Role and Techniques of Surgery in Carcinoma Cervix. Dr Vanita Jain Additional Professor OBGYN PGIMER, Chandigarh
|
|
|
- Kenneth Brown
- 5 years ago
- Views:
Transcription
1 Role and Techniques of Surgery in Carcinoma Cervix Dr Vanita Jain Additional Professor OBGYN PGIMER, Chandigarh




2
3 Points for Discussion Pattern of spread Therapeutic options Types of surgical procedures Stage wise treatment Special situations

4 Carcinoma cervix - Pattern of Spread Grows locally
5 Carcinoma cervix - Pattern of Spread Extends to paracervical tissues &pelvic organs & Spreads to regional lymph nodes

6 Carcinoma cervix - Pattern of Spread Metastasizes to distant structures later
7 Therapeutic modalities Surgery - limited to patients with stage I-IIa disease Radiotherapy - can be used in all stages of disease Chemotherapy Chemoradiation
8 Principles of treatment Both the primary lesion and the potential sites of spread should be evaluated and treated Optimal therapy consists of radiation or surgery ALONE - Morbidity is higher when both are combined Primary therapy should avoid planned use of both surgery & radiation
9 Types of surgical procedures
10 Surgical procedures in Carcinoma Cervix Fertility sparing surgeries Conization Trachelectomy Radical hysterectomy Laparoscopic assisted radical vaginal hysterectomy lymphadenectomy Staging lymphadenectomy Exentration Oophoropexy
11 Conization
12 Conization Removes the cervical lesion, the transformation zone & the endocervical canal in the shape of a cone along with endocervical curettage Is both diagnostic & therapeutic




13



14

15 Conization


16




17
18 Conization Presence of dysplasia either at the endocervical conization margin or in the endocervical curettings is a strong predictor of residual invasive disease Residual invasive disease 4 % when both are negative 33% when both are positive 22 % with positive endocervical conization margin Repeat conization should be performed to exclude more deeply invasive residual disease.
19 Radical trachelectomy
20 Radical trachelectomy The cervix and parametria are resected with placement of a cerclage so that the uterus can be preserved with a competent vaginaluterine junction. Radical trachelectomy can be performed transvaginally or transabdominally with lymphadenectomy.

21 Radical trachelectomy
22 Radical trachelectomy Selection criteria Lesion size < 2 cm Absence of overt LN metastases Absence of vascular / lymphatic space involvement
23 Radical hysterectomy




24
25 Radical hysterectomy Refers to the excision of the uterus en bloc with the parametrium (i.e., round, broad, cardinal, and uterosacral ligaments) and the upper one-third to one-half of the vagina,
26 Radical hysterectomy Inspection of abdomen and pelvis Inspection and palpation of pelvic & para-aortic lymph nodes Any suspicion of disease-frozen section to be done No gross evidence of metastatic disease-surgery begun Metastatic disease identified- abandon surgery
27 Types of radical hysterectomy Piver-Rutledge




28

29 Type I radical hysterectomy Extrafascial hysterectomy. The fascia of the cervix and lower uterine segment, which is rich in lymphatic, is removed with the uterus


30

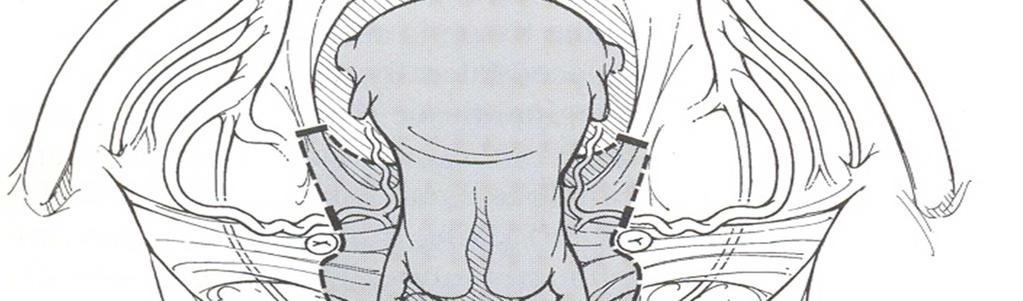
31 Type II radical hysterectomy The uterine artery is ligated where it crosses over the ureter and the uterosacral and cardinal ligaments are divided midway towards their attachment to the sacrum and pelvic sidewall, respectively. The upper onethird of the vagina is resected.
32

33 Type III radical hysterectomy The uterine artery is ligated at its origin from the superior vesical or internal iliac artery. Uterosacral and cardinal ligaments are resected at their attachments to the sacrum and pelvic sidewall. The upper one-half of the vagina is resected.


34
35 Types of radical hysterectomy IV - The ureter is completely dissected from the vesicouterine ligament, the superior vesical artery is sacrificed, and three-fourths of the vagina is resected V - There is additional resection of a portion of the bladder or distal ureter with ureteral reimplantation into the bladder.




36
37 Type II Vs Type III Hysterectomy The therapeutic efficacy of a type II comparable to that of a type III but with lower morbidity The type II operation was associated with Shorter mean operative time Less late urologic morbidity Similar recurrence rates & Cause-specific mortality 5year OS & DFS Type II procedure appears preferable as long as appropriate tumor clearance can be achieved
38 Laparoscopy-assisted radical vaginal hysterectomy (LARVH)
39 Laparoscopy-assisted radical vaginal hysterectomy (LARVH) Procedure : laparoscopic visualization of the abdominal cavity to exclude macroscopic disease Laparoscopic lymphadenectomy Radical vaginal hysterectomy (type II or III) Advantages : Less blood loss Better cosmetic results Faster recovery, Shorter hospitalization Complications Similar to those seen with abdominal surgery
40 Lymphadenectomy
41 Nodal stations First station-parametrial, internal iliac, external iliac, presacral,common iliac Second station- Para-aortic nodes



42

43 Lymphadenectomy


44 Lymphadenectomy
45 Sentinel node biopsy Hypothesis- tumor cells colonize one or a few lymph nodes before involving other nodes & there status accurately predicts the status of the remaining regional LNs. Procedure-Peritumoral injection of Tc-99 and/or a vital blue dye permits identification Reliability for clinical use - not yet established Status - investigational
46 Staging lymphadenectomy
47 Staging lymphadenectomy Aim- To discovers positive lymph nodes as clinical staging is imprecise Clinical stage fails to identify para-aortic involvement Stage 1b - 7 % StageIIb -18% Treatment plan changes in 40%
48 Staging lymphadenectomy Arguments in favor Surgical staging is the most accurate method of determining lymph node involvement. Therapeutic survival benefit of resecting bulky lymph nodes prior to chemo radiation Arguments against Delay in the institution of primary chemoradiotherapy Increased risk of morbidity (especially late bowel obstructions) with the combined modality approach.
49 Staging lymphadenectomy Methods Transperitoneal approach-radiotherapy induced bowel complications 30% Extraperitoneal dissection-postradiotherapy bowel complications-<5% Laparoscopic lymphadenectomy
50 Exenteration
51 Exenteration An ultraradical surgical procedure consisting of an en bloc resection of the female reproductive organs, lower urinary tract, and a portion of the rectosigmoid. Indications Recurrent or advanced gynecologic cancer Extensive central pelvic disease that cannot be resected with a lesser procedure Has received Radiation before Contraindications Presence of distant metastasis - 50% Unresectable or extrapelvic disease % Disease extending to pelvic side walls

52


53
54 LEER Laterally extended endopelvic resection For recurrent disease involving pelvic side walls Extended lateral resection plane Internal iliac vessels, endopelvic part of obturaror internus, coccygeus, iliococcygeus, pubococcygeus are removed Limited experience
55 OOPHOROPEXY
56 OOPHOROPEXY Aim: To shield the normal premenopausal ovary from the damaging effects of radiation Procedure: The ovaries and their vascular supply are brought out of the pelvis and sutured lateral and above the psoas muscle Ovarian failure can result despite oophoropexy because of scatter radiation and surgically induced changes in ovarian blood supply& innervation

57
58 Stagewise Surgical treatment
59 Lymph node metastasis Stage Pelvic LN(%) Para-aortic (%) Ia Ia2 4.8 <1 Ib IIa IIb III IVa 55 40
60 Stage Ia 1 Incidence of pelvic node metastasis - <1% LVSI Risk of nodal metastasis / central pelvic recurrence <3mm invasion & no LVSI lymph node dissection not needed Choices No LVSI Fertility desired - conization Fertility not desired extrafascial hysterectomy Ia 1 cervical adenocarcinoma expert pathological assessment
61 Stage Ia 2 & Ia 1with LVSI Incidence of pelvic node metastasis 3% - 8% lymph node dissection needed Choices lymphadenectomy + Radical hysterectomy (Type II) if fertility not desired Radical trachelectomy if fertility desired
62 Stage Ib1, nonbulky IIa Radical hysterectomy (TypeIII) plus pelvic/paraaortic lymphadenectomy OR Definitive radiation therapy (RT)
63 Surgery Vs RT Surgery Survival 85% 85% Radiation Complication Fistula 1-2 % Fistula 1-5% Vagina Shortened but lengthens Fibrosis Ovaries Conserved Destroyed Chronic effects Bl. Atony 3% Fibrosis 6-8% Mortality 1% 1% applicability < 65yrs,Healthy All patients
64 Stage Ib1, nonbulky IIa The optimal choice depends upon Patient's age Childbearing plans Disease stage Comorbidities Histopathological review Physician and patient preference.
65 Bulky stage Ib & IIa disease Options Primary chemoradiotherapy Post RT hysterctomy PreRT lymphadenectomy? OR Primary radical hysterectomy & lymphadenectomy followed by tailored RT Undiagnosed, coexisting pelvic mass Anatomic alterations making optimal RT difficult
66 Postchemoradiotherapy hysterectomy The rationale Many of the bulky tumors extend laterally beyond the tumoricidal isodose curve of the brachytherapy application They may contain hypoxic central areas, which do not respond well to RT. Indications No consensus Tumor size > 8 cm, A poor response to RT
67 Indications for adjuvant therapy High-risk disease Positive or close resection margins Positive lymph nodes Microscopic parametrial involvement Intermediate-risk disease Large tumor size (>4 cm) [51] Deep cervical stromal invasion (to the middle or deep one-third) Lymphovascular space invasion
68 Recurrent cervical cancer Treatment depends upon Mode of primary therapy Site of recurrence Central pelvic disease-exentration Disease invoving pelvic side walls-leer Small volume disease limited to cervix-type I/II hysterectomy
69 SPECIAL CIRCUMSTANCES Diagnosis and treatment during pregnancy Management of incidentally diagnosed cervical cancer after simple hysterectomy Carcinoma of the cervical stump
70 Diagnosis and treatment during pregnancy Pap +ve for malignancy, Colposcopy & biopsy cannot rule out malignancy A combined procedure of conization and cerclage in second trimester.
71 Treatment during pregnancy Stage I or IIA Early pregnancy - radical hysterectomy and therapeutic lymphadenectomy with the fetus left in-situ unless the patient is unwilling to terminate the pregnancy Pregnancy closer to fetal viability or patient unwilling to lose the baby may continue the pregnancy Caesarean with radical hysterectomy and therapeutic lymphadenectomy
72 Mode of delivery Microinvasive disease Vaginal delivery Evaluate episiotomy site Reevaluation and treatment six weeks postpartum Early lesions A classical cesarean-radical hysterectomy with lymphadenectomy, after fetal pulmonary maturity is established. Larger volume Classical cesarean delivery followed by RT
73 Incidentally diagnosed cancer after a simple hysterectomy Microinvasive disease : No additional therapy Invasive disease with no gross parametrial disease Radical parametrectomy and upper vaginectomy with therapeutic lymphadenectomy or RT Extensive disease: RT
74 Carcinoma of the cervical stump Early stage Radical trachelectomy with upper vaginectomy and therapeutic lymphadenectomy Surgery is preferred over RT because the ability to deliver adequate doses of RT compromised in patients with a short cervical stump Advanced disease - RT
75 Conclusion SURGERY Best role, only option : Preinvasive disease Definite role, alternate option : Early invasive disease Controversial role : Bulky disease Some role, only option : recurrent disease (RT failure)
76 Carcinoma cervix is a preventable disease Prevention is better than cure
77 THANK YOU
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
of surgical management of early invasive cervical cancer chapter Diagnosis and staging Wertheim described the principles
 chapter 14. Surgical management of early invasive cervical cancer CHAPTER 1 Wertheim described the principles of surgical management of invasive cervical cancer more than 100 years ago in his treatise
chapter 14. Surgical management of early invasive cervical cancer CHAPTER 1 Wertheim described the principles of surgical management of invasive cervical cancer more than 100 years ago in his treatise
Ritu Salani, M.D., M.B.A. Assistant Professor, Dept. of Obstetrics & Gynecology Division of Gynecologic Oncology The Ohio State University
 Cervical Cancer Ritu Salani, M.D., M.B.A. Assistant Professor, Dept. of Obstetrics & Gynecology Division of Gynecologic Oncology The Ohio State University Estimated gynecologic cancer cases United States
Cervical Cancer Ritu Salani, M.D., M.B.A. Assistant Professor, Dept. of Obstetrics & Gynecology Division of Gynecologic Oncology The Ohio State University Estimated gynecologic cancer cases United States
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Algorithms for management of Cervical cancer
 Algithms f management of Cervical cancer Algithms f management of cervical cancer are based on existing protocols and guidelines within the ESGO comunity and prepared by ESGO Educational Committe as a
Algithms f management of Cervical cancer Algithms f management of cervical cancer are based on existing protocols and guidelines within the ESGO comunity and prepared by ESGO Educational Committe as a
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
ECC or Margins Positive?
 CLINICAL PRESENTATION This practice algorithm has been specifically developed for M. D. Anderson using a multidisciplinary approach and taking into consideration circumstances particular to M. D. Anderson,
CLINICAL PRESENTATION This practice algorithm has been specifically developed for M. D. Anderson using a multidisciplinary approach and taking into consideration circumstances particular to M. D. Anderson,
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type)
") Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Cervical Cancer: 2018 FIGO Staging
 Cervical Cancer: 2018 FIGO Staging Jonathan S. Berek, MD, MMS Laurie Kraus Lacob Professor Stanford University School of Medicine Director, Stanford Women s Cancer Center Senior Scientific Advisor, Stanford
Cervical Cancer: 2018 FIGO Staging Jonathan S. Berek, MD, MMS Laurie Kraus Lacob Professor Stanford University School of Medicine Director, Stanford Women s Cancer Center Senior Scientific Advisor, Stanford
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
CARCINOMA CERVIX. Dr. PREETHI REDDY. B. M S OBG II yr POST GRADUATE.
 CARCINOMA CERVIX Dr. PREETHI REDDY. B M S OBG II yr POST GRADUATE. Introduction Cervical cancer is the second most common female malignancy worldwide. It is responsible for 4,66,000 deaths annually worldwide
CARCINOMA CERVIX Dr. PREETHI REDDY. B M S OBG II yr POST GRADUATE. Introduction Cervical cancer is the second most common female malignancy worldwide. It is responsible for 4,66,000 deaths annually worldwide
Cervical Cancer Guidelines L and SC Network July Introduction:
 Cervical Cancer Guidelines L and SC Network July 2018 Introduction: There was a total number of 442 cases of cervix cancer diagnosed in Lancashire and South Cumbria Cancer Network in the period 2005 2009
Cervical Cancer Guidelines L and SC Network July 2018 Introduction: There was a total number of 442 cases of cervix cancer diagnosed in Lancashire and South Cumbria Cancer Network in the period 2005 2009
Staging and Treatment Update for Gynecologic Malignancies
 Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
ESGO-ESTRO-ESP Cervical Cancer Clinical Practice Guidelines Management of early stages: algorithms focusing on the histological data
 ESGO-ESTRO-ESP Cervical Cancer Clinical Practice Guidelines Management of early stages: algorithms focusing on the histological data David Cibula Gynecologic Oncology Centre General University Hospital
ESGO-ESTRO-ESP Cervical Cancer Clinical Practice Guidelines Management of early stages: algorithms focusing on the histological data David Cibula Gynecologic Oncology Centre General University Hospital
Coversheet for Network Site Specific Group Agreed Documentation
 Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER
 UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
Role of Surgery in Cervical Cancer & Research Questions
 Role of Surgery in Cervical Cancer & Research Questions Arb-aroon Lertkhachonsuk, M.D., Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand Role of surgery in cervical cancer
Role of Surgery in Cervical Cancer & Research Questions Arb-aroon Lertkhachonsuk, M.D., Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand Role of surgery in cervical cancer
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป
 ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
Endometrial Cancer. Incidence. Types 3/25/2019
 Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
CPC on Cervical Pathology
 CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
Most common cancer Africans & Asians more prone because of poor socioeconomic condition Drastic decline in west as more detection of preinvasive
 CANCER CERVIX Most common cancer Africans & Asians more prone because of poor socioeconomic condition Drastic decline in west as more detection of preinvasive leison by PAP Smears. Etiology: Age - 2 peaks
CANCER CERVIX Most common cancer Africans & Asians more prone because of poor socioeconomic condition Drastic decline in west as more detection of preinvasive leison by PAP Smears. Etiology: Age - 2 peaks
MRI in Cervix and Endometrial Cancer
 28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
Chapter 8 Adenocarcinoma
 Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
MANAGEMENT OF CERVICAL CANCER
 MANAGEMENT OF CERVICAL CANCER Dr. Ujeen Shrestha Malla* and Prof. Dr. Zhang Shui Rong Department of Obstetrics and Gynaecology, Clinical Medical College of Yangtze University, Jingzhou Central Hospital,
MANAGEMENT OF CERVICAL CANCER Dr. Ujeen Shrestha Malla* and Prof. Dr. Zhang Shui Rong Department of Obstetrics and Gynaecology, Clinical Medical College of Yangtze University, Jingzhou Central Hospital,
Vaginal intraepithelial neoplasia
 Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
What We Have Learned from Over 1400 Radical Hysterectomy Operations in Chiang Mai University Hospital
 Thai Journal of Obstetrics and Gynaecology April 2008, Vol. 16, pp. 79-8561-167 SPECIAL ARTICLE What We Have Learned from Over 1400 Radical Hysterectomy Operations in Chiang Mai University Hospital Jatupol
Thai Journal of Obstetrics and Gynaecology April 2008, Vol. 16, pp. 79-8561-167 SPECIAL ARTICLE What We Have Learned from Over 1400 Radical Hysterectomy Operations in Chiang Mai University Hospital Jatupol
Jacqui Morgan March 6, 2019
 Jacqui Morgan March 6, 2019 Case 1 25yo, G2P1 Here for WWE, no problems, healthy, needs refill on OCPs. Pap- Abnormal Glandular Cells-NOS Now What?? Case 1 Colposcopy What findings? Case 1 ECC Cervical
Jacqui Morgan March 6, 2019 Case 1 25yo, G2P1 Here for WWE, no problems, healthy, needs refill on OCPs. Pap- Abnormal Glandular Cells-NOS Now What?? Case 1 Colposcopy What findings? Case 1 ECC Cervical
Uterine Cervix. Protocol applies to all invasive carcinomas of the cervix.
 Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Prognosis and recurrence pattern of patients with cervical carcinoma and pelvic lymph node metastasis
 NJOG 2009 June-July; 4 (1): 19-24 Prognosis and recurrence pattern of patients with cervical carcinoma and pelvic lymph node metastasis Eliza Shrestha 1, Xiong Ying 1,2, Liang Li-Zhi 1,2, Zheng Min 1,2,
NJOG 2009 June-July; 4 (1): 19-24 Prognosis and recurrence pattern of patients with cervical carcinoma and pelvic lymph node metastasis Eliza Shrestha 1, Xiong Ying 1,2, Liang Li-Zhi 1,2, Zheng Min 1,2,
Janjira Petsuksiri, M.D
 GYN malignancies Janjira Petsuksiri, M.D Outlines Cervical cancer Endometrial cancer Ovarian cancer Vaginal cancer Vulva cancer 2 CA Cervix Epidemiology - Second most common female cancer Risk factors
GYN malignancies Janjira Petsuksiri, M.D Outlines Cervical cancer Endometrial cancer Ovarian cancer Vaginal cancer Vulva cancer 2 CA Cervix Epidemiology - Second most common female cancer Risk factors
Staging. Carcinoma confined to the corpus. Carcinoma confined to the endometrium. Less than ½ myometrial invasion. Greater than ½ myometrial invasion
 5 th of June 2009 Background Most common gynaecological carcinoma in developed countries Most cases are post-menopausal Increasing incidence in certain age groups Increasing death rates in the USA 5-year
5 th of June 2009 Background Most common gynaecological carcinoma in developed countries Most cases are post-menopausal Increasing incidence in certain age groups Increasing death rates in the USA 5-year
Adjuvant Therapies in Endometrial Cancer. Emma Hudson
 Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
History and Classification of Radical Hysterectomy. Korea University Jae Yun Song
 History and Classification of Radical Hysterectomy Korea University Jae Yun Song Contents Introduction History of radical hysterectomy Classification of radical hysterectomy Introduction Hysterectomy Hystera
History and Classification of Radical Hysterectomy Korea University Jae Yun Song Contents Introduction History of radical hysterectomy Classification of radical hysterectomy Introduction Hysterectomy Hystera
What Causes Cervical Cancer? Symptoms of Cervical Cancer
 Cervical Health Awareness Month is a chance to raise awareness about how women can protect themselves from HPV (human papillomavirus) and cervical cancer. HPV is a very common infection that spreads through
Cervical Health Awareness Month is a chance to raise awareness about how women can protect themselves from HPV (human papillomavirus) and cervical cancer. HPV is a very common infection that spreads through
Uterus Malignancies /5/15
 Collecting Cancer Data: Uterus 2014-2015 NAACCR Webinar Series February 5, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Uterus 2014-2015 NAACCR Webinar Series February 5, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Invasive Cervical Cancer: Squamous Cell, Adenocarcinoma, Adenosquamous
 Note: If available, clinical trials should be considered as preferred treatment options for eligible patients (www.mdanderson.org/gynonctrials). Other co-morbidities are taken into consideration prior
Note: If available, clinical trials should be considered as preferred treatment options for eligible patients (www.mdanderson.org/gynonctrials). Other co-morbidities are taken into consideration prior
17 th ESO-ESMO Masterclass in clinical Oncology
 17 th ESO-ESMO Masterclass in clinical Oncology Cervical and endometrial Cancer Cristiana Sessa IOSI Bellinzona, Switzerland Berlin, March 28 th, 2018 Presenter Disclosures None Cervical Cancer Estimated
17 th ESO-ESMO Masterclass in clinical Oncology Cervical and endometrial Cancer Cristiana Sessa IOSI Bellinzona, Switzerland Berlin, March 28 th, 2018 Presenter Disclosures None Cervical Cancer Estimated
Cancer of the cervix uteri
 DOI: 10.1002/ijgo.12611 FIGO CANCER REPORT 2018 Cancer of the cervix uteri Neerja Bhatla 1, * Daisuke Aoki 2 Daya Nand Sharma 3 Rengaswamy Sankaranarayanan 4 1 Department of Obstetrics and Gynecology,
DOI: 10.1002/ijgo.12611 FIGO CANCER REPORT 2018 Cancer of the cervix uteri Neerja Bhatla 1, * Daisuke Aoki 2 Daya Nand Sharma 3 Rengaswamy Sankaranarayanan 4 1 Department of Obstetrics and Gynecology,
University of Kentucky. Markey Cancer Center
 University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
Cervical Cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version NCCN.org. Continue
 Version NCCN.org. Continue") NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2015 NCCN.org Continue Version 1.2015, 08/07/14 National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCN
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2015 NCCN.org Continue Version 1.2015, 08/07/14 National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCN
New Cancer Cases By Site Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3%
 Uterine Malignancy New Cancer Cases By Site 2010 Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3% Cancer Deaths By Site 2010 Lung 26% Breast 15% Colo-Rectal 9% Pancreas 7%
Uterine Malignancy New Cancer Cases By Site 2010 Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3% Cancer Deaths By Site 2010 Lung 26% Breast 15% Colo-Rectal 9% Pancreas 7%
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Advanced Pelvic Malignancy: Defining Resectability Be Aggressive. Lloyd A. Mack September 19, 2015
 Advanced Pelvic Malignancy: Defining Resectability Be Aggressive Lloyd A. Mack September 19, 2015 CONFLICT OF INTEREST DECLARATION I have no conflicts of interest Advanced Pelvic Malignancies Locally Advanced
Advanced Pelvic Malignancy: Defining Resectability Be Aggressive Lloyd A. Mack September 19, 2015 CONFLICT OF INTEREST DECLARATION I have no conflicts of interest Advanced Pelvic Malignancies Locally Advanced
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer
 in Cervical Cancer") Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications. Andres A. Roma, MD Cleveland Clinic
 Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
NAACCR Webinar Series /7/17
 COLLECTING CANCER DATA: UTERUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: UTERUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
SLN Mapping in Cervical Cancer. Memorial Sloan Kettering Cancer Center New York, USA
 Lead Grou p Log SLN Mapping in Cervical Cancer Nadeem R. Abu-Rustum, M.D. Memorial Sloan Kettering Cancer Center New York, USA Conflict of Interest Disclosure Nadeem R. Abu-Rustum, M.D. I have no financial
Lead Grou p Log SLN Mapping in Cervical Cancer Nadeem R. Abu-Rustum, M.D. Memorial Sloan Kettering Cancer Center New York, USA Conflict of Interest Disclosure Nadeem R. Abu-Rustum, M.D. I have no financial
Cervix. Lower part of the uterus Connects the body of the uterus to the vagina (birth canal)
") CERVICAL CANCER Cervix Lower part of the uterus Connects the body of the uterus to the vagina (birth canal) Cervical cancer Begins in the lining of the cervix Cells change from normal to pre-cancer (dysplasia)
CERVICAL CANCER Cervix Lower part of the uterus Connects the body of the uterus to the vagina (birth canal) Cervical cancer Begins in the lining of the cervix Cells change from normal to pre-cancer (dysplasia)
Cervixcancer. Vad är aktuellt? Jan Persson. Lund. Docent överläkare Dep of OB&G Skane univ hosp Lund Sweden
 Cervixcancer Copyright Jan Persson Lund Vad är aktuellt? Jan Persson Docent överläkare Dep of OB&G Skane univ hosp Lund Sweden Controversies Preop selection related stage ( stage 1b1>= 2 cm) Neoadjuvant
Cervixcancer Copyright Jan Persson Lund Vad är aktuellt? Jan Persson Docent överläkare Dep of OB&G Skane univ hosp Lund Sweden Controversies Preop selection related stage ( stage 1b1>= 2 cm) Neoadjuvant
ARROCase: Locally Advanced Endometrial Cancer
 ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
Gynecological Cancers
 Gynecological Cancers Outline Ovarian Cancer Uterine (Endometrial) Cancer Cervical Cancer Vulvar Cancer Vaginal Cancer Overian Cancer Ovarian cancer is cancer that forms in the tissue of the ovary and
Gynecological Cancers Outline Ovarian Cancer Uterine (Endometrial) Cancer Cervical Cancer Vulvar Cancer Vaginal Cancer Overian Cancer Ovarian cancer is cancer that forms in the tissue of the ovary and
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES CASE 1: FEMALE REPRODUCTIVE
 Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
Cervical Cancer, Version
 NCCN CLINICAL PRACTICE GUIDELINES IN ONCOLOGY Cervical Cancer, Version 3.2019 Wui-Jin Koh, MD/Chair 1,* ; Nadeem R. Abu-Rustum, MD 2,* ; Sarah Bean, MD 3 ; Kristin Bradley, MD 4 ; Susana M. Campos, MD,
NCCN CLINICAL PRACTICE GUIDELINES IN ONCOLOGY Cervical Cancer, Version 3.2019 Wui-Jin Koh, MD/Chair 1,* ; Nadeem R. Abu-Rustum, MD 2,* ; Sarah Bean, MD 3 ; Kristin Bradley, MD 4 ; Susana M. Campos, MD,
Para-aortic laparoscopic lymph-node dissection for advanced cervical cancers
 Para-aortic laparoscopic lymph-node dissection for advanced cervical cancers P. Mathevet, Hôpital Femme-Mère-Enfant, Bron Lymph-node involvement Is one of the major prognostic factor in gynecologic cancers.
Para-aortic laparoscopic lymph-node dissection for advanced cervical cancers P. Mathevet, Hôpital Femme-Mère-Enfant, Bron Lymph-node involvement Is one of the major prognostic factor in gynecologic cancers.
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
CERVICAL CANCER: A GUIDE FOR PATIENTS
 CERVICAL CANCER: A GUIDE FOR PATIENTS PATIENT INFORMATION BASED ON ESMO CLINICAL PRACTICE GUIDELINES This guide for patients has been prepared by Reliable Cancer Therapies (RCT) as a service to patients,
CERVICAL CANCER: A GUIDE FOR PATIENTS PATIENT INFORMATION BASED ON ESMO CLINICAL PRACTICE GUIDELINES This guide for patients has been prepared by Reliable Cancer Therapies (RCT) as a service to patients,
3/25/2019. Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates
 Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates") J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
Chapter 5 Stage III and IVa disease
 Page 55 Chapter 5 Stage III and IVa disease Overview Concurrent chemoradiotherapy (CCRT) is recommended for stage III and IVa disease. Recommended regimen for the chemotherapy portion generally include
Page 55 Chapter 5 Stage III and IVa disease Overview Concurrent chemoradiotherapy (CCRT) is recommended for stage III and IVa disease. Recommended regimen for the chemotherapy portion generally include
Proposed All Wales Vulval Cancer Guidelines. Dr Amanda Tristram
 Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Open Radical Cystectomy Tips and Tricks in Males and Females
 Open Radical Cystectomy Tips and Tricks in Males and Females Seth P. Lerner, MD, FACS Professor of Urology Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine
Open Radical Cystectomy Tips and Tricks in Males and Females Seth P. Lerner, MD, FACS Professor of Urology Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine
Cervical cancer is a disease in which malignant (cancer) cells form in the tissues of the cervix.
 cells form in the tissues of the cervix.") Cervical Cancer Cervical cancer is a disease in which malignant (cancer) cells form in the tissues of the cervix. The cervix is the lower, narrow end of the uterus (the hollow, pear-shaped organ where
Cervical Cancer Cervical cancer is a disease in which malignant (cancer) cells form in the tissues of the cervix. The cervix is the lower, narrow end of the uterus (the hollow, pear-shaped organ where
Intention-to-Treat Analysis of Radical Trachelectomy for Early-Stage Cervical Cancer With Special Reference to Oncologic Failures
 ORIGINAL STUDY Intention-to-Treat Analysis of Radical Trachelectomy for Early-Stage Cervical Cancer With Special Reference to Oncologic Failures Single-Institutional Experience in Hungary Robert Póka,
ORIGINAL STUDY Intention-to-Treat Analysis of Radical Trachelectomy for Early-Stage Cervical Cancer With Special Reference to Oncologic Failures Single-Institutional Experience in Hungary Robert Póka,
Imaging of endometrial and cervical cancer
 Insights Imaging (2010) 1:309 328 DOI 10.1007/s13244-010-0042-7 REVIEW Imaging of endometrial and cervical cancer Shilpa Patel & Sidath H. Liyanage & Anju Sahdev & Andrea G. Rockall & Rodney H. Reznek
Insights Imaging (2010) 1:309 328 DOI 10.1007/s13244-010-0042-7 REVIEW Imaging of endometrial and cervical cancer Shilpa Patel & Sidath H. Liyanage & Anju Sahdev & Andrea G. Rockall & Rodney H. Reznek
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
2009 USCAP Gyn Pathology Evening Session Case #3. Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA
 2009 USCAP Gyn Pathology Evening Session Case #3 Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA rzaino@psu.edu Clinical history Middle aged woman with an exophytic mass of
2009 USCAP Gyn Pathology Evening Session Case #3 Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA rzaino@psu.edu Clinical history Middle aged woman with an exophytic mass of
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Index. B Bilateral salpingo-oophorectomy (BSO), 69
, 69") A Advanced stage endometrial cancer diagnosis, 92 lymph node metastasis, 92 multivariate analysis, 92 myometrial invasion, 92 prognostic factors FIGO stage, 94 histological grade, 94, 95 histologic cell
A Advanced stage endometrial cancer diagnosis, 92 lymph node metastasis, 92 multivariate analysis, 92 myometrial invasion, 92 prognostic factors FIGO stage, 94 histological grade, 94, 95 histologic cell
Indication for Surgery in Endometrial & Cervical Cancer. everything you need to know in 30 minutes!!! Fabio Landoni, MD Gynecologic Department
 Indication for Surgery in Endometrial & Cervical Cancer everything you need to know in 30 minutes!!! Fabio Landoni, MD Gynecologic Department Risk Factors LVSI Myometrial invasion Nodes grade Adjuvant
Indication for Surgery in Endometrial & Cervical Cancer everything you need to know in 30 minutes!!! Fabio Landoni, MD Gynecologic Department Risk Factors LVSI Myometrial invasion Nodes grade Adjuvant
ENDOMETRIAL CANCER. Endometrial cancer is a great concern in UPDATE. For personal use only. Copyright Dowden Health Media
 For mass reproduction, content licensing and permissions contact Dowden Health Media. UPDATE ENDOMETRIAL CANCER Are lymphadenectomy and external-beam radiotherapy valuable in women who have an endometrial
For mass reproduction, content licensing and permissions contact Dowden Health Media. UPDATE ENDOMETRIAL CANCER Are lymphadenectomy and external-beam radiotherapy valuable in women who have an endometrial
Gynecologic Cancer InterGroup Cervix Cancer Research Network. The SHAPE Trial
 Gynecologic Cancer InterGroup Cervix Cancer Research Network The SHAPE Trial Comparing radical hysterectomy and pelvic node dissection against simple hysterectomy and pelvic node dissection in patients
Gynecologic Cancer InterGroup Cervix Cancer Research Network The SHAPE Trial Comparing radical hysterectomy and pelvic node dissection against simple hysterectomy and pelvic node dissection in patients
Gynecologic Oncologist. Surgery Chemotherapy Radiation Therapy Hormonal Therapy Immunotherapy. Cervical cancer
 Gynecologic Oncology Pre invasive vulvar, vaginal, & cervical disease Vulvar Cervical Endometrial Uterine Sarcoma Fallopian Tube Ovarian GTD Gynecologic Oncologist Surgery Chemotherapy Radiation Therapy
Gynecologic Oncology Pre invasive vulvar, vaginal, & cervical disease Vulvar Cervical Endometrial Uterine Sarcoma Fallopian Tube Ovarian GTD Gynecologic Oncologist Surgery Chemotherapy Radiation Therapy
Case Report Large Conization and Laparoendoscopic Single-Port Pelvic Lymphadenectomy in Early-Stage Cervical Cancer for Fertility Preservation
 Case Reports in Surgery Volume 2013, Article ID 207191, 4 pages http://dx.doi.org/10.1155/2013/207191 Case Report Large Conization and Laparoendoscopic Single-Port Pelvic Lymphadenectomy in Early-Stage
Case Reports in Surgery Volume 2013, Article ID 207191, 4 pages http://dx.doi.org/10.1155/2013/207191 Case Report Large Conization and Laparoendoscopic Single-Port Pelvic Lymphadenectomy in Early-Stage
Uterine Malignancies. Collecting Cancer Data: Uterine Malignancies 10/7/2010. NAACCR Webinar Series 1. Questions. Fabulous Prizes!!!
 Uterine October 7, 2010 NAACCR 2010-2011 Webinar Series Session 1 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes!!! 3 NAACCR 2010-2011 Webinar
Uterine October 7, 2010 NAACCR 2010-2011 Webinar Series Session 1 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes!!! 3 NAACCR 2010-2011 Webinar
Endometrial Cancer. Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines
 Gynecological Cancer Treatment Guidelines") Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines Endometrial Cancer Emad R. Sagr, MBBS, FRCSC Consultant Gynecology Oncology Security forces Hospital, Riyadh Epidemiology
Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines Endometrial Cancer Emad R. Sagr, MBBS, FRCSC Consultant Gynecology Oncology Security forces Hospital, Riyadh Epidemiology
Possibility of less radical treatment for patients with early invasive uterine cervical cancer
 doi:10.1111/jog.12980 J. Obstet. Gynaecol. Res. Vol. 42, No. 7: 876 882, July 2016 Possibility of less radical treatment for patients with early invasive uterine cervical cancer Miseon Kim, Shinichi Ishioka,
doi:10.1111/jog.12980 J. Obstet. Gynaecol. Res. Vol. 42, No. 7: 876 882, July 2016 Possibility of less radical treatment for patients with early invasive uterine cervical cancer Miseon Kim, Shinichi Ishioka,
Michael G. Kelly, MD Gynecologic Oncologist University of Colorado Cancer Center
 Michael G. Kelly, MD Gynecologic Oncologist University of Colorado Cancer Center 50 yo healthy postmenopausal female with BMI = 35 with screening PAP smear = AGUS. What is the next step? (1) Colposcopy
Michael G. Kelly, MD Gynecologic Oncologist University of Colorado Cancer Center 50 yo healthy postmenopausal female with BMI = 35 with screening PAP smear = AGUS. What is the next step? (1) Colposcopy
PORTEC-4. Patient seqnr. Age at inclusion (years) Hospital:
 Hospital:") May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
Evolving Treatment Strategies for Cervical Cancer
 Evolving Treatment Strategies for Cervical Cancer Nadeem Abu-Rustum, MD Memorial Sloan Kettering Cancer Center Evolving Treatment Strategies 1. Surgery 2. Radiation 3. Chemotherapy Incidence of cervix
Evolving Treatment Strategies for Cervical Cancer Nadeem Abu-Rustum, MD Memorial Sloan Kettering Cancer Center Evolving Treatment Strategies 1. Surgery 2. Radiation 3. Chemotherapy Incidence of cervix
Index. B Bladder, injury of, Bowel, injury of, , Brachytherapy, for cervical cancer, 357 Burns, electrosurgical,
 Perioperative Nursing Clinics 1 (2006) 375 379 Index Note: Page numbers of article titles are in boldface type. A Abdominal hysterectomy Acidosis, from insufflation, 323 Active electrode monitoring, in
Perioperative Nursing Clinics 1 (2006) 375 379 Index Note: Page numbers of article titles are in boldface type. A Abdominal hysterectomy Acidosis, from insufflation, 323 Active electrode monitoring, in
Cervical Cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version October 10, 2016 NCCN.org.
 Version October 10, 2016 NCCN.org.") NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2017 October 10, 2016 NCCN.org Continue Version 1.2017, 10/10/16 National Comprehensive Cancer Network, Inc. 2016, All rights
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2017 October 10, 2016 NCCN.org Continue Version 1.2017, 10/10/16 National Comprehensive Cancer Network, Inc. 2016, All rights
2016 Uterine Cancer Annual Report
 2016 Uterine Cancer Annual Report Overview At Carolinas HealthCare System s Levine Cancer Institute, we offer comprehensive care focused on using the latest technology and innovative techniques in the
2016 Uterine Cancer Annual Report Overview At Carolinas HealthCare System s Levine Cancer Institute, we offer comprehensive care focused on using the latest technology and innovative techniques in the
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Fertility-sparing surgery in young patients with cervical cancer
 Fertility-sparing surgery in young patients with cervical cancer Pr Catherine Uzan Chef de service Chirurgie et cancérologie gynécologique et mammaire, Pitié Evaluation BEFORE surgery Cancer: stage, type
Fertility-sparing surgery in young patients with cervical cancer Pr Catherine Uzan Chef de service Chirurgie et cancérologie gynécologique et mammaire, Pitié Evaluation BEFORE surgery Cancer: stage, type
What is Cervical Cancer?
 What is Cervical Cancer? Cervical cancer starts in a woman's cervix, the lower narrow part of the uterus. The uterus holds the growing fetus during pregnancy. The cervix connects the lower part of the
What is Cervical Cancer? Cervical cancer starts in a woman's cervix, the lower narrow part of the uterus. The uterus holds the growing fetus during pregnancy. The cervix connects the lower part of the
MRI for cervical and endometrial cancers. Dr Robert Bleehen Consultant Radiologist Cardiff & Vale UHB
 MRI for cervical and endometrial cancers Dr Robert Bleehen Consultant Radiologist Cardiff & Vale UHB RCR 06(1) RCR 06(1) Technique Pelvic multiphased-array coil Fasting? Buscopan? ABDOMEN!!! Cx:+/- HR
MRI for cervical and endometrial cancers Dr Robert Bleehen Consultant Radiologist Cardiff & Vale UHB RCR 06(1) RCR 06(1) Technique Pelvic multiphased-array coil Fasting? Buscopan? ABDOMEN!!! Cx:+/- HR
The Role of Radiation in the Management of Gynecologic Cancers. Scott Glaser, MD
 The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
 TOC NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level evidence,
TOC NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level evidence,
Management and Care of Women with Invasive Cervical Cancer: American Society of Clinical Oncology Resource-Stratified Clinical Practice Guideline
 Management and Care of Women with Invasive Cervical Cancer: American Society of Clinical Oncology Resource-Stratified Clinical Practice Guideline www.asco.org/rs-cervical-cancer-treatment-guideline Introduction
Management and Care of Women with Invasive Cervical Cancer: American Society of Clinical Oncology Resource-Stratified Clinical Practice Guideline www.asco.org/rs-cervical-cancer-treatment-guideline Introduction
Intra-operative frozen section analysis of common iliac lymph nodes in patients with stage IB1 and IIA1 cervical cancer
 Arch Gynecol Obstet (2012) 285:811 816 DOI 10.1007/s00404-011-2038-z GYNECOLOGIC ONCOLOGY Intra-operative frozen section analysis of common iliac lymph nodes in patients with stage IB1 and IIA1 cervical
Arch Gynecol Obstet (2012) 285:811 816 DOI 10.1007/s00404-011-2038-z GYNECOLOGIC ONCOLOGY Intra-operative frozen section analysis of common iliac lymph nodes in patients with stage IB1 and IIA1 cervical
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer
 THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
GYNECOLOGIC CANCER and RADIATION THERAPY. Jon Anders M.D. Radiation Oncology
 GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
What is endometrial cancer?
 Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Cervical Cancers Treatment Guideline KMHK
 Cervical Cancers Treatment Guideline KMHK 子宮頸癌修訂紀錄 修訂日期修訂內容摘要 修訂頁次 版本 97 年 98 年 99 年 100 年 101 年 102 年 103 年 104 年 子宮頸癌診療指引新制訂新增子宮頸篩檢凖則多科會議討論檢視後未修改多科會議討論檢視後未修改多科會議討論檢視後未修改多科會議討論檢視後未修改 ;stage Ia1 做 simple
Cervical Cancers Treatment Guideline KMHK 子宮頸癌修訂紀錄 修訂日期修訂內容摘要 修訂頁次 版本 97 年 98 年 99 年 100 年 101 年 102 年 103 年 104 年 子宮頸癌診療指引新制訂新增子宮頸篩檢凖則多科會議討論檢視後未修改多科會議討論檢視後未修改多科會議討論檢視後未修改多科會議討論檢視後未修改 ;stage Ia1 做 simple