Fellows Conference 01/21/2016
|
|
|
- Gilbert Goodman
- 5 years ago
- Views:
Transcription


1 Fellows Conference 01/21/2016
2 Outline Basics of transplantation Benefits of transplantation Immunosuppressive medications

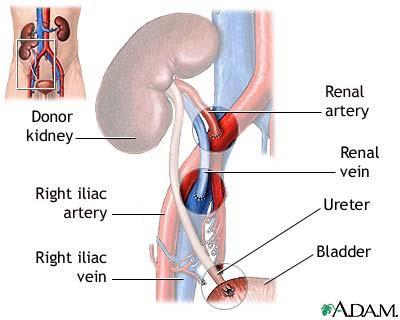
3 Anatomy of Renal Transplantation
4 Recipient Selection General medical condition. Cardiovascular screening. Age-appropriate routine cancer screening (pap smear, mammography, colonoscopy, PSA). Infection (HIV, Hepatitis, TB). Presence of preformed antibody (PRA). Pregnancy, prior transplant, blood transfusion Psychosocial evaluation, including compliance.
5 Benefits of Transplantation Life expectancy Cardiovascular benefits Quality of life Socioeconomic benefits
6 Life Expectancy Ojo, J Am Soc Neph, 2001;12:589
:8 Slide courtesy of Dr.")
7 Cardiovascular Benefits Foley, Am J Kidney Dis, 1998;32(S1):8 Slide courtesy of Dr. Robert Gaston
8 Quality of Life Numerous studies have detailed improved quality of life. Life satisfaction, physical and emotional well-being and ability to return to work higher in transplant recipients. Uremic complications more fully reversed. Fertility returns.
9 Socioeconomic Benefits Increased rates of return to work. Cost to society: First year after transplantation: > Annual cost of hemodialysis Thereafter: $10,000 per year.

10 Immunosuppressive Medications Slide courtesy of Dr. Meier-Kriesche


11 Immunosuppression use USRDS Patients age 18 & older receiving a first-time, kidney-only transplant. IL2-RA: interleukin-2 receptor antagonist.
12 Three-Signal Model Halloran, N Eng J Med, 2004;351:3715
13 Immunosuppressive Medications Induction: Corticosteroids Anti-thymocyte globulin (ATG) Alemtuzumab (Campath) IL-2 receptor antagonists Maintenance: Corticosteroids Calcineurin inhibitors (CNIs) mtor inhibitors Antimetabolites Belatacept
14 Immunosuppressive Medications Treatment of Rejection: Corticosteroids Anti-thymocyte globulin Intravenous Immunoglobulin (IVIG) Rituximab Bortezomib Plasmapheresis
15 Induction Agents Monoclonal (Daclizumab, Basiliximab, Alemtuzumab, OKT3) Polyclonal (Thymoglobulin, atgam) Depleting agents (Thymoglobulin, Alemtuzumab, OKT3) Non-depleting agents (Daclizumab, Basiliximab)
16 Corticosteroids Used for induction, maintenance and treatment of rejection. Mechanism of action: Inhibit function of dendritic cells. Inhibit translocation to nucleus of NF-κB. Suppress production of IL-1, IL-2, IL-3, IL-6, TNF-α, and γ-ifn. Adverse effects numerous and well-known.
17 Halloran, N Eng J Med, 2004;351:3715
18 Corticosteroids Component of >80% of transplant protocols. Given IV at high doses ( mg/day) for induction or treatment of rejection. Tapered to maintenance dose of 5-10 mg/day in early post-transplant phase. Should NOT be tapered off: increased risk of rejection and graft loss! Steroid free regimen: overall some benefits but graft survival likely worse.
19 Anti-thymocyte Globulin (Thymoglobulin) Used for induction and treatment of rejection. Prepared by immunization of rabbits with human lymphoid tissue. Causes depletion of peripheral blood lymphocytes. The optimal dose - 6 mg/kg Typical regimen of Thymoglobulin for induction consists of 1.5 mg/kg for 3 to 5 days Administered generally via central line for 3-10 days. Premedication required: acetaminophen, corticosteroids and antihistamine.
20 Anti-thymocyte Globulin: Adverse Effects Infusion-related reactions: chills, fevers, arthralgias. Lymphopenia. Thrombocytopenia. Prolonged immunosuppression: increased risk of opportunistic infections (PCP, CMV, fungal). Possibly increased risk of BK virus nephropathy.
21 Alemtuzumab (Campath) It is a humanized monoclonal antibody directed against CD52. CD52 is present on virtually all B- and T-cells as well as macrophages, NK cells, and some granulocytes. When the alemtuzumab antibody binds to CD52, it is thought to trigger an antibody-dependent lysis of the cell. The depletion of lymphocytes is so marked that it takes several months to a year post administration for the immune system of a patient to be fully reconstituted
22 Halloran, N Eng J Med, 2004;351:3715
23 Alemtuzumab: Adverse Effects Dosing: mg on the day of transplantation. A second dose on POD 1 or 4 can also be given. Side Effects: The depleting efficiency of alemtuzumab is so profound that it is invariably associated with side effects viz. neutropenia (70%), thrombocytopenia (52%), anemia (47%), nausea (54%), vomiting (41%), diarrhea (22%), headache (24%), dysthesias (15%), dizziness (12%), and AIHA(<5%).
24 IL-2 Receptor Blockers Basiliximab (Simulect ) and Daclizumab (Xenapax ). Block CD25 (IL-2 receptor) on activated T cells. Used for induction only. Almost no side effects, but also much less potent.
25 Halloran, N Eng J Med, 2004;351:3715
26 Calcineurin Inhibitors Used for maintenance immunosuppression. Two agents in clinical practice: Cyclosporine (Sandimmune, Gengraf, Neoral, generic; CysA) Tacrolimus (Prograf, generic; FK506). Generics NOT clinically therapeutically equivalent. At present are key to maintenance immunosuppression and a component of the majority of transplant protocols.
.")
27 Calcineurin Inhibitors: Mechanism of Action CsA: Cyclosporine FK506: Tacrolimus FKBP: FK Binding Protein CpN: Cyclophilin NF-AT: Nuclear Factor of Activated T-cells (ccytosolic component; n- nuclear component). Stepkowski, Expert Rev Mol Med, 2000;2(4):1
28 Halloran, N Eng J Med, 2004;351:3715
29 Calcineurin Inhibitors: Dosing and Monitoring Both medications are generally dosed twice per day, 12 hrs apart. Trough levels monitored: check approximately 12 hrs after last dose. In some cases C2 levels might be checked 2 hrs after administration. Cyclosporine is 35-40% bioavailable, tacrolimus approximately 25%. Oral to IV conversion 3-4:1. Both are metabolized by cytochrome P450 3A4 & 3A5.
, Comprehensive Clinical Nephrology, Mosby Elsevier,")
30 Calcineurin Inhibitors: Interactions Halloran, from Johnson (ed.), Comprehensive Clinical Nephrology, Mosby Elsevier, 2003.
31 Calcineurin Inhibitors: Interactions Drugs to use with caution: NSAIDs avoid. Amphotericin B & Aminoglycosides worsened nephrotoxicity. ACEi & ARBs use with caution. Statins avoid lovastatin, start others at lowest possible dose.
32 Calcineurin Inhibitors: P-Glycoprotein P-Glycoprotein (P-gp, also known as MDR1) is an ABC-transporter found among other places, in the intestine. It is thought to have evolved as a defense mechanism against harmful substances. It acts as an efflux pump for many substances including drugs (CNIs, colchicine, some cancer chemotherapeutic agents, digoxin, corticosteroids, antiretrovirals). Decreased P-gp expression, such as in diarrhea, leads to elevated drug levels.
33 Calcineurin Inhibitors: Adverse Effects Nephrotoxicity: Functional decrease in blood flow from afferent arteriolar vasoconstriction. Thrombotic microangiopathy (rare). Chronic interstitial fibrosis. Hyperkalemia, hypomagnesemia and type IV renal tubular acidosis. Cyclosporine thought to be more nephrotoxic.
34 Calcineurin Inhibitors: Adverse Effects Cyclosporine Tacrolimus Hypertension ++ + Pancreatic islet toxicity + ++ Neurotoxicity + ++ Hirsutism + - Hair loss - + Gum hypertrophy + - GI side effects - + Gastric motility - + Dyslipidemia + - Hyperuricemia ++ + K + / Mg Adapted from Danovitch, Handbook of Kidney Transplantation, Lippincott Williams & Wilkins, 2005
35 mtor Inhibitors Target site is the mammalian target of rapamycin (mtor), a key regulatory kinase in cell division. Sirolimus (Rapamune ) only available mtor inhibitor in the US. Administered once daily, 24-hour trough levels monitored. Also metabolized by P450 3A system, with interactions similar to the CNIs.

36 Sirolimus: Mechanism of Action SRL: Sirolimus FKBP: FK Binding Protein mtor: Mammalian target of rapamycin Cdk: cyclin-dependent kinase Stepkowski, Expert Rev Mol Med, 2000;2(4):1
37 Halloran, N Eng J Med, 2004;351:3715
38 Sirolimus: Adverse Effects Nephrotoxicity: Delays recovery from ATN. Potentiates cyclosporine nephrotoxicity. Induces proteinuria. Tubulotoxic. Impairment of wound healing. Dyslipidemia (increased LDL and TGs). Pneumonitis. Cytopenias and anemia.
39 Antimetabolites Azathioprine (Imuran, generic) is a purine analogue that is incorporated into RNA and inhibits cell replication. A mainstay of transplantation for 30 years, it has largely been replaced by the below drugs. Mycophenolate mofetil (Cellcept ) and enteric-coated mycophenolate sodium (Myfortic ) are prodrugs of mycophenolic acid (MPA), an inhibitor of inosine monophosphate dehydrogenase (IMPDH).
40 Mechanism of Action: MPA Prodrugs Stepkowski, Expert Rev Mol Med, 2000;2(4):1
41 Halloran, N Eng J Med, 2004;351:3715
42 Antimetabolites: Adverse Effects Azathioprine: Bone marrow suppression. Hepatitis. Azathioprine is inactivated by xanthine oxidase, therefore should not be used in combination with allopurinol. MPA prodrugs: GI toxicity: diarrhea, nausea, esophagitis. Leukopenia and anemia. Not different between formulations.
43 Antimetabolites: Interactions Azathioprine: Allopurinol Other marrow suppressive drugs MPA prodrugs: Cyclosporine Antacids Cholestyramine Ferrous sulfate OK to use with allopurinol
44 Belatacept: 1st Biological drug to get FDA approval for kidney transplant
45 Halloran, N Eng J Med, 2004;351:3715
46 Belatacept: Mechanism of Action This monoclonal antibody fusion protein is designed to act as a selective costimulation blocker. It binds to CD80/86 on antigen-presenting cells (APCs), blocking CD28-mediated costimulation of T cells. Costimulation blockade inhibits cell division, cytokine production, anergy, and apoptosis.

47 T-Cells Require Costimulation for Full Activation Signal 2 Costimulation between ligands Signal 1 Antigen triggers T-cell receptor Cytokine production T-cell proliferation APC=antigen-presenting cell

48 T-Cells Require Costimulation for Full Activation TCR signal only=no activation No Signal 2 Signal 1 only No cytokine production No cell division Becomes anergic Undergoes apoptosis APC=antigen-presenting cell; TCR=T-cell receptor; MHC=major histocompatibility complex


49 CTLA4 Negatively Regulates T-cell Activation CTLA4 (CD152) expression is induced by T-cell activation CTLA4 is structurally similar to CD28 CTLA4 binds CD80/86 with greater avidity than CD28 CTLA4 negatively regulates T-cell activation

50 Belatacept Potently and Selectively Blocks T-Cell Activation Belatacept Selective costimulation blocker No cell division No cytokine production Anergy Apoptosis
51 Belatacept: Potential Benefits When compared with CNI-based therapy, belatacept use is associated with significant advantages that seem to translate into better long-term allograft survival, including: Preservation of the GFR A favorable metabolic profile Fewer late rejections An impact on de novo donor-specific antibody (DSA) formation
52 Intravenous Immune Globulin Used primarily for treatment of antibody-mediated rejection. Mechanism of action: Reduction of alloantibodies through suppression of antibody formation. Increased catabolism of circulating antibodies. Adverse effects: Infusion-related reactions (myalgias, headaches). Severe headache & aseptic meningitis. Autoimmine hemolytic anemia. Sucrose-based IVIG can cause ARF.
53 Rituximab Used in the treatment of antibody-mediated rejection. Monoclonal antibody directed at CD20 antigen on B lymphocytes. Causes rapid and sustained depletion of B lymphocytes. Does not have direct activity against plasma cells and memory B cells, which do not express CD20. Adverse events: infusion reactions, and increased susceptibility to infection.
54 Bortezomib Mechanism of action Inhibits proteosome formation, thus interfering with protein degradation and leading to programmed cell death (apoptosis). Targets mature rapidly proliferating antibody-producing plasma cells. Also interferes with T-cell function, IL-1, IL-6 and TNF-α production.
55 Bortezomib Dosing 1.3 mg/m 2 (usual starting dose). In case of side effects, dose is reduced to 1.0 mg/m 2, then to 0.9 mg/m 2, then to 0.7 mg/m 2 (if needed). Metabolized by the liver and thus no need to adjust dose by renal function. Partially removed by dialysis (administer after dialysis). Cleared by plasmapheresis (administer after plasmapheresis).
56 Bortezomib Contraindications Moderate to severe pre-existing peripheral neuropathy Platelet count < 30,000/mm 3 ANC < 500/ mm 3 Hgb < 8 g/dl Uncontrolled hypotension
57 Bortezomib Adverse reactions Neurologic: peripheral neuropathy (mostly sensory: pain and paresthesias), fatigue, malaise, weakness, headache, insomnia Hematologic: leukopenia (especially days 1-11), neutropenia, anemia, thrombocytopenia GI: nausea, vomiting, anorexia, constipation CV: hypotension, edema ID: Herpes zoster infection
58 Other Agents OKT3 Used for induction and treatment of rejection, now largely replaced by anti-thymocyte globulin. Monoclonal antibody against CD3 Severe infusion reactions (pulmonary edema & capillary leak syndrome). Leflunomide (Arava ) Dihyroorotate dehydrogenase (DHODH) inhibitor. Used in certain clinical settings as an adjunct immunosuppressive.
Overview of New Approaches to Immunosuppression in Renal Transplantation
 Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Controversies in Renal Transplantation. The Controversial Questions. Patrick M. Klem, PharmD, BCPS University of Colorado Hospital
 Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
Liver Transplant Immunosuppression
 Liver Transplant Immunosuppression Michael Daily, MD, MS, FACS Surgical Director, Kidney and Pancreas Transplantation University of Kentucky Medical Center Disclosures No financial disclosures I will be
Liver Transplant Immunosuppression Michael Daily, MD, MS, FACS Surgical Director, Kidney and Pancreas Transplantation University of Kentucky Medical Center Disclosures No financial disclosures I will be
IMMUNOSUPPRESSIVE THERAPY Overview. Desensitization
 IMMUNOSUPPRESSIVE THERAPY Overview Two types of immune responses to allografts: Cellular response: foreign antigen recognition activate antigen-specific lymphocytes (T-cells) o Key mediator: T-cells o
IMMUNOSUPPRESSIVE THERAPY Overview Two types of immune responses to allografts: Cellular response: foreign antigen recognition activate antigen-specific lymphocytes (T-cells) o Key mediator: T-cells o
Immunosuppressants. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
Aljoša Kandus Renal Transplant Center, Department of Nephrology, University Medical Center Ljubljana, Slovenia
 Aljoša Kandus Renal Transplant Center, Department of Nephrology, University Medical Center Ljubljana, Slovenia Immunosuppression in kidney transplantation Aljoša Kandus Renal Transplant Center, Department
Aljoša Kandus Renal Transplant Center, Department of Nephrology, University Medical Center Ljubljana, Slovenia Immunosuppression in kidney transplantation Aljoša Kandus Renal Transplant Center, Department
OBJECTIVES. Phases of Transplantation and Immunosuppression
 Transplant and Immunosuppression: Texas Transplant Center April 29, 2017 Regina L. Ramirez, Pharm.D., BCPS PGY1 Pharmacy Residency Program Director Clinical Practice Specialist Solid Organ Transplant and
Transplant and Immunosuppression: Texas Transplant Center April 29, 2017 Regina L. Ramirez, Pharm.D., BCPS PGY1 Pharmacy Residency Program Director Clinical Practice Specialist Solid Organ Transplant and
Overview of Immunosuppression in Renal Transplantation
 Chapter 10 Overview of Immunosuppression in Renal Transplantation M. Ghanta, J. Dreier, R. Jacob and I. Lee Additional information is available at the end of the chapter http://dx.doi.org/10.5772/54865
Chapter 10 Overview of Immunosuppression in Renal Transplantation M. Ghanta, J. Dreier, R. Jacob and I. Lee Additional information is available at the end of the chapter http://dx.doi.org/10.5772/54865
9/30/ DISCLOSURES. + First: Why immunosuppress? Transplant Immunosuppression and Prophylaxis
 Transplant Immunosuppression and Prophylaxis Sarah Fitz, APN, MSN, ACNP-BC Loyola University Medical Center DISCLOSURES I am not being paid by any entity to endorse a specific product. Any mention of brand
Transplant Immunosuppression and Prophylaxis Sarah Fitz, APN, MSN, ACNP-BC Loyola University Medical Center DISCLOSURES I am not being paid by any entity to endorse a specific product. Any mention of brand
Post Transplant Immunosuppression: Consideration for Primary Care. Sameh Abul-Ezz, M.D., Dr.P.H.
 Post Transplant Immunosuppression: Consideration for Primary Care Sameh Abul-Ezz, M.D., Dr.P.H. Objectives Discuss the commonly used immunosuppressive medications and what you need to know to care for
Post Transplant Immunosuppression: Consideration for Primary Care Sameh Abul-Ezz, M.D., Dr.P.H. Objectives Discuss the commonly used immunosuppressive medications and what you need to know to care for
Better than Google- Click on Immunosuppression Renal Transplant. David Landsberg Oct
 Better than Google- Click on Immunosuppression Renal Transplant David Landsberg Oct 3 2008 OUTLINE History of Immunosuppression Trends in Immunosupression FK vs CYA Steroid Minimization CNI Avoidance Sirolimus
Better than Google- Click on Immunosuppression Renal Transplant David Landsberg Oct 3 2008 OUTLINE History of Immunosuppression Trends in Immunosupression FK vs CYA Steroid Minimization CNI Avoidance Sirolimus
Immunosuppressant medicines have allowed patients
 48 Clinical Pharmacist February 2010 Vol 2 Patients who tolerate a transplanted organ without the need for pharmacological intervention are few and far between. Several immunosuppressants can be used to
48 Clinical Pharmacist February 2010 Vol 2 Patients who tolerate a transplanted organ without the need for pharmacological intervention are few and far between. Several immunosuppressants can be used to
Why Do We Need New Immunosuppressive Agents
 Why Do We Need New Immunosuppressive Agents 1 Reducing acute rejection rates has not transplanted into better long-term graft survival Incidence of early acute rejection episodes by era Relative risk for
Why Do We Need New Immunosuppressive Agents 1 Reducing acute rejection rates has not transplanted into better long-term graft survival Incidence of early acute rejection episodes by era Relative risk for
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 30 November 2011
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 30 November 2011 NULOJIX 250 mg, powder for concentrate for solution for infusion B/1 (CIP code: 580 415-7) B/2 (CIP
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 30 November 2011 NULOJIX 250 mg, powder for concentrate for solution for infusion B/1 (CIP code: 580 415-7) B/2 (CIP
It s just not that into you:
 CSHP Clinical Symposium - It s just not that into you: The no-excuses truth to understanding rejection and transplant pharmacology Erica D. Greanya, PharmD Clinical Pharmacy Specialist Solid Organ Transplantation
CSHP Clinical Symposium - It s just not that into you: The no-excuses truth to understanding rejection and transplant pharmacology Erica D. Greanya, PharmD Clinical Pharmacy Specialist Solid Organ Transplantation
Literature Review: Transplantation July 2010-June 2011
 Literature Review: Transplantation July 2010-June 2011 James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Kidney Transplant Top 10 List: July Kidney
Literature Review: Transplantation July 2010-June 2011 James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Kidney Transplant Top 10 List: July Kidney
TRANSPLANT IMMUNOLOGY. Shiv Pillai Ragon Institute of MGH, MIT and Harvard
 TRANSPLANT IMMUNOLOGY Shiv Pillai Ragon Institute of MGH, MIT and Harvard Outline MHC / HLA Direct vs indirect allorecognition Alloreactive cells: where do they come from? Rejection and Immunosuppression
TRANSPLANT IMMUNOLOGY Shiv Pillai Ragon Institute of MGH, MIT and Harvard Outline MHC / HLA Direct vs indirect allorecognition Alloreactive cells: where do they come from? Rejection and Immunosuppression
Solid Organ Transplantation
 LOGO Solid Organ Transplantation Dr. Mohammad Taraz Clinical Pharmacist June 2011 2 Introduction Solid organ transplantation is a well accepted therapeutic option for patients with end-stage kidney, liver,
LOGO Solid Organ Transplantation Dr. Mohammad Taraz Clinical Pharmacist June 2011 2 Introduction Solid organ transplantation is a well accepted therapeutic option for patients with end-stage kidney, liver,
Medications in the Solid Organ Transplant Recipient
 Medications in the Solid Organ Transplant Recipient Monica Morgan, PharmD Transplant Pharmacist UT Southwestern Medical Center Solid Organ Transplant Program Objectives To describe the typical medications
Medications in the Solid Organ Transplant Recipient Monica Morgan, PharmD Transplant Pharmacist UT Southwestern Medical Center Solid Organ Transplant Program Objectives To describe the typical medications
BK virus infection in renal transplant recipients: single centre experience. Dr Wong Lok Yan Ivy
 BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
Why we need a new paradigm in immunosuppression USHERING A NEW ERA OF IMMUNOSUPPRESSION. Causes of death and graft loss after kidney transplantation
 USHERING A NEW ERA OF IMMUNOSUPPRESSION Flavio Vincenti 45 35 AR 3 (%) 25 15 5 35.7 Why we need a new paradigm in immunosuppression Incidence of early acute rejection episodes ( 6 months) 43.7 27.4 17.9
USHERING A NEW ERA OF IMMUNOSUPPRESSION Flavio Vincenti 45 35 AR 3 (%) 25 15 5 35.7 Why we need a new paradigm in immunosuppression Incidence of early acute rejection episodes ( 6 months) 43.7 27.4 17.9
Immunosuppressive therapy for graft-versus-host disease. Mohamad Mohty Institut Paoli-Calmettes, Marseille
 Immunosuppressive therapy for graft-versus-host disease Mohamad Mohty Institut Paoli-Calmettes, Marseille Survival according to GVHD grade (Joint SFGM-TC, DFCI and IBMTR data; N=607) Cahn et al., Blood
Immunosuppressive therapy for graft-versus-host disease Mohamad Mohty Institut Paoli-Calmettes, Marseille Survival according to GVHD grade (Joint SFGM-TC, DFCI and IBMTR data; N=607) Cahn et al., Blood
Innovation In Transplantation:
 Innovation In Transplantation: Improving outcomes Thomas C. Pearson Department of Surgery Emory Transplant Center CHOA Symposium October 22, 2016 Disclosures Belatacept preclinical and clinical trial were
Innovation In Transplantation: Improving outcomes Thomas C. Pearson Department of Surgery Emory Transplant Center CHOA Symposium October 22, 2016 Disclosures Belatacept preclinical and clinical trial were
Immunosuppression: evolution in practice and trends,
 American Journal of Transplantation 25; 5 (Part 2): 874 886 Blackwell Munksgaard Blackwell Munksgaard 25 Immunosuppression: evolution in practice and trends, 1993 23 Ron Shapiro a,, James B. Young b, Edgar
American Journal of Transplantation 25; 5 (Part 2): 874 886 Blackwell Munksgaard Blackwell Munksgaard 25 Immunosuppression: evolution in practice and trends, 1993 23 Ron Shapiro a,, James B. Young b, Edgar
Chapter 22: Hematological Complications
 Chapter 22: Hematological Complications 22.1: Perform a complete blood count at least (Not Graded): daily for 7 days, or until hospital discharge, whichever is earlier; two to three times per week for
Chapter 22: Hematological Complications 22.1: Perform a complete blood count at least (Not Graded): daily for 7 days, or until hospital discharge, whichever is earlier; two to three times per week for
Immunopathology of T cell mediated rejection
 Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham
 Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham Disclosure Employee: CTI Clinical Trials and Consulting
Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham Disclosure Employee: CTI Clinical Trials and Consulting
Renal Transplant. Tony Chacon. Program Head BCIT Nephrology Nursing Program.
 Renal Transplant Tony Chacon Program Head BCIT Nephrology Nursing Program Email: tony_chacon@bcit.ca Summary of CNA Renal Transplant Competencies Potential contraindications to renal transplant. Assessment/selection
Renal Transplant Tony Chacon Program Head BCIT Nephrology Nursing Program Email: tony_chacon@bcit.ca Summary of CNA Renal Transplant Competencies Potential contraindications to renal transplant. Assessment/selection
Tolerance Induction in Transplantation
 Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
Potential Catalysts in Therapeutics
 LIVER TRANSPLANTATION 20:S22 S31, 2014 SUPPLEMENT Potential Catalysts in Therapeutics Bruce A. Luxon Division of Gastroenterology-Hepatology, University of Iowa, Iowa City, IA Received July 23, 2014; accepted
LIVER TRANSPLANTATION 20:S22 S31, 2014 SUPPLEMENT Potential Catalysts in Therapeutics Bruce A. Luxon Division of Gastroenterology-Hepatology, University of Iowa, Iowa City, IA Received July 23, 2014; accepted
Transplant Immunosuppression in 2017 Hepatobiliary Liver Transplant Symposium 2017
 Transplant Immunosuppression in 2017 Hepatobiliary Liver Transplant Symposium 2017 Dr AJ Terblanche Paediatric Gastroenterology and Hepatology Unit, SBAH Paediatric Transplant Unit Wits Donald Gordon Medical
Transplant Immunosuppression in 2017 Hepatobiliary Liver Transplant Symposium 2017 Dr AJ Terblanche Paediatric Gastroenterology and Hepatology Unit, SBAH Paediatric Transplant Unit Wits Donald Gordon Medical
Kidney Transplant. November 4 th, 2016
 Kidney Transplant November 4 th, 2016 Brad West, MD, FACP Medical Director of Transplant Services, Memorial Medical Center Chairman Department of Nephrology, Springfield Clinic 1 Adjusted survival: 1993-1997
Kidney Transplant November 4 th, 2016 Brad West, MD, FACP Medical Director of Transplant Services, Memorial Medical Center Chairman Department of Nephrology, Springfield Clinic 1 Adjusted survival: 1993-1997
Solid Organ Transplantation 1. Chapter 55. Solid Organ Transplant, Self-Assessment Questions
 Solid Organ Transplantation 1 Chapter 55. Solid Organ Transplant, Self-Assessment Questions Questions 1 to 9 are related to the following case: A 38-year-old white man is scheduled to receive a living-unrelated
Solid Organ Transplantation 1 Chapter 55. Solid Organ Transplant, Self-Assessment Questions Questions 1 to 9 are related to the following case: A 38-year-old white man is scheduled to receive a living-unrelated
Intruduction PSI MODE OF ACTION AND PHARMACOKINETICS
 Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta482
 Immunosuppressive e therapy for kidney transplant in children and young people Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta482 NICE 2018. All rights reserved. Subject
Immunosuppressive e therapy for kidney transplant in children and young people Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta482 NICE 2018. All rights reserved. Subject
Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant
 SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham
 What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham SYMPHONY Study Ekberg et al. NEJM 2008 Excluded: DCD kidneys; CIT>30hours;
What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham SYMPHONY Study Ekberg et al. NEJM 2008 Excluded: DCD kidneys; CIT>30hours;
Divya Jain Arwindekar, DO Transplant Nephrologist Advocate Christ Medical Center & Associates in Nephrology
 Divya Jain Arwindekar, DO Transplant Nephrologist Advocate Christ Medical Center & Associates in Nephrology Not a cure to kidney disease, but it is a very effective treatment Patients still have chronic
Divya Jain Arwindekar, DO Transplant Nephrologist Advocate Christ Medical Center & Associates in Nephrology Not a cure to kidney disease, but it is a very effective treatment Patients still have chronic
Transplant Overview. Timothy J. Schroeder President and CEO CTI Clinical Trial and Consulting Services November 10, 2005
 Transplant Overview Timothy J. Schroeder President and CEO CTI Clinical Trial and Consulting Services November 10, 2005 CTI Clinical Trial and Consulting Services Drug Development Company focused in key
Transplant Overview Timothy J. Schroeder President and CEO CTI Clinical Trial and Consulting Services November 10, 2005 CTI Clinical Trial and Consulting Services Drug Development Company focused in key
2017 CST-Astellas Canadian Transplant Fellows Symposium. Management of Renal Dysfunction in Extra Renal Transplants
 2017 CST-Astellas Canadian Transplant Fellows Symposium Management of Renal Dysfunction in Extra Renal Transplants Jeffrey Schiff, MD Dr. Jeffrey Schiff is an Assistant Professor of Medicine at the University
2017 CST-Astellas Canadian Transplant Fellows Symposium Management of Renal Dysfunction in Extra Renal Transplants Jeffrey Schiff, MD Dr. Jeffrey Schiff is an Assistant Professor of Medicine at the University
Post Operative Management in Heart Transplant นพ พ ชร อ องจร ต ศ ลยศาสตร ห วใจและทรวงอก จ ฬาลงกรณ
 Post Operative Management in Heart Transplant นพ พ ชร อ องจร ต ศ ลยศาสตร ห วใจและทรวงอก จ ฬาลงกรณ Art of Good Cooking Good Ingredient Good donor + OK recipient Good technique Good team Good timing Good
Post Operative Management in Heart Transplant นพ พ ชร อ องจร ต ศ ลยศาสตร ห วใจและทรวงอก จ ฬาลงกรณ Art of Good Cooking Good Ingredient Good donor + OK recipient Good technique Good team Good timing Good
Immunosuppression for pediatric cardiac transplantation in the modern era
 Ž. Progress in Pediatric Cardiology 11 2000 115 129 Immunosuppression for pediatric cardiac transplantation in the modern era Bill A. Pietra, Mark M. Boucek Department of Pediatrics, Uni ersity of Colorado
Ž. Progress in Pediatric Cardiology 11 2000 115 129 Immunosuppression for pediatric cardiac transplantation in the modern era Bill A. Pietra, Mark M. Boucek Department of Pediatrics, Uni ersity of Colorado
American Journal of Transplantation 2009; 9 (Suppl 3): S1 S157 Wiley Periodicals Inc.
: S1 S157 Wiley Periodicals Inc.") American Journal of Transplantation 2009; 9 (Suppl 3): S1 S157 Wiley Periodicals Inc. 2009 The Authors Journal compilation 2009 The American Society of Transplantation and the American Society of Transplant
American Journal of Transplantation 2009; 9 (Suppl 3): S1 S157 Wiley Periodicals Inc. 2009 The Authors Journal compilation 2009 The American Society of Transplantation and the American Society of Transplant
Belatacept: An Opportunity to Personalize Immunosuppression? Andrew Adams MD/PhD Emory Transplant Center
 Belatacept: An Opportunity to Personalize Immunosuppression? Andrew Adams MD/PhD Emory Transplant Center Disclosure Research Funding from BMS. Learning Objectives -Define belatacept-resistant rejection
Belatacept: An Opportunity to Personalize Immunosuppression? Andrew Adams MD/PhD Emory Transplant Center Disclosure Research Funding from BMS. Learning Objectives -Define belatacept-resistant rejection
Chronic Kidney Disease & Transplantation. Paediatrics : 2004 FRACP
 Chronic Kidney Disease & Transplantation Paediatrics : 2004 FRACP ANZDATA Registry Mode of First Treatment - Paediatric 14 12 10 8 6 4 2 0 0-4 y 5-9 y 10-14 y 15-19 y Hospital CAPD Hospital HD Hospital
Chronic Kidney Disease & Transplantation Paediatrics : 2004 FRACP ANZDATA Registry Mode of First Treatment - Paediatric 14 12 10 8 6 4 2 0 0-4 y 5-9 y 10-14 y 15-19 y Hospital CAPD Hospital HD Hospital
Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial
: a randomised trial") Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial Journal club Feb 2014 Background and Rationale Despite substantial
Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial Journal club Feb 2014 Background and Rationale Despite substantial
Transplantation Immunology
 Transplantation Immunology Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation Children s Hospital New York Presbyterian
Transplantation Immunology Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation Children s Hospital New York Presbyterian
Transplantation Immunology
 Transplantation Immunology MHC Restricted Allograft Rejection Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation
Transplantation Immunology MHC Restricted Allograft Rejection Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation
Case Report Beneficial Effect of Conversion to Belatacept in Kidney-Transplant Patients with a Low Glomerular-Filtration Rate
 Case Reports in Transplantation, Article ID 190516, 4 pages http://dx.doi.org/10.1155/2014/190516 Case Report Beneficial Effect of Conversion to Belatacept in Kidney-Transplant Patients with a Low Glomerular-Filtration
Case Reports in Transplantation, Article ID 190516, 4 pages http://dx.doi.org/10.1155/2014/190516 Case Report Beneficial Effect of Conversion to Belatacept in Kidney-Transplant Patients with a Low Glomerular-Filtration
KIDNEY TRANSPLANTATION FOR THE INTERNIST. Marc Richards MD South Florida Kidney Disease and Hypertension Specialists BRRH Grand Rounds 5.8.
 KIDNEY TRANSPLANTATION FOR THE INTERNIST Marc Richards MD South Florida Kidney Disease and Hypertension Specialists BRRH Grand Rounds 5.8.2018 Goal of Lecture: OUTLINE CKD -> ESRD Workup for Transplant
KIDNEY TRANSPLANTATION FOR THE INTERNIST Marc Richards MD South Florida Kidney Disease and Hypertension Specialists BRRH Grand Rounds 5.8.2018 Goal of Lecture: OUTLINE CKD -> ESRD Workup for Transplant
Literature Review Transplantation
 Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
CAMPATH INDUCTION IN RENAL TRANSPLANTATION. by Kakit Edmond Chan. Thesis is submitted for the degree of MD [Res] of Imperial College London
![CAMPATH INDUCTION IN RENAL TRANSPLANTATION. by Kakit Edmond Chan. Thesis is submitted for the degree of MD [Res] of Imperial College London](/thumbs/80/80968355.jpg "CAMPATH INDUCTION IN RENAL TRANSPLANTATION. by Kakit Edmond Chan. Thesis is submitted for the degree of MD [Res] of Imperial College London") CAMPATH INDUCTION IN RENAL TRANSPLANTATION by Kakit Edmond Chan Thesis is submitted for the degree of MD [Res] of Imperial College London Department of Medicine Imperial College London kkchan 1 Abstract
CAMPATH INDUCTION IN RENAL TRANSPLANTATION by Kakit Edmond Chan Thesis is submitted for the degree of MD [Res] of Imperial College London Department of Medicine Imperial College London kkchan 1 Abstract
Chronic Kidney Disease (CKD) Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.
 Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.") Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol
 Josep M. Campistol") Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta481
 Immunosuppressive e therapy for kidney transplant in adults Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta481 NICE 2018. All rights reserved. Subject to Notice of rights
Immunosuppressive e therapy for kidney transplant in adults Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta481 NICE 2018. All rights reserved. Subject to Notice of rights
HLA and Non-HLA Antibodies in Transplantation and their Management
 HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
Atgam (lymphocyte immune globulin, anti-thymocyte globulin [equine])
![Atgam (lymphocyte immune globulin, anti-thymocyte globulin [equine])](/thumbs/83/88936551.jpg "Atgam (lymphocyte immune globulin, anti-thymocyte globulin [equine])") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.20.01 Subject: Atgam Page: 1 of 5 Last Review Date: June 24, 2016 Atgam Description Atgam (lymphocyte
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.20.01 Subject: Atgam Page: 1 of 5 Last Review Date: June 24, 2016 Atgam Description Atgam (lymphocyte
Kidney Transplantation: What Pharmacists & Technicians Need to Know
 Kidney Transplantation: What Pharmacists & Technicians Need to Know Amanda J. Condon, PharmD, BCPS Solid Organ Transplant Pharmacist University of New Mexico Hospitals Objectives PHARMACIST Describe mechanisms
Kidney Transplantation: What Pharmacists & Technicians Need to Know Amanda J. Condon, PharmD, BCPS Solid Organ Transplant Pharmacist University of New Mexico Hospitals Objectives PHARMACIST Describe mechanisms
Strategies for Desensitization
 Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
PanGraf Tacrolimus Capsules 0.5 / 1.0 / 5.0
 For the use of a Nephrologist / Transplant Surgeon or a Hospital or a Laboratory only PanGraf Tacrolimus Capsules 0.5 / 1.0 / 5.0 DESCRIPTION Tacrolimus is a macrolide lactone with potent immunosuppressive
For the use of a Nephrologist / Transplant Surgeon or a Hospital or a Laboratory only PanGraf Tacrolimus Capsules 0.5 / 1.0 / 5.0 DESCRIPTION Tacrolimus is a macrolide lactone with potent immunosuppressive
Immunosuppressive therapy in liver transplantation
 Journal of Hepatology 39 (2003) 664 678 Short Reviews on Liver Transplantation Associate Editor: Didier Samuel Immunosuppressive therapy in liver transplantation Filomena Conti 1, Emmanuel Morelon 2, Yvon
Journal of Hepatology 39 (2003) 664 678 Short Reviews on Liver Transplantation Associate Editor: Didier Samuel Immunosuppressive therapy in liver transplantation Filomena Conti 1, Emmanuel Morelon 2, Yvon
For Immediate Release Contacts: Jenny Keeney Astellas US LLC (847)
") For Immediate Release Contacts: Jenny Keeney Astellas US LLC (847) 317-5405 Lauren McDonnell GolinHarris (312) 729-4233 ASTELLAS RECEIVES FDA APPROVAL FOR USE OF PROGRAF (TACROLIMUS) IN CONJUNCTION WITH
For Immediate Release Contacts: Jenny Keeney Astellas US LLC (847) 317-5405 Lauren McDonnell GolinHarris (312) 729-4233 ASTELLAS RECEIVES FDA APPROVAL FOR USE OF PROGRAF (TACROLIMUS) IN CONJUNCTION WITH
Date: 23 June Context and policy issues:
 Title: Basiliximab for Immunosuppression During a Calcineurin Inhibitor Holiday in Renal Transplant Patients with Acute Renal Dysfunction: Guidelines for Use and a Clinical and Cost-Effectiveness Review
Title: Basiliximab for Immunosuppression During a Calcineurin Inhibitor Holiday in Renal Transplant Patients with Acute Renal Dysfunction: Guidelines for Use and a Clinical and Cost-Effectiveness Review
Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function
 ArtIcle Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function Guodong Chen, 1 Jingli Gu, 2 Jiang Qiu, 1 Changxi
ArtIcle Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function Guodong Chen, 1 Jingli Gu, 2 Jiang Qiu, 1 Changxi
Primary Nephrotic Syndrome. Mao Jianhua, Department of Nephrology, The Children s Hospital of Zhejiang University School of Medicine
 Primary Nephrotic Syndrome Mao Jianhua, Department of Nephrology, The Children s Hospital of Zhejiang University School of Medicine Introduction Nephrotic syndrome is a group of symptoms including proteins
Primary Nephrotic Syndrome Mao Jianhua, Department of Nephrology, The Children s Hospital of Zhejiang University School of Medicine Introduction Nephrotic syndrome is a group of symptoms including proteins
The common premise for immunosuppressive
 therapy update Current trends in immunosuppressive therapies for renal transplant recipients The common premise for immunosuppressive therapies in kidney transplantation is to use multiple agents to work
therapy update Current trends in immunosuppressive therapies for renal transplant recipients The common premise for immunosuppressive therapies in kidney transplantation is to use multiple agents to work
Lymphangioleiomyomatosis Patients:
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use RAPAMUNE safely and effectively. See full prescribing information for RAPAMUNE. RAPAMUNE (sirolimus)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use RAPAMUNE safely and effectively. See full prescribing information for RAPAMUNE. RAPAMUNE (sirolimus)
Mycophenolate Mofetil
 Mycophenolate Mofetil Cynthia L. Chen, MD The Permanente Medical Group, Northern California Diablo Service Area February 17, 2018 January 23, 2018 2011 Kaiser Foundation Health Plan, Inc. For internal
Mycophenolate Mofetil Cynthia L. Chen, MD The Permanente Medical Group, Northern California Diablo Service Area February 17, 2018 January 23, 2018 2011 Kaiser Foundation Health Plan, Inc. For internal
Immunopharmacology: Immunosuppression in Organ Transplanation
 Immunopharmacology: Immunosuppression in Organ Transplanation Prof D. A. Joyce Pharm 3320/3321 Organ Transplants, Australia Organ Donors (2013) Kidney 630 Liver 248 Heart 77 Lung 167 Pancreas 33 Bone Marrow
Immunopharmacology: Immunosuppression in Organ Transplanation Prof D. A. Joyce Pharm 3320/3321 Organ Transplants, Australia Organ Donors (2013) Kidney 630 Liver 248 Heart 77 Lung 167 Pancreas 33 Bone Marrow
Image: Bruce Wetzel - Harry Schaefer, Wikimedia Commons
 Image: Bruce Wetzel - Harry Schaefer, Wikimedia Commons Martin lversen Section of Lung Transplantation Rigshospitalet Copenhagen Denmark martin.iversen@dadlnet.dk Immunosuppression for the non-transplant
Image: Bruce Wetzel - Harry Schaefer, Wikimedia Commons Martin lversen Section of Lung Transplantation Rigshospitalet Copenhagen Denmark martin.iversen@dadlnet.dk Immunosuppression for the non-transplant
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies
 Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
The 1990s have seen major steps in the dissection of basic mechanisms
 Immunosuppressive Therapy and Protocols Angelo M. de Mattos The 1990s have seen major steps in the dissection of basic mechanisms of allorecognition, and renal graft survival has achieved unprecedented
Immunosuppressive Therapy and Protocols Angelo M. de Mattos The 1990s have seen major steps in the dissection of basic mechanisms of allorecognition, and renal graft survival has achieved unprecedented
Class I Ag processing. TAP= transporters associated with antigen processing Transport peptides into ER
 Antigen processing Class I Ag processing TAP= transporters associated with antigen processing Transport peptides into ER Proteosome degrades cytosolic proteins Large, multi-subunit complex Degrades foreign
Antigen processing Class I Ag processing TAP= transporters associated with antigen processing Transport peptides into ER Proteosome degrades cytosolic proteins Large, multi-subunit complex Degrades foreign
Nephrology Grand Rounds
 Nephrology Grand Rounds PTLD in Kidney Transplantation Charles Le University of Colorado 6/15/12 Objectives Background Pathogenesis Epidemiology and Clinical Manifestation Incidence Risk Factors CNS Lymphoma
Nephrology Grand Rounds PTLD in Kidney Transplantation Charles Le University of Colorado 6/15/12 Objectives Background Pathogenesis Epidemiology and Clinical Manifestation Incidence Risk Factors CNS Lymphoma
PUO in the Immunocompromised Host: CMV and beyond
 PUO in the Immunocompromised Host: CMV and beyond PUO in the immunocompromised host: role of viral infections Nature of host defect T cell defects Underlying disease Treatment Nature of clinical presentation
PUO in the Immunocompromised Host: CMV and beyond PUO in the immunocompromised host: role of viral infections Nature of host defect T cell defects Underlying disease Treatment Nature of clinical presentation
Belatacept: An Update of Ongoing Clinical Trials
 Belatacept: An Update of Ongoing Clinical Trials Michael D. Rizzari, MD University of Wisconsin Madison School of Medicine and Public Health, Madison, Wisconsin Abstract Belatacept is a fusion protein
Belatacept: An Update of Ongoing Clinical Trials Michael D. Rizzari, MD University of Wisconsin Madison School of Medicine and Public Health, Madison, Wisconsin Abstract Belatacept is a fusion protein
This study is currently recruiting participants.
 A Two Part, Phase 1/2, Safety, PK and PD Study of TOL101, an Anti-TCR Monoclonal Antibody for Prophylaxis of Acute Organ Rejection in Patients Receiving Renal Transplantation This study is currently recruiting
A Two Part, Phase 1/2, Safety, PK and PD Study of TOL101, an Anti-TCR Monoclonal Antibody for Prophylaxis of Acute Organ Rejection in Patients Receiving Renal Transplantation This study is currently recruiting
3/6/2017. Treatment of Detected Antibodies. I have financial relationship(s) with: Thoratec/St. Jude/Abbott Consultant CareDx Consultant/Speaker
 with: Thoratec/St. Jude/Abbott Consultant CareDx Consultant/Speaker") Treatment of Detected Antibodies Sean Pinney, MD Director, Advanced Heart Failure & Transplantation Mount Sinai Hospital New York, NY Sean Pinney, MD Associate Professor of Medicine Icahn School of Medicine
Treatment of Detected Antibodies Sean Pinney, MD Director, Advanced Heart Failure & Transplantation Mount Sinai Hospital New York, NY Sean Pinney, MD Associate Professor of Medicine Icahn School of Medicine
T Lymphocyte Activation and Costimulation. FOCiS. Lecture outline
 1 T Lymphocyte Activation and Costimulation Abul K. Abbas, MD UCSF FOCiS 2 Lecture outline T cell activation Costimulation, the B7:CD28 family Inhibitory receptors of T cells Targeting costimulators for
1 T Lymphocyte Activation and Costimulation Abul K. Abbas, MD UCSF FOCiS 2 Lecture outline T cell activation Costimulation, the B7:CD28 family Inhibitory receptors of T cells Targeting costimulators for
Mycophenolate Mofetil (MMF)
") SCG: For Transplant patients The following guidelines are designed to provide information relating to mycophenolate mofetil and to outline the responsibilities of the primary and secondary care teams in
SCG: For Transplant patients The following guidelines are designed to provide information relating to mycophenolate mofetil and to outline the responsibilities of the primary and secondary care teams in
Proton Pump Inhibitors do not Interact with the Immunosuppressant Enteric-Coated Mycophenolate Sodium
 Proton Pump Inhibitors do not Interact with the Immunosuppressant Enteric-Coated Mycophenolate Sodium S. Kofler, C. Wolf, Z. Sisic, J. Behr, M. Vogeser, M. Shipkova, B. Meiser, G. Steinbeck, B. Reichart,
Proton Pump Inhibitors do not Interact with the Immunosuppressant Enteric-Coated Mycophenolate Sodium S. Kofler, C. Wolf, Z. Sisic, J. Behr, M. Vogeser, M. Shipkova, B. Meiser, G. Steinbeck, B. Reichart,
Adverse effects of Immunotherapy. Asha Nayak M.D
 Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
FIT Board Review Corner March 2016
 FIT Board Review Corner March 2016 Welcome to the FIT Board Review Corner, prepared by Sarah Spriet, DO, and Tammy Peng, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
FIT Board Review Corner March 2016 Welcome to the FIT Board Review Corner, prepared by Sarah Spriet, DO, and Tammy Peng, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
What Every Non-hepatologist Should Know About Caring For Transplanted Patients. Gia Tyson, MD, MPH Ochsner Health System March 31, 2017
 What Every Non-hepatologist Should Know About Caring For Transplanted Patients Gia Tyson, MD, MPH Ochsner Health System March 31, 2017 Agenda Liver transplant statistics Post-transplant patient information
What Every Non-hepatologist Should Know About Caring For Transplanted Patients Gia Tyson, MD, MPH Ochsner Health System March 31, 2017 Agenda Liver transplant statistics Post-transplant patient information
Dr. Yi-chi M. Kong August 8, 2001 Benjamini. Ch. 19, Pgs Page 1 of 10 TRANSPLANTATION
 Benjamini. Ch. 19, Pgs 379-399 Page 1 of 10 TRANSPLANTATION I. KINDS OF GRAFTS II. RELATIONSHIPS BETWEEN DONOR AND RECIPIENT Benjamini. Ch. 19, Pgs 379-399 Page 2 of 10 II.GRAFT REJECTION IS IMMUNOLOGIC
Benjamini. Ch. 19, Pgs 379-399 Page 1 of 10 TRANSPLANTATION I. KINDS OF GRAFTS II. RELATIONSHIPS BETWEEN DONOR AND RECIPIENT Benjamini. Ch. 19, Pgs 379-399 Page 2 of 10 II.GRAFT REJECTION IS IMMUNOLOGIC
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
European Risk Management Plan. Measures impairment. Retreatment after Discontinuation
 European Risk Management Plan Table 6.1.4-1: Safety Concern 55024.1 Summary of Risk Minimization Measures Routine Risk Minimization Measures Additional Risk Minimization Measures impairment. Retreatment
European Risk Management Plan Table 6.1.4-1: Safety Concern 55024.1 Summary of Risk Minimization Measures Routine Risk Minimization Measures Additional Risk Minimization Measures impairment. Retreatment
BK Viral Infection and Malignancy in Renal Transplantation ~A Case History~
 BK Viral Infection and Malignancy in Renal Transplantation ~A Case History~ Mariko Toyoda, MD Department of Nephrology, Japanese Red Cross Kumamoto Hospital Statement of Disclosure The author does not
BK Viral Infection and Malignancy in Renal Transplantation ~A Case History~ Mariko Toyoda, MD Department of Nephrology, Japanese Red Cross Kumamoto Hospital Statement of Disclosure The author does not
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
Pancreas and Pancreas-Kidney Transplantation By: Kay R. Brown, CLCP
 Pancreas and Pancreas-Kidney Transplantation By: Kay R. Brown, CLCP Pancreas transplant recipients are usually under age 50. The majority of pancreas transplants are performed on diabetics, who are generally
Pancreas and Pancreas-Kidney Transplantation By: Kay R. Brown, CLCP Pancreas transplant recipients are usually under age 50. The majority of pancreas transplants are performed on diabetics, who are generally
4/28/2016. Disclosure. Management of Pediatric Hematopoietic Stem-Cell Transplant Complications. Objectives - Technician. Objectives - Pharmacist
 Disclosure Management of Pediatric Hematopoietic Stem-Cell Transplant Complications Jenna Bender has no actual or potential conflicts of interest to report Off-label use of medication will be discussed
Disclosure Management of Pediatric Hematopoietic Stem-Cell Transplant Complications Jenna Bender has no actual or potential conflicts of interest to report Off-label use of medication will be discussed
Desensitization in Kidney Transplant. James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver
 Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
Kidneytransplant pathologyrelatedto immunosuppressiveagents
 Kidneytransplant pathologyrelatedto immunosuppressiveagents Helmut Hopfer Pathologie Women, 53 years old. 16 months after kidney transplantation for diabetic nephropathy. Metabolicsyndromeandcoronaryheartdisease.
Kidneytransplant pathologyrelatedto immunosuppressiveagents Helmut Hopfer Pathologie Women, 53 years old. 16 months after kidney transplantation for diabetic nephropathy. Metabolicsyndromeandcoronaryheartdisease.
Objectives. The Immune Response. Mechanisms of T-Cell Activation. Balancing Act of Transplant 4/22/2015. Maintenance Immunosuppression
 Objectives Medication Needs of Transplant Recipients: Protecting the Gift of Life Adam Diamond, PharmD, BCPS Solid Organ Transplant Clinical Pharmacy Specialist Lahey Hospital and Medical Center Christin
Objectives Medication Needs of Transplant Recipients: Protecting the Gift of Life Adam Diamond, PharmD, BCPS Solid Organ Transplant Clinical Pharmacy Specialist Lahey Hospital and Medical Center Christin
Transplant Primer for ICU Pharmacists
 HISTORICAL OVERVIEW Margaret Fernandez, PharmD, BCPS Transplant Primer for ICU Pharmacists Jackson Memorial Hospital Miami, Florida First long term surviving kidney transplant performed in identical twins
HISTORICAL OVERVIEW Margaret Fernandez, PharmD, BCPS Transplant Primer for ICU Pharmacists Jackson Memorial Hospital Miami, Florida First long term surviving kidney transplant performed in identical twins
Evolving therapies for posterior uveitis. Infliximab (Remicade) Infliximab: pharmacology. FDA-approved monoclonal antibody therapy Target
 Infliximab: pharmacology. FDA-approved monoclonal antibody therapy Target") Evolving therapies for posterior uveitis Sam Dahr, M.D. September 17, 2005 Midwest Ophthalmology Conference Infliximab (Remicade) FDA approved for Crohn s disease, rheumatoid arthritis, and psoriatic arthritis
Evolving therapies for posterior uveitis Sam Dahr, M.D. September 17, 2005 Midwest Ophthalmology Conference Infliximab (Remicade) FDA approved for Crohn s disease, rheumatoid arthritis, and psoriatic arthritis
ACTEMRA (tocilizumab)
") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 1. Active Polyarticular Juvenile Idiopathic Arthritis (PJIA) b. Patient has an intolerance or has experienced
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 1. Active Polyarticular Juvenile Idiopathic Arthritis (PJIA) b. Patient has an intolerance or has experienced
ASSESSMENT OF THE PAEDIATRIC NEEDS IMMUNOLOGY DISCLAIMER
 European Medicines Agency Evaluation of Medicines for Human Use London, September 2006 Doc. Ref.: EMEA/381922/2006 ASSESSMENT OF THE PAEDIATRIC NEEDS IMMUNOLOGY DISCLAIMER The Paediatric Working Party
European Medicines Agency Evaluation of Medicines for Human Use London, September 2006 Doc. Ref.: EMEA/381922/2006 ASSESSMENT OF THE PAEDIATRIC NEEDS IMMUNOLOGY DISCLAIMER The Paediatric Working Party
15 Immunodeficiencies
 15 Immunodeficiencies A. Acquired causes of immunodeficiencies 1. Environmental (UV irradiation) 2. Drug induced (immunosuppressants) 3. non-hiv Viral (measles virus) Dr. Andrea Hubbard School of Pharmacy
15 Immunodeficiencies A. Acquired causes of immunodeficiencies 1. Environmental (UV irradiation) 2. Drug induced (immunosuppressants) 3. non-hiv Viral (measles virus) Dr. Andrea Hubbard School of Pharmacy
MabThera. SC. The wait is over. MabThera delivered in just 5 minutes. SC= subcutaneous injection
 MabThera SC. The wait is over. MabThera delivered in just 5 minutes Abbreviated Prescribing Information MabThera 1400 mg solution for subcutaneous (SC) injection (Rituximab) Indications: Indicated in adults
MabThera SC. The wait is over. MabThera delivered in just 5 minutes Abbreviated Prescribing Information MabThera 1400 mg solution for subcutaneous (SC) injection (Rituximab) Indications: Indicated in adults