Method Hannah Shotton
|
|
|
- Jonas Bryant
- 5 years ago
- Views:
Transcription
1 #asah

2 Method Hannah Shotton 2
3 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management 3
4 Introduction Previous work has focused on patients in NSC This study to examine entire acute pathway Presentation to discharge in secondary/acute and tertiary care Patients managed conservatively Patients undergoing active intervention 4
5 Introduction Expert Group: Neurosurgery Neuroradiology Neurology Stroke medicine Acute medicine Neurocritical care and anaesthesia Neuroscience nursing Lay representative 5
6 Aim To explore remediable factors in the process of care of patients admitted with the diagnosis of aneurysmal subarachnoid haemorrhage, looking at patients that underwent open surgery, interventional radiology and those managed conservatively 6
7 Objectives To assess the organisational structures and policies for: Diagnosis Decision making Definitive treatment Post treatment care Rehabilitation 7
8 Objectives To explore remediable factors in care of asah patients including: Initial assessment Admission process Diagnosis Decision making Treatment Rehabilitation 8
9 Hospital Participation Acute hospitals in England, Wales, Northern Ireland and the offshore islands 27 Neurosurgical & Neuroscience centres (NSCs) Organisational questionnaire Local Reporters, ambassadors, clinical lead 9
10 Study Population Adults presenting to secondary or tertiary care after suffering an asah Data collection period: 1 st July th September
11 Identification of Patients ICD10 code for SAH from hospital records Spreadsheet data Patients transferred between hospitals: data linked on NHS number & DoB 11
12 Data Collection Clinician questionnaires Responsible consultant in secondary or tertiary care Non-aneurysmal SAH excluded Maximum 4 cases/ consultant Case note extracts Secondary and tertiary care Initial presentation to discharge 12
13 Data Collection Peer review Multidisciplinary Advisor group Case notes plus questionnaires: secondary only, tertiary only, linked secondary/tertiary Opinion on quality of care Advisor assessment form 13
14 Data Collection Good Practice Room for improvement in clinical aspects of care Room for improvement in organisational aspects of care Room for improvement in BOTH clinical and organisational aspects of care Less than satisfactory 14

15 Case Inclusion 15

16 Data Returns 16
17 Organisational Data Alex Goodwin 17

18 Hospital Returns Table
19 Clinical Networks Formal 11.9% Informal 86.5% 19
20 Availability of Investigations Figure
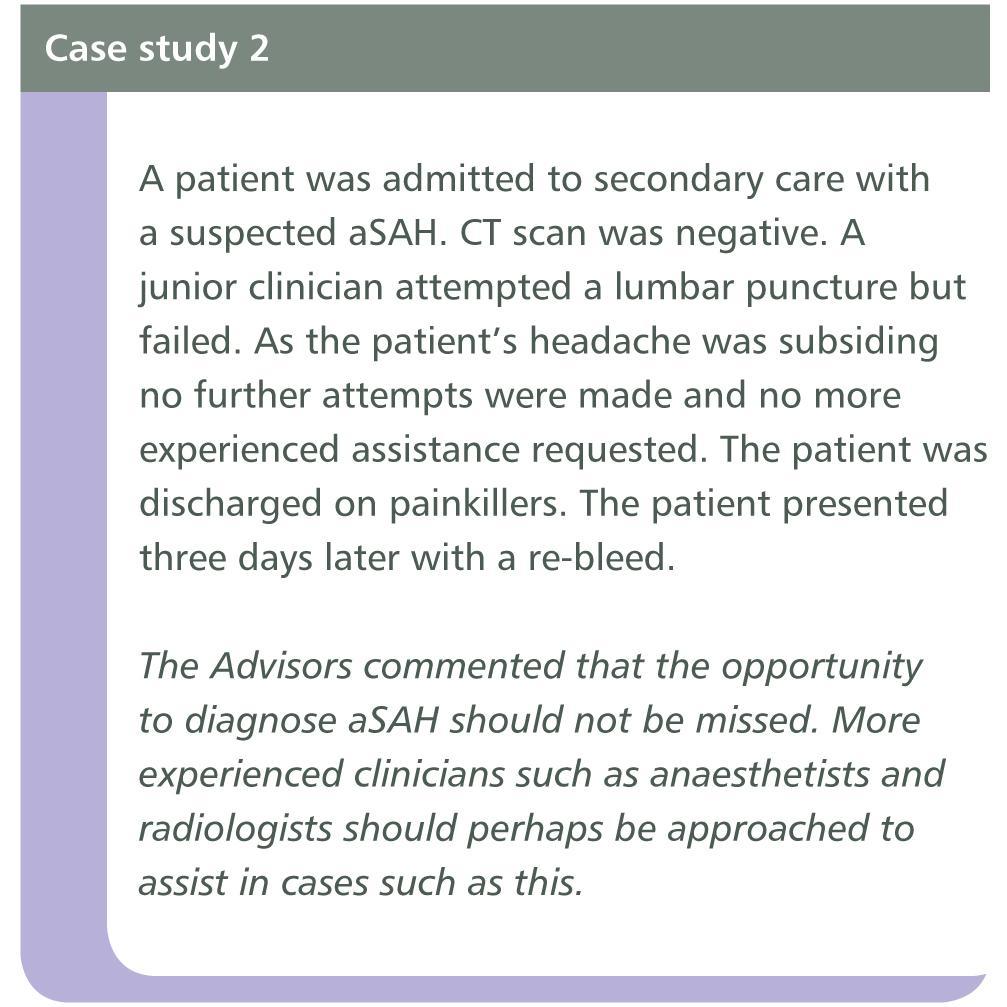
21 Lumbar Puncture 5.4% Unable to perform LP 25% Unable to perform LP 24/7 75% had no guidance as to who should perform LP 21
22 22
23 Secondary Care - Protocols Management of Acute 68% Severe Headache asah Management 72.4% 23

24 asah Management Protocol Includes Table
25 Average Journey Time to Nearest NSC Figure
26 Guidelines for Identifying Those for Conservative Management Only in 11.5% of hospitals Reasons for conservative management Suitability for intervention Co-morbidities Conscious state Age Pre-morbid independence & cognitive state Severity of bleed 26

27 Post-Procedure Support Available in Secondary Care Table

28 Governance - Regional Audit Table

29 Governance - Local Audit, M&M Table

30 Timing of Intervention Good Grade Table

31 Timing of Intervention Poor Grade Table

32 Availability of Staff Figure
")
33 In-patient Rehabilitation (NSC) Table
 Table")
34 Services Available Post-Discharge (NSC) Table
35 Organisational Data Key Findings in Secondary Care 32% had no protocol for managing headache 29% used WFNS grading 85% within 50 miles / 1 hour of NSC 70% had no formal transfer protocol 35
36 Organisational Data Key Findings in Tertiary Care 22/27 (81%) NSCs did not have a policy for optimal timing of definitive care 20/27 NSCs (75%) had no policy for preoperative care of asah 17/27 (63%) NSCs lacked interventional radiology services 7 days a week 36
37 Organisational Data Key Findings in Both Secondary & Tertiary Care 88% not part of formal network 25% of hospitals were unable to perform LPs 24/7 75% lacked policies for the performance of LPs 80% failed to participate in regional audit 40% of secondary hospitals offered neuropsychological support compared to 20/27 (75%) of NSCs 37
38 Organisational Data Recommendations Establish formal networks of care linking secondary and tertiary care Regional audit and MDT meetings should take place in all hospitals Availability of interventional neuroradiology should allow compliance with treating patients within 48 hours of onset 38
39 Secondary Care 39

40 Demographics - Age Table
41 First Presentation to Hospital Secondary care 82.4% Hospital with onsite NSC 17.6% 41

42 Day of Presentation Table

43 Time of Arrival Table
44 Initial Assessment Grade of Clinician Figure

45 Pre-morbid Functional Status 40% with Hypertension Table
46 GCS at First Assessment Figure

47 CT Scan - Timing Table

48 CT Scan - Delays Table
49 49

50 Appropriately Timed Diagnosis Table
51 Delayed or Overlooked Diagnosis (Advisors Form) Primary Care 17.6% of patients saw GP Delayed or overlooked in 32/75 Outcome affected in 23/32 Secondary Care Delay or overlooked in 12% Outcome affected in 10/49 Table
52 52
53 53

54 asah Management in Secondary Care - Nimodipine Table

55 Delays in Referral Process Table
56 Delayed Acceptance by NSC Lack of beds 13 Staffing issue 6 Other 17 Total 36 56
57 Delay in Transfer Delay in 17.9% Deterioration during delayed transfer 10/47 57

58 Conservative Management Table

59 Conservative Management Table

60 Conservative Management Table
61 Quality of Care in Secondary Care Figure

62 Quality of Care in Secondary Care Table
63 Secondary Care - Key Findings 32/75 patients in primary care had diagnosis overlooked 12.8% of patients in secondary care did not have a timely diagnosis 51 patients experienced a delay related to their CT scan, this delay resulted in an altered outcome for % of patients in secondary care did not have a CT scan within one hour of admission 63
64 Secondary Care - Key Findings 46.4% of patients did not receive Nimodipine in secondary care following diagnosis The decision to manage conservatively was considered appropriate in 94.1% of patients Delays in the referral process were more common out of hours 68.8% of patients received good care 64
65 Secondary Care - Recommendations The clinical presentation of asah should be highlighted in educational programmes Patients presenting with an acute severe headache should be thoroughly examined and a CT scan performed within one hour 65
66 Secondary Care - Recommendations Standard protocols for the management of patients with asah should be adopted Patients diagnosed with asah should be started on nimodipine 66
67 Tertiary Care Michael Gough 67
 Table 4.")
68 Source of Admission (Advisors Form) Table

69 Initial Assessment in NSC (Advisors Form) Poor examination 12.1% Poor planning I x 8.3% Table
")

70 Time to Consultant Review (Clinician Questionnaire) Clinically important 14% Not documented 45% Unknown 93 Table
 * Table 4.9 *Outcome affected in 2/14 13.")
71 Deficiencies in Admission Process (Advisors Form) * Table 4.9 *Outcome affected in 2/ % 71

72 Investigations Following Admission (Clinical Questionnaire) 73% underwent CTA: confirm aneurysm, plan T x * Table 4.10 * Data transfer crucial 72

73 Decision on Treatment Method (Clinical Questionnaire) Table 4.11 No documentation of discussion in nearly 1/4 73

74 Delay in Treatment Planning (Advisors Form) Table /24 = delay in performing CTA/DSA 74

75 Treatment Method for Aneurysm (Clinical Questionnaire) International Subarachnoid Aneurysm Trial (ISAT) Dependent/dead at 60/7: 25.4% v 36.4%, RRR 22.6% Table conservative management (15 presented to tertiary hospital) 75
 WFNS grade I 160 II")
76 Who Gave Consent? (Clinical Questionnaire) WFNS grade I 160 II 33 III 7 IV 2 Table

77 Delays in Definitive Treatment (Advisors Form) Delay in controlling aneurysm 21.6% >10% insufficient data 5/53: outcome affected 77


78 Day of Admission Time to Treatment in 246 Patients Mon-Thurs Fri-Sun < >48 Comparison of time from admission to intervention by day of admission 78
79 79

80 Time to Treatment Risk of Disease-specific Complications 80
81 Time to Treatment & Other Complications (Advisors Form) Table


 Table 4.")
82 Time to Treatment & Other Complications (Advisors Form) Table 4.18 Table
83 Time to Treatment Functional Status at Discharge 83

84 A 7-day Service Networks Interventional Radiology Surgeons AUDIT 84
 Table 4.")
85 Grade of Surgeon/Radiologist (Clinical Questionnaire) Table

86 Procedural Complications (Advisors Form) Table 4.24 Rupture during treatment 7/239 & 2/44 Thromboembolic 8/239: 4 CVA Failure to occlude: 1.7% v 0.5% Access vessel occlusion: 2.1% v 0.69% 86
 Table 4.")
87 Mortality Following Intervention (Advisors Form) Table 4.30 Identical to ISAT 87
 Table 4.32 Cochrane Review 4.")
88 Re-bleeding Post-intervention (Clinical Questionnaire) Table 4.32 Cochrane Review 4.2% 88
")
89 Outcome: Re-bleeding (Clinical Questionnaire) Table

90 Delayed Cerebral Ischaemia (Clinical Questionnaire) Table 4.39 Early brain injury > vasospasm Electrolytes, cortical spreading depression, microthrombosis 90
 Table 4.")
91 Treatment of Delayed Cerebral Ischaemia (Clinical Questionnaire) Table 4.41 Hypertension, Hypervolaemia, Haemodilution 91
92 Functional Status at Discharge The Need for Rehabilitation Services 2/3 had symptoms or disability 92

93 WFNS Grade and Outcome The Need for Rehabilitation Services <1/4 no symptoms or disability 93
 Table 4.")

94 In-patient Rehabilitation (Advisors Form) Table 4.47 Require formal assessment and planning 1y showed 1/3 cognitive impairment 94

95 Post-discharge Support for Patients with Symptoms or Disability Table 4.49 Advisors: inadequate in 35/164 (21.3%) 95

96 Functional Status at Discharge Neuropsychology Support Table 4.50 Good cognitive function = independent living, return to work 96


97 Organ Donation Table % of UK cadaveric donors = ICH 2012/13: 622/1212 Table

98 Organ Donation Reasons for No Donation * Table 5.3 * 1/8 refused by ITU consultant 19/43 = missed opportunities Audit donation rates Develop policies to increase 98
99 Recommendations - Tertiary Care Relevant professional bodies should develop nationallyagreed & audited protocols that include: Initial assessment and decision-making (MDT) with documentation Informed consent Timing of intervention Perioperative care Management of complications Rehabilitation Mental capacity of asah patients to give their own consent should be reviewed and a consensus document developed 99
100 Recommendations Tertiary Care The nationally agreed standard (National Clinical Guideline for Stroke) of securing ruptured aneurysms within 48 hours should be met consistently and comprehensively by the clinicians treating this group of patients. This will require providers to assess the service they deliver and move towards 7 day working Sufficient training opportunities for trainees to achieve competence Appropriately funded rehabilitation for all patients following an asah 100

101 Summary: Delays First Delay 20% 184 patients suffered a delay 68 patients had deficiencies in care that affected outcome Primary 25 Secondary 33 Tertiary 10 44% 36% Table
102 Overall Quality of Care Secondary & Tertiary Hospitals 2 0 care: 68.5% 3 0 care: 53.8% 2 0 care: 1.6% 3 0 care: 11.2% 102
103 Summary & Key Recommendations 427 patients 1 0 Care: 32/75 missed 23 affected 8 died 2 0 Care: 24 missed 17 affected 4 died No nimodipine 143/269 CT delay 51/390 4 affected 3 died 303 accepted NSC 36 delayed 2 died Poor assessment 132/ affected 9 died Delayed assessment 25/336 7 affected 3 died Education & protocols for the management of severe headache Treatment delayed > 48h re-bleeding complications disability Transfer delayed 47/ deteriorated 5 died 103
104 Summary & Key Recommendations 427 patients 1 0 Care: 32/75 missed 23 affected 8 died 2 0 Care: 24 missed 17 affected 4 died No nimodipine 143/269 CT delay 51/390 4 affected 3 died 303 accepted NSC 36 delayed 2 died Poor assessment 132/ affected 9 died Delayed assessment 25/336 7 affected 3 died Treatment delayed > 48h re-bleeding complications disability Transfer delayed 47/ deteriorated 5 died Standard protocols for networks: management in secondary care 104
105 Summary & Key Recommendations 427 patients 1 0 Care: 32/75 missed 23 affected 8 died 2 0 Care: 24 missed 17 affected 4 died No nimodipine 143/269 CT delay 51/390 4 affected 3 died 303 accepted NSC 36 delayed 2 died Poor assessment 132/ affected 9 died Delayed assessment 25/336 7 affected 3 died Transfer delayed 47/ deteriorated 5 died Formal networks and protocols for transfer 105
106 Summary & Key Recommendations 427 patients 1 0 Care: 32/75 missed 23 affected 8 died 2 0 Care: 24 missed 17 affected 4 died No nimodipine 143/269 CT delay 51/390 4 affected 3 died 303 accepted NSC 36 delayed 2 died Poor assessment 132/ affected 9 died Delayed assessment 25/336 7 affected 3 died Treatment delayed > 48h re-bleeding complications disability Transfer delayed 47/ deteriorated 5 died National protocols: management tertiary care 106
107 Summary & Key Recommendations 427 patients 1 0 Care: 32/75 missed 23 affected 8 died 2 0 Care: 24 missed 17 affected 4 died Conservative Management 136/150 died No nimodipine 143/269 CT delay 51/390 4 affected 3 died 303 accepted NSC 36 delayed 2 died Poor assessment 132/ affected 9 died Delayed assessment 25/336 7 affected 3 died Treatment delayed > 48h re-bleeding complications disability Transfer delayed 47/ deteriorated 5 died Radiology/Surgery 19/277 died 238/427 patients survived, many requiring rehabilitation 107
 patients with asah died 303 accepted NSC 36 delayed 2 died Poor assessment 132/427 26 affected 9 died Delayed assessment 25/336 7 affected 3 died")
108 Summary & Key Recommendations 1 0 Care: 32/75 missed 23 affected 8 died 427 patients 2 0 Care: 24 missed 17 affected 4 died Conservative Management/ No intervention 136/150 died No nimodipine 143/269 CT delay 51/390 4 affected 3 died 155/427 (36%) patients with asah died 303 accepted NSC 36 delayed 2 died Poor assessment 132/ affected 9 died Delayed assessment 25/336 7 affected 3 died Treatment delayed > 48h re-bleeding complications disability Transfer delayed 47/ deteriorated 5 died Radiology/Surgery 19/277died 108
109 Thank you 109
110
Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management
 0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
Introduction. Peripheral arterial disease. Hospital inpatient data - 5,498 FCE (2009/10), & 530 deaths in England alone
, & 530 deaths in England alone") 1 Introduction 2 Introduction Peripheral arterial disease Affects 20% adults in Europe and North America In the UK 500-1000/million PAD, 1-2% require amputation LLA 8-15% in people with diabetes with up
1 Introduction 2 Introduction Peripheral arterial disease Affects 20% adults in Europe and North America In the UK 500-1000/million PAD, 1-2% require amputation LLA 8-15% in people with diabetes with up
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Epidemiology And Treatment Of Cerebral Aneurysms At An Australian Tertiary Level Hospital
 ISPUB.COM The Internet Journal of Neurosurgery Volume 9 Number 2 Epidemiology And Treatment Of Cerebral Aneurysms At An Australian Tertiary Level Hospital A Granger, R Laherty Citation A Granger, R Laherty.
ISPUB.COM The Internet Journal of Neurosurgery Volume 9 Number 2 Epidemiology And Treatment Of Cerebral Aneurysms At An Australian Tertiary Level Hospital A Granger, R Laherty Citation A Granger, R Laherty.
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Report of the Welsh Neuroscience External Expert Review Group. All Wales Recommendations
 Report of the Welsh Neuroscience External Expert Review Group All Wales Recommendations Main Recommendations 1. The workforce delivering all aspects of care to people with acute and long term neurological
Report of the Welsh Neuroscience External Expert Review Group All Wales Recommendations Main Recommendations 1. The workforce delivering all aspects of care to people with acute and long term neurological
Proposed Neurosciences National Structure. Accountability Framework Neurological Alliance (Feedback Loop) National Advisory Group (Neurosciences)
 National Advisory Group (Neurosciences)") Accountability Framework Neurological Alliance (Feedback Loop) Proposed s National Structure National NHS England National Medical Director National Advisory Group (s) Regional NHS England Sub-Regional
Accountability Framework Neurological Alliance (Feedback Loop) Proposed s National Structure National NHS England National Medical Director National Advisory Group (s) Regional NHS England Sub-Regional
<INSERT COUNTRY/SITE NAME> All Stroke Events
 WHO STEPS STROKE INSTRUMENT For further guidance on All Stroke Events, see Section 5, page 5-15 All Stroke Events Patient Identification and Patient Characteristics (I 1) Stroke
WHO STEPS STROKE INSTRUMENT For further guidance on All Stroke Events, see Section 5, page 5-15 All Stroke Events Patient Identification and Patient Characteristics (I 1) Stroke
Management of Cerebral Aneurysms in Polycystic Kidney Disease. Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre
 Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Primary Versus Comprehensive: What is the Difference?
 Primary Versus Comprehensive: What is the Difference? April 26, 2018 Bethann Mercanti, PA-C Director of Clinical Practice Stroke Program Coordinator Cooper Neurological Institute Cooper Bon & Joint Institute
Primary Versus Comprehensive: What is the Difference? April 26, 2018 Bethann Mercanti, PA-C Director of Clinical Practice Stroke Program Coordinator Cooper Neurological Institute Cooper Bon & Joint Institute
A Best Practice Clinical Care Pathway for Major Amputation Surgery
 A Best Practice Clinical Care Pathway for Major Amputation Surgery April 2016 Introduction The perioperative mortality rate after major lower limb amputation in the UK is unacceptably high in modern medical
A Best Practice Clinical Care Pathway for Major Amputation Surgery April 2016 Introduction The perioperative mortality rate after major lower limb amputation in the UK is unacceptably high in modern medical
9 Diabetes care. Back to contents
 Back to contents Diabetes is a major risk factor for the development of peripheral vascular disease and 349/628 (55.6%) of the patients in this study had diabetes. Hospital inpatients with diabetes are
Back to contents Diabetes is a major risk factor for the development of peripheral vascular disease and 349/628 (55.6%) of the patients in this study had diabetes. Hospital inpatients with diabetes are
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015
 What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
How to make changes in the NHS
 How to make changes in the NHS Keith Willett Prof of Orthopaedic Trauma Surgery University of Oxford prev. National Clinical Director for Trauma Care ATOCP Conference Oxford 2016 Medical Director for Acute
How to make changes in the NHS Keith Willett Prof of Orthopaedic Trauma Surgery University of Oxford prev. National Clinical Director for Trauma Care ATOCP Conference Oxford 2016 Medical Director for Acute
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Medical technology guidance SCOPE Pipeline embolisation device for the treatment of
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Medical technology guidance SCOPE Pipeline embolisation device for the treatment of 1 Technology complex intracranial aneurysms 1.1 Description of
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Medical technology guidance SCOPE Pipeline embolisation device for the treatment of 1 Technology complex intracranial aneurysms 1.1 Description of
A. Service Specification
 A. Service Specification Service Specification No: 1767 Service Adult Highly Specialist Pain Management Services Commissioner Lead For local completion Lead For local completion 1. Scope 1.1 Prescribed
A. Service Specification Service Specification No: 1767 Service Adult Highly Specialist Pain Management Services Commissioner Lead For local completion Lead For local completion 1. Scope 1.1 Prescribed
SAFE HIP FRACTURES. Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust
 SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
はじめに 対象と方法 39: , 2017 SAH 183 WFNS
 39:107 原 著 39: 107 112, 2017 1 2 1 1 1 1 要旨 SAH 2010 1 2013 12 SAH 253 183 64 70 WFNS I III 72.7 Fisher CT 3 86.3 19.9 16.6 GR MD 73.2 73.1 80 WFNS Key words: subarachnoid hemorrhage, prognosis, rate of
39:107 原 著 39: 107 112, 2017 1 2 1 1 1 1 要旨 SAH 2010 1 2013 12 SAH 253 183 64 70 WFNS I III 72.7 Fisher CT 3 86.3 19.9 16.6 GR MD 73.2 73.1 80 WFNS Key words: subarachnoid hemorrhage, prognosis, rate of
Meeting the Future Challenge of Stroke
 Meeting the Future Challenge of Stroke Stroke Medicine Consultant Workforce Requirements 2011 201 Dr Christopher Price BASP Training and Education Committee Stroke Medicine Specialist Advisory Committee
Meeting the Future Challenge of Stroke Stroke Medicine Consultant Workforce Requirements 2011 201 Dr Christopher Price BASP Training and Education Committee Stroke Medicine Specialist Advisory Committee
Guidelines for the management of a patient with a subarachnoid haemorrhage
 Guidelines for the management of a patient with a subarachnoid haemorrhage Item Type Report Authors Health Service Executive (HSE) Citation Health Service Executive. Guidelines for the management of a
Guidelines for the management of a patient with a subarachnoid haemorrhage Item Type Report Authors Health Service Executive (HSE) Citation Health Service Executive. Guidelines for the management of a
Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS
 STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
NHS Rotherham Clinical Commissioning Group
 NHS Rotherham Clinical Commissioning Group Operational Executive: 2 nd November 2015 Governing Body: 4 th November 2015 Review of Stroke Care Pathway GP Lead: Dr Phil Birks Lead Executive: Keely Firth
NHS Rotherham Clinical Commissioning Group Operational Executive: 2 nd November 2015 Governing Body: 4 th November 2015 Review of Stroke Care Pathway GP Lead: Dr Phil Birks Lead Executive: Keely Firth
National Breast Cancer Audit next steps. Martin Lee
 National Breast Cancer Audit next steps Martin Lee National Cancer Audits Current Bowel Cancer Head & Neck Cancer Lung cancer Oesophagogastric cancer New Prostate Cancer - undergoing procurement Breast
National Breast Cancer Audit next steps Martin Lee National Cancer Audits Current Bowel Cancer Head & Neck Cancer Lung cancer Oesophagogastric cancer New Prostate Cancer - undergoing procurement Breast
Endovascular Treatment of Cerebral Arteriovenous Malformations. Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh
 Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Quality Surveillance Team. Major Trauma Services Quality Indicators
 Quality Surveillance Team Major Trauma Services Quality Indicators 1 MAJOR TRAUMA QUALITY INDICATORS Introduction These quality indicators have been commissioned by the National Clinical Director for Major
Quality Surveillance Team Major Trauma Services Quality Indicators 1 MAJOR TRAUMA QUALITY INDICATORS Introduction These quality indicators have been commissioned by the National Clinical Director for Major
Resource impact report: Eating disorders: recognition and treatment (NG69)
") Resource impact report: Eating disorders: recognition and treatment (NG69) Published: May 2017 Summary This report looks at the resource impact of implementing NICE s guideline on eating disorders: recognition
Resource impact report: Eating disorders: recognition and treatment (NG69) Published: May 2017 Summary This report looks at the resource impact of implementing NICE s guideline on eating disorders: recognition
Rationale for developing devastating brain injury pathways
 Rationale for developing devastating brain injury pathways Alex Manara Neuro ICU Southmead Hospital North Bristol NHS Trust Regional Clinical Lead in Organ Donation RCEM 2018 RCEM 2018 The Bristol Model
Rationale for developing devastating brain injury pathways Alex Manara Neuro ICU Southmead Hospital North Bristol NHS Trust Regional Clinical Lead in Organ Donation RCEM 2018 RCEM 2018 The Bristol Model
Canadian Best Practice Recommendations for Stroke Care 3.6 Acute Subarachnoid Hemorrhage
 Last Updated: May 21, 2013 Canadian Best Practice Recommendations for Stroke Care Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Contents Search Strategy... 2 CSN Current Recommendations...Error!
Last Updated: May 21, 2013 Canadian Best Practice Recommendations for Stroke Care Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Contents Search Strategy... 2 CSN Current Recommendations...Error!
Clinical manifestations, diagnosis and medical management of
 Clinical manifestations, diagnosis and medical management of aneurysmal SAH David Bervini, MD MAdvSurg Department of Neurosurgery Inselspital University of Bern Switzerland 1 2 3 Aneurysmal SAH Incidence:
Clinical manifestations, diagnosis and medical management of aneurysmal SAH David Bervini, MD MAdvSurg Department of Neurosurgery Inselspital University of Bern Switzerland 1 2 3 Aneurysmal SAH Incidence:
CONCISE GUIDE National Clinical Guidelines for Stroke 2nd Edition
 CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
Access to care: waiting times for special care patients accessing specialist services in a dental hospital
 Journal of Disability and Oral Health (2012) 13/1 27-34 Access to care: waiting times for special care patients accessing specialist services in a dental hospital Grace Kelly BDS MFDS RCSI 1 and June Nunn
Journal of Disability and Oral Health (2012) 13/1 27-34 Access to care: waiting times for special care patients accessing specialist services in a dental hospital Grace Kelly BDS MFDS RCSI 1 and June Nunn
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM)
") SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician ASWCN TAUNTON AND SOMERSET Taunton Lung MDT (11-2C-1) - 2011/12 Dr Sarah Foster Compliance Self Assessment LUNG MDT
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician ASWCN TAUNTON AND SOMERSET Taunton Lung MDT (11-2C-1) - 2011/12 Dr Sarah Foster Compliance Self Assessment LUNG MDT
A06/S(HSS)b Ex-vivo partial nephrectomy service (Adult)
b Ex-vivo partial nephrectomy service (Adult)") A06/S(HSS)b 2013/14 NHS STANDARD CONTRACT FOR EX-VIVO PARTIAL NEPHRECTOMY SERVICE (ADULT) PARTICULARS, SCHEDULE 2 THE SERVICES, A - SERVICE SPECIFICATION Service Specification No. Service Commissioner
A06/S(HSS)b 2013/14 NHS STANDARD CONTRACT FOR EX-VIVO PARTIAL NEPHRECTOMY SERVICE (ADULT) PARTICULARS, SCHEDULE 2 THE SERVICES, A - SERVICE SPECIFICATION Service Specification No. Service Commissioner
6. Endovascular aneurysm repair
 Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts
 Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts Exceptional healthcare, personally delivered Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts What is hydrocephalus? Hydrocephalus is the build up of an excess
Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts Exceptional healthcare, personally delivered Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts What is hydrocephalus? Hydrocephalus is the build up of an excess
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
Freedom of Information Act Request Physiotherapy Services for Neurological Conditions
 Freedom of Information Act Request Physiotherapy Services for Neurological Conditions 1. In total how many physiotherapists does C&V UHB employ? s services 33 qualified paediatric physiotherapy staff in
Freedom of Information Act Request Physiotherapy Services for Neurological Conditions 1. In total how many physiotherapists does C&V UHB employ? s services 33 qualified paediatric physiotherapy staff in
NHS RightCare Frailty Pathway An optimal frailty system
 NHS RightCare Frailty Pathway An optimal frailty system Martin Vernon National Clinical Director for Older People Adrian Hopper Consultant Physician & Frailty Pathway GiRFT Lead Alex Thompson Pathways
NHS RightCare Frailty Pathway An optimal frailty system Martin Vernon National Clinical Director for Older People Adrian Hopper Consultant Physician & Frailty Pathway GiRFT Lead Alex Thompson Pathways
Improving services for upper GI (OG) cancer Application template (Version 2)
 cancer Application template (Version 2)") Trust Clinical lead Improving services for upper GI (OG) cancer Application template (Version 2) Managerial lead Date completed 14 June 2013 Barnet & Chase Farm Hospitals NHS Trust Dr Marta Carpani Upper
Trust Clinical lead Improving services for upper GI (OG) cancer Application template (Version 2) Managerial lead Date completed 14 June 2013 Barnet & Chase Farm Hospitals NHS Trust Dr Marta Carpani Upper
Patient Information BRAIN ANEURYSMS (Including screening for familial aneurysms)
") Patient Information BRAIN ANEURYSMS (Including screening for familial aneurysms) 1 What is a cerebral aneurysm? An aneurysm is formed when there is a weakness in the blood vessel causing a ballooning or
Patient Information BRAIN ANEURYSMS (Including screening for familial aneurysms) 1 What is a cerebral aneurysm? An aneurysm is formed when there is a weakness in the blood vessel causing a ballooning or
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
The Royal College of Anaesthetists THE STRUCTURE OF A STANDARD
 ROYAL COLLEGE OF ANAESTHETISTS ACCREDITATION The Royal College of Anaesthetists THE STRUCTURE OF A STANDARD Page 1 of 10 The ACSA standard has 5 DOMAINS: 1. The Care Pathway 2. Equipment, Facilities and
ROYAL COLLEGE OF ANAESTHETISTS ACCREDITATION The Royal College of Anaesthetists THE STRUCTURE OF A STANDARD Page 1 of 10 The ACSA standard has 5 DOMAINS: 1. The Care Pathway 2. Equipment, Facilities and
(i) This FAQ does not deal with clinical issues (eg What is the definition of a stroke unit? or
 This FAQ does not deal with clinical issues (eg What is the definition of a stroke unit? or") STROKE INTEGRATED PERFORMANCE MEASURE RETURN (IPMR) FREQUENTLY ASKED QUESTIONS (FAQ) Prepared by NHS North West, Lancashire & Cumbria Cardiac & Stroke Network, Cheshire and Merseyside Clinical Networks
STROKE INTEGRATED PERFORMANCE MEASURE RETURN (IPMR) FREQUENTLY ASKED QUESTIONS (FAQ) Prepared by NHS North West, Lancashire & Cumbria Cardiac & Stroke Network, Cheshire and Merseyside Clinical Networks
Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage
 Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM)
") SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician GMCN ROYAL WOLVERHAMPTON HOSPITALS The Royal Wolverhampton Hospitals Trust Lung MDT (11-2C-1) - 2011/12 Dr Angela Morgan
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician GMCN ROYAL WOLVERHAMPTON HOSPITALS The Royal Wolverhampton Hospitals Trust Lung MDT (11-2C-1) - 2011/12 Dr Angela Morgan
(aneurysmal subarachnoid hemorrhage, 17%~60% :SAH. ,asah , 22%~49% : Willis. :1927 Moniz ;(3) 2. ischemic neurological deficit,dind) SAH) SAH ;(6)
 2. ischemic neurological deficit,dind) SAH) SAH ;(6)") ,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
Sentinel Stroke National Audit Programme (SSNAP)
") Sentinel Stroke National Audit Programme (SSNAP) Changes over Time: 4 years of data April 2013 March 2017 National results Based on stroke patients admitted to and/or discharged from hospital between April
Sentinel Stroke National Audit Programme (SSNAP) Changes over Time: 4 years of data April 2013 March 2017 National results Based on stroke patients admitted to and/or discharged from hospital between April
Bleeding in the brain: haemorrhagic stroke
 Call the Stroke Helpline: 0303 3033 100 or email: info@stroke.org.uk Bleeding in the brain: haemorrhagic stroke Some strokes are due to bleeding in or around the brain, and are known as haemorrhagic strokes.
Call the Stroke Helpline: 0303 3033 100 or email: info@stroke.org.uk Bleeding in the brain: haemorrhagic stroke Some strokes are due to bleeding in or around the brain, and are known as haemorrhagic strokes.
South East Coast Operational Delivery Network. Critical Care Rehabilitation
 South East Coast Operational Delivery Networks Hosted by Medway Foundation Trust South East Coast Operational Delivery Network Background Critical Care Rehabilitation The optimisation of recovery from
South East Coast Operational Delivery Networks Hosted by Medway Foundation Trust South East Coast Operational Delivery Network Background Critical Care Rehabilitation The optimisation of recovery from
Flow-diverting stents (in the Treatment of intracranial aneurysms)
") National Hospital for Neurology and Neurosurgery Flow-diverting stents (in the Treatment of intracranial aneurysms) Lysholm Department of Neuroradiology If you would like this document in another language
National Hospital for Neurology and Neurosurgery Flow-diverting stents (in the Treatment of intracranial aneurysms) Lysholm Department of Neuroradiology If you would like this document in another language
This booklet has been published by CREST (the Clinical Resource Efficiency Support Team).
.") This booklet has been published by CREST (the Clinical Resource Efficiency Support Team). CREST is a small committee of health care professionals established under the auspices of the Central Medical Advisory
This booklet has been published by CREST (the Clinical Resource Efficiency Support Team). CREST is a small committee of health care professionals established under the auspices of the Central Medical Advisory
Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181)
") Putting NICE guidance into practice Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181) Published: July 2014 This costing report accompanies Lipid modification:
Putting NICE guidance into practice Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181) Published: July 2014 This costing report accompanies Lipid modification:
Treatment of Unruptured Vertebral Artery Dissecting Aneurysms
 33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 29th April 2014 Compliance
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 29th April 2014 Compliance
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM)
") SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician CSCCN PORTSMOUTH HOSPITALS Portsmouth Colorectal MDT (11-2D-1) - 2011/12 Daniel OLeary Compliance Self Assessment COLORECTAL
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician CSCCN PORTSMOUTH HOSPITALS Portsmouth Colorectal MDT (11-2D-1) - 2011/12 Daniel OLeary Compliance Self Assessment COLORECTAL
Delivering 62 Day GP Cancer Waits in a Complex Landscape. Hannah Marder Cancer Manager University Hospitals Bristol
 Delivering 62 Day GP Cancer Waits in a Complex Landscape Hannah Marder Cancer Manager University Hospitals Bristol Overview The 62 day GP target Cancer pathways What causes breaches? Good practice and
Delivering 62 Day GP Cancer Waits in a Complex Landscape Hannah Marder Cancer Manager University Hospitals Bristol Overview The 62 day GP target Cancer pathways What causes breaches? Good practice and
lek Magdalena Puławska-Stalmach
 lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
What You Should Know About Cerebral Aneurysms
 American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
Diabetes (DIA) Measures Document
 Measures Document") Diabetes (DIA) Measures Document DIA Version: 2.1 - covering patients discharged between 01/07/2016 and present. Programme Lead: Liz Kanwar Clinical Lead: Dr Aftab Ahmad Number of Measures In Clinical
Diabetes (DIA) Measures Document DIA Version: 2.1 - covering patients discharged between 01/07/2016 and present. Programme Lead: Liz Kanwar Clinical Lead: Dr Aftab Ahmad Number of Measures In Clinical
Acute Heart Failure. Study protocol
 Acute Heart Failure Study protocol Study Advisory Group Lisa Anderson Cardiologist St Georges Joanne Bateman Lead pharmacist for cardiology Countess of Chester Paul Foley Cardiologist Swindon Jane Greaves
Acute Heart Failure Study protocol Study Advisory Group Lisa Anderson Cardiologist St Georges Joanne Bateman Lead pharmacist for cardiology Countess of Chester Paul Foley Cardiologist Swindon Jane Greaves
Measuring the Units. A review of patients who died with alcohol-related liver disease. SUMMARY Full report available to download at
 Measuring the Units A review of patients who died with alcohol-related liver disease SUMMARY Full report available to download at www.ncepod.org.uk Measuring the Units A review of patients who died with
Measuring the Units A review of patients who died with alcohol-related liver disease SUMMARY Full report available to download at www.ncepod.org.uk Measuring the Units A review of patients who died with
Clinical Commissioning Policy Statement: Flow Diverting Devices for Intracranial Aneurysms. April Reference : NHSCB/D03/PS/a
 Clinical Commissioning Policy Statement: Flow Diverting Devices for Intracranial Aneurysms April 2013 Reference : NHS Commissioning Board Clinical Commissioning Policy Statement: Flow Diverting Devices
Clinical Commissioning Policy Statement: Flow Diverting Devices for Intracranial Aneurysms April 2013 Reference : NHS Commissioning Board Clinical Commissioning Policy Statement: Flow Diverting Devices
Neuroscience ICU: A Statewide Critical Care Resource
 Neuroscience ICU: A Statewide Critical Care Resource Ansgar M Brambrink, MD, PhD Director, Neuroscience Intensive Care Unit Oregon Health & Science University Portland, OR Neurocritical care in the US
Neuroscience ICU: A Statewide Critical Care Resource Ansgar M Brambrink, MD, PhD Director, Neuroscience Intensive Care Unit Oregon Health & Science University Portland, OR Neurocritical care in the US
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography
 Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
D03/S/a NHS STANDARD CONTRACT FOR NEUROSURGERY (ADULT) SCHEDULE 2 THE SERVICES A. SERVICE SPECIFICATIONS. Service Specification No.
 SCHEDULE 2 THE SERVICES A. SERVICE SPECIFICATIONS. Service Specification No.") D03/S/a NHS STANDARD CONTRACT FOR NEUROSURGERY (ADULT) SCHEDULE 2 THE SERVICES A. SERVICE SPECIFICATIONS Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review D03/S/a
D03/S/a NHS STANDARD CONTRACT FOR NEUROSURGERY (ADULT) SCHEDULE 2 THE SERVICES A. SERVICE SPECIFICATIONS Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review D03/S/a
5 Diagnosis. Timely diagnosis. Back to contents
 5 5 Diagnosis Back to contents Study Advisory Group questions: Are there delays in diagnosis? Is there variation in how the cerebral palsies are described? signs can fluctuate, to avoid over-diagnosis
5 5 Diagnosis Back to contents Study Advisory Group questions: Are there delays in diagnosis? Is there variation in how the cerebral palsies are described? signs can fluctuate, to avoid over-diagnosis
Clinical Review of 20 Cases of Terson s Syndrome
 34 Clinical Review of 20 Cases of Terson s Syndrome Takashi SUGAWARA, M.D., Yoshio TAKASATO, M.D., Hiroyuki MASAOKA, M.D., Yoshihisa OHTA, M.D., Takanori HAYAKAWA, M.D., Hiroshi YATSUSHIGE, M.D., Shogo
34 Clinical Review of 20 Cases of Terson s Syndrome Takashi SUGAWARA, M.D., Yoshio TAKASATO, M.D., Hiroyuki MASAOKA, M.D., Yoshihisa OHTA, M.D., Takanori HAYAKAWA, M.D., Hiroshi YATSUSHIGE, M.D., Shogo
JAWDA Quarterly Waiting Time Guidelines for (Specialized and General Hospitals)
") JAWDA Waiting Time Guidelines for (Specialized and General Hospitals) January 2019 Page 1 of 22 Table of Contents Executive Summary... 3 About this Guidance... 4 Performance Indicators... 5 APPENDIX -
JAWDA Waiting Time Guidelines for (Specialized and General Hospitals) January 2019 Page 1 of 22 Table of Contents Executive Summary... 3 About this Guidance... 4 Performance Indicators... 5 APPENDIX -
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care
 SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
STROKE SERVICE STANDARDS. CLINICAL STANDARDS COMMITTEE June 2014
 STROKE SERVICE STANDARDS CLINICAL STANDARDS COMMITTEE June 2014 A Bhalla (Chair), G Subramanian P Gompertz, D Wilson, B Patel, K Harkness, T Hassan, MR Chowdhury, J Korner, F Doubal STROKE SERVICE STANDARDS
STROKE SERVICE STANDARDS CLINICAL STANDARDS COMMITTEE June 2014 A Bhalla (Chair), G Subramanian P Gompertz, D Wilson, B Patel, K Harkness, T Hassan, MR Chowdhury, J Korner, F Doubal STROKE SERVICE STANDARDS
AEROMEDICAL DECISION MAKING IN CEREBRAL ANEURYSMS. Pooshan Navāthé Michael Drane Peter Clem David Fitzgerald
 AEROMEDICAL DECISION MAKING IN CEREBRAL ANEURYSMS Pooshan Navāthé Michael Drane Peter Clem David Fitzgerald Disclaimer I receive a salary from the Commonwealth of Australia. I have no financial relationships
AEROMEDICAL DECISION MAKING IN CEREBRAL ANEURYSMS Pooshan Navāthé Michael Drane Peter Clem David Fitzgerald Disclaimer I receive a salary from the Commonwealth of Australia. I have no financial relationships
The research questions are presented in priority order, and are further elaborated with lay summaries and three-part questions where applicable.
 Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
Lothian Audit of the Treatment of Cerebral Haemorrhage (LATCH)
") 1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM
 NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
Maximising Delivery of Thrombectomy
 Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
How to get a Clinical Psychologist. Dr Ian Kneebone Consultant Clinical Psychologist & Visiting Reader
 How to get a Clinical Psychologist Dr Ian Kneebone Consultant Clinical Psychologist & Visiting Reader How to make a case to the new clinical commissioning groups (CCG) If CCGs do not eventuate basics should
How to get a Clinical Psychologist Dr Ian Kneebone Consultant Clinical Psychologist & Visiting Reader How to make a case to the new clinical commissioning groups (CCG) If CCGs do not eventuate basics should
Alzheimer s Society. Consultation response. Our NHS care objectives: A draft mandate to the NHS Commissioning Board.
 Alzheimer s Society Our NHS care objectives: A draft mandate to the NHS Commissioning Board 26 September 2012 Delivering Dignity Securing dignity in care for older people in hospitals and care homes: A
Alzheimer s Society Our NHS care objectives: A draft mandate to the NHS Commissioning Board 26 September 2012 Delivering Dignity Securing dignity in care for older people in hospitals and care homes: A
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Manchester Collaborative MTC Greater Manchester Major Trauma Centre Collaborative Network Organisation
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Manchester Collaborative MTC Greater Manchester Major Trauma Centre Collaborative Network Organisation
Six step guide to improving diabetes footcare. Putting feet. first
 Six step guide to improving diabetes footcare Putting feet first In England there are over 140 leg, foot or toe amputations a week. Diabetes related amputations and foot ulcers cost the NHS in England
Six step guide to improving diabetes footcare Putting feet first In England there are over 140 leg, foot or toe amputations a week. Diabetes related amputations and foot ulcers cost the NHS in England
SUMMARY Full report available to download at Lower Limb Amputation: Working Together
 Physiotherapists Interventional Radiologists Psychologists herapists TOccupational amputation co0ordinator SUMMARY Full report available to download at www.ncepod.org.uk Lower Limb Amputation: Working
Physiotherapists Interventional Radiologists Psychologists herapists TOccupational amputation co0ordinator SUMMARY Full report available to download at www.ncepod.org.uk Lower Limb Amputation: Working
Stroke Systems of Care. Sharon Webb, MD, FAANS, FACS, FAHA
 Stroke Systems of Care Sharon Webb, MD, FAANS, FACS, FAHA Disclosures No Disclosures Objectives Describe Systems of Care Describe stroke levels of care Discuss SC stroke council state Initiatives What
Stroke Systems of Care Sharon Webb, MD, FAANS, FACS, FAHA Disclosures No Disclosures Objectives Describe Systems of Care Describe stroke levels of care Discuss SC stroke council state Initiatives What
London Strategic Clinical Networks. Quality Standard. Version 1.0 (2015)
") London Strategic Clinical Networks Quality Standard Version 1.0 (2015) Supporting the delivery of equitable, high quality AKI care through collaboration www.londonaki.net @LondonAKI Overview The management
London Strategic Clinical Networks Quality Standard Version 1.0 (2015) Supporting the delivery of equitable, high quality AKI care through collaboration www.londonaki.net @LondonAKI Overview The management
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neuro-vascular Intervention in Stroke. Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust
 Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Stroke care in England, Wales and Northern Ireland. This report is for stroke survivors and their families
 Stroke care in England, Wales and Northern Ireland This report is for stroke survivors and their families Based on patients treated between August - November 2017 1 2 Table of Contents Glossary 5 Introduction
Stroke care in England, Wales and Northern Ireland This report is for stroke survivors and their families Based on patients treated between August - November 2017 1 2 Table of Contents Glossary 5 Introduction
abcdefghijklmnopqrstu
 CMO and Public Health Directorate Health Improvement Strategy Division Dear Colleague Scottish Abdominal Aortic Aneurysm Screening Programme This CEL outlines the plan for the implementation of the AAA
CMO and Public Health Directorate Health Improvement Strategy Division Dear Colleague Scottish Abdominal Aortic Aneurysm Screening Programme This CEL outlines the plan for the implementation of the AAA
Correlation of revised fisher scale with clinical
 Research Article Correlation of revised fisher scale with clinical grading (WFNS) in patients with non-traumatic subarachnoid haemorrhage Basti Ram S. 1, Kumbar Vishwanath G. 2*, Nayak Madhukar T., Xavier
Research Article Correlation of revised fisher scale with clinical grading (WFNS) in patients with non-traumatic subarachnoid haemorrhage Basti Ram S. 1, Kumbar Vishwanath G. 2*, Nayak Madhukar T., Xavier
The RAPID Programme Rapid Access to Pulmonary Investigation & Diagnosis
 Patient Experience National Network Awards (PENNA) The RAPID Programme 2016-2019 Rapid Access to Pulmonary Investigation & Diagnosis Kath Hewitt Lead Clinical Nurse Specialist Ailsa Rowlands Programme
Patient Experience National Network Awards (PENNA) The RAPID Programme 2016-2019 Rapid Access to Pulmonary Investigation & Diagnosis Kath Hewitt Lead Clinical Nurse Specialist Ailsa Rowlands Programme
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
N E W T O N. Hänggi D, Etminan N, Macdonald RL, Steiger HJ, Mayer SA, Aldrich F, Diringer MN, Hoh BJ, Mocco J, Strange P, Faleck HJ, Miller M
 N E W T O N Nimodipine microparticles to Enhance recovery While reducing TOxicity after subarachnoid hemorrhage Phase 1/2a Multicenter, Controlled, Randomized, Open Label, Dose Escalation, Safety, Tolerability,
N E W T O N Nimodipine microparticles to Enhance recovery While reducing TOxicity after subarachnoid hemorrhage Phase 1/2a Multicenter, Controlled, Randomized, Open Label, Dose Escalation, Safety, Tolerability,
Treat the Cause. summary. A review of the quality of care provided to patients treated for acute pancreatitis. Improving the quality of healthcare
 Treat the Cause A review of the quality of care provided to patients treated for acute pancreatitis summary Improving the quality of healthcare Treat the Cause A review of the quality of care provided
Treat the Cause A review of the quality of care provided to patients treated for acute pancreatitis summary Improving the quality of healthcare Treat the Cause A review of the quality of care provided
2010 National Audit of Dementia (Care in General Hospitals) Guy's and St Thomas' NHS Foundation Trust
 Guy's and St Thomas' NHS Foundation Trust") Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: Guy's and St Thomas' NHS Foundation Trust The 2010 national
Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: Guy's and St Thomas' NHS Foundation Trust The 2010 national
Sentinel Stroke National Audit Programme (SSNAP) Based on stroke patients admitted to hospital for thrombectomy between April 2016 and March 2017
 Based on stroke patients admitted to hospital for thrombectomy between April 2016 and March 2017") Thrombectomy Sentinel Stroke National Audit Programme (SSNAP) Thrombectomy Report for April 2016 - March 2017 National results July 2017 Based on stroke patients admitted to hospital for between April
Thrombectomy Sentinel Stroke National Audit Programme (SSNAP) Thrombectomy Report for April 2016 - March 2017 National results July 2017 Based on stroke patients admitted to hospital for between April
Osteoporosis: fragility fracture risk. Costing report. Implementing NICE guidance
 Osteoporosis: fragility fracture risk Costing report Implementing NICE guidance August 2012 NICE clinical guideline 146 1 of 15 This costing report accompanies the clinical guideline: Osteoporosis: assessing
Osteoporosis: fragility fracture risk Costing report Implementing NICE guidance August 2012 NICE clinical guideline 146 1 of 15 This costing report accompanies the clinical guideline: Osteoporosis: assessing
LCA Lung Clinical Forum. 21 st October 2014
 LCA Lung Clinical Forum 21 st October 2014 Welcome Dr Liz Sawicka Chair - LCA Lung Pathway Group Succession planning Dr Kate Haire Consultant in Public Health Medicine, LCA Commissioning Intentions for
LCA Lung Clinical Forum 21 st October 2014 Welcome Dr Liz Sawicka Chair - LCA Lung Pathway Group Succession planning Dr Kate Haire Consultant in Public Health Medicine, LCA Commissioning Intentions for
Subarachnoid Hemorrhage and Brain Aneurysm
 Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.