Sepsis Denials. Presented by James Donaher, RHIA, CDIP, CCS, CCS-P
|
|
|
- Jack Lee
- 6 years ago
- Views:
Transcription
1 Sepsis Denials Presented by James Donaher, RHIA, CDIP, CCS, CCS-P
2 Sepsis-1 2 From the first Sepsis Definition Conference in 1991 Defined sepsis as systemic response syndrome (SIRS) due to infection SIRS defined as meeting more than 1 of 4 findings: Body Temperature >38.0 C or <36.0 C Heart Rate > 20 beats/min Tachypnea >20 breaths/min or hyperventilation with PaCO 2 <32 mm Hg WBC (WBC) count > 12,000 cells/mm 3 Severe sepsis defined as sepsis associated with organ dysfunction Septic shock defined as sepsis with arterial hypotension despite adequate fluid resuscitation
3 Sepsis-2 3 Research data showed a need to modify Sepsis-1 criteria to better reflect evolving knowledge of the pathophysiology of SIRS and severe sepsis A second International Sepsis Definition Conference was convened in 2001 with the results published in 2003 The basic definitions for sepsis and severe sepsis remained in tact The criteria defining SIRS were greatly expanded (slide 6) Organ dysfunction variables for severe sepsis were more clearly defined Criteria for septic shock were specified under hemodynamic variables
4 Sepsis-2 4 As a diagnostic requirement, Sepsis-2 states some of the expanded criteria must be present Allows broad clinical flexibility in applying the criteria From Sepsis-2 comes the requirement for documentation supporting just how sick the patient appears (e.g. This toxic appearing patient. This very ill-appearing patient. ) Sepsis-2 eliminated the requirement for positive blood cultures to confirm a diagnosis of sepsis If in the physician s opinion, a criterion can be explained by a coexisting condition, then that criterion should not count!
5 Sepsis-2 5 Since 2003 the Surviving Sepsis Campaign consistently reaffirms the 2001 criteria as the current standard with even further detail added Unfortunately many continue to use the criteria established for Sepsis-1 which lack precision The most recent Surviving Sepsis Campaign guidelines released in early 2017 began to accept at least some of the Sepsis-3 definitions and criteria Eliminates severe sepsis as a category Eliminates SIRS along with all other specific clinical parameters of end-organ dysfunction Does not accept or recommend qsofa as best practice

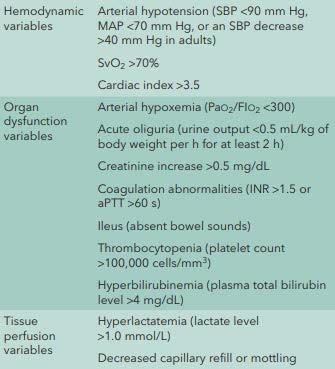
6 2001 Diagnostic Criteria for Sepsis 6

7 Rules for Sepsis 2 Diagnostic Criteria 7
8 Issues with Sepsis 8 High mortality rate Difficult to diagnose Variable clinical presentations Few unifying pathological features Could be an appropriate host response SIRS presentation may be non-infective Increased WBC counts could be indicative of a non-infectious process Medication-induced Stress-induced Sepsis is dynamic! Shifting clinical and laboratory manifestations Not all criteria present at once Resource-intensive and costly making it highly audited!
9 Sepsis-3 9 The Third International Consensus Definitions for Sepsis and Septic Shock published February 23, 2016 By a task force of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine among others Defines sepsis as life-threatening organ dysfunction caused by a dysregulated host response to infection [suspected or confirmed] The host is actually injuring its own tissues and organs Abandons the concept of sepsis as SIRS due to infection -- after 25 years! Sepsis-3 offers two standards for identifying organ dysfunction
10 SOFA: Defining Sepsis 10 Sequential [sepsis-related] Organ Failure Assessment Won out over the Logical Organ Dysfunction System (LODS) SOFA considered easier to calculate Previously used to assess mortality in intensive care units SOFA grades the function of 6 organ systems on a scale of 0 to 4 Based on the degree of dysfunction Uses objective measures (slide 13) Assumed to be 0 for patients with no preexisting organ dysfunction
11 SOFA: Meeting the Requirement 11 One-point increase in at least two organ systems Two-point increase or more in one organ system
12 SOFA: Six Organ Systems Used Respiratory 2. Coagulation 3. Hepatic 4. Cardiovascular 5. Central Nervous System 6. Renal
13 SOFA: Scoring 13
14 qsofa 14 q = quick Derived from SOFA through multivariate logistic regression that showed good predictive value of these more easily attained variables Bedside clinical approach to identify patients with high risk for adverse outcomes Designed to be fast and easy for the healthcare environment Does not require laboratory tests Based on the presence of 2 or more of 3 criteria Altered mentation Respiratory rate 22 breaths/min Systolic blood pressure 100 mm Hg A positive score would prompt clinicians to: Look for organ dysfunction Initiate or escalate therapy Consider critical care Intended as a useful tool and not a substitute for SOFA criteria Not accepted by the Surviving Sepsis Campaign as of 2017
15 Sepsis-3: Severe Sepsis and Septic Shock 15 Sepsis-3 considers the term severe sepsis to be redundant Sepsis without organ dysfunction does not exist Strict definition of septic shock: Persisting hypotension requiring vasopressors to maintain mean arterial pressure (MAP) > 65 mmhg and a serum lactate level > 2 mmol/l (18 mg/dl) despite adequate volume resuscitation.
16 Issues with Using SIRS Criteria 16 SIRS may reflect an appropriate host response to infection Infective and non-infective SIRS can co-exist Elevated WBC count could indicate stress and not infection Sepsis is dynamic and its manifestations can change without all criteria being present at once SIRS fails to promote an understanding of the underlying problem or disease process Hypotensive patients do not necessarily have shock Patients in shock may not be hypotensive
17 Issues with Using Sepsis-3 17 Inconsistent with the ICD-10-CM Official Guidelines for Coding and Reporting (OCG) Required under HIPAA Distinguishes between sepsis with or without organ dysfunction Adherence to Sepsis-3 by not reporting any cases of sepsis without organ dysfunction would disrupt: Coding Reimbursement Quality Analysis Regulatory Oversight
18 Issues with Using Sepsis-3 18 Additionally the Sepsis-3 consensus recommends Reporting R65.20 as principal for severe sepsis Reporting R65.21 as principal for septic shock I.d.1)(a) of the OCG states: For a diagnosis of sepsis, assign the appropriate code for the underlying systemic infection. If the type of infection or causal organism is not further specified, assign code A41.9, Sepsis, unspecified organism.
19 Issues with Using Sepsis-3 19 OCG continue with: A code from subcategory R65.2, Severe sepsis, should not be assigned unless severe sepsis or an associated acute organ dysfunction is documented. Following Sepsis-3 definitions will leave the expectations and practices for U.S. national coding and reporting requirements unmet The Sepsis-3 task force was comprised of 19 scientists Consensus for future clinical research Debate in the U.S. over early enough recognition of sepsis Limitations in the actual clinic setting
20 ACDIS Advisory Board 20 Letter to the Sepsis-3 authors indicating conflicts with OCG and current CMS quality measures Position white paper stating: While Sepsis-3 definitions set forth compelling evidence that cannot be dismissed, it remains to be seen how the clinical community will be able to operationalize or change its understanding of sepsis and septic shock. ACDIS cautioned against adopting the new guidelines into CDI programs
21 CMS 2015 Core Measure for Treating Sepsis 21 a.k.a Severe Sepsis/Septic Shock Early Management Bundle or SEP-1 Comes from the National Quality Foundation s early-goal-directed therapy (EGDT) Not well received by the medical community Would prefer sensitivity to specificity Inconsistent with the definitions used in evidence-based studies since 2001 Premature with no clear definitions for sepsis, severe sepsis or septic shock Reimbursement withheld if noncompliant with any portion of the measure which may be inappropriate for certain patients
22 CMS 2015 Core Measure for Treating Sepsis 22 Two main problems: CMS definition-selected lactate values are below the threshold of widely accepted and studied lactate levels Government-issued definitions for a disease that presents with a great deal of variability and where no gold standard definition exists Derived from the Surviving Sepsis Campaign and the National Quality Foundation definitions CMS altered the lactate value Next slide just to indicate the various methodologies --

23 23
24 Clinical Validation 24 Both a concept and a process Diagnoses documented in the medical record must be substantiated by clinical criteria generally accepted by the medical community Authoritative professional guidelines Consensus Evidence-based sources In the absence of such sources Clinical diagnostic standards that most clinicians in a comparable specialty would reasonably agree are sufficient for establishing a particular diagnosis
25 Clinical Validation 25 If the criteria are not met, but still the physician feels the diagnosis is valid, the physician must document a plausible alternative basis for the diagnosis that other clinicians would deem reasonable. Medicare requires that claims submitted for payment must not include codes for diagnoses that cannot be clinically validated. Payers and auditors apply clinical validation processes to professional and institutional claims to determine whether the submitted diagnoses are substantiated by widely accepted clinical criteria.
26 Clinical Validation 26 Payers focus on diagnoses known for clinical validation deficiencies: Sepsis Acute respiratory failure Pancreatitis Severe malnutrition Acute kidney injury Denials will often read although well documented
27 Clinical Validation 27 Clinicians need to keep current of authoritative standards and apply this in diagnosing patients Coders should not be held accountable for clinical validation Well beyond their scope But remain informed and involved If a clinician reasonably bases a diagnostic determination on something other than the widely recognized criteria, the rationale should be clearly stated I the record.
28 Clinical Validation 28 The 2017 ICD-10-CM Official Guidelines for Coding and Reporting (OCG), I.A.19, Code Assignment and Clinical Criteria: The assignment of a diagnosis code is based on the provider s diagnostic statement that the condition exists. The provider s statement the patient has a particular condition is sufficient. Code assignment is not abased on clinical criteria used b the provider to establish the diagnosis. Perplexing and problematic creating a dilemma for many! Actually just clarifying that it is the clinicians responsibility to ensure the diagnoses documented in the medical record are clinically valid.
29 Clinical Validation 29 Thus alleviating the coder from the responsibility for making such clinical distinctions Clinical validation remains a contractual, regulatory and statutory necessity! If clinicians do not consider the validity of diagnoses being reported, they will not be in compliance with CMS regulations and policies. This is where clinical documentation integrity and improvement comes into play!
30 Clinical Validation 30 CDI reviews the medical record concurrently and is in a position to have any necessary conversations with clinicians to ensure every diagnosis being documented is clinically valid The medical record should then be good to go at the time of discharge Ensuring clinical validity will ensure a solid appeal of any denial
31 Denials Management for Sepsis 31 Sepsis criteria used by hospitals may not have actually been intended for billing purposes Intended clinically to ensure better outcomes by casting a wide enough net to capture early sepsis Clinical parameters can and do change Consistent documentation of the patient s condition will always lead to appropriate coding, billing and reimbursement!
32 Denials Management for Sepsis 32 The only ironclad/bulletproof defense for a sepsis denial is documentation showing a clear delineation of a non-systemic infection! An H&P that adequately captures the severity of illness by the depiction of the patient s signs and symptoms Explanation of the significance of any workup findings (risk for organ dysfunction) Accounting of the patient s course of hospitalization (including response to treatment) When all of these depict a clinical picture of sepsis the record will withstand scrutiny! When documentation does not show anything beyond what is expected from a local infection, then it is not sepsis!
33 Denials Management for Sepsis 33 With definitions in flux, now is the time for facilities to review their sepsis criteria standards, required documentation and coding practices to avoid lost reimbursement Payers and auditors are using the new sepsis criteria Facilities will also need to begin to move in that direction Trickle down to coding criteria and guidelines has been slow! Clinicians and coders still use the old SIRS criteria Coders code from physician documentation This gap opens the door for denials! Education!
")
34 Denials Management for Sepsis (HCCA) 34
")
35 Denials Management for Sepsis (HCCA) 35
36 Thank you! 36
Sepsis: Mitigating Denials Amid Definition Disparity
 Sepsis: Mitigating Denials Amid Definition Disparity White Paper - April 2017 Sepsis Criteria at a Glance The Society of Critical Care Medicine (SCCM) met in 2016 to update the definition of sepsis. During
Sepsis: Mitigating Denials Amid Definition Disparity White Paper - April 2017 Sepsis Criteria at a Glance The Society of Critical Care Medicine (SCCM) met in 2016 to update the definition of sepsis. During
JAMA. 2016;315(8): doi: /jama
: doi: /jama") JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
What the ED clinician needs to know about SEPSIS - 3. Anna Morgan Consultant EM Barts Health
 What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
Sepsis clinical evolution: Understand essential challenges to developing effective queries
 Understand essential challenges to developing effective queries ADVICE FROM THE ACDIS REGULATORY COMMITTEE Summary: This paper provides a timeline of the various sepsis definitions and their implications
Understand essential challenges to developing effective queries ADVICE FROM THE ACDIS REGULATORY COMMITTEE Summary: This paper provides a timeline of the various sepsis definitions and their implications
Sepsis and Septic Shock: New Definitions for Adults
 PL Detail-Document #320424 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER April 2016 Sepsis and Septic
PL Detail-Document #320424 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER April 2016 Sepsis and Septic
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
How R are you coding severe sepsis? Why the R-code matters
 How R are you coding severe sepsis? Why the R-code matters WHITE PAPER Summary: This article briefly reviews aspects of differing definitions of severe sepsis, and provides commentary on perceived areas
How R are you coding severe sepsis? Why the R-code matters WHITE PAPER Summary: This article briefly reviews aspects of differing definitions of severe sepsis, and provides commentary on perceived areas
Global Updates on Sepsis. Lizzie Barrett Nurse Educator, Intensive Care Unit Nepean Hospital, Sydney, Australia Prepared August 2016
 Global Updates on Sepsis Lizzie Barrett Nurse Educator, Intensive Care Unit Nepean Hospital, Sydney, Australia Prepared August 2016 The global picture Sepsis affects approx. 30 million people worldwide
Global Updates on Sepsis Lizzie Barrett Nurse Educator, Intensive Care Unit Nepean Hospital, Sydney, Australia Prepared August 2016 The global picture Sepsis affects approx. 30 million people worldwide
3 papers from ED. counting sepsis sepsis 3 wet or dry?
 3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Wait, is this sepsis?
 Wait, is this sepsis? Reconciling Disparate Sepsis Definitions LAURA QUINNAN, M.D. NWH SEPSIS COMMITTEE CO-CHAIR, CHIEF OF MEDICINE AND MEDICAL DIRECTOR OF HOSPITALIST TEAM Goals Describe Sepsis-3 definitions
Wait, is this sepsis? Reconciling Disparate Sepsis Definitions LAURA QUINNAN, M.D. NWH SEPSIS COMMITTEE CO-CHAIR, CHIEF OF MEDICINE AND MEDICAL DIRECTOR OF HOSPITALIST TEAM Goals Describe Sepsis-3 definitions
Special Panel Session: New Sepsis Definition
 Special Panel Session: New Sepsis Definition 1 Today s Panelists Include: Richard Pinson, MD, FACP, CCS, Principal and Medical Director, Pinson and Tang Consultants James S. Kennedy, MD, CCS, CCDS, CDIP,
Special Panel Session: New Sepsis Definition 1 Today s Panelists Include: Richard Pinson, MD, FACP, CCS, Principal and Medical Director, Pinson and Tang Consultants James S. Kennedy, MD, CCS, CCDS, CDIP,
SUCCESS IN SEPSIS MORTALITY REDUCTION. Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar
 SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
Sepsis-3: clarity or confusion
 Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis Learning Collaborative: Sepsis New Definitions
 Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Sepsis - A Year in Transition
 Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
SEPSIS-3: THE NEW DEFINITIONS
 SEPSIS-3: THE NEW DEFINITIONS WHAT THEY SHOULD MEAN TO YOU MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK https://www.youtube.com/watch?v=1s8l5d2xr6w IN THE
SEPSIS-3: THE NEW DEFINITIONS WHAT THEY SHOULD MEAN TO YOU MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK https://www.youtube.com/watch?v=1s8l5d2xr6w IN THE
NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content
 NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content Adherence variables Q: within 3 hours of the start datetime. How can we document that monotherapy was started before
NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content Adherence variables Q: within 3 hours of the start datetime. How can we document that monotherapy was started before
A BRIEF HISTORY OF SEPSIS. Euan Mackay
 A BRIEF HISTORY OF SEPSIS Euan Mackay Aims History of sepsis definition Validity of new definition Hippocrates 4 th century BC Hippocrates introduced the term "σήψις the process of decay or decomposition
A BRIEF HISTORY OF SEPSIS Euan Mackay Aims History of sepsis definition Validity of new definition Hippocrates 4 th century BC Hippocrates introduced the term "σήψις the process of decay or decomposition
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Effectively Managing Sepsis Denials
 Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Text-based Document. Implications of the Sepsis-3 Definition on Nursing Research and Practice. Authors Peach, Brian C. Downloaded 5-Jul :03:48
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Sepsis: What Is It Really?
 Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Resuscitation Symposium Resuscitation Literature Update. Abdullah Al Reesi, MD, MSc, FACEP, FRCPC Sr. Consultant and HoD SQUH
 Resuscitation Symposium Resuscitation Literature Update Abdullah Al Reesi, MD, MSc, FACEP, FRCPC Sr. Consultant and HoD SQUH Objectives Review recent articles in sepsis New sepsis definition High versus
Resuscitation Symposium Resuscitation Literature Update Abdullah Al Reesi, MD, MSc, FACEP, FRCPC Sr. Consultant and HoD SQUH Objectives Review recent articles in sepsis New sepsis definition High versus
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Debugging Sepsis: Documentation and Coding Guidelines
 Debugging Sepsis: Documentation and Coding Guidelines Michael Kaitschuck, RHIA, CPHIMS, CPHQ, CCS, CCDS, CDIP Director of Coding and Clinical Documentation Improvement Harris Health System 1 SIRS Diagnostic
Debugging Sepsis: Documentation and Coding Guidelines Michael Kaitschuck, RHIA, CPHIMS, CPHQ, CCS, CCDS, CDIP Director of Coding and Clinical Documentation Improvement Harris Health System 1 SIRS Diagnostic
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Sepsis. Current Dilemmas in Diagnosing Sepsis. Chapter 2
 Chapter 2 Current Dilemmas in Diagnosing Derek Braun Derek Braun, Banner Health, 2901 N. Central Ave. Ste 180, Phoenix, AZ 85012 Email: derek.braun@bannerhealth.com Abbreviations: APACHE : Acute Physiology,
Chapter 2 Current Dilemmas in Diagnosing Derek Braun Derek Braun, Banner Health, 2901 N. Central Ave. Ste 180, Phoenix, AZ 85012 Email: derek.braun@bannerhealth.com Abbreviations: APACHE : Acute Physiology,
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Sepsis 3.0: pourquoi une nouvelle définition?
 Sepsis 3.0: pourquoi une nouvelle définition? Jean-Daniel Chiche, MD PhD MICU & Dept Infection, Immunity & Inflammation Hôpital Cochin & Institut Cochin, Paris-F JAMA 2016; 315(8) WHY 1991 & 2001 Definitions:
Sepsis 3.0: pourquoi une nouvelle définition? Jean-Daniel Chiche, MD PhD MICU & Dept Infection, Immunity & Inflammation Hôpital Cochin & Institut Cochin, Paris-F JAMA 2016; 315(8) WHY 1991 & 2001 Definitions:
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Sepsis and Septicemia: Clear up Coding and Documentation Confusion october 2009
 Sepsis and Septicemia: Clear Up Coding and Documentation Confusion W h i t e p a p e r Sepsis. Severe sepsis. SIRS. Septicemia. Unfortunately, this isn t a case of tomato, tomahto. Coders and physicians
Sepsis and Septicemia: Clear Up Coding and Documentation Confusion W h i t e p a p e r Sepsis. Severe sepsis. SIRS. Septicemia. Unfortunately, this isn t a case of tomato, tomahto. Coders and physicians
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis as Seen by the CMO. Randy C. Roth, MD Chief Medical Officer
 Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions
 Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Learning Objectives. Guidance Hierarchy. AHA Coding Clinic Update
 1 AHA Coding Clinic Update Nelly Leon Chisen, RHIA Director, Coding and Classification Executive Editor, Coding Clinic American Hospital Association Chicago, IL Learning Objectives At the completion of
1 AHA Coding Clinic Update Nelly Leon Chisen, RHIA Director, Coding and Classification Executive Editor, Coding Clinic American Hospital Association Chicago, IL Learning Objectives At the completion of
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Diagnosis and Management of Sepsis. Disclosures
 Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsi: nuove definizioni, approccio diagnostico e terapia
 GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
Update on Sepsis Diagnosis and Management
 CHAPTER 12 Update on Sepsis Diagnosis and Management Kevin Alexander, DPM INTRODUCTION Sepsis and septic shock have become a large problem in the health care system that affects at least 1 million people
CHAPTER 12 Update on Sepsis Diagnosis and Management Kevin Alexander, DPM INTRODUCTION Sepsis and septic shock have become a large problem in the health care system that affects at least 1 million people
Consensus Definitions for Sepsis and Septic Shock (Sepsis-III)
") Consensus Definitions for Sepsis and Septic Shock (Sepsis-III) Advantages and Disadvantages Dr. Luis García-Castrillo Content: Reasons for new definition. Advantages of Sepsis III. Disadvantages of Sepsis
Consensus Definitions for Sepsis and Septic Shock (Sepsis-III) Advantages and Disadvantages Dr. Luis García-Castrillo Content: Reasons for new definition. Advantages of Sepsis III. Disadvantages of Sepsis
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Basics from anatomy and physiology classes Local tissue reactions
 Septicaemia & SIRS Septicaemia is a life-threatening condition that arises when the physical reaction to an infection, causes damage to tissue and organs Basics from anatomy and physiology classes Local
Septicaemia & SIRS Septicaemia is a life-threatening condition that arises when the physical reaction to an infection, causes damage to tissue and organs Basics from anatomy and physiology classes Local
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Steps to Success in Sepsis ASHNHA Quality Webinar. Maryanne Whitney, RN, CNS, MSN Improvement Advisor, Cynosure Health
 1 Steps to Success in Sepsis ASHNHA Quality Webinar Maryanne Whitney, RN, CNS, MSN Improvement Advisor, Cynosure Health Goals for Today State the Problem: Create Awareness & Will Unravel the mysteries
1 Steps to Success in Sepsis ASHNHA Quality Webinar Maryanne Whitney, RN, CNS, MSN Improvement Advisor, Cynosure Health Goals for Today State the Problem: Create Awareness & Will Unravel the mysteries
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
SEPSIS & SEPTIC SHOCK
 SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
ICD-10-CM: The Sage Continues
 ICD-10-CM: The Sage Continues UHIMA Kathy DeVault, MSL, RHIA, CCS, CCS-P, FAHIMA UASI Kathy.devault@uasisolutions.com Objectives Review quality documentation Discuss use of unspecified codes Discuss opportunities
ICD-10-CM: The Sage Continues UHIMA Kathy DeVault, MSL, RHIA, CCS, CCS-P, FAHIMA UASI Kathy.devault@uasisolutions.com Objectives Review quality documentation Discuss use of unspecified codes Discuss opportunities
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
1. Improve Documentation Now
 Joseph C. Nichols, MD, Principal, Health Data Consulting, Seattle, Washington From Medscape Education Family Medicine: Transition to ICD-10: Getting Started. Posted: 06/19/2012 Target Audience: This activity
Joseph C. Nichols, MD, Principal, Health Data Consulting, Seattle, Washington From Medscape Education Family Medicine: Transition to ICD-10: Getting Started. Posted: 06/19/2012 Target Audience: This activity
GUIDELINES: PEER REVIEW TRAINING BOD G [Amended BOD ; BOD ; BOD ; Initial BOD ] [Guideline]
![GUIDELINES: PEER REVIEW TRAINING BOD G [Amended BOD ; BOD ; BOD ; Initial BOD ] [Guideline]](/thumbs/74/70362472.jpg "GUIDELINES: PEER REVIEW TRAINING BOD G [Amended BOD ; BOD ; BOD ; Initial BOD ] [Guideline]") GUIDELINES: PEER REVIEW TRAINING BOD G03-05-15-40 [Amended BOD 03-04-17-41; BOD 03-01-14-50; BOD 03-99-15-48; Initial BOD 06-97-03-06] [Guideline] I. Purpose Guidelines: Peer Review Training provide direction
GUIDELINES: PEER REVIEW TRAINING BOD G03-05-15-40 [Amended BOD 03-04-17-41; BOD 03-01-14-50; BOD 03-99-15-48; Initial BOD 06-97-03-06] [Guideline] I. Purpose Guidelines: Peer Review Training provide direction
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Cheryl Ericson, MS, RN, CCDS, CDIP, AHIMA Approved ICD 10 CM/PCS Trainer Clinical Documentation Program Manager for ezdi.
 A Venture of Cheryl Ericson, MS, RN, CCDS, CDIP, AHIMA Approved ICD 10 CM/PCS Trainer Clinical Documentation Program Manager for ezdi HIPAA Code Sets HIPAA legislation required use of the International
A Venture of Cheryl Ericson, MS, RN, CCDS, CDIP, AHIMA Approved ICD 10 CM/PCS Trainer Clinical Documentation Program Manager for ezdi HIPAA Code Sets HIPAA legislation required use of the International
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
WATCHMAN. For questions regarding WATCHMAN reimbursement, please contact:
 WATCHMAN IMPORTANCE OF DOCUMENTATION & THE IMPACT ON MS- DRG ASSIGNMENT This guide stresses the importance of documentation in capturing the appropriate acuity level for patients considered WATCHMAN candidates.
WATCHMAN IMPORTANCE OF DOCUMENTATION & THE IMPACT ON MS- DRG ASSIGNMENT This guide stresses the importance of documentation in capturing the appropriate acuity level for patients considered WATCHMAN candidates.
Inflammatory Statements
 Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Update in Sepsis. Conflicts of Interest: None. Bill Janssen, M.D.
 Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Sample page. For the Physical Therapist An essential coding, billing and reimbursement resource for the physical therapist CODING & PAYMENT GUIDE
 CODING & PAYMENT GUIDE 2019 For the Physical Therapist An essential coding, billing and reimbursement resource for the physical therapist Power up your coding optum360coding.com Contents Getting Started
CODING & PAYMENT GUIDE 2019 For the Physical Therapist An essential coding, billing and reimbursement resource for the physical therapist Power up your coding optum360coding.com Contents Getting Started
SEPSIS. Sepsis Dianna Foley, RHIA, CHPS. Sepsis Stats 3/3/2015
 Sepsis Dianna Foley, RHIA, CHPS SEPSIS Sepsis Stats Sepsis 10 th leading cause of death in the U.S. Affecting 3 in every 1,000 people Accounting for 1-2 % of hospitalizations Severe Sepsis Approximately
Sepsis Dianna Foley, RHIA, CHPS SEPSIS Sepsis Stats Sepsis 10 th leading cause of death in the U.S. Affecting 3 in every 1,000 people Accounting for 1-2 % of hospitalizations Severe Sepsis Approximately
Where Are We Now With Sepsis?
 WHITE PAPER Summary: The following white paper provides an overview of the history of sepsis definitions, the changes set in motion in 2016 with the publication of Sepsis-3, and the evidence surfacing
WHITE PAPER Summary: The following white paper provides an overview of the history of sepsis definitions, the changes set in motion in 2016 with the publication of Sepsis-3, and the evidence surfacing
12/12/2017. Notice. Sepsis is defined as life-threatening organ dysfunction due to a dysregulated host response to infection.
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Hospital Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.4 Measure Updates Presentation Transcript Speakers Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.4 Measure Updates Presentation Transcript Speakers Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
Introduction. Centers for Disease Control and Prevention (CDC),
,") When Prevention Fails: The Clinical and Economic Impact of Sepsis Introduction Healthcare-associated infections are one of the top 0 leading causes of death in the U.S. The US Centers for Disease Control
When Prevention Fails: The Clinical and Economic Impact of Sepsis Introduction Healthcare-associated infections are one of the top 0 leading causes of death in the U.S. The US Centers for Disease Control
ICD-10-CM 101 9/19/2016
 Presented by Cathy Jennings, BS, CPC, CPC-I, CEDC, CHONC AHIMA Approved ICD-10-CM/PCS Trainer Managing Consultant October 5, 2016 Disclaimer The speaker has no financial relationship to any products or
Presented by Cathy Jennings, BS, CPC, CPC-I, CEDC, CHONC AHIMA Approved ICD-10-CM/PCS Trainer Managing Consultant October 5, 2016 Disclaimer The speaker has no financial relationship to any products or
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Sepsis in primary care. what is good care?
 Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Andrea Blotsky MDCM FRCPC General Internal Medicine, McGill University Thursday, October 15, 2015
 The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
Compliance. TODAY January Improving the Medicare audit process. an interview with Gerard (Jerry) Mulcahy. See page 16
 Mulcahy. See page 16") Compliance TODAY January 2017 a publication of the health care compliance association www.hcca-info.org Improving the Medicare audit process an interview with Gerard (Jerry) Mulcahy Former Director, Medicare
Compliance TODAY January 2017 a publication of the health care compliance association www.hcca-info.org Improving the Medicare audit process an interview with Gerard (Jerry) Mulcahy Former Director, Medicare
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Inpatient Quality Reporting (IQR) Program
 Program") Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance