When to Treat Beyond Progression with Systemic Therapies? Manuela Schmidinger Medical University of Vienna, Austria
|
|
|
- Grace Dickerson
- 6 years ago
- Views:
Transcription
1
2 When to Treat Beyond Progression with Systemic Therapies? Manuela Schmidinger Medical University of Vienna, Austria

3 Is Treatment Beyond Progression a Valid Strategy? 1) NO YES?
4 Is Treatment Beyond Progression a Valid Strategy? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope
5 Is Treatment Beyond Progression a Valid Strategy? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Will most likely also comfort the treating physician (for the same reasons)
6 Is Treatment Beyond Progression a Valid Strategy? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Will most likely also comfort the treating physician (for the same reasons) 3) May be biologically reasonable and promising when the next drug inhibits targets that have been linked to resistance and progression
- inhibitors: stasis or regression and loss of vasculatur Induction of a hypoxic microenvironment (occurrence of resistance, epithelial to mesenchymal")
7 1. Paez-Ribes M et al., Cancer Cell 2009 March 3;15(3); Antiangiogenic Therapy Elicit Increased Local Invasion and Distant Metastasis 1 Pàez-Ribes et al. Page 21 Tumors first respond to VEGF(R)- inhibitors: stasis or regression and loss of vasculatur Induction of a hypoxic microenvironment (occurrence of resistance, epithelial to mesenchymal transition) Figure 8. Adaptive-Evasive Responses by Tumors to Antiangiogenic Therapies Schematic summary of adaptive responses to VEGF/VEGFR inhibitors (and likely other angiogenesis inhibitors) that elicit evasive resistance. Tumors respond to VEGF/VEGFR pathway inhibition with tumor stasis or regression and a loss of blood vessels, but mechanisms of evasive resistance to the antiangiogenic treatment are then induced that can variously enable revascularization via alternative proangiogenic signals, increased local invasiveness, and/or enhanced distant metastasis. Various VEGF-independent mechanisms enable revascularization and progression Switching to an agent that does not primarily target VEGF appears reasonable

8 Success Demonstrated with Biologically Reasonable Strategies Cabozantinib is an oral small molecule inhibitor of tyrosine kinases including MET, VEGF receptors, and AXL 3 Increased MET and AXL expression has been associated with poor prognosis and resistance to VEGFR inhibitors in RCC 1,2 4 1 Zhou L et al., Oncogene, 2015; 2 Ciamporcero E et al., Mol Cancer Ther, 2014; 3 Yakes FM et al., Mol Cancer Ther, 2011 ; 4. Choueiri TK et al,, N Engl J Med 2015
9 Is Treatment Beyond Progression a Valid Strategy? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Will most likely also comfort the treating physician (for the same reasons) 3) May be biologically reasonable and promising when the next drug inhibits targets that have been linked to resistance and progression 4) Is tempting if second-line studies are available and open for accrual
10 Is Treatment Beyond Progression a Valid Strategy? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Will most likely also the treating physician (for the same reasons) 3) May be biologically reasonable and promising when the next drug inhibits targets that have been linked to resistance and progression 4) Is tempting if second-line studies are available and open for accrual 5) Is supported by guidelines
![Treatment Guidelines for mrcc Treatment group Standard Option First line Good or intermediate risk Sunitinib [I,A] Bevacizumab + IFN-α [I,A] Pazopanib [I,A] High-dose IL-2 [III,C] Sorafenib [II,B]](/docs-images/74/71018029/images/11-1.jpg "Bevacizumab + low-dose IFN-α [III,A] Poor risk Temsirolimus [II,A] Sunitinib [II,B] Sorafenib [III,B] Second line Post-cytokines Post-TKIs Axitinib [I,A] Sorafenib [I,A] Pazopanib [II,A] Axitinib")
11 Treatment Guidelines for mrcc Treatment group Standard Option First line Good or intermediate risk Sunitinib [I,A] Bevacizumab + IFN-α [I,A] Pazopanib [I,A] High-dose IL-2 [III,C] Sorafenib [II,B] Bevacizumab + low-dose IFN-α [III,A] Poor risk Temsirolimus [II,A] Sunitinib [II,B] Sorafenib [III,B] Second line Post-cytokines Post-TKIs Axitinib [I,A] Sorafenib [I,A] Pazopanib [II,A] Axitinib [I,B] Everolimus [II,A] Sunitinib [III,A] Sorafenib [II,A] Nivolumab Cabozantinib Post-two TKIs Everolimus [II,A] Third line Post-TKI and mtor inhibitor Sorafenib [I,B] Other TKI [IV,B] Rechallenge [IV,B] IFN-α, interferon-α; IL, interleukin; VEGFR, VEGF receptor Escudier et al. Ann Oncol 2014
12 ...But Can We Maintain a Treatment Beyond Progression? SWITCHING TREATMENT MAINTAINING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Will most likely also comfort the treating physician (for the same reasons) 3) May be biologically reasonable and promising when the next drug inhibits targets that have been linked to resistance and progression 4) Is tempting if second-line studies are available and open for accrual 5) Is supported by guidelines
13 ...But Can We Maintain a Treatment Beyond Progression? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Is most likely a strategy to comfort the treating physician (for the same reasons) 3) May be biologically reasonable and promising when the next drug inhibits targets that have been linked to resistance and progression 4) Is tempting if second-line studies are available and open for accrual 5) Is supported by guidelines MAINTAINING TREATMENT 1) Evidence against?
14 Evidence (and What We Believe in) Depends on What Has Been Investigated
15 Former second-line studies did not include a treatment arm with the first-line agent given beyond progression Eligibility criteria: Histologically confirmed mrcc with clear cell component Failure of prior first-line regimen containing 1 of: Sunitinib Bevacizumab + IFN-α Temsirolimus Cytokine(s) N=741 R A N D O M I S A T I O N e.g. Sunitinib beyond progression Axitinib 5 mg BID Sorafenib 400 mg BID (NCT )
16 ...But Can We Maintain a Treatment Beyond Progression? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Is most likely a strategy to comfort the treating physician (for the same reasons) 3) May be biologically reasonable and promising when the next drug inhibits targets that have been linked to resistance and progression 4) Is tempting if second-line studies are available and open for accrual 5) Is supported by guidelines MAINTAINING TREATMENT 1) Evidence against? 2) RECIST: quantifies PD but : clinical evidence that this quantity is a clinically valid EP that should result in change of tx?
17 Analysis of the Growth Rate of RCC while Sunitinib Treatment Sunitinib more effectively reduce the growth rate of RCC when comapred with IFN-alpha this reduction was correlated with better PFS and OS 1 Sunitinib treatment is also associated with prolonged stability of growth rate 2 Growth rate over time for 234 patients who had evidence of tumor growth: Tumor growth rates remained stable in the overwhelming majority 1.SteinWD et al., Clin Cancer Res ; 18(8) April 15, 2012; 2.Burotto M et al., PLOS/one May 2014, Vol 9; Issu 5, e96316.
18 Using the median estimated growth rate and regression rate constants: theoretical curves depicting tumor quantity over time This allows to estimate the fraction of tumor at any given point in time that is still sensitive to therapy (blue line) A projected PFS of 7.3 months would be a valid treatment option in second-line Burotto M et al., PLOS/one May 2014, Vol 9; Issu 5, e96316
19 ...But Can We Maintain a Treatment Beyond Progression? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Is most likely a strategy to comfort the treating physician (for the same reasons) 3) May be biologically reasonable and promising when the next drug inhibits targets that have been linked to resistance and progression 4) Is tempting if second-line studies are available and open for accrual 5) Is supported by guidelines MAINTAINING TREATMENT 1) Evidence against? 2) RECIST: quantifies PD but : clinical evidence that this quantity is a clinically valid EP that should result in change of tx? 3) Clinical reasons
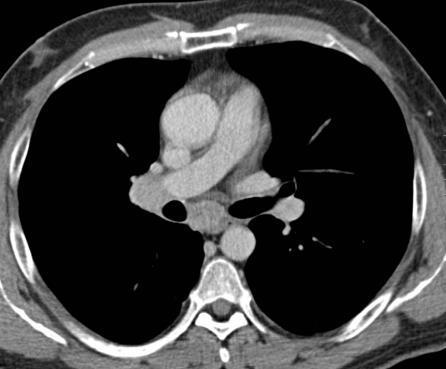
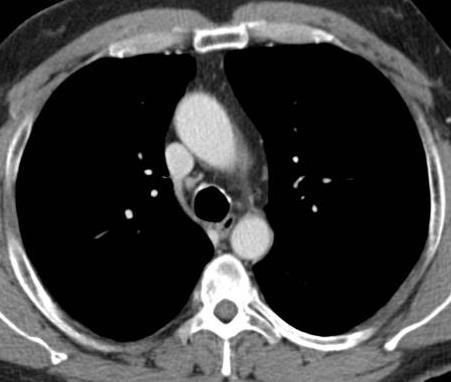
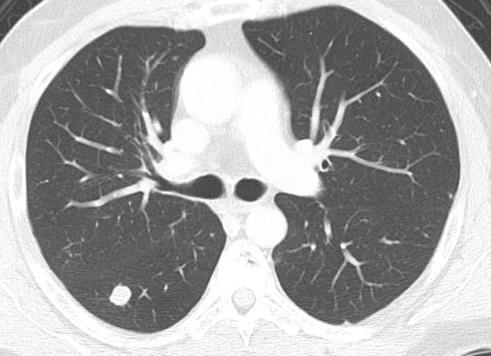
20 Patient CG Male patient, 28 years at diagnosis, dramatic weight loss since June 2012 December 2012: palpable tumor mass, diagnosis RCC Radical nephrectomy and cavotomy: pt4, Nx, G4, Vimentin positive, clear cell with necrosis and >80 % sarcomatoid percentage Few weeks after surgery: CRP, thrombocytosis; CTs: multiple 7 cm tumor masses at the site of nephrectomy, infiltration M. psoas, displacement of intestines Multiple lesions in M. quadratus lumborum 17 mm lesion between abdominal wall and colon ascendens Subcutaneous mets Liver mets Lung mets
21 Patient CG 1st-line Sunitinib: 50 mg April 2013 Major improvement in performance status, decrease of CRP and thrombocytosis Reports on tumor-associated symptoms during breaks, therefore 50 mg continuously Best response: RECIST SD (minor remission) Remained on first-line sunitinib for 12 months because withdrawal of treatment associated with pain, night sweats and fever

22 Rapid disease progression and deterioration of performance status at treatment discontinuation Short before sorafenib discontinuation 1 week after sorafenib discontinuation CT before second stop of sorafenib CT after final sorafenib discontinuation Desar IM et al., 2009 Acta Oncologica, 48:6,
23 ...But Can We Maintain a Treatment Beyond Progression? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Is most likely a strategy to comfort the treating physician (for the same reasons) 3) May be biologically reasonable and promising when the next drug inhibits targets that have been linked to resistance and progression 4) Is tempting if second-line studies are available and open for accrual 5) Is supported by guidelines MAINTAINING TREATMENT 1) Evidence against? 2) RECIST: quantifies PD but : clinical evidence that this quantity is a clinically valid EP that should result in change of tx? 3) Clinical reasons 4) Mixed responses
24 Mixed Responses The underlying biology of this phenomenon is poorly understood Pseudoprogression? Intratumor heterogeneity 1? Differences in site-specific TME, e.g excellent response of pancreatic metastases and poor response to LN-metastases 2?... Gerlinger M et al., New Engl J Med 2012; 2. Grassi P et al., Future Oncol 2014; 10(8),


25 64 yrs old Patient April 2016 with cc-mrcc Before Sunitinib 3 months after sunitinib


26 Before Sunitinib 3 months after sunitinib
27 Clinical Considerations in Patients with Mixed Response We will not be able to identify and target all new drivers of the disease, It might be difficult to optimize/influence the TME Why not maintaining a treatment that controls effectively some areas or the larger amount of metastases? and adding a local treatment for those metastases that do not behave?
28 Stereotactic Body Radiotherapy for Oligometastatic RCC as a Bridge Therapy to Delay Systemic treatment or to Delay Change of Systemic Treatment? Lesion-based control after SBRT Overall survival for all patients Ranck MC et al., Am J Clin Oncol 36, 6; December 2013
29 Adding a Local Treatment and Maintaining Systemic Treatment: Particularly useful in the case of stable extracerebral disease and newly diagnosed brain mets Degree of sunitinib penetration through the BAB and BBB is very low (< 5%) 1 Local control of BM by local treatment 1.Sobanska K et al., European review for medical and Pharmacol Sciences 2016; 20: ; 2.Ippen FM and Mahadevan A et al; J Oncol 2015
30 ...But Can We Maintain a Treatment Beyond Progression? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Is most likely a strategy to comfort the treating physician (for the same reasons) 3) May be biologically reasonable and promising when the next drug inhibits targets that have been linked to resistance and progression 4) Is tempting if second-line studies are available and open for accrual 5) Is supported by guidelines MAINTAINING TREATMENT 1) Evidence against? 2) RECIST: quantifies PD but : clinical evidence that this quantity is a clinically valid EP that should result in change of tx? 3) Clinical reasons 4) Mixed responses 5) Overcoming resistance is possible
31 Maintaining Treatment AND Overcoming Resistance: Alternative Strategy? WAIT Interrupting treatment on which progression and epithelial to mesenchymal transition 1 has occurred may allow the TME to reset Tumor may regain sensitivity to sunitinib 2 ESCALATE 1. Hammers HJ et al., Mol Cancer Ther 2010; 2. Hammers HJ et al., Mol Cancer Ther 2010

32 Vorher Nachher


33 Vorher Nachher
34 Maintaining Treatment AND Overcoming Resistance: Alternative Strategy? WAIT Interrupting treatment on which progression and epithelial to mesenchymal transition has occurred may allow the TME to reset 1 Tumor may regain sensitivity to sunitinib 2 ESCALATE Experiments conducted in xenografts and patients revealed that resistance can be overcome by dose escalation at the time point of disease progression 3 1. Bergers G and Hanahan D: Nat Rec Cancer 2008 ; 2. Hammers HJ et al., Mol Cancer Ther 2010; 3. Pili J Clin Oncol 2013




35 Patient FR courtesy of Dr. Ponhold April 2013 July 2013
36 ...Can We Maintain a Treatment Beyond Progression? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Is most likely a strategy to comfort the treating physician (for the same reasons) 3) May be biologically reasonable and promising when the next drug inhibits targets that have been linked to resistance and progression 4) Is tempting if second-line studies are available and open for accrual 5) Is supported by guidelines MAINTAINING TREATMENT 1) Evidence against? 2) RECIST: quantifies PD but : clinical evidence that this quantity is a clinically valid EP that should result in change of tx? 3) Clinical reasons 4) Mixed responses 5) Overcoming resistance is possible 6) Pseudoprogression
37 A New Challenge: PD-1 Inhibitors Do Not Move Progression-free survival Progression-Free Survival (Probability) Everolimus Median PFS, months (95% CI) Nivolumab 4.6 ( ) Everolimus 4.4 ( ) HR (95% CI): 0.88 ( ) P = Nivolumab No. of patients at risk Months Nivolumab Everolimus In a post-hoc analysis of patients who had not progressed or died at 6 months, median PFS was 15.6 months for nivolumab vs 11.7 months for everolimus (HR (95% CI): 0.64 ( ))
38 But Overall Survival Appears to Improve with Treatment Beyond Progression Median OS, months (95% CI) Treated beyond progression (N = 36) Not treated beyond progression (N = 92) 30.5 ( ) 15.2 ( ) 0.6 Patients treated beyond progression Censored Patients treated beyond progression Patients no treated beyond progression Patients not treated beyond progression Months

39 A challenge in mrcc patients undergoing check-point inhibitor treatment Tumor flaire phenomenon? How to deal with progression Progression of tumor cells that regained sensitivity for VEGF-I? TX beyond PD Pseudoprogression? RCC is a VEGF-driven disease TX beyond PD and adding a VEGF-I? Switching?
40 ...Can We Maintain a Treatment Beyond Progression? SWITCHING TREATMENT 1) Is what most patients would want: new drug= new hope 2) Is most likely a strategy to comfort the treating physician (for the same reasons) 3) May be biologically reasonable and promising when the next drug inhibits targets that have been linked to resistance and progression 4) Is tempting if second-line studies are available and open for accrual 5) Is supported by guidelines MAINTAINING TREATMENT 1) Evidence against? 2) RECIST: quantifies PD but : clinical evidence that this quantity is a clinically valid EP that should result in change of tx? 3) Clinical reasons 4) Mixed responses 5) Overcoming resistance is possible 6) Pseudoprogression 7) Limited resources

41 Are Second-Line Agents Easily Available Everywhere? E.g. Axitinib approval and launch status

42 Nivolumab RCC EMA Approval and Availability Challenging reimbursement situation in most CECOG countries Bulgaria Croatia Cyprus Czech Republic Estonia Greece Hungary Latvia Lithuania Poland Portugal Rumania Slovakia Slovenia
43 Treatment Beyond Progression is a Valid Strategy May be justified if: Acceptable treatment tolerance AND Clinical benefit AND Clinical need (symptoms upon discontinuation) OR Slow progression OR Mixed response (de novo brain mets and stable extracerebral disease or mixed response in extracerebral metastases) OR Room for dose escalation OR If progression occurs after a treatment break OR If pseudoprogression is suspected OR Any of the situations above AND limited drug availability/limited resources OR/AND If no clinical study open for accrual/no new drug available
44
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game?
 Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Second - Line Debate: Axitinib
 Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
Metastatic renal cancer (mrcc): Evidence-based treatment
: Evidence-based treatment") Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Metastatic Renal Cancer Medical Treatment
 Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
Innovaciones en el tratamiento del ca ncer renal. Enrique Grande
 Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Sequencing of therapies in mrcc. Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC
 Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Targeted and immunotherapy in RCC
 Targeted and immunotherapy in RCC Treatment options Surgery (radical VS partial nephrectomy) Thermal ablation therapy Surveillance Immunotherapy Molecular targeted therapy Molecular targeted therapy Targeted
Targeted and immunotherapy in RCC Treatment options Surgery (radical VS partial nephrectomy) Thermal ablation therapy Surveillance Immunotherapy Molecular targeted therapy Molecular targeted therapy Targeted
Linee guida terapeutiche oncologiche. Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona
 Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
Fifteenth International Kidney Cancer Symposium
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
David N. Robinson, MD
 David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
A Review in the Treatment Options for Renal Cell Cancer
 A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
Medical Management of Renal Cell Carcinoma
 Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
NEXT GENERATION DRUGS IN KIDNEY CANCER. Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden
 NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
Cytoreductive Nephrectomy
 Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
The Therapeutic Landscape in Advanced Renal Cell Carcinoma
 The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
Renal Cell Carcinoma: Status of Medical and Surgical Therapy. Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation
 Renal Cell Carcinoma: Status of Medical and Surgical Therapy Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation Metastatic Renal Cell Carcinoma: Evolution of Current Therapeutic Approaches
Renal Cell Carcinoma: Status of Medical and Surgical Therapy Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation Metastatic Renal Cell Carcinoma: Evolution of Current Therapeutic Approaches
Treatment Algorithm and Therapy Management in mrcc. Manuela Schmidinger Medical University of Vienna Austria
 Treatment Algorithm and Therapy Management in mrcc Manuela Schmidinger Medical University of Vienna Austria A Paradigm Shift in the Treatment of mrcc 1. Sunitinib 2. Sorafenib 3. Bevacizumab+IFN-alpha
Treatment Algorithm and Therapy Management in mrcc Manuela Schmidinger Medical University of Vienna Austria A Paradigm Shift in the Treatment of mrcc 1. Sunitinib 2. Sorafenib 3. Bevacizumab+IFN-alpha
Mechanisms of Resistance to Antiangiogenic. Martin J. Edelman, MD University of Maryland Greenebaum Cancer Center Dresden, 2012
 Mechanisms of Resistance to Antiangiogenic Agents Martin J. Edelman, MD University of Maryland Greenebaum Cancer Center Dresden, 2012 Angiogenesis: A fundamental attribute of cancer Premise of Anti-angiogenic
Mechanisms of Resistance to Antiangiogenic Agents Martin J. Edelman, MD University of Maryland Greenebaum Cancer Center Dresden, 2012 Angiogenesis: A fundamental attribute of cancer Premise of Anti-angiogenic
Sergio Bracarda MD. Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy
 San Donato Hospital Arezzo, Italy") Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY FOR THE RIGHT PATIENT
 Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea
 Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
Renal Cell Cancer: Present and Future. Bernard Escudier, Gustave Roussy
 Renal Cell Cancer: Present and Future Bernard Escudier, Gustave Roussy [HKIOF May 2017] Sponsored by Bristol- Myers Squibb OPDIVO Hong Kong prescribing information is available upon request Disclosures
Renal Cell Cancer: Present and Future Bernard Escudier, Gustave Roussy [HKIOF May 2017] Sponsored by Bristol- Myers Squibb OPDIVO Hong Kong prescribing information is available upon request Disclosures
Integrating novel therapy in advanced renal cell carcinoma
 Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
I Kid(ney) You Not: Updates on Renal Cell Carcinoma
 You Not: Updates on Renal Cell Carcinoma") Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Renal Cell Cancer. Clinical case study 1 & 2. Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland
 Renal Cell Cancer Clinical case study 1 & 2 Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland 1 Case study 1 - RCC and Lung Metastases Case study 1: Patient History Male, 63 years old Mild
Renal Cell Cancer Clinical case study 1 & 2 Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland 1 Case study 1 - RCC and Lung Metastases Case study 1: Patient History Male, 63 years old Mild
Dose individualization of sunitinib in mrcc: Toxicity-adjusted dose or Therapeutic drug monitoring
 Dose individualization of sunitinib in mrcc: Toxicity-adjusted dose or Therapeutic drug monitoring Alison Zhang 1, Peter Fox 1, Sally Coulter 4, Val Gebski 5, Bavanthi Balakrishnar 1, Christopher Liddle
Dose individualization of sunitinib in mrcc: Toxicity-adjusted dose or Therapeutic drug monitoring Alison Zhang 1, Peter Fox 1, Sally Coulter 4, Val Gebski 5, Bavanthi Balakrishnar 1, Christopher Liddle
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Why was HOPE 205 a Positive After Years of Negative Studies?
 Why was HOPE 205 a Positive After Years of Negative Studies? Prof. Dr. med. Viktor Grünwald Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation Why do we pursue combinations?
Why was HOPE 205 a Positive After Years of Negative Studies? Prof. Dr. med. Viktor Grünwald Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation Why do we pursue combinations?
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma
 for Metastatic Renal Cell Carcinoma") pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
Targeting fibroblast growth factor receptor (FGFR) pathway in renal cell carcinoma
 pathway in renal cell carcinoma") Targeting fibroblast growth factor receptor (FGFR) pathway in renal cell carcinoma Francesco Massari, Chiara Ciccarese, Matteo Santoni, Antonio Lopez-Beltran, Marina Scarpelli, Rodolfo Montironi & Liang
Targeting fibroblast growth factor receptor (FGFR) pathway in renal cell carcinoma Francesco Massari, Chiara Ciccarese, Matteo Santoni, Antonio Lopez-Beltran, Marina Scarpelli, Rodolfo Montironi & Liang
Management of High Risk Renal Cell Carcinoma
 Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016
 for Metastatic Renal Cell Carcinoma September 1, 2016") pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
 combination with everolimus with other relevant treatment options, perc considered the results of a submitted indirect treatment comparison (ITC) that included comparisons of lenvatinib in combination
combination with everolimus with other relevant treatment options, perc considered the results of a submitted indirect treatment comparison (ITC) that included comparisons of lenvatinib in combination
Brain mets under I.O.
 Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Cabozantinib for untreated locally advanced or metastatic renal cell carcinoma Final scope Remit/appraisal objective To appraise
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Cabozantinib for untreated locally advanced or metastatic renal cell carcinoma Final scope Remit/appraisal objective To appraise
Sequential Therapy in Renal Cell Carcinoma*
 Sequential Therapy in Renal Cell Carcinoma* Bernard Escudier, MD, Marine Gross Goupil, MD, Christophe Massard, MD, and Karim Fizazi, MD, PhD Because of the recent approval of several drugs for the treatment
Sequential Therapy in Renal Cell Carcinoma* Bernard Escudier, MD, Marine Gross Goupil, MD, Christophe Massard, MD, and Karim Fizazi, MD, PhD Because of the recent approval of several drugs for the treatment
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Current experience in immunotherapy for metastatic renal cell carcinoma
 Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce
 in the elderly ( 65y): Position of a SIOG Taskforce") Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce Medical treatment of metastatic RCC in the elderly ( 65y): Members of the SIOG Taskforce
Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce Medical treatment of metastatic RCC in the elderly ( 65y): Members of the SIOG Taskforce
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
Alternativas de Futuro en Cáncer Renal Enrique Grande
 Alternativas de Futuro en Cáncer Renal Enrique Grande Hospital Ramón y Cajal de Madrid The ncreasingly Challenging Field of mrcc Sorafenib (US 2005, EU 2006) 3,4 Sunitinib (US & EU 2006) 3,4 Early 1940s:
Alternativas de Futuro en Cáncer Renal Enrique Grande Hospital Ramón y Cajal de Madrid The ncreasingly Challenging Field of mrcc Sorafenib (US 2005, EU 2006) 3,4 Sunitinib (US & EU 2006) 3,4 Early 1940s:
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
Kidney Cancer Session
 New Frontiers in Urologic Oncology September 12 th, 2015 Kidney Cancer Session Moderator: Philippe E. Spiess, M.D. Invited Faculty Members: Wade J. Sexton, MD Jeremiah J. Morrissey, PhD Agenda for Session
New Frontiers in Urologic Oncology September 12 th, 2015 Kidney Cancer Session Moderator: Philippe E. Spiess, M.D. Invited Faculty Members: Wade J. Sexton, MD Jeremiah J. Morrissey, PhD Agenda for Session
What can we expect from running phase III trials: will all of them alter the current treatment algorithm?
 What can we expect from running phase III trials: will all of them alter the current treatment algorithm? 8 th European International Kidney Cancer Symposium Budapest, May 2013 Martin Gore PhD FRCP Royal
What can we expect from running phase III trials: will all of them alter the current treatment algorithm? 8 th European International Kidney Cancer Symposium Budapest, May 2013 Martin Gore PhD FRCP Royal
Evolution of Systemic Therapy Clinical Trials in VHL
 Evolution of Systemic Therapy Clinical Trials in VHL Ramaprasad Srinivasan, M.D., Ph.D. Investigator and Head, Molecular Cancer Section Urologic Oncology Branch Center for Cancer Research National Cancer
Evolution of Systemic Therapy Clinical Trials in VHL Ramaprasad Srinivasan, M.D., Ph.D. Investigator and Head, Molecular Cancer Section Urologic Oncology Branch Center for Cancer Research National Cancer
CLINICAL POLICY Department: Medical Management Document Name: Inlyta Reference Number: NH.PHAR.100 Effective Date: 05/12
 Page: 1 of 5 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Page: 1 of 5 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
New strategies and future of target therapy in advanced kidney cancer
 New strategies and future of target therapy in advanced kidney cancer VHL Gene Inactivation VHL Complex Disrupted VHL Protein HIF1-a, HIF2-a Accumulation VEGF PDGF TGF-α, CXCR4 Angiogenesis Endothelial
New strategies and future of target therapy in advanced kidney cancer VHL Gene Inactivation VHL Complex Disrupted VHL Protein HIF1-a, HIF2-a Accumulation VEGF PDGF TGF-α, CXCR4 Angiogenesis Endothelial
Angiogenesis and tumor growth
 Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The Current Champion: Angiogenesis inhibitors
 The Current Champion: Angiogenesis inhibitors Baek-Yeol RYOO University of Ulsan College of Medicine ASAN Medical Center Dept. of Oncology Seoul, Korea Survival probability Sorafenib: Overall Survival
The Current Champion: Angiogenesis inhibitors Baek-Yeol RYOO University of Ulsan College of Medicine ASAN Medical Center Dept. of Oncology Seoul, Korea Survival probability Sorafenib: Overall Survival
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015
 Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
pan-canadian Oncology Drug Review Final Clinical Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013
 for metastatic Renal Cell Carcinoma March 7, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
ASCO 2011 Genitourinary Cancer
 ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
17th ESO-ESMO Masterclass Clinical Oncology
 Metastatic Renal Cell Cancer: Evidence Based Treatment Manuela Schmidinger Medical University of Vienna, Austria Disclosures Honoraria for lectures or advisory boards from: Pfizer, Roche, BMS, Novartis,
Metastatic Renal Cell Cancer: Evidence Based Treatment Manuela Schmidinger Medical University of Vienna, Austria Disclosures Honoraria for lectures or advisory boards from: Pfizer, Roche, BMS, Novartis,
Advances in the Treatment of Renal Cell Carcinoma
 Advances in the Treatment of Renal Cell Carcinoma Developed in collaboration Learning Objectives Upon completion, participants should be able to: Identify patients with metastatic renal cell carcinoma
Advances in the Treatment of Renal Cell Carcinoma Developed in collaboration Learning Objectives Upon completion, participants should be able to: Identify patients with metastatic renal cell carcinoma
Prognostic Factors for mrcc: Relevance in Clinical Practice
 Prognostic Factors for mrcc: Relevance in Clinical Practice Daniel Heng MD MPH FRCPC Chair, GU Tumor Group Tom Baker Cancer Center University of Calgary Prognostic Factors Patient Factors Performance Status
Prognostic Factors for mrcc: Relevance in Clinical Practice Daniel Heng MD MPH FRCPC Chair, GU Tumor Group Tom Baker Cancer Center University of Calgary Prognostic Factors Patient Factors Performance Status
Clinical Biomarker in Kidney Cancer. Maria Nirvana Formiga, M.D., Ph.D.
 Clinical Biomarker in Kidney Cancer Maria Nirvana Formiga, M.D., Ph.D. Disclosures I am on the Speaker s Bureau with Pfizer and Bayer Clinical trials of BMS and Pfizer Kidney Cancer 70% new cases in developed
Clinical Biomarker in Kidney Cancer Maria Nirvana Formiga, M.D., Ph.D. Disclosures I am on the Speaker s Bureau with Pfizer and Bayer Clinical trials of BMS and Pfizer Kidney Cancer 70% new cases in developed
Checkpointinhibitoren in der Uro-Onkologie. Carsten Grüllich
 Checkpointinhibitoren in der Uro-Onkologie Carsten Grüllich 07.02.15 T-cell Aktivierung und Regulation T cell Costimulation Recognition MHC I Peptide b2m mrna Tumorantigen Tumor Pardoll Nature Rev Cancer
Checkpointinhibitoren in der Uro-Onkologie Carsten Grüllich 07.02.15 T-cell Aktivierung und Regulation T cell Costimulation Recognition MHC I Peptide b2m mrna Tumorantigen Tumor Pardoll Nature Rev Cancer
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? VEGF Is the Only Angiogenic Factor Present Throughout the Tumor Life Cycle
 Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Immunotherapy for the Treatment of Kidney and Bladder Cancer
 Immunotherapy for the Treatment of Kidney and Bladder Cancer Alan J. Koletsky, MD Genitourinary Cancer Research Program, Lynn Cancer Institute Clinical Asistant Professor of Biomedical Science The Charles
Immunotherapy for the Treatment of Kidney and Bladder Cancer Alan J. Koletsky, MD Genitourinary Cancer Research Program, Lynn Cancer Institute Clinical Asistant Professor of Biomedical Science The Charles
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients
 Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
Primary Care Management of the Kidney Cancer Patient
 Primary Care Management of the Kidney Cancer Patient Elaine Lam, MD Mountain States Cancer Conference 2016 November 5, 2016 Learning Objectives 1. Understand the mechanisms of action of currently approved
Primary Care Management of the Kidney Cancer Patient Elaine Lam, MD Mountain States Cancer Conference 2016 November 5, 2016 Learning Objectives 1. Understand the mechanisms of action of currently approved
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Imunoterapija u liječenju karcinoma bubrega. AUTOR: Milena Gnjidić
 Imunoterapija u liječenju karcinoma bubrega AUTOR: Milena Gnjidić IMUNOTERAPIJA U 2013 LIJEČENJU KARCINOMA BUBREGA Milena Gnjidić KBC Zagreb Hrvatska SWOC 12.2016 KARCINOM BUBREGA: SMJERNICE 2016 Nakon
Imunoterapija u liječenju karcinoma bubrega AUTOR: Milena Gnjidić IMUNOTERAPIJA U 2013 LIJEČENJU KARCINOMA BUBREGA Milena Gnjidić KBC Zagreb Hrvatska SWOC 12.2016 KARCINOM BUBREGA: SMJERNICE 2016 Nakon
Reference No: Author(s) Approval date: June Committee. Operational Date: July Review:
 Approval date: June Committee. Operational Date: July Review:") Reference No: Title: Author(s) Systemic anti-cancer therapy (SACT) guidelines for renal cell cancer Dr Alison Clayton Consultant Medical Oncologist & Dr Jane Hurwitz Consultant Medical Oncologist, Cancer
Reference No: Title: Author(s) Systemic anti-cancer therapy (SACT) guidelines for renal cell cancer Dr Alison Clayton Consultant Medical Oncologist & Dr Jane Hurwitz Consultant Medical Oncologist, Cancer
Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents
 in the Era of Targeted Agents") Conflict of Interest Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents None Patrick Medina, PharmD, BCOP Associate Professor University of Oklahoma OKC, OK Learning Objectives Epidemiology
Conflict of Interest Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents None Patrick Medina, PharmD, BCOP Associate Professor University of Oklahoma OKC, OK Learning Objectives Epidemiology
An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT )
") An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT02267967) J.M. Xu a, J. Li b, C.M. Bai c, N. Xu d, Z.W. Zhou e, Z.P. Li f, C.C. Zhou g, W. Wang h, J. Li
An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT02267967) J.M. Xu a, J. Li b, C.M. Bai c, N. Xu d, Z.W. Zhou e, Z.P. Li f, C.C. Zhou g, W. Wang h, J. Li
Prognostic Factors: Does It Really Matter if New Drugs for Targeted Therapy Will Be Used?
 european urology supplements 8 (2009) 478 482 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prognostic Factors: Does It Really Matter if New Drugs for Targeted Therapy Will
european urology supplements 8 (2009) 478 482 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prognostic Factors: Does It Really Matter if New Drugs for Targeted Therapy Will
Targeted Therapy in Advanced Renal Cell Carcinoma
 Targeted Therapy in Advanced Renal Cell Carcinoma Brian I. Rini, M.D. Department of Solid Tumor Oncology Glickman Urologic and Kidney Institute Cleveland Clinic Taussig Cancer Institute Cleveland, Ohio
Targeted Therapy in Advanced Renal Cell Carcinoma Brian I. Rini, M.D. Department of Solid Tumor Oncology Glickman Urologic and Kidney Institute Cleveland Clinic Taussig Cancer Institute Cleveland, Ohio
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Update on the treatment of metastatic clear cell and non-clear cell renal cell carcinoma
 Xu and Wu Biomarker Research (2015) 3:5 DOI 10.1186/s40364-015-0030-7 REVIEW Open Access Update on the treatment of metastatic clear cell and non-clear cell renal cell carcinoma Kevin Y Xu 1 and Shenhong
Xu and Wu Biomarker Research (2015) 3:5 DOI 10.1186/s40364-015-0030-7 REVIEW Open Access Update on the treatment of metastatic clear cell and non-clear cell renal cell carcinoma Kevin Y Xu 1 and Shenhong
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA. Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA
 UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenvatinib (Lenvima) for Renal Cell Carcinoma
 for Renal Cell Carcinoma") pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenvatinib (Lenvima) for Renal Cell Carcinoma January 4, 2019 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenvatinib (Lenvima) for Renal Cell Carcinoma January 4, 2019 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Targeted Therapies and Gut Microbiome in Renal Cell Carcinoma (RCC)
") Targeted Therapies and Gut Microbiome in Renal Cell Carcinoma (RCC) Nazli Dizman, MD Postdoctoral Fellow Department of Medical oncology & Experimental Therapeutics City of Hope Comprehensive Center December
Targeted Therapies and Gut Microbiome in Renal Cell Carcinoma (RCC) Nazli Dizman, MD Postdoctoral Fellow Department of Medical oncology & Experimental Therapeutics City of Hope Comprehensive Center December
Thoracic and head/neck oncology new developments
 Thoracic and head/neck oncology new developments Goh Boon Cher Department of Hematology-Oncology National University Cancer Institute of Singapore Research Clinical Care Education Scope Lung cancer Screening
Thoracic and head/neck oncology new developments Goh Boon Cher Department of Hematology-Oncology National University Cancer Institute of Singapore Research Clinical Care Education Scope Lung cancer Screening
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Guidelines on Renal Cell
 Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Complete Remission is a Reachable Goal in mrcc L. Albiges Institut Gustave Roussy
 Complete Remission is a Reachable Goal in mrcc L. Albiges Institut Gustave Roussy Is complete remission an achievable goal in mrcc? Lessons from observation Lessons from immunotherapy Current status in
Complete Remission is a Reachable Goal in mrcc L. Albiges Institut Gustave Roussy Is complete remission an achievable goal in mrcc? Lessons from observation Lessons from immunotherapy Current status in
Renal Cell Carcinoma Updated February 2016 by Dr. Safiya Karim (PGY 5 Medical Oncology Resident, University of Toronto)
") Renal Cell Carcinoma Updated February 2016 by Dr. Safiya Karim (PGY 5 Medical Oncology Resident, University of Toronto) Reviewed by Dr. Nimira Alimohamed (Staff Medical Oncologist, University of Calgary)
Renal Cell Carcinoma Updated February 2016 by Dr. Safiya Karim (PGY 5 Medical Oncology Resident, University of Toronto) Reviewed by Dr. Nimira Alimohamed (Staff Medical Oncologist, University of Calgary)
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management
: Diagnosis and Management") RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
How does histology alter treatment? Cora N. Sternberg, MD, FACP Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy
 How does histology alter treatment? Cora N. Sternberg, MD, FACP Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Targeting VHL/HIF in Clear Cell RCC VHL Bevacizumab (Antibody)
How does histology alter treatment? Cora N. Sternberg, MD, FACP Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Targeting VHL/HIF in Clear Cell RCC VHL Bevacizumab (Antibody)
Novel Molecular Molecular Therapies In Hepatocarcinoma Prof Eric
 Novel Molecular Therapies In Hepatocarcinoma Prof. Eric Raymond Department of Médical Oncology Hôpital Beaujon, Clichy Université Paris 7 Denis Diderot INSERM-U728 eric.raymond@bjn.aphp.fr HCC is a highly
Novel Molecular Therapies In Hepatocarcinoma Prof. Eric Raymond Department of Médical Oncology Hôpital Beaujon, Clichy Université Paris 7 Denis Diderot INSERM-U728 eric.raymond@bjn.aphp.fr HCC is a highly
CheckMate 025, as patients may derive a benefit, based on the opinion of the CGP and the mechanism of action of nivolumab.
 CheckMate 025, as patients may derive a benefit, based on the opinion of the CGP and the mechanism of action of nivolumab. perc noted that patients with brain metastases were excluded from the CheckMate
CheckMate 025, as patients may derive a benefit, based on the opinion of the CGP and the mechanism of action of nivolumab. perc noted that patients with brain metastases were excluded from the CheckMate
The Use of Inhibitors of Angiogenesis in Patients with Inoperable Locally Advanced or Metastatic Renal Cell Cancer: Guideline Recommendations
 Evidence-Based Series #3-8-4: Section 1 The Use of Inhibitors of Angiogenesis in Patients with Inoperable Locally Advanced or Metastatic Renal Cell Cancer: Guideline Recommendations S. Hotte, T. Waldron,
Evidence-Based Series #3-8-4: Section 1 The Use of Inhibitors of Angiogenesis in Patients with Inoperable Locally Advanced or Metastatic Renal Cell Cancer: Guideline Recommendations S. Hotte, T. Waldron,
The Met Pathway as a Target in RCC
 The Met Pathway as a Target in RCC Harriet Kluger, M.D. Associate Professor Yale Cancer Center Disclosures pertinent to this presentation - none c-met Pathway (Biocarta) Rationale for c-met targeting in
The Met Pathway as a Target in RCC Harriet Kluger, M.D. Associate Professor Yale Cancer Center Disclosures pertinent to this presentation - none c-met Pathway (Biocarta) Rationale for c-met targeting in
Case(s): How to Deal with Mixed Response Giuseppe Procopio
: How to Deal with Mixed Response Giuseppe Procopio") Case(s): How to Deal with Mixed Response Giuseppe Procopio Fondazione IRCCS Istituto Nazionale dei Tumori, Milano Disclosures Advisory: Astellas, Bayer, GSK Consultant: Pfizer, Novartis Background Mixed
Case(s): How to Deal with Mixed Response Giuseppe Procopio Fondazione IRCCS Istituto Nazionale dei Tumori, Milano Disclosures Advisory: Astellas, Bayer, GSK Consultant: Pfizer, Novartis Background Mixed
Sunitinib Treatment for Metastatic Renal Cell Carcinoma in Patients with Von Hippel-Lindau Disease
 pissn 1598-2998, eissn 2005-9256 Cancer Res Treat. 2013;45(4):349-353 Case Report http://dx.doi.org/10.4143/crt.2013.45.4.349 Open Access Sunitinib Treatment for Metastatic Renal Cell Carcinoma in Patients
pissn 1598-2998, eissn 2005-9256 Cancer Res Treat. 2013;45(4):349-353 Case Report http://dx.doi.org/10.4143/crt.2013.45.4.349 Open Access Sunitinib Treatment for Metastatic Renal Cell Carcinoma in Patients
RIP-Tag2 mouse model as a Paradigm for Target. Search in NETs
 RIP-Tag2 mouse model as a Paradigm for Target Search in NETs Oriol Casanovas, Ph.D. Tumor Angiogenesis Group INSTITUT CATALÀ d ONCOLOGIA IDIBELL Barcelona (SPAIN) Therapeutic Targeting of the Tumor Stroma
RIP-Tag2 mouse model as a Paradigm for Target Search in NETs Oriol Casanovas, Ph.D. Tumor Angiogenesis Group INSTITUT CATALÀ d ONCOLOGIA IDIBELL Barcelona (SPAIN) Therapeutic Targeting of the Tumor Stroma
Axitinib in renal cell carcinoma: now what do we do?
 Renal Cell Carcinoma Axitinib in renal cell carcinoma: now what do we do? Ian D. Davis Monash University Eastern Health Clinical School, Level 2, Box Hill, Victoria 3128, Australia Correspondence to: Ian
Renal Cell Carcinoma Axitinib in renal cell carcinoma: now what do we do? Ian D. Davis Monash University Eastern Health Clinical School, Level 2, Box Hill, Victoria 3128, Australia Correspondence to: Ian
Prospettive future nel trattamento medico del mrcc. Francesco Massari Oncologia Medica Policlinico S Orsola-Malpighi Bologna
 Prospettive future nel trattamento medico del mrcc Francesco Massari Oncologia Medica Policlinico S Orsola-Malpighi Bologna 3 rd YOUNG SPECIALIST RENAL CARE Firenze, 09 Aprile 2016 Renal cell carcinoma
Prospettive future nel trattamento medico del mrcc Francesco Massari Oncologia Medica Policlinico S Orsola-Malpighi Bologna 3 rd YOUNG SPECIALIST RENAL CARE Firenze, 09 Aprile 2016 Renal cell carcinoma
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Immunotherapy for the Treatment of Cancer
 Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
SBRT for lung metastases: Case report
 SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know
 Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current