The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
|
|
|
- Sharon Todd
- 6 years ago
- Views:
Transcription
1 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin

2 Norman Barrett Smiles
3 [A brief digression - Chair becoming anxious now] The Role of the Pathologist in Excluding Barrett s in the First Place
 or worse still features consistent with Barrett s when it is not Lifelong surveillance anyone?")
4 How common is this scenario in your practice? Endoscopist says:? Barrett s Endoscopist does: biopsies from oesophagogastric junction Pathologist says: Blah, blah, blah (i.e. a descriptive report without conclusion) or worse still features consistent with Barrett s when it is not Lifelong surveillance anyone?
5 A full endoscopic report What is needed? Endoscopic impression as to the presence or absence of Barrett s and its extent Biopsies from the native oesophagus - clearly designated A pathologist who is alert to the diagnostic possibilities Pathology report - useful to the clinician and therefore the patient [New BSG guidelines]


6 2004 Biopsy HGD Oesophagectomy

7 Oesophageal Mapping Biopsies
 EUS EMR ESD Ablation")
8 2015 Radically Changed Model Biopsies +++ (multiwell blocks) EUS EMR ESD Ablation Oesophagectomy
9 2015 Radically Changed Model Central role in the multidisciplinary management Challenge our existing practices Improve the reproducibility of our analysis Provide clinically useful reports
10 Classification of Dysplasia/Neoplasia in Barrett s No dysplasia Indefinite for dysplasia Low grade dysplasia High grade dysplasia Intramucosal adenocarcinoma (at least) Invasive adenocarcinoma


11 Examples of short and comprehensive proformas for reporting histopathology diagnosis and surveillance biopsy findings. BSG guidelines (Fitzgerald et al. Gut 2014; 63:7-42)

12 Low Grade Dysplasia Nuclei enlarged, crowded, hyperchromatic, ovoid May have visible nucleoli Mitoses + Usually stratified Changes reach the luminal surface Discernible demarcation useful when present Goblet cells usually lost Interobserver agreement not great
13 Foveolar Dysplasia Other Patterns of Dysplasia in Barrett s Little or no loss of nuclear polarity Easily missed! Should regard as high grade Serrated Dysplasia Epithelial serration Elongated nuclei Prominent eosinophilic cytoplasm Should regard as high grade GOOD NEWS! Both patterns tend to occur in association with more conventional dysplasia
14 Indefinite for dysplasia WHEN? 1) Inflammation 2) Basal glandular atypia /dysplasia/ basal crypt dysplasia-like atypia 3) Poor orientation (Tangential sections)/loss of surface epithelium EXPLAIN WHY


15 Indefinite for dysplasia due to inflammation May make interpretation almost impossible Occasionally the differential diagnosis includes florid reactive atypia and high grade dysplasia
 Basal crypt dysplasia Surface maturation")
16 Indefinite for dysplasia due to basal glandular atypia Basal Crypt Dysplasia-like Atypia (BCDLA) Basal crypt dysplasia Surface maturation (+)


17 Indefinite for dysplasia Loss of surface epithelium Poor orientation/tangential cut
 May be stratified but often more disorganised Interobserver agreement generally")
18 High Grade Dysplasia Nuclei more enlarged and rounded Greater hyperchromasia More pleomorphism Nucleoli more prominent Mitoses ++ (atypical) May be stratified but often more disorganised Interobserver agreement generally good


19 Intramucosal Adenocarcinoma Single cells in lamina propria Cribriform or lateral growth pattern Often little or no desmoplastic response Often report as intramucosal carcinoma at least


20 Invasive Adenocarcinoma Can be difficult diagnosis to make on mucosal biopsies! Other tumour types
 p53 - aberrant")
 - p53 interpretation module")
21 Ki67 Help...is at hand? Alpha-Methyl-CoA racemase (AMACR) p53 - aberrant expression (+/-) - adjunct to routine clinical diagnosis (BSG 2014) - p53 interpretation module significant / not significant Levels Second opinion
 All cases of suspected dysplasia are reviewed by a second GI pathologist Given the difficulties associated with the")
22 What needs a second opinion? (BSG 2014) All cases of suspected dysplasia are reviewed by a second GI pathologist Given the difficulties associated with the management of the indefinite for dysplasia category, all such cases should also be reviewed by a second GI pathologist
23 Interobserver (and intraobserver) agreement 2015 Agreement (+) Agreement (-) Non-dysplastic Indefinite for dysplasia High grade dysplasia Vs Low grade dysplasia Carcinoma (International variation in thresholds of diagnosis)



24 Is there a solution? Not Sure Definite Dysplasia Carcinoma

 2or 3 slices per cassette")
25 Endomucosal Resection (EMR) Pinned on cork/similar Deep margin inked Serially sectioned at 2-3mm (through closest edge if a lesion visible) 2or 3 slices per cassette 3 levels each

26 Endomucosal Resections the Good Avoidance of oesophagectomy

27 Endomucosal Resections the Bad Poor differentiation Submucosal invasion Incomplete excision Lymphovascular invasion
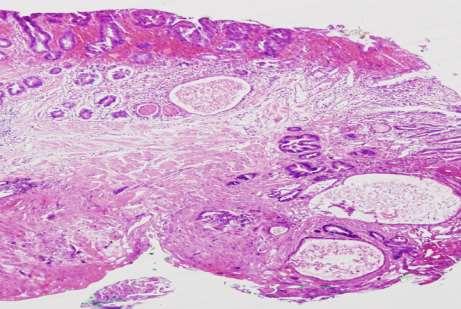
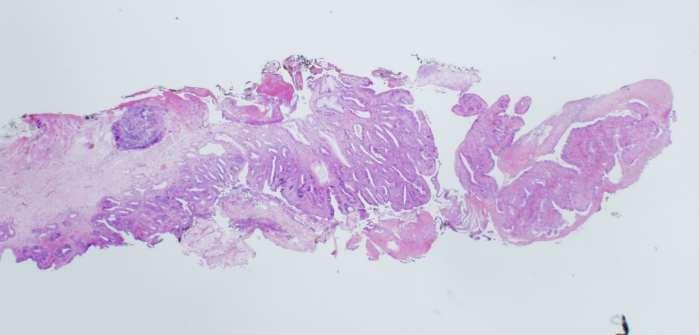
28 Endomucosal Resection The Ugly Pin Cautery.Fragmentation..Surface loss...curling edges

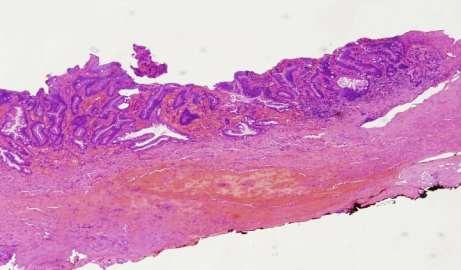
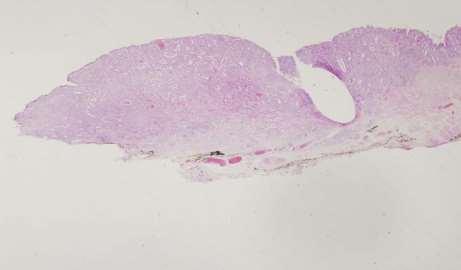
29 Learn to recognise the submucosa Beware the double muscularis mucosae
30 Local reporting template for endomucosal resection specimens (EMR s) of oesophageal lesions Macroscopy: Site of tumour: Maximum tumour dimension (mm) (if known): Number of specimens: Size of each specimen (mm): Microscopy: Tumour type: Adenocarcinoma / Squamous / Other (specify) Lauren classification (if applicable): intestinal or diffuse / mixed Differentiation by worst area: Well / Moderate / Poor Substage: Not assessible M1 - High grade dysplasia M2 - Intramucosal carcinoma (invasion of lamina propria) M3 - Infiltration of muscularis mucosae SM - Submucosa if so, distance of tumour beyond muscularis mucosae (mm): Margins: Deep margin involved: Yes / No / Not assessible If no, distance of tumour to deep margin (mm): Peripheral margin: Carcinoma /High grade dysplasia /Low grade dysplasia /Intestinal metaplasia / Not assessible Lymphatic or Vascular invasion: Yes / No, If yes, which Pathological stage (TNM 7th edition): pt... Comments:
31 Subclassification of pt1a oesophageal adenocarcinoma BSG Guidelines 2014 Vieth 2014 m1: Carcinoma in-situ or with questionable invasion beyond the basement membrane m2: Invasion into the lamina propria m3: Invasion into the muscularis mucosa HGD: High grade dysplasia M1: Invasion into lamina propria M2: Invasion into inner duplicated muscularis mucosae M3: Invasion into the space between the two layers of duplicated MM M4: Invasion into the outer layer of the duplicated MM

 pt 1 (m3)")
 pt 1")
32 pt 1 (m1) (HGD) MiB1 and p53 Vieth pt 1 (m2) pt 1 (m1) pt 1 (m2) pt 1 (m3) pt 1 (m3) pt 1 (m4) pt 1 (sm1) pt 1 (sm1)

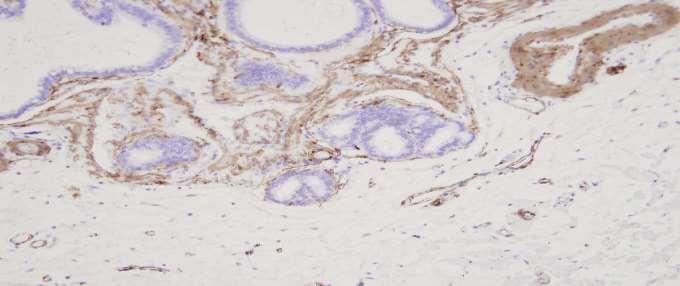
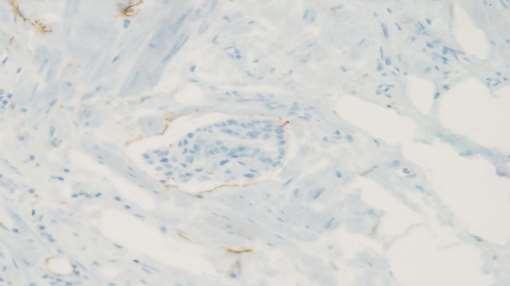
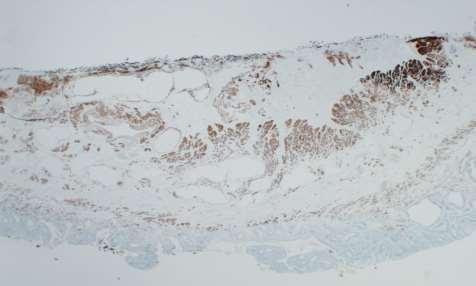
33 EMR s use of immunohistochemistry

34 Post radiofrequency ablation biopsies/emrs Beware of buried glands! Squamous re-epithelialisation Loss of glandular surface for evaluation Mimicry of glandular dysplasia Mimicry of invasive adenocarcinoma (Squamous re-epithelialisation over invasive adenocarcinoma)
35 Please Help exclude Barrett s when appropriate Confine second opinion practice to LGD (for the moment) Consider change to mirror the altered management landscape Embrace the EMR!

36
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Earlyoesophagealcancer. dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia
 Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Burning Issues in the Esophagus
 Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Squamous Cell Carcinoma of the Head and Neck (SCCHN)
") Squamous Cell Carcinoma of the Head and Neck (SCCHN) Part 1 Bruce M. Wenig, M.D. Dept. of Pathology & Laboratory Medicine Continuum Health Partners New York, NY College of American Pathologists 2004. Materials
Squamous Cell Carcinoma of the Head and Neck (SCCHN) Part 1 Bruce M. Wenig, M.D. Dept. of Pathology & Laboratory Medicine Continuum Health Partners New York, NY College of American Pathologists 2004. Materials
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL
 THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations
 Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
Part 1. A pragmatic approach to common problems in esophageal biopsy pathology
 Part 1 A pragmatic approach to common problems in esophageal biopsy pathology How I can help more patients than I hurt Barbara J McKenna University of Michigan barbmcke@med.umich.edu Case 1 The following
Part 1 A pragmatic approach to common problems in esophageal biopsy pathology How I can help more patients than I hurt Barbara J McKenna University of Michigan barbmcke@med.umich.edu Case 1 The following
Histopathology: Cervical HPV and neoplasia
 Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition
 SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Diagnosis and grading of dysplasia in Barrett s oesophagus ... J Clin Pathol 2006;59: doi: /jcp
 1029 MY APPROACH Diagnosis and grading of dysplasia in Barrett s oesophagus R D Odze... This review focuses on the pathological features of dysplasia in Barrett s oesophagus. Two categorisation schemes
1029 MY APPROACH Diagnosis and grading of dysplasia in Barrett s oesophagus R D Odze... This review focuses on the pathological features of dysplasia in Barrett s oesophagus. Two categorisation schemes
LARYNGEAL DYSPLASIA. Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital
 LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology
 New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations
 Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
12/7/2011. Pathological mimics of malignancy in the GI tract. Professor Neil A Shepherd President, British Division of the IAP
 Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
ESMO Preceptorship Gastrointestinal Tumours Valencia October 2017
 www.esmo.org ESMO Preceptorship Valencia 06-07 October 2017 Gastrointestinal Tumours I have no conflicts of interest to declare Fátima Carneiro Gastrointestinal tumours Multidisciplinary management, standards
www.esmo.org ESMO Preceptorship Valencia 06-07 October 2017 Gastrointestinal Tumours I have no conflicts of interest to declare Fátima Carneiro Gastrointestinal tumours Multidisciplinary management, standards
Pathology in Slovenian CRC screening programme: Organisation and quality assurance. Snježana Frković Grazio and Matej Bračko
 Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Barrett s s Dysplasia
 Barrett s s Dysplasia Mary P. Bronner,, MD Director, GI Pathology Section Head, Molecular Pathology Cleveland Clinic Foundation Neoplastic Progression in Barrett s s Esophagus Chronic Reflux GERD Metaplasia
Barrett s s Dysplasia Mary P. Bronner,, MD Director, GI Pathology Section Head, Molecular Pathology Cleveland Clinic Foundation Neoplastic Progression in Barrett s s Esophagus Chronic Reflux GERD Metaplasia
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Epithelial Columnar Breast Lesions: Histopathology and Molecular Markers
 29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
Upper GIT IV Gastric cancer
 Upper GIT IV Gastric cancer Luigi Tornillo PathoBasic 23.10.2014 Pathology Introduction Classification Morphogenesis Problems Intraepithelial neoplasia Surveillance EGJ Predictive factors Gastric cancer
Upper GIT IV Gastric cancer Luigi Tornillo PathoBasic 23.10.2014 Pathology Introduction Classification Morphogenesis Problems Intraepithelial neoplasia Surveillance EGJ Predictive factors Gastric cancer
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
CLINICAL EFFECTIVENESS
 Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
RFA and Cyrotherapy for Esophageal Disease
 RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Evaluation of Breast Specimens Removed by Needle Localization Technique
 Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Changes to the diagnosis and management of Barrett s Oesophagus
 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours
 60 3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours Compilation and editing and of this volume: Prof. Chandu de Silva (Consultant Histopathologist) List of contributors Consultant
60 3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours Compilation and editing and of this volume: Prof. Chandu de Silva (Consultant Histopathologist) List of contributors Consultant
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Division of Anatomic Pathology & Molecular Oncology, University of Utah and ARUP Laboratories, Huntsman Cancer Institute, Salt Lake City, UT, USA
 REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
NPQR Quality Payment Program (QPP) Measures 21_18247_LS.
 Measures 21_18247_LS.") NPQR Quality Payment Program (QPP) Measures 21_18247_LS MEASURE ID: QPP 99 MEASURE TITLE: Breast Cancer Resection Pathology Reporting pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes)
NPQR Quality Payment Program (QPP) Measures 21_18247_LS MEASURE ID: QPP 99 MEASURE TITLE: Breast Cancer Resection Pathology Reporting pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes)
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
number Done by Corrected by Doctor Maha Shomaf
 number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease
 GASTROENTEROLOGY 2010;138:746 774 AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease AGA Podcast interview: www.gastro.org/gastropodcast. Learning
GASTROENTEROLOGY 2010;138:746 774 AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease AGA Podcast interview: www.gastro.org/gastropodcast. Learning
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS
 PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Current issues in Barrett s oesophagus and the oesophago-gastric junction
 Current issues in Barrett s oesophagus and the oesophago-gastric junction Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The changing role of
Current issues in Barrett s oesophagus and the oesophago-gastric junction Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The changing role of
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Case in discussion. Common diagnostic problems in gallbladder pathology 62, F
 Common diagnostic problems in gallbladder pathology N. Volkan Adsay, M.D. 62, F Case in discussion Underwent cholecystectomy with the diagnosis of chronic cholecystititis and cholelithiasis Professor and
Common diagnostic problems in gallbladder pathology N. Volkan Adsay, M.D. 62, F Case in discussion Underwent cholecystectomy with the diagnosis of chronic cholecystititis and cholelithiasis Professor and
One of the more common specimens encountered by
 Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
proposed Vienna classification of gastrointestinal
 Gut 2;47:251 255 251 For list of authors ayliations, please see appendix. Correspondence to: Dr R Schlemper, Department of Internal Medicine, Fukuoka University School of Medicine, 7-45-1 Nanakuma, Jonan-ku,
Gut 2;47:251 255 251 For list of authors ayliations, please see appendix. Correspondence to: Dr R Schlemper, Department of Internal Medicine, Fukuoka University School of Medicine, 7-45-1 Nanakuma, Jonan-ku,
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Pathology of the oesophagus and the stomach. Neil A Shepherd Gloucester, UK. Bristol Pathology 1 st Year Training School, The layers of the GI tract
 Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Dysplasia, Mimics and Other Controversies
 Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Macro- and microacinar proliferations of the prostate
 Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Demystifying Endometrial Hyperplasia
 Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School
 Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading?
 Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Urinary Bladder, Ureter, and Renal Pelvis
 Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
CPC on Cervical Pathology
 CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Columnar Cell Lesions. Columnar Cell Lesions and Flat Epithelial Atypia
 Columnar Cell Lesions and Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Columnar Cell Lesions Lesions characterized by columnar epithelial cells
Columnar Cell Lesions and Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Columnar Cell Lesions Lesions characterized by columnar epithelial cells
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
PRACTICAL ROADMAP EPITHELIUM A. JOVANOVIĆ
 PRACTICAL ROADMAP EPITHELIUM A. JOVANOVIĆ Epithelia Simple epithelia Stratified epithelia Simple squamous Simple cuboidal Simple columnar Pseudostratified Stratified squamous - non keratinized - keratinized
PRACTICAL ROADMAP EPITHELIUM A. JOVANOVIĆ Epithelia Simple epithelia Stratified epithelia Simple squamous Simple cuboidal Simple columnar Pseudostratified Stratified squamous - non keratinized - keratinized
Pathology of bladder cancer in Egypt; a current study.
 Pathology of bladder cancer in Egypt; a current study. Thesis Submitted for partial fulfillment of Master degree in urology By Mohamed Atef Mohamed Ahmed M.B.B.CH Supervised by Prof.Dr.: Omar Mohamed Abdel-
Pathology of bladder cancer in Egypt; a current study. Thesis Submitted for partial fulfillment of Master degree in urology By Mohamed Atef Mohamed Ahmed M.B.B.CH Supervised by Prof.Dr.: Omar Mohamed Abdel-
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Pathologic Assessment of Invasion in TUR Specimens. A. Lopez-Beltran. T1 (ct1)
") Pathologic Assessment of Invasion in TUR Specimens A. Lopez-Beltran T1 (ct1) 1 Prognostic factors for progression/invasive disease Ta,T1,CIS- NMIBC :TNM 2017 ESSENTIAL: Grade T stage CIS Number of lesions
Pathologic Assessment of Invasion in TUR Specimens A. Lopez-Beltran T1 (ct1) 1 Prognostic factors for progression/invasive disease Ta,T1,CIS- NMIBC :TNM 2017 ESSENTIAL: Grade T stage CIS Number of lesions