The pain of it all. Rod MacLeod MNZM. Hibiscus Hospice, Auckland and University of Auckland
|
|
|
- Morris Griffin
- 5 years ago
- Views:
Transcription
1 The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland
2 Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage or describe in terms of such damage or both. (It is a combined sensory, emotional and cognitive phenomenon)
, pain from cancer (maybe not so accepted), pain from chronic illness?")
3 PAIN as an experience According to the person s capacity to control it effectively and to ascribe a meaning to it e.g. pain post-op (accepted), pain from cancer (maybe not so accepted), pain from chronic illness?
4 Concept of pain Nociception can be influenced by nonnociceptive pathophysiologic (e.g. abnormal nervous system processing) or psychological factors It is SUBJECTIVE to the patient (patient is reporting a true experience), even in the absence of an obvious demonstrable origin. Pain is what the patient says it is

5 Acute pain An event which alerts the organism to the presence of harmful stimuli in the internal or external environment Ends predictably May provoke an autonomic response May follow cancer therapy Will follow trauma Incident pain/episodic

6 Chronic pain repetitive stimulus in which there is recurrent and/or progressive tissue injury, e.g. cancer, osteoarthritis chronically painful ; persistent nociceptor activation hard to predict an end often gets worse evokes a different emotional response Often no meaning can be ascribed to it Could it be called acute persisting pain?
7 Aetiology of pain Cancer o nerve root compression o liver capsule pain o bone metastases Caused by treatment o chronic post-operative o peripheral neuropathy following chemotherapy Related to cancer/debility o muscle spasm o pressure areas o herpes zoster o constipation Unrelated concurrent disorders o osteoporosis o angina o arthritis o UTIs
 cortex, hypothalamus: influence of emotions and arousal on patient s pain tolerance")
8 Pain threshold Useful concept in management of pain Encompasses the two models of physiology and psychology Central pathway connections and inhibitory pathways from the pre-frontal (emotional) cortex, hypothalamus: influence of emotions and arousal on patient s pain tolerance threshold

9 Pain threshold Cannot be measured but can be modified o control of other symptoms o good quality sleep o feeling secure o psychological support o explanation o relaxation, massage o diversional activities o reduce anxiety/depression o being at peace
10 Physical Cancer-disease itself Therapy side effects Non cancer pathology Chronic fatigue Insomnia Spiritual Meaning of life Culture Religion/Belief Helplessness Total Pain Social Emotional Anger Anxiety Sadness Loss Fear Disfigurement Relationships Roles Cultural Attitude
11 Pain assessment Why bother with proper pain assessment?
12 Pain assessment Why bother with proper pain assessment? To help with a diagnosis To help with the appropriate treatment/management To assess loss of function caused by the pain and the appropriate measures required to correct this
13 Principles of pain assessment Obtain a detailed history, including pain characteristics, intensity etc Do a psycho-socio-spiritual assessment Do a physical examination Provide a diagnosis Set short term realistic goals (aim to minimise pain) Review regularly
14 SITES SEVERITY NATURE DURATION PERIODICITY PRECIPITANTS RELIEVING FACTORS NUISANCE VALUE SIGNIFICANCE EXAMINATION INVESTIGATION TABULATION/RECORDING REVIEW
15 Pain assessment Associated phenomena sweating, restlessness, vomiting, loss of sensation? Analgesic history what drug, dosage, effect? Enquire about mobility, sleep, ADL, contact with children, social
16 Pain assessment Look out for all pains Ask patient what s/he thinks is the cause of pain, correct misconceptions, explain, reassure. For example - cancer~pain~cancer~death, therefore maybe pain~death Psychological assessment, fears, weakness, anxiety, worry, concerns Spiritual assessment
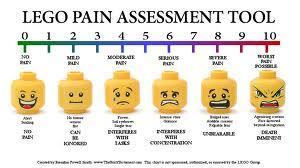
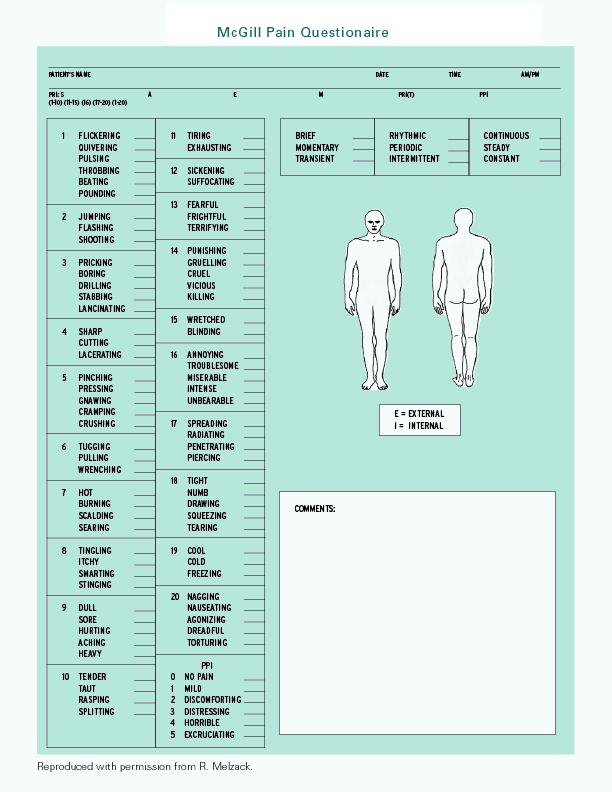
17 Measurement of pain Quantifying the intensity of pain is an essential part of initial and ongoing pain assessment A variety of validated pain scales are available to assist in the measurement of pain Select a method of assessing pain intensity and incorporate it into routine clinical use
18 Pain measurement Uni-dimensional scales verbal rating scale (VRS) numeric rating scale (NRS) visual analogue scale (VAS) The choice of pain scale may depend on the patient's age, ability to communicate, or other specific circumstances
19
20
21
22
23 Pain management - principles Set short term realistic goals, e.g. sleep at night, pain free on movement Includes prevention and prompt response not crises intervention, use as required medications Skillful prescribing tailor-made to patient and cause Keep an open mind; drug and non-drug measures Discuss and explain to patients and families Give support Involve the MDT remember total pain may require total approach Review the outcomes regularly
24 Pain management by the mouth, by the clock, by the ladder (individual) increasing the strength of analgesic following any increase in pain know well the properties of at least one drug at each level balance against distressing side-effects consider other routes of administration consider adjuvant therapy at each stage tailor make according to each patient s response
25 WHO Analgesic Ladder Step 1 Mild Pain Non-opioid Step 2 Moderate Pain Weak opioid +/- non-opioid Step 3 Severe Pain Strong opioid +/- non-opioid Adjuvants including steroids Psychosocial and spiritual aspects Specific therapies
26 Pain in advancing cancer for example ¾ have pain ¼ have no pain 1/5 have one pain 4/5 have two or more pains 1/3 have four or more pains
27 Initiating morphine in opioid naïve patients start with small regular oral (if possible) of immediate release drug titration with slow release morphine is less effective than immediate release and is not recommended prescribe morphine elixir (immediate release) (2.5 to 5 mg) every four hours regularly and titrate
28 Morphine prescribe when/as required doses of 1/5th to 1/6th of the regular 24 hour dose for breakthrough, episodic or incident pain document the amount of morphine taken once a stable dosing regimen is achieved (2 to 3 days) convert to a long-acting preparation calculate the total 24 hour dose of immediate release morphine required from breakthrough and regular dosing, divide by two and give twice daily when required doses of 1/5th to 1/6th of the regular 24 hour dose should be prescribed as immediate release once again for pain between doses
29 Morphine if the patient can no longer swallow give ½ the total 24 hour oral dose by continuous subcutaneous infusion when/as required doses of 1/5th to 1/6th of the regular 24 hour dose should be prescribed once again for pain between doses
30 Opioid rotation opioid rotation (or changing from one opioid to another) is often used when tolerance to the analgesic effects of opioids (stimulation of NMDA receptors) or severe adverse effects occur works because of the difference in the mix of opioid receptors stimulated by each individual opioid in each individual patient most often from morphine to oxycodone, fentanyl or methadone rotation should only occur under supervision and by a specialist as conversion doses are difficult to predict
31 Practice points for morphine No upper dose can be slowly up-titrated until effective dose reached (as long as the pain is opioid sensitive) Always start combination laxative (stool softener plus stimulant) e.g. Movicol etc Nausea and drowsiness are common when starting, but usually settle within one week. Warn about driving
32 Oxycodone and hydromorphone better oral availability than morphine alternative to morphine also indicated if patient experiences side effects with morphine: sedation delirium hallucinations nausea and/or vomiting pruritis
33 Oxycodone and hydromorphone Plasma concentrations increase with renal failure (by about 50%) Half life prolonged by about 1 hour in renal impairment Safer to use in renal impairment than morphine, but dose might need reducing in renal impairment. Avoid in severe impairment
34 Fentanyl transcutaneous patch Indications Side effects from morphine (laxative dose can be halved once starting on fentanyl) Renal failure Poor compliance with oral medications or aversion to tablets Dysphagia
35 Methadone longer half-life than morphine and complex pharmacokinetics. Dose conversions are complex and the response is variable seek specialist help Pethidine has short duration of action (2-3 hrs) no place in palliative care
36 Barriers to pain assessment and adequate management Patient related Reluctance to report pain Reluctance to follow treatment recommendations Fear of tolerance and addiction Concern about side-effects Belief that pain is an inevitable consequence and must be accepted Fear of disease progression Fear of injections
37 Barriers to pain assessment and adequate management Professional-related Failure to evaluate and appreciate the severity of the pain problem Poor assessment of pain Knowledge deficits in cancer pain assessment and treatment and lack of perception thereof Misconceptions re drug side-effects, drug combinations, tolerance, addiction.
38 Barriers to pain assessment and adequate management Institutional-related Lack of a language of pain Failure to use validated pain measurement tools in clinical practice Lack of time committed to pain as a priority Lack of economic resources committed to its treatment Serious legal restrictions to drug prescribing and availability
39 Weak opioids Tramadol in pain associated with cancer, morphine is more effective than tramadol oral tramadol is 5 times weaker than oral morphine. many side effects often not any advantage in using it
40 Weak opioids Codeine/dihydrocodeine 10 times weaker then morphine Metabolised to morphine (10%) 5-10% Caucasians may be unable to metabolise to morphine Combination with other opioids is illogical Once maximum codeine dose reached (240mg/24 hours) start patient on recommended morphine dose (2.5 5mg every four hours)
41 Common symptoms to look for Gastrointestinal system Nausea/vomiting Constipation Diarrhoea Intestinal obstruction Mouth care Taste alteration/dry mouth Central nervous system Depression Delirium Disorders of sleep and wakefulness Anxiety/fear Respiratory system Dyspnoea (breathlessness) Cough Hiccup Excessive (retained) secretions Haemoptysis Itch (pruritus) Sweating Terminal restlessness
42 Questions?
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
May 2015 Clinical Nurse Educator Arohanui Hospice
 May 2015 Clinical Nurse Educator Arohanui Hospice End of Life Care, what s on top? Feedback from last session (Physiology of Dying) Volunteer to present at August meeting Presentation: Breaking Bad News
May 2015 Clinical Nurse Educator Arohanui Hospice End of Life Care, what s on top? Feedback from last session (Physiology of Dying) Volunteer to present at August meeting Presentation: Breaking Bad News
Acute Pain NETP: SEPTEMBER 2013 COHORT
 Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
Narcotic Analgesics. Jacqueline Morgan March 22, 2017
 Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Analgesia. This is widely used in palliative care. It has antipyretic and analgesic effects but no anti-
 Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Opioid rotation or switching may be considered if a patient obtains pain relief with one opioid and is suffering severe adverse effects.
 Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Managing Care at End of Life:
 Managing Care at End of Life: Physical Suffering Pain & Dyspnea Verna Sellers, MD, MPH, AGSF Medical Director Centra PACE Lynchburg, Virginia 1 Speaker Disclosures: Dr. Sellers has disclosed that she has
Managing Care at End of Life: Physical Suffering Pain & Dyspnea Verna Sellers, MD, MPH, AGSF Medical Director Centra PACE Lynchburg, Virginia 1 Speaker Disclosures: Dr. Sellers has disclosed that she has
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
10/08/59 PAIN IS THE MOST COMMON TREATABLE SYMPTOM OF CANCER CURRENT EVIDENCE BASED CONCEPTS: MANAGEMENT OF CANCER PAIN PAIN AN UNMET CLINICAL NEED IN
 Pain is a frequent complication of cancer, and is common in many other life-limiting illnesses MANAGEMENT OF CANCER PAIN A/Prof Ghauri Aggarwal FRACP, FAChPM, FFPMANZCA Palliative Medicine Physician Sydney
Pain is a frequent complication of cancer, and is common in many other life-limiting illnesses MANAGEMENT OF CANCER PAIN A/Prof Ghauri Aggarwal FRACP, FAChPM, FFPMANZCA Palliative Medicine Physician Sydney
Complicated pain. Dr Stephanie Lippett
 Complicated pain Dr Stephanie Lippett UK incidence & prevalence of cancer pain 1% of UK population are living with cancer at present 70% of cancer patients experience pain 70-90% of patients with advanced
Complicated pain Dr Stephanie Lippett UK incidence & prevalence of cancer pain 1% of UK population are living with cancer at present 70% of cancer patients experience pain 70-90% of patients with advanced
Regional Renal Training
 Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Pain management in palliative care. Dr. Stepanie Lippett and Sister Karen Davies-Linihan
 Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain management in Paediatric Palliative Care. Dr Jane Nakawesi 14 th August 2017
 Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
Pain Management in Older Adults. Mary Shelkey, PhD, ARNP
 Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative care for heart failure patients. Susan Addie
 Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
PAIN MANAGEMENT & MAXIMIZING QUALITY OF LIFE DURING TREATMENT
 PAIN MANAGEMENT & MAXIMIZING QUALITY OF LIFE DURING TREATMENT Brandy Ficek, MD Medical Director of Quality of Life and Palliative Medicine Cancer Treatment Centers of America Rocky Mountain Blood Cancer
PAIN MANAGEMENT & MAXIMIZING QUALITY OF LIFE DURING TREATMENT Brandy Ficek, MD Medical Director of Quality of Life and Palliative Medicine Cancer Treatment Centers of America Rocky Mountain Blood Cancer
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults
 SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
Best Practice Statement ~ November The management of pain in patients with cancer
 Best Practice Statement ~ November 2009 The management of pain in patients with cancer NHS Quality Improvement Scotland is committed to equality and diversity. We have assessed this Best Practice Statement
Best Practice Statement ~ November 2009 The management of pain in patients with cancer NHS Quality Improvement Scotland is committed to equality and diversity. We have assessed this Best Practice Statement
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Facts About Morphine and Other Opioid Medicines In Palliative Care. Find out more at: palliativecare.my. Prepared by: Printing sponsored by:
 Facts About Morphine and Other Opioid Medicines In Palliative Care Find out more at: palliativecare.my Prepared by: Printing sponsored by: What is this brochure about? Opioid medicines are pain relievers.
Facts About Morphine and Other Opioid Medicines In Palliative Care Find out more at: palliativecare.my Prepared by: Printing sponsored by: What is this brochure about? Opioid medicines are pain relievers.
Understanding pain in 5 minutes
 Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Pain -Measurement. Dr Thiru Thirukkumaran
 Pain -Measurement Dr Thiru Thirukkumaran Palliative Care Physician (CMO), Northwest Palliative Care Services, Burnie, Tasmania. Senior Lecturer in Palliative Medicine Rural Clinical School - Burnie, University
Pain -Measurement Dr Thiru Thirukkumaran Palliative Care Physician (CMO), Northwest Palliative Care Services, Burnie, Tasmania. Senior Lecturer in Palliative Medicine Rural Clinical School - Burnie, University
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Overview of Pain Types and Prevalence
 Pain Resource Nurse Overview of Pain Types and Prevalence Pain Resource Nurse Program Module 1 The Resource Center of the Alliance of State Pain Initiatives University of Wisconsin Board of Regents, 2011
Pain Resource Nurse Overview of Pain Types and Prevalence Pain Resource Nurse Program Module 1 The Resource Center of the Alliance of State Pain Initiatives University of Wisconsin Board of Regents, 2011
Foundations of Palliative Care Series
 Foundations of Palliative Care Series Developed by: Tim Sakaluk MD, Ingrid See CPL, Tammy Dyson SW, Sharon Salomons SCP!!!!!! This course was developed in collaboration with the UBC Learning Circle to
Foundations of Palliative Care Series Developed by: Tim Sakaluk MD, Ingrid See CPL, Tammy Dyson SW, Sharon Salomons SCP!!!!!! This course was developed in collaboration with the UBC Learning Circle to
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline
 GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management
 Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Doncaster & Bassetlaw Cancer Locality. Palliative Care Core Formulary
 Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Syringe driver in Palliative Care
 Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Pain. Christine Illingworth. Community Nurse St Luke s Hospice 17/5/17
 Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY
 GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
Pain Assessment & Management. For General Nursing Orientation
 Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
PAIN TERMINOLOGY TABLE
 PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
Strong opioids for palliative care patients
 Other formats Strong opioids for palliative care patients If you need this information in another format such as audio tape or computer disk, Braille, large print, high contrast, British Sign Language
Other formats Strong opioids for palliative care patients If you need this information in another format such as audio tape or computer disk, Braille, large print, high contrast, British Sign Language
The Mid Yorkshire Macmillan Specialist Palliative Care Team
 The Mid Yorkshire Macmillan Specialist Palliative Care Team Morphine and Strong Opioid information leaflet Information for patients/carers The mere mention of Morphine can be enough to conjure up all sorts
The Mid Yorkshire Macmillan Specialist Palliative Care Team Morphine and Strong Opioid information leaflet Information for patients/carers The mere mention of Morphine can be enough to conjure up all sorts
Opioid Type Pain Killers
 Opioid Type Pain Killers Information for patients, relatives and carers For more information, please contact: Palliative Care Team 01904 725835 (York) 01723 342446 (Scarborough) Renal Department 01904
Opioid Type Pain Killers Information for patients, relatives and carers For more information, please contact: Palliative Care Team 01904 725835 (York) 01723 342446 (Scarborough) Renal Department 01904
Pain Management During Endof-life
 Pain Management During Endof-life The more that we understand about how pain works and how to relieve this suffering, the gentler and easier we can make end-of-life for patients who are suffering from
Pain Management During Endof-life The more that we understand about how pain works and how to relieve this suffering, the gentler and easier we can make end-of-life for patients who are suffering from
Q&A: Opioid Prescribing for Chronic Non-Malignant Pain
 NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
Pain Management in the Elderly. Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN
 Pain Management in the Elderly Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN Objectives So How Much Do You Really Know? www.geriatricpain.org Geriatric Pain Knowledge Assessment The Geriatric
Pain Management in the Elderly Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN Objectives So How Much Do You Really Know? www.geriatricpain.org Geriatric Pain Knowledge Assessment The Geriatric
Enhanced Community Palliative Support Services. Lynne Ghasemi St Luke s Hospice
 Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
Using strong opiods for pain in palliative care
 Using strong opiods for pain in palliative care What are strong opioids? They are strong medicines used to control pain when weaker painkillers have not been effective. (They can also sometimes be used
Using strong opiods for pain in palliative care What are strong opioids? They are strong medicines used to control pain when weaker painkillers have not been effective. (They can also sometimes be used
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
A PATIENT GUIDE FOR MANAGING PAIN
 A PATIENT GUIDE FOR MANAGING PAIN PAIN MANAGEMENT Knowing the Facts Pain can be controlled. Pain is common after surgery and with many types of illnesses. Most patients with acute and chronic pain can
A PATIENT GUIDE FOR MANAGING PAIN PAIN MANAGEMENT Knowing the Facts Pain can be controlled. Pain is common after surgery and with many types of illnesses. Most patients with acute and chronic pain can
Medications for the Treatment of Neuropathic Pain
 Medications for the Treatment of Neuropathic Pain February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation Neuropathic Pain Pain, paresthesias, and sensory
Medications for the Treatment of Neuropathic Pain February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation Neuropathic Pain Pain, paresthesias, and sensory
sensory nerves, motor nerves, autonomic nerves
 damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic: long term, begins subtly
damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic: long term, begins subtly
Non Malignant Pain: Symptom Management
 Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
21 st June BDS BASHD Therapeutics Pain and Analgesia. BASHD Therapeutics Analgesics and Pain Management. Links to other BASHD content
 Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
Pain---how common is it? Easing the Pain Approaches to Managing Pain Associated with Serious Illness. Definitions
 Easing the Pain Approaches to Managing Pain Associated with Serious Illness Christine S.Ritchie, MD, MSPH, FACP, FAAHPM Harris Fishbon Distinguished Professor Courtesy J Kutner 2 Definitions Acute pain:
Easing the Pain Approaches to Managing Pain Associated with Serious Illness Christine S.Ritchie, MD, MSPH, FACP, FAAHPM Harris Fishbon Distinguished Professor Courtesy J Kutner 2 Definitions Acute pain:
MND Just in Case kit Information for GPs
 MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
Conservative Management of Uraemia
 Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Pain. Fears and Facts. What is pain? Factors that Affect People with Pain. Symptom Management
 Symptom Management Pain Pain is an unpleasant physical or emotional experience. While not all cancer patients will experience pain, approximately two thirds of patients will have pain at some point during
Symptom Management Pain Pain is an unpleasant physical or emotional experience. While not all cancer patients will experience pain, approximately two thirds of patients will have pain at some point during
Pain Control After Surgery. Patient Information
 Pain Control After Surgery Patient Information What is Pain? Pain is an uncomfortable feeling that tells you something may be wrong in your body. Pain is your body s way of sending a warning to your brain.
