Primary PCI State of the Art. A/Prof Michael Nguyen Fremantle Hospital/Fiona Stanley Hospital Perth Australia JCR Meeting Busan 2014
|
|
|
- Horatio Welch
- 5 years ago
- Views:
Transcription
1 Primary PCI State of the Art A/Prof Michael Nguyen Fremantle Hospital/Fiona Stanley Hospital Perth Australia JCR Meeting Busan 2014
2 Content Evidence of Primary PCI vs Thrombolysis When, Why, How Transfer PCI Facilitated PCI Pharmacoinvasive approach To Aspirate or not to Aspirate Adjunctive anticoagulation Culprit only vs Preventative PCI My Overview
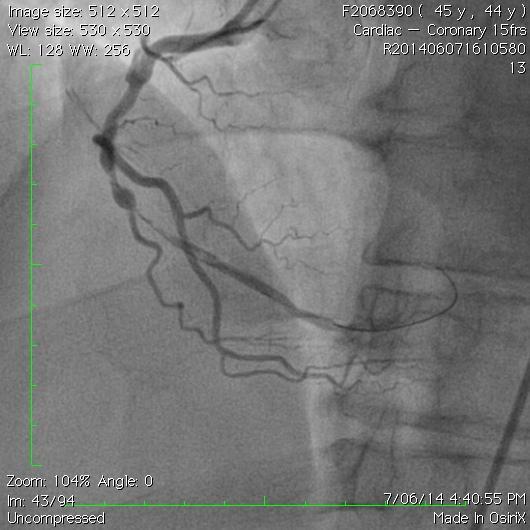
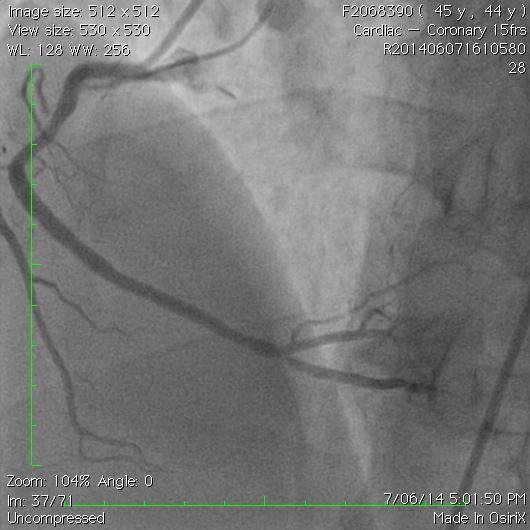
3 Case: Mr Complex 78 yo man presents with severe central chest pain to regional hospital (60 minutes from PCI capable hospital). Pain started 60 minute ago ECG 4 mm of inferior ST elevation PHX NIDDM Smoker Due to have prostatic surgery for prostate cancer
4 What next? Transfer PPCI? Thrombolysis and wait? Thrombolysis and transfer for rescue PCI if needed? Thrombolysis and invasive strategy irrespective of ST segment resolution?
5 Reperfusion Therapy Class I Recommendation All STEMI patients should undergo rapid evaluation for reperfusion therapy and have a reperfusion strategy implemented promptly after contact with the medical system. (Level of Evidence: A) Medical system goal is to facilitate rapid recognition and treatment of patients with STEMI such that door-to-needle (or medical contact to-needle) time for initiation of fibrinolytic therapy can be achieved within 30 minutes or that door-toballoon (or medical contact to-balloon) time for PCI can be kept within 90 minutes. Antman EM, et al. Available at: Accessed November 1, 2005.
6 Patient Mortality (%) Goal of Fibrinolytic Therapy Alone: Open Arteries and Reduce Mortality GUSTO-I (STK vs t-pa) Angiographic Investigators: Post-lytic TIMI Flow Predicts Mortality Days 2 Years 7.9 TIMI 3 TIMI 0,1,2 90 min TIMI Flow Post-fibrinolytic Ross AM, et al. Circulation. 1998;97:
7 Pharmacologic Reperfusion Class I Recommendations Available Resources STEMI patients presenting to a facility without the capability for expert, prompt intervention with primary PCI within 90 minutes of first medical contact should undergo fibrinolysis unless contraindicated (Level of Evidence: A) Antman EM, et al. J Am Coll Cardiol. Available at: Accessed November 1, 2005.
8 ACC/AHA STEMI Guidelines: Primary Percutaneous Coronary Intervention Class I Recommendations Level of Evidence: B Primary PCI should be performed as quickly as possible (goal of medical contact-to-balloon or door-to-balloon time < 90 minutes). If the symptom duration is within 3 hours and the expected door-to-balloon time minus the expected door-to-needle time is: < 60 mins - primary PCI preferred > 60 mins - fibrinolytic therapy preferred If symptom duration is greater than 3 hours, primary PCI is generally preferred. Antman EM, et al. J Am Coll Cardiol. Available at:

9 Time Dependency?
10 Absolute Risk Difference in Death (%) Mortality With 1 PCI Vs Time Circle sizes = sample size of the individual study. Solid line = weighted meta-regression. P = min Favors PCI Favors Lysis PCI-Related Time Delay (door-to-balloon, door to-needle) For every 10 min delay to PCI: 1% reduction in mortality difference vs lytics Nallamothu BK, Bates ER. Am J Cardiol. 2003:92:824
11 17 STEMI trials Received either Primary PCI (N=2267) Facilitated PCI (N=2237) PCI vs Faciliated PCI: Meta-analysis Short term outcomes (< 42 days) Death, CVA, non-fatal re-mi Urgent TVR, re-bleed Keely EC, Boura JA, Grines CL. Lancet, 2006
12 Facilitated PCI Meta-analysis f-pci (%) PCI (%) OR (95% CI) Initial TIMI (2.22, 4.45) Final TIMI (0.88, 1.64) Death (1.01, 1.87) Urgent TVR (1.23, 4.66) ICH P= Keely EC, Boura JA, Grines CL. Lancet, 2006
13 Facilitated PCI Meta-analysis Conclusions Facilitated PCI offers no benefit over primary PCI and should not be used outside of the context of randomized clinical trials Furthermore, facilitated interventions with thrombolytic based regimens should be avoided.







14 PCI Hospital Ambulance/ER STREAM design Pharmaco-invasive approach STEMI <3 hrs from onset symptoms, PPCI <60 min not possible, 2 mm ST-elevation in 2 leads RANDOMIZATION 1:1 by IVRS, OPEN LABEL Strategy A: pharmaco-invasive Strategy B: primary PCI <75y:full dose Aspirin Clopidogrel: LD 300 mg + 75 mg QD Enoxaparin: 30 mg IV + 1 mg/kg SC Q12h ECG at 90 min: ST resolution 50% YES After 75y: 20% ½ of dose the TNK planned recruitment, the TNK Aspirin dose was Clopidogrel: reduced by 75 mg QD 50% among Enoxaparin: patients years mg/kg of SC age. Q12h NO no lytic Antiplatelet and antithrombin treatment according to local standards angio >6 to 24 hrs PCI/CABG if indicated immediate angio + rescue PCI if indicated Standard primary PCI Primary endpoint: composite of all cause death or shock or CHF or reinfarction up to day 30 Armstrong et al NEJM 2013;368(15):
15 All-cause mortality
16 Cardiac mortality
17 All-cause mortality before & after amendment Patients randomized before Am. (n=382) Patients randomized after Am. (n=1,510)
18 Mr Complex Thrombolysis given at Regional hospital and patient transferred to your hospital. On arrival patient still has 2/10 pain and 2mm Inferior ST elevation What next?
19 Radial vs Femoral
20 RIFLE STEACS - flow chart Design 1001 patients enrolled between January 2009 and July 2011 in 4 clinical sites in Italy DESIGN: Prospective, randomized (1:1), parallel group, multi-center trial. Femoral arm (N=501) Radial arm (N=500) INCLUSION CRITERIA: all ST Elevation Myocardial infarction (STEMI) eligible for primary percutaneous coronary intervention. ESCLUSION CRITERIA: contraindication to any of both percutaneous arterial access. international normalized ratio (INR) > 2.0. Femoral arm (N=534) Clinical follow-up at 1 month in 100% Intention-to-treat analysis Radial arm (N=467) Clinical follow-up at 1 month in 100%
21 RIFLE STEACS results 30-day NACE rate p = femoral arm radial arm 21.0% 13.6% p = p = % 12.2% 7.2% 7.8% NACE MACCE Bleedings Net Adverse Clinical Event (NACE) = MACCE + bleeding
22 RIFLE STEACS results 30-day NACE rate p = femoral arm radial arm 21.0% 13.6% p = p = % 12.2% 7.2% 7.8% NACE MACCE Bleedings Net Adverse Clinical Event (NACE) = MACCE + bleeding Major Adverse Cardiac and Cerebrovascular event (MACCE) = composite of cardiac death, myocardial infarction, target lesion revascularization, stroke
23 RIFLE STEACS results 30-day MACCE rate p = femoral arm radial arm 9.2% 5.2% p = p = p = % 1.2% 1.8% 1.2% 0.6% 0.8% Cardiac death Myocardial Infarction Target Lesion Revascularization Cerebrovascular Accident
 0.001 LAD culprit 1.7 (1.2-2.6) 0.006 TIMI 0 basal 1.4 (1.0-2.1) 0.073 LVEF <50% 1.6 (1.1-2.5) 0.025 TIMI 0-1 final 2.4 (1.1-5.1) 0.024")
24 RIFLE STEACS results 30-day NACE predictors p= OR CI 95% p value Female gender 1.5 ( ) CKD 2.1 ( ) Radial access 0.6 ( ) Killip class 1.8 ( ) LAD culprit 1.7 ( ) TIMI 0 basal 1.4 ( ) LVEF <50% 1.6 ( ) TIMI 0-1 final 2.4 ( ) 0.024
25 STEMI-RADIAL A Prospective Randomized Trial of Radial vs. Femoral Access in Patients with ST-Segment Elevation Myocardial Infarction
26 STEMI-RADIAL - objectives To compare radial vs femoral approach in primary PCI for patients with STEMI < 12 hours in very high volume radial centers (> 80% primary PCI)
27 STEMI RADIAL - results 30-day bleeding and access site compl. femoral radial 5.3% 2.8% 1.1% 0.3% 0.3% 0.3% 0.9% 0.6% 0.8% 0.8% 0.0% 0.3% Gastrointestinal Hb drop 4g/dL w/o overt Hb drop 3g/dL with overt Hematoma 15cm Transfusion Vascular complication
28 STEMI RADIAL - results 30-day MACE femoral arm radial arm p = % 3.5% 3.1% p = % p = % 1.2% p = % 0.3% MACE Death MI Stroke MACE = composite of death, myocardial infarction and stroke

29

30

