STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia.
|
|
|
- Bennett Nicholson
- 5 years ago
- Views:
Transcription
1 STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia.
2 PART 1 Systems of care for STEMI.
3 STEMI Management Coronary angiogram +/- stenting. Prehospital thrombolysis followed by rescue or routine angiogram +/- stenting
4 Untreated STEMI Danchin N, et al. Long-Term Survival After Lysis or PCI in STEMI. Circulation
5 Pre-hospital thrombolysis STEMI patients with significant delays to primary angioplasty.

6

7 HNE Health. Area: 130, 000 square Kilometres. One 24/7 cath. Lab. Distance of farthest hospital to JHH: Over 500 kilometres.


8

9 STEMI care team 24/7 on call. Supported by: -NSW ambulance. Emergency, Retrieval and ICU teams
10 STEMI - Systems of care onwards Estimated first medical contact to cath. lab arrival time > 60 min. Fibrinolysis versus primary angioplasty.
11 Hunter AMI Registry Non-randomised PHT and Primary PCI experience. August 2008 to August Data was prospectively collected.
12 Aims In patients with STEMI: safety of pre-hospital thrombolysis Risk of death (nonrandomised) across Hunter New England
13 Outcomes All-cause mortality. Bleeding.
14
15 Results PHT (n=150) PPCI (n=334) P-value Age Mean ± S.D. 62±13 65± yr. no. (%) 27 (18) 88 (26) 0.01 Males no. (%) 114 (76) 251 (75) 0.8 S/blood pressure Mean ± S.D. 125±25 131±
16 Results PHT (n=150) PPCI (n=334) P Value First medical contact to treatment (Range) min. 35 (6 95) 130 (45 300) Distance to cath. lab. (Km) Median (Range) 120 (8-483) 20 (5 69) Length of stay mean ± S.D. 4±3 4±3 1 Ejection Fraction (%) Mean ± S.D. 49±10 47±7 0.2 Peak Troponin Mean ± S.D. 44±28 50±
17 Results PHT (n=150) Primary PCI (n=334) P-Value Coronary Angiography 92% 100% <0.001 Rescue PCI 27% NA - Median Time from symptom to angiography (Range) Hours. 28 (2-245) 3.5 (1 17) <0.001 Initial TIMI flow 2 45% 8% <0.001
18 1 year all-cause mortality
19 Results PHT PPCI Safety outcomes Total bleeding No. (%) 14 (9%) 17 (5%) TIMI major Bleeding - No. (%) 2 (1.4) 0 Intracranial Haemorrhage -No. (%) 1 (0.7) 0
20 Conclusions Our real-world experience shows that PHT followed by early transfer to a PCI-capable centre is a safe and effective reperfusion strategy.

21

22

23
24 PART 2 LVEDP as a treatment target in STEMI
25

26
27 LVEDP measurement.

28 LVEDP measurement.
29 Physiology Indicative of the hemodynamic health of the left ventricle. Preload Contractility Compliance and stiffness Myocardial Ischemia Afterload


30 LV Compliance
/(2 X wall thickness) Gjesdal, O. et al. (2011) Cardiac remodeling at the population level risk factors, screening, and outcomes Nat. Rev. Cardiol. doi:10.1038/nrcardio.2011.154")
31 Law of Laplace: Wall stress increases the tension in the myocardium and thus reduces myocardial blood flow and counteracts myocardial shortening LV wall stress = (LV pressure X radius)/(2 X wall thickness) Gjesdal, O. et al. (2011) Cardiac remodeling at the population level risk factors, screening, and outcomes Nat. Rev. Cardiol. doi: /nrcardio
32 Significance of LVEDP Adverse LV remodelling Heart failure. Mortality.
33 675 pts, (STEMI= 43%). LVEDP 26.5 mmhg LVEDP and MACE in STEMI In hospital mortality 4.9% vs 2.4% In hospital HF 37% vs 28% 3 months mortality 3 months MACE 1 year MACE 16% vs 11% 1 year mortality 13% (66% STEMI ) vs 5% 2 year MACE year mortality 1909 (out of 5745) pts 22 mmhg - - 4% vs 2% 12% vs 7% (out of 3602 pts) 18 mmhg 3.1% vs 1.5% 6.3% vs 3.7% % vs 17% 6% vs 4%

34 Brienesse S, Davies A, et al. Under review.
.")
35 Aortic valvuloplasty and LVEDP - Severe AS undergoing BAV patients from MGH. -Inhospital MACE. -OR 1.08, for each mm Hg rise in pressure; 95% CI ). -Independent of LVEF.

36 CABG and LVEDP Patients undergoing CABG. 602 pts had LVEF < 35%. Cut-off LVEDP = 18 mmhg. Increased mortality.
37 LVEDP as a treatment target
38 Reperfusion and LVEDP STEMI, N=29 LVEDP measured before and after PPCI. Dropped by 5.7 ± 2.9 mmhg. Changes in LVEDP post primary PCI. AM Heart Hosp J Winter;8(2):E86-90

39 LVAD and LVEDP Seidel T, et al. Circulation. 2017;135: doi: /CIRCULATIONAHA
40 CRT and LVEDP N=17 Invasive haemodynami cs at baseline and 1 month post CRT (plus OMT). 30% reduction in LVEDP and PCWP

41 Research question Does reducing LVEDP after primary PCI prevent LV remodeling and improve outcomes?
42 JHH data /236 patients (64%) Median LVEDP: 22 mmhg (IQR: 19 30) Median follow up: 13 months (IQR: 4 17 months) All-cause mortality: 5% (7 out of 152). 6.6% vs 2.6%, RR: 2.5, P=0.2, CI: to , NNT (Harm): 25
43 P=0.2
44 How to reduce LVEDP Nitrates and frusemide by affecting preload and afterload.
45 Our proposed clinical trial program Phase 1 Dose finding/safety study. Phase 2 Randomised, doubleblind study with LV remodelling endpoint. Phase 3 Randomised, doubleblind multi-centre study with clinical endpoints
46 Phase 1 Acute haemodynamic, dose finding/safety study. Aim : Find the dose of nitrate, in conjunction with a single bolus of frusemide, which can be used to reduce LVEDP following Primary PCI?
47 Phase 1 Inclusion criteria STEMI with LVEDP 20 mmhg after intervention to infarct related artery.
48 Phase 1 Intervention Frusemide 40mg IV plus escalating GTN doses - 100mcg every minute (up to 1000 mcg over 10 minutes).
49 Phase 1 End points Dose of GTN needed to cause 20% reduction in LVEDP. Effect on systolic blood pressure?
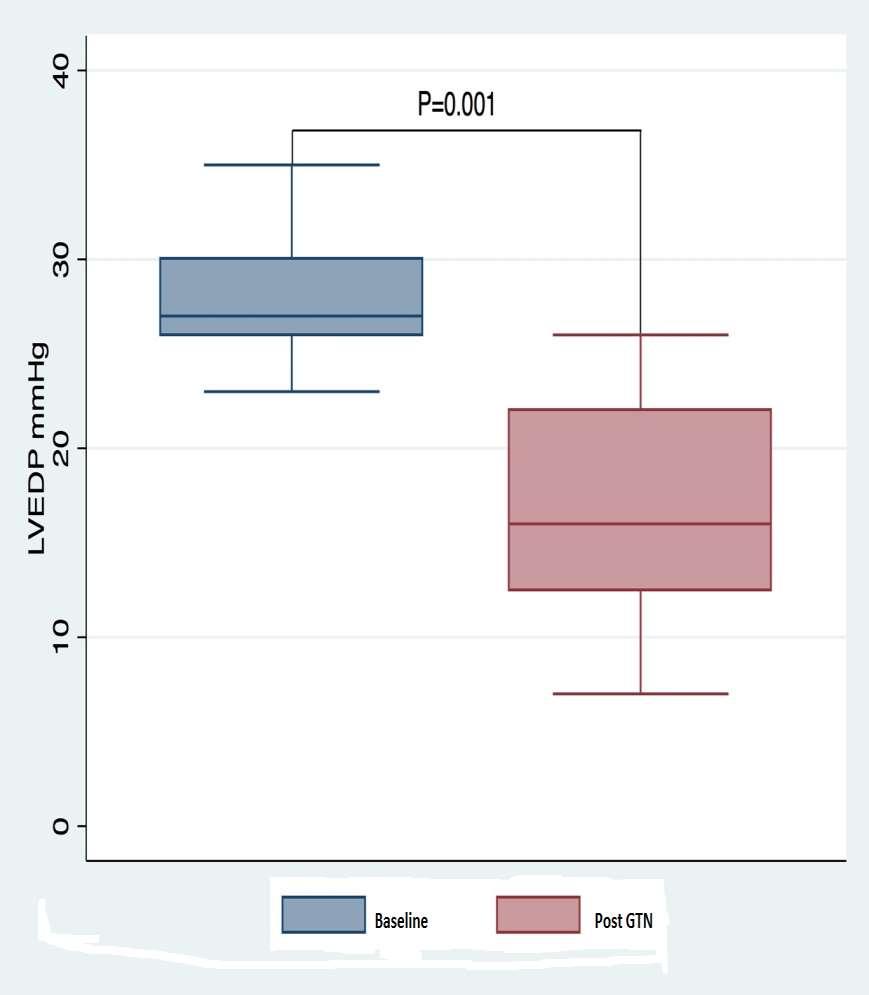
50 Results - Phase 1 Recruitment N=10, Age 65±7, Males=5 (50%), Anterior=5 (50%) Variable response: Median=200 mcg (Range: ), Mean 260±180 Systemic BP: 9% reduction (7 16%). No symptoms.
51 LVEDP (mmhg) Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Patient 7 Patient 8 Patient 9 Patient ±3 mmhg ±4 mmhg BASELINE POST GTN
52
53 Phase 1 - Conclusion Safe in STEMI. Reduce LVEDP. Effect of LVEDP reduction should be tested in prospective RCTs.
54 Phase 2 RCT. Research question? Do nitrates and frusemide affect remodelling and Infarct size in STEMI patients with raised LVEDP?
55 Phase 2 Inclusion criteria: STEMI with LVEDP 20 mmhg. Systolic BP 100 mmhg.
56 Phase 2 Exclusion criteria: Inability to informed consent. Patients presenting with cardiogenic shock Cardiopulmonary resuscitation. Any ventricular arrhythmias requiring treatment. Current life-threatening condition (other than vascular disease) with life expectancy < 1year. Severe infection, or any significant trauma (fractures, burns etc.) Pregnancy. Contraindications to cardiac magnetic resonance imaging. Renal impairment with known egfr < 30 ml/min or maintenance haemodialysis.
57 Phase 2 Intervention Primary PCI (All patients). Randomised to treatment or placebo arm. Treatment arm: Oral Lasix 40mg daily and Isosorbide mononitrate mg daily for 3 months.
58 Phase 2 CMR and Echo Baseline and 3 months. Blood tests Troponin, BNP, UECs, Creatinine. Follow up 3 and 12 months.
59 Sample calculation N=50 (25 in each arm). Placebo arm adverse remodelling of 10% Intervention arm reverse remodelling of 5% P=0.05, Power = 80%.
60 Phase 2 End points Primary safety end point: Safety and tolerability of ISMN and frusemide. Primary efficacy endpoint: Change in left ventricular end diastolic volume index from post-mi to 3 months. Secondary endpoints: Death, MI, Stroke and HF.
61 Progress - Phase 2 Ethics Funding Heart Foundation.
62 Acknowledgements Prof Boyle and Fletcher. HNE Health Research and Translation Centre. NSW Ambulance. Dr Leitch and Bastian Interventional group Collins, Hatton, Bhagwandeen and Thambar. Dr Turner, Singham, Hackworthy and sonographers. ATs and Fellows- A Davies, M McGee, N Whitehead, D Baker, Al-Omary. Deb Bick and cath lab staff. Cardiac techs.
63 Thank you.
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION. STREAM 1Y AHA 2013 P Sinnaeve
 STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
How to do Primary Angioplasty. - Patients with Cardiogenic Shock
 How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
Myocardial Infarction In Dr.Yahya Kiwan
 Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction. Is it beneficial to patients?
 Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Assist Devices in STEMI- Intra-aortic Balloon Pump
 Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Recovering Hearts. Saving Lives.
 Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Management of Cardiogenic shock. Prof. Christian JM Vrints
 Management of Cardiogenic shock Prof. Christian JM Vrints none conflicts Management of Cardiogenic Shock Incidence and trends Importance of early revascularization Multivessel disease Left main disease
Management of Cardiogenic shock Prof. Christian JM Vrints none conflicts Management of Cardiogenic Shock Incidence and trends Importance of early revascularization Multivessel disease Left main disease
M/39 CC D. => peak CKMB (12 hr later) ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #
 ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #") Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies
 Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
The Strategic Reperfusion Early After STEMI study Implications for clinical practice
 The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
The Window for Fibrinolysis. Frans Van de Werf, MD, PhD Leuven, Belgium
 The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
STEMI and Cardiogenic Shock. The rules and solution. Dave Kettles St Dominics and Frere Hospitals East London ZA
 STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Decision for fibrinolysis or primary PCI in the prehospital phase
 Decision for fibrinolysis or primary PCI in the prehospital phase Nicolas Danchin, Hôpital Européen Georges Pompidou, Paris, France Disclosures Research grants: Astrazeneca, Eli-Lilly, GSK, Merck, Novartis,
Decision for fibrinolysis or primary PCI in the prehospital phase Nicolas Danchin, Hôpital Européen Georges Pompidou, Paris, France Disclosures Research grants: Astrazeneca, Eli-Lilly, GSK, Merck, Novartis,
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση. Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας
 Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
Patient Transfer. Mark de Belder The James Cook University Hospital Middlesbrough
 Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
Critical Review Form Therapy Objectives: Methods:
 Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities
 The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
PHARMACO-INVASIVE STRATEGY COMPARED WITH PPCI: DESIGN AND MAIN OUTCOMES OF THE STREAM TRIAL
 PHARMACO-INVASIVE STRATEGY COMPARED WITH PPCI: DESIGN AND MAIN OUTCOMES OF THE STREAM TRIAL Frans Van de Werf Leuven, Belgium Disclosures Study grant from Boehringer Ingelheim to perform the STREAM trial,
PHARMACO-INVASIVE STRATEGY COMPARED WITH PPCI: DESIGN AND MAIN OUTCOMES OF THE STREAM TRIAL Frans Van de Werf Leuven, Belgium Disclosures Study grant from Boehringer Ingelheim to perform the STREAM trial,
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Approach to Multi Vessel disease with STEMI
 Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting
 How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
Primary Percutaneous Coronary Intervention
 The big 5 in PCI Primary Percutaneous Coronary Intervention W. Wijns (Aalst, BE) Disclosures Consulting Fees: on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the
The big 5 in PCI Primary Percutaneous Coronary Intervention W. Wijns (Aalst, BE) Disclosures Consulting Fees: on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the
A Future for the IABP in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany
 University of Lübeck, Germany") A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
Management of ST-elevation myocardial infarction Update 2009 Late comers: which options?
 European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
STEMI ST Elevation Myocardial Infarction
 STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
Counterpulsation. John N. Nanas, MD, PhD. Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece
 John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
IABP SHOCK II trial:
 IABP SHOCK II trial: Randomized comparison of intraaortic balloon counterpulsation versus optimal medical therapy in addition to early revascularization in acute myocardial infarction complicated by cardiogenic
IABP SHOCK II trial: Randomized comparison of intraaortic balloon counterpulsation versus optimal medical therapy in addition to early revascularization in acute myocardial infarction complicated by cardiogenic
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI?
 SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
Improving STEMI outcomes in Denmark. Michael Rahbek Schmidt, MD, PhD. Aarhus University Hospital Skejby Denmark
 Improving STEMI outcomes in Denmark Michael Rahbek Schmidt, MD, PhD. Aarhus University Hospital Skejby Denmark Presenter Disclosure Information Study funded by Fondation Leducq Michael Rahbek Schmidt The
Improving STEMI outcomes in Denmark Michael Rahbek Schmidt, MD, PhD. Aarhus University Hospital Skejby Denmark Presenter Disclosure Information Study funded by Fondation Leducq Michael Rahbek Schmidt The
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY
 ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
Xi Li, Jing Li, Frederick A Masoudi, John A Spertus, Zhenqiu Lin, Harlan M Krumholz, Lixin Jiang for the China PEACE Collaborative Group
 China PEACE risk estimation tool for inhospital death from acute myocardial infarction: an early risk classification tree for decisions about fibrinolytic therapy Xi Li, Jing Li, Frederick A Masoudi, John
China PEACE risk estimation tool for inhospital death from acute myocardial infarction: an early risk classification tree for decisions about fibrinolytic therapy Xi Li, Jing Li, Frederick A Masoudi, John
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology
 Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
FFR-guided Complete vs. Culprit Only Revascularization in AMI Patients Ki Hong Choi, MD On Behalf of FRAME-AMI Investigators
 FFR-guided Complete vs. Culprit Only Revascularization in AMI Patients Ki Hong Choi, MD On Behalf of FRAME-AMI Investigators Heart Vascular Stroke Institute, Samsung Medical Center, Seoul, Republic of
FFR-guided Complete vs. Culprit Only Revascularization in AMI Patients Ki Hong Choi, MD On Behalf of FRAME-AMI Investigators Heart Vascular Stroke Institute, Samsung Medical Center, Seoul, Republic of
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
PCI Update Qesaria 2009
 PCI Update Qesaria 2009 Amit Segev Interventional Cardiology Chaim Outline Primary PCI Non-ST elevation ACS Multi-vessel disease Hemodynamic assessment of borderline lesions - FFR Stable AP Non-coronary
PCI Update Qesaria 2009 Amit Segev Interventional Cardiology Chaim Outline Primary PCI Non-ST elevation ACS Multi-vessel disease Hemodynamic assessment of borderline lesions - FFR Stable AP Non-coronary
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Treatment of ST-elevation myocardial infarction in China: Where are we?
 Treatment of ST-elevation myocardial infarction in China: Where are we? Associate Professor, Yihong Sun, MD Peking University People s Hospital Beijing, China Disclosure conflict of Interest The Challenges
Treatment of ST-elevation myocardial infarction in China: Where are we? Associate Professor, Yihong Sun, MD Peking University People s Hospital Beijing, China Disclosure conflict of Interest The Challenges
Mild Hypothermia in Cardiogenic Shock Complicating Myocardial Infarction the Randomized SHOCK-COOL Trial
 Mild Hypothermia in Cardiogenic Shock Complicating Myocardial Infarction the Randomized SHOCK-COOL Trial Georg Fuernau, Johannes Beck, Steffen Desch, Ingo Eitel, Christian Jung, Sandra Erbs, Norman Mangner,
Mild Hypothermia in Cardiogenic Shock Complicating Myocardial Infarction the Randomized SHOCK-COOL Trial Georg Fuernau, Johannes Beck, Steffen Desch, Ingo Eitel, Christian Jung, Sandra Erbs, Norman Mangner,
Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI
 Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI Gamal Abdelhady, Emad Mahmoud Department of interventional
Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI Gamal Abdelhady, Emad Mahmoud Department of interventional
Management of STEMI in era of Reperfusion. Eagles Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police
 Management of STEMI in era of Reperfusion Eagles 2007 Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police STEMI in US ST Segment Elevation Myocardial Infarction (STEMI) ~500 K per year Thrombolysis
Management of STEMI in era of Reperfusion Eagles 2007 Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police STEMI in US ST Segment Elevation Myocardial Infarction (STEMI) ~500 K per year Thrombolysis
Influence of Location and Size of Myocardial Infarction on Post-infarction Remodelling
 Influence of Location and Size of Myocardial Infarction on Post-infarction Remodelling Masci PG, MD ; Ganame J, MD ; Francone M, MD, PhD # ; Desmet W, MD ; Iacucci I, MD # ; Barison A, MD ; Carbone I,
Influence of Location and Size of Myocardial Infarction on Post-infarction Remodelling Masci PG, MD ; Ganame J, MD ; Francone M, MD, PhD # ; Desmet W, MD ; Iacucci I, MD # ; Barison A, MD ; Carbone I,
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Ventricular tachycardia and ischemia. Martin Jan Schalij Department of Cardiology Leiden University Medical Center
 Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
Controversies on Primary angioplasty in STEMI
 Controversies on Primary angioplasty in STEMI 원주의대이승환 Case ( 51/M) CC C.C: ongoing squeezing chest pain D : for 2 hours Risk factors Current smoker ( 40 PYs) Hypercholesterolemia (+) Case ( 51/M) Physical
Controversies on Primary angioplasty in STEMI 원주의대이승환 Case ( 51/M) CC C.C: ongoing squeezing chest pain D : for 2 hours Risk factors Current smoker ( 40 PYs) Hypercholesterolemia (+) Case ( 51/M) Physical
BEDSIDE ASSESSMENT OF PATIENTS WITH STEMI
 BEDSIDE ASSESSMENT OF PATIENTS WITH STEMI Prof. Maria Dorobantu, PhD, FESC, FACC Emergency Hospital of Bucharest, Romania Presenter Disclosures There are no conflicts/ grants/ disclosures for this presentation.
BEDSIDE ASSESSMENT OF PATIENTS WITH STEMI Prof. Maria Dorobantu, PhD, FESC, FACC Emergency Hospital of Bucharest, Romania Presenter Disclosures There are no conflicts/ grants/ disclosures for this presentation.
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI
 Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
Thrombolysis, adjunctive pharmacology and interventions
 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation ESC Annual Congress Munich, 2012 Thrombolysis, adjunctive pharmacology and interventions
ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation ESC Annual Congress Munich, 2012 Thrombolysis, adjunctive pharmacology and interventions
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR
 PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
Is it safe to discharge patients 24 hours after uncomplicated successful primary percutaneous coronary intervention
 Is it safe to discharge patients 24 hours after uncomplicated successful primary percutaneous coronary intervention DA Jones, J Howard, S Gallagher, KS Rathod, A Jain, S Mohiddin, C Knight, A Mathur, EJ
Is it safe to discharge patients 24 hours after uncomplicated successful primary percutaneous coronary intervention DA Jones, J Howard, S Gallagher, KS Rathod, A Jain, S Mohiddin, C Knight, A Mathur, EJ
APPENDIX F: CASE REPORT FORM
 APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function?
 Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function? Avi Shimony, MD, FESC Cardiology Division Soroka University Medical Center Ben-Gurion University, Beer-Sheva Disclosure
Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function? Avi Shimony, MD, FESC Cardiology Division Soroka University Medical Center Ben-Gurion University, Beer-Sheva Disclosure
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
ST-Elevation Myocardial Infarction & Cardiogenic Shock. - What Should We Do?
 ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
Transfer in D2B. Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland. The Problem
 Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
Characteristics of Transient ST-Elevation versus ST-Elevation and Non-ST-Elevation Myocardial Infarction
 Characteristics of Transient ST-Elevation versus ST-Elevation and Non-ST-Elevation Myocardial Infarction Blondheim DS, Shochat M, Asif A, Kazatsker M, Frimerman A, Vassilenko L, Abu Fane R, Neiman E, Barel
Characteristics of Transient ST-Elevation versus ST-Elevation and Non-ST-Elevation Myocardial Infarction Blondheim DS, Shochat M, Asif A, Kazatsker M, Frimerman A, Vassilenko L, Abu Fane R, Neiman E, Barel
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki. 2013, American Heart Association
 NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
STEMI Care 2014 at the Crossroads: Taking the right road
 STEMI Care 2014 at the Crossroads: Taking the right road Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Vice President, The Canadian Association of Interventional Cardiology Director,
STEMI Care 2014 at the Crossroads: Taking the right road Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Vice President, The Canadian Association of Interventional Cardiology Director,
Mode of admission and its effect on quality indicators in Belgian STEMI patients
 2015 Mode of admission and its effect on quality indicators in Belgian STEMI patients Prof dr M Claeys National Coordinator STEMI registry 29-6-2015 Background The current guidelines for the management
2015 Mode of admission and its effect on quality indicators in Belgian STEMI patients Prof dr M Claeys National Coordinator STEMI registry 29-6-2015 Background The current guidelines for the management
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
PPCI in STEMI. ESC at the 22nd Annual Conference of the Saudi Heart Association February 21th, 2011
 PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
HOW TO PERFORM LEFT VENTRICULAR ASSISTANCE IN THE CATHLAB. Andreas Baumbach, MD FESC FRCP Bristol Heart Institute University Hospitals Bristol UK
 HOW TO PERFORM LEFT VENTRICULAR ASSISTANCE IN THE CATHLAB Andreas Baumbach, MD FESC FRCP Bristol Heart Institute University Hospitals Bristol UK Disclosure I have no conflicts of interest regarding this
HOW TO PERFORM LEFT VENTRICULAR ASSISTANCE IN THE CATHLAB Andreas Baumbach, MD FESC FRCP Bristol Heart Institute University Hospitals Bristol UK Disclosure I have no conflicts of interest regarding this
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft
 Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
New Horizons in Cardiogenic Shock. Timothy D. Henry, MD Director of Cardiology Cedars-Sinai Heart Institute
 New Horizons in Cardiogenic Shock Timothy D. Henry, MD Director of Cardiology Cedars-Sinai Heart Institute AMI Shock Mortality Unchanged in > 20 years 74355 US AMI/CGS cases per year 1,2 78954 78500 79823
New Horizons in Cardiogenic Shock Timothy D. Henry, MD Director of Cardiology Cedars-Sinai Heart Institute AMI Shock Mortality Unchanged in > 20 years 74355 US AMI/CGS cases per year 1,2 78954 78500 79823
Acute Myocardial Infarction Complicated by Cardiogenic Shock
 Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
STEMI AND MULTIVESSEL CORONARY DISEASE
 STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
Φαινόμενο No-Reflow. Απεικόνιση με CMR, κλινική συσχέτιση και προγνωστική σημασία
 Φαινόμενο No-Reflow. Απεικόνιση με CMR, κλινική συσχέτιση και προγνωστική σημασία Θεόδωρος. Καραμήτσος MD PhD Honorary Consultant in Cardiology University of Oxford Centre for Clinical Magnetic Resonance
Φαινόμενο No-Reflow. Απεικόνιση με CMR, κλινική συσχέτιση και προγνωστική σημασία Θεόδωρος. Καραμήτσος MD PhD Honorary Consultant in Cardiology University of Oxford Centre for Clinical Magnetic Resonance
and Treatment in Emergency Care) Trial: Intravenous Glucose, Insulin & Potassium (GIK) in Emergency Medical Services
 Trial: Intravenous Glucose, Insulin & Potassium (GIK) in Emergency Medical Services") Results of the IMMEDIATE (Immediate Myocardial Metabolic Enhancement DuringInitial Assessment and Treatment in Emergency Care) Trial: A Double Blinded Randomized Controlled Trial of Intravenous Glucose,
Results of the IMMEDIATE (Immediate Myocardial Metabolic Enhancement DuringInitial Assessment and Treatment in Emergency Care) Trial: A Double Blinded Randomized Controlled Trial of Intravenous Glucose,
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Timing of angiography for high- risk ACS
 Timing of angiography for high- risk ACS Christian Spaulding, MD, PhD, FESC, FACC Cardiology Department Cochin Hospital, Inserm U 970 Paris Descartes University Paris, France A very old story. The Interventional
Timing of angiography for high- risk ACS Christian Spaulding, MD, PhD, FESC, FACC Cardiology Department Cochin Hospital, Inserm U 970 Paris Descartes University Paris, France A very old story. The Interventional
Subsequent management and therapies
 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Subsequent management and therapies Marco Valgimigli, MD, PhD University of Ferrara ITALY
ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Subsequent management and therapies Marco Valgimigli, MD, PhD University of Ferrara ITALY
Acute Coronary Syndrome
 Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Update on the management of STEMI. Elliot Rapaport, M.D. San Francisco, CA December 14, 2007
 Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
STEMI Presentation and Case Discussion. Case #1
 STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST ESC Congress 2011 Pathophysiology of HFPEF Vascular Remodeling & Pulmonary Hypertension Carolyn S.P. Lam MBBS, MRCP, MS Case Presentation 81 yo woman with dyspnoea &
DECLARATION OF CONFLICT OF INTEREST ESC Congress 2011 Pathophysiology of HFPEF Vascular Remodeling & Pulmonary Hypertension Carolyn S.P. Lam MBBS, MRCP, MS Case Presentation 81 yo woman with dyspnoea &
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
MODULE 2 THE CLINICAL ENIGMA: RANDOMIZED TRIALS vs CLINICAL PRACTICE. Nico H. J. Pijls, MD, PhD Catharina Hospital Eindhoven The Netherlands
 MODULE 2 THE CLINICAL ENIGMA: RANDOMIZED TRIALS vs CLINICAL PRACTICE Nico H. J. Pijls, MD, PhD Catharina Hospital Eindhoven The Netherlands Disclosure All presenters have a speaker agreement with Maquet
MODULE 2 THE CLINICAL ENIGMA: RANDOMIZED TRIALS vs CLINICAL PRACTICE Nico H. J. Pijls, MD, PhD Catharina Hospital Eindhoven The Netherlands Disclosure All presenters have a speaker agreement with Maquet
Antonio Colombo. Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy. Miracor Symposium. Speaker: 15. Parigi: May 16-19, 2017
 Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Frans Van de Werf, MD, PhD Leuven, Belgium
 STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis
STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis