Discussion of Job Content Validation and Isokinetic Technology Gary Soderberg, Ph.D., PT, FAPTA i March 2006 Testing of human function is difficult because of the great capability associated with our
A Discussion of Job Content Validation and Isokinetic Technology Gary Soderberg, Ph.D., PT, FAPTA i March 2006 Testing of human function is difficult because of the great capability associated with our
A descriptive profile of age-specific knee extension flexion strength in elite junior tennis players
 728 ORIGINAL ARTICLE A descriptive profile of age-specific knee extension flexion strength in elite junior tennis players Todd S Ellenbecker, E Paul Roetert, Tetsuro Sueyoshi, Scott Riewald... Br J Sports
728 ORIGINAL ARTICLE A descriptive profile of age-specific knee extension flexion strength in elite junior tennis players Todd S Ellenbecker, E Paul Roetert, Tetsuro Sueyoshi, Scott Riewald... Br J Sports
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas Phone: Fax:
 Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 MENISCAL REPAIR PROTOCOL Longitudinal Meniscal Repair This rehabilitation
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 MENISCAL REPAIR PROTOCOL Longitudinal Meniscal Repair This rehabilitation
Functional Outcome Measures for Knee Dysfunction Assessment
 Functional Outcome Measures for Knee Dysfunction Assessment Douglas R. Keskula, PhD, PT, ATC; Jewell B. Duncan, MD; Virginia L. Davis, MEd, PT, ATC; Paula W. Finley, PT ABSTRACT: Maximizing the functional
Functional Outcome Measures for Knee Dysfunction Assessment Douglas R. Keskula, PhD, PT, ATC; Jewell B. Duncan, MD; Virginia L. Davis, MEd, PT, ATC; Paula W. Finley, PT ABSTRACT: Maximizing the functional
KNEE AND LEG EXERCISE PROGRAM
 KNEE AND LEG EXERCISE PROGRAM These exercises are specifically designed to rehabilitate the muscles of the hip and knee by increasing the strength and flexibility of the involved leg. This exercise program
KNEE AND LEG EXERCISE PROGRAM These exercises are specifically designed to rehabilitate the muscles of the hip and knee by increasing the strength and flexibility of the involved leg. This exercise program
PROPRIOCEPTION AND FUNCTION AFTER ANTERIOR CRUCIATE RECONSTRUCTION
 PROPRIOCEPTION AND FUNCTION AFTER ANTERIOR CRUCIATE RENSTRUCTION D. S. BARRETF From the Royal National Orthopaedic Hospital, Stanmore We have assessed 45 patients who had undergone anterior cruciate reconstruction
PROPRIOCEPTION AND FUNCTION AFTER ANTERIOR CRUCIATE RENSTRUCTION D. S. BARRETF From the Royal National Orthopaedic Hospital, Stanmore We have assessed 45 patients who had undergone anterior cruciate reconstruction
FOOTBALL INJURY PREVENTION
 FOOTBALL INJURY PREVENTION Football is the sport traditionally associated with knee ligament injuries. We are all aware of the seriousness of the knee injury produced by the classic clip. The injury prevention
FOOTBALL INJURY PREVENTION Football is the sport traditionally associated with knee ligament injuries. We are all aware of the seriousness of the knee injury produced by the classic clip. The injury prevention
MENISCAL REPAIR WITH WEIGHT RESTRICTIONS CLINICAL PRACTICE GUIDELINES
 MENISCAL REPAIR WITH WEIGHT RESTRICTIONS CLINICAL PRACTICE GUIDELINES Progression is time and criterion-based, dependent on soft tissue healing, patient demographics and clinician evaluation. Contact Ohio
MENISCAL REPAIR WITH WEIGHT RESTRICTIONS CLINICAL PRACTICE GUIDELINES Progression is time and criterion-based, dependent on soft tissue healing, patient demographics and clinician evaluation. Contact Ohio
Research Theme. Cal PT Fund Research Symposium 2015 Christopher Powers. Patellofemoral Pain to Pathology Continuum. Applied Movement System Research
 Evaluation and Treatment of Movement Dysfunction: A Biomechanical Approach Research Theme Christopher M. Powers, PhD, PT, FAPTA Understanding injury mechanisms will lead to the development of more effective
Evaluation and Treatment of Movement Dysfunction: A Biomechanical Approach Research Theme Christopher M. Powers, PhD, PT, FAPTA Understanding injury mechanisms will lead to the development of more effective
Chronic Ankle Instability Does Not Affect Lower Extremity Functional Performance
 Chronic Ankle Instability Does Not Affect Lower Extremity Functional Performance By: Kerry M. Demeritt, Sandra J. Shultz, Carrie L. Docherty, Bruce M. Gansneder, and David H. Perrin. Demeritt, K. M., Shultz,
Chronic Ankle Instability Does Not Affect Lower Extremity Functional Performance By: Kerry M. Demeritt, Sandra J. Shultz, Carrie L. Docherty, Bruce M. Gansneder, and David H. Perrin. Demeritt, K. M., Shultz,
ACL REHABILITATION PROTOCOL
 Name: ID: Date Of Surgery :DD / MM / YYYY Procedure: ACL REHABILITATION PROTOCOL Note :If another procedure like meniscus repair or OATS (Osteochondralautograft transfer) has been done along with ACL reconstruction
Name: ID: Date Of Surgery :DD / MM / YYYY Procedure: ACL REHABILITATION PROTOCOL Note :If another procedure like meniscus repair or OATS (Osteochondralautograft transfer) has been done along with ACL reconstruction
3/21/2011 PCL INJURY WITH OPERATIVE TREATMENT A CASE STUDY PCL PCL MECHANISM OF INJURY PCL PREVALENCE
 PCL PCL INJURY WITH OPERATIVE TREATMENT A CASE STUDY K. Anderson, S. Hjortedal, Y. Jingi, E. Sutcliffe & S. Witschen Washington State University Origin Posterior aspect of tibia Insertion Medial femoral
PCL PCL INJURY WITH OPERATIVE TREATMENT A CASE STUDY K. Anderson, S. Hjortedal, Y. Jingi, E. Sutcliffe & S. Witschen Washington State University Origin Posterior aspect of tibia Insertion Medial femoral
Utility of Instrumented Knee Laxity Testing in Diagnosis of Partial Anterior Cruciate Ligament Tears
 Utility of Instrumented Knee Laxity Testing in Diagnosis of Partial Anterior Cruciate Ligament Tears Ata M. Kiapour, Ph.D. 1, Ali Kiapour, Ph.D. 2, Timothy E. Hewett, Ph.D. 3, Vijay K. Goel, Ph.D. 2. 1
Utility of Instrumented Knee Laxity Testing in Diagnosis of Partial Anterior Cruciate Ligament Tears Ata M. Kiapour, Ph.D. 1, Ali Kiapour, Ph.D. 2, Timothy E. Hewett, Ph.D. 3, Vijay K. Goel, Ph.D. 2. 1
Chapter 14 Training Muscles to Become Stronger
 Chapter 14 Training Muscles to Become Stronger Slide Show developed by: Richard C. Krejci, Ph.D. Professor of Public Health Columbia College 11.22.11 Objectives 1. Describe the following four methods to
Chapter 14 Training Muscles to Become Stronger Slide Show developed by: Richard C. Krejci, Ph.D. Professor of Public Health Columbia College 11.22.11 Objectives 1. Describe the following four methods to
Concurrent validity evidence of partial weight bearing lower extremity performance measure
 The University of Toledo The University of Toledo Digital Repository Master s and Doctoral Projects Concurrent validity evidence of partial weight bearing lower extremity performance measure Jamila Gilbert
The University of Toledo The University of Toledo Digital Repository Master s and Doctoral Projects Concurrent validity evidence of partial weight bearing lower extremity performance measure Jamila Gilbert
Posterior Cruciate Ligament Rehabilitation
 Posterior Cruciate Ligament Rehabilitation Phase 6: Running program for Return to Sports : 24 Weeks after surgery onward Goals: 1. Safely recondition the injured area for the demands of sports activity.
Posterior Cruciate Ligament Rehabilitation Phase 6: Running program for Return to Sports : 24 Weeks after surgery onward Goals: 1. Safely recondition the injured area for the demands of sports activity.
Effect of trunk position on anterior tibial displacement measured by the KT-1000 in uninjured subjects.
 Effect of trunk position on anterior tibial displacement measured by the KT-1000 in uninjured subjects. By: William G Webright, David H Perrin, Bruce M Gansneder. Webright, W.G., Perrin, D.H., and Gansneder,
Effect of trunk position on anterior tibial displacement measured by the KT-1000 in uninjured subjects. By: William G Webright, David H Perrin, Bruce M Gansneder. Webright, W.G., Perrin, D.H., and Gansneder,
Resistive Eccentric Exercise: Effects of Visual
 Resistive Eccentric Exercise: Effects of Visual Feed back on Maximum Moment of Knee Extensors and Flexors Eleftherios Kellis, BScl Vasilios Baltzopoulos, Ph D, M Phil, BSc2 Copyright 1996. All rights reserved.
Resistive Eccentric Exercise: Effects of Visual Feed back on Maximum Moment of Knee Extensors and Flexors Eleftherios Kellis, BScl Vasilios Baltzopoulos, Ph D, M Phil, BSc2 Copyright 1996. All rights reserved.
The Orthopaedic Journal of Sports Medicine, 1(1), DOI: / ª The Author(s) 2013
, DOI: / ª The Author(s) 2013") Differences in Knee Kinematics Between Awake and Anesthetized Patients During the Lachman and Pivot-Shift Tests for Anterior Cruciate Ligament Deficiency Takehiko Matsushita,* MD, PhD, Shinya Oka,* MD,
Differences in Knee Kinematics Between Awake and Anesthetized Patients During the Lachman and Pivot-Shift Tests for Anterior Cruciate Ligament Deficiency Takehiko Matsushita,* MD, PhD, Shinya Oka,* MD,
Re-establishing establishing Neuromuscular
 Re-establishing establishing Neuromuscular Control Why is NMC Critical? What is NMC? Physiology of Mechanoreceptors Elements of NMC Lower-Extremity Techniques Upper-Extremity Techniques Readings Chapter
Re-establishing establishing Neuromuscular Control Why is NMC Critical? What is NMC? Physiology of Mechanoreceptors Elements of NMC Lower-Extremity Techniques Upper-Extremity Techniques Readings Chapter
Jennifer L. Cook, MD
 Jennifer L. Cook, MD Florida Joint Replacement and Sports Medicine Center 5243 Hanff Lane New Port Richey, FL 34652 Phone: (727)848-4249 Fax: (727) 841-8934 ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION POST-OPERATIVE
Jennifer L. Cook, MD Florida Joint Replacement and Sports Medicine Center 5243 Hanff Lane New Port Richey, FL 34652 Phone: (727)848-4249 Fax: (727) 841-8934 ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION POST-OPERATIVE
chapter Exercise Technique for Alternative Modes and Nontraditional Implement Training
 chapter 16 Exercise Technique for Alternative Modes and Nontraditional Implement Training Chapter Objectives Understand the basic guidelines for performing resistance exercise with alternative modes and
chapter 16 Exercise Technique for Alternative Modes and Nontraditional Implement Training Chapter Objectives Understand the basic guidelines for performing resistance exercise with alternative modes and
ANATOMIC ACL RECONSTRUCTION RECOVERY & REHABILITATION PROTOCOL
 ANATOMIC ACL RECONSTRUCTION RECOVERY & REHABILITATION PROTOCOL PREOPERATIVE: If you have suffered an acute ACL injury and surgery is planned, the time between injury and surgery should be used to regain
ANATOMIC ACL RECONSTRUCTION RECOVERY & REHABILITATION PROTOCOL PREOPERATIVE: If you have suffered an acute ACL injury and surgery is planned, the time between injury and surgery should be used to regain
Week 1 Orthotics- 1. Knee brace locked in full extension at all times except for rehab exercises 2. Elastic bandage as needed to control swelling
 General Principles: This protocol was designed to provide the rehabilitation professional with a guideline of postoperative care. It should be stressed that this is only a protocol and should not be a
General Principles: This protocol was designed to provide the rehabilitation professional with a guideline of postoperative care. It should be stressed that this is only a protocol and should not be a
Associations between isolated bundle tear of anterior cruciate ligament, time from injury to surgery, and clinical tests
 Journal of Orthopaedic Surgery 2014;22(2):209-13 Associations between isolated bundle tear of anterior cruciate ligament, time from injury to surgery, and clinical tests August Wai-Ming Fok, WP Yau Division
Journal of Orthopaedic Surgery 2014;22(2):209-13 Associations between isolated bundle tear of anterior cruciate ligament, time from injury to surgery, and clinical tests August Wai-Ming Fok, WP Yau Division
Exercise Therapy for Patients with Knee OA Knee Exercise Protocol Knee Home Exercise Programme
 Chapter FOUR Exercise Therapy for Patients with Knee OA Knee Exercise Protocol Knee Home Exercise Programme Chris Higgs Cathy Chapple Daniel Pinto J. Haxby Abbott 99 n n 100 General Guidelines Knee Exercise
Chapter FOUR Exercise Therapy for Patients with Knee OA Knee Exercise Protocol Knee Home Exercise Programme Chris Higgs Cathy Chapple Daniel Pinto J. Haxby Abbott 99 n n 100 General Guidelines Knee Exercise
ROLAND RAMIREZ ATC, LAT, PT, SCS, CSCS Asst. Athletic Trainer Rehabilitation Coordinator Houston Texans
 ROLAND RAMIREZ ATC, LAT, PT, SCS, CSCS Asst. Athletic Trainer Rehabilitation Coordinator Houston Texans DS2 = Dynamic Stabilization and Strengthening Platform Low friction platform initially created for
ROLAND RAMIREZ ATC, LAT, PT, SCS, CSCS Asst. Athletic Trainer Rehabilitation Coordinator Houston Texans DS2 = Dynamic Stabilization and Strengthening Platform Low friction platform initially created for
The Knee. Two Joints: Tibiofemoral. Patellofemoral
 Evaluating the Knee The Knee Two Joints: Tibiofemoral Patellofemoral HISTORY Remember the questions from lecture #2? Girth OBSERVATION TibioFemoral Alignment What are the consequences of faulty alignment?
Evaluating the Knee The Knee Two Joints: Tibiofemoral Patellofemoral HISTORY Remember the questions from lecture #2? Girth OBSERVATION TibioFemoral Alignment What are the consequences of faulty alignment?
GOALS. Full knee extension ROM Good quadriceps control (> 20 no lag SLR) Minimize pain Minimize swelling Normal gait pattern
 Minimize pain Minimize swelling Normal gait pattern") Hamstring ACL Rehabilitation Guidelines David R. McAllister, MD UCLA Department of Orthoapeadic Surgery Sports Medicine Service (310)206-5250 FAX (310) 825-1311 General Information: The following ACL rehabilitation
Hamstring ACL Rehabilitation Guidelines David R. McAllister, MD UCLA Department of Orthoapeadic Surgery Sports Medicine Service (310)206-5250 FAX (310) 825-1311 General Information: The following ACL rehabilitation
MOON ACL Rehabilitation Guidelines
 MOON ACL Rehabilitation Guidelines M.o.o.n.Team Members General Information: The following ACL rehabilitation guidelines are based on a review of the randomized controlled trials related to ACL rehabilitation.
MOON ACL Rehabilitation Guidelines M.o.o.n.Team Members General Information: The following ACL rehabilitation guidelines are based on a review of the randomized controlled trials related to ACL rehabilitation.
Theodore Ganley, MD Lawrence Wells, MD J. Todd Lawrence, MD, PhD Anterior Cruciate Ligament Reconstruction Protocol (Revised March 2018)
") Theodore Ganley, MD Lawrence Wells, MD J. Todd Lawrence, MD, PhD Anterior Cruciate Ligament Reconstruction Protocol (Revised March 2018) ***Please refer to written prescription for any special instructions
Theodore Ganley, MD Lawrence Wells, MD J. Todd Lawrence, MD, PhD Anterior Cruciate Ligament Reconstruction Protocol (Revised March 2018) ***Please refer to written prescription for any special instructions
Post Operative ACL Reconstruction Protocol Brian J. White, MD
 Post Operative ACL Reconstruction Protocol Brian J. White, MD www.western-ortho.com The intent of this protocol is to provide guidelines for progression of rehabilitation. It is not intended to serve as
Post Operative ACL Reconstruction Protocol Brian J. White, MD www.western-ortho.com The intent of this protocol is to provide guidelines for progression of rehabilitation. It is not intended to serve as
Anterior Cruciate Ligament (ACL) Reconstruction Protocol. Hamstring Autograft, Allograft, or Revision
 Reconstruction Protocol. Hamstring Autograft, Allograft, or Revision") Anterior Cruciate Ligament (ACL) Reconstruction Protocol Hamstring Autograft, Allograft, or Revision As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp,
Anterior Cruciate Ligament (ACL) Reconstruction Protocol Hamstring Autograft, Allograft, or Revision As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp,
Sheena Black, MD. Orthopaedic Surgery, Sports Medicine PHYSICAL THERAPY PRESCRIPTION ACL RECONSTRUCTION HAMSTRING TENDON TECHNIQUE
 PHYSICAL THERAPY PRESCRIPTION ACL RECONSTRUCTION HAMSTRING TENDON TECHNIQUE Name: Date: Post-Operative Diagnosis: Right Left ACL Reconstruction Graft: BTB Hamstring Allograft Additional Procedures: Lateral
PHYSICAL THERAPY PRESCRIPTION ACL RECONSTRUCTION HAMSTRING TENDON TECHNIQUE Name: Date: Post-Operative Diagnosis: Right Left ACL Reconstruction Graft: BTB Hamstring Allograft Additional Procedures: Lateral
STATE OF THE ART OF ACL SURGERY (Advancements that have had an impact)
") STATE OF THE ART OF ACL SURGERY (Advancements that have had an impact) David Drez, Jr., M.D. Clinical Professor of Orthopaedics LSU School of Medicine Financial Disclosure Dr. David Drez has no relevant
STATE OF THE ART OF ACL SURGERY (Advancements that have had an impact) David Drez, Jr., M.D. Clinical Professor of Orthopaedics LSU School of Medicine Financial Disclosure Dr. David Drez has no relevant
ADOLESCENT SPORTS INJURIES. Orthopaedics in Motion April 5, 2017 John Lammli, MD
 ADOLESCENT SPORTS INJURIES Orthopaedics in Motion April 5, 2017 John Lammli, MD OVERVIEW: Shoulder Injuries Knee Injuries Leg/Ankle Injuries SHOULDER INJURIES Injuries to the shoulder girdle are vast and
ADOLESCENT SPORTS INJURIES Orthopaedics in Motion April 5, 2017 John Lammli, MD OVERVIEW: Shoulder Injuries Knee Injuries Leg/Ankle Injuries SHOULDER INJURIES Injuries to the shoulder girdle are vast and
Knee Injury Assessment
 Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
Dynamic stability after ACL injury: who can hop?
 Knee Surg, Sports Traumatol, Arthrosc (2000) 8 :262 269 KNEE DOI 10.1007/s001670000130 K. S. Rudolph M. J. Axe L. Snyder-Mackler Dynamic stability after ACL injury: who can hop? Received: 17 January 2000
Knee Surg, Sports Traumatol, Arthrosc (2000) 8 :262 269 KNEE DOI 10.1007/s001670000130 K. S. Rudolph M. J. Axe L. Snyder-Mackler Dynamic stability after ACL injury: who can hop? Received: 17 January 2000
ACL Rehabilitation Guidelines
 ACL Rehabilitation Guidelines General Information: These guidelines have been developed to service the spectrum of ACL injured people (non-athlete elite athlete). For this reason, example exercises are
ACL Rehabilitation Guidelines General Information: These guidelines have been developed to service the spectrum of ACL injured people (non-athlete elite athlete). For this reason, example exercises are
Test-Retest Reliability of the Lateral Step-up Test in Young Adult Healthy Subjects
 Test-Retest Reliability of the Lateral Step-up Test in Young Adult Healthy Subjects Capt Michael Ross, MSEd, PT' linicians often assess muscular performance in order to determine an individual's level
Test-Retest Reliability of the Lateral Step-up Test in Young Adult Healthy Subjects Capt Michael Ross, MSEd, PT' linicians often assess muscular performance in order to determine an individual's level
NONOPERATIVE REHABILITATION FOLLOWING ACL INJURY ( Program)
") Therapist: Phone: NONOPERATIVE REHABILITATION FOLLOWING ACL INJURY (3-3-4-4 Program) IMMEDIATE INJURY PHASE (Day 1 to Day 7) Restore full passive knee extension Diminish joint swelling and pain Restore
Therapist: Phone: NONOPERATIVE REHABILITATION FOLLOWING ACL INJURY (3-3-4-4 Program) IMMEDIATE INJURY PHASE (Day 1 to Day 7) Restore full passive knee extension Diminish joint swelling and pain Restore
Obesity is associated with reduced joint range of motion (Park, 2010), which has been partially
, which has been partially") INTRODUCTION Obesity is associated with reduced joint range of motion (Park, 2010), which has been partially attributed to adipose tissues around joints limiting inter-segmental rotations (Gilleard, 2007).
INTRODUCTION Obesity is associated with reduced joint range of motion (Park, 2010), which has been partially attributed to adipose tissues around joints limiting inter-segmental rotations (Gilleard, 2007).