Pain Control After Surgery Patient Information What is Pain? Pain is an uncomfortable feeling that tells you something may be wrong in your body. Pain is your body s way of sending a warning to your brain.
"Opium teaches only one thing, which is; that aside from physical suffering there is nothing real." André Malraux MAN'S FATE
 "Opium teaches only one thing, which is; that aside from physical suffering there is nothing real." André Malraux MAN'S FATE Pain Management in the Older Adult 5 TH VITAL SIGN Pain is a common problem
"Opium teaches only one thing, which is; that aside from physical suffering there is nothing real." André Malraux MAN'S FATE Pain Management in the Older Adult 5 TH VITAL SIGN Pain is a common problem
PAIN MANAGEMENT IN UROLOGY
 24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
Fact Sheet. Zohydro ER (hydrocodone bitartrate) Extended-Release Capsules, CII
 Extended-Release Capsules, CII") Zohydro ER (hydrocodone bitartrate) Extended-Release Capsules, CII Fact Sheet Zohydro ER (hydrocodone bitartrate) Extended-Release Capsule, CII, is a long-acting (extendedrelease) type of pain medication
Zohydro ER (hydrocodone bitartrate) Extended-Release Capsules, CII Fact Sheet Zohydro ER (hydrocodone bitartrate) Extended-Release Capsule, CII, is a long-acting (extendedrelease) type of pain medication
Cancer Pain. Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center
 Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Cancer Pain: A Clinical Overview. Linda A. King, MD Section of Palliative Care and Medical Ethics
 Cancer Pain: A Clinical Overview Linda A. King, MD Section of Palliative Care and Medical Ethics Objectives Define Palliative Care Review prevalence of cancer pain Know barriers to cancer pain management
Cancer Pain: A Clinical Overview Linda A. King, MD Section of Palliative Care and Medical Ethics Objectives Define Palliative Care Review prevalence of cancer pain Know barriers to cancer pain management
Slow Release Opioids. Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For the Treatment of Pain
 Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For the Treatment of Pain") NHS Greater Glasgow And Clyde Pain Management Service Information for Adult Patients who are Prescribed Slow Release Opioids Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For
NHS Greater Glasgow And Clyde Pain Management Service Information for Adult Patients who are Prescribed Slow Release Opioids Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
Approach to symptom control near the end-of-life
 Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Opioids in Palliative Care
 Opioids in Palliative Care Brooke Building Palliative Care Team 0161 206 4609 All Rights Reserved 2017. Document for issue as handout. What are strong opioids? Strong opioids are painkillers which are
Opioids in Palliative Care Brooke Building Palliative Care Team 0161 206 4609 All Rights Reserved 2017. Document for issue as handout. What are strong opioids? Strong opioids are painkillers which are
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly
 Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Blueprint for Prescriber Continuing Education Program
 CDER Final 10/25/11 Blueprint for Prescriber Continuing Education Program I. Introduction: Why Prescriber Education is Important Health care professionals who prescribe extended-release (ER) and long-acting
CDER Final 10/25/11 Blueprint for Prescriber Continuing Education Program I. Introduction: Why Prescriber Education is Important Health care professionals who prescribe extended-release (ER) and long-acting
NHS Grampian Protocol For The Prescribing And Administration Of Oral Opioids Following Trauma Or Surgery in Adults. Consultation Group: See Page 5
 NHS...... Grampian Acute Sector NHS Grampian Protocol For The Prescribing And Administration Of Oral Opioids Following Trauma Or Surgery in Adults Co-ordinators: Consultant Anaesthetist, Lead Acute Pain
NHS...... Grampian Acute Sector NHS Grampian Protocol For The Prescribing And Administration Of Oral Opioids Following Trauma Or Surgery in Adults Co-ordinators: Consultant Anaesthetist, Lead Acute Pain
Sharon A Stephen, PhD, ARNP, ACHPN. September 23, 2014
 Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Pain. November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine
 Internal Medicine, Palliative Medicine") Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital.
 Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Foundations of Safe and Effective Pain Management
 Foundations of Safe and Effective Pain Management Evidence-based Education for Nurses, 2018 Module 1: The Multi-dimensional Nature of Pain Module 2: Pain Assessment and Documentation Module 3: Management
Foundations of Safe and Effective Pain Management Evidence-based Education for Nurses, 2018 Module 1: The Multi-dimensional Nature of Pain Module 2: Pain Assessment and Documentation Module 3: Management
PAIN MANAGEMENT IN CHILDREN
 SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 PAIN MANAGEMENT IN CHILDREN Aziza Shad, MD Ellen Wasserman Chair of Pediatrics Chief, Division of Pediatric Hematology
SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 PAIN MANAGEMENT IN CHILDREN Aziza Shad, MD Ellen Wasserman Chair of Pediatrics Chief, Division of Pediatric Hematology
I. Chronic Pain Information Page 2-3. II. The Role of the Primary Care Physician in Chronic Pain Management Page 3-4
 SUTTER MEDICAL FOUNDATION (SMF) 2750 GATEWAY OAKS DRIVE, #150 SACRAMENTO, CA 95833 SPA PCP Treatment & Referral Guidelines PAIN MANAGEMENT Developed June 1, 2003 Revised (Format Revisions) November 13,
SUTTER MEDICAL FOUNDATION (SMF) 2750 GATEWAY OAKS DRIVE, #150 SACRAMENTO, CA 95833 SPA PCP Treatment & Referral Guidelines PAIN MANAGEMENT Developed June 1, 2003 Revised (Format Revisions) November 13,
Neuropathic Pain in Palliative Care
 Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN
 Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN Oncology Clinical Nurse Specialist, Senior Research Specialist City of Hope Definition of Pain Pain is an unpleasant sensory and emotional
Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN Oncology Clinical Nurse Specialist, Senior Research Specialist City of Hope Definition of Pain Pain is an unpleasant sensory and emotional
Pain in dementia. Prof Rowan Harwood Geriatrician, NUH. Disclaimer
 Pain in dementia Prof Rowan Harwood Geriatrician, NUH Disclaimer Pain What is pain? Pain Pain is what the patient says it is McCaffery 1968 Pain An unpleasant sensory or emotional experience associated
Pain in dementia Prof Rowan Harwood Geriatrician, NUH Disclaimer Pain What is pain? Pain Pain is what the patient says it is McCaffery 1968 Pain An unpleasant sensory or emotional experience associated
INFORMATION FOR PATIENTS. Let s Manage Pain
 INFORMATION FOR PATIENTS Let s Manage Pain 1 About this booklet Persistent pain, also called chronic pain, is pain which continues for longer than expected. Pain can affect all areas of your life. People
INFORMATION FOR PATIENTS Let s Manage Pain 1 About this booklet Persistent pain, also called chronic pain, is pain which continues for longer than expected. Pain can affect all areas of your life. People
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04
 Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
Morphine and strong opioid information
 Morphine and strong opioid information MY Medicines Helpline: 01924 541398 Monday to Friday 9am to 5pm Use this space for patient ID label Name: DOB: NHS Number: Hospital Number: The mere mention of Morphine
Morphine and strong opioid information MY Medicines Helpline: 01924 541398 Monday to Friday 9am to 5pm Use this space for patient ID label Name: DOB: NHS Number: Hospital Number: The mere mention of Morphine
Peripheral neuropathy (PN)
") Peripheral neuropathy (PN) damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic:
Peripheral neuropathy (PN) damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic: