Trimodality Therapy for Muscle Invasive Bladder Cancer
|
|
|
- Doris Underwood
- 5 years ago
- Views:
Transcription

1 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton, Alberta
2 Key Learning Objectives By participating in this session, health care professionals will: Review the evidence for trimodality therapy in muscle invasive bladder cancer Understand how trimodality therapy is delivered Identify optimal candidates for a bladder-sparing approach
3 Trimodality Therapy for Muscle Invasive Bladder Cancer ICUC 2015 Brita Danielson MD FRCPC Radiation Oncology, Cross Cancer Institute
4 Bladder Preservation with Trimodality Therapy What Why How
5 Bladder Preservation with Trimodality Therapy What Why How
6 What is Trimodality Therapy (TMT)? 1) Maximal TURBT followed by 2) External beam radiation therapy combined with 3) Chemotherapy (various concurrent, neoadjuvant, and adjuvant protocols) Cystoscopic assessment During chemort: response to therapy Follow-up surveillance Radical cystectomy reserved as a salvage option: incomplete response invasive local recurrence
7 Bladder Preservation with Trimodality Therapy What Why How
8 Why consider TMT? Radical cystectomy with pelvic LN dissection is the longstanding standard of care for muscle invasive bladder cancer 5 year OS rates: 55-60% in contemporary series
9 Why consider TMT? Some patients are not surgical candidates Age Comorbidities Even in patients fit for cystectomy, removal of bladder may lead to morbidity and affect patient comfort and QOL Despite sophisticated techniques for urinary diversion and option of orthotopic neobladder with continent urinary diversion
10 Organ Preservation Organ-preserving multimodality therapies have been established in other malignancies Head and neck cancer Cervical cancer Anal canal cancer
11 TMT vs Radical Cystectomy No RCTs that have directly compared radical surgery to TMT bladder-preservation UK Phase III RCT: SPARE (Selective Bladder Preservation Against Radical Excision) failed to accrue patients Indirect comparison between two approaches is difficult Selection bias TMT patients tend to be older with more comorbidities Clinico-pathologic stage discordance Clinical under-staging in 50% of patients
12 Evidence for TMT Decades of experience with bladderpreservation approaches single institution and cooperative group studies Recent pooled analysis of 6 RTOG Trials (Mak et al, Journal of Clinical Oncology, Dec, 2014) 468 patients treated for bladder preservation (5 phase II trials, 1 phase III trial)
13 RTOG Pooled Analysis Median follow-up of 4.3 years (7.8 years among survivors) 5 year OS rate: 57% 10 year OS rate: 36% Similar to contemporary cystectomy studies
14 RTOG Pooled Analysis Complete response to chemort was 69% Local failure rate of 43% Most local failures were non muscle-invasive 80% of patients had an intact bladder at 5 years Indications for salvage cystectomy: 62%: incomplete response to chemort 36%: invasive local recurrence on follow-up 2%: other causes Distant mets develop in 1/3 of patients
15 T2 vs T3/4 disease: RTOG Subgroup Analysis Higher T-stage associated with decreased OS 5 yr OS: 62% T2 vs 49% T3/4 10 yr OS: 41% T2 vs 30% T3/4 TMT for the elderly: Patients age 75 (n= 80): no difference in rates of complete response, DSS, and bladder-intact survival
16 Common concerns regarding TMT Long Term Toxicity Pooled analysis of RTOG studies (Efstathiou et al, Journal of Clinical Oncology, 2009) Late grade 3 GU toxicity: 5.7% Late grade 3 GI toxicity: 1.9% Other series confirm low risk of toxicity, good QOL outcomes, and preservation of a functional bladder ie: cystectomy for contracted bladder: 0% in MGH series, 2% (3 patients) in Erlangen series
17 Common concerns regarding TMT Curability and Feasibility of salvage cystectomy Patients in the pooled analysis of RTOG studies who required salvage cystectomy still had a 5 yr DSS rate of 60%, and 10 year DSS rate of 47% Risk of complications from radical cystectomy after TMT is acceptable compared with upfront cystectomy 16% incidence of major complications and 2.2% rate of mortality within 90 days (Eswara et al, Journal of Urology, 2012) However, orthotopic neobladder reconstruction has a higher risk of functional complications after pelvic RT

18 Bladder Preservation with Trimodality Therapy What Why How
19 How is Trimodality Therapy delivered? Patient Selection: Ideal candidates for TMT: Small tumor (< 5 cm) Unifocal disease Absence of in situ tumors Visibly and microscopically complete TURBT Absence of hydronephrosis No pelvic lymph node metastases Good bladder function at baseline Agreeable to follow-up cystoscopy
20 How is Trimodality Therapy delivered? Maximal TURBT Start chemort within 6-8 weeks EBRT: Standard fractionation (1.8 2Gy per fraction) At least Gy to pelvic LN, 65 Gy to bladder 6-7 week course of daily treatments Use of IMRT to better target treatment volumes and avoid normal surrounding tissue In cystectomy candidates, second-look cystoscopy may be done after Gy to ensure response Salvage cystectomy is considered in patients with residual disease
21
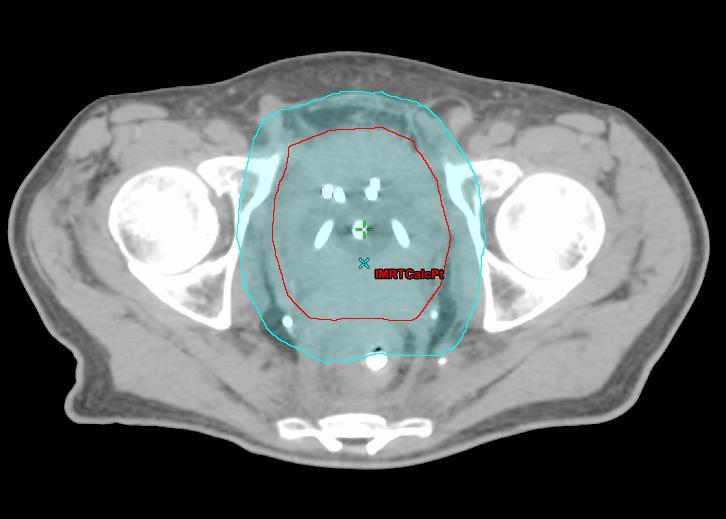
22
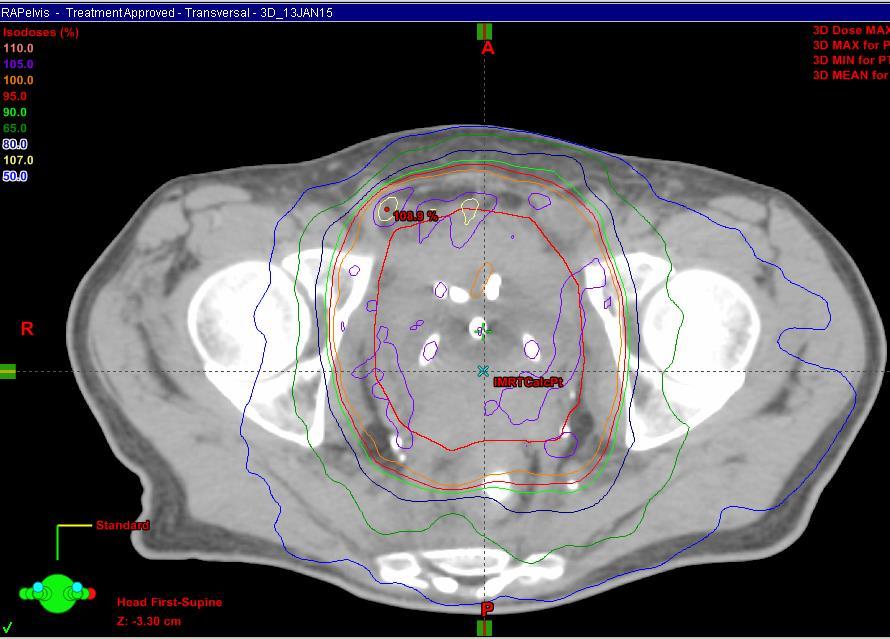
23
24 EBRT Side effects Acute: Fatigue Irritative voiding symptoms Loose stool, diarrhea Late: Change in bladder habits <5% risk of bladder contracture or ulceration requiring cystectomy Proctitis Rare: small bowel injury (obstruction, perforation, fistula), second malignancy
25 How is Trimodality Therapy delivered? Chemo: Concurrent cisplatin most commonly used Given q 1-3 weeks during RT (depending on dose) Weekly carboplatin for patients with poor renal function Some patients receive neoadjuvant chemo prior to chemort Cisplatin/gemcitabine x 3 cycles
26 Follow-up after Trimodality Therapy Cystoscopy ± biopsy and cytology q 3 months for 1 year, then at increasing intervals CT abdomen and pelvis q 3-6 months for 2 years, then at increasing intervals CXR q 6 months for 3 years, then at increasing intervals
27 Conclusions TMT is a safe and effective treatment approach that should be offered to good candidates with muscle invasive bladder cancer Survival rates comparable to surgery Acceptable late toxicity Vast majority of survivors preserve their bladders When counseling patients with muscle-invasive bladder cancer concerning their treatment options, organ-sparing TMT cannot be ignored. (Rödel, JCO Editorial, 2014)
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer
 Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer
 Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
Dr. Tareq Salah Ahmed,MD,ESMO. Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate
 Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists. Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Point/Counterpoint: Quality of Life Considerations for Patients with Muscle Invasive Bladder Cancer Pro Trimodality Therapy
 Point/Counterpoint: Quality of Life Considerations for Patients with Muscle Invasive Bladder Cancer Pro Trimodality Therapy Kimberley S. Mak, MD, MPH Assistant Professor Boston Medical Center Boston University
Point/Counterpoint: Quality of Life Considerations for Patients with Muscle Invasive Bladder Cancer Pro Trimodality Therapy Kimberley S. Mak, MD, MPH Assistant Professor Boston Medical Center Boston University
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Bladder Preservation Protocols in the Treatment of Muscle-Invasive Bladder Cancer
 Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Cochrane metaanalysis 5 year OS Intent to treat
 RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
AUA Guidelines for Invasive Bladder Cancer: What s New?
 AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER
 RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
Chemotherapy and Bladder Cancer. Blayne Welk UBC Urology Grand Rounds June 4, 2008
 Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
September 10, Dear Dr. Clark,
 September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Breast cancer Can I still keep my breast?
 Bladder Cancer Organ-Sparing Approaches SAMO Interdisciplinary Workshop on Urogenital Tumors September 15, 2012 Daniel R. Zwahlen, MD Radiation Oncology Breast cancer Can I still keep my breast? History
Bladder Cancer Organ-Sparing Approaches SAMO Interdisciplinary Workshop on Urogenital Tumors September 15, 2012 Daniel R. Zwahlen, MD Radiation Oncology Breast cancer Can I still keep my breast? History
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline
 Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
5/26/16: CT scan of the abdomen showed a multinodular liver disease highly suspicious for metastasis and hydronephrosis of the right kidney.
 Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Partial Cystectomy for Invasive Bladder Cancer
 European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Debate: Adjuvant vs. Neoadjuvant Therapy for Urothelial Cancer
 Debate: Adjuvant vs. Neoadjuvant Therapy for Urothelial Cancer Kala Sridhar, MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital GU Medical Oncology Site Group Head Associate Professor, University
Debate: Adjuvant vs. Neoadjuvant Therapy for Urothelial Cancer Kala Sridhar, MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital GU Medical Oncology Site Group Head Associate Professor, University
Case 1. Receives induction BCG weekly x 6 without significant toxicity Next step should be:
 Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
Subject Index. Androgen antiandrogen therapy, see Hormone ablation therapy, prostate cancer synthesis and metabolism 49
 OOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index Androgen antiandrogen therapy, see Hormone ablation therapy, synthesis and metabolism 49 Bacillus Calmette-Guérin adjunct therapy with transurethral resection
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index Androgen antiandrogen therapy, see Hormone ablation therapy, synthesis and metabolism 49 Bacillus Calmette-Guérin adjunct therapy with transurethral resection
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
Bladder Cancer in Primary Care. Dr Penny Kehagioglou Consultant Clinical Oncologist
 Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Old and New Radiation for Bladder and Upper Tract Cancers. Bridget Koontz Radiation Oncology Duke Cancer Institute
 Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Bladder replacement in men and women: when and when not? Outline. Continent Diversion History
 1 Bladder replacement in men and women: when and when not? Eila C. Skinner, MD Professor of Clinical Urology Keck USC School of Medicine Outline 1) Selection criteria for orthotopic diversion: Tumor-related
1 Bladder replacement in men and women: when and when not? Eila C. Skinner, MD Professor of Clinical Urology Keck USC School of Medicine Outline 1) Selection criteria for orthotopic diversion: Tumor-related
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015
 Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Radiation Oncology MOC Study Guide
 Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Bladder Cancer. Clinical Case Conference
 Bladder Cancer Clinical Case Conference Clinical Case 89 yo M with gross hematuria Labs: Chem: BUN/Cr increased 22/1.27 CBC: H/H 13/36, WBCs wnl UA: >50 RBCs, otherwise wnl UCx: No growth Cystoscopy at
Bladder Cancer Clinical Case Conference Clinical Case 89 yo M with gross hematuria Labs: Chem: BUN/Cr increased 22/1.27 CBC: H/H 13/36, WBCs wnl UA: >50 RBCs, otherwise wnl UCx: No growth Cystoscopy at
Organ-sparing treatment of invasive transitional cell bladder carcinoma
 Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
PSA is rising: What to do? After curative intended radiotherapy: More local options?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer
 Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer") Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Point-Counterpoint: Radiation & Bladder Cancer
 Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
ARROCase: Locally Advanced Endometrial Cancer
 ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK
 Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Highlighting Clinical Trials Muscle Invasive Bladder Cancer
 Highlighting Clinical Trials Muscle Invasive Bladder Cancer Part I: The Basics of MIBC Clinical Trials June 19, 2018 Presented by: Dr. Peter Black is a urologic oncologist at Vancouver General Hospital,
Highlighting Clinical Trials Muscle Invasive Bladder Cancer Part I: The Basics of MIBC Clinical Trials June 19, 2018 Presented by: Dr. Peter Black is a urologic oncologist at Vancouver General Hospital,
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016
 BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER
 UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
BLADDER CANCER: PATIENT INFORMATION
 BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
receive adjuvant chemotherapy
 Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
Adjuvant Therapies in Endometrial Cancer. Emma Hudson
 Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Bladder-sparing, Combined-modality Approach for Muscle-invasive Bladder Cancer
 75 Bladder-sparing, Combined-modality Approach for Muscle-invasive Bladder Cancer A Multi-institutional, Long-term Experience Sisto Perdona, MD 1 Riccardo Autorino, MD, PhD 2 Rocco Damiano, MD 3 Marco
75 Bladder-sparing, Combined-modality Approach for Muscle-invasive Bladder Cancer A Multi-institutional, Long-term Experience Sisto Perdona, MD 1 Riccardo Autorino, MD, PhD 2 Rocco Damiano, MD 3 Marco
Chemotherapy Treatment Algorithms for Urology Cancer
 Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
GYNECOLOGIC CANCER and RADIATION THERAPY. Jon Anders M.D. Radiation Oncology
 GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Curie - davinci connection
 Organ sparing treatment in MIBC: Robot assisted laparoscopy & Interstitial Radiotherapy brachytherapy Curie - davinci connection Geert Smits MD PhD FEBU Rijnstate Hospital, Arnhem, NL 010 Geert Smits Intuitive:
Organ sparing treatment in MIBC: Robot assisted laparoscopy & Interstitial Radiotherapy brachytherapy Curie - davinci connection Geert Smits MD PhD FEBU Rijnstate Hospital, Arnhem, NL 010 Geert Smits Intuitive:
Malignant Peripheral Nerve Sheath Tumor post Wide Excision with Multiple Lung Metastases: the Role and Treatment Consideration of RT
 Malignant Peripheral Nerve Sheath Tumor post Wide Excision with Multiple Lung Metastases: the Role and Treatment Consideration of RT Case Number: RT2009-64(M) Potential Audiences: Intent Doctor, Oncology
Malignant Peripheral Nerve Sheath Tumor post Wide Excision with Multiple Lung Metastases: the Role and Treatment Consideration of RT Case Number: RT2009-64(M) Potential Audiences: Intent Doctor, Oncology
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery
 Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Cervical Cancer Guidelines L and SC Network July Introduction:
 Cervical Cancer Guidelines L and SC Network July 2018 Introduction: There was a total number of 442 cases of cervix cancer diagnosed in Lancashire and South Cumbria Cancer Network in the period 2005 2009
Cervical Cancer Guidelines L and SC Network July 2018 Introduction: There was a total number of 442 cases of cervix cancer diagnosed in Lancashire and South Cumbria Cancer Network in the period 2005 2009
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
PORTEC-4. Patient seqnr. Age at inclusion (years) Hospital:
 Hospital:") May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Bladder Cancer Canada November 21st, Bladder Cancer 2018: A brighter light at the end of the cystoscope
 Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Bladder Preservation for muscle invasive disease. Nicholas
 Bladder Preservation for muscle invasive disease Nicholas James @Prof_Nick_James 1 Overview Evidence base for bladder preservation as alternative to surgery Chemoradiotherapy compared to radiotherapy alone
Bladder Preservation for muscle invasive disease Nicholas James @Prof_Nick_James 1 Overview Evidence base for bladder preservation as alternative to surgery Chemoradiotherapy compared to radiotherapy alone
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
TREATMENT OF INVASIVE bladder cancer remains a
 Combined-Modality Treatment and Selective Organ Preservation in Invasive Bladder Cancer: Long-Term Results By Claus Rödel, Gerhard G. Grabenbauer, Reinhard Kühn, Thomas Papadopoulos, Jürgen Dunst, Martin
Combined-Modality Treatment and Selective Organ Preservation in Invasive Bladder Cancer: Long-Term Results By Claus Rödel, Gerhard G. Grabenbauer, Reinhard Kühn, Thomas Papadopoulos, Jürgen Dunst, Martin
Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer Center Contemporary Experience
 International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
ROBOTIC VS OPEN RADICAL CYSTECTOMY
 ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer
 in Cervical Cancer") Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
A phase II study of weekly paclitaxel and cisplatin followed by radical hysterectomy in stages IB2 and IIA2 cervical cancer AGOG14-001/TGOG1008
 A phase II study of weekly paclitaxel and cisplatin followed by radical hysterectomy in stages IB2 and IIA2 cervical cancer AGOG14-001/TGOG1008 NCT02432365 Chyong-Huey Lai, MD On behalf of Principal investigator
A phase II study of weekly paclitaxel and cisplatin followed by radical hysterectomy in stages IB2 and IIA2 cervical cancer AGOG14-001/TGOG1008 NCT02432365 Chyong-Huey Lai, MD On behalf of Principal investigator
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Lung Cancer Radiotherapy
 Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Radiation Therapy: From Fallacy to Science
 27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
Chemotherapy for Urological Cancers
 Chemotherapy for Urologic Cancers Matthew Rettig, MD Associate Professor Department of Medicine Division of Hematology-Oncology Department of Urology Medical Director, Prostate Cancer Program Institute
Chemotherapy for Urologic Cancers Matthew Rettig, MD Associate Professor Department of Medicine Division of Hematology-Oncology Department of Urology Medical Director, Prostate Cancer Program Institute
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer
 Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Early radical cystectomy in NMIBC Marko Babjuk
 Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Invasive Bladder Transitional Cell Carcinoma OBJECTIVES
 Invasive Bladder Transitional Cell Carcinoma UBC Urology Grand Rounds 7 September 2005 John Morrell R5 OBJECTIVES Review role of lymphadenectomy Review role of chemotherapy Review results of bimodal bladder
Invasive Bladder Transitional Cell Carcinoma UBC Urology Grand Rounds 7 September 2005 John Morrell R5 OBJECTIVES Review role of lymphadenectomy Review role of chemotherapy Review results of bimodal bladder
Radiochemotherapy after Transurethral Resection is an Effective Treatment Method in T1G3 Bladder Cancer
 Radiochemotherapy after Transurethral Resection is an Effective Treatment Method in T1G3 Bladder Cancer Z. AKÇETIN 1, J. TODOROV 1, E. TÜZEL 1, D.G. ENGEHAUSEN 1, F.S. KRAUSE 1, R. SAUER 2, K.M. SCHROTT
Radiochemotherapy after Transurethral Resection is an Effective Treatment Method in T1G3 Bladder Cancer Z. AKÇETIN 1, J. TODOROV 1, E. TÜZEL 1, D.G. ENGEHAUSEN 1, F.S. KRAUSE 1, R. SAUER 2, K.M. SCHROTT
Greater Baltimore Medical Center Sandra & Malcolm Berman Cancer Institute
 2008 ANNUAL REPORT Greater Baltimore Medical Center Sandra & Malcolm Berman Cancer Institute Cancer Registry Report The Cancer Data Management System/ Cancer Registry collects data on all types of cancer
2008 ANNUAL REPORT Greater Baltimore Medical Center Sandra & Malcolm Berman Cancer Institute Cancer Registry Report The Cancer Data Management System/ Cancer Registry collects data on all types of cancer
Brachytherapy for Bladder carcinoma
 Brachytherapy for Bladder carcinoma Geert Smits MD PhD FEBU Onco-urology, Robotsurgery 010 Intuitive: International proctor Electa: Scientific collaboration Stichting vrienden Rijnstate Intellectual property
Brachytherapy for Bladder carcinoma Geert Smits MD PhD FEBU Onco-urology, Robotsurgery 010 Intuitive: International proctor Electa: Scientific collaboration Stichting vrienden Rijnstate Intellectual property
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Part II: Treatment. A Woman-to-Woman Talk with Dr. Armine Smith. Wednesday, March 8, Presented by
 Women & Bladder Cancer A Woman-to-Woman Talk with Dr. Armine Smith Wednesday, March 8, 2017 Part II: Treatment Presented by Dr. Smith is an Assistant Professor of Urology at Johns Hopkins University and
Women & Bladder Cancer A Woman-to-Woman Talk with Dr. Armine Smith Wednesday, March 8, 2017 Part II: Treatment Presented by Dr. Smith is an Assistant Professor of Urology at Johns Hopkins University and