C.W. Shafer, MD HIV Specialist, AAHIVM Sioux Falls Family Medicine Residency Falls Community Health
|
|
|
- Curtis Rich
- 5 years ago
- Views:
Transcription

1 C.W. Shafer, MD HIV Specialist, AAHIVM Sioux Falls Family Medicine Residency Falls Community Health
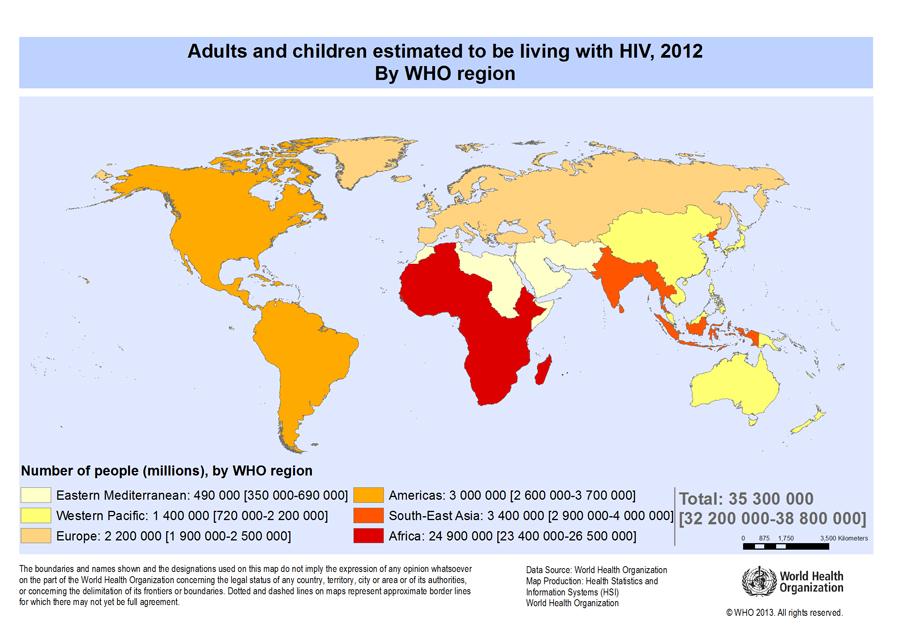
2 Objectives 1. Discuss the current status of the statewide, nationwide and worldwide HIV/AIDS epidemics. 2. Describe the impact of HIV on the management of the pregnant patient. 3. Discuss Pre- and Post-Exposure Prophylaxis for HIV.
3
4 HIV in the U.S.A. 658,000 deaths 1,200,000 HIV- infected ~50,000 new cases per year 12.8% remain undiagnosed (~156,300 individuals)
5 South Dakota HIV Statistics Through cumulative HIV/AIDS cases since people living with HIV in SD 31 new cases in 2014; 19 males, 12 females African Americans comprise 23% of living cases, <1% of gen l population Native Americans: 16% of living cases, 9 % of gen l population
6 South Dakota Residents Reported Infected with HIV/AIDS: Cumulative Cases by County, Harding Perkins Corson 6 Campbell Walworth < 5 McPherson Edmunds Brown 12 Marshall < 5 Day < 5 Roberts < 5 Butte 6 Custer < 5 Pennington 160 Meade 14 Ziebach Dewey < 5 Lawrence Stanley Hughes Haakon < 5 Fall River < 5 Shannon 30 Jackson < 5 Bennett < 5 Jones < 5 Mellette < 5 Todd 8 Sully Potter < 5 Lyman < 5 Tripp < 5 0 Cases 1-5 Cases 6-30 Cases Cases Hyde Faulk Buffalo < 5 Hand Brule < 5 Jerauld Aurora Spink < 5 Beadle 13 Douglas Charles Mix Gregory < 5 < 5 Clark < 5 Kingsbury < 5 Hamlin Grant < 5 Deuel < 5 Sanborn Miner Lake Moody < 5 < 5 6 Davison Hanson McCook 8 < 5 Hutchinson < 5 Bon Homme 7 Codington 9 Turner < 5 Yankton 30 Brookings 10 Minnehaha 310 Clay 16 Lincoln 6 Union 7 8

7 South Dakota HIV as of Exposure Category Heterosexual - 30% MSM - 35% Injection Drug Use - 15% MSM and IDU - 4% Perinatal/Peds - 2% Transfusion - 2% Unspecified - 8%
8 South Dakota Residents Infected by HIV, by Gender, Cases reported HIV (female) HIV (male) Total AIDS
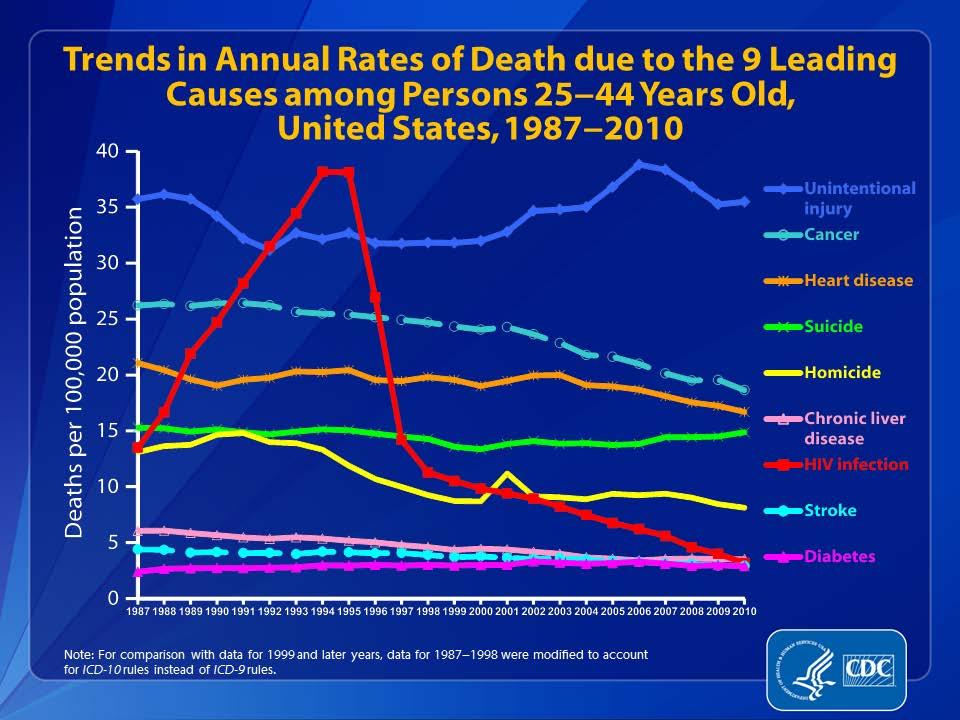
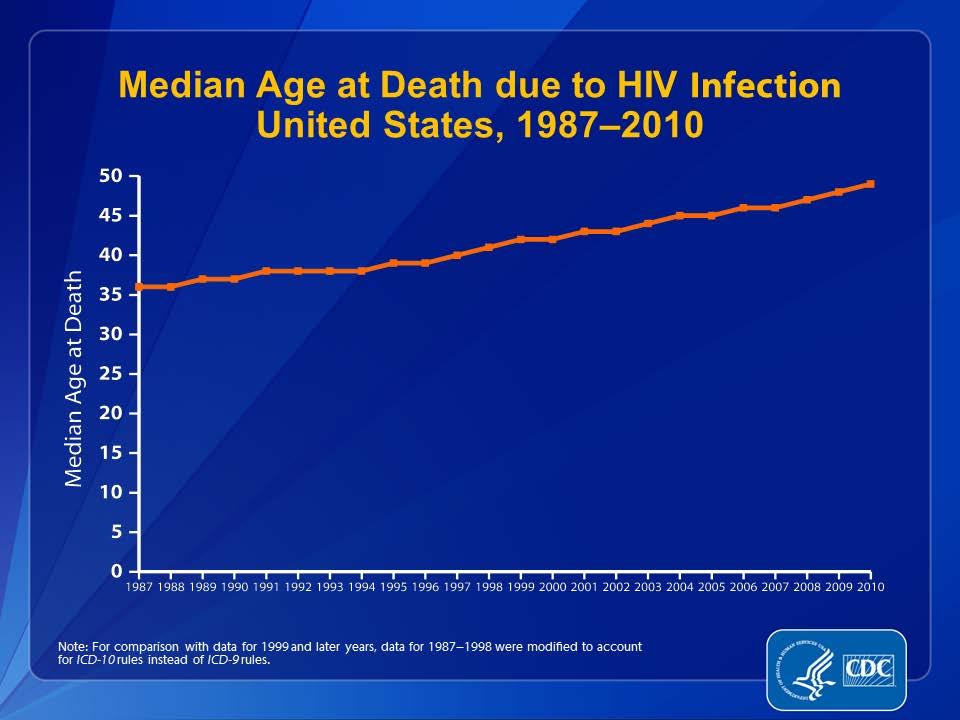
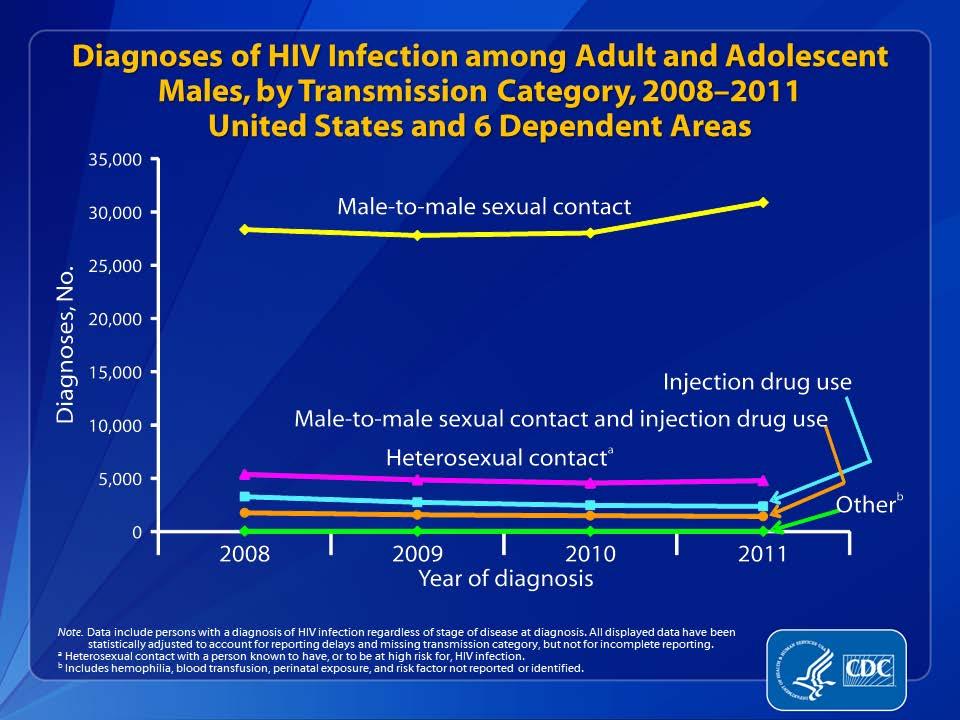
9 HIV trends in the USA Mortality Mode of transmission Race Gender
10
11
12
13 Percentages of Stage 3 (AIDS) Classifications among Adults and Adolescents with HIV Infection, by Transmission Category and Year of Diagnosis, United States and 6 Dependent Areas Note. All displayed data have been statistically adjusted to account for reporting delays and missing transmission category, but not for incomplete reporting. a Heterosexual contact with a person known to have, or to be at high risk for, HIV infection. b Includes hemophilia, blood transfusion, perinatal exposure, and risk factor not reported or not identified.
14
15 Adults and Adolescents Living with Diagnosed HIV Infection Ever Classified as Stage 3 (AIDS), by Sex, United States and 6 Dependent Areas Note. All displayed data have been statistically adjusted to account for reporting delays, but not for incomplete reporting.
16 Stage 3 (AIDS) Classifications among Adults and Adolescents with Diagnosed HIV Infection, by Race/Ethnicity, United States and 6 Dependent Areas Note. All displayed data have been statistically adjusted to account for reporting delays, but not for incomplete reporting. a Hispanics/Latinos can be of any race. b Includes Asian/Pacific Islander legacy cases.
17 Survival after Classification of Stage 3 (AIDS) during , by Months Survived and Race/Ethnicity United States and 6 Dependent Areas Note. Data exclude persons whose month of diagnosis or month of death is unknown. a Includes Asian/Pacific Islander legacy cases. b Hispanics/Latinos can be of any race.
18 Trends in the Percentage Distribution of Deaths due to HIV Infection by Sex, United States, Note: For comparison with data for 1999 and later years, data for were modified to account for ICD-10 rules instead of ICD-9 rules.
19 What Should I Know About HIV? 1. Relevance 2. Risk Behaviors 3. Testing 4. Medications
20 How is This Even Relevant to Me? Whether you realize it or not, HIV is here in SD Some of your patients are involved in high-risk behaviors Patients you are seeing may not mention their HIV If you don t ask, they won t tell
21 HIV: A Quick Review of the Basics The current HIV paradigm: just another chronic disease Essentially no impact on life expectancy in a significant subset of patients HIV transmission is behavior-based Tremendous progress has been made in HIV treatment, but neither a cure or a vaccine is practical Patients with HIV are just like you and me
22 HIV High-Risk Behaviors Engaging in anal, oral or vaginal sex with MSM, multiple or anonymous partners Injecting drugs with a shared needle Being diagnosed with an STD Exchanging sex for drugs or money Having rec d blood products 78 to 85 in US
23 Who Should Be Tested for HIV? All pregnant women Anyone diagnosed with any STD Everyone age (2006 CDC recommendation for opt-out testing ) At least one time and more often based on risk Up to every 3 months based on ongoing risk Understand the possibility of false positives

24 Opt-Out Testing for HIV
25 Available HIV tests Enzyme Immunoassay (EIA) Detects HIV Antibody Rapid EIA Blood Urine Saliva HIV-1 Multispot New confirmatory test Western Blot Old confirmatory test HIV-1 RNA (Quantitative) use only when acute retroviral syndrome is suspected 4 th Generation combined Ab/Ag test
26 HIV Testing at Avera and Sanford Generation 4 HIV: HIV 1 and 2 antibody PLUS a p24 antigen Turnaround time: Within 1 hour Confirmatory test still required
27 HIV Testing in Pregnancy All women should be tested at 1 st visit Higher risk of false positive EIA s in pregnancy Repeat testing in 3 rd trimester for women at increased risk of HIV: HIV prevalence in pregnant women is > 1 per 1,000 Incarcerated women Jurisdictions with elevated HIV incidence Individuals (OR THEIR PARTNERS) involved in highrisk behaviors
28 Anti-Retroviral Medication Issues Take all or take none (suboptimal adherence leads to development of resistance) Potentially-serious adverse events Marrow suppression: zidovudine Pancreatitis: didanosine, stavudine and others Hepatotoxicity: multiple, esp. nevirapine and PI s CNS side effects: efavirenz Hyperglycemia and Hyperlipidemia: PI s Bone and renal toxicity: Tenofovir
29 What do I need to know about HAART? (Highly Active Anti-Retroviral Therapy) DRUG INTERACTIONS DRUG INTERACTIONS DRUG INTERACTIONS Be aware of side effects
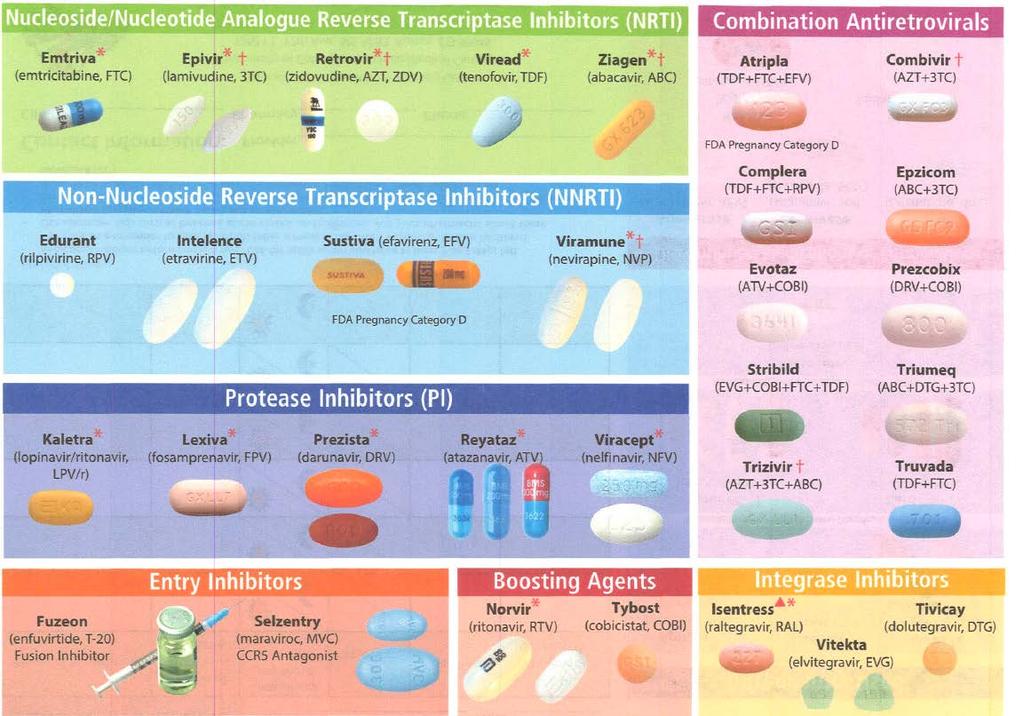
30 HIV Medication Timeline 1987 Zidovudine (AZT/Retrovir) Didanosine (DdI or Videx) 1992 Zalcitabine (DdC or Hivid) Stavudine (D4T or Zerit) 1995 Lamivudine (3TC or Epivir), Saquinavir (Invirase, Fortovase) 1996 Ritonavir (Norvir), Indinavir (Crixivan), Nevirapine (Viramune)
31 HIV Medication Timeline 1997 Nelfinavir (Viracept), Delavirdine (Rescriptor) 1998 Efavirenz (Sustiva), Abacavir (Ziagen) 1999 Amprenavir (Agenerase) 2000 Lopinavir/ Ritonavir (Kaletra) 2001 Tenofovir (Viread) 2003 Emtricitabine (Emtriva), Fosamprenavir (Lexiva), Enfuvertide (Fuzeon) Tipranavir (Aptivus) 2006 Darunavir (Prezista), Efavirenz/emtracitabine/tenofovir (Atripla)
32 HIV Medication Timeline 2007 Maraviroc (Selzentry), Raltegravir (Isentress) Etravirine (Intelence) Rilpivirine (Edurant), Emtricitabine/rilpivirine/tenofovir (Complera) Elvitegravir/cobicistat/emtricitabine/ tenofovir disproxil (Stribild) Dolutegravir (Tivicay)
33 HIV Medication Timeline Dolutegravir/abacavir/lamivudine (Triumeq), Elvitegravir (Vitekta), Cobicistat (Tybost) Darunavir/cobicistat (Prezcobix), Atazanavir/cobicistat (Evotaz), Elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide (Genvoya)
34
35 Common Lab Abnormalities Neutropenia is common Elevated protein is common Atazanavir (Reyataz) causes high bilirubin Zidovudine (Retrovir) causes a high MCV Cobicistat (Tybost, Prezcobix, Evotaz, Stribild, Genvoya) can cause a false elevation in Cr
36 Objectives 1. Discuss the current status of the statewide, nationwide and worldwide HIV/AIDS epidemics. 2. Describe the impact of HIV on the management of the pregnant patient. 3. Discuss Pre- and Post-Exposure Prophylaxis for HIV.
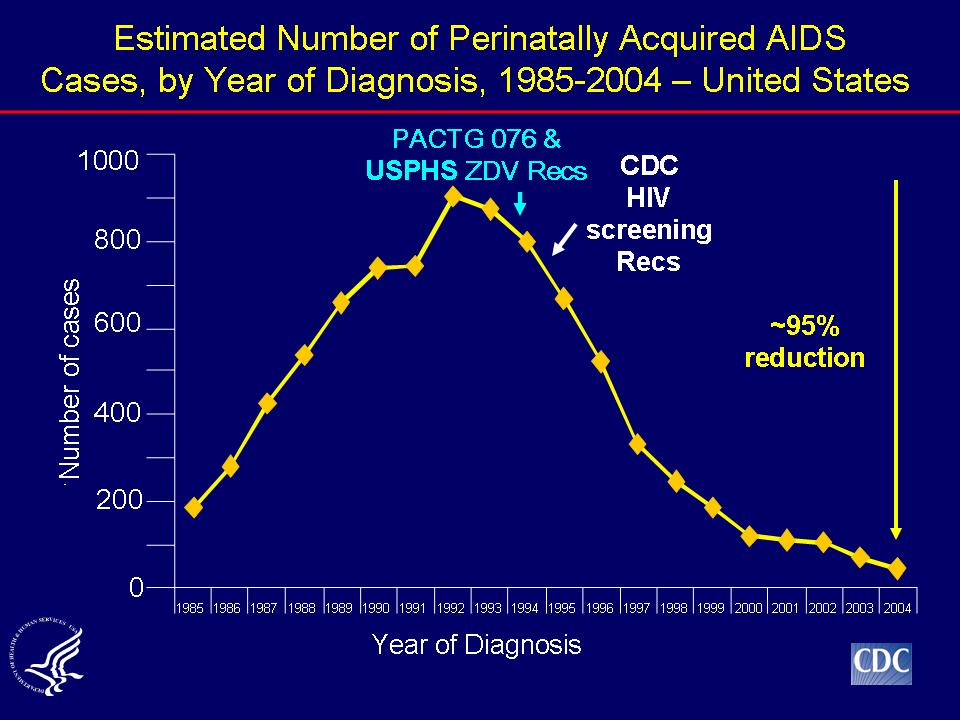
37 Perinatal HIV Transmission Risk Untreated: Approx % AZT Monotherapy: 8% Prophylactic C/S: 3-5% Combination ART: <1%
38
39 ACTG 076 Trial (U.S. and France) ZDV vs. placebo ZDV mono-therapy starting at weeks, IV ZDV intrapartum, and neonatal ZDV for 6 weeks Mother-to-Child-Transmission (MCTC) at 18 months: 8.3% in the ZDV arm 25.5% in the placebo arm
40 CDC Short-course ZDV Trial (Thailand) ZDV vs. placebo ZDV mono-therapy starting at 36 weeks (No IV ZDV, no neonatal ZDV) MTCT at 6 months: 9.4% in the ZDV arm 18.9% in the placebo arm
41 The Ditrame Trial (Cote d Ivoire, Burkina Faso) ZDV vs. placebo, Breastfeeding ZDV mono-therapy at 36 weeks, plus 1 week postpartum for mom MCTC at 6 months: 18% in the ZDV arm 27.5% in the placebo arm MCTC at 15 months: 21.5% in the ZDV arm 30.6% in the placebo arm
42 Case 1: B.P. 34 y/o Sudanese female Arrived in 2007 with known HIV diagnosis Had a 2 y/o HIV-negative son Initial labs: CD4: 14 Viral load: 195,000 Numerous striking skin lesions on her face Genital lesions positive for HSV ART started but poor adherence led to multi-class resistance
43 Case 1, Con t. Became pregnant in late 2007; G9P8 Already on lopinavir/ritonavir (Kaletra), emtracitabine/tenofovir (Truvada), and zidovudine Viral loads repeatedly < 50 copies. CD4: ~200 HGSIL Pap NSVD at 39 6/7 weeks (ART plus 076 ZDV protocol) Infant shown to be HIV negative Persistent HGSIL cervical conization scheduled, IUD to be placed at the same time
44 Case 1, Con t. 3 months later, pregnancy test positive ART: darunavir/ritonavir, emtracitabine/tenofovir (Truvada) and zidovudine CD4 s now in the 200 s-300 s EGA Details 25 weeks Viral load weeks Viral load weeks Viral load: QNS 37 weeks No show 37 ½ wks Presents to L&D with heavy bleeding
45 Case 1, Con t. Emergent classical C/S for near-complete abruption Transverse lie, difficult extraction, needle stick during closure of the wound Mom, infant, and surgeon did fine Current status: ART: darunavir, ritonavir, tenofovir and dolutegravir CD4: 651 Viral load: 48 copies ASCUS (s/p LEEP) with HPV typing negative for hi risk
46 Case 2A: S.Z. 35 y/o male Ethiopian immigrant, in the U.S. >15 years, graduated from high school in MD Presents to clinic in July 2012 with persistent cough, dysphagia, and oral thrush Rapid HIV test is positive CXR: bilat. Infiltrates subsequently dx d with PCP CD4 count: 6, HIV RNA Quant: 433,000
47 Case 2B: S.I. 34 y/o wife of S.Z. (who was diagnosed July, 2012) Delivered her second child in Sep, 2011 In December, 2011 presented to clinic and was diagnosed with pharyngitis. Fever, HA, ST, rash, and adenopathy In August, 2012 was found to be HIV positive CD4: 1191, HIV RNA: 3,400 Infant was HIV negative
48 ART: Who Gets Treated in Pregnancy? Everybody Those who require ART for their own health Those who need it only to reduce MTCT Especially Patients with acute sero-conversion Women diagnosed late in pregnancy
49 ART-Naïve Women Start immediately or as soon as possible Factors to consider Genotype CD4 count N/V related to pregnancy Patient readiness/ability to adhere NRTI backbone with one or more NRTI s that have high transplacental levels: ZDV, 3TC, FTC, TDF, ABC Nevirapine can be used is CD4 < 250
50 Women on ART Who Become Pregnant If the regimen is working, keep taking it Efavirenz: Okay to continue despite known risk of neural tube defects Nevirapine: Okay regardless of CD4 ARV resistance testing for anyone with detectable viremia (HIV RNA of > 500 copies)
51 Pre-conception Counseling in HIV Basic pre-conception issues The good old days of HIV care Risk/benefit Turkey basters and other creative options Sperm-washing Current practice: PrEP Tenofovir/emtracitabinedaily for the uninfected partner Timed intercourse; use condoms all the rest of the time
52 Mode of Delivery Scheduled C/S at 38 weeks if HIV RNA>1,000 (or unknown) Scheduled C/S not recommended if HIV RNA<1,000. (No additional risk reduction is conferred)
53 What About SROM/Labor in Patients Scheduled for C/S? Duration of ROM/labor 1996 study showed 4 hours of ROM was a significant cut-off 2001 study showed 2% increase in MTCT/hour of ROM HIV RNA level Current ART regimen
54 Intrapartum Prophylaxis Continue antepartum ART regardless of mode of delivery IV Zidovudine? Yes, if HIV RNA >1,000 (or unknown) near delivery Not required if HIV RNA <1,000 near delivery (and patient is on ART with no concerns of poor adherence) Zidovudine dose: 2 mg/kg IV over the first hour, then 1 mg/kg/hruntil cord clamp
55 OB Procedures in HIV: Avoid if Possible Antepartum: Amniocentesis Intrapartum: AROM Routine use of fetal scalp leads IUPC placement? Operative delivery Forceps Vacuum Episiotomy
56 No-Prenatal-Care Patients Presenting in Labor Rapid HIV test ASAP If positive, treat as if infected (don t wait for confirmatory test) Continue to treat infant as if mom has HIV until confirmatory test proves negative
57 What do I need to know about HAART? (Highly Active Anti-Retroviral Therapy) DRUG INTERACTIONS DRUG INTERACTIONS DRUG INTERACTIONS DRUG INTERACTIONS DRUG INTERACTIONS DRUG INTERACTIONS Be aware of side effects
58 OB Drug Interactions Methergine levels increased by Protease Inhibitors and Cobicistat-containing ARV s (CYP3A4 Inhibitors) Norvir (ritonavir) Reyataz (atazanavir) Prezista (darunavir) Kaletra (lopinavir/ritonavir) Stribild, Tybost, Prezcobix, Evotaz, Genvoya Risk of ergot toxicity, severe vasospasm, increased BP, and ischemia
59 OB Drug Interactions, Con t Methergine levels decreased by CYP3A4 inducers, leading to lack of effectiveness of methergine Sustiva, Atripla (efavirenz) Intelence (etravirine) Viramune (nevirapine) Oxytocin, misoprostol (Cytotec) and Hemabate (carboprost tromethamine) do not interact with HIV medications and may be used in women taking ART
60 Hormonal Contraception? Efavirenz, most protease inhibitors, Stribild, and to a lesser extent, nevirapine all decrease hormonal contraception levels. Raltegravir, dolutegravir and etravirine: no impact Maraviroc: serum levels increased when combined with estrogens
61 OCP s and Atazanavir Atazanavir/ritonavir: Decreases ethinyl estradiol, increases norgestimate. Need to use an OCP containing no less than 35 mcg ethinyl estradiol Atazanavir alone: Increases ethinyl estradiol 48% and increases norethindrone 110%. Need to use an OCP containing no more than 30 mcg ethinyl estradiol.
62 Drug Interactions Resources Epocrates Arv.ucsf.edu Call your clinical pharmacist
63 What About the Baby? Bathe before any injections No breastfeeding (in the developed world) Initial lab: CBC for a baseline ZDV 8 mg/kg/day divided q 12 hours Continue for 4-6 weeks (per ACTG 076), depending on risk Dosage adjustment for pre-term infants PCP prophylaxis following discontinuation of ZDV, based on risk Follow-up labs: HIV-1 RNA (Quant): At days, 1-2 months and 4-6 months of age. CBC at 1 month Standard HIV EIA at months of age to ensure serodeconversion
64 Case 3: D.T. 26 y/o female refugee from Liberia Arrived in SF in 2008 Found to be HIV positive Initial numbers: CD4: 1,020 HIV RNA: 229,000 Patient essentially in denial about HIV dx
65 Case 3, (Con t) Date CD ,
66 Case 3 (Con t) G1Po presented for OB care in early 2 nd trimester, EDC of Oral thrush, ill-appearing, perineal ulcer: HSV Briefly took Atripla Genotype showed NNRTI resistance Refused to take any more ARV s Did take prophylactic meds for PCP and MAC Primary C/S scheduled at 38 weeks (pt declines) Presented in labor at 38 3/7, intact membranes, 5 cm
67 Case 3 (Con t) Received ZDV 2 mg/kg bolus over 1 hour Primary C/S performed without difficulty Apgars 8 and 9 Medically unremarkable postpartum and neonatal course. Baby confirmed to be HIV negative at 4 months of age
68 Perinatal Guidelines
69 Objectives 1. Discuss the current status of the statewide, nationwide and worldwide HIV/AIDS epidemics. 2. Describe the impact of HIV on the management of the pregnant patient. 3. Discuss Pre- and Post-Exposure Prophylaxis for HIV.
70 Post-Exposure Prophylaxis What do I tell my patient? What do I tell my spouse? What do I tell my self?
71 Reported Blood and Body Fluid Exposures by Profession Nurses: 48.6% Residents and fellows: 7.7% Attendings: 7.7% Non-lab techs: 4.5% Resp. therapists: 3.6% CNA s: 3.2%
72 Occupational Exposure: Risk of HIV Transmission Percutaneous: 20/6,135 (0.33%) Mucosal: 1/1,143 (0.09%) Intact Skin: 0/2,712
73 Fear the Fluids? Implicated fluids: blood, semen, vaginal secretions and fluids with visible blood. Potentially infectious: CSF, synovial, pleural, peritoneal, pericardial, and amniotic fluid. Considered safe: feces, nasal secretions, saliva, gastric secretions, sputum, sweat, tears, urine, and vomitus.
74 Estimated Per Act Risk of HIV Acquisition by Exposure Route (per 10,000 exposures) Blood transfusion: 9,000 Needle sharing (IVDU): 67 Receptive/insertive anal IC: 50/6.5 Needle stick: 30 Receptive/insertive penile/vaginal IC: 10/5 Receptive/insertive penile/oral IC: 1/0.5
75 Sexual Assault Risks and benefits of HIV prophylaxis should be discussed with every sexual assault patient No good data, but case reports of HIV seroconversion from sexual assault exist
76 HIV in Sexual Assault: A Little Perspective Risk of transmission from single episode of consensual vaginal intercourse with HIV positive man: 0.1% Risk of transmission from single episode of consensual anal intercourse with HIV positive man: 2%
77 High Risk Sexual Assault Male on male rapists Location in a high-prevalence region or country Multiple assailants Anal sexual assault Sexual assaults where either the assailant or the victim has trauma, bleeding or genital lesions
78 Post-Exposure Prophylaxis (PEP) Usually NOT indicated Rapid HIV test for source patient, if possible Initiation: sooner is better Goal is within 1-2 hours Benefit decreased after hours Not recommended after 72 hours Duration: 4 weeks (arbitrary) PEPline:
79 Pre-Exposure Prophylaxis (PrEP) Tenofovir/emtracitabine (Truvada) approved in 2012 for use in HIV-uninfected individuals at substantial risk of HIV acquisition. HIV sero-disconcordant couples HIV negative partner in a couple wishing to conceive Criteria for PrEP Proven to be HIV-negative Must be able to strictly adhere to a daily med regimen Must be tested for HIV at least every 3 months
80 Resources -HIV Telephone Consultation Service: (Mon-Fri, Central Time) -Perinatal HIV Hotline: PEPline: (7 days/week, Central Time) -PrEPline: (855-HIV-PReP) (Mon-Fri, Central Time) -
HIV MEDICATIONS AT A GLANCE. Atripla 600/200/300 mg tablet tablet daily. Complera 200/25/300 mg tablet tablet daily
 HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/
HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/
HIV Drugs and the HIV Lifecycle
 HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
HIV and Psychiatry: The 2016 Update. 16 September, 2016
 HIV and Psychiatry: The 2016 Update 16 September, 2016 C.W. Shafer, MD HIV Specialist, AAHIVM Sioux Falls Family Medicine Residency Center for Family Medicine/Falls Community Health Sioux Falls, SD Objectives
HIV and Psychiatry: The 2016 Update 16 September, 2016 C.W. Shafer, MD HIV Specialist, AAHIVM Sioux Falls Family Medicine Residency Center for Family Medicine/Falls Community Health Sioux Falls, SD Objectives
U.S. DEPARTMENT OF HUD 04/11/2017 STATE: SOUTH DAKOTA ADJUSTED HOME INCOME LIMITS
 Rapid City, SD HUD Metro FMR Area Custer County, SD HUD Metro FMR Area 30% LIMITS 13650 15600 17550 19500 21100 22650 24200 25750 VERY LOW INCOME 22750 26000 29250 32500 35100 37700 40300 42900 60% LIMITS
Rapid City, SD HUD Metro FMR Area Custer County, SD HUD Metro FMR Area 30% LIMITS 13650 15600 17550 19500 21100 22650 24200 25750 VERY LOW INCOME 22750 26000 29250 32500 35100 37700 40300 42900 60% LIMITS
1 PERSON 2 PERSON 3 PERSON 4 PERSON 5 PERSON 6 PERSON 7 PERSON 8 PERSON
 Rapid City, SD HUD Metro FMR Area 30% LIMITS 14750 16850 18950 21050 22750 24450 26150 27800 VERY LOW INCOME 24550 28050 31550 35050 37900 40700 43500 46300 60% LIMITS 29460 33660 37860 42060 45480 48840
Rapid City, SD HUD Metro FMR Area 30% LIMITS 14750 16850 18950 21050 22750 24450 26150 27800 VERY LOW INCOME 24550 28050 31550 35050 37900 40700 43500 46300 60% LIMITS 29460 33660 37860 42060 45480 48840
HIV Management Update 2015
 9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
Antiretroviral Dosing in Renal Impairment
 Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
THE HIV LIFE CYCLE. Understanding How Antiretroviral Medications Work
 THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION
 WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION A1. PARTICIPANT ID: ENTER NUMBER HERE - - - ONLY IF ID LABEL IS NOT AVAILABLE A2. VISIT #: A3. VERSION DATE: 1 0 /
WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION A1. PARTICIPANT ID: ENTER NUMBER HERE - - - ONLY IF ID LABEL IS NOT AVAILABLE A2. VISIT #: A3. VERSION DATE: 1 0 /
Nothing to disclose.
 Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital HIV UPDATE FOR THE PRIMARY CARE PROVIDER Nothing to disclose. 1 Outline Epidemiology Screening / testing for HIV
Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital HIV UPDATE FOR THE PRIMARY CARE PROVIDER Nothing to disclose. 1 Outline Epidemiology Screening / testing for HIV
Blood-Borne Pathogens and Post-Exposure Prophylaxis
 Blood-Borne Pathogens and Post-Exposure Prophylaxis Christopher Behrens MD Northwest Association of Occupational and Environmental Medicine October 2017 with thanks to Shireesha Dhanireddy MD Disclosures
Blood-Borne Pathogens and Post-Exposure Prophylaxis Christopher Behrens MD Northwest Association of Occupational and Environmental Medicine October 2017 with thanks to Shireesha Dhanireddy MD Disclosures
An HIV Update Jan Clark, PharmD Specialty Practice Pharmacist
 An HIV Update - 2019 Jan Clark, PharmD Specialty Practice Pharmacist 2 The goal of this program is to provide a review and update of HIV care and to provide a forum for discussing the current local and
An HIV Update - 2019 Jan Clark, PharmD Specialty Practice Pharmacist 2 The goal of this program is to provide a review and update of HIV care and to provide a forum for discussing the current local and
HIV Update Objectives. Epidemiology. Epidemiology, Transmission and Natural History. Transmission Risk by Exposure. Transmission 9/29/2014
 Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
WOMEN'S INTERAGENCY HIV STUDY METABOLIC STUDY: MS01 SPECIMEN COLLECTION FORM
 WOMEN'S INTERAGENCY HIV STUDY METABOLIC STUDY: MS01 SPECIMEN COLLECTION FORM ID LABEL HERE ---> VERSION DATE 10/01/07 - - - VISIT #: FORM COMPLETED BY: A1. DATE OF BLOOD DRAW: / / M D Y A2. Do you take
WOMEN'S INTERAGENCY HIV STUDY METABOLIC STUDY: MS01 SPECIMEN COLLECTION FORM ID LABEL HERE ---> VERSION DATE 10/01/07 - - - VISIT #: FORM COMPLETED BY: A1. DATE OF BLOOD DRAW: / / M D Y A2. Do you take
0.14 ( 0.053%) UNAIDS 10% (94) ( ) (73-94/6 ) 8,920
 UNAIDS 10% (94) ( ) (73-94/6 ) 8,920") 0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
ANTIRETROVIRAL TREATMENTS (Part 1of
 CCR5 CO-RECEPTOR ANTAGONISTS maraviroc (MVC) Selzentry 25mg, 75mg, FUSION INHIBITORS 20mg/mL ANTIRETROVIRAL TREATMENTS (Part 1of 5) oral soln enfuvirtide (ENF, T-20) Fuzeon 90mg/mL pwd for SC inj after
CCR5 CO-RECEPTOR ANTAGONISTS maraviroc (MVC) Selzentry 25mg, 75mg, FUSION INHIBITORS 20mg/mL ANTIRETROVIRAL TREATMENTS (Part 1of 5) oral soln enfuvirtide (ENF, T-20) Fuzeon 90mg/mL pwd for SC inj after
Daclatasvir (Daklinza ) Drug Interactions with HIV Medications
 Drug Interactions with HIV Medications") Daclatasvir/Sofosbuvir (Daklinza /Sovaldi TM ) Drug Interactions A Quick Guide for Clinicians April 2017 John J Faragon, PharmD, BCPS, AAHIVP Mechanism of Action and Route of Metabolism for Daclatasvir
Daclatasvir/Sofosbuvir (Daklinza /Sovaldi TM ) Drug Interactions A Quick Guide for Clinicians April 2017 John J Faragon, PharmD, BCPS, AAHIVP Mechanism of Action and Route of Metabolism for Daclatasvir
HIV medications HIV medication and schedule plan
 Living with HIV (human immunodeficiency virus) It may be scary to find out that you re HIV-positive or have AIDS. Coping with this news may be difficult. Although HIV is a serious infection, people with
Living with HIV (human immunodeficiency virus) It may be scary to find out that you re HIV-positive or have AIDS. Coping with this news may be difficult. Although HIV is a serious infection, people with
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care
 Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 03/07/18 SECTION: DRUGS LAST REVIEW DATE: 02/19/19 LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
Obstetrics and HIV An Update. Jennifer Van Horn MD University of Utah
 Obstetrics and HIV An Update Jennifer Van Horn MD University of Utah Obstetrics and HIV Perinatal transmission Testing Antiretroviral therapy Antepartum management Intrapartum management Postpartum management
Obstetrics and HIV An Update Jennifer Van Horn MD University of Utah Obstetrics and HIV Perinatal transmission Testing Antiretroviral therapy Antepartum management Intrapartum management Postpartum management
24/7 SOBRIETY PROJECT
 24/7 SOBRIETY PROJECT OFFICE OF ATTORNEY GENERAL LARRY LONG State Program Coordinator Bill Mickelson SOUTH DAKOTA 24/7 PROJECT Harding Perkins Corson Campbell McPherson Brown Marshall Roberts Walworth
24/7 SOBRIETY PROJECT OFFICE OF ATTORNEY GENERAL LARRY LONG State Program Coordinator Bill Mickelson SOUTH DAKOTA 24/7 PROJECT Harding Perkins Corson Campbell McPherson Brown Marshall Roberts Walworth
HIV Infection & AIDS in Low- and Middle-Income Countries
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 25: HIV Infection & AIDS in Low- and Middle-Income Countries Author P. Van de Perre, MD, PhD Chapter Editor Michelle Doll, MD, MPH Topic Outline Key Issues
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 25: HIV Infection & AIDS in Low- and Middle-Income Countries Author P. Van de Perre, MD, PhD Chapter Editor Michelle Doll, MD, MPH Topic Outline Key Issues
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications
 and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications") Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Antiretrovial Crushable/Liquid Formulation Chart
 Antiretrovial Crushable/Liquid Formulation Chart Eliza Dollard, PharmD; Nafeesa Chin-Beckford, PharmD; Laura Aragon, PharmD Last Updated: 04/2016 Agent How Supplied Crushable Status **Products listed in
Antiretrovial Crushable/Liquid Formulation Chart Eliza Dollard, PharmD; Nafeesa Chin-Beckford, PharmD; Laura Aragon, PharmD Last Updated: 04/2016 Agent How Supplied Crushable Status **Products listed in
continuing education for pharmacists
 continuing education for pharmacists HIV/AIDS: Overview and Resources for Pharmacists Mona T. Thompson, R.Ph., PharmD Volume XXXIII, No. 9 Dr. Mona T. Thompson has no relevant financial relationships to
continuing education for pharmacists HIV/AIDS: Overview and Resources for Pharmacists Mona T. Thompson, R.Ph., PharmD Volume XXXIII, No. 9 Dr. Mona T. Thompson has no relevant financial relationships to
WELCOME Substance Abuse Prevention Specialist Training
 WELCOME Substance Abuse Prevention Specialist Training When working in ATOD prevention do you ever feel like this? Or this..? Or maybe this..? During the course of our time together, we have a very important
WELCOME Substance Abuse Prevention Specialist Training When working in ATOD prevention do you ever feel like this? Or this..? Or maybe this..? During the course of our time together, we have a very important
ADAP Monitoring Provider Prescribing Patterns. Amanda Bowes, NASTAD Christine Rivera and Dr. Charles Gonzalez, NYS AIDS Institute
 ADAP Monitoring Provider Prescribing Patterns Amanda Bowes, NASTAD Christine Rivera and Dr. Charles Gonzalez, NYS AIDS Institute WEBINAR ETIQUETTE All questions or comments can be shared either via the
ADAP Monitoring Provider Prescribing Patterns Amanda Bowes, NASTAD Christine Rivera and Dr. Charles Gonzalez, NYS AIDS Institute WEBINAR ETIQUETTE All questions or comments can be shared either via the
HIV THERAPY STRATEGIES FOR THIRD LINE. issues to consider when faced with few drug options
 STRATEGIES FOR THIRD LINE HIV THERAPY issues to consider when faced with few drug options A PUBLICATION FROM Information, Inspiration and Advocacy for People Living With HIV/AIDS MAY 2008 Most people living
STRATEGIES FOR THIRD LINE HIV THERAPY issues to consider when faced with few drug options A PUBLICATION FROM Information, Inspiration and Advocacy for People Living With HIV/AIDS MAY 2008 Most people living
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
The ART of Antiretroviral Therapy in Critically-ill Patients with HIV
 The ART of Antiretroviral Therapy in Critically-ill Patients with HIV Tyler Finocchio, PharmD, BCPS PGY2 Critical Care Pharmacy Resident Avera McKennan Hospital & University Health Center February 10 th,
The ART of Antiretroviral Therapy in Critically-ill Patients with HIV Tyler Finocchio, PharmD, BCPS PGY2 Critical Care Pharmacy Resident Avera McKennan Hospital & University Health Center February 10 th,
October 26-28: Training Day 1
 Peer Linkage and Re-Engagement of HIV- Positive Women of Color October 26-28: Training Day 1 Peer Linkage and Re -Engagement of HIV - Positive Women of Color Convening Training Trainers Today: Alicia Downes
Peer Linkage and Re-Engagement of HIV- Positive Women of Color October 26-28: Training Day 1 Peer Linkage and Re -Engagement of HIV - Positive Women of Color Convening Training Trainers Today: Alicia Downes
Nobel /03/28. HIV virus and infected CD4+ T cells
 Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
Guidance for Non-HIV-Specialized Providers Caring for Persons with HIV Displaced by Disasters
 Guidance for Non-HIV-Specialized Providers Caring for Persons with HIV Displaced by Disasters Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidance for Non-HIV-Specialized Providers Caring for Persons with HIV Displaced by Disasters Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Selecting an Initial Antiretroviral Therapy (ART) Regimen
 Regimen") Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
OB/GYN CHART REVIEW DRAFT: NOT FOR DISTRTIBUTION
 OB/GYN CHART REVIEW A summary of OB/GYN clinical chart review results designed to monitor the quality of care provided by a Ryan White funded OB/GYN primary care site as part of the Atlanta EMA s quality
OB/GYN CHART REVIEW A summary of OB/GYN clinical chart review results designed to monitor the quality of care provided by a Ryan White funded OB/GYN primary care site as part of the Atlanta EMA s quality
Medscape's Antiretroviral Pocket Guide for the Treatment of HIV Infection
 Table 3. Characteristics of Nucleoside Reverse Transcriptase Inhibitors (NRTIs) Generic Name (Abbreviation) / Trade Name Abacavir (ABC) / Ziagen Trizivir with ZDV + 3TC Epzicom with 3TC Didanosine (ddi)
Table 3. Characteristics of Nucleoside Reverse Transcriptase Inhibitors (NRTIs) Generic Name (Abbreviation) / Trade Name Abacavir (ABC) / Ziagen Trizivir with ZDV + 3TC Epzicom with 3TC Didanosine (ddi)
Approach for the Newly Diagnosed HIV Positive Patient
 Approach for the Newly Diagnosed HIV Positive Patient Jason E. Farley, PhD, MPH, ANP-BC, FAAN, AACRN Associate Professor & NP, Johns Hopkins University School of Nursing & Medicine Director, AETC Adult-Gerontology
Approach for the Newly Diagnosed HIV Positive Patient Jason E. Farley, PhD, MPH, ANP-BC, FAAN, AACRN Associate Professor & NP, Johns Hopkins University School of Nursing & Medicine Director, AETC Adult-Gerontology
Appropriate Use & Safety Edits
 Appropriate Use & Safety Edits Envolve Pharmacy Solutions provides a variety of safety edits to promote the use of the right medication, in the right patient, at the right time. These edits are routinely
Appropriate Use & Safety Edits Envolve Pharmacy Solutions provides a variety of safety edits to promote the use of the right medication, in the right patient, at the right time. These edits are routinely
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Fluconazole dimenhydrinate, diphenhydramine. Raltegravir or dolutegravir with antacids
 Supportive therapy Summary of interactions Table 1. Summary of potential interactions between antiretroviral agents and supportive therapy Interactions with enzyme inhibitors (protease inhibitors and elvitegravir/cobicistat)
Supportive therapy Summary of interactions Table 1. Summary of potential interactions between antiretroviral agents and supportive therapy Interactions with enzyme inhibitors (protease inhibitors and elvitegravir/cobicistat)
HIV/AIDS Prenatal Care for HIV+ Mothers. 1. Algorithm for Prenatal Screening & Care (Antepartum)
") 1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+ Mothers a.
1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+ Mothers a.
HIV/AIDS Prenatal Care for HIV+ Mothers. 1. Algorithm for Prenatal Screening & Care (Antepartum)
") 7/10/18 njm 1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+
7/10/18 njm 1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+
HIV THERAPY STRATEGIES FOR FIRST LINE. issues to think about when going on therapy for the first time
 STRATEGIES FOR FIRST LINE HIV THERAPY issues to think about when going on therapy for the first time A PUBLICATION FROM Information, Inspiration and Advocacy for People Living With HIV/AIDS MAY 2008 Deciding
STRATEGIES FOR FIRST LINE HIV THERAPY issues to think about when going on therapy for the first time A PUBLICATION FROM Information, Inspiration and Advocacy for People Living With HIV/AIDS MAY 2008 Deciding
HIV Treatment Guidelines
 HIV Treatment Guidelines Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject What Are Treatment Guidelines? Issued by variety of global and country-based
HIV Treatment Guidelines Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject What Are Treatment Guidelines? Issued by variety of global and country-based
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
HIV basics. Katya Calvo Medical Director of Antimicrobial Stewardship
 HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
Labor & Delivery Management for Women Living with HIV. Pooja Mittal, DO Lisa Rahangdale, MD
 Labor & Delivery Management for Women Living with HIV Pooja Mittal, DO Lisa Rahangdale, MD Statistics for Perinatally Acquired HIV Timing of Perinatal HIV Transmission Most transmission occurs close to
Labor & Delivery Management for Women Living with HIV Pooja Mittal, DO Lisa Rahangdale, MD Statistics for Perinatally Acquired HIV Timing of Perinatal HIV Transmission Most transmission occurs close to
The Future of HIV: Advances in Drugs and Research. Shauna Gunaratne December 17, 2018
 The Future of HIV: Advances in Drugs and Research Shauna Gunaratne December 17, 2018 Overview Epidemiology Science of HIV How HIV treatment and management have changed over the years New medicines and
The Future of HIV: Advances in Drugs and Research Shauna Gunaratne December 17, 2018 Overview Epidemiology Science of HIV How HIV treatment and management have changed over the years New medicines and
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV
 POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
 Page 1 of 5 ENLGLISH / ESPAÑOL / PORTUGUÉS / FRANÇAIS Share 3 Drug Chart for HIV Treatment CURRENT EDITION ABOUT SENSE BACK ISSUES MSMGF HOME CONTACT US There are a number of antiretroviral (ARV) medications
Page 1 of 5 ENLGLISH / ESPAÑOL / PORTUGUÉS / FRANÇAIS Share 3 Drug Chart for HIV Treatment CURRENT EDITION ABOUT SENSE BACK ISSUES MSMGF HOME CONTACT US There are a number of antiretroviral (ARV) medications
Midwestern Underwriting Conference 2016
 UNDERWRITING HIV: THE FAIRY TALE HAS BECOME REALITY Midwestern Underwriting Conference 2016 Jean-Marc Fix, FSA, MAAA VP, R&D, Optimum Re Insurance Co. AGENDA Where are we with HIV? The risk The ideal case
UNDERWRITING HIV: THE FAIRY TALE HAS BECOME REALITY Midwestern Underwriting Conference 2016 Jean-Marc Fix, FSA, MAAA VP, R&D, Optimum Re Insurance Co. AGENDA Where are we with HIV? The risk The ideal case
NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION. Jason E. Vercher, PA-C, AAHIVM
 NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION Jason E. Vercher, PA-C, AAHIVM Disclosures No disclosures to report Learning Objectives q Identify Individuals who would benefit from non-occupational
NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION Jason E. Vercher, PA-C, AAHIVM Disclosures No disclosures to report Learning Objectives q Identify Individuals who would benefit from non-occupational
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING**, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir) Stavudine
COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir) Stavudine
Sculpting a Better Regimen: The ART of HIV Medications
 Sculpting a Better Regimen: The ART of HIV Medications Kelly Peddy, PharmD, MPA Clinical Pharmacy Specialist - Ambulatory Care Memorial Hospital of South Bend November 30, 2017 For HealthTrust Members
Sculpting a Better Regimen: The ART of HIV Medications Kelly Peddy, PharmD, MPA Clinical Pharmacy Specialist - Ambulatory Care Memorial Hospital of South Bend November 30, 2017 For HealthTrust Members
Obstetric Complications in HIV-Infected Women. Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School
 Obstetric Complications in HIV-Infected Women Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School Obstetric Complications and HIV Obstetric complications are not increased in
Obstetric Complications in HIV-Infected Women Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School Obstetric Complications and HIV Obstetric complications are not increased in
NON-OCCUPATIONAL POST EXPOSURE PREVENTION. when you think you were exposed to hiv within the past three days
 NON-OCCUPATIONAL POST EXPOSURE PREVENTION when you think you were exposed to hiv within the past three days A PUBLICATION FROM Information, Inspiration and Advocacy for People Living With HIV/AIDS MAY
NON-OCCUPATIONAL POST EXPOSURE PREVENTION when you think you were exposed to hiv within the past three days A PUBLICATION FROM Information, Inspiration and Advocacy for People Living With HIV/AIDS MAY
JULUCA (dolutegravir sodium-rilpivirine hydrochloride) oral tablet
 oral tablet") JULUCA (dolutegravir sodium-rilpivirine hydrochloride) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
JULUCA (dolutegravir sodium-rilpivirine hydrochloride) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
World AIDS Day Year-by-Year Milestones in HIV/AIDS. healthlibrary
 World AIDS Day 2014 Year-by-Year Milestones in HIV/AIDS (Adapted from The POZ Timeline: Milestones in the HIV/AIDS Pandemic with additions compiled by Eric Brus, Director of HIV Health Promotion, AIDS
World AIDS Day 2014 Year-by-Year Milestones in HIV/AIDS (Adapted from The POZ Timeline: Milestones in the HIV/AIDS Pandemic with additions compiled by Eric Brus, Director of HIV Health Promotion, AIDS
U=U NHIVNA HIV, Fertility and Contraception in the era of
 HIV, Fertility and Contraception in the era of U=U NHIVNA 2018 Yvonne Gilleece Consultant in HIV and Sexual Health Brighton &Sussex University Hospitals NHS Trust Honorary Senior Lecturer Brighton & Sussex
HIV, Fertility and Contraception in the era of U=U NHIVNA 2018 Yvonne Gilleece Consultant in HIV and Sexual Health Brighton &Sussex University Hospitals NHS Trust Honorary Senior Lecturer Brighton & Sussex
HIV/AIDS Update 2007
 HIV/AIDS Update 2007 Joanne J. Orrick, Pharm.D., BCPS Clinical Assistant Professor University of Florida Faculty, Florida/Caribbean AIDS Education and Training Center orricjj@ufl.edu www.faetc.org orricjj@ufl.edu
HIV/AIDS Update 2007 Joanne J. Orrick, Pharm.D., BCPS Clinical Assistant Professor University of Florida Faculty, Florida/Caribbean AIDS Education and Training Center orricjj@ufl.edu www.faetc.org orricjj@ufl.edu
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update
 Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
 Antiretroviral Medications: What you need to know Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Associate Professor, Department of Pharmacy Practice Jefferson College of Pharmacy, Thomas Jefferson University
Antiretroviral Medications: What you need to know Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Associate Professor, Department of Pharmacy Practice Jefferson College of Pharmacy, Thomas Jefferson University
MEDICATION RELATED ISSUES IN THE HIV PATIENT. LEONARD SOWAH, MBChB, MPH, FACP
 MEDICATION RELATED ISSUES IN THE HIV PATIENT LEONARD SOWAH, MBChB, MPH, FACP Overview Evalua;on and ini;al of a HIV pa;ent with respect to medica;ons Triaging of pa;ent to determine ideal follow up plan
MEDICATION RELATED ISSUES IN THE HIV PATIENT LEONARD SOWAH, MBChB, MPH, FACP Overview Evalua;on and ini;al of a HIV pa;ent with respect to medica;ons Triaging of pa;ent to determine ideal follow up plan
PrE-Exposure Prophylaxis (PrEP) A Tool at Your Hand to Fight HIV
 A Tool at Your Hand to Fight HIV") PrE-Exposure Prophylaxis (PrEP) A Tool at Your Hand to Fight HIV Laura Beauchamps, MD Assistant Professor Division of Infectious Diseases University of Mississippi Medical Center Principal Investigator
PrE-Exposure Prophylaxis (PrEP) A Tool at Your Hand to Fight HIV Laura Beauchamps, MD Assistant Professor Division of Infectious Diseases University of Mississippi Medical Center Principal Investigator
Drug Treatment Program Update
 Drug Treatment Program Update As of March 211 Drug Treatment Program Update A key component of the Centre s mandate is to monitor the impact of HIV/AIDS on British Columbia. The Centre provides essential
Drug Treatment Program Update As of March 211 Drug Treatment Program Update A key component of the Centre s mandate is to monitor the impact of HIV/AIDS on British Columbia. The Centre provides essential
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop
 HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
Preventing Mother to Child HIV Transmission: Are We There Yet?!'
 Preventing Mother to Child HIV Transmission: Are We There Yet?!' 2017 Michigan Clincal Nursing Conference for HIV and STD Care May 18, 2017 Frankenmuth MI 1 Theodore B. Jones, MD Maternal Fetal Medicine
Preventing Mother to Child HIV Transmission: Are We There Yet?!' 2017 Michigan Clincal Nursing Conference for HIV and STD Care May 18, 2017 Frankenmuth MI 1 Theodore B. Jones, MD Maternal Fetal Medicine
Genotyping and Drug Resistance in Clinical Practice. Case Studies
 Genotyping and Drug Resistance in Clinical Practice Case Studies 12/02 40 year old Hispanic male Dx with HIV 1995 + Hx of PCP > 1x, HepC Medication history: AZT, Crixivan, Videx EC, Sustiva, Zerit, Ziagen,
Genotyping and Drug Resistance in Clinical Practice Case Studies 12/02 40 year old Hispanic male Dx with HIV 1995 + Hx of PCP > 1x, HepC Medication history: AZT, Crixivan, Videx EC, Sustiva, Zerit, Ziagen,
Register for notification of guideline updates at
 Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States Visit the AIDSinfo website
Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States Visit the AIDSinfo website
HIV in in Women Women
 HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
Matters of the HAART: An Update on Current Treatment Options for HIV
 Matters of the HAART: An Update on Current Treatment Options for HIV Jason Alegro, PharmD, BCPS Assistant Professor of Clinical Sciences, Roosevelt University Infectious Diseases Clinical Pharmacy Specialist,
Matters of the HAART: An Update on Current Treatment Options for HIV Jason Alegro, PharmD, BCPS Assistant Professor of Clinical Sciences, Roosevelt University Infectious Diseases Clinical Pharmacy Specialist,
A Fatal Imbalance. Tropical diseases: 18 new drugs (incl. 8 for malaria) 1.3% 21 new drugs for neglected diseases. Tuberculosis: 3 new drugs
 1.3% 21 new drugs for neglected diseases. Tuberculosis: 3 new drugs") ADDRESSING GAPS IN INNOVATION FOR NEGLECTED PATIENTS: DNDI ANDPEDIATRIC HIV/AIDS Rachel Cohen, Regional Executive Director, DNDi North America Proposals for a Global Innovation System that Responds to
ADDRESSING GAPS IN INNOVATION FOR NEGLECTED PATIENTS: DNDI ANDPEDIATRIC HIV/AIDS Rachel Cohen, Regional Executive Director, DNDi North America Proposals for a Global Innovation System that Responds to
treatment passport 1
 treatment passport 1 Why keep a treatment history? Keeping a short record of your treatment history can help in many ways. It can help you understand your health and treatment. It can help if your doctor
treatment passport 1 Why keep a treatment history? Keeping a short record of your treatment history can help in many ways. It can help you understand your health and treatment. It can help if your doctor
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course
 Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
ALABAMA S ADAP FORMULARY OFFERS 117 MEDICATIONS
 ALABAMA S ADAP FORMULARY OFFERS 117 MEDICATIONS - 2014 Alabama s ADAP formulary offers a minimum of one medication from each HIV antiretroviral class approved by the U.S. Food and Drug Administration (FDA).
ALABAMA S ADAP FORMULARY OFFERS 117 MEDICATIONS - 2014 Alabama s ADAP formulary offers a minimum of one medication from each HIV antiretroviral class approved by the U.S. Food and Drug Administration (FDA).
I. HIV Epidemiology. HIV Infection A Primer. Objectives. Disclosures 7/18/2014
 Objectives HIV Infection A Primer Discuss the worldwide and domestic epidemiology of HIV infection Review HIV Biology Review HIV Transmission and Prevention Review HIV diagnosis Describe the approaches
Objectives HIV Infection A Primer Discuss the worldwide and domestic epidemiology of HIV infection Review HIV Biology Review HIV Transmission and Prevention Review HIV diagnosis Describe the approaches
Exploring HIV in 2017: What a pharmacist needs to know
 Exploring HIV in 2017: What a pharmacist needs to know Lifecycle of the HIV virus a. HIV spread through mucous membrane contact, damaged tissue contact, or blood contact with: blood, semen, rectal fluids,
Exploring HIV in 2017: What a pharmacist needs to know Lifecycle of the HIV virus a. HIV spread through mucous membrane contact, damaged tissue contact, or blood contact with: blood, semen, rectal fluids,
PREVENTION OF HIV IN THE TIMES OF PREP. Daniela Chiriboga, MD Florida Department of Health in Polk County
 PREVENTION OF HIV IN THE TIMES OF PREP Daniela Chiriboga, MD Florida Department of Health in Polk County MAKING THE CASE FOR PREVENTION The Epidemic in Florida Population in 2014: 19.6 million (3 rd in
PREVENTION OF HIV IN THE TIMES OF PREP Daniela Chiriboga, MD Florida Department of Health in Polk County MAKING THE CASE FOR PREVENTION The Epidemic in Florida Population in 2014: 19.6 million (3 rd in
What s New. In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group
 What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
When to Start ART. Reduction in HIV transmission. ? Reduction in HIV-associated inflammation and associated complications» i.e. CV disease, neuro, etc
 When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
HIV and PEP. LTC Rose Ressner WRNMMC ID staff Oct 2014 UNCLASSIFIED
 HIV and PEP LTC Rose Ressner WRNMMC ID staff Oct 2014 UNCLASSIFIED Disclaimer The views expressed in this presentation are those of the speaker and do not reflect the official policy of the Department
HIV and PEP LTC Rose Ressner WRNMMC ID staff Oct 2014 UNCLASSIFIED Disclaimer The views expressed in this presentation are those of the speaker and do not reflect the official policy of the Department
The ART of Managing Drug-Drug Interactions in Patients with HIV
 The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
2016 Perinatal Treatment Guidelines Update
 Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
BHIVA ART Guideline 2014 update: SEARCH PROTOCOL: main databases search
 BHIVA ART Guideline 2014 update: SEARCH PROTOCOL: main databases search Search 1 :When to Initiate ART Covers Questions 1-5 including to prevent transmission Component Description Review area Objectives
BHIVA ART Guideline 2014 update: SEARCH PROTOCOL: main databases search Search 1 :When to Initiate ART Covers Questions 1-5 including to prevent transmission Component Description Review area Objectives
Overview of HIV. LTC Paige Waterman
 Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
Perinatal Care and Prevention. Jennifer Janelle, MD Assistant Professor of Medicine University of Florida at Gainesville
 Perinatal Care and Prevention Jennifer Janelle, MD Assistant Professor of Medicine University of Florida at Gainesville Objectives Develop patient centered, team based, treatment and delivery plans to
Perinatal Care and Prevention Jennifer Janelle, MD Assistant Professor of Medicine University of Florida at Gainesville Objectives Develop patient centered, team based, treatment and delivery plans to
HIV Overview. Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program
 HIV Overview Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program www.hivresearch.org 1 Outline HIV Virology, Transmission, and Pathogenesis
HIV Overview Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program www.hivresearch.org 1 Outline HIV Virology, Transmission, and Pathogenesis
Prevention of Perinatal HIV Transmission
 Prevention of Perinatal HIV Transmission Emily Adhikari, MD Division of Maternal-Fetal Medicine Obstetrics and Gynecology University of Texas Southwestern Medical Center February 20, 2018 None Understand
Prevention of Perinatal HIV Transmission Emily Adhikari, MD Division of Maternal-Fetal Medicine Obstetrics and Gynecology University of Texas Southwestern Medical Center February 20, 2018 None Understand
2015 OPSC Annual Convention. syllabus. February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California
 2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California SUNDAY, FEBRUARY 8, 2015: 10:00am - 11:00am Primary Care of the HIV Patient Presented by Jim Lee,
2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California SUNDAY, FEBRUARY 8, 2015: 10:00am - 11:00am Primary Care of the HIV Patient Presented by Jim Lee,
Antiretroviral Pregnancy Registry
 Preterm Birth, low birth weight and fetal antiretroviral exposure: Estimated gestational age and birth weight data from singleton live births, 1989 through 31 January 2009 K. Beckerman, J. Albano, M. Martinez-Tristani,
Preterm Birth, low birth weight and fetal antiretroviral exposure: Estimated gestational age and birth weight data from singleton live births, 1989 through 31 January 2009 K. Beckerman, J. Albano, M. Martinez-Tristani,
Approach to a Patient Newly Diagnosed with HIV, Including ART Basics Rajesh T. Gandhi, M.D.
 Approach to a Patient Newly Diagnosed with HIV, Including ART Basics Rajesh T. Gandhi, M.D. Disclosures: grant support from Gilead, Roche, EBSCO Objectives Apply current guidelines to initial evaluation
Approach to a Patient Newly Diagnosed with HIV, Including ART Basics Rajesh T. Gandhi, M.D. Disclosures: grant support from Gilead, Roche, EBSCO Objectives Apply current guidelines to initial evaluation
Medication Errors Focus on the HIV-Infected Patient
 Medication Errors Focus on the HIV-Infected Patient Nimish Patel, Pharm.D., Ph.D., AAHIVP Associate Professor Albany College of Pharmacy & Health Sciences I do not have any conflict of interest in relation
Medication Errors Focus on the HIV-Infected Patient Nimish Patel, Pharm.D., Ph.D., AAHIVP Associate Professor Albany College of Pharmacy & Health Sciences I do not have any conflict of interest in relation
Human Immunodeficiency Virus (HIV)
") HIV INFECTION! Human Immunodeficiency Virus (HIV) Infects human cells and causes gradual loss of immune system function, and these immune alterations predispose to the opportunistic infections, neoplasms,
HIV INFECTION! Human Immunodeficiency Virus (HIV) Infects human cells and causes gradual loss of immune system function, and these immune alterations predispose to the opportunistic infections, neoplasms,
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES?
 WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
Objectives. HIV Treatment in Recently In 1996 the introduction of protease inhibitors decreasing the death rate of those infected by 50%.
 Objectives Identify modes HIV transmission and methods of prevention. HIV Treatment in 2010 Lisa D. Inge, Pharm.D., BCPS, AAHIVE Assistant Director, Jacksonville Campus Clinical Assistant Professor University
Objectives Identify modes HIV transmission and methods of prevention. HIV Treatment in 2010 Lisa D. Inge, Pharm.D., BCPS, AAHIVE Assistant Director, Jacksonville Campus Clinical Assistant Professor University