Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
|
|
|
- Gwenda Lawson
- 5 years ago
- Views:
Transcription
1 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
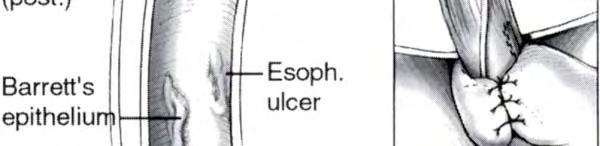
 & Lortat-Jacob (1957) Columnar epithelium-lined esophagus Ulcers in this area: Barrett s ulcers Ultimatately l named Barrett s")
2 Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined by squamous epithelium Columnar lining due to congenital shortening Tubular portion of stomach trapped in the chest Allison/Johnstone (1953) & Lortat-Jacob (1957) Columnar epithelium-lined esophagus Ulcers in this area: Barrett s ulcers Ultimatately l named Barrett s esophagus


3 Change in distal esophageal epithelium Any length Recognized as columnar mucosa on EGD Confirmation of intestinal metaplasia Multiple biopsies Pre-malignant lesion for adenocarcinoma 1. Sharma P, McQuaid KR, Dent J, et al. A critical review of the diagnosis and management of Barrett s esophagus: the AGA Chicago workshop. Gastroenterology 2004;127: Wang KK, Sampliner RE. Updated Guidelines 2008 for the Diagnosis, Surveillance and Therapy of Barrett s Esophagus. Am J Gastroenterol 2008;103:


4 Gastric fundus: resembles stomach epithelium Junctional: resembles cardiac epithelium Intestinal: glandular l epithelium characterized by the goblet cell
5 Squamocolumnar junction Juxtaposition of pale squamous epithelium and red columnar epithelium Z-line Gastroesophageal junction Esophagus ends and Stomach begins Most proximal part of the gastric folds When Z-line above GE junction = Barrett s
6 1. Spechler SJ. Barrett s Esophagus. N Engl J Med 2002;346(11):
7 Metaplastic process at GE junction Squamous to columnar conversion Exposure to exceed acid Prolapse of esophageal mucosa into gastric milieu Inflammatory changes Loss of muscle function Mechanically defective sphincter Free reflux w/ higher degrees of mucosal injury Acid and Bile reflux
8 Chronic GERD = Barrett s in 5% to 15% pts Unclear: Severe esophagitis w/o BE Relative symptoms with severe dysplasia Genetic predisposition? Barrett s gene remains elusive Hereditary pattern: BE occurs in family ygroups more often Low penetrance (no 1 st degree relative correlation) 1. Csendes A, et al. Prevalence of Barrett s esophagus by endoscopy and histologic studies: a prospective evaluation of 306 control subjects and 376 patients with symptoms of gastroesophageal reflux. Dis Esophagus 2000;13: Romero Y, et al. Barrett s esophagus: prevalence in symptomatic relatives. Am J Gastroenterol 2002;97:
9


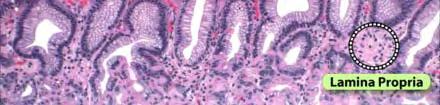



10 Intestinal metaplasia Goblet cells = mucous producing cells Alcian blue stain differentiates from normal stomach tissue



11 15 to 25% if low-grade dysplasia included 5 to 10% if only high-grade h dysplasia Histologic examination 4 categories: No dysplasia Indefinite Low grade dysplasia High grade dysplasia Non-dysplastic: 5 to 10% per year progress to dysplasia 1. Reid et al. Gastroenterology 102:1212, 1992
12 Advanced neoplasia confined to epithelium Limited by basement membrane Not found in lamina propria No regression Precursor and marker for invasive cancer Dx: Esophagoscopy and biopsy Histopathologic Interpretation: Establishing presence of dysplasia Grading dysplastic changes Distinguishing HGD from invasive cancer
13 Reid et al: 5yr probability of cancer 59% if HGD on initial EGD 31% if HGD on surveillance EGD Buttar et al: 3yr probability of cancer 56% if multifocal HGD (> 5 crypts) 14% if focal HGD (< crypts) Cleveland Clinic: Esophagectomy for HGD Invasive cancer present in 45% pts final pathology 1. Reid BJ, et al. Optimizing endoscopic biopsy detection of early cancers in Barrett s high-grade grade dysplasia. Am J Gastroenterol 2000;95: Buttar NS, et al. Extent of high-grade dysplasia in Barrett s esophagus correlates with risk of adenocarcinoma. Gastroenterology 2001;120:
14 Incidence 300% to 500% last 40 yrs 40% in asymptomatic patients (no GERD) Unpredictable Barrett s lifetime Cancer risk as function of duration of Barrett s Annual incidence of malignant transformation 05%to10% 0.5% 1.0% OR 125 x greater than gen. population p




15
16 Remains controversial Inability to predict BE prior to endoscopy Invasiveness & expense of EGD Increasing asymptomatic population Not enough evidence for recommendation Prevention of a very rare malignancy 7,000 EAC cases in US % asymptomatic Age of onset > 70yrs High chance of missed lesions on EGD
17 1. Shaheen N, Ransohoff DF. Gastroesophageal reflux, barrett esophagus, and esophageal cancer: scientific review. JAMA 2002;287:
18 Proposed predictors: Male gender Age > 40 yrs Obesity Heartburn Long duration GERD (> 13 yrs) Early recognition warrants early surveillance Life expectancy of EAC pts: Longer if dx by screening EGD rather than at onset of symptoms Not yet recommended



19 Non-dysplastic & Low grade dysplasia Highly effective Medical & Surgical Rx Medical = Proton Pump Inhibitors 1 st line agents for esophagitis Reduced incidence of dysplasia Surgical = Antireflux surgery Nissen, Dor, Toupet Fundoplications Long term relief of symptoms Regression of dysplasia and intestinal i metaplasia Prevention of HGD and adenocarcinoma
20 1. El Serag HB, et al. Proton pump inhibitors are associated with reduced incidence of dysplasia in Barrett s esophagus. Am J Gastroenterol 2004;99:
21 Hofstetter et al: 85 pts w/be at 5 yrs after surgery 80% asymptomatic and 20% recurrence of reflux 81% normal post-op 24hr ph monitoring DeMeester et al: 37 pts with 73% loss of intestinal metaplasia Gurski et al: 77 surgical pts & 14 medical pts Low grade dysplasia regression: 36.8% and 7% Low grade to non-dysplastic: 68% Eight pts progressed (all with long segment BE) Median time of biopsy proved regression: 18.5 months Regression is dependent on length of BE segment and time of f/u after surgery
22 LOTUS multicenter randomized trial Medical vs Surgical Rx of GERD pts with Barrett s 554 patients with GERD 60 pts with BE (28 to PPI, 32 to LARS) 4 pts with treatment failure Esophageal ph better controlled after LARS No difference in post-operative complications Similar level of symptomatic reflux control Success of LARS is similar in pts w or w/o BE





23 Collis-Belsey procedure Nissen Fundoplication

24 Schnell et al: Endoscopic surveillance q3 months for 1 st year, q6 months 2 nd year, yearly thereafter Mean follow up 7.3 years Only 16% cohort developed cancer



25 1. Schnell TG, et al. Long term non-surgical management of Barrett s esophagus with high-grade dysplasia. Gastroenterology 2001;120(7):
26 1,550 Barrett's patients 7,000 EGDs 46,000 Barrett's specimens read by the same pathologist Intensive endoscopic surveillance with biopsies rather than immediate esophagectomy is the management of choice for patients with flat HGD and no cancer Surgical resection of the esophagus should be reserved only for those patients in whom cancer has been documented
27 Dysplasia Documentation Follow-up None Two EGD w/bx in1 yr Endoscopy q 3 yrs Low Grade High Grade Highest grade Bx within 6 months Expert pathologist Mucosal irregularity Repeat EGD w/ bx within 3 months Expert pathologist 1 yr interval until no dysplasia x 2 Endoscopic resection q 3 month EGD surveillance or intervention based on results and patient 1. Wang KK, Sampliner RE. Updated Guidelines 2008 for the Diagnosis, Surveillance and Therapy of Barrett s Esophagus. Am J Gastroenterol 2008;103:
28 Endoscopic Mucosal Resection Less invasive than esophagectomy Saline lift, snare removal, band tecnique Determines depth of invasion of visible lesion Endoscopic excision of lesions up to 1.5cm Ell et al: 98% survival at 5 yrs Highly selected pts with early EAC Well diff. intramucosal tumors w/o lymph invasion Short-segment Barrett s esophagus 1. Ell C, et al. Curative endoscopic resection of early esophageal adenocarcinomas (Barrett s cancer). Gastrointest Endosc 2007;65:3-10.
29 Endoscopic ablation: Electrocoagulation l Laser Argon-beam coagulation Radiofrequency ablation Photodynamic therapy (PDT) PDT Porfimer sodium Light of specific wavelength (630 nm) Intracellular l reaction leads to cell death Strictures Residual buried Barrett s dysplasia and cancer
30 Remains the standard of care for HGD High volume centers = low mortality Minimally invasive approach Vagal-sparing esophagectomy No vagotomy or pyloroplasty 95% cancer survival at 5 years Early cancers confined to mucosa No need for extensive lymphadenectomy y 1. Peyre C, DeMeester SR, Rizzetto C, et al. Vagal-sparing esophagectomy: the ideal operation for intramucosal adenocarcinoma and Barrett s with high grade dysplasia. Ann Surg 2007;246:
31 1. Rice TW, et al. Refining esoghageal cancer staging. J Thorac Cardiovasc Surg 2003;125:

32 Described by Akiyama et al in Japan Reduced morbidity Dumping syndrome Diarrhea Weight loss Stripping Invagination of muscle Colon interposition 1. DeMeester SR. New Options for the Therapy of Barrett s High Grade Dysplasia and Intramucosal Adenocarcinoma: Endoscopic Mucosal Resection versus Vagal-Sparing Esophagectomy. Ann Thorac Surg2008;85:
33 Das et al: 742 pts 99 pts (13.4%) treated w/emr 643 (86.6%) pts treated w/esophagectomy Stage 0 and Stage 1 esophageal cancer Follow up for 56 and 59 m respectively No statistical significance in 5 yr survival Most EMR pts were stage 0 Esophagectomy pts were stage 1 1. Das A, et al. A Comparison of Endoscopic Treatment t and Surgery in Early Esophageal Cancer: An Analysis of Surveillance Epidemiology and End Results Data. Am J Gastroenterol 2008;103:
34 Barrett s esophagus is as much a surgical as it is a medical disease Early detection is key to success in management Surveillance even after anti-reflux therapy is of utmost importance With new endoscopic advances; careful selection of patients for treatment approach Goal is: Keep Cancer Away
35
36 A 58 y.o. male with history of GERD undergoes EGD with biopsy results of high grade dysplasia. What s the next step in management of this patient? a. Esophagectomy b. Medical trial with PPI s c. Endoscopic Mucosal Resection d. Repeat EGD and biopsy in 3 months Answer: d
37 Intestinal metaplasia is differentiated from gastric metaplasia by presence of: a. Parietal cells b. G cells c. Goblet cells d. Columnar epithelium Answer: c
38 Which of the following statements about Barrett s is NOT true? a. 40% of patients are asymptomatic b. Treatment is directed based on degree of dysplasia c. If dysplastic segment < 3cm, no intervention is necessary d. Severe esophagitis can mask areas with intestinal metaplasia e. 0.5% to 1.0% pts/yr progress to adenocarcinoma Answer: c
39 Which of the following statements about Barrett s is NOT true? a. Most pts who develop carcinoma in Barrett s are men aged 55 to 60 b. Pts with high grade dysplasia should undergo esophagectomy c. Endoscopic surveillance effectively reduces the stage at presentation to stage 2 or lower d. Barrett s occurs in 10% to 15% of pts with GERD e. Low-grade dysplasia should be treated with an antireflux procedure as well as antacids Answer: e
40
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Endoscopic Management of Barrett s Esophagus
 Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Chapter 12: Training in Pathology. DDSEP Chapter 13: Question 19
 DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
The normal esophagus is lined with squamous epithelium.
 .. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
.. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Is Radiofrequency Ablation Effective In Treating Barrett s Esophagus Patients with High-Grade Dysplasia?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of the distal esophagus, gastroesophageal junction and gastric cardia?
 Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia
 ...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Speaker disclosure. Objectives. GERD: Who and When to Treat 7/21/2015
 GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
Barrett's Esophagus: Sorting Out the Controversy
 Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Everything Esophagus: Barrett s Esophagus. Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina
 Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
In 1998, the American College of Gastroenterology issued ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
This medical position statement considers a series of
 GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
What s New in the Management of Esophageal Disease
 What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful in characterizing esophageal location
 Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus. Original Policy Date
 MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
DISCLOSURES. This program meets the requirements for GI specific Category 1 contact hours. M
 DISCLOSURES Educational Dimensions is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center s Commission on Accreditation. Successful completion: Participants
DISCLOSURES Educational Dimensions is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center s Commission on Accreditation. Successful completion: Participants
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Barrett s Esophagus: State of the Art Management
 In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
RFA and Cyrotherapy for Esophageal Disease
 RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
Barrett s Esophagus. lining of the lower esophagus that bears his name (i.e., Barrett's esophagus). We now
. We now") Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Relative risk of dysplasia for patients with intestinal metaplasia in the distal oesophagus and in the gastric cardia
 Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Changes to the diagnosis and management of Barrett s Oesophagus
 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
From reflux to esophageal cancer. Josh Boys, MD TCV 2 nd year indentured servant
 From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
Barrett s Esophagus. Radiofrequency Ablation with the HALO Technology A Reference Book
 Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Medicare Advantage Medical Policy
 Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Slide 1. Slide 2. Slide 3 DISCLOSURES EXPECTED OUTCOMES DIAGNOSIS AND TREATMENT
 Slide 1 DIAGNOSIS AND TREATMENT 1 Slide 2 DISCLOSURES Successful completion: Participants must attend the entire program, including any resulting Q & A, and submit required documentation. Conflict of interest:
Slide 1 DIAGNOSIS AND TREATMENT 1 Slide 2 DISCLOSURES Successful completion: Participants must attend the entire program, including any resulting Q & A, and submit required documentation. Conflict of interest:
The increasing incidence of esophageal adenocarcinoma
 GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
Vital staining and Barrett s esophagus
 Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Adenocarcinoma of the distal esophagus is a recognized
 ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
Barrett s Esophagus: Are We Making any Progress?
 3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus
 Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus Robert J. Korst, MD, a,b Sobeida Santana-Joseph, MSN, a,b John R. Rutledge, MAS,
Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus Robert J. Korst, MD, a,b Sobeida Santana-Joseph, MSN, a,b John R. Rutledge, MAS,
Barrett esophagus. Bible class Inselspital
 Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Chapter 2 Complications of Gastroesophageal Reflux Disease
 Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Section: Medicine Effective Date: July 15, 2015 Subsection: Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: June 2015 Page: 1 of 16 Cryoablation for Barrett s Esophagus Description Barrett s esophagus (BE) is a condition in which the normal squamous epithelium is replaced by specialized
Last Review Status/Date: June 2015 Page: 1 of 16 Cryoablation for Barrett s Esophagus Description Barrett s esophagus (BE) is a condition in which the normal squamous epithelium is replaced by specialized
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Proton Pump Inhibitors Are Associated with Reduced Incidence of Dysplasia in Barrett s Esophagus
 American Journal of Gastroenterology ISSN 0002-9270 C 2004 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2004.30228.x Published by Blackwell Publishing ORIGINAL CONTRIBUTIONS Proton Pump Inhibitors
American Journal of Gastroenterology ISSN 0002-9270 C 2004 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2004.30228.x Published by Blackwell Publishing ORIGINAL CONTRIBUTIONS Proton Pump Inhibitors
Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell
 Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell Department of Internal Medicine 2, HSK Wiesbaden, Wiesbaden, Germany Correspondence to Oliver Pech, MD, PhD, Department of Gastroenterology,
Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell Department of Internal Medicine 2, HSK Wiesbaden, Wiesbaden, Germany Correspondence to Oliver Pech, MD, PhD, Department of Gastroenterology,
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Burning Issues in the Esophagus
 Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Barrett's Esophagus and Indications for Anti-reflux Procedures. Gamal Marey SUNY Downstate Medical Center (RUMC) 7/3/2014
 7/3/2014") Barrett's Esophagus and Indications for Anti-reflux Procedures Gamal Marey SUNY Downstate Medical Center (RUMC) 7/3/2014 History 46 y/o. female, 109 lbs, with PMH significant for long standing acid reflux
Barrett's Esophagus and Indications for Anti-reflux Procedures Gamal Marey SUNY Downstate Medical Center (RUMC) 7/3/2014 History 46 y/o. female, 109 lbs, with PMH significant for long standing acid reflux
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, by Am. Coll. of Gastroenterology ISSN /02/$22.00
 THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
Disclosures. Heartburn and Barrett s Esophagus. Heartburn and Barrett s Esophagus. GERD is common in the U.S. None
 Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Disclosures. Gastroesophageal Reflux Disease. Gastroesophageal Reflux Disease
 Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France
 Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France Barrett s esophagus (BE) is an acquired condition in which the normal squamous epithelium
Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France Barrett s esophagus (BE) is an acquired condition in which the normal squamous epithelium
235 60th Street, West New York, NJ T: (201) F: (201) Main Street, Hackensack, NJ T: (201)
 F: (201) Main Street, Hackensack, NJ T: (201)") 235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Barrett's Esophagus WHAT IS BARRETTT'S ESOPHAGUS? Barrett's esophagus
235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Barrett's Esophagus WHAT IS BARRETTT'S ESOPHAGUS? Barrett's esophagus
4/24/2015. History of Reflux Surgery. Recent Innovations in the Surgical Treatment of Reflux
 Recent Innovations in the Surgical Treatment of Reflux Scott Carpenter, DO, FACOS, FACS Mercy Hospital Ardmore Ardmore, OK History of Reflux Surgery - 18 th century- first use of term heartburn - 1934-
Recent Innovations in the Surgical Treatment of Reflux Scott Carpenter, DO, FACOS, FACS Mercy Hospital Ardmore Ardmore, OK History of Reflux Surgery - 18 th century- first use of term heartburn - 1934-
Accepted Manuscript. CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D
 Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Photodynamic Therapy for High Grade Esophageal Dysplasia. California Technology Assessment Forum
 TITLE: AUTHOR: PUBLISHER NAME: Photodynamic Therapy for High Grade Esophageal Dysplasia Jeffrey A. Tice, M.D. Assistant Adjunct Professor of Medicine Division of General Internal Medicine Department of
TITLE: AUTHOR: PUBLISHER NAME: Photodynamic Therapy for High Grade Esophageal Dysplasia Jeffrey A. Tice, M.D. Assistant Adjunct Professor of Medicine Division of General Internal Medicine Department of
Frozen Section Analysis of Esophageal Endoscopic Mucosal Resection Specimens in the Real-Time Management of Barrett s Esophagus
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:173 178 Frozen Section Analysis of Esophageal Endoscopic Mucosal Resection Specimens in the Real-Time Management of Barrett s Esophagus GANAPATHY A. PRASAD,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:173 178 Frozen Section Analysis of Esophageal Endoscopic Mucosal Resection Specimens in the Real-Time Management of Barrett s Esophagus GANAPATHY A. PRASAD,*
What Is Barrett s Esophagus?
 What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
Occult Esophageal Adenocarcinoma
 ANNALS OF SURGERY Vol. 230, No. 3, 433 440 1999 Lippincott Williams & Wilkins, Inc. Occult Esophageal Adenocarcinoma Extent of Disease and Implications for Effective Therapy John J. Nigro, MD,* Jeffrey
ANNALS OF SURGERY Vol. 230, No. 3, 433 440 1999 Lippincott Williams & Wilkins, Inc. Occult Esophageal Adenocarcinoma Extent of Disease and Implications for Effective Therapy John J. Nigro, MD,* Jeffrey
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Current challenges in Barrett s esophagus
 MEDICAL GRAND ROUNDS TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY Current challenges in Barrett s esophagus GARY W. FALK, MD * Director, Center for Swallowing and Esophageal
MEDICAL GRAND ROUNDS TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY Current challenges in Barrett s esophagus GARY W. FALK, MD * Director, Center for Swallowing and Esophageal
Henry Moon was one of the giants in academic pathology during my early years.
 Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series
 E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Ablation. See specific types, e.g., Thermal ablation Achalasia, 53 75 described, 53 features of, 53 management of past options, 54 POEM
Index Note: Page numbers of article titles are in boldface type. A Ablation. See specific types, e.g., Thermal ablation Achalasia, 53 75 described, 53 features of, 53 management of past options, 54 POEM
National Digestive Diseases Information Clearinghouse
 Barrett s Esophagus National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is Barrett s esophagus? Barrett s esophagus is
Barrett s Esophagus National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is Barrett s esophagus? Barrett s esophagus is
Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease
 Original Article Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease From Military Hospital, Rawalpindi Obaid Ullah Khan, Abdul Rasheed Correspondence: Dr. Abdul
Original Article Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease From Military Hospital, Rawalpindi Obaid Ullah Khan, Abdul Rasheed Correspondence: Dr. Abdul
How to stage early BE cancer - EUS or endoscopic removal?
 How to stage early BE cancer - EUS or endoscopic removal? Presented by Bas Weusten Institution St. Antonius Hospital, Nieuwegein Academic Medical Center, Amsterdam case 56 y old female patient Lung transplant
How to stage early BE cancer - EUS or endoscopic removal? Presented by Bas Weusten Institution St. Antonius Hospital, Nieuwegein Academic Medical Center, Amsterdam case 56 y old female patient Lung transplant
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Treat Barrett s, Remove the Risk. HALO System
 Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
Barrett s esophagus, reflux esophagitis, and eosinophilic esophagitis F. P. Vleggaar, P. D. Siersema Utrecht, the Netherlands
 DDW HIGHLIGHTS F. P. Vleggaar, P. D. Siersema Utrecht, the Netherlands Many new and exciting endoscopy-related studies on Barrett s esophagus, reflux esophagitis, and eosinophilic esophagitis were presented
DDW HIGHLIGHTS F. P. Vleggaar, P. D. Siersema Utrecht, the Netherlands Many new and exciting endoscopy-related studies on Barrett s esophagus, reflux esophagitis, and eosinophilic esophagitis were presented
L was termed Barrett s esophagus (BE) after the
 after the") ORIGINAL ARTICLES Barrett s Esophagus With High-Grade Dysplasia: An Indication for Esophagectomy? Manuel Pera, MD, Victor F. Trastek, MD, Herschel A. Carpenter, MD, Mark S. Allen, MD, Claude Deschamps,
ORIGINAL ARTICLES Barrett s Esophagus With High-Grade Dysplasia: An Indication for Esophagectomy? Manuel Pera, MD, Victor F. Trastek, MD, Herschel A. Carpenter, MD, Mark S. Allen, MD, Claude Deschamps,