Treatment Optimization for EMTCT
|
|
|
- Chad Webb
- 5 years ago
- Views:
Transcription

1 Treatment Optimization for EMTCT Dr Madeleine Muller With thanks to CN Mnyani and Linda-Gail Bekker SA HIV Clinician s Society Meeting 25 Nov 2017
2 Having children is one of the greatest joys and privileges of being human The double tragedy of HIV for the mom-to-be

3 We have effective drugs. There is no reason why any mother should die of AIDS. There is no cause for any child to be born with HIV If we work hard enough we can virtually eliminate mother-to-child transmission. Ban Ki Moon NY, September 2009

4 To Eliminate MTCT Remember the PMTCT cascade! Pre-conception Pregnancy and Labour Post-natal Every non-infertile couple whether both infected or discordant, should be asked what their reproductive intentions are at every clinic contact.
5 % Risk of transmission without intervention Transmission time During Pregnancy No BF BF 6/12 BF 24/ During labour During BF OVERALL
6 Trends in reduction of MTCT: study results over time 1994 ACTG Bangkok AP/IP ZDV 2000 PHPT 2004: PHPT-2 HAART Transmission (%) 1998 Abidjan AP/IP ZDV 1999 PETRA AZT/3TC 1999 ZDV HIVNET 012 sdnvp ZDV + NVP 2002 DITRAME +1 ZDV + NVP 2003: DITRAME +1.1 ZDV/3TC+ NVP

7 PACTG 076 USPHS AZT Recommendations 80% decline
8 Outline How do we protect Our fertile women Our women that are pregnant Our newborn babies
9 Protecting our moms SAFER CONCEPTION PLANNED PREGNANCY AND HIV PREVENTION

10 Needing updating?? Safer conception guidelines for the non-infertile HIV infected couple.

11
12 Some Key tools HIV +ve partner: Suppress the VL! Minimise condom free sex MMC! PrEP for HIV negative partner
13 The New wave in Prevention
14 Partner 1 Study Partner 1: studied heterosexual discordant couples By 2016: condomless sex acts NO transmissions if VL <200copies /ml VL <200 - Maximum possible likelihood of transmission of HIV to HIV negative partner is zero U=U
15 Minimise Condomless sex
16 When shall we go for it doc? Help patients identify their most fertile time every month VL can be affected by illness, STIs, drug interactions etc. 20 /10 Rule Take average cycle length: subtract 20 / subtract 10 E.g. if you have a 33 day cycle You are fertile from day 13 to day 23
17 Don t forget MMC
18 PrEP
19 PrEP 101 For the HIV Negative Partner Who is unsure of sexual partner s status Truvada Once A day
20 Evidence for oral PrEP efficacy reducing susceptibility Study, population Partners PrEP Study Heterosexual couples Kenya, Uganda (n=4758) TDF2 Study Heterosexuals Botswana (n=1219) Bangkok Tenofovir Study (BTS) IDUs Thailand (n=2413) iprex MSM Brazil, Ecuador, Peru, South Africa, Thailand, US (n=2499) PrEP agent # of HIV infections PrEPefficacy PrEP TDF/FTC 13 TDF 17 placebo 52 TDF/FTC TDF TDF/FTC (95% CI) publication 75% (55-87%) 67% (44-81%) Baeten et al. N Engl J Med % (16-83%) Thigpen et al. N Engl J Med % (10-72%) Choopanya et al. Lancet % (15-63%) Grant et al. N Engl J Med 2010
21 When taken, PrEP is estimated to be % protective against HIV For those with tenofovir detected in blood samples* HIV protection from PrEP was extremely high: Partners PrEP HIV risk reduction any tenofovir 90% iprex / iprex OLE any tenofovir 92% 4-6 doses/week % 7 doses/week % * compared to tenofovir not detected (restricted to active PrEP arm Baeten et al. NEJM 2012; Grant et al. NEJM 2010; Anderson et al. Science Transl Med 2012; Grant et al. Lancet ID 2014
22 Public sector: Key Populations First population targeted: Sex workers Next Key population Young women aged years old
23 PrEP Data from pharmacokinetic studies: up to 20 days of PrEP needed before achieving full protection for vaginal intercourse (vs 7 days for rectal tissue) lead-time required to achieve steady state levels of TDF in blood and tissues

24
25 PrEP PrEP may be discontinued 28 days after the last potential exposure to HIV-infected fluids o.if no continuing substantial risk for acquiring HIV infection
26 Steps to PrEP Script Check eligibility and motivation Screen for HIV, Hep B, creatinine, pregnancy, (Hep B vaccination if HepB neg) Start on Truvada and counsel on lead in time: 7 days for men 20 days for women Give condoms Regular follow up: HIV testing, creatinine, STI screening If no longer at risk: continue for 28 days
27 PMTXT cascade phase 2 THE MOM-TO-BE
28 HIV in pregnancy HIV acquisition during pregnancy and immediately following pregnancy remains high despite increased access to and initiation of antiretroviral therapy (ART). In SA: maternal HIV incidence rate 10.7 per 100 person years (PY), and 12.4 per 100 PY in urban health facilities in 2013 Moodley D, et al. Incident HIV infection in pregnant and lactating women and its effect on mother-to-child transmission in South Africa. J Infect Dis May 1;203(9): Moodley D, at al. High HIV incidence during pregnancy: compelling reason for repeat HIV testing. AIDS Jun 19;23(10):
29 Acute infection and transmission... In a recent meta-analysis, MTCT risk was significantly higher among women with incident vs. chronic HIV infection in the postpartum period (odds ratio [OR] 2.9, 95% confidence interval [CI] ) or in pregnancy/postpartum periods combined (OR 2.3, 95% CI ) Johnson LF, et al. The contribution of maternal HIV seroconversion during late pregnancy and breastfeeding to mother-to-child transmission of HIV. J Acquir Immune Defic Syndr Apr 1;59(4): Goga AE, et al; South Africa PMTCT Evaluation (SAPMCTE) Team.. Population-level effectiveness of PMTCT Option A on early mother-to-child (MTCT) transmission of HIV in South Africa: implications for eliminating MTCT. J Glob Health Dec;6(2) Drake AL, et al. Incident HIV during pregnancy and postpartum and risk of mother-to-child HIV transmission: a systematic review and meta-analysis. PLoS Med Feb 25;11(2):e
30 PrEP in pregnancy
31 Data on safety of PrEP during pregnancy limited clinician to discuss potential risks and benefits of PrEP initiation or maintenance during pregnancy
32 No mention of pregnancy

33

34 2015 Risks, benefits and alternatives of continuing PrEP during pregnancy and breastfeeding should be discussed Further research is needed to fully evaluate PrEP use during pregnancy and breastfeeding
35 Preventing HIV transmission in pregnancy
36 SA guidelines Retesting of pregnant and postpartum women who initially test HIV negative
37 mmmmm
38 Background The French Perinatal Cohort study: an ongoing, prospective, observational study involving 90 perinatal centres in France 8075 HIV-infected mother/infant pairs included from 2000 to 2011 Perinatal transmission analysed according to maternal VL at delivery and timing of ART initiation (Mandelbrot L, et al CID)
39 Results 80.4% had prenatal HIV diagnosis VL <50 copies/ml at delivery: Timing of ART % with VL<50 c/ml Preconception st T nd T rd T 44.1 (P <0.001) (Mandelbrot L, et al CID)

40 Perinatal transmission (Mandelbrot L, et al CID)
41 French Perinatal Cohort study Results Few cases of transmission with VL <50 c/ml at delivery occurred when ART was started beyond the 1 st T or interrupted during the pregnancy ART initiated in the 1 st T, nearly as effective as preconception ART (Mandelbrot L, et al CID)
42 SA guidelines 2015
43 SA guidelines From January 2015, all HIV-infected pregnant and breastfeeding women initiated on an EFV-based FDC TDF+3TC (FTC)+EFV Regardless of CD4 count, WHO stage or infant feeding practice FDC continued for life once started WHO B+ PROGRAM
44 SA guidelines Second-line regimen Failing on a TDF-based 1st line regimen AZT + 3TC + LPV/r AZT + TDF + 3TC + LPV/r (4 drugs if HBV co-infected) Failing on a d4t or AZT-based 1st line regimen TDF + 3TC (or FTC) + LPV/r Diarrhoea associated with LPV/r switch LPV/r to ATV/r
45 SA guidelines Threshold for treatment failure: VL>1000, A adherence counselling, B Bugs C Correct drugs D Drug interactions Repeat VL in 1 month with your 2 nd line drugs 2 nd VL undetectable or reduction in VL 1 log (10-fold), continue existing regimen VL unchanged or increased, switch to 2 nd line therapy

46

47 Safety of EFV in pregnancy WHO guidance based on available data and programmatic experience: EFV use in early pregnancy not associated with increased birth defects or other significant toxicities
48 Safety of TDF in pregnancy Concerns about... o Congenital abnormalities o Growth restriction o Loss of bone mineral density (maternal and fetal) o Low birth weight o Preterm delivery o Pregnancy losses

49
50
51 Conclusions TDF-based ART in pregnancy No evidence of increased risk of: Congenital anomalies Maternal and infant adverse outcomes Pregnancy loss or miscarriage Small for gestational age Low birth weight Infant mortality at age >14 days
52 Conclusions TDF-based ART in pregnancy Data limited and inconclusive evidence on: Effects of in utero TDF exposure on bone and long-term growth Neonatal deaths <14 days in very preterm (<14 weeks) infants
53 Adverse pregnancy outcomes
54 Adverse pregnancy outcomes Suggestion that cart is responsible for increased risk of adverse pregnancy outcomes Conflicting results from different studies: Different populations studied Available obstetric care Adjustment for confounders; selection of exposure categories?inflammatory effect of HIV infection (Li N, et al. JID 2015)
55 Discussion Potential mechanisms for ART and adverse pregnancy outcomes: Immune reconstitution reverses pregnancy-associated cytokine changes Disruption of physiological angiogenesis in the placenta lower placental weight, placental abnormalities, and placental insufficiency (Li N, et al. JID 2015)

56
57 Background Systematic review of studies from low-, middle- and high-income countries Studies done between January 1980 and June measure: to assess association between selected pregnancy outcomes and ART initiation pre-conception vs. after conception
58 Results 11 studies with mother infant pairs Women who started ART before conception significantly more likely to: deliver preterm (RR 1 20, 95% CI ) very preterm (1 53, ) have LBW infants (1 30, ) than were those who began ART after conception
59 Results Associations highest in studies done in low- and middleincome countries where background rates of PTD and LBW are higher than in high-income countries Association with PI-use often reported background risk factors for these pregnancy outcomes not always controlled for
60 Results Few data exist for neonatal mortality No significant difference in risk of very LBW, SGA, severe SGA, and stillbirths data for the extent and severity of these risks are scarce and of low quality
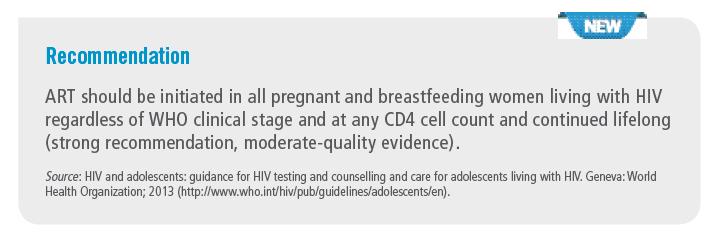
61 WHO guidelines 2015
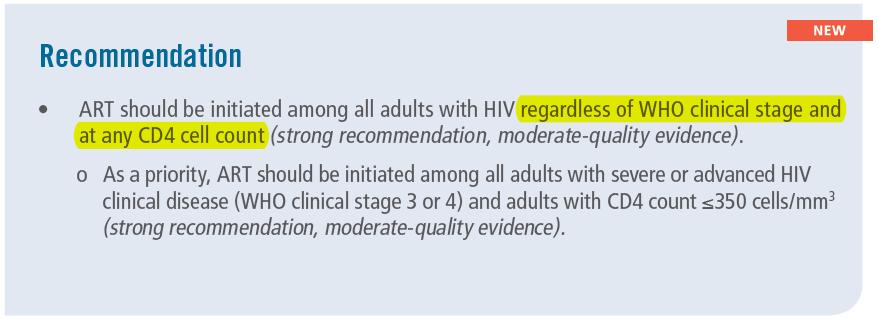
62 WHO guidelines 2015
63 Rationale Increasing evidence that untreated HIV infection may be associated with: development of several non-aids-defining conditions (CVD, kidney and liver disease, several types of cancer and neurocognitive disorders) initiating ART earlier reduces such events and improves survival
64 (START: Strategic Timing of Antiretroviral Treatment)
65
66 Interesting case 30 yr P1G2 CD4 183; FDC initiated at 23 weeks Presented at 32 weeks with preeclampsia, and respiratory symptoms Initial D x of PTB Further investigations metastatic HCC



67

68 WHO guidelines 2015

69 WHO guidelines 2016
70 WHO guidelines 2016
71 WHO guidelines 2016 Recommendation applies to breastfeeding and nonbreastfeeding populations Health benefits of universal ART for pregnant and breastfeeding women outweigh potential harm Health benefits immunological and clinical the decision to initiate treatment remains a personal one that must be made on the basis of informed consent
72 WHO guidelines 2016 Pregnant or breastfeeding women Preferred 1 st line regimen TDF + 3TC (or FTC) + EFV Alternative 1 st line regimens AZT + 3TC + EFV (or NVP) TDF + 3TC (or FTC) + NVP
73 WHO guidelines 2016 ABC or boosted PIs (ATV/r, DRV/r, LPV/r) in special circumstances Safety and efficacy data on use of dolutegravir (DTG) and EFV 400 in pregnant women not yet available
74 WHO guidelines 2016 Pregnant or breastfeeding women Preferred 2 nd line regimen 2 NRTIs + ATV/r or LPV/r Alternative 2 nd line regimen 2 NRTIs + DRV/r (similar to adults and adolescents)

75 To be updated in 2017
76 British guidelines Women conceiving on an effective cart continue regimen even if it contains EFV or does not contain AZT Treatment naïve Acceptable backbones: o AZT+3TC o TDF+FTC o ABC+3TC
77 British guidelines Recommended 3 rd agent: EFV, NVP (CD4 <250) or a boosted PI No routine dose alterations recommended during pregnancy if ARVs used at adult licensed doses Consider 3 rd T therapeutic dose monitoring if combining TDF and ATV/r
78 British guidelines Treatment naïve presenting after 28 weeks If VL unknown or > , a 3 or 4 drug regimen that includes raltegravir is suggested
79 British guidelines VL monitoring during pregnancy, at 36 weeks and at delivery If not suppressed at 36 weeks, o Adherence counselling o Resistance test if appropriate o Consider therapeutic drug monitoring o Optimize to best regimen o Consider intensification

80 mmmmmmmmm 2016 update
81 US guidelines ART should be initiated as early in pregnancy as possible ART during pregnancy generally does not increase the risk of birth defects No restriction on EFV use before 8 weeks gestation
82 US guidelines Women who become pregnant on suppressive EFVcontaining regimens should continue their current regimens Safety and PK data on tenofovir alafenamide use in pregnancy insufficient to recommend for ARV-naïve women AZT monotherapy during pregnancy no longer recommended
83 The new...
84 Safety of integrase inhibitors Lack of safety data on integrase inhibitor (raltegravir and dolutegravir) use during pregnancy and breastfeeding Some experience with raltegravir Very limited with dolutegravir
85 Safety of integrase inhibitors No published safety or efficacy data on outcomes of dolutegravir use during pregnancy Calcium or iron supplements (commonly used in pregnancy) could significantly reduce dolutegravir drug levels Transaminases need to be monitored
86 Safety of integrase inhibitors In the absence of well-controlled studies in pregnant women, dolutegravir and raltegravir should be used only if the perceived benefits outweigh the risk.
87 Dolutagravir: current evidence Recommendations for the Use of Antiretroviral Drugs in Pregnant Women with HIV Infection and Interventions to Reduce Perinatal HIV Transmission in the United States (aids.info) Preliminary human data suggest that use of dolutegravir during pregnancy is not associated with an increased risk of birth defects and miscarriage. But more data are needed, particularly with dolutegravir exposure before conception, to reach definitive conclusions, according to analyses presented at IAS Evidence limited to 2 studies and case reports.(small numbers 133 / 42 / 116) : High placental transfer
88 Darunavir/ ritonavir FDA recommendation Darunavir/r: Give twice daily during pregnancy Unless already suppressed on Darunavir/r and twice daily dosing will compromise adherence
89 Rilpivirine / Etravirine Pregnancy Category B No change in dosage needed.

90
91 Study design Retrospective cohort study of pregnant HIV-infected women in 11 centres in the US Study period: Included 101 women who initiated ART, intensified their regimen, or switched to a new regimen due to detectable viraemia (HIV RNA >40 copies/ml) at 20 weeks gestation
92 Results and conclusion Median VL at time of ART intervention was copies/ml (IQR: ) Found rapid viral load reduction with integrase inhibitorcontaining regimen Limitations: retrospective study; small sample size
93 Discussion Raltegravir twice-daily dosing o RCT (excl. pregnant women) looking at once-daily dosing (800mg) o Longer time to viral suppression esp. with VL > or CD4 <200 at baseline Insufficient data to recommend dolutegravir and elvitegravir (once-daily dosing) use in pregnancy
94 Prevention of HIV transmission during labour. INTRAPARTUM
95 SA Guidelines Test All women in labour for HIV Only need consent once during pregnancy HIV positive: sdnvp, Truvada STAT. AZT every 3 hours. Start 1TFE the next day
96 British guidelines Untreated presenting intrapartum: Stat dose of NVP; commence AZT, 3TC and raltegravir (FDC) IV AZT during labour and delivery throughout.
97 French Perinatal Cohort study Discussion Reports that neither C/S nor intrapartum IV AZT offer additional protection against perinatal transmission if LDL VL Postnatal prophylaxis (AZT or NVP) for the infant: Trials needed to evaluate whether still required when mother has long-term optimal VL control with no breastfeeding (Mandelbrot L, et al CID)
98 Protecting baby POST EXPOSURE PROPHYLAXIS
99 Phase 1: the 28 days after labour
100 Three Scenarios for PEP for labour 1 The virally suppressed mom 6 weeks NVP 2 The mom who has just started ART (within 4 weeks prior to labour) resistance unlikely 12 weeks NVP if breast feeding 3 The mom who has a VL >1000 (been on ART >3months) AZT and NVP for 6 weeks. No breast feeding
101 Phase 2: the breast feeding mom
102 Breast feeding PEP/ PrEP options for baby 1 Newly diagnosed Breast feeding mom Mom on 1TFE Start baby on AZT and NVP if PCR negative stop AZT, continue NVP 12 weeks 2 Breastfeeding mom >6 weeks and VL >1000 AZT is NOT a best choice for prevention? Use of three drugs? But what of resistance ASK an EXPERT
103 Neonatal PEP AZT Extensively studied as neonatal PEP Potential toxic (bone marrow suppression) High genetic barrier Reduced efficacy in preventing breastfeeding transmission Used in UK twice a day for 28 days if mother VL LDL NVP Evidence has confirmed NVP efficacy Very few adverse events (in neonates) Risk of NVP resistance Better choice in preventing breast feeding transmission of HIV Once daily in South Africa
104 British Guidelines If mother VL LDL AZT for 28 days (bd dosing) If mother VL > 50 copies /ml Use a three anti-retroviral therapy for 4 weeks.
105 Sugandhi N, et al.
106 HEU children Data from Botswana both weight for age and length for age significantly lower in HEU infants exposed to ART in utero Long-term impact unknown Could predispose the child to subsequent poorer health, obesity, chronic disease or cognitive dysfunction (Sugandhi N, et al. AIDS 2013, 27 (Suppl 2):S187 S195)
107 HEU children (Mofenson LM CID) Limited data, 1º from high-resource settings, suggest that: HIV and possibly ART exposure may be associated with immunologic and biologic abnormalities that could predispose HEU children to: increased risk of illness and mortality, particularly in the first few years of life
108 HEU children (Mofenson LM CID) Firm conclusions about potential long-term effects of prolonged exposure to ART in utero and during breastfeeding in the HEU child, are lacking Role of socioeconomic factors
109 The HIV infected baby NEONATAL ART


110 SA Journal HIV Medicine

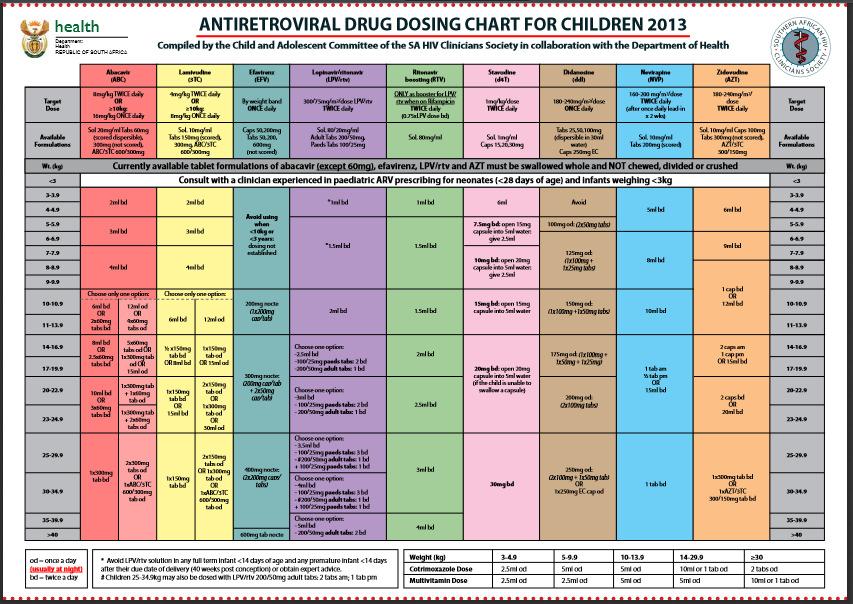
111 ABACAVIR No dosing instructions for children <3kg due to lack of PK studies Insufficient data to recommend its use in infants < 3 months old
 e.g. Born prematurely at 34 weeks: NO Kaletra until 8 weeks old")
112 LOPINAVIR/ritonavir CONTRA-INDICATED in any term baby less than 2 weeks of age AND in Premature babies until they have reached 42 weeks gestational age (so 2 weeks corrected age) e.g. Born prematurely at 34 weeks: NO Kaletra until 8 weeks old
 2mg/kg/dose RISK OF OVERDOSING THE")
113 Lamivudine Paediatric dose (> 4 weeks) 4 mg/kg/dose Neonatal dose (<4 weeks) 2mg/kg/dose RISK OF OVERDOSING THE NEONATE

114 Zidovudine Standard AZT paediatric dose: risk of anaemia in premature infants: use neonatal ARV chart After 6 weeks of age the SA ARV drug dosing chart can be used.

115 Nevirapine Use neonatal dosing chart to avoid under or overdosing No lead-in dose over a14 day period required.

116 Neonatal Management: Steps

117 Neonatal Management: Steps
118 Neonatal ART Dosage Chart Only if <28 days AND >2.5kg Lamivudine (3TC) Zidovudine(AZT) Nevirapine (NVP) Target dose 2mg/kg/dose 4mg/kg/dose 6mg/kg/dose TWICE daily (BD) TWICE daily (BD) TWICE daily (BD) Available formulation 10mg/ml 10mg/ml 10mg/ml Weight (kg) Dose in ml Dose in mg Dose in ml Dose in mg Dose in ml Dose in mg 2.5-< < < < < < ml BD 0.7 ml BD 0.8 ml BD 0.9 ml BD 1.0 ml BD 1.2ml BD 6 mg BD 7 mg BD 8 mg BD 9 mg BD 10 mg BD 12 mg BD 1.2 ml BD 1.4 ml BD 1.6 ml BD 1.8 ml BD 2.0 ml BD 2.4 ml BD 12 mg BD 14 mg BD 16 mg BD 18 mg BD 20 mg BD 24 mg BD 1.8 ml BD 2.1 ml BD 2.4 ml BD 2.7 ml BD 3.0 ml BD 3.6 ml BD 18 mg BD 21 mg BD 24 mg BD 27 mg BD 30 mg BD 36 mg BD 118
119 CF16
120 Slide 119 CF16 LEE: Update to 2013 Candice Fick, 2015/05/17
121 Monitoring Test CD4 count and percentage VL FBC Cholesterol, Triglycerides (DOH Guidelines 2014) Timing At initiation Then every 12 months At initiation After 6 monthsthen 1yr of into ART, then annually ALL children as baseline Child on AZT baseline, 1,2,3 monthly then annually Children on Lopinavir/ritonavir, baseline and thenannually ALT Child on NVP and TB treatment baseline,repeat if child develops rash or jaundice It is essential to check the weight, height and development at each visit.
122 Implications for practice
123 The EMTCT cascade: new key messages Prevent HIV infection Remember PrEP Protect the mom: ARVs soon and forever Cover labour: intrapartum and PEP Raltagravir? Cover Breastfeeding

124 Thanks to Dr. Mnyani Dr. Hendrix Dr. Anderson Dr. Cottrill Dr. Johnson Dr Lochan Dr James Nuttall
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 3 June 2017 We have effective drugs. There is no reason why any mother should die of AIDS. There
Using new ARVs in pregnancy Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 3 June 2017 We have effective drugs. There is no reason why any mother should die of AIDS. There
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Dr Kerry Uebel Slides courtesy of Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 5 August 2017 We have effective drugs. There is no reason why
Using new ARVs in pregnancy Dr Kerry Uebel Slides courtesy of Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 5 August 2017 We have effective drugs. There is no reason why
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20
 Introduction Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20 Proportions HIV infections 19% amongst adolescents (- 29.5% nationally 15
Introduction Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20 Proportions HIV infections 19% amongst adolescents (- 29.5% nationally 15
PAEDIATRIC HIV INFECTION. Dr Ashendri Pillay Paediatric Infectious Diseases Specialist
 PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
2016 Perinatal Treatment Guidelines Update
 Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010
 THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES?
 WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
Infertility Treatment and HIV
 Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC
Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC
Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM
 Dept of O+G NRMSM") Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM SA Background Population: 48m Annual number of deliveries:1,2m 97% of women attend the first ANC 71% of women attend 5 th ANC visit 97% of
Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM SA Background Population: 48m Annual number of deliveries:1,2m 97% of women attend the first ANC 71% of women attend 5 th ANC visit 97% of
Update on global guidelines. and emerging issues on perinatal HIV prevention. WHO 2013 Consolidated ARV Guidelines
 WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Dr Wendy Mphatswe SA HIV Clinician s Society Meeting 15 July 2017 Overview 1. HIV epidemic 2. HIV response (Fast Track) 3. Goal of therapy in pregnant and breastfeeding women
Using new ARVs in pregnancy Dr Wendy Mphatswe SA HIV Clinician s Society Meeting 15 July 2017 Overview 1. HIV epidemic 2. HIV response (Fast Track) 3. Goal of therapy in pregnant and breastfeeding women
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA. Date
 CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis. Against the motion
 All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis Against the motion Hermione Lyall Imperial Healthcare NHS Trust, London, UK Acknowledgements: Pat Tookey, Ali Judd, Claire
All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis Against the motion Hermione Lyall Imperial Healthcare NHS Trust, London, UK Acknowledgements: Pat Tookey, Ali Judd, Claire
SA HIV Clinicians Society Adult ART guidelines
 SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
Emerging Issues in HIV and Pregnancy. Lynne M. Mofenson, MD. HIV Senior Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation
 Emerging Issues in HIV and Pregnancy Lynne M. Mofenson, MD HIV Senior Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation Perinatal Transmission in the ART Era What s New? Antepartum ARV drug
Emerging Issues in HIV and Pregnancy Lynne M. Mofenson, MD HIV Senior Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation Perinatal Transmission in the ART Era What s New? Antepartum ARV drug
What s New. In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group
 What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
Infant feeding in the ARV era. Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital
 Infant feeding in the ARV era Gerhard Theron Gerhard Theron Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital Global HIV infections: 2007 12 countries account for
Infant feeding in the ARV era Gerhard Theron Gerhard Theron Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital Global HIV infections: 2007 12 countries account for
Prevention of Perinatal HIV Transmission
 Prevention of Perinatal HIV Transmission Emily Adhikari, MD Division of Maternal-Fetal Medicine Obstetrics and Gynecology University of Texas Southwestern Medical Center February 20, 2018 None Understand
Prevention of Perinatal HIV Transmission Emily Adhikari, MD Division of Maternal-Fetal Medicine Obstetrics and Gynecology University of Texas Southwestern Medical Center February 20, 2018 None Understand
Paediatric ART: eligibility criteria and first line regimens. (revised) Dave le Roux 13 August 2016
 Dave le Roux 13 August 2016") Paediatric ART: eligibility criteria and first line regimens (revised) Dave le Roux 13 August 2016 Outline Eligibility criteria for starting ART Evolving evidence for earlier ART W Cape, National, WHO
Paediatric ART: eligibility criteria and first line regimens (revised) Dave le Roux 13 August 2016 Outline Eligibility criteria for starting ART Evolving evidence for earlier ART W Cape, National, WHO
Dr Graham P Taylor Reader in Communicable Diseases
 HIV in Pregnancy Joint RCOG/BHIVA Multidisciplinary Conference Dr Graham Taylor Imperial College London Friday 20 January 2012, Royal College of Obstetricians and Gynaecologist, London Prevention of post-partum
HIV in Pregnancy Joint RCOG/BHIVA Multidisciplinary Conference Dr Graham Taylor Imperial College London Friday 20 January 2012, Royal College of Obstetricians and Gynaecologist, London Prevention of post-partum
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City
 PrEP 2013 Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Slide #2 U.S.: New HIV Infections Per Year ~50,000
PrEP 2013 Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Slide #2 U.S.: New HIV Infections Per Year ~50,000
HIV: Pregnancy in Serodiscordant Couple. Dr Chow TS ID Clinic HPP
 HIV: Pregnancy in Serodiscordant Couple Dr Chow TS ID Clinic HPP Sexual Reproductive Health and Rights The recognition of the sexual and reproductive health and rights (SRHR) of all individuals and couples
HIV: Pregnancy in Serodiscordant Couple Dr Chow TS ID Clinic HPP Sexual Reproductive Health and Rights The recognition of the sexual and reproductive health and rights (SRHR) of all individuals and couples
WESTERN CAPE ART GUIDELINES PRESENTATION 2013
 WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
The next generation of ART regimens
 The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
All HIV+ Women on Antiretroviral Therapy Should Breastfeed in Both Low and High Resource Settings VOTE NO!!
 All HIV+ Women on Antiretroviral Therapy Should Breastfeed in Both Low and High Resource Settings VOTE NO!! Lynne Mofenson MD Elizabeth Glaser Pediatric AIDS Foundation My Esteemed Opponent Will Likely
All HIV+ Women on Antiretroviral Therapy Should Breastfeed in Both Low and High Resource Settings VOTE NO!! Lynne Mofenson MD Elizabeth Glaser Pediatric AIDS Foundation My Esteemed Opponent Will Likely
DEPARTMENT. Treatment Recommendations for. Pregnant and Breastfeeding Women: Critical Issues Consolidated ARV Guidelines. Dr.
 2013 Consolidated ARV Guidelines H I V / A I D S Treatment Recommendations for DEPARTMENT Pregnant and Breastfeeding Women: Critical Issues Dr. Nathan Shaffer Objectives of Presentation obackground ooverview
2013 Consolidated ARV Guidelines H I V / A I D S Treatment Recommendations for DEPARTMENT Pregnant and Breastfeeding Women: Critical Issues Dr. Nathan Shaffer Objectives of Presentation obackground ooverview
TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES
 POLICY BRIEF HIV TREATMENT TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES JULY 2017 WHO This policy brief provides advice on a phased approach to transitioning to new WHO-recommended HIV treatment
POLICY BRIEF HIV TREATMENT TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES JULY 2017 WHO This policy brief provides advice on a phased approach to transitioning to new WHO-recommended HIV treatment
1. Africa Centre for Health and Population Studies 2. London School of Hygiene and Tropical Medicine 3. University College London
 A systematic review of the effects of interrupted antiretroviral interventions for prevention of mother-to-child transmission of HIV on maternal disease progression and survival Naidu KK 1, Mori R 2, Newell
A systematic review of the effects of interrupted antiretroviral interventions for prevention of mother-to-child transmission of HIV on maternal disease progression and survival Naidu KK 1, Mori R 2, Newell
Tunisian recommendations on ART : process and results
 Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
Malaysian Consensus Guidelines on Antiretroviral Therapy Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh
 Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
ARV Consolidated Guidelines 2015
 ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
Objectives. Outline. Section 1: Interaction between HIV and pregnancy. Effects of HIV on Pregnancy. Section 2: Mother-to-Child-Transmission (MTCT)
") Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Clinical skills building - HIV drug resistance
 Clinical skills building - HIV drug resistance Richard Lessells Clinical case 44-year old HIV-positive male HIV diagnosis 2010 Pre-treatment CD4+ count not known Initiated first-line ART (TDF/FTC/EFV)
Clinical skills building - HIV drug resistance Richard Lessells Clinical case 44-year old HIV-positive male HIV diagnosis 2010 Pre-treatment CD4+ count not known Initiated first-line ART (TDF/FTC/EFV)
HIV Treatment Evolution. Kimberly Y. Smith MD MPH Vice President and Head, Global Research and Medical Strategy Viiv Healthcare
 HIV Treatment Evolution Kimberly Y. Smith MD MPH Vice President and Head, Global Research and Medical Strategy Viiv Healthcare Overview of the Evolution of Antiretroviral Therapy Early Treatment 1987
HIV Treatment Evolution Kimberly Y. Smith MD MPH Vice President and Head, Global Research and Medical Strategy Viiv Healthcare Overview of the Evolution of Antiretroviral Therapy Early Treatment 1987
WHO s early release guidelines on PrEP: implications for emtct. Dominika Seidman, MD October 13, 2015
 WHO s early release guidelines on PrEP: implications for emtct Dominika Seidman, MD October 13, 2015 Outline Evidence behind WHO early release guidelines on PrEP PrEP eligibility according to the WHO Rationale
WHO s early release guidelines on PrEP: implications for emtct Dominika Seidman, MD October 13, 2015 Outline Evidence behind WHO early release guidelines on PrEP PrEP eligibility according to the WHO Rationale
Management of the HIV-Exposed Infant
 Management of the HIV-Exposed Infant Katherine Knapp, MD Medical Director, Perinatal Program Department of Infectious Diseases St. Jude Children s Research Hospital Disclosures No conflicts of interest
Management of the HIV-Exposed Infant Katherine Knapp, MD Medical Director, Perinatal Program Department of Infectious Diseases St. Jude Children s Research Hospital Disclosures No conflicts of interest
The Future of HIV: Advances in Drugs and Research. Shauna Gunaratne December 17, 2018
 The Future of HIV: Advances in Drugs and Research Shauna Gunaratne December 17, 2018 Overview Epidemiology Science of HIV How HIV treatment and management have changed over the years New medicines and
The Future of HIV: Advances in Drugs and Research Shauna Gunaratne December 17, 2018 Overview Epidemiology Science of HIV How HIV treatment and management have changed over the years New medicines and
PrEP Dosing Strategies
 PrEP Dosing Strategies Outline o Background PrEP absorption and tissue penetration o Oral versus topical o Lead in and lead out dosing Time to protection o Cycling on and off PrEP o Balancing toxicity
PrEP Dosing Strategies Outline o Background PrEP absorption and tissue penetration o Oral versus topical o Lead in and lead out dosing Time to protection o Cycling on and off PrEP o Balancing toxicity
Perinatal HIV Exposure: Antiretroviral Management. Danielle McDonald, PharmD PGY-2 Pediatric Pharmacotherapy Resident
 Perinatal HIV Exposure: Antiretroviral Management Danielle McDonald, PharmD PGY-2 Pediatric Pharmacotherapy Resident A presentation for HealthTrust Members June 1, 2018 Learning Objectives for Pharmacists
Perinatal HIV Exposure: Antiretroviral Management Danielle McDonald, PharmD PGY-2 Pediatric Pharmacotherapy Resident A presentation for HealthTrust Members June 1, 2018 Learning Objectives for Pharmacists
The NEW ARV Guidelines FAQs
 The NEW ARV Guidelines FAQs Dr Madeleine Muller MBChB (Pret).MRCGP(Lon).Dip Hiv Man IYDSA Clinical Advisor Acknowledgments IYDSA for materials and support NDOH for slides CDC our funder HIV Clinician Society
The NEW ARV Guidelines FAQs Dr Madeleine Muller MBChB (Pret).MRCGP(Lon).Dip Hiv Man IYDSA Clinical Advisor Acknowledgments IYDSA for materials and support NDOH for slides CDC our funder HIV Clinician Society
Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update
 Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Preventing Mother to Child HIV Transmission: Are We There Yet?!'
 Preventing Mother to Child HIV Transmission: Are We There Yet?!' 2017 Michigan Clincal Nursing Conference for HIV and STD Care May 18, 2017 Frankenmuth MI 1 Theodore B. Jones, MD Maternal Fetal Medicine
Preventing Mother to Child HIV Transmission: Are We There Yet?!' 2017 Michigan Clincal Nursing Conference for HIV and STD Care May 18, 2017 Frankenmuth MI 1 Theodore B. Jones, MD Maternal Fetal Medicine
The New National Guidelines. Feeding in the Context of HIV. Dr. Godfrey Esiru; National PMTCT Coordinator
 The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
HIV/AIDS Prenatal Care for HIV+ Mothers. 1. Algorithm for Prenatal Screening & Care (Antepartum)
") 7/10/18 njm 1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+
7/10/18 njm 1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+
CCC ARV Dosing Recommendations for HIV-exposed infants Updated
 USERS NOTE: Please note this document does not provide guidance on overall decisionmaking regarding what medication(s) to use for HIV-exposed infants. This document is meant to facilitate ARV dosing for
USERS NOTE: Please note this document does not provide guidance on overall decisionmaking regarding what medication(s) to use for HIV-exposed infants. This document is meant to facilitate ARV dosing for
Disclosure. Learning Objectives. Epidemiology. Transmission. Risk of Transmission PRE-EXPOSURE PROPHYLAXIS (PREP) FOR HIV PREVENTION 50,000.
 FOR HIV PREVENTION 50,000.") Disclosure PRE-EXPOSURE PROPHYLAXIS (PREP) FOR HIV PREVENTION I have no financial interest in and/or affiliation with any external organizations in relation to this CE program. DaleMarie Vaughan, PharmD
Disclosure PRE-EXPOSURE PROPHYLAXIS (PREP) FOR HIV PREVENTION I have no financial interest in and/or affiliation with any external organizations in relation to this CE program. DaleMarie Vaughan, PharmD
Pediatric HIV Update NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE
 UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE 3/13/2013 Contents Group Work Instructions... 2 PMTCT... 3 Case Study 1: Unbooked Pregnant Women... 3 Case Study 2: First ANC
UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE 3/13/2013 Contents Group Work Instructions... 2 PMTCT... 3 Case Study 1: Unbooked Pregnant Women... 3 Case Study 2: First ANC
2009 Revisions of WHO ART Guidelines. November 2009
 2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09
2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09
during conception, pregnancy and lactation at 2 U.S. medical centers
 Use of HIV preexposure prophylaxis during conception, pregnancy and lactation at 2 U.S. medical centers Dominika Seidman, MD Shannon Weber, Maria Teresa Timoney, Karishma Oza, Elizabeth Mullins, Rodney
Use of HIV preexposure prophylaxis during conception, pregnancy and lactation at 2 U.S. medical centers Dominika Seidman, MD Shannon Weber, Maria Teresa Timoney, Karishma Oza, Elizabeth Mullins, Rodney
Outline. Aim with PMTCT. How are children transmitted. Prevention of mother-to-child transmission of HIV. How does HIV transmit to children?
 Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
Figure S1: Overview of PMTCT Options A and B. Prevention of Mother to Child HIV Transmission (PMTCT)
") Figure S1: Overview of PMTCT Options A and B Prevention of Mother to Child HIV Transmission (PMTCT) Option A: combined Antiretroviral therapy (ART) for all women meeting WHO 2010 criteria for initiation
Figure S1: Overview of PMTCT Options A and B Prevention of Mother to Child HIV Transmission (PMTCT) Option A: combined Antiretroviral therapy (ART) for all women meeting WHO 2010 criteria for initiation
Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps
 Appendix 4 Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps Lynne M. Mofenson, MD Eunice Kennedy Shriver National Institute of
Appendix 4 Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps Lynne M. Mofenson, MD Eunice Kennedy Shriver National Institute of
PrEP for Women: HIV Prevention in Family Planning Settings
 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention PrEP for Women: HIV Prevention in Family Planning Settings Dawn K. Smith, MD, MS, MPH Division of HIV/AIDS Prevention dsmith1@cdc.gov
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention PrEP for Women: HIV Prevention in Family Planning Settings Dawn K. Smith, MD, MS, MPH Division of HIV/AIDS Prevention dsmith1@cdc.gov
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Mother to Child HIV Transmission
 Koff WC. NEJM 2010;363:e7 Mother to Child HIV Transmission Why We Still Need New Prevention Modalities Lynne M. Mofenson, M.D. Maternal and Pediatric Infectious Disease Branch Eunice Kennedy Shriver National
Koff WC. NEJM 2010;363:e7 Mother to Child HIV Transmission Why We Still Need New Prevention Modalities Lynne M. Mofenson, M.D. Maternal and Pediatric Infectious Disease Branch Eunice Kennedy Shriver National
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
hiv/aids Programme Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants
 hiv/aids Programme Programmatic update Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants EXECUTIVE SUMMARY April 2012 EXECUTIVE SUMMARY Recent developments
hiv/aids Programme Programmatic update Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants EXECUTIVE SUMMARY April 2012 EXECUTIVE SUMMARY Recent developments
2nd line failure, provincial evaluation process for 3rd line therapy, 3rd line treatment options James Nuttall
 2nd line failure, provincial evaluation process for 3rd line therapy, 3rd line treatment options James Nuttall Paediatric Infectious Diseases Unit, Red Cross War Memorial Children s Hospital & University
2nd line failure, provincial evaluation process for 3rd line therapy, 3rd line treatment options James Nuttall Paediatric Infectious Diseases Unit, Red Cross War Memorial Children s Hospital & University
Epatite B: fertilità, gravidanza ed allattamento, aspetti clinici e terapeutici. Ivana Maida
 Epatite B: fertilità, gravidanza ed allattamento, aspetti clinici e terapeutici Ivana Maida Positivity for HBsAg was found in 0.5% of tested women In the 70s and 80s, Italy was one of the European countries
Epatite B: fertilità, gravidanza ed allattamento, aspetti clinici e terapeutici Ivana Maida Positivity for HBsAg was found in 0.5% of tested women In the 70s and 80s, Italy was one of the European countries
What to expect. Neonatal HIV management. Background 3/9/2017. ID Update in Children Background. The straightforward.
 What to expect Background Neonatal HIV management Prof. Nicolette du Plessis Paediatric Infectious Diseases University of Pretoria nicolette.duplessis@up.ac.za The straightforward The difficult The impossible
What to expect Background Neonatal HIV management Prof. Nicolette du Plessis Paediatric Infectious Diseases University of Pretoria nicolette.duplessis@up.ac.za The straightforward The difficult The impossible
Rajesh T. Gandhi, M.D.
 HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
ART for HIV Prevention:
 ART for HIV Prevention: KENNETH H. MAYER, M.D. Brown University/The Fenway Institute August 22, 2009 APPROACHES TO PREVENT HIV TRANSMISSION DECREASE SOURCE OF INFECTION Barrier Protection Treat STI Antiretroviral
ART for HIV Prevention: KENNETH H. MAYER, M.D. Brown University/The Fenway Institute August 22, 2009 APPROACHES TO PREVENT HIV TRANSMISSION DECREASE SOURCE OF INFECTION Barrier Protection Treat STI Antiretroviral
HIV IN PREGNANCY. Practices for Maintaining Maternal Health and Preventing Perinatal HIV Transmission. University of Tennessee Health Science Center
 HIV IN PREGNANCY Practices for Maintaining Maternal Health and Preventing Perinatal HIV Transmission Nina K. Sublette, PhD, FNP University of Tennessee Health Science Center College of Nursing: Department
HIV IN PREGNANCY Practices for Maintaining Maternal Health and Preventing Perinatal HIV Transmission Nina K. Sublette, PhD, FNP University of Tennessee Health Science Center College of Nursing: Department
Biomedical Prevention in HIV
 Biomedical Prevention in HIV CHART - CCAS-CDC 3 RD Joint Meeting Montego Bay, Jamaica August 21-26,2011 Presented by Tina Hylton-Kong, ERTU-CHART Some Slides from Impact of ART on HIV Transmission Wafaa
Biomedical Prevention in HIV CHART - CCAS-CDC 3 RD Joint Meeting Montego Bay, Jamaica August 21-26,2011 Presented by Tina Hylton-Kong, ERTU-CHART Some Slides from Impact of ART on HIV Transmission Wafaa
CROI 2016 Update NEAETC, March 21, Sigal Yawetz, MD Brigham and Women s Hospital Harvard Medical School
 CROI 2016 Update NEAETC, March 21, 2016 Sigal Yawetz, MD Brigham and Women s Hospital Harvard Medical School CROI 2016 Update NEAETC, March 21, 2016 UNITED STATES EPIDEMIOLOGY Estimating the lifetime risk
CROI 2016 Update NEAETC, March 21, 2016 Sigal Yawetz, MD Brigham and Women s Hospital Harvard Medical School CROI 2016 Update NEAETC, March 21, 2016 UNITED STATES EPIDEMIOLOGY Estimating the lifetime risk
Antiretroviral Drugs for HIV Seronegative People: It works in trials, what about the real world?
 Antiretroviral Drugs for HIV Seronegative People: It works in trials, what about the real world? Lut Van Damme 11 Oct 2012 1 Disclaimer Gilead donated the study product for the FEM-PrEP trial I participated
Antiretroviral Drugs for HIV Seronegative People: It works in trials, what about the real world? Lut Van Damme 11 Oct 2012 1 Disclaimer Gilead donated the study product for the FEM-PrEP trial I participated
Updates on Revised Antiretroviral Treatment Guidelines Overview 27 March 2013
 Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
Overview of 2013 WHO consolidated ARV guidelines and update plans. Marco Vitoria HIV/AIDS Department WHO Geneva September 2014
 AMDS ANNUAL STAKEHOLDERS AND PARTNERS MEETING Overview of 2013 WHO consolidated ARV guidelines and update plans Marco Vitoria HIV/AIDS Department WHO Geneva September 2014 AMDS ANNUAL STAKEHOLDERS AND
AMDS ANNUAL STAKEHOLDERS AND PARTNERS MEETING Overview of 2013 WHO consolidated ARV guidelines and update plans Marco Vitoria HIV/AIDS Department WHO Geneva September 2014 AMDS ANNUAL STAKEHOLDERS AND
Breast Feeding for Women with HIV?
 Breast Feeding for Women with HIV? CHIVA / BHIVA Hermione Lyall Imperial Healthcare NHS Trust 17.11.17 Acknowledgements: Nell Freeman-Romilly, Pat Tookey, Claire Townsend, Claire Thorne, Kate Francis,
Breast Feeding for Women with HIV? CHIVA / BHIVA Hermione Lyall Imperial Healthcare NHS Trust 17.11.17 Acknowledgements: Nell Freeman-Romilly, Pat Tookey, Claire Townsend, Claire Thorne, Kate Francis,
Advances in HIV science and treatment. Report on the global AIDS epidemic,
 HIV biomolecular advances and treatment updates David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia UNAIDS: global l HIV infections
HIV biomolecular advances and treatment updates David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia UNAIDS: global l HIV infections
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV
 TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
The Science behind Preexposure Prophylaxis (PrEP) Yunus Moosa Department of Infectious Diseases UKZN
 Yunus Moosa Department of Infectious Diseases UKZN") The Science behind Preexposure Prophylaxis (PrEP) Yunus Moosa Department of Infectious Diseases UKZN 1 Ongoing HIV transmission despite expanding access to ART SA 18 16 14 12 10 8 6 4 2 0 Treatment exposure
The Science behind Preexposure Prophylaxis (PrEP) Yunus Moosa Department of Infectious Diseases UKZN 1 Ongoing HIV transmission despite expanding access to ART SA 18 16 14 12 10 8 6 4 2 0 Treatment exposure
Pediatric Antiretroviral Resistance Challenges
 Pediatric Antiretroviral Resistance Challenges Thanyawee Puthanakit, MD The HIVNAT, Thai Red Cross AIDS research Center The Research Institute for Health Science, Chiang Mai University Outline The burden
Pediatric Antiretroviral Resistance Challenges Thanyawee Puthanakit, MD The HIVNAT, Thai Red Cross AIDS research Center The Research Institute for Health Science, Chiang Mai University Outline The burden
James Nuttall Paediatric Infectious Diseases Unit Red Cross Children s Hospital
 James Nuttall Paediatric Infectious Diseases Unit Red Cross Children s Hospital Paediatric HIV Infection Symposium, August 21, 2010, Red Cross Children s Hospital Overview of talk The 2010 paediatric guidelines
James Nuttall Paediatric Infectious Diseases Unit Red Cross Children s Hospital Paediatric HIV Infection Symposium, August 21, 2010, Red Cross Children s Hospital Overview of talk The 2010 paediatric guidelines
Revised Anti- Retroviral Treatment Guideline Update For Frontline Clinical Health Professionals 3/13/2013
 Revised Anti- Retroviral Treatment Guideline Update For Frontline Clinical Health Professionals 3/13/2013 The following document highlights the changes National department of Health ARV treatment guidelines
Revised Anti- Retroviral Treatment Guideline Update For Frontline Clinical Health Professionals 3/13/2013 The following document highlights the changes National department of Health ARV treatment guidelines
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
HIV 101. Applications of Antiretroviral Therapy
 HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
Labor & Delivery Management for Women Living with HIV. Pooja Mittal, DO Lisa Rahangdale, MD
 Labor & Delivery Management for Women Living with HIV Pooja Mittal, DO Lisa Rahangdale, MD Statistics for Perinatally Acquired HIV Timing of Perinatal HIV Transmission Most transmission occurs close to
Labor & Delivery Management for Women Living with HIV Pooja Mittal, DO Lisa Rahangdale, MD Statistics for Perinatally Acquired HIV Timing of Perinatal HIV Transmission Most transmission occurs close to
PRE-EXPOSURE PROPHYLAXIS FOR HIV: EVIDENCE AND GENDER CONSIDERATIONS. Jean R. Anderson M.D. Director, Johns Hopkins HIV Women s Health Program
 PRE-EXPOSURE PROPHYLAXIS FOR HIV: EVIDENCE AND GENDER CONSIDERATIONS Jean R. Anderson M.D. Director, Johns Hopkins HIV Women s Health Program Disclosures None Objectives Review the evidence regarding the
PRE-EXPOSURE PROPHYLAXIS FOR HIV: EVIDENCE AND GENDER CONSIDERATIONS Jean R. Anderson M.D. Director, Johns Hopkins HIV Women s Health Program Disclosures None Objectives Review the evidence regarding the
Obstetrics and HIV An Update. Jennifer Van Horn MD University of Utah
 Obstetrics and HIV An Update Jennifer Van Horn MD University of Utah Obstetrics and HIV Perinatal transmission Testing Antiretroviral therapy Antepartum management Intrapartum management Postpartum management
Obstetrics and HIV An Update Jennifer Van Horn MD University of Utah Obstetrics and HIV Perinatal transmission Testing Antiretroviral therapy Antepartum management Intrapartum management Postpartum management
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents
 Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents Victor Musiime, MBChB, MMED, PhD Senior Lecturer, Makerere University Investigator, Joint Clinical Research Centre (JCRC)
Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents Victor Musiime, MBChB, MMED, PhD Senior Lecturer, Makerere University Investigator, Joint Clinical Research Centre (JCRC)
Principles of Antiretroviral Therapy
 Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Dr Sonia Raffe. Royal Sussex County Hospital, Brighton. 21 st Annual Conference of the British HIV Association (BHIVA)
") 21 st Annual Conference of the British HIV Association (BHIVA) Dr Sonia Raffe Royal Sussex County Hospital, Brighton 21-24 April 2015, The Brighton Centre 21 st Annual Conference of the British HIV Association
21 st Annual Conference of the British HIV Association (BHIVA) Dr Sonia Raffe Royal Sussex County Hospital, Brighton 21-24 April 2015, The Brighton Centre 21 st Annual Conference of the British HIV Association
PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT
 PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT Dr Chewe Luo MMed (Paeds), Mtrop Paed, PhD Senior Adviser and Team Leader Country Programme Scale up HIV Section Programme Division UNICEF, NY
PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT Dr Chewe Luo MMed (Paeds), Mtrop Paed, PhD Senior Adviser and Team Leader Country Programme Scale up HIV Section Programme Division UNICEF, NY
Historic Perspective on HIV and TB Research in Pregnant Women
 Historic Perspective on HIV and TB Research in Pregnant Women Lynne M. Mofenson, M.D. Senior HIV Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation High Burden of TB/HIV in Women - 2016 TB HIV
Historic Perspective on HIV and TB Research in Pregnant Women Lynne M. Mofenson, M.D. Senior HIV Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation High Burden of TB/HIV in Women - 2016 TB HIV
PMTCT UPDATE. AWACC CONFERENCE DURBAN SEPT 2013 Dr HM Sebitloane Chief Specialist, Dept of O+G, NRMSM
 PMTCT UPDATE AWACC CONFERENCE DURBAN SEPT 2013 Dr HM Sebitloane Chief Specialist, Dept of O+G, NRMSM Outline Background Risk of MTCT Historical ARV interventions SA PMTCT program Rationale for changes
PMTCT UPDATE AWACC CONFERENCE DURBAN SEPT 2013 Dr HM Sebitloane Chief Specialist, Dept of O+G, NRMSM Outline Background Risk of MTCT Historical ARV interventions SA PMTCT program Rationale for changes
Where are we going after effectiveness studies?
 Where are we going after effectiveness studies? Nyaradzo M. Mgodi (MBChB, MMed) UZ-UCSF Collaborative Research Program Harare, Zimbabwe MTN Annual Meeting 28 March 2011, Arlington, VA Introduction 30 years
Where are we going after effectiveness studies? Nyaradzo M. Mgodi (MBChB, MMed) UZ-UCSF Collaborative Research Program Harare, Zimbabwe MTN Annual Meeting 28 March 2011, Arlington, VA Introduction 30 years
Perinatal Care and Prevention. Jennifer Janelle, MD Assistant Professor of Medicine University of Florida at Gainesville
 Perinatal Care and Prevention Jennifer Janelle, MD Assistant Professor of Medicine University of Florida at Gainesville Objectives Develop patient centered, team based, treatment and delivery plans to
Perinatal Care and Prevention Jennifer Janelle, MD Assistant Professor of Medicine University of Florida at Gainesville Objectives Develop patient centered, team based, treatment and delivery plans to
The 2017 Namibia ART Guidelines. Tadesse T. Mekonen, MD, MPH, AAF-HIV
 The 2017 Namibia ART Guidelines Tadesse T. Mekonen, MD, MPH, AAF-HIV Q1-Table 1 List at least four key new recommendations in the 2017 Namibian ART Guidelines Q2-Table-2 46yo, Male, on AZT/TDF/FTC/ATVr
The 2017 Namibia ART Guidelines Tadesse T. Mekonen, MD, MPH, AAF-HIV Q1-Table 1 List at least four key new recommendations in the 2017 Namibian ART Guidelines Q2-Table-2 46yo, Male, on AZT/TDF/FTC/ATVr
Pediatric Antiretroviral Therapy
 Update on Pediatric Antiretroviral Therapy Lynne M. Mofenson, M.D. Pediatric, Adolescent and Maternal AIDS Branch National Institute of Child Health and Human Development National Institutes of Health
Update on Pediatric Antiretroviral Therapy Lynne M. Mofenson, M.D. Pediatric, Adolescent and Maternal AIDS Branch National Institute of Child Health and Human Development National Institutes of Health
PMTCT Max Kroon Mowbray Maternity Hospital Division of Neonatal Medicine School of Child and Adolescent Health University of Cape Town
 PMTCT 2010 Max Kroon Mowbray Maternity Hospital Division of Neonatal Medicine School of Child and Adolescent Health University of Cape Town Prevention of Mother-To-Child Transmission of HIV or Prevention
PMTCT 2010 Max Kroon Mowbray Maternity Hospital Division of Neonatal Medicine School of Child and Adolescent Health University of Cape Town Prevention of Mother-To-Child Transmission of HIV or Prevention