Jason Zurba BSc RRT Supervisor Royal Columbian Hospital
|
|
|
- Leonard Davis
- 5 years ago
- Views:
Transcription


1 Jason Zurba BSc RRT Supervisor Royal Columbian Hospital
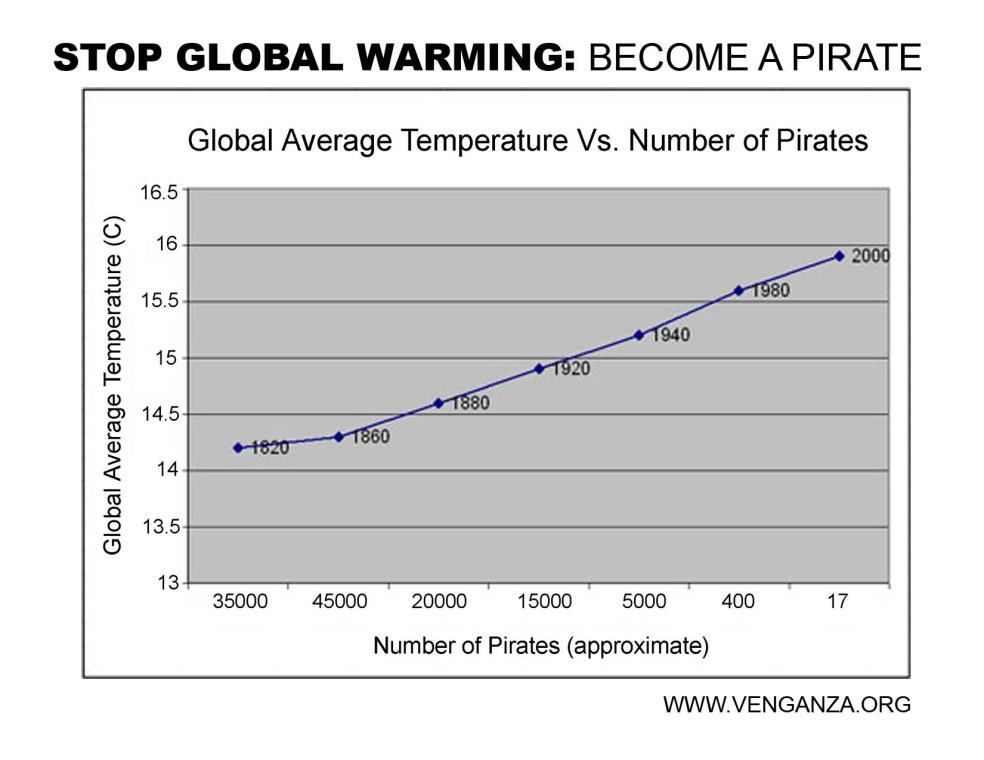
2 Outline Why we started looking at this What our own data has shown us What the literature tells us about intubation What we have changed How this applies to Neonates



3

4 Nursing Royal Columbian Hospital Airway Committee Respiratory Therapists Physicians: ICU Emergency Anesthesia Administration

5 Mandate Leave your ego at the door Airway Incidents Equipment Protocols Education
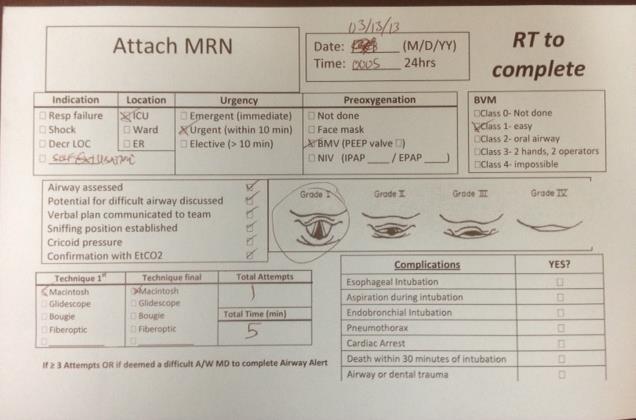
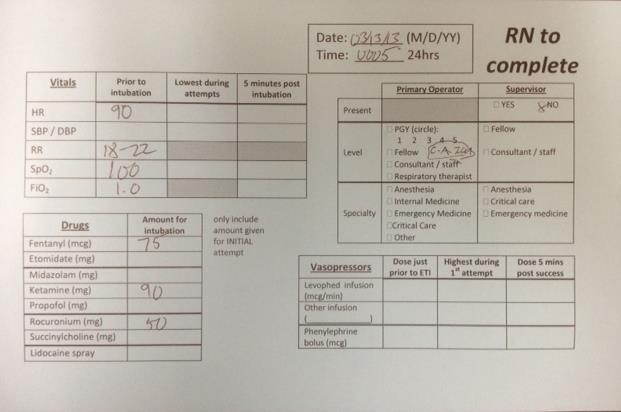
6 Intubation Data Collection at Royal Columbian Hospital
7
8
9 July 2012 to November DOCUMENTED INTUBATIONS

10 INDICATIONS RESP FAIL DEC LOC SHOCK OTHER NO DATA
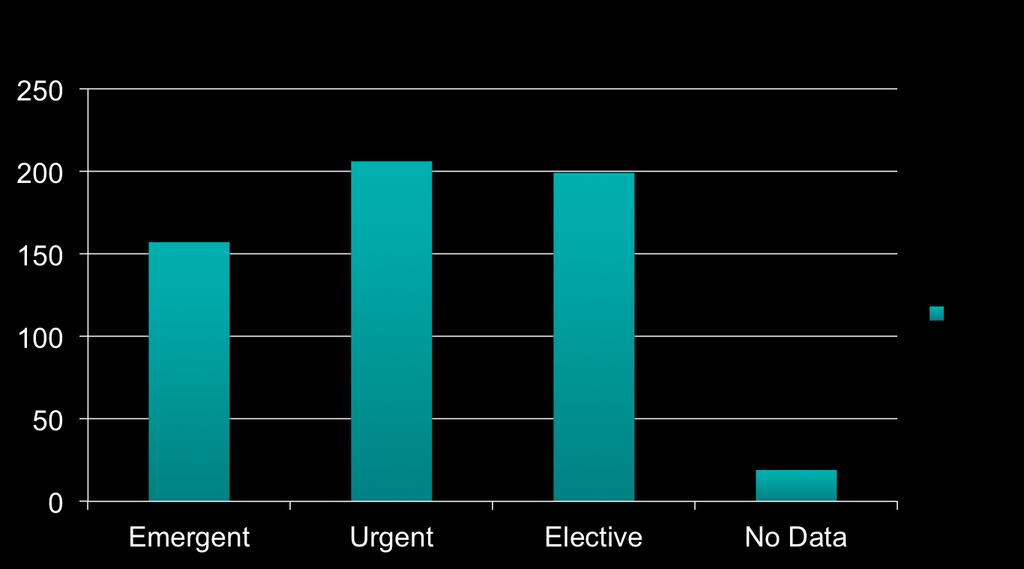
11 Urgency

12 BVM Class
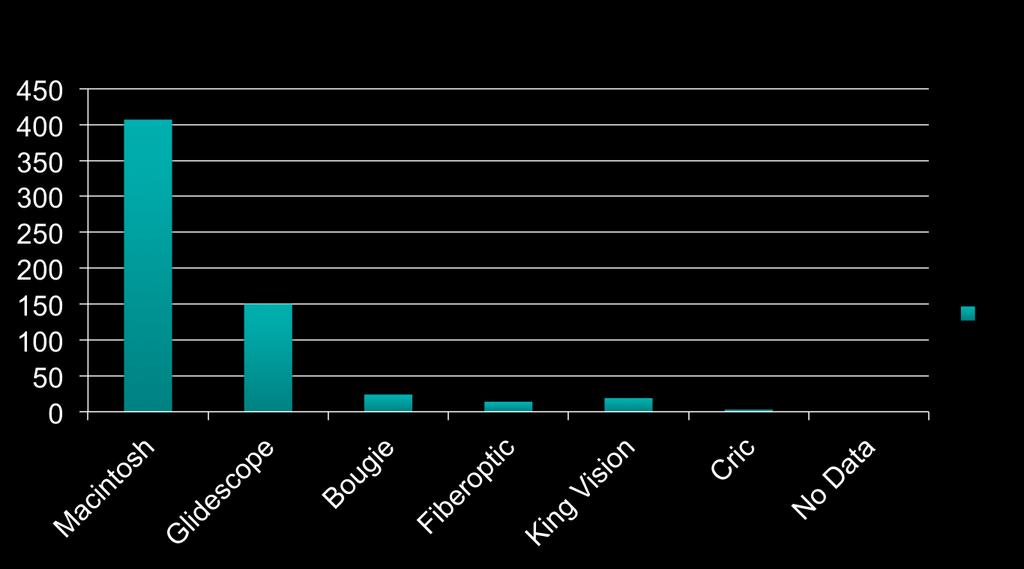
13 Techniques

14 Complications Severe: SBP <70mmHg if >90 mmhg O2 Sat n <80% if >90% Esophageal intubation Other: aspiration, dental trauma, endobronchial intubation, pneumothorax Cardiac Arrest or Death
15 Key findings 1 Attempt (n =224 ) >1 Attempt (n=108) Other Complications % Severe Complications % vs 41% 8.0% vs 30% 1. Others Complications: Aspiration, dental trauma, endobronchial intubation, pneumothorax or any severe complication 2. Severe Complication: - Hypotension: Systolic blood pressure <70mmHg if >90mmHg prior to attempt - Hypoxia: oxygen saturation <80% if >90% prior to attempt -Esophageal intubation -Cardiac Arrest -Death within 30 Min of Intubation
16 Greater than one attempt at ETI was associated with a 4-fold increase in severe, and a 5-fold increase in total complications. Although previous publications found greater than 2 attempts associated with increased complications, recent publications found this association with greater than one attempt, consistent with our findings.
17 Should RTs be intubating? A. Yes, of course B. No, are you nuts?

18 Is It just Us? Do we Just Suck at Intubation at RCH? Fiberoptic intubation gone horribly wrong
19 Do we suck at RCH? A. Yup, you suck B. Nope, that sounds normal C. Nope, you guys are some kind of A/W wizards
20 Complications Rates Authors Jaber 2006 (ICU)N=253 Griesdale (unpublished) (ICU) Jaber 2010 (ICU) N=121 Sackles 2013 N=1828 RCH Data, N=332 Total complications Severe Complications 50% 28% 38% 24% 34% 21% 25% 19% 15%

21 How do we measure up to others

22 Complications Increase with >1 Attempt Authors Griesdale 2008 n=136 Sackles 2013 n=1828 RCH Data n=332 Absolute Risk of Adverse Event 18% 38% 14% 53% 8% 41%

23 Prospective cohort study of pts intubated by ICU team N=136 Excluded Cardiac arrest pts >1 attempt associated with risk of severe complications OR 3.31 (95% CI:1.30,8.40, p=0.01)
")
24 Retrospective analysis of 4 years of QI data N= attempt complications 14.2% (95% CI12.4%-16.2% >1 attempt complications 47.2%(95% CI 41.8%-52.7%)
25
26 What are some things we can fix?

27 First pass success PGY-1 38% PGY-2 52% PGY-3 66% Anesthesia Resident 85% Higher year of training RR.74 95%[CI] P<.01 Anesthesia Resident RR.52 95%[CI].2-1 P=.03

28 Lessons People with more experience have better success

29 N=322 Anesthesia Residents out of OR intubations Complications decreased with attending Supervision 21.7% vs 6.1% P=.0001

30 Lesson Anesthetists are the experts
31 So.. How many intubations does it take to become good?
32 How many Intubations should you do to show competency A. 5 B. 10 C. 20 D. 30 E. >30

33 57 successful intubations to have 90% success rate Still improving into the 80s
34 472 intubations by 20 trainees (msi, RT, EMT) All pts prescreened to be easy intubations Analysis of data predicted 90% success after 47 intubations existing Direct laryngoscope intubation training..is inadequate for non-anaesthesia healthcare workers Emphasis should be placed on effective ventilation and oxygenation using BVM

35 Small number of ER residents (3) 342 intubations over 2 years 74.7 intubations to achieve 90% successful intubation (95% CI )

36 Lesson RT intubation competency programs are probably not adequate.

37 33 airway cases identified Identified contributing issues Lack of airway assessment Failure to alter technique when difficult a/w Lack of airway strategy Failure to alter failing technique

38 Lessons Assess Plan and communicate an airway strategy If it looks tough, do something different If something isn t working, don t do it again
39 With anticipated DTI 70% anesthetists didn t change technique > 60% progressed to CICV SGA regularly rescued failed intubation Transtracheal jet high complications rate of death when used as rescue

40 Lesson Change technique for difficult A/W Don t use transtracheal jet SGAs are pretty cool
41 How many of you regularly see DL fail during intubation and the second attempt is DL again?
42 When first attempt DL unsuccessful, repeated DL 80% failure rate. Recommend identification and detailing difficult A/W details

43 Lesson If it isnt working, don t keep doing it no matter how tempting Clearly identify Difficult A/W
44 Previous difficult intubation (DTI) 6 times more likely to be DTI again Previous failed intubation 22 times more likely to fail again. As a result of findings Denmark created database

45 Lesson Clearly identify people with difficult A/W Listen if someone says it was difficult

46 But I Gotta Intubate! It s an Emerrrrrrgency!
47 They Can Usually Wait Less than 1/3 of our pts were Emergent Intubations of Critically ill are usually urgent, not emergent (Griesdale 2011)
48 N=649,359 Favourable Neurological outcome; Intubation SGA BVM

 BVM 2.")
49 N=649,359 Favourable Neurological outcome; Intubation 1.0% (95% CI 0.9%-1.1%) SGA 1.1% (95% CI 1.1%-1.2%) BVM 2.9%(95% CI 2.9%-3.0%)

50 Lesson It may be better to use BVM than intubate (at least in cardiac arrest)
51 But what if I can t manually ventilate them?

52 4 year observational study N=53, cases of impossible mask ventilation Only 19 of these were difficult a/w

53 Lesson Impossible mask ventilation is extremely rare. Even if you do meet them, they will probably be easy to intubate
54 N=128 Apneic oxygenation Decreased desaturation during intubation absolute risk reduction 16.7% P=0.016
55 Lesson Apneic oxygenation may further decrease your risk of desaturation during intubation
56 What if you put it all together?
 life threatening complications 34%-21% other complications")
57 Two phase Multi-center Use of Intubation Bundle Preoxygenation, 2 operators, RSI, Cricoid, EtCO2, Protective ventilation, Fluid loading N=244 (123 before, 121 after) life threatening complications 34%-21% other complications 21%-9%

58 Griesdale et al 2011 (unpublished) Use of a checklist Serious Complication

59 Lesson Use a checklist, they work!

60 307 Hospitals 4 Countries 1 year Prospective ICU, ED, OR Airway Cases: Death Brain Damage Unexpected ICU
61 NAP 4 4 Common themes identified 1) Lack of airway assessment 2) Lack of airway strategy 3) Avoidance of awake techniques 4) The failure to plan for Failure: repeated attempts using the same people/equipment
62 NAP 4 98/133 no documented airway exam 66 may be difficult -1 change in airway strategy needle Cricothyrotomy: Rate 64% (16/25) Failure Failure to use capnography implicated in 82% of ICU airway deaths and brain damage
63 NAP4 Recommendations Develop a checklist for intubation Standardize Difficult A/W equipment Including SGA and Aintree catheters Do more awake FOB intubations Investigate A/W critical incidents Appoint an A/W lead anesthetist in all institutions. Capnography is mandatory
64 NAP4 Reccomendations Identify Difficult A/W patients Establish good communication between ICU, ER, and Anesthesia Establish clear lines of communication to escalate A/W events to individuals with appropriate skills.

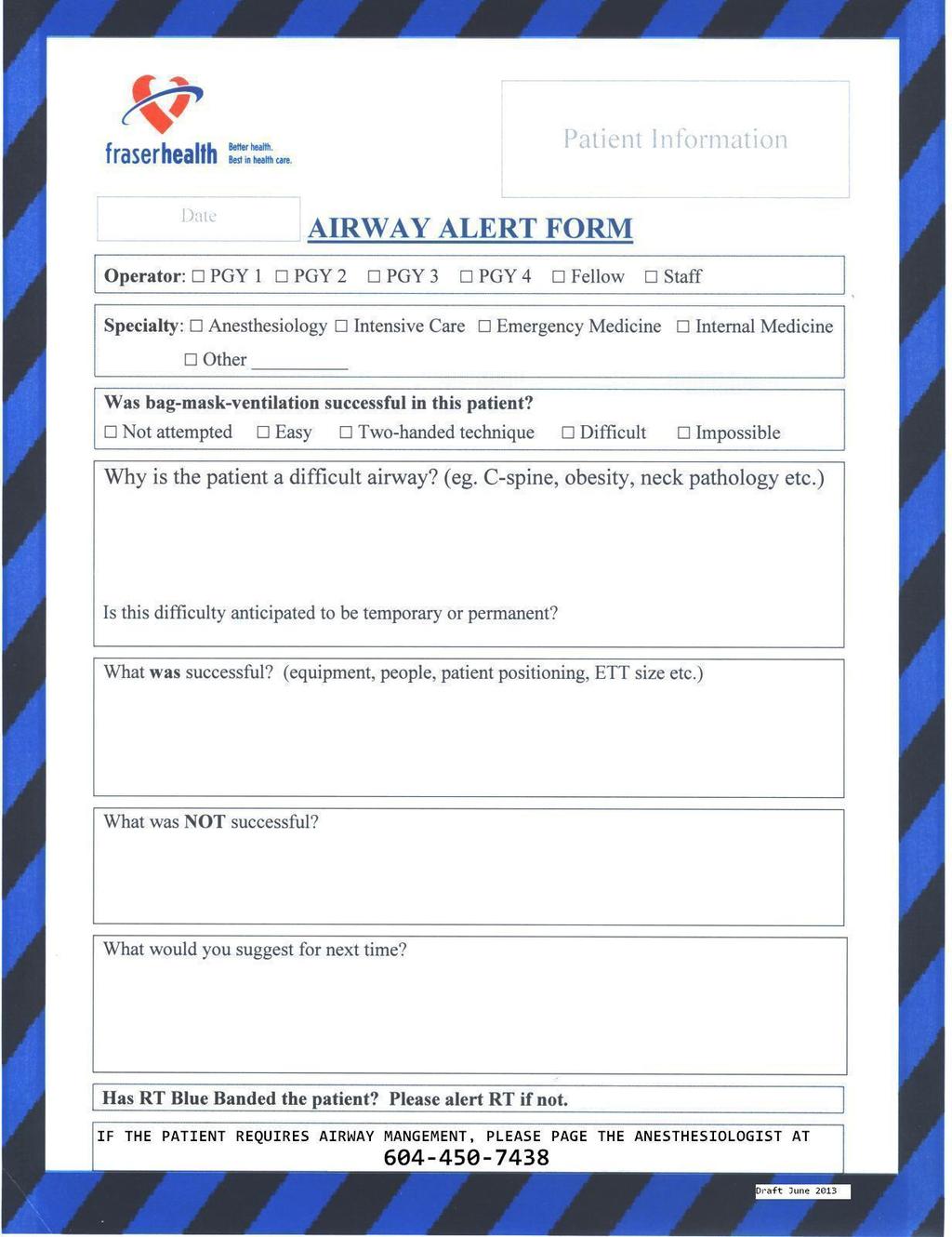
65 What have we done so far Difficult Airway Recognition Blue wrist band Blue sign for HOB Airway Alert form
66
67 24 hour a day response from a rover Anesthesiologist for difficult airways Empowered any member of team to escalate airway emergencies
68 ETCO2 monitoring at every intubation Standardize difficult intubation equipment Standardize intubation procedure Preprinted orders
69 Pre-printed Orders: Intubation Royal Columbian Hospital (trial) DRAFT Form ID: Rev: April 10 th 2014 Page: 1 of 1 DRUG & FOOD ALLERGIES Mandatory o Optional: Prescriber check (P) to initiate, cross out and initial any orders not indicated. 1. PREPARATION- PRE-INTUBATION Airway Competent MD, RT and RN present Airway equipment present and consideration for adjuncts discussed Planned strategy for intubation verbally communicated to all team members (see back) Airway assessment and positioning completed: Assess for contraindications prior to positioning (e.g. any cervical spine instability?) Sniffing position required? (e.g. Troop pillow, flannels/pillows) Potential for difficult airway discussed with team Breathing and Pre-oxygenation Apneic oxygenation (15lpm nasal prongs) Assisted Bag Valve Mask Non-Invasive Ventilation (NIV) as ordered by MD Circulation: RN to ensure patent IV and all medications are prepared prior to start. IV 500 ml SODIUM CHLORIDE 0.9% bolus over 15 mins Monitor BP Q 3 min during and for 20 min post intubation medications and until stable o o NOREPINEPHRINE Infusion at 5 mcg/min if MAP less than 60 mmhg PHENYLEPHRINE 50 to 100 mcg IV PRN 2. INTUBATION (consider standardized medications): o Rapid Sequence Induction (RSI) Induction / Analgesia Agents: ETOMIDATE 0.3 mg/kg IV (Prepare 20mg in syringe) KETAMINE 1.5 to 2.0 mg/kg IV (Prepare 200 mg in syringe) Fentanyl 1 to 2 mcg/kg (Prepare 250mcg in syringe) Other: Neuromuscular Blockade: o SUCCINYLOCHOLINE 1.5 mg/kg IV Prepare: Patient weight: o ROCURONIUM 1 mg/kg IV Prepare: mg IV o Awake Intubation mg IV GLYCOPYRROLATE 0.4 mg IV Topicalization with Lidocaine 5ml/kg o KETAMINE 0.25 to 0.5 mg/kg IV PRN Prepare: mg IV PRN MIDAZOLAM 0.05 mg/kg IV PRN Prepare: mg IV PRN 3. POST- INTUBATION Confirm placement with waveform CO2 and auscultation CXR Was this a difficult Airway? If yes, RT to ensure Difficult Airway Bundle implemented Date (dd/mm/yyyy) Time Prescriber Signature Printed Name or College ID#
70
71
72 So. Should RTs be intubating? If our competency programs are inadequate We often don t do enough intubations to maintain competency Dealing with failed A/W is beyond our scope We are unable to do awake fiberoptic intubations Open cricothyrotomy is beyond our scope Greater than one attempt significantly increases severe complications
73 So..Should RTs intubate? A. Yes B. No
74 How have the initiatives worked so far?
75 Difficult airway identification system Has been huge success. Every difficult airway (?) is being labelled and documented FHA is adopting system
76 Extubation of Difficult A/W Empowered RTs to refuse orders to extubate difficult airways Identified difficult A/W require anesthetist to be present for extubation

77 So, how has the order set worked? In 11 months we have had 17 uses of the order set Approx 10% usage
78 What about babies? Maybe RTs should intubate babies?
79 Neonatal ETI Data collection cards now kept in NICU Overall complication rates 54% Complication rates with 1 st pass success 29% Complication rates increase to 83% thereafter

80 Complications with Intubation
81 Maybe we suck at intubating babies?
82 5 level 3 NICUs One year study ETI attempts 203 patients
 60% decompensation+esophageal Providers with more experience more")
83 Neonatal ETI Low frequency, High-stakes events Success rates poor (at best 72%) 60% decompensation+esophageal Providers with more experience more successful

84
85 Going to get worse No routine intubations for meconium No longer ethical to practice after death Working hours for DRs reduced Reduction in invasive ventilation
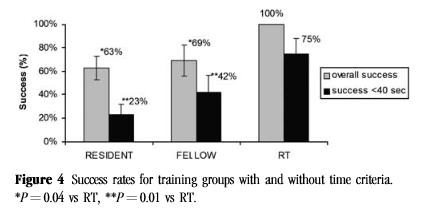
86 50 ETI assessed Residents (25), NICU Fellows (13), RTs (12)
87
88
89 Why difference Adult to Neo Difficult airway uncommon Limited techniques and adjuncts Uncommon procedure even for Attending Physicians
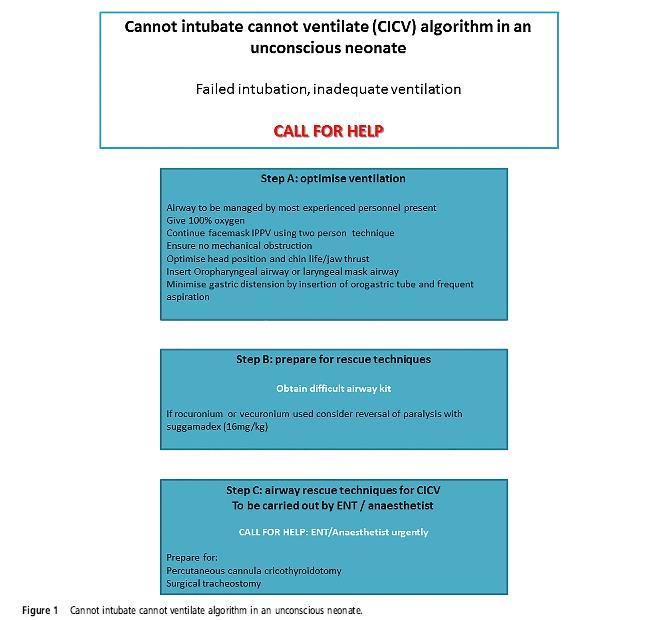
90 What do you do if you cant intubate a neonate???
91 Telephone survey of all 59 level 3 NICU in UK 7% had CICV algorithm
92
93 Cautious Maybe Smaller, dedicated staff Take on the dedicated role Reasonable competency program
INTUBATION/RSI. PURPOSE: A. To facilitate secure, definitive control of the airway by endotracheal intubation in an expeditious and safe manner
 Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Tracheal Intubation in ICU: Life saving or life threatening?
 Tracheal Intubation in ICU: Life saving or life threatening? Prof. Sheila Nainan Myatra Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai, India sheila150@hotmail.com Three
Tracheal Intubation in ICU: Life saving or life threatening? Prof. Sheila Nainan Myatra Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai, India sheila150@hotmail.com Three
Question: Is this patient an infant? A patient less than 12 months old is considered an infant. Please check the box next to the appropriate choice.
 Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Kelowna June 2011 Airway Assessment and Management. Golden, BC
 Kelowna June 2011 Airway Assessment and Management Dr. Bruce Starke Golden, BC Not really... I am unable to identify any potential conflict of interest and I am unable to identify any potential conflict
Kelowna June 2011 Airway Assessment and Management Dr. Bruce Starke Golden, BC Not really... I am unable to identify any potential conflict of interest and I am unable to identify any potential conflict
ADVANCED AIRWAY MANAGEMENT
 The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
Emergency Department/Trauma Adult Airway Management Protocol
 Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Exclusion Criteria 1. Operator or supervisor feels specific intra- procedural laryngoscopy device will be required.
 FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Care Unit (FELLOW)
") Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Joint Theater Trauma System Clinical Practice Guideline
 Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients CASE REPORT FORM
 INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
AVOIDING THE CRASH 3: RELAX, OPTIMAL POST-AIRWAY MANAGEMENT AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
Airway Management and The Difficult Airway
 Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill
 Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill Matthew W. Semler, MD; David R. Janz, MD, MSc; Robert J. Lentz, MD; Daniel T. Matthews, MD; Brett C. Norman,
Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill Matthew W. Semler, MD; David R. Janz, MD, MSc; Robert J. Lentz, MD; Daniel T. Matthews, MD; Brett C. Norman,
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
RAPID SEQUENCE INTUBATION FOR THE RURAL DOC
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Pearls and Pitfalls of Rapid Sequence Intubation
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/pearls-and-pitfalls-of-rapid-sequenceintubation/3829/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/pearls-and-pitfalls-of-rapid-sequenceintubation/3829/
This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway.
 PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
by Weingart S, Nickson C, Rabinovich J, Strayer R. version
 EMCrit Call/Response Intubation Ch Plan HOp Killers-Hemodynamics, Ox, ph RSI Awake DSI RSA ICP/Vascular Induction Agent/Muscle Relaxant Push-Dose Presss Failed Airway Plan Verbalized Cric-Con Evaluation
EMCrit Call/Response Intubation Ch Plan HOp Killers-Hemodynamics, Ox, ph RSI Awake DSI RSA ICP/Vascular Induction Agent/Muscle Relaxant Push-Dose Presss Failed Airway Plan Verbalized Cric-Con Evaluation
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Interfacility Protocol Protocol Title:
 Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Can't Intubate, Can't oxygenate (CICO) The new terminology What is the Military Experience What is the Civilian Experience What is your role.
 The new terminology What is the Military Experience What is the Civilian Experience What is your role.") Disclaimer The views in the presentation are the author's, and do not reflect the views of the Department of Defence I am a full time Australian Defence Force Procedural Specialist (Anaesthetist) Can't
Disclaimer The views in the presentation are the author's, and do not reflect the views of the Department of Defence I am a full time Australian Defence Force Procedural Specialist (Anaesthetist) Can't
A Successful RSI Program
