Esophageal cancer: Biology, natural history, staging and therapeutic options
|
|
|
- Barbra Phelps
- 6 years ago
- Views:
Transcription
1 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section, Department of Surgery, Odense University Hospital, Denmark. University of Southern Denmark
 I III) (Subcardial) Stomach")
2 Anatomy Esophageal cancer Cardia cancer (Type I-III) I III) (Subcardial) Stomach cancer
 Siewert,, Type III: Gastric cancer (80% Barrett)")
3 Anatomy / Definitions Siewert,, Type I: Esophageal cancer Siewert,, Type II: True cardia cancer (stomach( stomach) Siewert,, Type III: Gastric cancer (80% Barrett)
4 Biology In the Western world, distal esophageal and GE adenocarcinoma is increasing in incidence faster than any other type of gastrointestinal cancer (Blot, Jama 1991) Metaplasia Dysplasia - Adenocarcinoma Reflux/Barrett Alcohol,, smoking, obesity, dietary deficiency, Helicobacter pylori, oro-pharyngeal cancer,
5 Staging & Resectability assessment AJCC & UICC staging correlate to longterm survival,, but estimates need improvement.. AJCC does not accurately predict survival in patients receiving multimodal therapy (Rizk,, J Clin Oncol 2007) Malignant LN Total number of examined LN (Rizk,, J Thorac Cardiovasc Surg 2006)
6 Staging & Resectability assessment Genes/molecules with prognostic impact cyclin D1, E-cadherin beta-catenin EGFR, Her-2/Neu, APC, TGF-beta, Endoglin, CTGF, upa MMP-1,3,7,9 TIMP T( h )1/T( h )2 balance CRP PTHrP Cox-2 P53, NF-kappaB Bcl-2, The best prognostic estimate is probably a combination of: several biomarkers macroscopically and microscopically description of tumor extent and lymph node involvement (Lagarde,, Ann Surg Oncol 2007)
 High-volume referral centers detect more metastases in EC than regional centers (van Vliet,, Am J Gastroenterol")
7 Staging & Resectability assessment Multidisciplinary teams are associated with improved outcome in esophageal cancer (Stephens, Dis Esophagus 2006) High-volume referral centers detect more metastases in EC than regional centers (van Vliet,, Am J Gastroenterol 2006)
8 Staging & Resectability assessment Esophageal cancer Palliation CT/PET-CT (Thorax/abdomen) Disseminated disease EUS Neo-adjuvant therapy indicated Neo-adjuvant therapy NOT indicated PET-CT 2-3 weeks therapy Laparoscopy + LUS (Thoracoscopy) PET-CT Responders Adjuvant therapy Resection Poor general condition/severe co- morbidity Non- Responders Con t Neo- adjuvant therapy
9 Staging: Cost-effectiveness CT+US vs EUS vs CT+LAP vs EUS+LAP/LUS EUS+LAP/LUS superior to CT based strategies (Mortensen, Surg Endosc 2000) CT vs EUS-FNA vs PET-CT vs Thoracoscopy/lap.sc vs combined strategies EUS-FNA + CT most inexpensive strategy (Using PET-CT in stead of CT increased the figures,, but was also more expensive) (Wallace, Ann Thorac Surg 2002)

10 Staging & Resectability assessment Don t forget the neck! 10-15% 15% of the patients have malignant supraclavicular nodes (Van Vliet,, J Surg Oncol 2007) US-FNA is cheap and simple
11 Staging & Resectability assessment Esophageal cancer Neck US (FNA) Palliation CT/PET-CT (Thorax/abdomen) Disseminated disease EUS Neo-adjuvant therapy indicated Neo-adjuvant therapy NOT indicated PET-CT 2-3 weeks therapy Laparoscopy + LUS (Thoracoscopy) PET-CT Responders Adjuvant therapy Resection Poor general condition/severe co- morbidity Non- Responders Con t Neo- adjuvant therapy
12 Treatment options Intended Curative Esophagectomy or resection of distal esophagus/proximal proximal stomach Endoscopic Mucosal Resection (EMR) Definitive chemoradiotherapy Palliative Relieving dysphagia Prolonging survival (chemotherapy) Symptomatic treatment
13 Treatment (left-sided) Thoraco-abdominal abdominal resection Transhiatal resection Combined abdominal and right sided thoracotomy (Lewis-Tanner) Abdominal resection (selected type (II)/III)
14 Surgical Treatment Combined abdominal and right sided thoracotomy OPEN resection THORACOSCOPIC/ LAPAROSCOPIC resection
 Virtual CT laparoscopic simulation (Lee, J Am Coll Surg")
15 Minimally invasive surgery Virtual CT thoracoscopy simulation (Morita, Abdom Imaging 2007) Virtual CT laparoscopic simulation (Lee, J Am Coll Surg 2003)

 may provide")

16 Minimally invasive surgery Thoracoscopic and Laparoscopic Ultrasound (TUS / LUS) may provide important information during minimally invasive procedures
17 Minimally invasive surgery Open vs Thoracoscopic assissted vs Minimally invasive Median blood loss: Operating time: Minimally invasive < Assisted < Open Assisted < Open < Minimally invasive Median hospitalization: Minimally invasive < Assisted < Open Advanced disease: Stricture formation: Open > Minimally invasive > Assisted Open < Assisted < Minimally invasive Survival and lymph node clearance: no differences (Smithers,, Ann Surg 2007)

 developed LN mets.")
 local recurrence 5-y cause-specific specific")
18 EMR EMR in cancers invading the muscularis mucosa is controversial (retrospective,, multicentre study,, N0, n=104 (111 lesions) 86 patients no further treatment 2 (1.9%) developed LN mets. 1 (1%) organ mets. 23 (20.7%) local recurrence 5-y cause-specific specific survival was 95% (Katada, Endoscopy 2007)
19 Neo-Adjuvant Treatment Mucinous cancer and Signet-ring cell cancer seem to have improved response to neo-adjuvant CRT (Chirieac, Clin Cancer Res 2005) (and neo-adjuvant therapy may provide a better chance of R0 resection in large GE junction tumors) Neo-adjuvant therapy + surgery > surgery alone in esophageal cancer, but there may be an increased operative risk (Gebski,, Lancet Oncol 2007)
20 Neo-Adjuvant Treatment Size (proportion) of residual carcinoma after CRT in esophageal cancer is significantly correlated with patterns of locoregional and distant failure (Rothagi,, Cancer 2005) Therefore, we need to find the responders within a few weeks of treatment! PET-CT is superior to other imaging modalities regarding the identification of responders to neoadjuvant therapy (Wong, Abdom Imaging 2007)
21 Neo-Adjuvant Treatment Esophageal cancer Neck US (FNA) Palliation CT/PET-CT (Thorax/abdomen) Disseminated disease EUS Neo-adjuvant therapy indicated Neo-adjuvant therapy NOT indicated PET-CT 2-3 weeks therapy Laparoscopy + LUS (Thoracoscopy) PET-CT Responders Adjuvant therapy Resection Poor general condition/severe co- morbidity Non- Responders Con t Neo- adjuvant therapy
22 Prognostic factors following surgery Preoperative morbidity (but not age) is important (Johansson, J Gastrointest Surg 2000) 30-d morbidity and mortality are lower in high-volume centers (Dimick,, Ann Thorac Surg 2001) 30-d mortality < 5% in experienced centers
23 Prognostic factors following surgery Size,, differentiation and subtype T stage N stage Vascular invasion Perineural and lymphatic invasion Ratio: Invaded/removed lymph nodes Residual tumor (R1/R2) - proximal margin - distal margin - circumferential margin (< 1mm) (Saha,, Dis Esophagus 2001) (Dexter,, Gut 2001) (Griffiths, Eur J Surg Oncol 2006)
24 Prognostic factors following surgery En-bloc vs transhiatal resection 50% vs 25% 5-y 5 survival (Sihvo,, Am J Gastroenterol 2004) En-bloc > Transhiatal if 1-88 positive nodes! (>8 positive nodes: n.d.).) (Johansson, Arch Surg 2004)

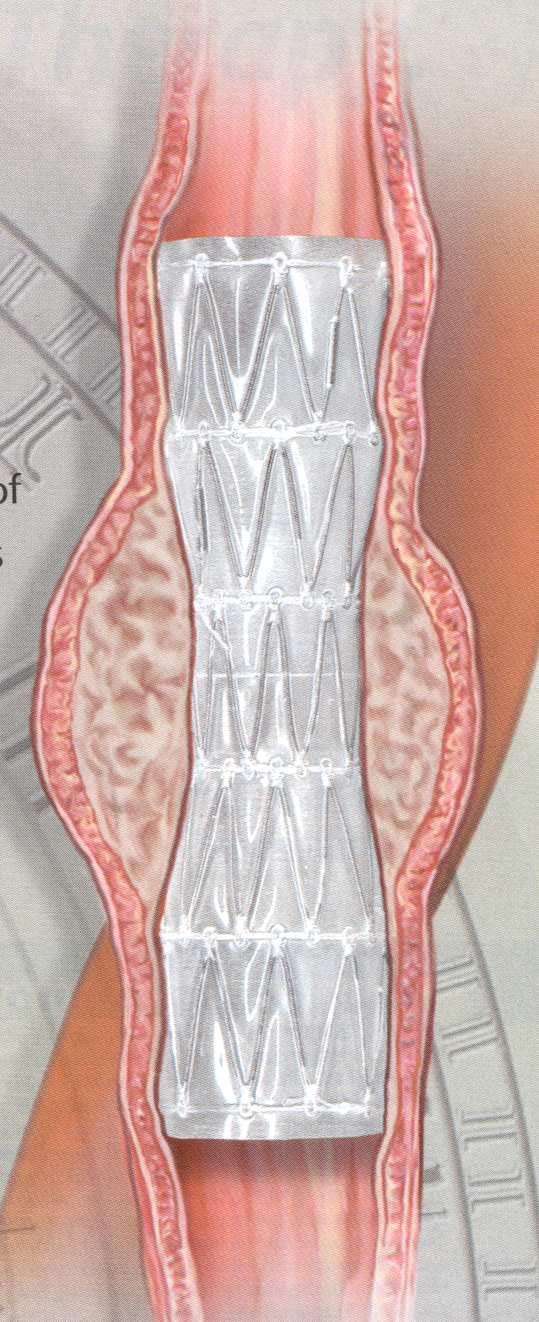
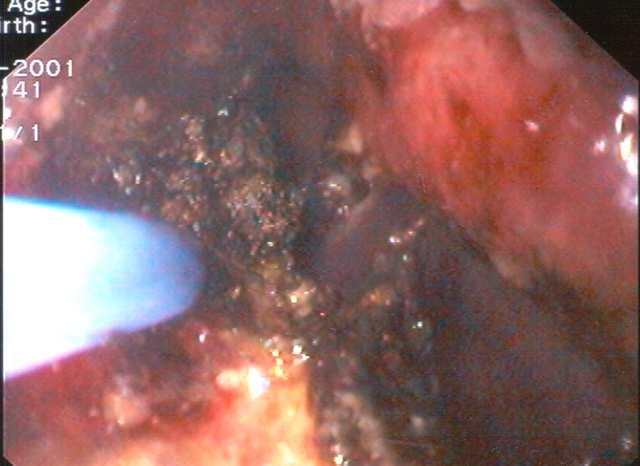
25 Treatment options Palliative Relieving dysphagia (APC/SEMS)
26 Conclusion Multidisciplinary evaluation & treatment High-volume centers Individual staging and tailored treatment Identification of responders/non non-responders to neo-adjuvant (adjuvant) therapy Focus on molecular, genetic and other factors regarding diagnosis, classification and treatment
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
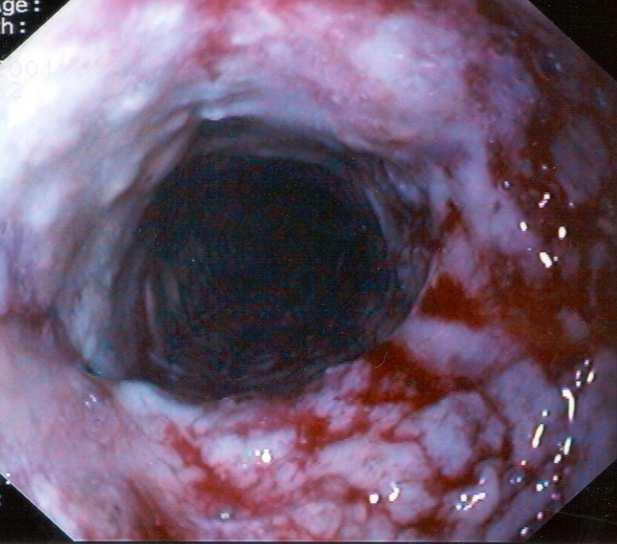
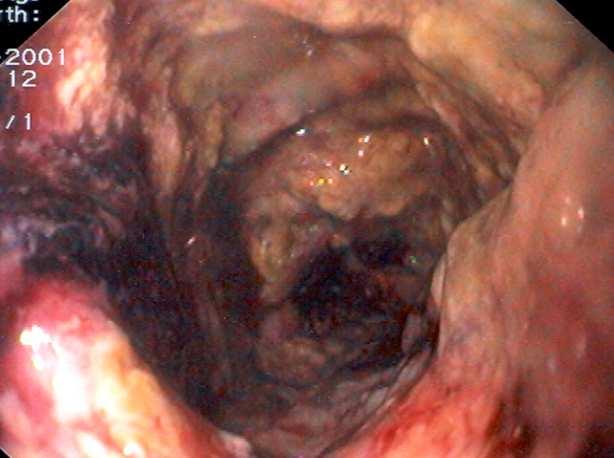
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Determining the Optimal Surgical Approach to Esophageal Cancer
 Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD
 Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
ESOPHAGEAL CANCER. Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds
 ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
Esophageal Cancer. Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care. David Demos MD Thoracic Surgery Aurora Cancer Care
 Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Adenocarcinoma of gastro-esophageal junction - Case report
 Case Report denocarcinoma of gastro-esophageal junction - Case report nupsingh Dhakre 1*, Ibethoi Yengkhom 2, Harshin Nagori 1, nup Kurele 1, Shreedevi. Patel 3 1 2 nd year Resident, 2 3rd year Resident,
Case Report denocarcinoma of gastro-esophageal junction - Case report nupsingh Dhakre 1*, Ibethoi Yengkhom 2, Harshin Nagori 1, nup Kurele 1, Shreedevi. Patel 3 1 2 nd year Resident, 2 3rd year Resident,
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
Minimally Invasive Esophagectomy
 Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Determining Resectability and Appropriate Surgery for Esophageal Cancer
 Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
B Breast cancer, managing risk of lobular, in hereditary diffuse gastric cancer, 51
 Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
1. Epidemiology of Esophageal Cancer 2. Operative Strategies 3. Minimally Invasive Esophagectomy 4. Video
 Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
A Proposed Strategy for Treatment of Superficial Carcinoma. in the Thoracic Esophagus Based on an Analysis. of Lymph Node Metastasis
 Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
سرطان المعدة. Gastric Cancer حمود حامد
 سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
The Learning Curve for Minimally Invasive Esophagectomy
 The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
7/20/2017. Esophageal Cancer: A Less Common But Deadly Cancer. Objectives. Disclosure Statement NYNPA Conference October Saratoga New York
 Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
How to stage early BE cancer - EUS or endoscopic removal?
 How to stage early BE cancer - EUS or endoscopic removal? Presented by Bas Weusten Institution St. Antonius Hospital, Nieuwegein Academic Medical Center, Amsterdam case 56 y old female patient Lung transplant
How to stage early BE cancer - EUS or endoscopic removal? Presented by Bas Weusten Institution St. Antonius Hospital, Nieuwegein Academic Medical Center, Amsterdam case 56 y old female patient Lung transplant
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Overall survival analysis of neoadjuvant chemoradiotherapy and esophagectomy for esophageal cancer
 Original Article Overall survival analysis of neoadjuvant chemoradiotherapy and esophagectomy for esophageal cancer Faisal A. Siddiqui 1, Katelyn M. Atkins 2, Brian S. Diggs 3, Charles R. Thomas Jr 1,
Original Article Overall survival analysis of neoadjuvant chemoradiotherapy and esophagectomy for esophageal cancer Faisal A. Siddiqui 1, Katelyn M. Atkins 2, Brian S. Diggs 3, Charles R. Thomas Jr 1,
Towards a more personalized approach in the treatment of esophageal cancer focusing on predictive factors in response to chemoradiation Wang, Da
 University of Groningen Towards a more personalized approach in the treatment of esophageal cancer focusing on predictive factors in response to chemoradiation Wang, Da IMPORTANT NOTE: You are advised
University of Groningen Towards a more personalized approach in the treatment of esophageal cancer focusing on predictive factors in response to chemoradiation Wang, Da IMPORTANT NOTE: You are advised
Clinicopathologic and prognostic factors of young and elderly patients with esophageal adenocarcinoma: is there really a difference?
 Diseases of the Esophagus (2008) 21, 596 600 DOI: 10.1111/j.1442-2050.2008.00817.x Original article Clinicopathologic and prognostic factors of young and elderly patients with esophageal adenocarcinoma:
Diseases of the Esophagus (2008) 21, 596 600 DOI: 10.1111/j.1442-2050.2008.00817.x Original article Clinicopathologic and prognostic factors of young and elderly patients with esophageal adenocarcinoma:
 Lya Crichlow, MD Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference Case presentation 56 year old male who presented with 1 week history of dysphagia Unable to tolerate solids
Lya Crichlow, MD Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference Case presentation 56 year old male who presented with 1 week history of dysphagia Unable to tolerate solids
Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006
 Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006 Esophageal Cancer - Est. 15,000 cases in 2006 - Est. 14,000 deaths - Overall 5-year survival: 15.6% - 33.6 % for local
Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006 Esophageal Cancer - Est. 15,000 cases in 2006 - Est. 14,000 deaths - Overall 5-year survival: 15.6% - 33.6 % for local
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Newly Diagnosed Cases Cancer Related Death NCI 2006 Data
 Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Earlyoesophagealcancer. dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia
 Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
CLINICAL EFFECTIVENESS
 Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Basic Principles of Esophageal Surgery. 1 Surgical Anatomy of the Esophagus... 3
 Contents Basic Principles of Esophageal Surgery 1 Surgical Anatomy of the Esophagus... 3 D. C. Broering, J. Walter, Z. Halata ] Topography of the esophagus... 3 ] Development of the esophagus... 4 ] Structure
Contents Basic Principles of Esophageal Surgery 1 Surgical Anatomy of the Esophagus... 3 D. C. Broering, J. Walter, Z. Halata ] Topography of the esophagus... 3 ] Development of the esophagus... 4 ] Structure
Diagnosis and Preoperative Staging of Esophageal Cancer
 2 Diagnosis and Preoperative Staging of Esophageal Cancer ARNOLD J. MARKOWITZ, MD HANS GERDES, MD The clinical presentation of esophageal cancer in the United States and Europe has been changing, but unfortunately,
2 Diagnosis and Preoperative Staging of Esophageal Cancer ARNOLD J. MARKOWITZ, MD HANS GERDES, MD The clinical presentation of esophageal cancer in the United States and Europe has been changing, but unfortunately,
Esophageal Cancer. What is esophageal cancer?
 Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand?
 MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
How to treat early gastric cancer? Endoscopy
 How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
Lymph node invasion might have more prognostic impact than R status in advanced esophageal adenocarcinoma
 The American Journal of Surgery (2013) 205, 711-717 Clinical Surgery Lymph node invasion might have more prognostic impact than R status in advanced esophageal adenocarcinoma Magali Cabau, M.D. a, Guillaume
The American Journal of Surgery (2013) 205, 711-717 Clinical Surgery Lymph node invasion might have more prognostic impact than R status in advanced esophageal adenocarcinoma Magali Cabau, M.D. a, Guillaume
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Endoscopic Ultrasonography Clinical Impact. Giancarlo Caletti. Gastroenterologia Università di Bologna. Caletti
 Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
 Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
Surgical strategies in esophageal cancer
 Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
The CROSS road in neoadjuvant therapy for esophageal cancer: long-term results of CROSS trial
 Editorial The CROSS road in neoadjuvant therapy for esophageal cancer: long-term results of CROSS trial Ian Wong, Simon Law Division of Esophageal and Upper Gastrointestinal Surgery, Department of Surgery,
Editorial The CROSS road in neoadjuvant therapy for esophageal cancer: long-term results of CROSS trial Ian Wong, Simon Law Division of Esophageal and Upper Gastrointestinal Surgery, Department of Surgery,
Characteristics and prognostic factors of synchronous multiple primary esophageal carcinoma: A report of 52 cases
 Thoracic Cancer ISSN 1759-7706 ORIGINAL ARTICLE Characteristics and prognostic factors of synchronous multiple primary esophageal carcinoma: A report of 52 cases Mei Li & Zhi-xiong Lin Department of Radiation
Thoracic Cancer ISSN 1759-7706 ORIGINAL ARTICLE Characteristics and prognostic factors of synchronous multiple primary esophageal carcinoma: A report of 52 cases Mei Li & Zhi-xiong Lin Department of Radiation
Oesophagogastric Cancer The Patient s Pathway
 National helpline: 0121 704 9860 V1 Oesophagogastric Cancer The Patient s Pathway {Based on The St Thomas Hospital Pathway} Registered Charity No. 1062461 Contents Introduction 3-5 Curative pathway 5-7
National helpline: 0121 704 9860 V1 Oesophagogastric Cancer The Patient s Pathway {Based on The St Thomas Hospital Pathway} Registered Charity No. 1062461 Contents Introduction 3-5 Curative pathway 5-7
Gastric Cancer: Etiologic Factors. H. Pylori diet (salt, nitrates) lifestyle (smoking, obesity) familial (~10% in West) diet hereditary
 lifestyle (smoking, obesity) familial (~10% in West) diet hereditary") Issue #1: Premalignant Lesions Gastric Cancer: Etiologic Factors H. Pylori diet (salt, nitrates) lifestyle (smoking, obesity) familial (~10% in West) diet hereditary HNPCC DGC Lauren Classification of
Issue #1: Premalignant Lesions Gastric Cancer: Etiologic Factors H. Pylori diet (salt, nitrates) lifestyle (smoking, obesity) familial (~10% in West) diet hereditary HNPCC DGC Lauren Classification of
Treatment Strategy for Non-curative Resection of Early Gastric Cancer. Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea
 Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Di Lu 1#, Xiguang Liu 1#, Mei Li 1#, Siyang Feng 1#, Xiaoying Dong 1, Xuezhou Yu 2, Hua Wu 1, Gang Xiong 1, Ruijun Cai 1, Guoxin Li 3, Kaican Cai 1
 Case Report Three-port mediastino-laparoscopic esophagectomy (TPMLE) for an 81-year-old female with early-staged esophageal cancer: a case report of combining single-port mediastinoscopic esophagectomy
Case Report Three-port mediastino-laparoscopic esophagectomy (TPMLE) for an 81-year-old female with early-staged esophageal cancer: a case report of combining single-port mediastinoscopic esophagectomy
Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012
 Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012 Esophageal Leiomyoma Introduction Case presentation Operative video Discussion Esophageal Leiomyoma Benign tumors of the
Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012 Esophageal Leiomyoma Introduction Case presentation Operative video Discussion Esophageal Leiomyoma Benign tumors of the
ESOPHAGEAL CANCER. Epidemiology 3/22/2017. Esophageal Carcinoma: subtypes. Esophageal Adenocarcinoma (EAC) Epidemiology.
 Epidemiology.") ESOPHAGEAL CANCER Disclosures Sushil Ahlawat, MD, FACP, FASGE, AGAF Associate Professor of Medicine Director of Endoscopy RUTGERS NJMS Nothing to disclose. Esophageal Carcinoma: subtypes Subtype Squamous
ESOPHAGEAL CANCER Disclosures Sushil Ahlawat, MD, FACP, FASGE, AGAF Associate Professor of Medicine Director of Endoscopy RUTGERS NJMS Nothing to disclose. Esophageal Carcinoma: subtypes Subtype Squamous
Gastric Cancer: Surgery and Regional Therapy. Epidemiology. Risk factors
 Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Original articledote_1350. S. P. Mehta, 1 P. Jose, 1,2 A. Mirza, 3 S. A. Pritchard, 3 J. D. Hayden, 1 and H. I. Grabsch 2
 1..7 Diseases of the Esophagus (2012), DOI: 10.1111/j.1442-2050.2012.01350.x Original articledote_1350 Comparison of the prognostic value of the 6th and 7th editions of the Union for International Cancer
1..7 Diseases of the Esophagus (2012), DOI: 10.1111/j.1442-2050.2012.01350.x Original articledote_1350 Comparison of the prognostic value of the 6th and 7th editions of the Union for International Cancer
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
A study on clinicopathological features and prognostic factors of patients with upper gastric cancer and middle and lower gastric cancer.
 Biomedical Research 2018; 29 (2): 365-370 ISSN 0970-938X www.biomedres.info A study on clinicopathological features and prognostic factors of patients with upper gastric cancer and middle and lower gastric
Biomedical Research 2018; 29 (2): 365-370 ISSN 0970-938X www.biomedres.info A study on clinicopathological features and prognostic factors of patients with upper gastric cancer and middle and lower gastric
SMALL BOWEL ADENOCARCINOMA. Dr. C. Jeske
 SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
Stenting for Esophageal Cancer Technical Issues and Outcomes
 Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Determining the optimal number of lymph nodes harvested during esophagectomy
 Original Article Determining the optimal number of lymph nodes harvested during esophagectomy Khaldoun Almhanna, Jill Weber, Ravi Shridhar, Sarah Hoffe, Jonathan Strosberg, Kenneth Meredith Department
Original Article Determining the optimal number of lymph nodes harvested during esophagectomy Khaldoun Almhanna, Jill Weber, Ravi Shridhar, Sarah Hoffe, Jonathan Strosberg, Kenneth Meredith Department
Surgery for Gastric and Oesophageal Cancer
 Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition
 22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Pancreatic Adenocarcinoma
 Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
MEDIASTINAL STAGING surgical pro
 MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
Current status of gastric ESD in Korea. Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea
 Current status of gastric ESD in Korea Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea Contents Brief history of gastric ESD in Korea ESD/EMR for gastric adenoma
Current status of gastric ESD in Korea Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea Contents Brief history of gastric ESD in Korea ESD/EMR for gastric adenoma
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Esophageal Cancer: A Multimodality Approach to Detection and Staging
 Esophageal Cancer: A Multimodality Approach to Detection and Staging, MBA Topic: Esophageal Cancer Imaging: A multimodality approach Conference: Society of Thoracic Imaging Location: Date/Time: March 14,
Esophageal Cancer: A Multimodality Approach to Detection and Staging, MBA Topic: Esophageal Cancer Imaging: A multimodality approach Conference: Society of Thoracic Imaging Location: Date/Time: March 14,
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Health-related quality of life measure distinguishes between low and high clinical T stages in esophageal cancer
 Original Article Page 1 of 5 Health-related quality of life measure distinguishes between low and high clinical T stages in esophageal cancer Biniam Kidane 1,2, Amir Ali 1, Joanne Sulman 2,3, Rebecca Wong
Original Article Page 1 of 5 Health-related quality of life measure distinguishes between low and high clinical T stages in esophageal cancer Biniam Kidane 1,2, Amir Ali 1, Joanne Sulman 2,3, Rebecca Wong
Approaches to Surgical Treatment of Gastric Cancer. Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service
 Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ
 Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ 1. Introduction 2. Epidemiology 3. Gastric cancer and pancreatic cancer a. Risk factors b. Symptoms c. Location d. Diagnosis e. Histopathology
Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ 1. Introduction 2. Epidemiology 3. Gastric cancer and pancreatic cancer a. Risk factors b. Symptoms c. Location d. Diagnosis e. Histopathology
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
L impatto dell imaging sulla definizione della strategia terapeutica
 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
Three Case Reports of Neoplasms of the Esophagogastric Junction
 Case report Three Case Reports of Neoplasms of the Esophagogastric Junction Roberto Rodríguez, MD, 1 Isabel Díaz, MD, 2 Alejandro Flórez, MD, 2 Fabiola Donado, MD. 3 1 Internist, Gastroenterologist, Endoscopist
Case report Three Case Reports of Neoplasms of the Esophagogastric Junction Roberto Rodríguez, MD, 1 Isabel Díaz, MD, 2 Alejandro Flórez, MD, 2 Fabiola Donado, MD. 3 1 Internist, Gastroenterologist, Endoscopist
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer
 Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research