31
32 Anticoagulation? Heparin alone? Heparin and Glycoprotein 2b3a? Bivalirudin?
 R 1:1 Bivalirudin monotherapy (± provisional GP IIb/IIIa) Emergent angiography, followed")

33 Harmonizing Outcomes with Revascularization and Stents in AMI 3602 pts with STEMI with symptom onset 12 hours Aspirin, thienopyridine UFH + GP IIb/IIIa inhibitor (abciximab or eptifibatide) R 1:1 Bivalirudin monotherapy (± provisional GP IIb/IIIa) Emergent angiography, followed by triage to CABG Primary PCI Medical Rx 3006 pts eligible for stent randomization R 3:1 Paclitaxel-eluting TAXUS stent Bare metal EXPRESS stent Clinical FU at 30 days, 6 months, 1 year, and then yearly through 3 years; angio FU at 13 months Stone, GW N Engl J Med 2008;358:
34 Major Bleeding (%) 3-Year Major Bleeding (non-cabg)* Bivalirudin alone (n=1800) Heparin + GPIIb/IIIa (n=1802) 10.5% % 6.0% 6.9% 3-yr HR (95%CI) 0.64 (0.51, 0.80) 2 P= Months * Intracranial, intraocular, retroperitoneal, access site bleed requiring intervention/surgery, hematoma 5 cm, hgb 3g/dL with or 4g/dL w/o overt source; reoperation for bleeding; or blood product transfusion Stone, GW Lancet 2011 Published online June 13. DOI: /S (11)
35 Cardiac Mortality (%) ' Time in Months 3-Year Cardiac Mortality Time in Months Heparin + GPIIb/IIIa (n=1802) Bivalirudin alone (n=1800) yr HR (95%CI) 0.56 (0.40, 0.80) P= % % 2.1% 2.9% Months Stone, GW Lancet 2011 Published online June 13. DOI: /S (11)
 Bivalirudin (n=1800) 3 year HR (95% CI) 0.49 0.28 0.86 p=0.01 2.2% 1.")
36 Cardiac mortality (%) 3-Year Cardiac Mortality Landmark analysis day HR (95% CI) 0.62 ( ) p= % 1.8% Heparin + GP IIb/IIIa (n=1802) Bivalirudin (n=1800) 3 year HR (95% CI) p= % 1.1% Months Stone, GW Lancet 2011 Published online June 13. DOI: /S (11)
37 Reinfarction (%) 3-Year Reinfarction Bivalirudin alone (n=1800) Heparin + GPIIb/IIIa (n=1802) 8.2% % 3.6% 6.2% 3-yr HR (95%CI) 0.76 (0.59, 0.99) P= Months Stone, GW Lancet 2011 Published online June 13. DOI: /S (11)
 Bivalirudin (n=1800) 0 3 6 9 12 15 18 21 24 27 30 33 36 4.4% Months Stone, GW Lancet 2011 Published online June 13. DOI:10.")
38 Reinfarction (%) 3-Year Reinfarction Landmark analysis day HR (95% CI) 3-year HR (95% CI) 1.07 ( ) p= ( ) p= % 1.9% 1.8% Heparin + GPIIb/IIIa (n=1802) Bivalirudin (n=1800) % Months Stone, GW Lancet 2011 Published online June 13. DOI: /S (11)
39 3-Year Stent Thrombosis (ARC Definite/Probable) Stent Thrombosis (%) Bivalirudin alone (n=1611) Heparin + GPIIb/IIIa (n=1591) 3.5% 5.1% 4.5% % HR (95%CI) 0.89 (0.65, 1.23) p= Months ARC= Academic Research Consortium Stone, GW Lancet 2011 Published online June 13. DOI: /S (11)
40 How Effective are Antithrombotic Therapies in PPCI Dr Adeel Shahzad Dr Rod Stables (PI) Liverpool Heart and Chest Hospital Liverpool, UK
41 Single centre RCT Trial recruitment: Feb Nov 2013 Bivalirudin v Unfractionated Heparin 22 months STEMI patients Randomised at presentation Acute phase management with Primary PCI Philosophy for clinical teams: Assess Every Patient - Every Time
42 1917 patients scheduled for emergency angiography 29 (1.5%) already randomised in the trial 59 (3.0%) met one or more other exclusion criteria 1829 eligible for recruitment
43 1917 patients scheduled for emergency angiography 29 (1.5%) already randomised in the trial 59 (3.0%) met one or more other exclusion criteria 1829 eligible for recruitment 1829 Randomised Representative Real-World Population
44 Characteristic Bivalirudin (%) Heparin (%) P2Y12 use - Any Clopidogrel Prasugrel Ticagrelor GPI use Radial arterial access PCI performed
45 Dual oral anti-platelet therapy pre-procedure Heparin: 70 units/kg body weight pre-procedure Bivalirudin: Bolus 0.75 mg/kg Infusion 1.75 mg/kg/hr - procedure duration GPI - Abciximab Selective ( bailout ) use in both groups ESC guideline indications
46
47 Bivalirudin Heparin n % % n MACE % v 5.7 % 52 Absolute risk increase = 3.0% (95% CI 0.6, 5.4) Relative risk = 1.52 (95% CI ) P=0.01
48 Event curve shows first event experienced
49 Bivalirudin Heparin n % % n Death % v 4.3 % 39 CVA % v 1.2% 11 Reinfarction % v 0.9% 8 TLR % v 0.7% 6 Any MACE % v 5.7 % 52
50 Bivalirudin Heparin n % % n Death % v 4.3 % 39 CVA % v 1.2% 11 Reinfarction % v 0.9% 8 TLR % v 0.7% 6 Any MACE % v 5.7 % 52
51 ARC definite or probable stent thrombosis events Bivalirudin Heparin n % % n All Events % v 0.9 % 6 Relative risk = 3.91 (95% CI ) P=0.001
52 Major Bleed BARC grade 3-5 Bivalirudin Heparin n % % n Major Bleed % v 3.1 % 28 Relative risk = 1.15 (95% CI ) P=0.59
53 Mr Complex Heparin alone with plan for GPIIb/IIIa bailout Thrombectomy?
54 Bivalirudin versus Heparin and Heparin plus Tirofiban in Patients with AMI Undergoing PCI Thirty-Day and One-Year Outcomes of the BRIGHT Trial Yaling Han, MD, FACC On behalf of the BRIGHT investigators
55 Trial Design (clinicaltrials.gov number: NCT ) 2194 patients with AMI eligible for emergent PCI R Bivalirudin alone N=735 Biv 0.75mg/kg bolus mg /kg/h infusion (0.3mg/kg bolus if ACT< 225s). Bailout GPI permitted. Biv infusion (0.2mg/kg/h) continued for at least 30 min post PCI. Heparin alone N=729 Heparin 100U/kg bolus + additional dose if ACT <200 s. Bailout GPI permitted ACT goal = Heparin plus tirofiban N=730 Heparin 60U/kg bolus. Tirofiban 10μg/kg bolus μg/kg/min infusion for h. ACT goal = Clinical follow-up at 30 days and one year
, NNT=12.3 - UFH vs. H+T, p=0.04 Relative risk 0.78 (0.61-0.99), NNT=26.2 P=0.74 P<0.")
56 Primary and Principal Secondary Endpoint Events at 30 Days (%) P< Biv vs. UFH, p=0.009 Relative risk 0.67 ( ), NNT= Biv vs. H+T, p < Relative risk 0.52 ( ), NNT= UFH vs. H+T, p=0.04 Relative risk 0.78 ( ), NNT=26.2 P=0.74 P<0.001 Biv=bivalirudin; UFH=Heparin; H+T=heparin + tirofiban
 P=0.02 (Biv vs. H+T) Biv=bivalirudin; UFH=Heparin; H+T=heparin + tirofiban")
57 (%) Safety Endpoints at 30 days P=0.77 (3-way) P=0.07 (3-way) P=0.04 (Biv vs. pooled H) P=0.12 (Biv vs. UFH) P=0.02 (Biv vs. H+T) Biv=bivalirudin; UFH=Heparin; H+T=heparin + tirofiban
58
59 Thrombus Aspiration During PCI for STEMI NEW Recommendation I IIa IIb III Aspiration thrombectomy is reasonable for patients undergoing primary PCI 59

60 Thrombus Aspiration during Percutaneous coronary intervention in Acute myocardial infarction Study (TAPAS) Mortality and reinfarction at 1 year F. Zijlstra, MD PhD Thoraxcenter University Medical Center Groningen, The Netherlands FZ
61 1071 STEMI patients randomized 535 were assigned to thrombus aspiration 536 were assigned to conventional PCI 33 did not undergo PCI 502 underwent primary PCI 295 underwent TA followed by direct stenting 153 underwent TA with additional balloon dilation 54 had crossover to conventional PCI 33 did not undergo PCI 503 underwent primary PCI 485 underwent balloon dilation followed by stenting 12 underwent conventional PCI with additional TA 6 had crossover to TA 530 complete follow-up at 1 year 530 complete follow-up at 1 year FZ
62 Mortality at 1 year 12 Conventional PCI Thrombus-Aspiration 10 Mortality (%) Log-Rank p = Time (days) *Unpublished results
63 Mortality or non-fatal ReMI at 1 year Death or Reinfarction (%) 12 Conventional PCI Thrombus-Aspiration Log-Rank p = Time (days) *Unpublished results

64 UCR Uppsala Clinical Research Center Thrombus Aspiration in ST- Elevation myocardial infarction in Scandinavia (TASTE trial) trial hypothesis Aspiration of the blood clot or thrombus that causes a heart attack, before balloon dilatation and stenting, improves survival Ole Fröbert, MD, PhD - on behalf of the TASTE investigators Departement of Cardiology Örebro University Hospital Sweden
65 Methods 29 Swedish, 1 Danish and 1 Icelandic hospital Multicenter, prospective, randomized, controlled open-label trial enrolling 7244 patients who had a diagnosis of STelevation myocardial infarction (STEMI) Novel Registry-Based Randomized Clinical Trial concept: national heart registries served as platforms for randomization, case reports and follow-up no patients lost to follow-up powerful tool to capture outcome data with a high degree of fidelity inexpensive Half of the patients were assigned to balloon treatment only (known as percutaneous coronary intervention, or PCI) and the other half had their blood clot aspirated before PCI
66 TASTE and previous studies on thrombus aspiration TASTE TASTE TAPAS JETSTENT AIMI INFUSE-AMI VAMPIRE PREPARE Chevalier Kaltoft MUSTELA X AMINE ST PIHRATE EXPIRA DEAR-MI Liistro Number of patients
67 All-cause mortality at 30 days HR 0.94 ( ), P=0.63
68 Thrombectomy? Case by case Large thrombus burden Complete occlusion of vessel acts as significant adjunct to PPCI procedure.
69
70
71 Mr Complex What next? PCI to non-culprit lesion during same procedure PCI to non-culprit before discharge? PCI to non-culprit in 2 weeks? PCI only if refractory angina? PCI only if objective evidence of ischemia with functional tesing? Refer for CABG? (NIDDM, Multi-vessel disease)
72 Primary PCI in STEMI (ACC 2013 STEMI guidelines) I IIa IIb III Primary PCI is reasonable in patients with STEMI if there is clinical and/or ECG evidence of ongoing ischemia between 12 and 24 hours after symptom onset. I IIa IIb III Harm PCI should not be performed in a noninfarct artery at the time of primary PCI in patients with STEMI who are hemodynamically stable

73 Preventive Angioplasty in Myocardial Infarction Trial PRAMI Trial Randomised multicentre single-blind trial conducted in five UK cardiac centres N Engl J Med September 1 st 2013;369. DOI: /NEJMoa
, p<0.")
74 Cardiac Death, Nonfatal MI or Refractory Angina in patients having infarct-artery PCI Hazard Ratio 0.35 (95% CI 0.21 to 0.58), p<0.001 Risk Reduction 65% n=234 n=231
75 Cardiac Death, Nonfatal MI or Refractory Angina in patients having infarct-artery PCI Hazard Ratio 0.36 (95% CI 0.18 to 0.73), p= Risk Reduction 64% 11 Preventive PCI No Preventive PCI n=234 n=231
76 Prami

77 CVLPRIT trial
78 Content My Overview Evidence of Primary PCI vs Thrombolysis When, Why, How Primary PCI in PCI capable hospital. DTB < 90min Transfer PCI DTB <120 min from FMC Pharmaco-invasive approach is preferred option if patient presents < 3hrs and Primary or Transfer PCI unable to be achieved. To Aspirate or not to Aspirate Jury is out. Individual cases selection. Reasonable for high thrombotic burden to aid with PCI procedure.
79 CONTENT My Overview Adjunctive anticoagulation - Heparin with GP Iib/IIIa bailout is reasonable especially with radial access. Data conflicting Culprit only vs Preventative PCI Preventative PCI reasonable option however timing is open at time of procedure, before discharge, few weeks after discharge, following objective evidence of ischemia all reasonable.
Bivalirudin Clinical Trials Update Evidence and Future Perspectives
 Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION. STREAM 1Y AHA 2013 P Sinnaeve
 STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
Pharmaco-Invasive Approach for STEMI
 Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI
 HORIZONS-AMI: A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI Gregg W. Stone MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Gregg W. Stone
HORIZONS-AMI: A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI Gregg W. Stone MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Gregg W. Stone
Is the role of bivalirudin established?
 Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
The Strategic Reperfusion Early After STEMI study Implications for clinical practice
 The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
Novel Anticoagulation Therapy in Acute Coronary Syndrome
 Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction. Is it beneficial to patients?
 Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Updated and Guideline Based Treatment of Patients with STEMI
 Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN
 What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN October 2011 Part 2 Summary of newer antithrombotic and antiplatelet agents in STEMI Role of thrombectomy in PPCI
What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN October 2011 Part 2 Summary of newer antithrombotic and antiplatelet agents in STEMI Role of thrombectomy in PPCI
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology
 Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
Columbia University Medical Center Cardiovascular Research Foundation
 STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
Update on Antithrombotic Therapy in Acute Coronary Syndrome
 Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
From STEMIs to Stents: Updates in PCI practice
 From STEMIs to Stents: Updates in PCI practice Arnold Seto, MD, MPA Assistant Clinical Professor, UC-Irvine and Long Beach VA Director of Interventional Cardiology Research Hospitalizations in the U.S.
From STEMIs to Stents: Updates in PCI practice Arnold Seto, MD, MPA Assistant Clinical Professor, UC-Irvine and Long Beach VA Director of Interventional Cardiology Research Hospitalizations in the U.S.
New Insights on Reperfusion Choices Implications of STREAM. Paul W Armstrong MD
 New Insights on Reperfusion Choices Implications of STREAM ESC STEMI Satellite Symposium August 31 2014 Aligning Optimal Care to Time Place and Person Paul W Armstrong MD Disclosure Statement Paul W. Armstrong
New Insights on Reperfusion Choices Implications of STREAM ESC STEMI Satellite Symposium August 31 2014 Aligning Optimal Care to Time Place and Person Paul W Armstrong MD Disclosure Statement Paul W. Armstrong
The Window for Fibrinolysis. Frans Van de Werf, MD, PhD Leuven, Belgium
 The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
Thrombus Aspiration in ST- Elevation myocardial infarction in Scandinavia (TASTE trial)
") UCR Uppsala Clinical Research Center Thrombus Aspiration in ST- Elevation myocardial infarction in Scandinavia (TASTE trial) Main results at 30 days Ole Fröbert, MD, PhD - on behalf of the TASTE investigators
UCR Uppsala Clinical Research Center Thrombus Aspiration in ST- Elevation myocardial infarction in Scandinavia (TASTE trial) Main results at 30 days Ole Fröbert, MD, PhD - on behalf of the TASTE investigators
Optimal antithrombotic therapy:
 Optimal antithrombotic therapy: upstream and during primary PCI. Steen D Kristensen, MD, DMSc, FESC Professor and Consultant Interventional Cardiologist Aarhus University, Denmark UNIVERSITY OF AARHUS
Optimal antithrombotic therapy: upstream and during primary PCI. Steen D Kristensen, MD, DMSc, FESC Professor and Consultant Interventional Cardiologist Aarhus University, Denmark UNIVERSITY OF AARHUS
PPCI in STEMI. ESC at the 22nd Annual Conference of the Saudi Heart Association February 21th, 2011
 PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
Thrombus Aspiration before PCI: Routine Mandatory. Professor Clinical Cardiology Academic Medical Center University of Amsterdam
 Seoul, 27 April TCT AP 2010 Thrombus Aspiration before PCI: Routine Mandatory Robbert J de Winter MD PhD FESC Professor Clinical Cardiology Academic Medical Center University of Amsterdam AMC Amsterdam
Seoul, 27 April TCT AP 2010 Thrombus Aspiration before PCI: Routine Mandatory Robbert J de Winter MD PhD FESC Professor Clinical Cardiology Academic Medical Center University of Amsterdam AMC Amsterdam
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Update on the management of STEMI. Elliot Rapaport, M.D. San Francisco, CA December 14, 2007
 Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
ST-Elevation MI: Update on Bivalirudin and DES
 ST-Elevation MI: Update on Bivalirudin and DES George D. Dangas, MD, FACC, FSCAI, FAHA Professor of Medicine Director, Cardiovascular Innovation Mount Sinai Medical Center, New York, NY Disclosure Research
ST-Elevation MI: Update on Bivalirudin and DES George D. Dangas, MD, FACC, FSCAI, FAHA Professor of Medicine Director, Cardiovascular Innovation Mount Sinai Medical Center, New York, NY Disclosure Research
bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company
 SMC No. (638/10) The Medicines Company") bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company 06 August 2010 The Scottish Medicines Consortium (SMC) has completed its
bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company 06 August 2010 The Scottish Medicines Consortium (SMC) has completed its
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI
 Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI Charles A. Simonton MD, FACC, FSCAI Sanger Clinic Medical Director Clinical Innovation and Research Carolinas Heart
Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI Charles A. Simonton MD, FACC, FSCAI Sanger Clinic Medical Director Clinical Innovation and Research Carolinas Heart
PHARMACO-INVASIVE STRATEGY COMPARED WITH PPCI: DESIGN AND MAIN OUTCOMES OF THE STREAM TRIAL
 PHARMACO-INVASIVE STRATEGY COMPARED WITH PPCI: DESIGN AND MAIN OUTCOMES OF THE STREAM TRIAL Frans Van de Werf Leuven, Belgium Disclosures Study grant from Boehringer Ingelheim to perform the STREAM trial,
PHARMACO-INVASIVE STRATEGY COMPARED WITH PPCI: DESIGN AND MAIN OUTCOMES OF THE STREAM TRIAL Frans Van de Werf Leuven, Belgium Disclosures Study grant from Boehringer Ingelheim to perform the STREAM trial,
The Need for Rescue PCI after Failed Fibrinolysis: Who, When and Why.
 Implementing the pharmacoinvasive strategy in STEMI The Need for Rescue PCI after Failed Fibrinolysis: Who, When and Why. 7:20-7:40 Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Director,
Implementing the pharmacoinvasive strategy in STEMI The Need for Rescue PCI after Failed Fibrinolysis: Who, When and Why. 7:20-7:40 Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Director,
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies
 Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
STEMI AND MULTIVESSEL CORONARY DISEASE
 STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
Otamixaban for non-st-segment elevation acute coronary syndrome
 Otamixaban for non-st-segment elevation acute coronary syndrome September 2011 This technology summary is based on information available at the time of research and a limited literature search. It is not
Otamixaban for non-st-segment elevation acute coronary syndrome September 2011 This technology summary is based on information available at the time of research and a limited literature search. It is not
Trial Update- TOTAL. Jonathan Byrne
 Trial Update- TOTAL Jonathan Byrne No conflicts of interest Background- rationale for thrombectomy Major Limitation of primary PCI: distal embolisation and reduced flow Stonel JACC 2002;39:591-7 Henriques
Trial Update- TOTAL Jonathan Byrne No conflicts of interest Background- rationale for thrombectomy Major Limitation of primary PCI: distal embolisation and reduced flow Stonel JACC 2002;39:591-7 Henriques
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting
 How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
Pathophysiology of ACS
 Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Thrombolysis, adjunctive pharmacology and interventions
 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation ESC Annual Congress Munich, 2012 Thrombolysis, adjunctive pharmacology and interventions
ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation ESC Annual Congress Munich, 2012 Thrombolysis, adjunctive pharmacology and interventions
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department
: Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department") ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department decision-making. They have become the cornerstone of many ED protocols for
ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department decision-making. They have become the cornerstone of many ED protocols for
STEMI: Eight Areas of Unmet Needs
 STEMI: Eight Areas of Unmet Needs Paul A. Gurbel, M.D. Sinai Center for Thrombosis Research, Baltimore, Maryland, U.S.A. Professor of Medicine, Johns Hopkins University School of Medicine Adjunct Professor
STEMI: Eight Areas of Unmet Needs Paul A. Gurbel, M.D. Sinai Center for Thrombosis Research, Baltimore, Maryland, U.S.A. Professor of Medicine, Johns Hopkins University School of Medicine Adjunct Professor
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 9, 2013
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
STEMI Primary Percutaneous Coronary Intervention
 STEMI Primary Percutaneous Coronary Intervention Abdul Razek Maaty, MD Professor of Medicine Outline Primary PCI Aspiration, manual thrombectomy and distal protection devices Choice of stent Pharmacothaerpy,
STEMI Primary Percutaneous Coronary Intervention Abdul Razek Maaty, MD Professor of Medicine Outline Primary PCI Aspiration, manual thrombectomy and distal protection devices Choice of stent Pharmacothaerpy,
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI
 Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Scottish Medicines Consortium
 Scottish Medicines Consortium bivalirudin, 250mg powder for concentrate for solution for injection or infusion (Angiox ) No. (516/08) The Medicines Company UK Ltd 07 November 2008 The Scottish Medicines
Scottish Medicines Consortium bivalirudin, 250mg powder for concentrate for solution for injection or infusion (Angiox ) No. (516/08) The Medicines Company UK Ltd 07 November 2008 The Scottish Medicines
Cindy L. Grines MD FACC FSCAI
 Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation?
 What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation? Keun-Ho Park, Myung Ho Jeong, Min Goo Lee, Jum Suk Ko,
What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation? Keun-Ho Park, Myung Ho Jeong, Min Goo Lee, Jum Suk Ko,
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Myocardial Infarction In Dr.Yahya Kiwan
 Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
The Role of DHMC as an ST Elevation Myocardial Infarction Receiving Center in a Regional STEMI Care Network:
 The Role of DHMC as an ST Elevation Myocardial Infarction Receiving Center in a Regional STEMI Care Network: Nathaniel Niles, MD CREST Symposium November 7th, 28 STEMI = Acute Coronary Thrombosis STEMI
The Role of DHMC as an ST Elevation Myocardial Infarction Receiving Center in a Regional STEMI Care Network: Nathaniel Niles, MD CREST Symposium November 7th, 28 STEMI = Acute Coronary Thrombosis STEMI
M/39 CC D. => peak CKMB (12 hr later) ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #
 ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #") Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI
 Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
 A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC
 Mitchell W. Krucoff, MD, FACC") Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Bivalirudin should be indicated for all patients with STEMI. Adnan Kastrati Deutsches Herzzentrum, Munich, Germany
 Bivalirudin should be indicated for all patients with STEMI Adnan Kastrati Deutsches Herzzentrum, Munich, Germany 1 Heparin+IIb/IIIa, heparin alone or bivalirudin in STEMI: Do we have the answer? 2 Heparin+IIb/IIIa,
Bivalirudin should be indicated for all patients with STEMI Adnan Kastrati Deutsches Herzzentrum, Munich, Germany 1 Heparin+IIb/IIIa, heparin alone or bivalirudin in STEMI: Do we have the answer? 2 Heparin+IIb/IIIa,
Is there a real need for new agents to optimize efficacy/safety balance
 Anticoagulation in acute coronary syndrome Is there a real need for new agents to optimize efficacy/safety balance Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures
Anticoagulation in acute coronary syndrome Is there a real need for new agents to optimize efficacy/safety balance Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures
Optimal Duration and Dose of Antiplatelet Therapy after PCI
 Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction
 Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Frans Van de Werf, MD, PhD Leuven, Belgium
 STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis
STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis
QUT Digital Repository:
 QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI
 Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI Gamal Abdelhady, Emad Mahmoud Department of interventional
Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI Gamal Abdelhady, Emad Mahmoud Department of interventional
Revived indications for thrombus aspiration during primary PCI: Unanswered questions after TAPAS
 Revived indications for thrombus aspiration during primary PCI: Unanswered questions after TAPAS Gregg W. Stone MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Gregg
Revived indications for thrombus aspiration during primary PCI: Unanswered questions after TAPAS Gregg W. Stone MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Gregg
PERCUTANEOUS CORONARY INTERVENTION AND BLEEDING COMPLICATIONS
 PERCUTANEOUS CORONARY INTERVENTION AND BLEEDING COMPLICATIONS *Sudhakar George, 1 Rob Butler, 1,2 James Nolan, 1,2 Mamas A. Mamas 1,2 1. Royal Stoke University Hospital, Stoke-on-Trent, UK 2. Keele Cardiovascular
PERCUTANEOUS CORONARY INTERVENTION AND BLEEDING COMPLICATIONS *Sudhakar George, 1 Rob Butler, 1,2 James Nolan, 1,2 Mamas A. Mamas 1,2 1. Royal Stoke University Hospital, Stoke-on-Trent, UK 2. Keele Cardiovascular
Transfer in D2B. Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland. The Problem
 Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 8, 2014
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Primary PCI in patients with STEMI Abbott Vascular. All rights reserved.
 Primary PCI in patients with STEMI Primary PCI in patients with STEMI Agenda 2 Primary PCI in patients with STEMI Definition: angioplasty ± stenting without prior or concomitant fibrinolytic therapy Objectives
Primary PCI in patients with STEMI Primary PCI in patients with STEMI Agenda 2 Primary PCI in patients with STEMI Definition: angioplasty ± stenting without prior or concomitant fibrinolytic therapy Objectives
Management of ST-elevation myocardial infarction Update 2009 Late comers: which options?
 European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
MULTIcentre evaluation of Single high-dose. acute myocardial infarction study
 MULTIcentre evaluation of Single high-dose Tirofiban bolus TiRofiban vs. versus with sirolimus eluting stent or barein metal stent in during primary PCI STEMI acute myocardial infarction study M. Valgimigli,
MULTIcentre evaluation of Single high-dose Tirofiban bolus TiRofiban vs. versus with sirolimus eluting stent or barein metal stent in during primary PCI STEMI acute myocardial infarction study M. Valgimigli,
Thrombolysis in Acute Myocardial Infarction
 CHAPTER 70 Thrombolysis in Acute Myocardial Infarction J. S. Hiremath Introduction Reperfusion of the occluded coronary artery at the earliest is the most important aim of management of STEMI. Once a flow
CHAPTER 70 Thrombolysis in Acute Myocardial Infarction J. S. Hiremath Introduction Reperfusion of the occluded coronary artery at the earliest is the most important aim of management of STEMI. Once a flow
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Horizon Scanning Centre November 2012
 Horizon Scanning Centre November 2012 Cangrelor to reduce platelet aggregation and thrombosis in patients undergoing percutaneous coronary intervention99 SUMMARY NIHR HSC ID: 2424 This briefing is based
Horizon Scanning Centre November 2012 Cangrelor to reduce platelet aggregation and thrombosis in patients undergoing percutaneous coronary intervention99 SUMMARY NIHR HSC ID: 2424 This briefing is based
STEMI Presentation and Case Discussion. Case #1
 STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
Update on STEMI Guidelines. Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center
 Update on STEMI Guidelines Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center All Rights Reserved, Duke Medicine 2008 Disclosures Research Grants: NHLB, AHRQ, AstraZeneca,
Update on STEMI Guidelines Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center All Rights Reserved, Duke Medicine 2008 Disclosures Research Grants: NHLB, AHRQ, AstraZeneca,
Critical Review Form Therapy Objectives: Methods:
 Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
Approach to Multi Vessel disease with STEMI
 Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Diabetic Patients: Current Evidence of Revascularization
 Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki. 2013, American Heart Association
 NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
Registerbaserade randomiserade kliniska pro vningar Innovativa exempel fra n dagens pa ga ende hja rt- forskning i Sverige
 Registerbaserade randomiserade kliniska pro vningar Innovativa exempel fra n dagens pa ga ende hja rt- forskning i Sverige SWEDE HEART Stefan James, Professor Kardiologi Vetenskaplig ledeare UCR, Uppsala
Registerbaserade randomiserade kliniska pro vningar Innovativa exempel fra n dagens pa ga ende hja rt- forskning i Sverige SWEDE HEART Stefan James, Professor Kardiologi Vetenskaplig ledeare UCR, Uppsala
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI?
 SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
EXAMINATION trial. Manel Sabaté Hospital Clínic, Barcelona (On behalf of the Examination Investigators)
") Manel Sabaté Hospital Clínic, Barcelona (On behalf of the Examination Investigators) Disclosures Investigator Initiated Trial: NCT00828087. Unrestricted grant from Abbott to the Spanish Heart Foundation.
Manel Sabaté Hospital Clínic, Barcelona (On behalf of the Examination Investigators) Disclosures Investigator Initiated Trial: NCT00828087. Unrestricted grant from Abbott to the Spanish Heart Foundation.
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008.
 Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
PCI Update Qesaria 2009
 PCI Update Qesaria 2009 Amit Segev Interventional Cardiology Chaim Outline Primary PCI Non-ST elevation ACS Multi-vessel disease Hemodynamic assessment of borderline lesions - FFR Stable AP Non-coronary
PCI Update Qesaria 2009 Amit Segev Interventional Cardiology Chaim Outline Primary PCI Non-ST elevation ACS Multi-vessel disease Hemodynamic assessment of borderline lesions - FFR Stable AP Non-coronary
The role of pre hospital thrombolysis. Aaron Frimerman Hillel Yaffe Medical Center Hadera Israel
 The role of pre hospital thrombolysis Aaron Frimerman Hillel Yaffe Medical Center Hadera Israel Is thrombolysis still valid? Disclosure I am an Interventional Cardiologist STEMI is mainly a thrombotic
The role of pre hospital thrombolysis Aaron Frimerman Hillel Yaffe Medical Center Hadera Israel Is thrombolysis still valid? Disclosure I am an Interventional Cardiologist STEMI is mainly a thrombotic
Patient Transfer. Mark de Belder The James Cook University Hospital Middlesbrough
 Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
ORIGINAL ARTICLE. Rescue PCI Versus a Conservative Approach for Failed Fibrinolysis in Patients with STEMI
 Heart Mirror Journal From Affiliated Egyptian Universities and Cardiology Centers Vol. 6, No. 3, 2012 ISSN 1687-6652 ORIGINAL ARTICLE for Failed Fibrinolysis in Patients with STEMI Mohamed Salem, MD, PhD;
Heart Mirror Journal From Affiliated Egyptian Universities and Cardiology Centers Vol. 6, No. 3, 2012 ISSN 1687-6652 ORIGINAL ARTICLE for Failed Fibrinolysis in Patients with STEMI Mohamed Salem, MD, PhD;
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations