Pediatric TB Updates, Tools, and Adorable Faces
|
|
|
- Vernon Matthews
- 5 years ago
- Views:
Transcription



1 Pediatric TB Updates, Tools, and Adorable Faces Andrea T. Cruz, MD, MPH Baylor College of Medicine Santa Fe, New Mexico November 6, 2018
2 Disclosures I am on the data safety monitoring board for a trial of TB preventive therapy for children with multidrug resistant TB infection being conducted in South Africa. The photographs of my kids are presented with the permission of their families
3 Objectives Revisions in TB infection guidelines Tests of infection Treatment options Routes of administration of therapy Self administered Health department supported Source case investigations
4 Scenario #1 2yo previously healthy boy emigrating from Guatemala No known TB contacts, BCG status unknown, normal CXR Has no scar on deltoid 10 20% of BCG recipients do not have a scar TST: 10mm Caveat: the TST is always 10mm. What do you do? Does it change based on BCG status? On TST induration? On age? On other factors?

5 Testing for Infection
6 Comparison of TST & IGRAs Characteristic TST IGRA Antigens studied Many ESAT-6, CFP-10, (TB-7.7) Cross-reactivity with BCG Yes Unlikely Cross-reactivity with NTM Yes Less Likely Estimated sensitivity, TB in 75-90% 75-95% immunocompetent adults Estimated specificity, TB in 70-95% % immunocompetent adults Distinguish between TB infection No No and TB disease Boosting Yes No Patient visits required Two One
7 Newest Generation QuantiFERON Differences 3 rd generation 4 th generation Name QuantiFERON Gold QuantiFERON-Plus # of tubes 3 4 CD4 detection Yes: ESAT-6, CFP-10, TB 7.7 Yes: ESAT-6, CFP-10 CD8 detection No Yes: 6 MHC class I peptides Sensitivity 89-96% 91-96% Specificity 98-99% 98-99% Goal: improved sensitivity, especially in PLHIV or persons with recent infection; fewer indeterminate results (unclear if actually meets these goals)

8 What is a Positive TST? 5 mm 10 mm 15 mm HIV infected Contact to a TB case Child in whom you suspect TB disease Children < 4 years of age Children exposed to high risk adults Immigrants from highprevalence regions Children with diabetes or other immunocompromising conditions 2018 Red Book Anyone, even without risk factors
 and a tuberculin needle and syringe Don t need to draw blood You get an interpretable response No borderline or indeterminate results")
9 TST Advantages First used in 1907 We know a LOT about the dynamics and limitations Availability: Lab? What lab? Can be done whenever and wherever You need a kid (with an arm) and a tuberculin needle and syringe Don t need to draw blood You get an interpretable response No borderline or indeterminate results Cost: Tuberculin solution is cheap! Important for families and public health departments

10 TST Disadvantages: Interpretation Up to 20% of children don t return for TST interpretation But > 20% of parents are upset when a blood draw fails Sliding scale is confusing Red Book Table (3.82) is not There are issues with variation in TST induration measurement Come on how hard is it to measure a bump on an arm?



11 How hard can it be? We even skin test cows. So are we seriously saying that a toddler is more unruly than a 1,500 lb dairy cow? (Kids are not little adults; or really little bovines)
 eat soil But not my kids. Definitely not my kids.")
12 TST Disadvantages: False positives False positives BCG vaccine But vaccine used in those countries because they have a lot more TB, so threshold for treating kids from these countries is low CDC doesn t alter threshold for interpretation based on BCG status Nontuberculous species I know other people s children (and patients) eat soil But not my kids. Definitely not my kids. But kids do well with TB meds; it s ok to over treat some
13 TST: Cost Some argue that TST costs are > IGRA costs when include indirect costs of testing IGRA costs often reimbursed by insurance companies In TX, costs about $90/test for QuantiFERONs But. many of my kids and their families are uninsured So is the same cost model applicable for all families? WHO: IGRAs not recommended in low and middle income countries
14 Cost of QuantiFERON at commercial labs So, yes, the family has to return for testing, but even then it may still be cheaper for them test/infectious disease testing/tb blood test cost quest Very reputable website (not fake news)

15 LCA: method of differentiating between discordant results when there exists no reference standard Evaluated performance of TST, QFT, and TSPOT in US and foreign born HIV uninfected and infected children and adults Dichotomized ages as < 5 and 5 years of age Thorax 11/2018
16 Pediatrics

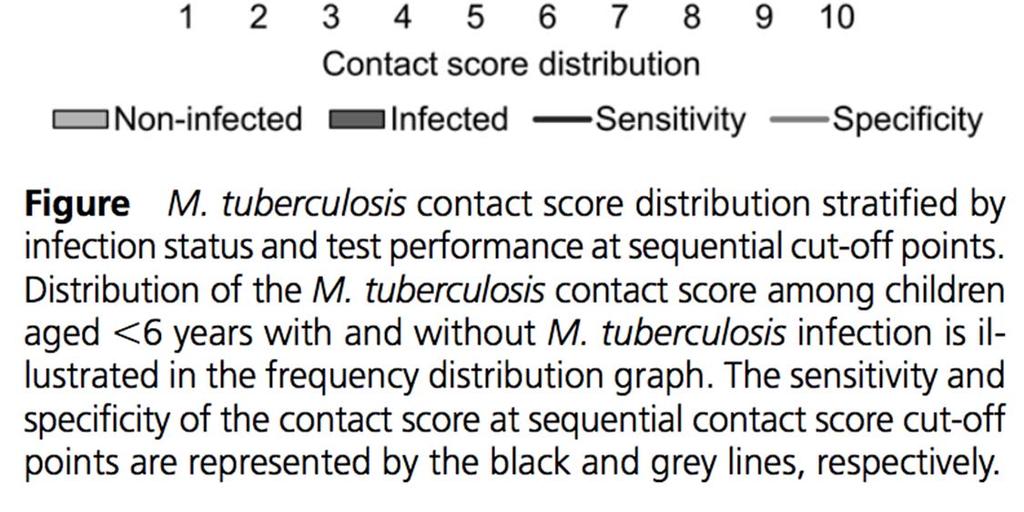
17 TST/IGRA Summary Data Foreign-born, 5 yrs TST had roughly same performance as coin flip for predicting LTBI Both QFT and TSPOT had high PPVs Foreign-born, < 5 yrs LTBI prevalence by LCA was 4% For TST 10mm as positive, PPV was 10% Almost all + TST results were false positives

18 2015 vs 2018 Red Book: IGRAs Recommendation Age* 5 years 2 years Preferred test for BCG recipients Yes Unchanged Use in immunocompromised children Cautiously Unchanged *States that some experts use down to 1 year of age
19 There continue to be roles for both tests IGRAs when TSTs: TSTs are ambiguously read (the ubiquitous non integer positive TST) You suspect TB disease and the TST is 0mm Immunocompromised kids Families need more convincing prior to treatment TSTs when IGRAs: IGRAs are borderline or indeterminate You suspect TB disease and the IGRA is negative or uninterpretable Immunocompromised kids

20 TB Infection Regimens
21 Infection Regimens We select regimens based on safety, tolerability, efficacy We know TB therapy is effective if taken as suggested However, completion rates abysmal with the traditionally-used 9 months of INH (9H): ~ 50% Completion inversely associated with duration of therapy Pediatric emphasis historically has been on 9H

22 905 children (2-17-yrs-old) from US, Canada, Brazil, China, Spain Pediatric cohort nested within PREVENT RCT Variable 3HP 9INH p= Progression to disease 0% 0.74% 0.11 Treatment completion 88.1% 80.9% Discontinuation due to AE 0.6% 0.2% 0.63 Drug related hepatotoxicity 0% 0% JAMA Pediatr 2015;169(3):247
 9H (given by families) 53% REF 9H (given by DOT) 89% 7.1 (3.5 14.")
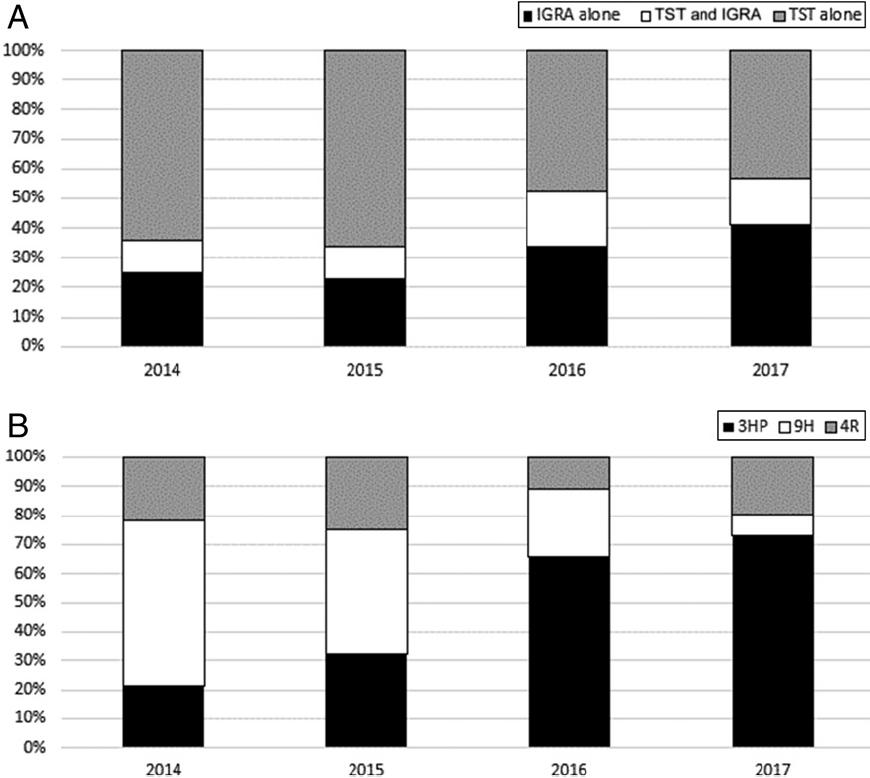
23 Pediatrics 2018;141(2):e HP vs 4RIF vs 9H, retrospective, non-randomized, Shift in study period in diagnosis, treatment: Diagnosed by TST alone: 65% 45% Treated with INH: 60% 8% Completion not associated with race/ethnicity or test of infection Completion frequencies: Regimen % completion OR (CI) 9H (given by families) 53% REF 9H (given by DOT) 89% 7.1 ( ) 4RIF (given by families) 84% 4.6 ( ) 4RIF (given by DOT) 97% 30.6 ( ) 3HP (given by DOT) 97% 27.4 ( )
 No known treatment failures Completion higher with RIF (84% vs 69%, p<0.")
24 4RIF vs 9H, nonrandomized, retrospective study Drug toxicity all dermatologic (1.5% in RIF, 0.7% in INH, non-signif) No known treatment failures Completion higher with RIF (84% vs 69%, p<0.0001) Completion rates higher when: IGRA used for diagnosis Children identified in contact tracing Shorter regimens used Pediatr Infect Dis J 2018;37(3):224
25 2015 vs 2018 Red Book: LTBI Regimens Recommendation Preferred regimen INH No specific preference (this is order in Red Book): 3HP* 4RIF 9H RIF role Limited: Expanded INH intolerance INH resistance in source case isolate 3HP Use in 12 years Use in 2 years *States that some experts think 3HP is the preferred regimen
26 Pediatrics
27 Rifampin Dosing Dosing initially used for RIF was in adults who weighed far less than TB patients do today Resulted in a 60-70% dose reduction Children metabolize many TB drugs faster than adults Need higher mg/kg dose to achieve target serum concentration (8 μg/ml) Recognition that there is substantial between-child variation in metabolism of certain TB drugs
 No")
28 2015 vs 2018 Red Book: RIF dosing (mg/kg/day) Recommendation Standard treatment TB meningitis Non meningitic TB, infants, toddlers Exceed adult maximum (600mg) No Yes
29 Routes of Administration


30 Scenario #2 8yo referred to see you for + IGRA performed after child did not complete 9 INH following a positive TST Pediatrician restarted INH You delve into barriers family faces: Cannot afford rifampin 9 months is a LONG time Family unclear on rationale for therapy What do you do now? Change regimen? Change way we give it?
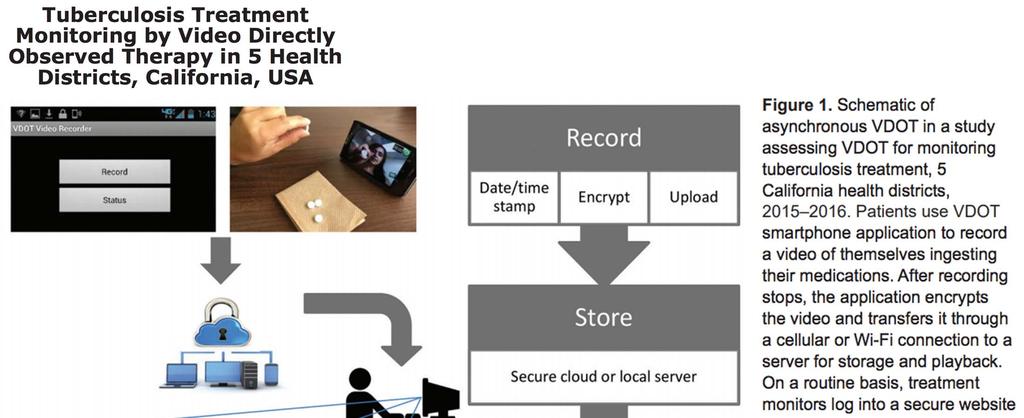
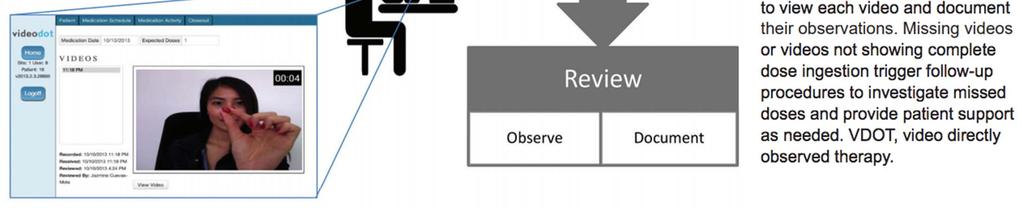
31 Routes of administration Self administered therapy (SAT) Family fills prescription, administers medication to child Enhanced SAT (ESAT) Health department drops off meds, family administers them Video directly observed therapy (vdot) Health department drops off meds periodically, family uses app to securely send video of child taking meds Traditional (in person) directly observed therapy (DOPT) Health department drops off meds, watches family administer them
32 Pros and cons of the options Route Pros Cons SAT Low cost (to system) High cost (to family) ~50% of children will complete therapy ESAT vdot DOPT Removes barrier of finding pharmacy, paying for prescription Intermediate in cost between SAT, DOT Convenience for families Lower cost than DOPT Allows for closest monitoring of highrisk children Does not address barrier of family giving the medication Assumes a degree of tech savviness Need IT infrastructure for secured data portal Acceptability to some families Cost
33 Monitoring while on therapy May have to see in clinic less frequently if on DOPT (or video DOPT) Few children need baseline or serial LFTs. Exceptions: Obesity Existing liver disease or comorbid medical conditions Receipt of other hepatically metabolized medications Low threshold for stopping meds and checking LFTs were the child to have any GI symptoms Importance of anticipatory guidance
34

35 Lean: promethazine + codeine + Sprite +/ Jolly Ranchers Pediatrics Dro: hydroponically grown marijuana
36 Teens, Substance Use & Abuse Drug Prevalence of use Ethanol 28 41% of high school seniors 6 million teens binge drink Marijuana 40% use, 23% used in last month Cocaine 6.8% Heroin 2.9% Inhalants 11.4% Methamphetamines 3.8% Prescription Stimulants 1.7 3% Prescription Sedatives % Prescription Opioids 4 12% J Adolesc Health 2012;51:6;; Can J Psychiatry 2012;57:745
37 My philosophy Our families face a lot of barriers to receiving care Financial Health literacy Transportation Linguistic Blaming families for not completing therapy is a cop out Instead, recognizing that there are things we as providers can do to make completion of therapy easier, we need to be asking how can we make things easier for our families
38 Source Case Investigations



39 How much contact is enough? A. Mother with cavitary disease, child sleeps in same bedroom B. Grandfather who visited once for Thanksgiving, holding his newborn granddaughter C. ICU nurse who cared for a premature baby while baby was intubated D. Respiratory therapist who helped transport a diabetic adolescent with cavitary disease during a 1 hour ambulance ride
40 The conundrum of the exposed young child Risk of progression from infection to disease is high Age at Primary Infection (year) No Disease (%) Pulmonary TB (%) CNS or Miliary Disease (%) < < 0.5 > < 0.5 We have mixed faith in the value of tests of infection for the youngest, most vulnerable children

41 Defining household contact This should not be a rigid definition Grandmother who cares for the child each day while parents are at work? Aunt who lives across the street and watches the baby frequently?
42 Establishing when contact was broken Try to triangulate information from index case and child s caregivers Err on the side of caution and assume a later date of breaking contact Explain potentially life threatening consequences of missed prevention opportunities Also explain to parents how well young children tolerate TB medications Try to link to other events: has your child been around X since Halloween?
43 Some of our Houston data Treated over 750 children for TB exposure, health departments Over 99% of families agreed to start therapy Over 99% of children who started window prophylaxis completed therapy Incredibly well tolerated Received treatment for weeks
44 Exposed children Approximately 5% of children with an initial 0mm TST converted TST conversion: Associated with a parent being the source case Not associated with smear status or being a household contact What does this mean? Proxies we often use for risk of being contagious are not great These factors donʼt help us risk stratify which young children would receive most benefit from window prophylaxis
45 Opportunities for improvement Better ways to assess exposure Historical variables Newer diagnostic modalities Optimizing window prophylaxis Expansion of video DOT
46

47 Cough aerosols are a better proxy of contact acquisition of infection than smear positivity Measure concentrations of viable bacteria in colony forming units (CFUs) Contacts of persons with high CFU cases had larger IGRA results than contacts of cases with lower CFUs IGRA conversion less associated with smear positivity in cases Suggests possibility of using cough generated aerosols to target preventive strategies PLoS One; e published ahead of print 10/29/18
48 Optimizing window prophylaxis Switch to rifampin? Keeping on INH, then changing to a shorter regimen only if the 2 nd TST is positive? Do we change plan based on how long we suspect a child will be on medication? Household contact vs not Persistently positive smear status in source case The youngest children
49 Pediatrics
50 Conclusions New recommendations exist for TB infection diagnosis and treatment Most non TB providers continue to rely upon the TST and 9 months of INH, despite acknowledged poor specificity and completion rates, respectively Likely reflects reduced awareness, not resistance to change Publication of new guidelines alone will not immediately change practice Feel comfortable nudging providers be an agent of change
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Jeffrey R. Starke, M.D. has the following disclosures to make:
 AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Disclosures. Current Issues and Controversies in Child and Adolescent Tuberculosis 02/24/2016. NSTC 2016 Annual Meeting
 Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
TB Intensive Tyler, Texas December 2-4, 2008
 TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
Tuberculosis Exposure, Infection, and Disease Among Children with Medical Comorbidities
 Tuberculosis Exposure, Infection, and Disease Among Children with Medical Comorbidities Andrea T. Cruz, MD, MPH, Omar Merchant, Affan Zafar, and Jeffrey R. Starke, MD Department of Pediatrics February
Tuberculosis Exposure, Infection, and Disease Among Children with Medical Comorbidities Andrea T. Cruz, MD, MPH, Omar Merchant, Affan Zafar, and Jeffrey R. Starke, MD Department of Pediatrics February
New Standards for an Old Disease:
 New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Interpretation of TST & IGRA results. Objectives
 Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Tuberculosis: Where Are We Now?
 Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination
 IUATLD North American Region Conference February 24, 2017 Vancouver, BC Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
IUATLD North American Region Conference February 24, 2017 Vancouver, BC Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
Sharing the Care: Working Together on LTBI Treatment and Management Webinar. September 24, Curry International Tuberculosis Center
 TB Infection Diagnostics and Treatment Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention 1 Curry International
TB Infection Diagnostics and Treatment Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention 1 Curry International
결핵노출접촉자감염관리 서울아산병원감염내과 김성한
 결핵노출접촉자감염관리 서울아산병원감염내과 김성한 TB incidence (2012) TB incidence South Korea 108 China 73 Taiwan 68 Portucal 26 Japan 19 Spain 14 US 3.6 * unit- per 100,000 population Adapted from WHO Adapted from WHO Emerg
결핵노출접촉자감염관리 서울아산병원감염내과 김성한 TB incidence (2012) TB incidence South Korea 108 China 73 Taiwan 68 Portucal 26 Japan 19 Spain 14 US 3.6 * unit- per 100,000 population Adapted from WHO Adapted from WHO Emerg
Latent TB Infection (LTBI) Strategies for Detection and Management
 Strategies for Detection and Management") Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Pediatric TB Basics and Evaluation and Management of Exposed Neonates
 Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
TB Nurse Case Management
 TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines
 Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination
 Four Corners TB and HIV Conference November 3, 2015 Durango, CO The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
Four Corners TB and HIV Conference November 3, 2015 Durango, CO The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION
 TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
Tuberculosis in Children and Adolescents 2017
 Tuberculosis in Children and Adolescents 2017 George D. McSherry, MD Division of Infectious Diseases Penn State Children s Hospital and Pediatric Section Northeastern Regional Training and Medical Consultation
Tuberculosis in Children and Adolescents 2017 George D. McSherry, MD Division of Infectious Diseases Penn State Children s Hospital and Pediatric Section Northeastern Regional Training and Medical Consultation
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Contact Investigation
 Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Isoniazid Preventive Therapy (IPT)
") Isoniazid Preventive Therapy (IPT) Josefina Cadorna-Carlos, M.D. Professor of Pediatrics U E R M M M C Objectives 1. Define IPT. 2. Discuss the indications for IPT. 3. Present RCT s for IPT (6H vs 9H).
Isoniazid Preventive Therapy (IPT) Josefina Cadorna-Carlos, M.D. Professor of Pediatrics U E R M M M C Objectives 1. Define IPT. 2. Discuss the indications for IPT. 3. Present RCT s for IPT (6H vs 9H).
Pediatric Tuberculosis
 Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Santa Clara County Tuberculosis Screening Requirement for School Entrance Effective June 1, 2014
 Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
The Origin of Swine Flu
 How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Using Interferon Gamma Release Assays for Diagnosis of TB Infection
 Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Michael J. Huey, MD. NYSCHA Annual Meeting WE-2, October 19, 2016
 Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
Conflict of Interest Disclosures:
 Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
The Most Widely Misunderstood Test of All
 The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
Thorax Online First, published on December 8, 2009 as /thx
 Thorax Online First, published on December 8, 2009 as 10.1136/thx.2009.119677 Title Page Cost effectiveness of the NICE guidelines for screening for latent tuberculosis infection: the Quantiferon-TB gold
Thorax Online First, published on December 8, 2009 as 10.1136/thx.2009.119677 Title Page Cost effectiveness of the NICE guidelines for screening for latent tuberculosis infection: the Quantiferon-TB gold
Childhood Tuberculosis Some Basic Issues. Jeffrey R. Starke, M.D. Baylor College of Medicine
 Childhood Tuberculosis Some Basic Issues Jeffrey R. Starke, M.D. Baylor College of Medicine TUBERCULOSIS IS A SOCIAL DISEASE WITH MEDICAL IMPLICATIONS THE GREAT PARADOX OF TUBERCULOSIS A CAUTIONARY TALE
Childhood Tuberculosis Some Basic Issues Jeffrey R. Starke, M.D. Baylor College of Medicine TUBERCULOSIS IS A SOCIAL DISEASE WITH MEDICAL IMPLICATIONS THE GREAT PARADOX OF TUBERCULOSIS A CAUTIONARY TALE
Ian Kitai TB Specialist. Division of Infectious Diseases Sickkids
 Ian Kitai TB Specialist Division of Infectious Diseases Sickkids Review Clinical presentation of TB disease childhood How to assess risk for TB infection How to assess risk for disease if infected TST
Ian Kitai TB Specialist Division of Infectious Diseases Sickkids Review Clinical presentation of TB disease childhood How to assess risk for TB infection How to assess risk for disease if infected TST
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Screening for Tuberculosis Infection. Harlingen, TX. Linda Dooley, MD has the following disclosures to make:
 TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
AT HIGH RISK OF PROGRESSING TO ACTIVE TB? Senior Lecturer and Consultant Physician University Hospitals of Leicester UK
 HOW WELL DO IGRAS PERFORM IN THE IDENTIFICATION OF PERSONS WHO ARE AT HIGH RISK OF PROGRESSING TO ACTIVE TB? Dr Pranab Haldar MD MRCP Senior Lecturer and Consultant Physician University Hospitals of Leicester
HOW WELL DO IGRAS PERFORM IN THE IDENTIFICATION OF PERSONS WHO ARE AT HIGH RISK OF PROGRESSING TO ACTIVE TB? Dr Pranab Haldar MD MRCP Senior Lecturer and Consultant Physician University Hospitals of Leicester
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Pediatric Tuberculosis: The Essentials October 8, 2014
 Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
Detecting latent tuberculosis using interferon gamma release assays (IGRA)
") Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
Revised Technical Instructions for Civil Surgeons. October 9, 2018
 Revised Technical Instructions for Civil Surgeons October 9, 2018 Speakers Joanna Regan Centers for Disease Control and Prevention Shereen Katrak California Department of Public Health Pennan Barry California
Revised Technical Instructions for Civil Surgeons October 9, 2018 Speakers Joanna Regan Centers for Disease Control and Prevention Shereen Katrak California Department of Public Health Pennan Barry California
Diagnosis of tuberculosis
 Diagnosis of tuberculosis Madhukar Pai, MD, PhD Assistant Professor, Epidemiology McGill University, Montreal, Canada madhukar.pai@mcgill.ca Global TB Case Detection A major concern 2.6 million new smear
Diagnosis of tuberculosis Madhukar Pai, MD, PhD Assistant Professor, Epidemiology McGill University, Montreal, Canada madhukar.pai@mcgill.ca Global TB Case Detection A major concern 2.6 million new smear
Advanced Concepts in Pediatric Tuberculosis
 Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges
 Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges David Karol, MD, MA Bureau of Prisons, FMC Butner Duke University Medical Center June 26, 2013 No Disclosures
Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges David Karol, MD, MA Bureau of Prisons, FMC Butner Duke University Medical Center June 26, 2013 No Disclosures
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Latent TB Infection (LTBI)
") Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without