Advanced Cardiac Life Support ACLS
|
|
|
- Janel Ford
- 5 years ago
- Views:
Transcription


1 Essential Medical Training, LLC Providing Quality, Professional Training Advanced Cardiac Life Support ACLS Course Study Guide and Agenda office fax
2 Course Outline and General Information Today s course is provided by: Essential Medical Training, LLC office fax treasurecoastcpr@gmail.com Topics Include: System of care Course: Advanced Cardiac Life Support (ACLS) Effective High-Performance Team Dynamics System Approach Airway Support ACS, Stroke Cardiac Arrest: VF/pVT, PEA, Asystole, Bradycardia, SVT, & Post Cardiac Arrest Care Course time: Approximately 7.0 hours Curriculum: American Heart Association (2015 Edition) Course book: Advanced Cardiac Life Support 2016 (ISBN: ) The following information is a guide and basic course outline. The information within this packet is limited and maybe incomplete. Students should refer to their course books and American Heart Association s Emergency Cardiovascular Care handbook for complete and accurate information. Upon completion of the course you will receive a course completion card. You will receive your card within 30 days after the class. Recommended renewal is every two years. Lost Cards: If you lose your card you can obtain a duplicate by contacting us. The cost for a duplicate card is currently $25 and subject to change without notice. Thank you for choosing Essential Medical Training, LLC for your training needs. ENJOY YOUR CLASS!
 and the OHCA (Out-of-Hospital Cardiac Arrest).")
3 SYSTEM OF CARE Effective resuscitation requires a systematic approach using the American Heart Association (AHA) chain of survival. The AHA has created a visual system-specific chain of survival for both the IHCA (In-hospital Cardiac Arrest) and the OHCA (Out-of-Hospital Cardiac Arrest). Figure 1: System-Specific Chain of Survival Rapid Response Teams (RRT) and Medical Emergency Teams (MET) In recent studies, 80% IHCA patients had documented abnormal vital signs for up to 8 hours prior to cardiac arrest. The purpose of these teams are to identify and treat early clinical deterioration of a patient, thereby improving patient overall outcome. Mortality rates remains high with an average survival rate of approximately 24% for IHCA even with advanced care. There are published studies that report a 17%-65% drop in cardiac arrest with early recognition and intervention. Acute Coronary Syndrome (ACS) The primary goals of therapy for patients with ACS are: 1. Reducing the amount of myocardial necrosis that occurs from an acute myocardial infarction. In doing so, you help prevent heart failure and other cardiovascular complications. 2. Prevent major adverse cardiac events 3. Treat acute, life-threatening complications such as VF, pulseless VT (pvt) and other serious rhythms. Prompt diagnosis and treatment offers the greatest potential benefit for myocardial salvage. Acute Stroke There has been significant improvement in stroke care in the past 5 years. Community and professional education is the key to recognition and treatment of stroke patients. EMS has become an integral part of the system with increased training for EMS personnel in recognition and transportation to a stroke center who are prepared to treat such emergencies.
4 Post-Cardiac Arrest Care Patients who achieve a return of spontaneous circulation (ROSC) after cardiac arrest need specialized care to reduce the chance of mortality. Healthcare providers should consider targeted temperature management (TTM) for adult patients who achieve ROSC and remain comatose. The recommended temperature is 32 C and 36 C (89.6 F and 95.2 F) for at least 24 hours. Providers should use 100% oxygen during resuscitation but should titrate inspired oxygen to the lowest level needed to achieve an arterial oxygen saturation of 94% or greater after ROSC. Providers should avoid excessive ventilations because of possible increased intrathoracic pressure and decreased cerebral flow. Ventilations should start at a rate of 10/min to maintain PETCO2 of mm Hg. EMS should consider transportation to a facility capable of providing coronary reperfusion for patients who have ROSC but are suspected of having a coronary artery occlusion. EFFECTIVE HIGH-PERFORMANCE TEAM DYNAMICS Successful resuscitation requires a team of healthcare professionals that perform a variety of interventions. High-performance teams are not only comprised of healthcare providers who can perform advanced skills but also requires a demonstration of clear communications and team work. Team Leader Every high performing team needs a leader that can keep order and rhythm during the resuscitation. The leader is responsible for ensuring that each intervention is completed on time and in the correct sequence. It is important that the team leader demonstrates excellent team behavior in their leadership of the resuscitation team. Occasionally, the team leader will need to act as a coach or teacher to help train future team leaders. After the resuscitation, the team leader should facilitate a review of the team s performance with the intent of looking for areas to improve in the resuscitative attempt. Team Member The team member must be proficient in their skills and clearly understand their roles and responsibilities. A team member committed to success will be knowledgeable about the algorithms. Eight Elements of Effective Team Dynamics 1. Clear roles and responsibilities- Each team member should know their limitations. Team leaders should delegate tasks for efficiency. 2. Knowing your limitations- Team members that are given a task outside of their scope of training should immediately notify the team leader. 3. Constructive interventions- Both team members and team leaders are responsible to speak up if they see another team member that is about to make a mistake. 4. Knowledge sharing- team members should share information with each other and to their team leader. Likewise, team leaders should communicate information to the entire team.
5 5. Summarizing and reevaluating- it is good for team members to repeat or summarize the status of the resuscitation so that the team knows the progress or next step in the resuscitation. 6. Closed-Loop communications- When the team leader gives an order, the team member should make eye contact and confirm the order. The team leader listens to the repeated order to confirm it was received correctly. 7. Clear message- Repeating the order allows both to ensure that the order was received correctly. If the team member thinks that the order is incorrect, they should question the order, respectfully, to avoid a possible mistake. 8. Mutual respect- teams must work together. SYSTEMATIC APPROACH Healthcare providers should use a systematic approach when caring for acutely ill patients. A systematic approach using the BSL assessment includes: Primary Assessment o Check for responsiveness o Call for help o Check breathing and pulse Agonal gasps are not normal breathing and is a sign of cardiac arrest Pulse checks should last no longer than 5 to 10 seconds Respiratory arrest patients should be ventilated every 5 to 6 seconds Cardiac arrest patients with advanced airway should be ventilated every 6 seconds Excessive ventilations increase intrathoracic pressure, decreasing venous return to the heart and diminishes cardiac output o Chest compressions should be started if no pulse is present. Compressions are at least 2 inches deep Compression rate is 100 to 120 per minute Compressions should not be interrupted for longer than 10 seconds Compressors should change every 2 minutes to prevent fatigue o Defibrillation should occur as soon as possible. CPR starting with chest compressions should be started immediately following each shock Secondary Assessment o More in-depth head to toe assessment o H s and T s should be considered for cause of cardiac arrest
6 ACUTE CORONARY SYNDROME (ACS) ACLS providers must be able to assess and stabilize patients with ACS. The 12-lead ECG is used to classify the patients in one of three categories. The categories are ST-segment elevation (acute, ongoing injury), ST-segment depression (ischemia), and normal ECG. Sudden cardiac arrest and hypotensive bradyarrhythmia s can occur with acute ischemia. Including VF and pulseless VT. The most common symptom of myocardial ischemia and infarction is retrosternal chest discomfort. The patient may explain this as a pressure like discomfort or tightness. This discomfort can radiate to the shoulders, neck, one or both arms, or jaw. They may present with nausea, sweating, dizziness, or short of breath. Assessment and treatment include administering oxygen to patients with an oxygen saturation less than 90%. A dose of 160 to 325 mg of non-enteric coated aspirin prevents additional thrombus formation. Administering a dose of aspirin can be beneficial provided the patient has not taken aspirin, does not have a true aspirin allergy, and not recent GI bleeding. The patient should chew the aspirin. Nitroglycerin is effective in reducing ischemic chest discomfort. Nitroglycerin reduces LV and RV preload through peripheral arterial and venous dilation. Administer 1 sublingual nitroglycerin (tab or spray) every 3 to 5 minutes. Nitroglycerin should not be given to patients with systolic pressures below 90 mm Hg. Nitroglycerin should be administered cautiously or not at all in patients with inferior wall MI or recent use of phosphodiesterase inhibitor (Cialis, Viagra). Morphine can be used to relieve chest discomfort unresponsive to nitroglycerin. Morphine causes vasodilation so give in small increments. Fluids should be the first line therapy for hypotension. A 12-lead ECG should be obtained as soon as possible. A 12-lead ECG is the only way to identify a STEMI. Reperfusion is the goal of a STEMI patient. Administering fibrinolytic within 30 minutes of arrival or perform a PCI within 90 minutes of arrival. ACUTE STROKE Stroke is a general term used to refer to a neurological impairment caused by a disruption in blood flow to a part of the brain. There are two major types of strokes which are ischemic and hemorrhagic. Ischemic is caused by an occlusion in a particular part of the brain. Ischemic strokes account for 87% of all strokes. Hemorrhagic is a rupture of a blood vessel in the brain and this type of stroke accounts for 13% of all strokes. Fibrinolytic therapy is contraindicated in hemorrhagic strokes. Ischemic stroke patients have a small window of opportunity (<3 hours or 4.5 hours for selected patients) to receive valuable fibrinolytic therapy. Signs and symptoms associated with a stoke are: Sudden weakness or numbness of the face, arm, or leg, particularly to one side of the body Sudden onset of confusion Trouble speaking Vision problem Trouble with walking or maintaining balance Severe headache
7 Activating the EMS system quickly is crucial to managing the stroke patient. The EMS crew can perform a neurological evaluation such as the Cincinnati Prehospital Stroke Scale. This scale is based on 3 findings and can be performed quickly: Facial droop Arm drift Abnormal speech It is important that EMS crews identify acute strokes and relay the information to the emergency department. The ED will need to quickly perform a CT in order to identify whether it is an ischemic stroke or a hemorrhagic stroke. It is recommended that a CT be performed within 25 minutes of arriving at the hospital and read within 45 of arriving at the hospital. The window of fibrinolytic treatment must be initiated within 3 hours of the initial symptoms. CARDIAC ARREST The cardiac arrest algorithm consists of two pathways: Shockable rhythm (VF/Pulseless VT) Left side Non-shockable rhythm (Asystole, PEA) Right side Treatment of Ventricular fibrillation (VF) is most effective with CPR and a shock from a defibrillator. If a defibrillator is not immediately available, CPR should be started until one becomes available. Chest compressions should be continued while the defibrillator is charging. Before the shock is delivered, the team member will call for all clear. The chance of survival decreases by 10 percent for every minute that passes that CPR and a defibrillator isn t used on a patient in a shockable rhythm. The first drug of choice is Epinephrine. This drug is used mainly because of its β- adrenergic effects of vasoconstriction. Vasoconstriction increases cerebral and coronary blood blow. Epinephrine is given after the second shock at a dose of 1mg IV/IO every 3 to 5 minutes. Vasopressin has been REMOVED from the algorithm. The first drug of choice for antiarrhythmic is Amiodarone at a dose of 300mg IV/IO followed by one additional dose of 150mg IV/IO. Lidocaine can still be used if Amiodarone is not available. Lidocaine is given in the first dose of 1 to 1.5 mg/kg with repeat dose of half the initial dose every 5-10 minutes to a max dose of 3mg/kg. Magnesium Sulfate should be used for torsades de pointes with a loading dose of 1 to 2 g IV/IO diluted in 10 ml of saline given over 5 to 20 minutes. It is recommended that quantitative capnography be used with intubated patients. This allows recognition of ROSC and monitoring of effective chest compressions. A PETCO2 that falls below 10 mm Hg will indicate a need to improve the quality of chest compressions. The right side of the algorithm is asystole and PEA. This side has one main drug of Epinephrine along with high quality CPR. Identifying underlying conditions using the H s and T s.
8 N o t S h o c k a b l e Pulseless Arrest Algorithm BLS, call for help, start CPR Give oxygen when available Attach monitor/defibrillator when available Shockable Check Rhythm Shockable Rhythm? VF/VT Asystole/PEA Give 1 shock AED or Manual (120j-200j) biphasic Resume CPR (start with chest compressions) Resume CPR Vascular access Epinephrine 1mg q 3-5 min Check Rhythm Shockable Rhythm? Check Rhythm Shockable Rhythm? Give 1 shock AED or Manual (120j-200j) biphasic Resume CPR immediately after shock Vascular access Epinephrine 1mg q 3-5 min Check Rhythm Shockable Rhythm? Give 1 shock AED or Manual (120j-200j) biphasic Resume CPR immediately after shock Antiarrhythmics Amiodarone 300mg IV/IO - 2nd dose 150mg Lidocaine 1-1.5mg/kg (can be considered) Magnesium Sulfate 1-2 g IV/IO Torsades de Pointes Push hard and fast at least per minute Compress at least 2 inches Ensure chest recoil Minimize interruptions in chest compressions Atropine no longer used in Asystole/PEA After advanced airway no longer synchronize CPR Look for reversible causes: Hypovolemia Toxins Hypoxia Tamponade Cardiac Hydrogen ion (acidosis) Tension Pneumothorax Hypoglycemia Thrombosis Hypothermia Trauma This algorithm is a summary and should be used only as a guide in conjunction with the course book.
9 Bradycardia with a Pulse Algorithm Assess appropriateness for clinical condition. Heart rate typically < 50/min if Bradyarrythmias Identify and treat underlying cause Maintain patent airway; assist breathing if necessary Oxygen (if hypoxemic) Cardiac monitor to identify rhythm; monitor blood pressure and oximetry IV Access 12-Lead ECG if available; don t delay therapy Monitor and observe NO Persistent bradyarrhythmia causing: Hypotension? Acutely altered mental status? Signs of shock? Ischemic chest discomfort? Acute Heart failure? YES Atropine If Atropine is ineffective: Transcutaneous pacing OR Dopamine infusion OR Epinephrine infusion Consider: Expert consultation Transvenous pacing Dose/Details Atropine IV Dose: First dose: 0.5 mg bolus Repeat every 3-5 minutes Maximum 3 mg Dopamine IV infusion 2-10 mcg/kg per minute Epinephrine IV infusion 2-10 mcg per minute This algorithm is a summary and should be used only as a guide in conjunction with the course book.
10 Tachycardia with a Pulse Algorithm Assess appropriateness for clinical condition. Heart rate typically 150/min if Tachyarrythmias Identify and treat underlying cause Maintain patent airway; assist breathing if necessary Oxygen (if hypoxemic) Cardiac monitor to identify rhythm; monitor blood pressure and oximetry IV Access Persistent tachyarrhythmia causing: Hypotension? Acutely altered mental status? Signs of shock? Ischemic chest discomfort? Acute Heart failure? NO Wide QRS? 0.12 seconds NO YES IV access and 12-Lead ECG if available Vagal maneuvers Adenosine (if regular) ß-Blocker or calcium channel blocker Consider expert consultation YES Synchronized cardioversion Consider sedation If regular narrow complex, consider adenosine IV access and 12-Lead ECG if available Consider adenosine only if regular and monomorphic Consider antiarrhythmic infusion Consider expert consultation Dose/Details Synchronized Cardioversion Initial recommended doses: Narrow regular: J Narrow irregular: J biphasic or 200 J monophasic Wide regular: 100 J Wide irregular: defibrillation does (NOT synchronized) Adenosine IV Dose: First dose: 6 mg rapid IV push; follow with NS flush. Second dose: 12 mg if required. Antiarrhythmic Infusion for Stable Wide-QRS Tachycardia Procainamide IV Dose: mg/min until arrhythmia suppressed, hypotension ensures, QRS duration increases >50%, or maximum dose 17 mg/kg given. Maintenance infusion: 1-4 mg/min. Avoid if prolonged QT or CHF. Amiodarone IV dose: First dose: 150 mg over 10 min. Repeat as needed if VT recurs. Follow by maintenance infusion of 1 mg/min for first 6 hours. Sotalol IV Dose: 100 mg (1.5mg/kg) over 5 minutes. Avoid if prolonged QT. This algorithm is a summary and should be used only as a guide in conjunction with the course book.

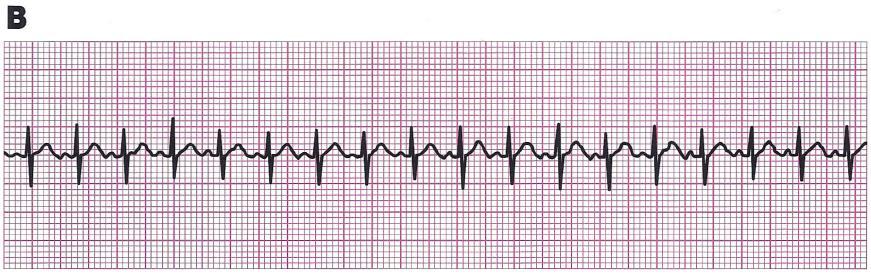
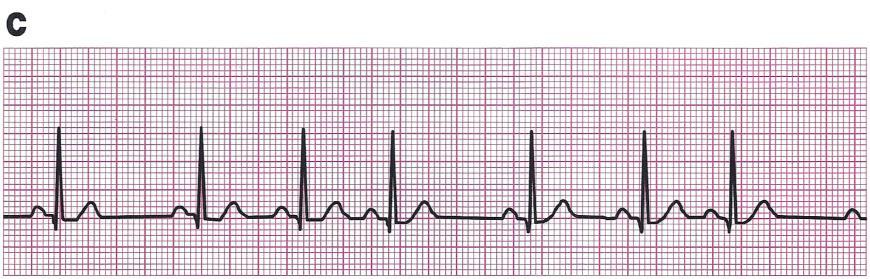
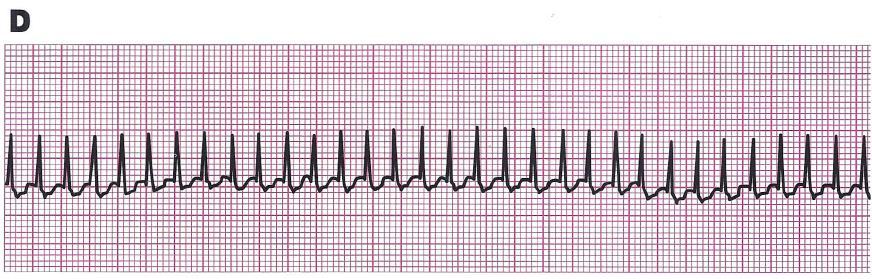
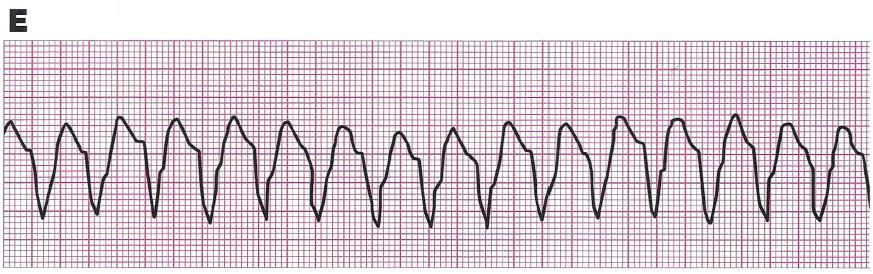
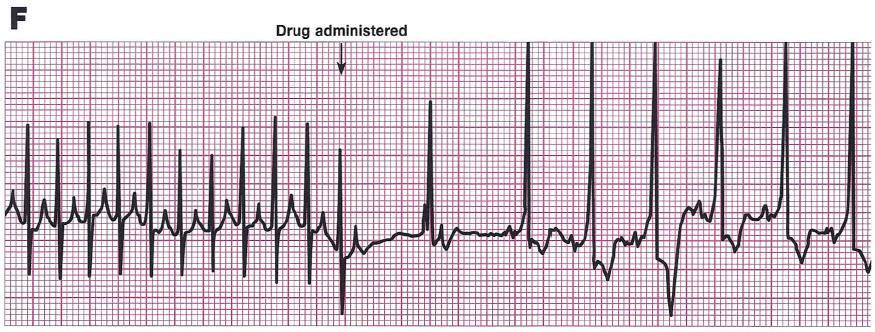
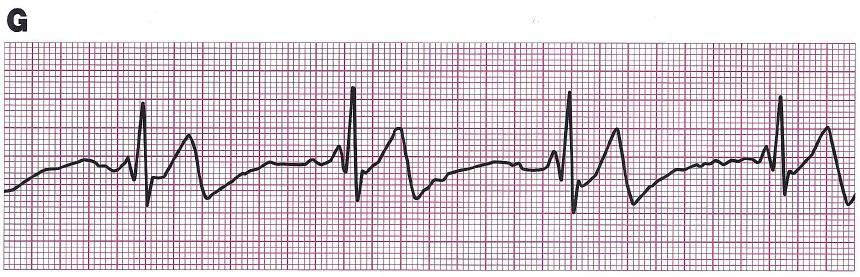
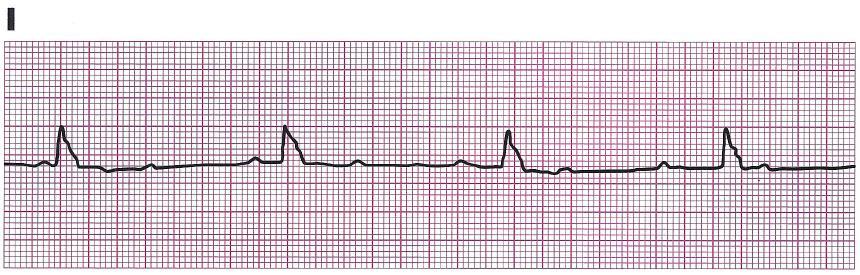
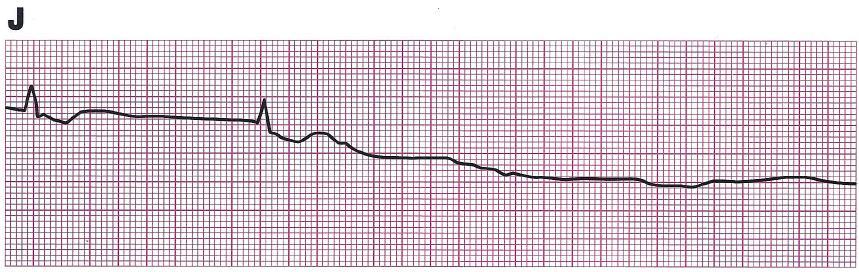
11 ECG Rhythms
12

13
14 Answers to Rhythms A. Sinus Rhythm B. Sinus Tachycardia C. Sinus Arrhythmia D. Narrow-complex Tachycardia E. Wide-complex Tachycardia F. SVT converting to sinus rhythm with adenosine administration G. Sinus bradycardia H. Junctional bradycardia I. Complete heart block with ventricular escape rhythm (3rd degree) J. Agonal rhythm progressing to asystole
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
Unstable: Hypotension/Shock, Fever, Altered Mental Status, Chest discomfort, Acute Heart Failure Saturation <94%, Systolic BP < 90mmHg
 Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
national CPR committee Saudi Heart Association (SHA). International Liason Commission Of Resuscitation (ILCOR)
. International Liason Commission Of Resuscitation (ILCOR)") 2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
MICHIGAN. State Protocols
 MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
ACLS. Advanced Cardiac Life Support Practice Test Questions. 1. The following is included in the ACLS Survey?
 1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
European Resuscitation Council
 European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
Final Written Exam ASHI ACLS
 Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Advanced Cardiac Life Support G 2010
 Advanced Cardiac Life Support G 2010 Produced by the Advanced Cardiac Life Support Council of the Irish Heart Foundation March 2012 Introduction: The Arrhythmia and ACLS Councils of the Irish Heart Foundation
Advanced Cardiac Life Support G 2010 Produced by the Advanced Cardiac Life Support Council of the Irish Heart Foundation March 2012 Introduction: The Arrhythmia and ACLS Councils of the Irish Heart Foundation
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines
 Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Michigan Adult Cardiac Protocols TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Asystole Section 2-1 Bradycardia Section 2-2 Cardiac Arrest General Section 2-3 Cardiac Arrest ROSC Section 2-4 Chest Pain Acute Coronary Syndrome
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Asystole Section 2-1 Bradycardia Section 2-2 Cardiac Arrest General Section 2-3 Cardiac Arrest ROSC Section 2-4 Chest Pain Acute Coronary Syndrome
HigHligHts of the 2018 Focused In 2015 Updates to the American Heart Association Guidelines for CPR and ECC: Advanced Cardiovascular Life
 Highlights of the 2018 Focused Updates to the American Heart Association Guidelines for CPR and ECC: Advanced Cardiovascular Life Support and Pediatric Advanced Life Support - Heart and Stroke Foundation
Highlights of the 2018 Focused Updates to the American Heart Association Guidelines for CPR and ECC: Advanced Cardiovascular Life Support and Pediatric Advanced Life Support - Heart and Stroke Foundation
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket
 BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
ADULT TREATMENT GUIDELINES
 A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION
 RECERTIFICATION EXAMINATION") ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular
 Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care 1 DR. Alireza Abootalebi Assistant Professor Of
Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care 1 DR. Alireza Abootalebi Assistant Professor Of
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
ACLS Study Guide Key guidelines recommendations for healthcare professionals:
 1 ACLS Study Guide 0.849. Key guidelines recommendations for healthcare professionals: Effective teamwork techniques should be learned and practiced regularly. Professional rescuers should use quantitative
1 ACLS Study Guide 0.849. Key guidelines recommendations for healthcare professionals: Effective teamwork techniques should be learned and practiced regularly. Professional rescuers should use quantitative
Advanced Resuscitation - Adult
 C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
1. Normal sinus rhythm 2. SINUS BRADYCARDIA
 1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
Update of CPR AHA Guidelines
 Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
THE EVIDENCED BASED 2015 CPR GUIDELINES
 SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES (EXECUTIVE SUMMARY) Page 1 FORWARD Since 2000, the International Liaison Committee on Resuscitation (ILCOR) has published
SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES (EXECUTIVE SUMMARY) Page 1 FORWARD Since 2000, the International Liaison Committee on Resuscitation (ILCOR) has published
Advanced Resuscitation - Child
 C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
Advanced Resuscitation - Adolescent
 C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University
 Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University Cardiac arrest Cardiac arrest can be caused by 4 rhythms: Ventricular fibrillation
Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University Cardiac arrest Cardiac arrest can be caused by 4 rhythms: Ventricular fibrillation
Utah EMS Protocol Guidelines: Cardiac
 Utah EMS Protocol Guidelines: Cardiac Version 1 / November 1, 2013 Cardiac Patient Care Guidelines These guidelines were created to provide direction for each level of certified provider in caring for
Utah EMS Protocol Guidelines: Cardiac Version 1 / November 1, 2013 Cardiac Patient Care Guidelines These guidelines were created to provide direction for each level of certified provider in caring for
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
Supplemental Digital Content 1. Simulation scenarios and critical action checklist for debriefing
 Supplemental Digital Content 1. Simulation scenarios and critical action checklist for debriefing Simulation Scenario #1 I. Title (ACS)-VF-Asystole-ROSC II. Target learner 6-7 medical students per team
Supplemental Digital Content 1. Simulation scenarios and critical action checklist for debriefing Simulation Scenario #1 I. Title (ACS)-VF-Asystole-ROSC II. Target learner 6-7 medical students per team
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Chain of Survival. Highlights of 2010 American Heart Guidelines CPR
 Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
Cardiopulmonary Resuscitation in Adults
 Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Lecture. ALS Algorithm
 Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005
 RESUSCITATION GUIDELINES 2005") THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care
THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care
VENTRICULAR FIBRILLATION. 1. Safe scene, standard precautions. 2. Establish unresponsiveness, apnea, and pulselessness. 3. Quick look (monitor)
") LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
THE EVIDENCED BASED 2015 CPR GUIDELINES
 SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES Page 1 Chapter 3 ACLS AND SPECIAL SITUATIONS CHAPTER The International Liaison Committee on Resuscitation (ILCOR)
SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES Page 1 Chapter 3 ACLS AND SPECIAL SITUATIONS CHAPTER The International Liaison Committee on Resuscitation (ILCOR)
ADULT CARDIAC EMERGENCIES
 ADULT CARDIAC EMERGENCIES Last Revised: September 2018 Cardiac Emergencies Section A 1 CARDIOPULMONARY ARREST NOTE: High quality CPR includes: 1. Chest Compressions at a depth of at least 2 inches 2. Rate
ADULT CARDIAC EMERGENCIES Last Revised: September 2018 Cardiac Emergencies Section A 1 CARDIOPULMONARY ARREST NOTE: High quality CPR includes: 1. Chest Compressions at a depth of at least 2 inches 2. Rate
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
Asystole / PEA (PEDIATRIC)
") FRRCKSBURG MS Asystole / A (ATRC) 1 Check for Responsiveness Check for Breathing Check for Carotid ulse nitiate CR o As soon as a mechanical external compression device (i.e. Lucas 2) (rocedure 11) becomes
FRRCKSBURG MS Asystole / A (ATRC) 1 Check for Responsiveness Check for Breathing Check for Carotid ulse nitiate CR o As soon as a mechanical external compression device (i.e. Lucas 2) (rocedure 11) becomes
Simulation 15: 51 Year-Old Woman Undergoing Resuscitation
 Simulation 15: 51 Year-Old Woman Undergoing Resuscitation Flow Chart Flow Chart Opening Scenario Section 1 Type: DM Arrive after 5-6 min in-progress resuscitation 51 YO female; no pulse or BP, just received
Simulation 15: 51 Year-Old Woman Undergoing Resuscitation Flow Chart Flow Chart Opening Scenario Section 1 Type: DM Arrive after 5-6 min in-progress resuscitation 51 YO female; no pulse or BP, just received
Yolo County Health & Human Services Agency
 Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
ADULT CARDIAC EMERGENCIES
 ADULT CARDIAC EMERGENCIES Last Revised: July 2017 Cardiac Emergencies Section A 1 CARDIOPULMONARY ARREST NOTE: High quality CPR includes: 1. Chest Compressions at a depth of at least 2 inches 2. Rate of
ADULT CARDIAC EMERGENCIES Last Revised: July 2017 Cardiac Emergencies Section A 1 CARDIOPULMONARY ARREST NOTE: High quality CPR includes: 1. Chest Compressions at a depth of at least 2 inches 2. Rate of
ACLS: 2015 Update. What s new? Or:
 ACLS: 2015 Update Or: What s new? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery CME Faculty Disclosure Dr. Shulman has no affiliation
ACLS: 2015 Update Or: What s new? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery CME Faculty Disclosure Dr. Shulman has no affiliation
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
ACLS/ACS Updates 2015
 ACLS/ACS Updates 2015 Advanced Cardiovascular Life Support by: Fareed Al Nozha, JBIM, ABIM, FKFSH&RC(Cardiology) Consultant Cardiologist Faculty, National CPR Committee, ACLS Program Head, SHA Dr Abdulhalim
ACLS/ACS Updates 2015 Advanced Cardiovascular Life Support by: Fareed Al Nozha, JBIM, ABIM, FKFSH&RC(Cardiology) Consultant Cardiologist Faculty, National CPR Committee, ACLS Program Head, SHA Dr Abdulhalim
table of contents adult treatment guidelines
 table of contents adult treatment guidelines A1 ADULT PATIENT CARE... 3 A2 CHEST PAIN SUSPECTED ACUTE CORONARY SYNDROME/STEMI...4 5 A3 CARDIAC ARREST INITIAL CARE AND CPR...6 7 A4 VENTRICULAR FIBRILLATION
table of contents adult treatment guidelines A1 ADULT PATIENT CARE... 3 A2 CHEST PAIN SUSPECTED ACUTE CORONARY SYNDROME/STEMI...4 5 A3 CARDIAC ARREST INITIAL CARE AND CPR...6 7 A4 VENTRICULAR FIBRILLATION
WHAT DO YOU SEE WHEN YOU STIMULATE BETA
 CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
ADVANCED LIFE SUPPORT
 ANSWERS IN ITALICS WITH REFERENCES 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care professionals equipped with a manual defibrillator, the providers
ANSWERS IN ITALICS WITH REFERENCES 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care professionals equipped with a manual defibrillator, the providers
Emergency Cardiac Care Guidelines 2015
 Emergency Cardiac Care Guidelines 2015 VACEP 2016 William Brady, MD University of Virginia Guidelines 2015 Basic Life Support & Advanced Cardiac Life Support Acute Coronary Syndrome Pediatric Advanced
Emergency Cardiac Care Guidelines 2015 VACEP 2016 William Brady, MD University of Virginia Guidelines 2015 Basic Life Support & Advanced Cardiac Life Support Acute Coronary Syndrome Pediatric Advanced
JUST SAY NO TO DRUGS?
 JUST SAY NO TO DRUGS? THE EVIDENCE BEHIND MEDICATIONS USED IN CARDIAC RESUSCITATION NTI 2014 CLASS CODE 148 Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives 1. Discuss the historical evidence supporting
JUST SAY NO TO DRUGS? THE EVIDENCE BEHIND MEDICATIONS USED IN CARDIAC RESUSCITATION NTI 2014 CLASS CODE 148 Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives 1. Discuss the historical evidence supporting
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Johnson County Emergency Medical Services Page 23
 Non-resuscitation Situations: Resuscitation should not be initiated in the following situations: Prolonged arrest as evidenced by lividity in dependent parts, rigor mortis, tissue decomposition, or generalized
Non-resuscitation Situations: Resuscitation should not be initiated in the following situations: Prolonged arrest as evidenced by lividity in dependent parts, rigor mortis, tissue decomposition, or generalized
1. What would you do first to restore oxygenation and ventilation to an unresponsive, breathless, near-drowning victim?
 ACLS Provider Course SAMPLE ACLS PRE-TEST EXAM This is a single-answer multiple-choice examination. There is only one correct answer to each question. 1. What would you do first to restore oxygenation
ACLS Provider Course SAMPLE ACLS PRE-TEST EXAM This is a single-answer multiple-choice examination. There is only one correct answer to each question. 1. What would you do first to restore oxygenation
ALS MODULE 7 Pharmacology
 ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
PALS Review 2015 Guidelines
 PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
Prior to taking ACLS, it is assumed that you are proficient and currently certified in Basic Life
 Table of Contents Overview of Advanced Cardiovascular Life Support... 2 Updates to ACLS in 2015... 3 Chain of Survival... 4 Adult BLS Chain of Survival... 4 BLS and ACLS Surveys... 5 The BLS Survey...
Table of Contents Overview of Advanced Cardiovascular Life Support... 2 Updates to ACLS in 2015... 3 Chain of Survival... 4 Adult BLS Chain of Survival... 4 BLS and ACLS Surveys... 5 The BLS Survey...
Portage County EMS Patient Care Guidelines. Cardiac Arrest
 Portage County EMS Patient Care Guidelines Cardiac Arrest Note: These guidelines are based on (or adapted from) the current American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency
Portage County EMS Patient Care Guidelines Cardiac Arrest Note: These guidelines are based on (or adapted from) the current American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency
table of contents pediatric treatment guidelines
 table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation
 The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
Department of Paediatrics Clinical Guideline. Advanced Paediatric Life Support. Sequence of actions. 1. Establish basic life support
 Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
2015 Interim Training Materials
 2015 Interim Training Materials ACLS Manual and ACLS EP Manual Comparison Chart Assessment sequence Manual, Part 2: The Systematic Approach, and Part BLS Changes The HCP should check for response while
2015 Interim Training Materials ACLS Manual and ACLS EP Manual Comparison Chart Assessment sequence Manual, Part 2: The Systematic Approach, and Part BLS Changes The HCP should check for response while
The 2015 BLS & ACLS Guideline Updates What Does the Future Hold?
 The 2015 BLS & ACLS Guideline Updates What Does the Future Hold? Greater Kansas City Chapter Of AACN 2016 Visions Critical Care Conference Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Independent CNS/Staff
The 2015 BLS & ACLS Guideline Updates What Does the Future Hold? Greater Kansas City Chapter Of AACN 2016 Visions Critical Care Conference Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Independent CNS/Staff
MASTER SYLLABUS
 A. Academic Division: Health Sciences B. Discipline: Respiratory Care MASTER SYLLABUS 2018-2019 C. Course Number and Title: RESP 2330 Advanced Life Support Procedures D. Course Coordinator: Tricia Winters,
A. Academic Division: Health Sciences B. Discipline: Respiratory Care MASTER SYLLABUS 2018-2019 C. Course Number and Title: RESP 2330 Advanced Life Support Procedures D. Course Coordinator: Tricia Winters,
CARDIAC ARREST GENERAL CONSIDERATION
 CARDIAC ARREST GENERAL CONSIDERATION A. Age delineation: Infant CPR guidelines apply to victims less than one year of age; Child CPR guidelines apply to victims one year of age to the onset of adolescence
CARDIAC ARREST GENERAL CONSIDERATION A. Age delineation: Infant CPR guidelines apply to victims less than one year of age; Child CPR guidelines apply to victims one year of age to the onset of adolescence
TABLE OF CONTENTS. Page 2 of 52
 Page 1 of 52 TABLE OF CONTENTS Table of Contents...2 List of Figures...4 List of Tables...4 Unit One: ACLS Overview...5 Preparing for ACLS...5 Organization of the ACLS Course...5 2015 ACLS Guideline Changes...6
Page 1 of 52 TABLE OF CONTENTS Table of Contents...2 List of Figures...4 List of Tables...4 Unit One: ACLS Overview...5 Preparing for ACLS...5 Organization of the ACLS Course...5 2015 ACLS Guideline Changes...6
Requirements to successfully complete PALS:
 The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
Consider Treatable Underlying Causes Early
 Page 1 of 8 Cardiac Arrest Timeout Checklist Assign roles for Pit Crew CPR o Compressors x 2 o Airway o Lead responsible for coordinating team, making decisions o Medications Continuous compressions at
Page 1 of 8 Cardiac Arrest Timeout Checklist Assign roles for Pit Crew CPR o Compressors x 2 o Airway o Lead responsible for coordinating team, making decisions o Medications Continuous compressions at
Shifts 28, 29, 30 Quizzes
 Shifts 28, 29, 30 Quizzes Name: Score: Date: 1. You are on the scene of a 4 year old in cardiac arrest. CPR is initiated and an E.T. tube has been placed, an I.V. has been established. What is the correct
Shifts 28, 29, 30 Quizzes Name: Score: Date: 1. You are on the scene of a 4 year old in cardiac arrest. CPR is initiated and an E.T. tube has been placed, an I.V. has been established. What is the correct
TEACHING BASIC LIFE SUPPORT (& ALS)
") TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
ACLS: 2015 Update. Anything New?
 ACLS: 2015 Update Anything New? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery Copyright 2017 by Sea Courses Inc. All rights
ACLS: 2015 Update Anything New? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery Copyright 2017 by Sea Courses Inc. All rights
HealthCare Training Service
 HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
Outline of the 2005 European Resuscitation Council Guidelines
 Practice Guidelines Launch Outline of the 2005 European Resuscitation Council Guidelines Mary Rose Cassar, Diane Tabone Introduction Resuscitation guidelines are revised and updated about every 5 years
Practice Guidelines Launch Outline of the 2005 European Resuscitation Council Guidelines Mary Rose Cassar, Diane Tabone Introduction Resuscitation guidelines are revised and updated about every 5 years
Welcome to ACLS with Medical Education Angels!
 Welcome to ACLS with Medical Education Angels! For your greatest success, please be aware that the AHA assumes those taking ACLS have the ability to interpret and determine appropriate treatments for a
Welcome to ACLS with Medical Education Angels! For your greatest success, please be aware that the AHA assumes those taking ACLS have the ability to interpret and determine appropriate treatments for a
ACLS Emergency Cardiac Drug Therapy (bolded = changes based on 2005 AHA ACLS Guidelines) revised 01/18/07
 revised 01/18/07") Oxygen Acute Chest Pain Suspected hypoxemia of any cause or c/o SOB Cardiopulmonary Arrest correct hypoxemia by O2 tension O2 content tissue oxygenation O2 Toxicity with high FIO2s May cause CO2 if a CO2
Oxygen Acute Chest Pain Suspected hypoxemia of any cause or c/o SOB Cardiopulmonary Arrest correct hypoxemia by O2 tension O2 content tissue oxygenation O2 Toxicity with high FIO2s May cause CO2 if a CO2
ACLS & Beyond. Christa Creech, Pharm.D. PGY-2 Emergency Medicine Pharmacy Resident October 7 th, 2018
 ACLS & Beyond Christa Creech, Pharm.D. PGY-2 Emergency Medicine Pharmacy Resident October 7 th, 2018 Objectives List recent changes to ACLS guidelines applicable to pharmacists Recognize reversible causes
ACLS & Beyond Christa Creech, Pharm.D. PGY-2 Emergency Medicine Pharmacy Resident October 7 th, 2018 Objectives List recent changes to ACLS guidelines applicable to pharmacists Recognize reversible causes
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Manual Defibrillation. CPR AGE: 18 years LOA: Altered HR: N/A RR: N/A SBP: N/A Other: N/A
 ROC AMIODARONE, LIDOCAINE OR PLACEBO FOR OUT OF HOSPITAL CARDIAC ARREST DUE TO VENTRICULAR FIBRILLATION OR TACHYCARDIA (ALPS) STUDY: MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic
ROC AMIODARONE, LIDOCAINE OR PLACEBO FOR OUT OF HOSPITAL CARDIAC ARREST DUE TO VENTRICULAR FIBRILLATION OR TACHYCARDIA (ALPS) STUDY: MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic
Lesson 4-3: Cardiac Emergencies. CARDIAC EMERGENCIES Angina, AMI, CHF and AED
 Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Pediatric Advanced Life Support Essentials
 chapter 14 Pediatric Advanced Life Support Essentials Sharon E. Mace, MD, FACEP, FAAP 1Discuss the new developments in resuscitation science. Review new 2010 2 American Heart Association Guidelines for
chapter 14 Pediatric Advanced Life Support Essentials Sharon E. Mace, MD, FACEP, FAAP 1Discuss the new developments in resuscitation science. Review new 2010 2 American Heart Association Guidelines for