Knee Sprains and Acute Knee Hemarthrosis
 Knee Sprains and Acute Knee Hemarthrosis Misdiagnosis of Anterior Cruciate Ligament Tears FRANK R. NOYES, MD, LONNIE PAULOS, MD, LISA A. MOOAR, BA, and BEN SIGNER, BA Key Words: Anterior cruciate ligament,
Knee Sprains and Acute Knee Hemarthrosis Misdiagnosis of Anterior Cruciate Ligament Tears FRANK R. NOYES, MD, LONNIE PAULOS, MD, LISA A. MOOAR, BA, and BEN SIGNER, BA Key Words: Anterior cruciate ligament,
Femoral Condyle Rehabilitation Guidelines
 Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Brace: Protect healing tissue from load and shear forces Decrease pain and effusion Restore full passive knee extension
Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Brace: Protect healing tissue from load and shear forces Decrease pain and effusion Restore full passive knee extension
Is Knee Laxity Change after Anterior Cruciate Ligament Injury and Surgery Related to Open Kinetic Chain Knee Extensor Training Load?
 Is Knee Laxity Change after Anterior Cruciate Ligament Injury and Surgery Related to Open Kinetic Chain Knee Extensor Training Load? Matthew C. Morrissey, Mark C. Perry, John B. King DIVISION OF APPLIED
Is Knee Laxity Change after Anterior Cruciate Ligament Injury and Surgery Related to Open Kinetic Chain Knee Extensor Training Load? Matthew C. Morrissey, Mark C. Perry, John B. King DIVISION OF APPLIED
KLT Knee Laxity Tester
 ART 56 2.1 11/2017-E KLT Knee Laxity Tester For Instrumented Stability Testing of the Knee Joint KLT Knee Laxity Tester for instrumented stability testing of the knee joint Injuries of the anterior cruciate
ART 56 2.1 11/2017-E KLT Knee Laxity Tester For Instrumented Stability Testing of the Knee Joint KLT Knee Laxity Tester for instrumented stability testing of the knee joint Injuries of the anterior cruciate
Anteroposterior tibiofemoral displacements during isometric extension efforts The roles of external load and knee flexion angle
 winner of the rehabilitation award Anteroposterior tibiofemoral displacements during isometric extension efforts The roles of external load and knee flexion angle KENNETH A. JURIST, MD, AND JAMES C. OTIS,*
winner of the rehabilitation award Anteroposterior tibiofemoral displacements during isometric extension efforts The roles of external load and knee flexion angle KENNETH A. JURIST, MD, AND JAMES C. OTIS,*
Accelerated Rehabilitation Following ACL-PTG Reconstruction & PCL Reconstruction with Medial Collateral Ligament Repair
 Page 1 of 7 Accelerated Rehabilitation Following ACL-PTG Reconstruction & PCL Reconstruction with Medial Collateral Ligament Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore
Page 1 of 7 Accelerated Rehabilitation Following ACL-PTG Reconstruction & PCL Reconstruction with Medial Collateral Ligament Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore
Nicholas Robert Heebner. B.S. Kinesiology, The Pennsylvania State University, M.S. Sports Medicine, University of Pittsburgh, 2012
 THE EFFECT OF JUMP DISTANCE ON BIOMECHANICAL RISK FACTORS FOR ACL INJURY DURING LANDING AND THEIR RELATIONSHIP WITH SENSORIMOTOR CHARACTERISTICS AT THE KNEE by Nicholas Robert Heebner B.S. Kinesiology,
THE EFFECT OF JUMP DISTANCE ON BIOMECHANICAL RISK FACTORS FOR ACL INJURY DURING LANDING AND THEIR RELATIONSHIP WITH SENSORIMOTOR CHARACTERISTICS AT THE KNEE by Nicholas Robert Heebner B.S. Kinesiology,
Baseline Time to Stabilization Identifies Anterior Cruciate Ligament Rupture Risk in Collegiate Athletes
 Sean Baseline Time to Stabilization Identifies Anterior Cruciate Ligament Rupture Risk in Collegiate Athletes Kevin M. DuPrey,* y DO, Kathy Liu,z PhD, Peter F. Cronholm, MD, Andrew S. Reisman,{ MD, Steven
Sean Baseline Time to Stabilization Identifies Anterior Cruciate Ligament Rupture Risk in Collegiate Athletes Kevin M. DuPrey,* y DO, Kathy Liu,z PhD, Peter F. Cronholm, MD, Andrew S. Reisman,{ MD, Steven