DRUGS THAT ACT IN THE CNS
|
|
|
- Kathryn Burke
- 5 years ago
- Views:
Transcription
1 DRUGS THAT ACT IN THE CNS Drugs for Neurodegenerative Diseases 2 Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1
 unless given above recommended doses, where it loses its selectivity.")
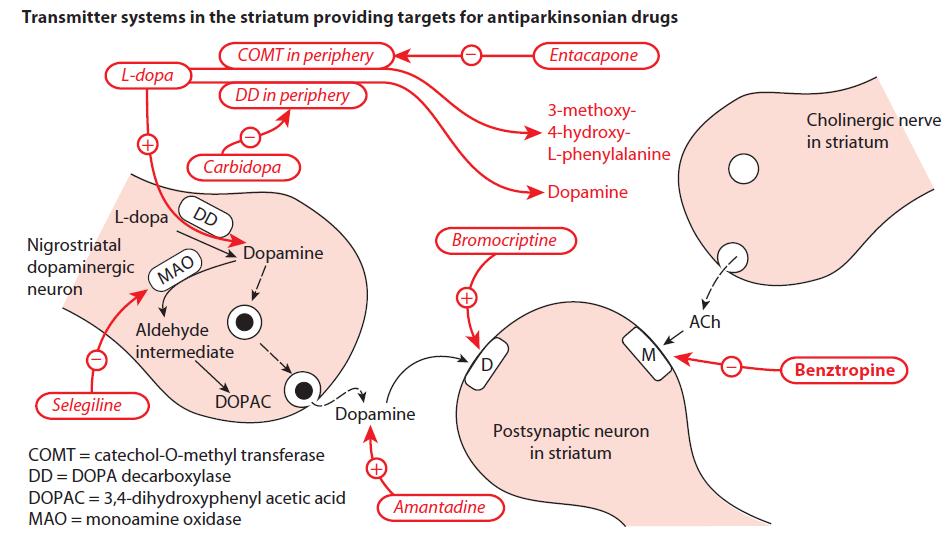
2 DRUGS USED IN PARKINSON S DISEASE/ B. Selegiline and rasagiline Selegiline, also called deprenyl, selectively inhibits monoamine oxidase (MAO) type B (metabolizes dopamine) at low to moderate doses. It does not inhibit MAO type A (metabolizes norepinephrine and serotonin) unless given above recommended doses, where it loses its selectivity. By decreasing the metabolism of dopamine, selegiline increases dopamine levels in the brain.
3 DRUGS USED IN PARKINSON S DISEASE/ B. Selegiline and rasagiline Unlike nonselective MAOIs, selegiline at recommended doses has little potential for causing hypertensive crises. However, the drug loses selectivity at high doses, and there is a risk for severe hypertension. Selegiline is metabolized to methamphetamine and amphetamine, whose stimulating properties may produce insomnia if the drug is administered later than mid-afternoon. Rasagiline, an irreversible and selective inhibitor of brain MAO type B, has five times the potency of selegiline. Unlike selegiline, rasagiline is not metabolized to an amphetamine-like substance.

4 DRUGS USED IN PARKINSON S DISEASE/ C. COMT inhibitors
5 DRUGS USED IN PARKINSON S DISEASE/ C. COMT inhibitors Normally, the methylation of levodopa by catechol-o-methyltransferase (COMT) to 3-Omethyldopa is a minor pathway for levodopa metabolism. However, when peripheral dopamine decarboxylase activity is inhibited by carbidopa, a significant concentration of 3-O-methyldopa is formed that competes with levodopa for active transport into the CNS. Entacapone and tolcapone selectively and reversibly inhibit COMT. Inhibition of COMT by these agents leads to decreased plasma concentrations of 3-Omethyldopa, increased central uptake of levodopa, and greater concentrations of brain dopamine.
6 DRUGS USED IN PARKINSON S DISEASE/ C. COMT inhibitors/pharmacokinetics: Oral absorption of both drugs occurs readily and is not influenced by food. They are extensively bound to plasma albumin, with a limited volume of distribution. Tolcapone has a relatively long duration of action (probably due to its affinity for the enzyme) compared to entacapone, which requires more frequent dosing. Both drugs are extensively metabolized and eliminated in feces and urine. The dosage may need to be adjusted in patients with moderate or severe cirrhosis.
7 DRUGS USED IN PARKINSON S DISEASE/ C. COMT inhibitors/adverse effects: Both drugs exhibit adverse effects that are observed in patients taking levodopa carbidopa, including diarrhea, postural hypotension, nausea, anorexia, dyskinesias, hallucinations, and sleep disorders. Most seriously, hepatic necrosis is associated with tolcapone use. Entacapone does not exhibit this toxicity and has largely replaced tolcapone.
8 DRUGS USED IN PARKINSON S DISEASE/ D. Dopamine receptor agonists This group of antiparkinsonian compounds includes bromocriptine, an ergot derivative, the nonergot drugs, ropinirole, pramipexole, rotigotine, and the newer agent, apomorphine. These agents have a longer duration of action than that of levodopa and are effective in patients exhibiting fluctuations in response to levodopa. Initial therapy with these drugs is associated with less risk of developing dyskinesias and motor fluctuations as compared to patients started on levodopa. Apomorphine is an injectable dopamine agonist that is used in severe and advanced stages of the disease to supplement oral medications. Side effects severely limit the utility of the dopamine agonists



9 DRUGS USED IN PARKINSON S DISEASE/ D. Dopamine receptor agonists/ 1. Bromocriptine:
10 DRUGS USED IN PARKINSON S DISEASE/ D. Dopamine receptor agonists/ 1. Bromocriptine: The actions of the ergot derivative bromocriptine are similar to those of levodopa, except that hallucinations, confusion, delirium, nausea, and orthostatic hypotension are more common, whereas dyskinesia is less prominent. It should be used with caution in patients with a history of myocardial infarction or peripheral vascular disease. Because bromocriptine is an ergot derivative, it has the potential to cause pulmonary fibrosis.
11 DRUGS USED IN PARKINSON S DISEASE/ D. Dopamine receptor agonists/ 2. nonergot drugs: Apomorphine, pramipexole, ropinirole, and rotigotine are nonergot dopamine agonists that are approved for the treatment of Parkinson s disease. These agents alleviate the motor deficits in patients who have never taken levodopa and also in patients with advanced Parkinson s disease who are treated with levodopa. Dopamine agonists may delay the need to use levodopa in early Parkinson s disease and may decrease the dose of levodopa in advanced Parkinson s disease.

12 DRUGS USED IN PARKINSON S DISEASE/ D. Dopamine receptor agonists/ 2. nonergot drugs:
13 DRUGS USED IN PARKINSON S DISEASE/ D. Dopamine receptor agonists/ 2. nonergot drugs: Unlike the ergotamine derivatives, these agents do not exacerbate peripheral vascular disorders or cause fibrosis. Nausea, hallucinations, insomnia, dizziness, constipation, and orthostatic hypotension are among the more distressing side effects of these drugs, but dyskinesias are less frequent than with levodopa. Pramipexole is mainly excreted unchanged in the urine, and dosage adjustments are needed in renal dysfunction. Cimetidine inhibits renal tubular secretion of organic bases and may significantly increase the half-life of pramipexole.
14 DRUGS USED IN PARKINSON S DISEASE/ E. Amantadine: It was accidentally discovered that the antiviral drug amantadin, used to treat influenza, has an antiparkinsonian action. Amantadine has several effects on a number of neurotransmitters implicated in parkinsonism, including increasing the release of dopamine, blocking cholinergic receptors, and inhibiting the N-methyld-aspartate (NMDA) type of glutamate receptors. Current evidence supports action at NMDA receptors as the primary action at therapeutic concentrations.
15 DRUGS USED IN PARKINSON S DISEASE/ E. Amantadine: Note: If dopamine release is already at a maximum, amantadine has no effect. The drug may cause restlessness, agitation, confusion, and hallucinations, and, at high doses, it may induce acute toxic psychosis. Orthostatic hypotension, urinary retention, peripheral edema, and dry mouth also may occur. Amantadine is less efficacious than levodopa, and tolerance develops more readily. However, amantadine has fewer side effects.
16 DRUGS USED IN PARKINSON S DISEASE/ F. Antimuscarinic agents: The antimuscarinic agents are much less efficacious than levodopa and play only an adjuvant role in antiparkinsonism therapy. The actions of benztropine, trihexyphenidyl, procyclidine, and biperiden are similar, although individual patients may respond more favorably to one drug. Blockage of cholinergic transmission produces effects similar to augmentation of dopaminergic transmission, since it helps to correct the imbalance in the dopamine/acetylcholine ratio. These agents can induce mood changes and produce xerostomia (dryness of the mouth), constipation, and visual problems typical of muscarinic blockers. They interfere with gastrointestinal peristalsis and are contraindicated in patients with glaucoma, prostatic hyperplasia, or pyloric stenosis.
17 17
18 DRUGS USED IN ALZHEIMER S DISEASE The most common early symptom is short-term memory loss. As the disease advances, symptoms can include problems with language, disorientation (including easily getting lost), loss of motivation, not managing self care, and behavioural issues. AD distinguishing feature is the loss of cortical neurons, particularly cholinergic neurons. Current therapies aim to either improve cholinergic transmission within the CNS or prevent excitotoxic actions resulting from overstimulation of NMDA-glutamate receptors in selected areas of the brain. Pharmacologic intervention for Alzheimer s disease is only palliative and provides modest short-term benefit. None of the available therapeutic agents alter the underlying neurodegenerative process.
19 DRUGS USED IN ALZHEIMER S DISEASE/ A. AChE inhibitors Numerous studies have linked the progressive loss of cholinergic neurons and, presumably, cholinergic transmission within the cortex to the memory loss that is a hallmark symptom of Alzheimer s disease. It is postulated that inhibition of acetylcholinesterase (AChE) within the CNS will improve cholinergic transmission, at least at those neurons that are still functioning. The reversible AChE inhibitors approved for the treatment of mild to moderate Alzheimer s disease include donepezil, galantamine, and rivastigmine. All of them have some selectivity for AChE in the CNS, as compared to the periphery.
20 DRUGS USED IN ALZHEIMER S DISEASE/ A. AChE inhibitors Galantamine may also augment the action of acetylcholine at nicotinic receptors in the CNS. At best, these compounds provide a modest reduction in the rate of loss of cognitive functioning in Alzheimer patients. Rivastigmine is the only agent approved for the management of dementia associated with Parkinson s disease.



21 DRUGS USED IN ALZHEIMER S DISEASE/ AChE inhibitors

22 DRUGS USED IN ALZHEIMER S DISEASE/ B. NMDA receptor antagonist Memantine is an NMDA receptor antagonist indicated for Alzheimer s disease
23 DRUGS USED IN ALZHEIMER S DISEASE/ B. NMDA receptor antagonist Stimulation of glutamate receptors in the CNS appears to be critical for the formation of certain memories. However, overstimulation of glutamate receptors, particularly of the NMDA type, may result in excitotoxic effects on neurons and is suggested as a mechanism for neurodegenerative or apoptotic (programmed cell death) processes. Binding of glutamate to the NMDA receptor assists in the opening of an ion channel that allows Ca2+ to enter the neuron. Excess intracellular Ca2+ can activate a number of processes that ultimately damage neurons and lead to apoptosis. Memantine is an NMDA receptor antagonist indicated for moderate to severe Alzheimer s disease.
24 DRUGS USED IN ALZHEIMER S DISEASE/ B. NMDA receptor antagonist It acts by blocking the NMDA receptor and limiting Ca2+ influx into the neuron, such that toxic intracellular levels are not achieved. Memantine is well tolerated, with few dose-dependent adverse events. Expected side effects, such as confusion, agitation, and restlessness, are indistinguishable from the symptoms of Alzheimer s disease. Given its different mechanism of action and possible neuroprotective effects, memantine is often given in combination with an AChE inhibitor.
25 DRUGS USED IN ALZHEIMER S DISEASE 25
26 DRUGS USED IN MULTIPLE SCLEROSIS Multiple sclerosis is an autoimmune inflammatory demyelinating disease of the CNS. The course of MS is variable. For some, MS may consist of one or two acute neurologic episodes. In others, it is a chronic, relapsing, or progressive disease that may span 10 to 20 years. Historically, corticosteroids (for example, dexamethasone and prednisone) have been used to treat acute exacerbations of the disease. Chemotherapeutic agents, such as cyclophosphamide and azathioprine, have also been used.

27 DRUGS USED IN MULTIPLE SCLEROSIS/ A. Disease-modifying therapies The major target of medications is to modify the immune response through inhibition of white blood cell mediated inflammatory processes that eventually lead to myelin sheath damage and decreased or inappropriate axonal communication between cells. 1. Interferon β1a and interferon β1b: The immunomodulatory effects of interferon help to diminish the inflammatory responses that lead to demyelination of the axon sheaths. Adverse effects of these medications may include depression, local injection site reactions, hepatic enzyme increases, and flu-like symptoms.
28 DRUGS USED IN MULTIPLE SCLEROSIS/ A. Disease-modifying therapies 2. Glatiramer: Glatiramer is a synthetic polypeptide that resembles myelin protein and may act as a decoy to T-cell attack. Some patients experience a post-injection reaction that includes flushing, chest pain, anxiety, and itching. It is usually self-limiting. 3. Fingolimod: Fingolimod is an oral drug that alters lymphocyte migration, resulting in fewer lymphocytes in the CNS. Fingolimod may cause first-dose bradycardia and is associated with an increased risk of infection and macular edema.
29 DRUGS USED IN MULTIPLE SCLEROSIS/ A. Disease-modifying therapies 4. Teriflunomide: Teriflunomide is an oral pyrimidine synthesis inhibitor that leads to a lower concentration of active lymphocytes in the CNS. Teriflunomide may cause elevated liver enzymes. It should be avoided in pregnancy. 5. Dimethyl fumarate: Dimethyl fumarate is an oral agent that may alter the cellular response to oxidative stress to reduce disease progression. Flushing and abdominal pain are the most common adverse events. 6. Natalizumab: Natalizumab is a monoclonal antibody indicated for MS in patients who have failed first-line therapies. 7. Mitoxantrone: Mitoxantrone is a cytotoxic anthracycline analog that kills T cells and may also be used for MS.
30 DRUGS USED IN MULTIPLE SCLEROSIS/ B. Symptomatic treatment Many different classes of drugs are used to manage symptoms of MS such as spasticity, constipation, bladder dysfunction, and depression. Dalfampridine, an oral potassium channel blocker, improves walking speeds in patients with MS. It is the first drug approved for this use.
31 DRUGS USED IN AMYOTROPHIC LATERAL SCLEROSIS ALS is characterized by progressive degeneration of motor neurons, resulting in the inability to initiate or control muscle movement. Riluzole, an NMDA receptor antagonist, is currently the only drug indicated for the management of ALS. It is believed to act by inhibiting glutamate release and blocking sodium channels. Riluzole may improve survival time and delay the need for ventilator support in patients suffering from ALS.
Drugs Affecting the Central Nervous System
 Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
Drug Therapy of Parkinsonism. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Neurodegenerative diseases
 Neurodegenerative diseases Hiwa K. Saaed, PhD Department of Pharmacology & Toxicology College of Pharmacy University of Sulaimani Hiwa.saaed@univsul.edu.iq 2018-19 Neurodegenerative diseases of the CNS
Neurodegenerative diseases Hiwa K. Saaed, PhD Department of Pharmacology & Toxicology College of Pharmacy University of Sulaimani Hiwa.saaed@univsul.edu.iq 2018-19 Neurodegenerative diseases of the CNS
History Parkinson`s disease. Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson
 Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Drug Management of Parkinsonism. By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.)
; MSc. (Ped.); MHPE (Ed.)") Drug Management of Parkinsonism By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.) Drug management of Parkinsonism Levodopa Ergot derivatives noamine Oxidaes Inhibitors Catechol-Omethyl
Drug Management of Parkinsonism By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.) Drug management of Parkinsonism Levodopa Ergot derivatives noamine Oxidaes Inhibitors Catechol-Omethyl
Drugs used in Parkinsonism
 Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ 40 mv. Resting Membrane. Potential. Time (msec) Depolarization! Hyperpolarized. Na + equilibrium. Action. Potential. Threshold.
 Depolarization! Hyperpolarized. Na + equilibrium. Action. Potential. Threshold.") Local Anesthetics Local anesthetics Block nerve conduction of sensory impulses and, in higher concentrations, motor impulses from the periphery to the CNS. Na+ ion channels are blocked to prevent the transient
Local Anesthetics Local anesthetics Block nerve conduction of sensory impulses and, in higher concentrations, motor impulses from the periphery to the CNS. Na+ ion channels are blocked to prevent the transient
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to
 parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs
 Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs Dopaminergic Drugs: Actions Symptoms of parkinsonism are caused by depletion of dopamine in CNS Amantadine: makes more of dopamine available
Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs Dopaminergic Drugs: Actions Symptoms of parkinsonism are caused by depletion of dopamine in CNS Amantadine: makes more of dopamine available
Medications used to treat Parkinson s disease
 Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
DRUG TREATMENT OF PARKINSON S DISEASE. Mr. D.Raju, M.pharm, Lecturer
 DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
Margo J Nell Dept Pharmacology
 Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1)
") 475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
PARKINSON S MEDICATION
 PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Chapter 20. Media Directory. Amyotrophic Lateral Sclerosis. Alzheimer s Disease. Huntington s Chorea. Multiple Sclerosis
 Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University
 Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Treatment of Parkinson s Disease and of Spasticity. Satpal Singh Pharmacology and Toxicology 3223 JSMBS
 Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
What s new for diagnosing and treating Parkinson s Disease?
 What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
Parkinson s Disease Medications: Professionals Edition
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Parkinson s disease Therapeutic strategies. Surat Tanprawate, MD Division of Neurology University of Chiang Mai
 Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Pal Riba, M.D., Ph.D. Department of Pharmacology and Pharmacotherapy Semmelweis University, Budapest, Hungary November 7, 2017
 Pal Riba, M.D., Ph.D. Department of Pharmacology and Pharmacotherapy Semmelweis University, Budapest, Hungary November 7, 2017 Definition of neurodegeneration Irreversible death of neurons resulting in
Pal Riba, M.D., Ph.D. Department of Pharmacology and Pharmacotherapy Semmelweis University, Budapest, Hungary November 7, 2017 Definition of neurodegeneration Irreversible death of neurons resulting in
Edyta Gołąbiewska PhD
 Edyta Gołąbiewska PhD The depth of anesthesia has been divided into four sequential stages: Stage 1: Analgesia (induction) Stage 2: Excitement Stage 3: Surgical anesthesia Stage 4: Medullary paralysis
Edyta Gołąbiewska PhD The depth of anesthesia has been divided into four sequential stages: Stage 1: Analgesia (induction) Stage 2: Excitement Stage 3: Surgical anesthesia Stage 4: Medullary paralysis
Parkinson's Disease. Robert L. Copeland, Ph.D. Howard University College of Medicine Department of Pharmacology
 Parkinson's Disease Robert L. Copeland, Ph.D. Howard University College of Medicine Department of Pharmacology 18 February 2002 Parkinson Disease Neurological disease affecting over four million patients
Parkinson's Disease Robert L. Copeland, Ph.D. Howard University College of Medicine Department of Pharmacology 18 February 2002 Parkinson Disease Neurological disease affecting over four million patients
Best Medical Treatments for Parkinson s disease
 Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Parkinson s Pharmacology
 PHPP 517 (IT-III) Fall 2011 JACOBS Wed 10/12 8:00 8:50 AM 1 Learning objectives 1. Describe the direct and indirect pathways of the extrapyramidal system and its modulation by ACh and DA. 2. Contrast the
PHPP 517 (IT-III) Fall 2011 JACOBS Wed 10/12 8:00 8:50 AM 1 Learning objectives 1. Describe the direct and indirect pathways of the extrapyramidal system and its modulation by ACh and DA. 2. Contrast the
The symptoms of the Parkinson s disease may vary from person to person. The symptoms might include the following:
 1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Lecture 5 Skeletal muscle relaxants. Pharmacologic management of parkinsonism and other movement disorders.
 Lecture 5 Skeletal muscle relaxants. Pharmacologic management of parkinsonism and other movement disorders. I. SKELETAL MUSCLE RELAXANTS Skeletal muscle relaxants are pharmacologically active substances
Lecture 5 Skeletal muscle relaxants. Pharmacologic management of parkinsonism and other movement disorders. I. SKELETAL MUSCLE RELAXANTS Skeletal muscle relaxants are pharmacologically active substances
XADAGO (safinamide) oral tablet
 oral tablet") XADAGO (safinamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
XADAGO (safinamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
2-The age at onset of PD is variable, usually between 50 and 80 years, with a mean onset of 55 years (1).
.") Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Elements for a public summary
 VI.2 VI.2.1 Elements for a public summary Overview of disease epidemiology Parkinson s disease affects individuals globally (WHO 2006). It is the most common serious movement disorder, including speech
VI.2 VI.2.1 Elements for a public summary Overview of disease epidemiology Parkinson s disease affects individuals globally (WHO 2006). It is the most common serious movement disorder, including speech
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Communicating About OFF Episodes With Your Doctor
 Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
Cardinal Features of Parkinson s. Management of Parkinson s Disease. Drug Induced Parkinson s. Other Parkinson s Symptoms.
 Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Re-Submission. Scottish Medicines Consortium. rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd.
 (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd.") Scottish Medicines Consortium Re-Submission rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd 10 November 2006 The Scottish Medicines Consortium (SMC) has completed
Scottish Medicines Consortium Re-Submission rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd 10 November 2006 The Scottish Medicines Consortium (SMC) has completed
SIFROL Composition Properties Indication
 SIFROL Boehringer Composition 1 tablet contains: 0.125, 0.25 or 1.0 mg, (S)-2- amino-4,5,6,7-tetrahydro-6-propylamino-benzothiazole dihydrochloride monohydrate equivalent to 0.088, 0.18 or 0.7 mg pramipexole
SIFROL Boehringer Composition 1 tablet contains: 0.125, 0.25 or 1.0 mg, (S)-2- amino-4,5,6,7-tetrahydro-6-propylamino-benzothiazole dihydrochloride monohydrate equivalent to 0.088, 0.18 or 0.7 mg pramipexole
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
New Medicines Committee Briefing July 2011
 New Medicines Committee Briefing July 2011 Pramipexole immediate-release (Mirapexin ) and Pramipexole modifiedrelease (Mirapexin prolonged release) for the treatment of Parkinson s Disease Pramipexole
New Medicines Committee Briefing July 2011 Pramipexole immediate-release (Mirapexin ) and Pramipexole modifiedrelease (Mirapexin prolonged release) for the treatment of Parkinson s Disease Pramipexole
Dorset Medicines Advisory Group SHARED CARE GUIDELINES FOR PRESCRIBING ENTACAPONE (INCLUDING IN COMBINATION) OR OPICAPONE IN PARKINSON S DISEASE
 OR OPICAPONE IN PARKINSON S DISEASE") SHARED CARE GUIDELINES FOR PRESCRIBING ENTACAPONE (INCLUDING IN COMBINATION) OR OPICAPONE IN PARKINSON S DISEASE INDICATION By inhibiting metabolism of levodopa, entacapone or opicapone allow a reduction
SHARED CARE GUIDELINES FOR PRESCRIBING ENTACAPONE (INCLUDING IN COMBINATION) OR OPICAPONE IN PARKINSON S DISEASE INDICATION By inhibiting metabolism of levodopa, entacapone or opicapone allow a reduction
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Prior Authorization with Quantity Limit Program Summary
 Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Parkinson s Disease Update. Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015
 Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
Presenter. Dr. Ronald Lucchino
 Adverse Drug Reactions in Adults with Down Syndrome Presenter Dr. Ronald Lucchino rvluc@comcast.net PURPOSE To increase staff awareness that older adults with DD may have higher levels of medication in
Adverse Drug Reactions in Adults with Down Syndrome Presenter Dr. Ronald Lucchino rvluc@comcast.net PURPOSE To increase staff awareness that older adults with DD may have higher levels of medication in
Parkinson s Disease. Gillian Sare
 Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
SIFROL â. Contraindications Hypersensitivity to pramipexole or any other component of the product.
 SIFROL â Composition 1 tablet contains 0.088, 0.18 & 0.7 mg (S) 2 amino 4,5,6,7-tetrahydro-6-propylamino-benzothiazole (= pramipexole base) equivalent to 0.125, 0.25 & 1 mg of pramipexole dihydrochloride
SIFROL â Composition 1 tablet contains 0.088, 0.18 & 0.7 mg (S) 2 amino 4,5,6,7-tetrahydro-6-propylamino-benzothiazole (= pramipexole base) equivalent to 0.125, 0.25 & 1 mg of pramipexole dihydrochloride
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych
 Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.
Prof dr Aleksandar Raskovic DIRECT VASODILATORS
 Prof dr Aleksandar Raskovic DIRECT VASODILATORS Direct vasodilators Minoxidil (one of the most powerful peripheral arterial dilators) Opening of KATP channels, efflux of K, lose of Ca and smooth muscle
Prof dr Aleksandar Raskovic DIRECT VASODILATORS Direct vasodilators Minoxidil (one of the most powerful peripheral arterial dilators) Opening of KATP channels, efflux of K, lose of Ca and smooth muscle
Classes of Neurotransmitters. Neurotransmitters
 1 Drugs Outline 2 Neurotransmitters Agonists and Antagonists Cocaine & other dopamine agonists Alcohol & its effects / Marijuana & its effects Synthetic & Designer Drugs: Ecstasy 1 Classes of Neurotransmitters
1 Drugs Outline 2 Neurotransmitters Agonists and Antagonists Cocaine & other dopamine agonists Alcohol & its effects / Marijuana & its effects Synthetic & Designer Drugs: Ecstasy 1 Classes of Neurotransmitters
Parkinson s Disease and Its Treatment
 Parkinson s Disease and Its Treatment By H. David Bergman, Ph.D. Dean, Southwestern Oklahoma State University, College of Pharmacy Goals and Objectives Goals: To provide the pharmacist with information
Parkinson s Disease and Its Treatment By H. David Bergman, Ph.D. Dean, Southwestern Oklahoma State University, College of Pharmacy Goals and Objectives Goals: To provide the pharmacist with information
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Making Every Little Bit Count: Parkinson s Disease. SHP Neurobiology of Development and Disease
 Making Every Little Bit Count: Parkinson s Disease SHP Neurobiology of Development and Disease Parkinson s Disease Initially described symptomatically by Dr. James Parkinson in 1817 in An Essay on the
Making Every Little Bit Count: Parkinson s Disease SHP Neurobiology of Development and Disease Parkinson s Disease Initially described symptomatically by Dr. James Parkinson in 1817 in An Essay on the
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
'BAD GUYS' AMONG THE ANTIPARKINSONIAN DRUGS
 Medicinska naklada - Zagreb, Croatia Conference paper 'BAD GUYS' AMONG THE ANTIPARKINSONIAN DRUGS Zvezdan Pirtošek Centre for Extrapyramidal Disorders, Department of Neurology, UMCL, Zaloška 2, Ljubljana,
Medicinska naklada - Zagreb, Croatia Conference paper 'BAD GUYS' AMONG THE ANTIPARKINSONIAN DRUGS Zvezdan Pirtošek Centre for Extrapyramidal Disorders, Department of Neurology, UMCL, Zaloška 2, Ljubljana,
CE Prn. Pharmacy Continuing Education from WF Professional Associates ABOUT WFPA LESSONS TOPICS ORDER CONTACT PHARMACY EXAM REVIEWS
 CE Prn Pharmacy Continuing Education from WF Professional Associates ABOUT WFPA LESSONS TOPICS ORDER CONTACT PHARMACY EXAM REVIEWS Parkinson s Disease Parkinson s disease (PD) is a chronic, progressive,
CE Prn Pharmacy Continuing Education from WF Professional Associates ABOUT WFPA LESSONS TOPICS ORDER CONTACT PHARMACY EXAM REVIEWS Parkinson s Disease Parkinson s disease (PD) is a chronic, progressive,
Key Concepts and Issues in Parkinson s Disease in 2016
 Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
PD: Key Treatment Considerations
 PD: Key Treatment Considerations 2018 Management of Neurologic and Neurosurgical Disorders in Daily Practice Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 11/27/2018 1 Outline Treatment
PD: Key Treatment Considerations 2018 Management of Neurologic and Neurosurgical Disorders in Daily Practice Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 11/27/2018 1 Outline Treatment
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn
 Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn Objectives What agents do we currently have available and what do we ideally need? What biomarkers exist for
Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn Objectives What agents do we currently have available and what do we ideally need? What biomarkers exist for
Qualitative and Quantitative Composition
 DATA SHEET KEMADRIN Tablets Procyclidine Hydrochloride 5 mg Tablets Qualitative and Quantitative Composition White, round, biconvex tablets, one face with a break line and coded KT above the break line
DATA SHEET KEMADRIN Tablets Procyclidine Hydrochloride 5 mg Tablets Qualitative and Quantitative Composition White, round, biconvex tablets, one face with a break line and coded KT above the break line
Commonly encountered medications and their side effects - what the generalist needs to know
 Commonly encountered medications and their side effects - what the generalist needs to know Jeremy Cosgrove Consultant Neurologist Leeds Teaching Hospitals NHS Trust Outline: Parkinson s medications and
Commonly encountered medications and their side effects - what the generalist needs to know Jeremy Cosgrove Consultant Neurologist Leeds Teaching Hospitals NHS Trust Outline: Parkinson s medications and
Drugs for Parkinson s Disease
 This Clinical Resource gives subscribers additional insight related to the Recommendations published in July 2017 ~ Resource #330705 Drugs for Parkinson s Disease Parkinson s disease is characterized by
This Clinical Resource gives subscribers additional insight related to the Recommendations published in July 2017 ~ Resource #330705 Drugs for Parkinson s Disease Parkinson s disease is characterized by
Parkinson's Disease and how you can make a difference with medication
 Parkinson's Disease and how you can make a difference with medication Alyson Franks Parkinson's and Movement Disorder Nurse Specialist Royal Hallamshire Hospital No treatment all Complementary Therapy
Parkinson's Disease and how you can make a difference with medication Alyson Franks Parkinson's and Movement Disorder Nurse Specialist Royal Hallamshire Hospital No treatment all Complementary Therapy
Antidepressants. Dr Malek Zihlif
 Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
March 2004 Parkinson s Disease H01
 W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 March 2004 Parkinson s Disease 707-000-04-003-H01 FLORIDA PHARMACISTS READ THIS VERY IMPORTANT CE BROKER
W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 March 2004 Parkinson s Disease 707-000-04-003-H01 FLORIDA PHARMACISTS READ THIS VERY IMPORTANT CE BROKER
PDL Class: Parkinson s Drugs
 Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review: September 2013 Date of Last Review:
Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review: September 2013 Date of Last Review:
Any interventions, where RCTs in PD are not available, are not included in the tables.
 Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Treatment of Alzheimer s disease
 NORTH AND EAST DEVON HEALTHCARE COMMUNITY SHARED CARE PRESCRIBING GUIDELINE http://www.devonpct.nhs.uk/treatments/ne_devon_shared_care_guidelines.aspx#a Treatment of Alzheimer s disease Acetylcholinesterase
NORTH AND EAST DEVON HEALTHCARE COMMUNITY SHARED CARE PRESCRIBING GUIDELINE http://www.devonpct.nhs.uk/treatments/ne_devon_shared_care_guidelines.aspx#a Treatment of Alzheimer s disease Acetylcholinesterase
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Primary Care Prescribing Protocol to Support the Diagnosis and Management of People with Dementia
 Primary Care Prescribing Protocol to Support the Diagnosis and Management of People with Dementia This prescribing guideline provides the necessary information and guidance to support clinicians in the
Primary Care Prescribing Protocol to Support the Diagnosis and Management of People with Dementia This prescribing guideline provides the necessary information and guidance to support clinicians in the
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019
 WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Cholinergic antagonists
 Cholinergic antagonists Cholinergic antagonists: They are also called anticholinergic drugs or cholinergic blockers, this group include: 1.Antimuscarinic agents ( atropine, ipratropium, scopolamine) 2.
Cholinergic antagonists Cholinergic antagonists: They are also called anticholinergic drugs or cholinergic blockers, this group include: 1.Antimuscarinic agents ( atropine, ipratropium, scopolamine) 2.
What is the best medical therapy for early Parkinson's disease? Medications Commonly Used for Parkinson's Disease
 FPIN's Clinical Inquiries Treatment of Early Parkinson's Disease Clinical Question What is the best medical therapy for early Parkinson's disease? Evidence-Based Answer Treatment of early Parkinson's disease
FPIN's Clinical Inquiries Treatment of Early Parkinson's Disease Clinical Question What is the best medical therapy for early Parkinson's disease? Evidence-Based Answer Treatment of early Parkinson's disease
ANTIPARKINSONIAN DRUGS. DRUGs ACT ON CNS (Pharmacology) Unit-5(8)
 Unit-5(8)") ANTIPARKINSONIAN DRUGS DRUGs ACT ON CNS (Pharmacology) Unit-5(8) Parkinsonism (PD) Extrapyramidal motor function disorder characterized by Rigidity Tremor Hypokinesia/Bradykinesia Impairment of postural
ANTIPARKINSONIAN DRUGS DRUGs ACT ON CNS (Pharmacology) Unit-5(8) Parkinsonism (PD) Extrapyramidal motor function disorder characterized by Rigidity Tremor Hypokinesia/Bradykinesia Impairment of postural
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N.
 PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
Dementia Pharmacotherapy
 Dementia Pharmacotherapy 1 early therapeutic interventions can maximize pharmacologic efficacy with these agents 2 Selecting a Medication Not enough evidence to recommend one agent over another based on
Dementia Pharmacotherapy 1 early therapeutic interventions can maximize pharmacologic efficacy with these agents 2 Selecting a Medication Not enough evidence to recommend one agent over another based on
Appendix N: Research recommendations
 Appendix N: recommendations N.1 First-line treatment of motor symptoms recommendation 1 Interventions What is the effectiveness of initial levodopa monotherapy versus initial levodopa-dopamine agonist
Appendix N: recommendations N.1 First-line treatment of motor symptoms recommendation 1 Interventions What is the effectiveness of initial levodopa monotherapy versus initial levodopa-dopamine agonist
Rotigotine patches (Neupro) in early Parkinson s disease Edited by AdRes Health Economics & Outcomes Research
 in early Parkinson s disease Edited by AdRes Health Economics & Outcomes Research") Rotigotine patches (Neupro) in early Parkinson s disease Edited by AdRes Health Economics & Outcomes Research Synthetic DRUG PROFILE Introduction Parkinson s disease (PD) is a neurodegenerative disorder
Rotigotine patches (Neupro) in early Parkinson s disease Edited by AdRes Health Economics & Outcomes Research Synthetic DRUG PROFILE Introduction Parkinson s disease (PD) is a neurodegenerative disorder
LESSON ASSIGNMENT. Cholinergic Blocking Agents (Anticholinergic Agents).
.") LESSON ASSIGNMENT LESSON 10 Cholinergic Blocking Agents (Anticholinergic Agents). TEXT ASSIGNMENT Paragraphs 10-1 through 10-4. LESSON OBJECTIVES 10-1. From a list of statements, select the statement that
LESSON ASSIGNMENT LESSON 10 Cholinergic Blocking Agents (Anticholinergic Agents). TEXT ASSIGNMENT Paragraphs 10-1 through 10-4. LESSON OBJECTIVES 10-1. From a list of statements, select the statement that
Medication Management & Strategies When the levodopa honeymoon is over
 Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
8/28/2017. Behind the Scenes of Parkinson s Disease
 BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
Part 2: How Your Brain and Nervous System Work
 Part 2: How Your Brain and Nervous System Work with Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one onone relationship with a qualified
Part 2: How Your Brain and Nervous System Work with Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one onone relationship with a qualified
Anticholinergics. COMT* Inhibitors. Dopaminergic Agents. Dopamine Agonists. Combination Product
 Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts