HIV Treatment: New and Veteran Drugs Classes
|
|
|
- Magdalen McDaniel
- 5 years ago
- Views:
Transcription
1 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013
2 Overview Many excellent antiretroviral agents are available in resource rich settings to treat HIV infected patients These include agents for older and newer drug classes An intimate knowledge of the characteristic of each class and individual drug is crucial for optimal therapeutic decision making Key virological and pharmacological drug characteristics often dictate how these drugs are best chosen and combined
3 What are the Barriers to Successful Antiretroviral Therapy?

4 Characteristics of Antiretroviral Drugs Drug Virus Adherence Pharmacology Potency/Resistant Dosing schedule Adverse events Absorption/metabolism Drug interactions Mechanism of action Concentration Viral mutations
5 Goals for Successful Antiretroviral Therapy Continued suppression of viral replication No or minimal toxicity and adverse events Convenient with no or minimal reduction in quality of life Priority

6 HIV Drug Targets RNA RT RNA DNA RT DNA DNA RNA RNA Provirus Proteins
7 NRTI NRTI RNA RT RNA DNA RT DNA DNA RNA RNA Provirus Proteins
8 NRTI Tenofovir (TDF) Abacavir (ABC) Emtricitabine (FTC) Lamivudine (3TC) Zidovudine (AZT, ZDV) Didanosine (ddi) Stavudine (D4T)
9 NRTI Tenofovir (TDF) Abacavir (ABC) Emtricitabine (FTC) Lamivudine (3TC) Zidovudine (AZT, ZDV) Didanosine (ddi) - Rarely used due to increased toxicity Stavudine (D4T) Rarely used due to increased toxicity
10 NRTI Tenofovir (TDF) Abacavir (ABC) Emtricitabine (FTC) Lamivudine (3TC) Zidovudine (AZT, ZDV)
11 NRTI Tenofovir (TDF) Abacavir (ABC) Emtricitabine (FTC) Lamivudine (3TC) Zidovudine (AZT, ZDV)
12 Cross Resistance Among NRTI Stanford HIV Drug Resistance Database, Robert Shafer PI, January 2012

13 Cross Resistance Among NRTI Stanford HIV Drug Resistance Database, Robert Shafer PI, January 2012
14 HIV Drug Targets NNRTI RNA RT RNA DNA RT DNA DNA RNA RNA Provirus Proteins
15 NNRTI Efavirenz (EFV) Nevirapine (NVP) Etravirine (ETV) Rilpivirine (RPV)
16 Structures of NNRTIs Nevirapine Efavirenz TMC12
17 Cross Resistance Among NNRTI Stanford HIV Drug Resistance Database, Robert Shafer PI, January 2012
18 Resistance to Nevirapine with Single Mutation Increased Fold Change to NVP with Mutation K103N Stanford Resistance Database, Dec 2010

19 Resistance to Efavirenz with Single Mutation Increased Fold Change to EFV with Mutation K103N Stanford Resistance Database, Dec 2010
20 Structures of NNRTIs Nevirapine Efavirenz Etravirine
21 DUET-1 and DUET-2: DRV/r + TMC125 + OBR in Highly Treatment Experienced Patients Screening 6 weeks 600 patients target per trial 48-week treatment period with optional 48-week extension 24-week primary analysis TMC125 + BR* (including DRV/r) Placebo + BR* (including DRV/r) *BR = DRV/r with optimised NRTIs and optional enfuvirtide Follow up 4 weeks Viral load >5,000 HIV-1 RNA copies/ml and stable therapy for 8 weeks 1 NNRTI MU, at screening or in documented historical genotype 3 primary PI mutations at screening Primary endpoint was the proportion of patients achieving viral load <50 HIV-1 RNA copies/ml when all patients had reached Week 24 or discontinued
22 Patients with viral load <50 copies at Week 24 DUET-1 DUET-2 Responders (%) + 95% CI TMC125 + BR (n=304) Placebo + BR (n=308) p= % 39% Responders (%) + 95% CI TMC125 + BR (n=295) Placebo + BR (n=296) p= % 44% Time (weeks) Time (weeks) CI = confidence interval; intent-to-treat (ITT) population; TLOVR = time to loss of virological response imputation algorithm
23 ETR Weighted Score Mutations have accumulative effect Impact on virological response relative to weight of mutation Mutation Weight Y181I 3 Y181V 3 K101P 2.5 L100I 2.5 Y181C 2.5 M230L 2.5 E138A 1.5 V106I 1.5 G190S 1.5 V179F 1.5 V90I 1 V179D 1 K101E 1 K101H 1 A98G 1 V179T 1 G190A 1

24 Relation Between Total Score and Virological Response
25 ETR Weighted Score Mutations have accumulative effect Impact on virological response relative to weight of mutation Mutation Weight Y181I 3 Y181V 3 K101P 2.5 L100I 2.5 Y181C 2.5 M230L 2.5 E138A 1.5 V106I 1.5 G190S 1.5 V179F 1.5 V90I 1 V179D 1 K101E 1 K101H 1 A98G 1 V179T 1 G190A 1
26 Etravirine (TMC 125) and Rilpivirine (TMC 278)
27 Structures of NNRTIs Nevirapine Efavirenz Etravirine TMC125: Molecular flexibility

28 Structures of NNRTIs TMC125 Etravirine Etravirine Rilpivirine
29 Single Tablet Regimen Eviplera (Complera) One pill taken once daily containing: Tenofovir 300 mg Emtricitabine (FTC) 200 mg Rilpivirine 25 mg
30 ECHO and THRIVE: Double-blind, double-dummy studies in treatment-naïve patients 48 weeks primary analysis 96 weeks final analysis ECHO (TMC278-C209) TMC278 25mg qd + TDF/FTC + EFV pbo qd (N=346) N=690 patients 1:1 EFV 600mg qd + TDF/FTC + TMC278 pbo qd (N=344) THRIVE (TMC278-C215) N=678 patients 1:1 TMC278 25mg qd + 2 N(t)RTIs* + EFV pbo qd (N=340) EFV 600mg qd + 2 N(t)RTIs* + TMC278 pbo qd (N=338) *Investigator s choice: TDF/FTC (60%); AZT/3TC (30%); ABC/3TC (10%) Cohen C, et al. HIV Abstract O432
31
32 48 Week Virologic Outcome of Randomized Treatment Rilpivirine % N=686 Efavirenz % N=682 HIV-1 RNA < Virologic failure 13 9 Discontinued study due to adverse event or death Discontinued study for other reasons Missing data 1 <1 Pooled Data from the TMC278-C209 and TMC278-C215 Trials Source: FDA Label May 2011
33 48 Week Virologic Outcome of Randomized Treatment Rilpivirine % N=686 Efavirenz % N=682 HIV-1 RNA < Virologic failure 13 9 Discontinued study due to adverse event or death Discontinued study for other reasons Missing data 1 <1 Pooled Data from the TMC278-C209 and TMC278-C215 Trials Source: FDA Label May 2011
34 48 Week Virologic Outcome of Randomized Treatment Rilpivirine % N=686 Efavirenz % N=682 HIV-1 RNA < Virologic failure 13 9 Discontinued study due to adverse event or death Discontinued study for other reasons Missing data 1 <1 Pooled Data from the TMC278-C209 and TMC278-C215 Trials Source: FDA Label May 2011
35 Selected Treatment-Emergent Adverse Drug Reactions of at least Moderate Intensity* (Grades 2-4) Occurring in at Least 2% of Antiretroviral Treatment- Naïve HIV-1 Infected Adult Subjects (Week 48) Rilpivirine % N=686 Efavirenz % N=682 Nausea 1 3 Abdominal pain 1 2 Vomiting 1 2 Fatigue 1 2 Rash 3 11 Nervous System Headache 3 3 Dizziness 1 7 Psychiatric Disorders Depressive disorders 4 3 Insomnia 3 3 Abnormal dreams 1 4 Pooled Data from the TMC278-C209 and TMC278-C215 Trials Source: FDA Label May 2011
36 Incidence of Depressive Disorders Including:depressed mood, depression, dysphoria, major depression, mood altered, negative thoughts, suicide attempt, suicidal ideation Rilpivirine % N=686 Efavirenz % N=682 Depressive disorders (All severities) Depressive disorders (Grade 3 and 4) Study discontinuation due to depressive disorders Suicide attempt 2 0 Suicide ideation 1 3 Pooled Data from the TMC278-C209 and TMC278-C215 Trials Source: FDA Label May 2011
37 Pooled ECHO and THRIVE: Wk 96 FTC/TDF Dataset VL <50 c/ml by Baseline Viral Load (Snapshot) VL <50 c/ml (%) RPV EFV 74 Overall 100K >100K to 500K >500K Baseline HIV-1 RNA, copies/ml
38 Pooled ECHO and THRIVE: Wk 96 FTC/TDF Dataset VL <50 c/ml by Baseline Viral Load (Snapshot) VL <50 c/ml (%) EFV Overall 100K >100K to 500K >500K Baseline HIV-1 RNA, copies/ml
39 Pooled ECHO and THRIVE: Wk 96 FTC/TDF Dataset VL <50 c/ml by Baseline Viral Load (Snapshot) VL <50 c/ml (%) RPV 74 Overall 100K >100K to 500K 60 >500K Baseline HIV-1 RNA, copies/ml
40 Resistance Among Virological Failures Resistance (Geno + Phen) to study drug Resistance to a background regimen drug Rilpivirine % N=92 Efavirenz % N=60 41 (RPV) 25 (EFV) Pooled Data from the TMC278-C209 and TMC278-C215 Trials Source: FDA Label May 2011
41 FDA Label Update December 2012 The following points should be considered when initiating therapy with Rilpivirine (EDURANT): More rilpivirine treated subjects with HIV-1 RNA greater than 100,000 copies/ml at the start of therapy experienced virologic failure (HIV-1 RNA 50 copies/ml) compared to EDURANT treated subjects with HIV-1 RNA less than or equal to 100,000 copies/ml Regardless of HIV-1 RNA at the start of therapy, more rilpivirine treated subjects with CD4+ cell count less than 200 cells/mm 3 experienced virologic failure compared to EDURANT treated subjects with CD4+ cell count greater than or equal to 200 cells/mm 3 The observed virologic failure rate in rilpivirine treated subjects conferred a higher rate of overall treatment resistance and cross-resistance to the NNRTI class compared to efavirenz More subjects treated with rilpivirine developed tenofovir and lamivudine/emtricitabine associated resistance compared to efavirenz FDA Packet Insert, December 2012

42 Cross Resistance Among NNRTI Stanford HIV Drug Resistance Database, Robert Shafer PI, January 2012
43 Protease Inhibitors Protease inhibitors RNA RT RNA DNA RT DNA DNA RNA RNA Provirus Proteins
44 Protease Inhibitors Atazanvir (ATV ATV/r) Darunavir (DRV DRV/r) Lopinavir (LPV LPV/r) fosamprenavir (fapv fapv/r) Indinavir (IDV IDV/r) Saquinavir (SQV SQV/r) Nelfinavir (NFV) Ritonavir (RTV)
45 Protease Inhibitors Atazanvir (ATV ATV/r) Darunavir (DRV DRV/r) Lopinavir (LPV LPV/r) famp/r No unique benefit higher risk of DRV MU IDV/r No unique benefit higher toxicity SQV/r No unique benefit NFV No unique benefit low genetic barrier RTV No unique benefit high toxicity at 600 x 2 boosting only
46 Protease Inhibitors Atazanvir (ATV ATV/r) Darunavir (DRV DRV/r) Lopinavir (LPV LPV/r)
47 Protease Inhibitors Genetic Barrier to Resistance The key feature of boosted protease inhibitors is their high genetic barrier to resistance This is a function of both virology and pharmacology
48 Genetic Barrier to Resistance: Virology and Pharmacology
 Drug level to inhibit WT")
49 Drug level Minimal Plasma level of drug (Cmin) Drug level to inhibit WT virus
50 Estimating the Barrier to Resistance Minimal Plasma level of drug (Cmin) Drug level to inhibit WT virus
51 Estimating the Barrier to Resistance Minimal Plasma level of drug (Cmin) Drug level to inhibit WT virus
52 Estimating the Barrier to Resistance Minimal Plasma level of drug (Cmin) Is this the clinically relevant Genetic Barrier to Resistance? Drug level to inhibit WT virus
53 Correcting for Protein Binding of Drug in Plasma Minimal Plasma level of drug (Cmin) Drug level to inhibit WT virus
54 Estimating the Barrier to Resistance Minimal Plasma level of drug (Cmin) Drug level to inhibit WT virus corrected for protein binding Drug level to inhibit WT virus
55 How Much Resistance from a Single Mutation to the Drug Minimal Plasma level of drug (Cmin) Drug level to inhibit most potent single mutation to the drug Drug level to inhibit WT virus corrected for protein binding Drug level to inhibit WT virus
56 PI/r Summary Resistance: High genetic barrier to resistance Partial cross-resistance between drugs Good activity Retains relatively good activity when partial resistance present Toxicity: Substantial toxicity (somewhat less with ATV/r 300/100) PK: Fair, once daily dosing possible for most drugs but just barely
57 Integrase Inhibitors RNA RT RNA DNA RT RNA RNA Proteins DNA DNA Provirus Integrase inhibitors
58 Integrase Inhibitor
59 Integrase Inhibitors Raltegravir (RAL) Elvitegravir (EVG) Dulotegravir (DTG) - Investigational

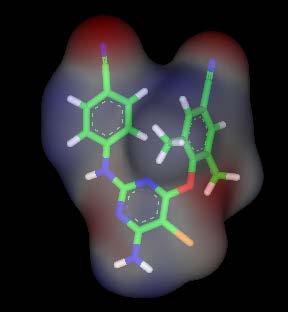
60 Integrase Inhibitor in Active Site RCSB Protein Data Base

61 Integrase Inhibitor in Active Site RCSB Protein Data Base

62 Key Raltegravir Mutations Stanford HIV Data Base
63 Raltegravir
64 RAL Resistance: Three Pathways N155H Q148K/H/R Y143C L74M L74M E92Q E92Q E92Q T97A T97A T97A V151I V151I E138A G163R G163R E138K S230R G163K S2 30R G140A G140S G163R Witmer et al, ICAAC 2008
65 Genotype Phenotype Correlations of RAL Mutations 600 Q148 Pathway Fold-Change IC Q148H Q148H/G140S Q148K Q148K/E138A Q148K/G140A Q148K/E138A/G140A Q148R Q148R/G140S
66 Elvitegravir
67 EVG: Correlation of EVG and RAL Susceptibility Among Virological Failure Isolates RAL fold-change (relative to NL4-3) R 2 = 0.66 G140S/C + Q148H/R/K G140S + Q148K mixture E138K + S147G + Q148R Other IN mutation patterns No change EVG fold-change (relative to NL4-3) McColl DJ et al. Antiviral Therapy 2007;12:Abstr. 9.
68 Quad Pill - Stribild Elvitegravir 150 mg Cobicistat 150 mg Emtricitabine 200 mg Tenofovir disoproxil fumarate 300 mg
69 Study Design n=350 Treatment- naive Any CD4 count Quad QD EFV/FTC/TDF QHS Placebo n=350 EFV/FTC/TDF QHS Quad Placebo QD Week 48 Week 192
70 Week 48 and 96 HIV-1 RNA < 50 Percentage of subjects (%) % 84% 84% 82% 7% 7% 9% 6% 8% 9% 11% 5% 0 W48 W96 W48 W96 W48 W96 Virologic Success Virologic Failure No data at W48 (or 96) QUAD (STBD) EFV/FTC/TDF (ATR)
71 Common Adverse Events Quad (n=348) Treatment Emergent Adverse Events in 10% of subjects (%) EFV/FTC/TDF (n=352) Diarrhea 23% 19% Nausea * 21% 14% Abnormal Dreams ^ 15% 27% Upper Respiratory Infection 14% 11% Headache 14% 9% Fatigue 12% 13% Insomnia * 9% 14% Depression 9% 11% Dizziness ^ 7% 24% Rash # 6% 12% * p < 0.05 ^ p < # p=0.009
72 Median Change from Baseline in Serum Creatinine Change from BL in Serum Creatinine (mg/dl) (IQR) BL Week
73 Integrase & NNRTI Resistance Through Week 48 Quad (n=348) EFV/FTC/TDF (n=352) Subjects Analyzed for Resistance*, n (%) 14 (4) 17 (5) Subjects with Resistance to ARV Regimen, n (%) 8 (2) 8 (2) Any Primary Integrase-R, n 7 Any Primary NNRTI-R n 8 Any Primary NRTI-R, n 8 2 *Subjects who experienced either suboptimal virologic response or rebound or had HIV-1 RNA 400 c/ml at their last visit.
74 Quad Compared to ATV/r + Truvada in Treatment Naive HIV-1 Infected Subjects (n=350) Quad QD Treatment naive ATV/r+FTC/TDF Placebo QD (n=350) ATV/r + FTC/TDF QD Quad Placebo QD Week 48 Week 192 E DeJesus et al 19 th CROI, Seattle, March 7, Poster # 627
75 Quad Compared to ATV/r + Truvada Week 48 HIV RNA < 50
76 Integrase, PI, NRTI Resistance Through Week 48 Quad (n=353) ATV/r + FTC/TDF (n=355) Subjects Analyzed for Resistance a, n (%) 12 (3) 8 (2) Subjects with Resistance to ARV Regimen, n (%) 5 (1) 0 Any Primary Integrase-R, n 4 - Any Primary PI-R, n - 0 Any Primary NRTI-R, n 4 0 Subjects who experienced either suboptimal virologic response or rebound or had HIV-1 RNA 400 c/ml at their last visit.
77 Dolutegravir
78
79
80 Dolutegravir: Rapid and Durable Antiviral Activity Week 96 Efficacy Analysis (<50 c/ml) Percent Subjects with HIV-1 RNA <50 c/ml (TLOVR) 88% 79% 78% 72% Week 95% confidence intervals are derived using the normal approximation. Stellbrink et al,19 th CROI, Seattle, March, 2012
81 Dolutegravir Treatment Response and Safety by Key Subgroups in Treatment Naive HIV Infected Individuals Subgroup analysis of DTG studies in drug naïve patients SPRING 2: DTG versus RAL SINGLE: DTG versus EFV Brinson C et al. CROI 2013 Atlanta. Abstract 554

82 Proportion With Plasma HIV RNA <50 at Week 48 FDA Snapshot Brinson C et al. CROI 2013 Atlanta. Abstract 554
83 Adverse Events Leading to Withdrawal Brinson C et al. CROI 2013 Atlanta. Abstract 554
84 Antiviral Activity of Dolutegravir in Subjects With Failure on an Integrase Inhibitor-Based Regimen: Week 24 Phase 3 Results From VIKING-3 HIV-1 RNA 500 copies/ml *Resistance to RAL and/or EVG *Resistance to 2 ART classes other than INIs Functional monotherapy phase DTG 50 mg BID and continue failing regimen Optimised phase DTG 50 mg BID + optimised background regimen with OSS 1 Screening period up to a maximum of 42 days Screening visit ~Day -35 Day 1 Day 8 Week 24 analysis *Screening or documented historical evidence. Week 48 analysis Nichols, G. et al. HIV11, Glasgow, UK; November 2012 ; Oral # O232.
 Week 24 by Snapshot (MSDF): 72/114 (63%) <50 copies/ml 37/114 (32%) were virologic non-responders - 6/114 (5%) changed OBR Only 5/114 (4%) were nonresponders for discontinuation due")
85 Day 8 and Week 24 Efficacy Endpoints 100 Day 8 change from BL: log 10 copies/ml, P< % CI, to (ITT-E, N=183) Week 24 by Snapshot (MSDF): 72/114 (63%) <50 copies/ml 37/114 (32%) were virologic non-responders - 6/114 (5%) changed OBR Only 5/114 (4%) were nonresponders for discontinuation due to AEs Percentage of subjects with HIV-1 RNA <50 copies/ml Overall, 63% were fully suppressed at Week 24 by Snapshot algorithm BL D8 W4 W8 W12 W16 W24 Time Week 24 population (N=114) was those subjects who had opportunity to reach Week 24 at time of data cut-off Nichols, G. et al. HIV11, Glasgow, UK; November 2012 ; Oral # O232.
86 Dolutegravir (DTG) Versus Raltegravir (RAL) in ART- Experienced, Integrase-Naive Subjects: 24-Week Interim Results From SAILING (ING111762) Pozniak A et al. CROI 2013 Atlanta. Abstract 179LB
 Pozniak A et al. CROI 2013 Atlanta.")
87 Dolutegravir (DTG) Versus Raltegravir (RAL) in ART- Experienced, Integrase-Naive Subjects: 24-Week Interim Results From SAILING (ING111762) Pozniak A et al. CROI 2013 Atlanta. Abstract 179LB

88 Baseline Characteristics Pozniak A et al. CROI 2013 Atlanta. Abstract 179LB
89 Week 24 Results Pozniak A et al. CROI 2013 Atlanta. Abstract 179LB
90 Integrase Inhibitor Summary Resistance: Very potent and rapid activity RAL and EVG broad cross-resistance Apparent less cross resistance with DTG Toxicity: Very few toxicities (currently appears to be very well tolerated and safe) PK: RAL BID EVG QD with boosting DTG QD without boosting (BID may increase genetic barrier further)
91 Summary Many excellent antiretroviral drugs are now available for HIV infected patients Both veteran and newer classes offer advantages in certain combinations and clinical situations Virological and pharmacological characteristics such as the genetic barrier to resistance and drug half life differ not only between classes, but also among agents of the same class These factors need to be considered when making therapeutic decisions
Update on HIV Drug Resistance. Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School
 Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
HIV Treatment: State of the Art 2013
 HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
STRIBILD (aka. The Quad Pill)
") NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects
 VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
Integrase Strand Transfer Inhibitors on the Horizon
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches
 Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
2 nd Line Treatment and Resistance. Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012
 2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
Antiretroviral Drugs
 Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
ART: The New, The Old and The Ugly
 ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
Second-Line Therapy NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
SELECTING THE BEST ART FOR EACH PATIENT
 SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
Disclosures. Update on HIV Drug Therapy: A Case based Discussion. Case # 1: Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv
 Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
NNRTI Resistance NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER NNRTI Resistance David H. Spach, MD Principal Investigator, NW AETC Professor of Medicine, Division of Infectious Diseases University of Washington Last Updated:
NORTHWEST AIDS EDUCATION AND TRAINING CENTER NNRTI Resistance David H. Spach, MD Principal Investigator, NW AETC Professor of Medicine, Division of Infectious Diseases University of Washington Last Updated:
Continuing Education for Pharmacy Technicians
 Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Disclosures. Introduction to ARV Drug Resistance New Clinicians Workshop 12/9/16. Introduction. ARS Question
 Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
Disclosures. Introduction to ARV Drug Resistance New Clinicians Workshop. Introduction. ARS Question 12/6/2017
 Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
HIV Treatment Update. Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London
 HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
Criteria for Oral PrEP
 Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Switching antiretroviral therapy to safer strategies based on integrase inhibitors
 Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
Bon Usage des Antirétroviraux dans l Infection par le VIH
 Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
Are the current doses of ARV correct. Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine
 Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Resistance to Integrase Strand Transfer Inhibitors
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Resistance to Integrase Strand Transfer Inhibitors David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Resistance to Integrase Strand Transfer Inhibitors David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases
Antiretroviral Dosing in Renal Impairment
 Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
HIV - Therapy Principles
 HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
Antiretroviral Therapy: What to Start
 FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
First line ART Rilpirivine A New NNRTI. Chris Jack Physician, Durdoc Centre ethekwini
 First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
Resistance Characteristics of Integrase Inhibitors
 Resistance Characteristics of Integrase Inhibitors Madrid, November 2016 Jonathan M Schapiro, MD National Hemophilia Center, Israel Stanford University School of Medicine, USA Disclaimer Presentation includes
Resistance Characteristics of Integrase Inhibitors Madrid, November 2016 Jonathan M Schapiro, MD National Hemophilia Center, Israel Stanford University School of Medicine, USA Disclaimer Presentation includes
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies. Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine
 Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
BHIVA Best of CROI Feedback Meetings. London Birmingham North West England Cardiff Gateshead Edinburgh
 BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
Third Agent Advantages Disadvantages. Component Tenofovir/emtricitabine (TDF/FTC) 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily
 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily") Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
VIKING STUDIES. Efficacy and safety of dolutegravir. treatment-experienced subjects
 VIKING STUDIES Efficacy and safety of dolutegravir treatment-experienced subjects (DTG) in UK/DLG/0083/14e(2) Date of preparation: February 2017 Prescribing information is available at the end of this
VIKING STUDIES Efficacy and safety of dolutegravir treatment-experienced subjects (DTG) in UK/DLG/0083/14e(2) Date of preparation: February 2017 Prescribing information is available at the end of this
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care
 Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
The ART of Managing Drug-Drug Interactions in Patients with HIV
 The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
Case # 1. Case #1 (cont d)
") Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
HIV in in Women Women
 HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
Somnuek Sungkanuparph, M.D.
 HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents
 Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents Victor Musiime, MBChB, MMED, PhD Senior Lecturer, Makerere University Investigator, Joint Clinical Research Centre (JCRC)
Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents Victor Musiime, MBChB, MMED, PhD Senior Lecturer, Makerere University Investigator, Joint Clinical Research Centre (JCRC)
Clinical support for reduced drug regimens. David A Cooper The University of New South Wales Sydney, Australia
 Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The next generation of ART regimens
 The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop
 HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
Resistance Analyses of Integrase Strand Transfer Inhibitors within Phase 3 Clinical Trials of Treatment-Naive Patients
 Viruses 2014, 6, 2858-2879; doi:10.3390/v6072858 Review OPEN ACCESS viruses ISSN 1999-4915 www.mdpi.com/journal/viruses Resistance Analyses of Integrase Strand Transfer Inhibitors within Phase 3 Clinical
Viruses 2014, 6, 2858-2879; doi:10.3390/v6072858 Review OPEN ACCESS viruses ISSN 1999-4915 www.mdpi.com/journal/viruses Resistance Analyses of Integrase Strand Transfer Inhibitors within Phase 3 Clinical
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
SINGLE. Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects
 in treatment-naïve subjects") SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
CL Vavro, 1 J Huang, 2 C Avatapally, 1 S Min, 1 and M Ait-Khaled 3. GlaxoSmithKline: 1 Research Triangle Park,NC, USA; 2 Toronto, ON, Canada; 3
 Durable Efficacy and Limited Integrase Resistance Evolution in Subjects Receiving Dolutegravir After Failing Prior Integrase Inhibitor (INI) Regimens: Week 48 Results from VIKING-3 CL Vavro, 1 J Huang,
Durable Efficacy and Limited Integrase Resistance Evolution in Subjects Receiving Dolutegravir After Failing Prior Integrase Inhibitor (INI) Regimens: Week 48 Results from VIKING-3 CL Vavro, 1 J Huang,
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING**, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir) Stavudine
COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir) Stavudine
HIV Drugs and the HIV Lifecycle
 HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
Treatment strategies for the developing world
 David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
ARVs in Development: Where do they fit?
 The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
INTERGRASE INHIBITORS- WHAT S NEW?
 INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
Integrase Inhibitors in the Treatment HIV-Infection. Andrew Zolopa, MD Stanford University
 Integrase Inhibitors in the Treatment HIV-Infection Andrew Zolopa, MD Stanford University 1 IAS-USA 212 Guidelines Updated Recommendations When to start ART is now recommended for all patients, regardless
Integrase Inhibitors in the Treatment HIV-Infection Andrew Zolopa, MD Stanford University 1 IAS-USA 212 Guidelines Updated Recommendations When to start ART is now recommended for all patients, regardless
Management of NRTI Resistance
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Management of NRTI Resistance David Spach, MD Principal Investigator, NW AETC Professor of Medicine, Division of Infectious Diseases University of Washington
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Management of NRTI Resistance David Spach, MD Principal Investigator, NW AETC Professor of Medicine, Division of Infectious Diseases University of Washington
What are the most promising opportunities for dose optimisation?
 What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
Management of ART Failure. EACS Advanced HIV Course 2015 Dr Nicky Mackie
 Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
Introduction to HIV Drug Resistance. Kevin L. Ard, MD, MPH Massachusetts General Hospital Harvard Medical School
 Introduction to HIV Drug Resistance Kevin L. Ard, MD, MPH Massachusetts General Hospital Harvard Medical School Objectives 1. Describe the epidemiology of HIV drug resistance in sub-saharan Africa. 2.
Introduction to HIV Drug Resistance Kevin L. Ard, MD, MPH Massachusetts General Hospital Harvard Medical School Objectives 1. Describe the epidemiology of HIV drug resistance in sub-saharan Africa. 2.
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications
 and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications") Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
L infettivologia del 3 millennio: AIDS ed altro
 L infettivologia del 3 millennio: AIDS ed altro VI Convegno Nazionale 15-16 -17 maggio 2014 Centro Congressi Hotel Ariston Paestum (SA) Nuove molecole ad azione anti-hiv Annalisa Saracino Clinica Malattie
L infettivologia del 3 millennio: AIDS ed altro VI Convegno Nazionale 15-16 -17 maggio 2014 Centro Congressi Hotel Ariston Paestum (SA) Nuove molecole ad azione anti-hiv Annalisa Saracino Clinica Malattie
Virological suppression and PIs. Diego Ripamonti Malattie Infettive - Bergamo
 Virological suppression and PIs Diego Ripamonti Malattie Infettive - Bergamo Ritonavir-boosted PIs Boosted PIs: 3 drugs in one The intrinsic antiretroviral activity Viral suppression and high baseline
Virological suppression and PIs Diego Ripamonti Malattie Infettive - Bergamo Ritonavir-boosted PIs Boosted PIs: 3 drugs in one The intrinsic antiretroviral activity Viral suppression and high baseline
History (August 2010) Therapy for Experienced Patients. History (September 2010) History (November 2010) 12/2/11
 Therapy for Experienced Patients. History (September 2010) History (November 2010) 12/2/11") (August 2010) Therapy for Experienced Patients Hiroyu Hatano, MD, MHS Assistant Professor of Medicine University of California San Francisco Medical Management of AIDS December 2011 42M HIV (CD4=450, VL=6250,
(August 2010) Therapy for Experienced Patients Hiroyu Hatano, MD, MHS Assistant Professor of Medicine University of California San Francisco Medical Management of AIDS December 2011 42M HIV (CD4=450, VL=6250,
Cases from the Clinic(ians): Case-Based Panel Discussion
: Case-Based Panel Discussion") Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi
 6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
Principles of HIV Drug Resistance: Resistance to New Drug Classes. Mark A Wainberg McGill University AIDS Centre Montreal, Quebec, Canada
 Principles of HIV Drug Resistance: Resistance to New Drug Classes Mark A Wainberg McGill University AIDS Centre Montreal, Quebec, Canada Why Is It Important to Understand HIV Drug Resistance? 1. Resistance
Principles of HIV Drug Resistance: Resistance to New Drug Classes Mark A Wainberg McGill University AIDS Centre Montreal, Quebec, Canada Why Is It Important to Understand HIV Drug Resistance? 1. Resistance
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Disclosures. Introduction to ARV Drug Resistance New Clinicians Workshop. Introduction. ARS Question
 Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
HIV Update Allegra CPD Day Program Port Elizabeth Dr L E Nojoko
 HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
Didactic Series. Switching Regimens in the Setting of Virologic Suppression
 Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Single Pill Combinations Versus Generics: Prescribing Practices in a New Healthcare Era
 Activity Code FM285 Single Pill Combinations Versus Generics: Prescribing Practices in a New Healthcare Era Monica Gandhi MD, MPH Clinic Director, Ward 86 HIV Clinic, SFGH/UCSF Learning Objectives Upon
Activity Code FM285 Single Pill Combinations Versus Generics: Prescribing Practices in a New Healthcare Era Monica Gandhi MD, MPH Clinic Director, Ward 86 HIV Clinic, SFGH/UCSF Learning Objectives Upon
Second and third line paediatric ART strategies
 Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
Nobel /03/28. HIV virus and infected CD4+ T cells
 Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
The New Agents: Management of Experienced Patients and Resistance. Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine
 The New Agents: Management of Experienced Patients and Resistance Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine T.D. 45 year old man with HIV infection diagnosed in 2000 On multiple
The New Agents: Management of Experienced Patients and Resistance Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine T.D. 45 year old man with HIV infection diagnosed in 2000 On multiple
Perspectivesconcernantles InhibiteursNon Nucléosidiquesde la Transcriptase Inverse (INNTI)
") Perspectivesconcernantles InhibiteursNon Nucléosidiquesde la Transcriptase Inverse (INNTI) Gianni Di Perri Dept. de Maladies Infectieuses Universitè de Turin Ospedale Amedeo di Savoia Fusion inhibitors
Perspectivesconcernantles InhibiteursNon Nucléosidiquesde la Transcriptase Inverse (INNTI) Gianni Di Perri Dept. de Maladies Infectieuses Universitè de Turin Ospedale Amedeo di Savoia Fusion inhibitors
Friday afternoon Programme
 Friday afternoon Programme Pharmacology and TDM Dr Marta Boffito Consultant Physician, C&W Resistance to new anti-retrovirals Dr Steve Taylor Consultant Physician, Birmingham HIVPA Annual Conference 2008
Friday afternoon Programme Pharmacology and TDM Dr Marta Boffito Consultant Physician, C&W Resistance to new anti-retrovirals Dr Steve Taylor Consultant Physician, Birmingham HIVPA Annual Conference 2008
Clinical Management of Resistance. AMJ Wensing, MD, PhD
 Clinical Management of Resistance AMJ Wensing, MD, PhD Changing treatment paradigm First Line Second Line? New First Line North America Western Europe: Eastern Europe Africa mix South America mix More
Clinical Management of Resistance AMJ Wensing, MD, PhD Changing treatment paradigm First Line Second Line? New First Line North America Western Europe: Eastern Europe Africa mix South America mix More
Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies. Joel Gallant, MD, MPH Johns Hopkins University School of Medicine
 Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies Joel Gallant, MD, MPH Johns Hopkins University School of Medicine Initial Regimen: DHHS Guidelines 3/27/2012 Preferred Regimens
Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies Joel Gallant, MD, MPH Johns Hopkins University School of Medicine Initial Regimen: DHHS Guidelines 3/27/2012 Preferred Regimens
Supplementary information
 Supplementary information Dose-response Curve Slope Sets Class-Specific Limits on Inhibitory Potential of Anti-HIV Drugs Lin Shen 1,2, Susan Peterson 1, Ahmad R. Sedaghat 1, Moira A. McMahon 1,2, Marc
Supplementary information Dose-response Curve Slope Sets Class-Specific Limits on Inhibitory Potential of Anti-HIV Drugs Lin Shen 1,2, Susan Peterson 1, Ahmad R. Sedaghat 1, Moira A. McMahon 1,2, Marc
CROI 2013: New Drugs for Treatment and PrEP
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER CROI 2013: New Drugs for Treatment and PrEP Brian R. Wood, MD Medical Director, NW AETC Project ECHO Assistant Professor of Medicine, University of Washington
NORTHWEST AIDS EDUCATION AND TRAINING CENTER CROI 2013: New Drugs for Treatment and PrEP Brian R. Wood, MD Medical Director, NW AETC Project ECHO Assistant Professor of Medicine, University of Washington
Selecting an Initial Antiretroviral Therapy (ART) Regimen
 Regimen") Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Actualización y Futuro en VIH
 Actualización y Futuro en VIH Dr. Santiago Moreno Servicio de Enfermedades Infecciosas Hospital U. Ramón y Cajal. Universidad de Alcalá. IRYCIS. Madrid Agenda Control of the HIV-epidemic Coinfections Antiretroviral
Actualización y Futuro en VIH Dr. Santiago Moreno Servicio de Enfermedades Infecciosas Hospital U. Ramón y Cajal. Universidad de Alcalá. IRYCIS. Madrid Agenda Control of the HIV-epidemic Coinfections Antiretroviral
Kimberly Adkison, 1 Lesley Kahl, 1 Elizabeth Blair, 1 Kostas Angelis, 2 Herta Crauwels, 3 Maria Nascimento, 1 Michael Aboud 1
 Pharmacokinetics of Dolutegravir and Rilpivirine After Switching to the Two-Drug Regimen From an Efavirenz- or Nevirapine- Based Antiretroviral Regimen: SWORD-1 & -2 Pooled PK Analysis Kimberly Adkison,
Pharmacokinetics of Dolutegravir and Rilpivirine After Switching to the Two-Drug Regimen From an Efavirenz- or Nevirapine- Based Antiretroviral Regimen: SWORD-1 & -2 Pooled PK Analysis Kimberly Adkison,
ARVs on an Empty Stomach: Food Interaction Studies in a resource Limited Setting
 ARVs on an Empty Stomach: Food Interaction Studies in a resource Limited Setting Dr. Andrew D Kambugu, FRCP (UK) Infectious Diseases Institute, Makerere University Outline of Discussion Key Definitions
ARVs on an Empty Stomach: Food Interaction Studies in a resource Limited Setting Dr. Andrew D Kambugu, FRCP (UK) Infectious Diseases Institute, Makerere University Outline of Discussion Key Definitions
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 03/07/18 SECTION: DRUGS LAST REVIEW DATE: 02/19/19 LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use
 Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use Calvin Cohen MD Harvard Vanguard Medical Associates CRI New England Vice Chair, Science Steering Cmte, INSIGHT Boston MA Learning
Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use Calvin Cohen MD Harvard Vanguard Medical Associates CRI New England Vice Chair, Science Steering Cmte, INSIGHT Boston MA Learning
THE HIV LIFE CYCLE. Understanding How Antiretroviral Medications Work
 THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
RESEARCH B/F/TAF in Treatment-Naïve HIV-1 and HIV-1 RNA Suppressed Switch Patients
 RESEARCH B/F/TAF in Treatment-Naïve HIV-1 and HIV-1 RNA Suppressed Switch Patients Kirsten White Gilead Sciences, Inc., Foster City, CA Background Bictegravir (BIC; B) is a novel, unboosted integrase strand
RESEARCH B/F/TAF in Treatment-Naïve HIV-1 and HIV-1 RNA Suppressed Switch Patients Kirsten White Gilead Sciences, Inc., Foster City, CA Background Bictegravir (BIC; B) is a novel, unboosted integrase strand
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 9 May 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 9 May 2012 EDURANT 25 mg film-coated tablets B/30 (CIP code: 219 472-9) Applicant: JANSSEN-CILAG rilpivirine ATC code
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 9 May 2012 EDURANT 25 mg film-coated tablets B/30 (CIP code: 219 472-9) Applicant: JANSSEN-CILAG rilpivirine ATC code
HIV Treatment Evolution. Kimberly Y. Smith MD MPH Vice President and Head, Global Research and Medical Strategy Viiv Healthcare
 HIV Treatment Evolution Kimberly Y. Smith MD MPH Vice President and Head, Global Research and Medical Strategy Viiv Healthcare Overview of the Evolution of Antiretroviral Therapy Early Treatment 1987
HIV Treatment Evolution Kimberly Y. Smith MD MPH Vice President and Head, Global Research and Medical Strategy Viiv Healthcare Overview of the Evolution of Antiretroviral Therapy Early Treatment 1987
Antiretroviral Therapy
 Antiretroviral Therapy Scott M. Hammer, M.D. 1986 1990 ZDV monorx 1990 1995 Alternative NRTI monorx Combination NRTI Rx Introduction of NNRTI s Antiretroviral resistance Pathogenetic concepts Evolution
Antiretroviral Therapy Scott M. Hammer, M.D. 1986 1990 ZDV monorx 1990 1995 Alternative NRTI monorx Combination NRTI Rx Introduction of NNRTI s Antiretroviral resistance Pathogenetic concepts Evolution
WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION
 WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION A1. PARTICIPANT ID: ENTER NUMBER HERE - - - ONLY IF ID LABEL IS NOT AVAILABLE A2. VISIT #: A3. VERSION DATE: 1 0 /
WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION A1. PARTICIPANT ID: ENTER NUMBER HERE - - - ONLY IF ID LABEL IS NOT AVAILABLE A2. VISIT #: A3. VERSION DATE: 1 0 /
HIV MEDICATIONS AT A GLANCE. Atripla 600/200/300 mg tablet tablet daily. Complera 200/25/300 mg tablet tablet daily
 HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/
HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/