 RSI A Successful RSI Program Requires understanding of: Indications Contraindications Limitations Requires knowledge of: Physiology Pharmacology Airway techniques Goals of RSI Success rates comparable
RSI A Successful RSI Program Requires understanding of: Indications Contraindications Limitations Requires knowledge of: Physiology Pharmacology Airway techniques Goals of RSI Success rates comparable
In accordance with protocols, this patient should be transported to which medical facility?
 NOTE: Please select the most appropriate answer based on the Westchester Regional On-Line Medical Control Physician (OLMC) Regional System Overview, as well as current regional and state EMS protocols
NOTE: Please select the most appropriate answer based on the Westchester Regional On-Line Medical Control Physician (OLMC) Regional System Overview, as well as current regional and state EMS protocols
CASE REPORT FORM (v )
") INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM (v 1.2 30.09.18) SITE INFORMATION
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM (v 1.2 30.09.18) SITE INFORMATION
GENERAL ANAESTHESIA AND FAILED INTUBATION
 GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Emergency Airway Management. Richard P. Dutton, M.D., M.B.A. Chief Quality Officer US Anesthesia Partners
 Emergency Airway Management Richard P. Dutton, M.D., M.B.A. Chief Quality Officer US Anesthesia Partners Disclosures I have studied a lot of airway gizmos over the years. I have no financial interest in
Emergency Airway Management Richard P. Dutton, M.D., M.B.A. Chief Quality Officer US Anesthesia Partners Disclosures I have studied a lot of airway gizmos over the years. I have no financial interest in
Airway Management in the Multiply Traumatized Patient
 Airway Management in the Multiply Traumatized Patient Toronto Anesthesia Symposium April 18, 2015 Dr. Jeffrey Wassermann Department of Anesthesia St. Michael s Hospital University of Toronto Airway Management
Airway Management in the Multiply Traumatized Patient Toronto Anesthesia Symposium April 18, 2015 Dr. Jeffrey Wassermann Department of Anesthesia St. Michael s Hospital University of Toronto Airway Management
MAKING RSI SAFER. Nick Taylor ETU THK 2015
 MAKING RSI SAFER Nick Taylor ETU THK 2015 GOALS 1. AIRWAY ASSESSMENT AND PLAN 2. MAXIMALLY PREOXYGENATE 3. HAEMODYNAMIC STABILITY PART 1 : AIRWAY ASSESSMENT AND PLAN LEMON: AIRWAY ASSESS AND PLAN Look
MAKING RSI SAFER Nick Taylor ETU THK 2015 GOALS 1. AIRWAY ASSESSMENT AND PLAN 2. MAXIMALLY PREOXYGENATE 3. HAEMODYNAMIC STABILITY PART 1 : AIRWAY ASSESSMENT AND PLAN LEMON: AIRWAY ASSESS AND PLAN Look
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
The Pediatric Airway. Andrew Wackett, MD
 The Pediatric Airway Andrew Wackett, MD Objectives 1) Demonstrate understanding of the indications for intubation 2) Perform rapid sequence intubation 3) Learn the pharmacology behind emergency airway
The Pediatric Airway Andrew Wackett, MD Objectives 1) Demonstrate understanding of the indications for intubation 2) Perform rapid sequence intubation 3) Learn the pharmacology behind emergency airway
CONFLICT OF INTEREST NONE
 Airway Dr Albert Buchel MD CCFP EM CAC EM. Assistant Professor, Department of emergency medicine Program Director CCFP EM residency University of Manitoba CONFLICT OF INTEREST NONE AIRWAY TIPS PASSING
Airway Dr Albert Buchel MD CCFP EM CAC EM. Assistant Professor, Department of emergency medicine Program Director CCFP EM residency University of Manitoba CONFLICT OF INTEREST NONE AIRWAY TIPS PASSING
Post Resuscitation (ROSC) Care
 Care") Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
ENDOTRACHEAL INTUBATION POLICY
 POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Airway Management. Key points. Rapid Sequence Intubation. Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway
 Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
VANDERBILT UNIVERSITY MEDICAL CENTER DIVISION OF ANESTHESIOLOGY CRITICAL CARE MEDICINE AIRWAY MANAGEMENT
 These guidelines are based upon medical literature review and expert opinion and are intended to provide recommendations for in the care of critically ill patients. Best Practice Guidelines Checklist for
These guidelines are based upon medical literature review and expert opinion and are intended to provide recommendations for in the care of critically ill patients. Best Practice Guidelines Checklist for
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
VUMC Multidisciplinary Surgical Critical Care Service
 VUMC Multidisciplinary Surgical Critical Care Service SICU Standard Operating Procedure: Guidelines for Intubation I. Definition Intubation is required for SICU patients who cannot maintain a patent airway,
VUMC Multidisciplinary Surgical Critical Care Service SICU Standard Operating Procedure: Guidelines for Intubation I. Definition Intubation is required for SICU patients who cannot maintain a patent airway,
General Medical Procedure. Emergency Airway Techniques (General Airway Protocol)
") General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
Joint Trauma System. Airway Trauma Injury Management
 Joint Trauma System Airway Trauma Injury Management 1 Agenda Contributors Purpose Summary Key Principles of CPG Performance Improvement (PI) Monitoring References List of Appendices in CPG 2 Contributors
Joint Trauma System Airway Trauma Injury Management 1 Agenda Contributors Purpose Summary Key Principles of CPG Performance Improvement (PI) Monitoring References List of Appendices in CPG 2 Contributors
Waitin In The Wings. Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider
 Indications and Use for the Pre-Hospital Provider") Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation
 Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
DIFFICULT AIRWAY MANAGMENT. Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr)
") DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
Rapid Sequence Induction
 Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Winston Cheung, Elizabeth Fugaccia, David Milliss and Govindasamy Thanakrishnan ORIGINAL ARTICLES ABSTRACT
 Operator anaesthesiology training and after endotracheal intubation in the intensive care unit: a 3-year, prospective, observational study Winston Cheung, Elizabeth Fugaccia, David Milliss and Govindasamy
Operator anaesthesiology training and after endotracheal intubation in the intensive care unit: a 3-year, prospective, observational study Winston Cheung, Elizabeth Fugaccia, David Milliss and Govindasamy
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Resuscitation Patient Management Tool May 2015 MET Event
 OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY. Procedural Sedation Questions
 Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
Management of the Airway
 Management of the Airway Kristen Bridges, M.D. Kings County Hospital Center November 12 th 2015 Case Presentation 64F PMHx CHF EF 5-10%, NYHF III-IV, atrial fibrillation/la thrombus, CVA x2, DM, HTN Home
Management of the Airway Kristen Bridges, M.D. Kings County Hospital Center November 12 th 2015 Case Presentation 64F PMHx CHF EF 5-10%, NYHF III-IV, atrial fibrillation/la thrombus, CVA x2, DM, HTN Home
Emergency Department Guideline. Procedural Sedation and Analgesia Policy for the Registered Nurse
 Emergency Department Guideline Purpose: To ensure safe, consistent patient monitoring and documentation standards when procedure related sedation and analgesia is indicated. Definitions: Minimal Sedation
Emergency Department Guideline Purpose: To ensure safe, consistent patient monitoring and documentation standards when procedure related sedation and analgesia is indicated. Definitions: Minimal Sedation
Analgesic-Sedatives Drug Dose Onset
 Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
I. Subject. Moderate Sedation
 I. Subject II. III. Moderate Sedation Purpose To establish criteria for the monitoring and management of patients receiving moderate throughout the hospital Definitions A. Definitions of three levels of
I. Subject II. III. Moderate Sedation Purpose To establish criteria for the monitoring and management of patients receiving moderate throughout the hospital Definitions A. Definitions of three levels of
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Safe Use of Opioids in Hospitals: Addressing The Joint Commission Sentinel Event Alert
 Safe Use of Opioids in Hospitals: Addressing The Joint Commission Sentinel Event Alert Physician-Patient Alliance for Health & Safety (PPAHS) www.ppahs.org Panelists Michael Wong, JD - Physician-Patient
Safe Use of Opioids in Hospitals: Addressing The Joint Commission Sentinel Event Alert Physician-Patient Alliance for Health & Safety (PPAHS) www.ppahs.org Panelists Michael Wong, JD - Physician-Patient
Interesting Capnography Cases
 Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
FAILED INTUBATION DURING RSI: PLAN A, C & D
 FAILED INTUBATION DURING RSI: PLAN A, C & D MODULE: NOVICE & AIRWAY TARGET: NOVICE INITIAL ASSESSMENT OF COMPETENCY ALL ANAESTHETISTS BACKGROUND: Management of the Can t Intubate, Can t Ventilate situation
FAILED INTUBATION DURING RSI: PLAN A, C & D MODULE: NOVICE & AIRWAY TARGET: NOVICE INITIAL ASSESSMENT OF COMPETENCY ALL ANAESTHETISTS BACKGROUND: Management of the Can t Intubate, Can t Ventilate situation
TRACHEOSTOMY EMERGENCIES
 TRACHEOSTOMY EMERGENCIES MODULE: AIRWAY TARGET: ALL ANAESTHETISTS, INTENSIVISTS, ED & ACUTE PHYSICIANS, FOUNDATION DOCTORS BACKGROUND: Around 16% of ICU patients may have a tracheostomy. Life- threatening
TRACHEOSTOMY EMERGENCIES MODULE: AIRWAY TARGET: ALL ANAESTHETISTS, INTENSIVISTS, ED & ACUTE PHYSICIANS, FOUNDATION DOCTORS BACKGROUND: Around 16% of ICU patients may have a tracheostomy. Life- threatening
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C
 Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Emergency Cricothyrotomy
 Emergency Cricothyrotomy SWORBHP Live Paramedic Rounds June 15, 2012 Sameer Mal PGY4 Emergency Medicine Dwayne Cottel Regional Paramedic Educator Overview BVM Ventilation Intro to Cricothyrotomy Relevant
Emergency Cricothyrotomy SWORBHP Live Paramedic Rounds June 15, 2012 Sameer Mal PGY4 Emergency Medicine Dwayne Cottel Regional Paramedic Educator Overview BVM Ventilation Intro to Cricothyrotomy Relevant
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Resuscitation Checklist
 Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 Available ONLY at: BMC-B BMC-D BMC-N BMC-S Intubation Phase Notify Therapy for STAT intubation SUB Rapid Sequence Induction(SUB)* ***The above subphase is available at the end of the powerplan under the
Available ONLY at: BMC-B BMC-D BMC-N BMC-S Intubation Phase Notify Therapy for STAT intubation SUB Rapid Sequence Induction(SUB)* ***The above subphase is available at the end of the powerplan under the
POLICY. Number: Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE. Authorization
 POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
Airway management problem during anaesthesia. Airway management problem in ICU / HDU. Airway management problem occurring in the Emergency Department
 4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
Acute Respiratory Failure
 Acute Respiratory Failure Family Medicine Update Big Sky, Montana January, 2014 Mark Tieszen, MD, FCCM, FCCP Sanford Medical Center Fargo Critical Care Medicine mark.tieszen@sanfordhealth.org Acute Respiratory
Acute Respiratory Failure Family Medicine Update Big Sky, Montana January, 2014 Mark Tieszen, MD, FCCM, FCCP Sanford Medical Center Fargo Critical Care Medicine mark.tieszen@sanfordhealth.org Acute Respiratory
CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR
 CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR 801-467-0800 Phone 800-800-HFJV (4358) Hotline TABLE OF CONTENTS Respiratory Care Considerations..3 Physician Considerations
CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR 801-467-0800 Phone 800-800-HFJV (4358) Hotline TABLE OF CONTENTS Respiratory Care Considerations..3 Physician Considerations
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT AVOIDING THE CRASH 1: DON T INTUBATE, OPTIMIZE PRE-AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD
 ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
It costs you nothing, but gains everything for your patient!
 It costs you nothing, but gains everything for your patient! Attend the entire presentation Complete and submit the evaluation This session is approved for: ANCC hours CECBEMS hours No partial credit will
It costs you nothing, but gains everything for your patient! Attend the entire presentation Complete and submit the evaluation This session is approved for: ANCC hours CECBEMS hours No partial credit will
Consensus Statement: ADULT Rapid Sequence Intubation and Post-Intubation Analgesia and Sedation for Major Trauma Patients.
 Consensus Statement: ADULT Rapid Sequence Intubation and Post-Intubation and Sedation for Major Trauma Patients Participants: Dr. James French, SJRH EM and NBTP Sue Benjamin RN, NBTP Julie Ringuette RN,
Consensus Statement: ADULT Rapid Sequence Intubation and Post-Intubation and Sedation for Major Trauma Patients Participants: Dr. James French, SJRH EM and NBTP Sue Benjamin RN, NBTP Julie Ringuette RN,
Procedural Sedation in the Rural ER
 Procedural Sedation in the Rural ER Hal Irvine MD FCFP Rural FP Anesthetist Sundre, Alberta June 17, 2011 Disclosure I do not have any affiliations (financial or otherwise) with a commercial organization
Procedural Sedation in the Rural ER Hal Irvine MD FCFP Rural FP Anesthetist Sundre, Alberta June 17, 2011 Disclosure I do not have any affiliations (financial or otherwise) with a commercial organization
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
Adult Intubation Skill Sheet
 Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management
 yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
2
 1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
(31189) Hypothermia Initiation Phase One
 Hypothermia Initiation Phase One") Hypothermia Initiation Phase One Diagnosis Allergies For hypothermia tracking purposes only. Please do not uncheck.- Required Cardiac Emergency Tracking For hypothermia tracking purposes only. Consults
Hypothermia Initiation Phase One Diagnosis Allergies For hypothermia tracking purposes only. Please do not uncheck.- Required Cardiac Emergency Tracking For hypothermia tracking purposes only. Consults
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
Airway Management Adult
 Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
CLINICAL VIGNETTE 2016; 2:3
 CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
Don t let your patients turn blue! Isn t it about time you used etco 2?
 Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
Prehospital Medication Assisted Intubation
 Prehospital Medication Assisted Intubation Supersedes: 09-11-06 Effective: 01-29-10 This document includes the protocol for prehospital medication assisted intubation (MAI). Also included are clinical
Prehospital Medication Assisted Intubation Supersedes: 09-11-06 Effective: 01-29-10 This document includes the protocol for prehospital medication assisted intubation (MAI). Also included are clinical
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Physical Exam. T 97.4, HR 76, BP 90/51, Sat 96% Lethargic Lungs clear Heart regular Abdomen soft, epigastric tenderness, distension
 Case Report 58yM with non-bilious non-bloody vomiting for one week. Also reported epigastric abdominal pain. PMH: obesity, HTN, HIV, prior CVA with left sided weakness, bipolar disorder PSH: none SH: former
Case Report 58yM with non-bilious non-bloody vomiting for one week. Also reported epigastric abdominal pain. PMH: obesity, HTN, HIV, prior CVA with left sided weakness, bipolar disorder PSH: none SH: former
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Pediatric Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
STAYTON FIRE DISTRICT PROTOCOL QUIZ
 STAYTON FIRE DISTRICT PROTOCOL QUIZ Name 1. Please list the appropriate EMS Level for each of the Scope of Practice items below EMR Emergency Medical Responder B Basic Conduct primary and secondary patient
STAYTON FIRE DISTRICT PROTOCOL QUIZ Name 1. Please list the appropriate EMS Level for each of the Scope of Practice items below EMR Emergency Medical Responder B Basic Conduct primary and secondary patient
RAPID SEQUENCE INTUBATION FOR THE RURAL DOC
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
All I need is an LMA
 All I need is an LMA Narasimhan Sim Jagannathan, M.D. Associate Chairman, Academic Affairs Director, Pediatric Anesthesia Research Ann & Robert H. Lurie Children s Hospital of Chicago Associate Professor
All I need is an LMA Narasimhan Sim Jagannathan, M.D. Associate Chairman, Academic Affairs Director, Pediatric Anesthesia Research Ann & Robert H. Lurie Children s Hospital of Chicago Associate Professor
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected