Challenge in Lebanon as around the World
|
|
|
- Silas Morrison
- 5 years ago
- Views:
Transcription
1 OPL 22nd Pharmaceutical Congress 2014 Tuberculosis A Continuing i Public Health Challenge in Lebanon as around the World Myrna Germanos Haddad Hematology/Immunology Lab Hotel-Dieu de France Hospital Beirut
2 Tuberculosis Key facts in 2013 Second only to HIV/AIDS as the greatest killer worldwide 9 million people infected (1/3) 1.5 million died from the disease. > 95% of TB deaths in low and middle income countries children became ill with TB HIV negative e children died of TB. Globally in 2013, an estimated people developed multidrug resistant TB (MDR TB). The Millennium Development Goal : to reverse the spread of TB by Between 1990 and 2013,: 37 million lives were saved through TB diagnosis and treatment between 2000 and 2013 (45%)
3 Ministry of Labor August 2014
4
5 / Health 22 October 2014 Last updated at 15:17 GMT WHO revises global tuberculosis estimate up by 500,000 : in million people had developed TB around the world, up from 8.6 million in 2012, the WHO said About 1.5 million people died from TB, including 360,000 people p who were HIV positive TB kills 1.3m, second only to HIV.
6 History of TB (1) TB has affected humans for millennia May have evolved from Mycobacterium bovis acquired by humans from domesticated animals ~15,000 years ago Endemic in humans in villages ~ 10,000 years Epidemic in the cities Europe after 1600 (cities)
7 Egyptian mommies History of TB (2)
8 History of TB (3) BC Aristotle When one comes near consumptives one does contract their disease The reason is that the breath is bad and heavy In approaching the consumptive, one breathes this pernicious air. One takes the disease because in this air there is something disease producing. Described by Hippocrate
9 History of TB (4) Historically known by a variety of names, including: Consumption Wasting disease White plague TB was a death sentence for many Vintage image circa 1919 Image credit: National Library of Medicine
10
11 History of TB (5) Scientific Discoveries in 1800s Until mid 1800s, many believed TB was hereditary 1865 Jean Antoine Villemin proved TBwas contagious 1882 Robert Koch discovered M. tuberculosis, the bacterium that causes TB Mycobacterium tuberculosis Image credit: Janice Haney Carr





12 M tuberculosis as causative agent for tuberculosis Robert Koch
13 History of TB (6) 1882 Robert Koch one seventh of all human beings die of tuberculosis and if one considers only the productive middle age groups, tuberculosis carries away one third and often more of these
14 History of TB (7) Sanatoriums Before TB antibiotics, many patients were sent to sanatoriums Patients followed a regimen of bed rest, open air, and sunshine TB patients who could not afford sanatoriums often died at home Sanatorium patients resting outside 14
15
16 The Armenian Sanatorium (Azounieh)
17 The Armenian Sanatorium (Azounieh). Patients from Lebanon and surrounding countries, (Syria, (y Iraq, Palestine, Saudi Arabia, Kuwait, and Egypt) The Iraqi and Saudi Arabian Governments have maintained beds for their respective destitute patients. However, after the Lebanese Civil War this no longer takes place.
18 The Bhannes sanatorium 1910 ( Filles de la Charité)
19 Breakthrough in the Fight Against TB (1) Drugs that could kill TB bacteria were discovered Streptomycin (SM) discovered in 1943 ( S.A. WAKSMANN) Isoniazid (INH) and p aminosalicylic acid (PAS) discovered between 1943 and 1952 Pyrazinamide, ethambutol, rifampicine
20 Breakthrough in the Fight Against TB (2) After 50 years : 2013 Bedaquiline (Sirturo ) FDA approved Only availbale in the US
21 Breakthrough in the Fight Against TB (3) TB death rates began to drop dramatically Each year, fewer people got TB Most TB sanatoriums ( US and Europe) had closed by mid 1970s
22 Breakthrough in the Fight Against TB (4) TB rates decreased before TB drugs available Better nutrition, less crowded ddhousing Public health efforts Earlier diagnosis Limit transmission to close contacts TB sanatoria Surgery
23 Increase in TB in mid 1980s TB Resurgence Contributing factors: Inadequate funding for TB control programs TB HIV co infection epidemic Increased dimmigration i i from countries where TB is common (globalization allows TB to travel) Increase and spread of March Newsweek Magazine Cover multidrug resistant TB March 16, 1992 Newsweek Magazine Cover
24
25 TB History Timeline 1993: TB cases decline due to increased funding and enhanced dtb control efforts 1865: Jean Antoine 1943: Streptomycin Villemin (SM) a drug used to proved TB is treat TB is contagious discovered Mid 1970s: Most TB sanatoriums closed : : Mid 1980s: Robert Koch discovers Two more drugs are Unexpected rise in TB M. tuberculosis discovered to treat TB: cases INH and PAS
26 TB Transmission (1) Transmission is defined as the spread of an organism, such as M. tuberculosis, fromone one person to another.
27 M. tuberculosis causes most TB Mycobacteria that cause TB: M. tuberculosis M. bovis M. africanum M. microti M. canetti TB Transmission (2) Types of Mycobacteria Mycobacteria that do not cause TB e.g., M. avium complex M. tuberculosis

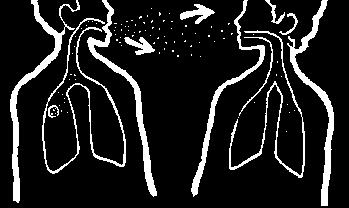
28 TB Transmission (3) TB is spread person to person through the airvia droplet nuclei M. tuberculosis may be expelled when an infectious person: Coughs Sneezes Speaks Sings Transmission occurs when another person inhales droplet nuclei
29 TB Transmission (4) Dots in air represent droplet nuclei containing M. tuberculosis
30 TB Transmission (5) Probability that TB will be transmitted depends on: Infectiousness of person with TB disease Environment in which exposure occurred Length of exposure Virulence (strength) th) of the tubercle bacilli The best way to stop transmission is to: Isolate infectious persons Provide effective treatment to infectious persons as soon as possible
31 TB Pathogenesis
32 TB Pathogenesis (1) How an infection or disease develops in the body.
33 TB Pathogenesis (2) Latent TB Infection (LTBI) Occurs when tubercle bacilli arein the body, but the immune system is keeping them under control Dt Detected tdby the Mantoux tuberculin skin test t(tst) or by blood tests such as interferon gamma release assays (IGRAs) which include: QuantiFERON TB Gold test (QFT G) QuantiFERON TB Gold In Tube (QFT GIT) T Spot.TB test (T SPOT) People with LTBI are NOT infectious
34 TB Pathogenesis (3) TB Disease Develops when immune system cannot keep tubercle bacilli under control May develop very soon after infection or many years after infection About 10% of all people with normal immune systems who have LTBI will develop TB disease at some point in their lives People with TB disease are often infectious
35 TB Pathogenesis (4) Droplet nuclei containing tubercle bacilli areinhaled, Droplet nuclei containing tubercle bacilli are inhaled, enter the lungs, and travel to small air sacs (alveoli)
36 TB Pathogenesis (5) 2 bronchiole blood vessel tubercle bacilli alveoli li Tubercle bacilli multiply in alveoli, where infection begins
37 TB Pathogenesis (6) 3 bone brain lung kidney A small number of tubercle bacilli enter bloodstream and spread throughout body
38 TB Pathogenesis (7) LTBI 4 special immune cells form a barrier shell (in this example, bacilli are in the lungs) Within 2 to 8 weeks the immune system produces special immune cells called macrophages that surround the tubercle bacilli These cells form a barrier shell that keeps the bacilli contained and under control (LTBI) 38
39 TB Pathogenesis (8) TB Disease 5 shell breaks down and tubercle bacilli escape and multiply (in this example, TB disease develops in the lungs) If the immune system CANNOT keep tubercle bacilli under control, bacillibeginbegin to multiplyrapidly and cause TB disease This process can occur in different places in the body
40 TB Invades/Infects the Lung Effective immune response Infection limited it to small area of lung Immune response insufficient i
 (10-30%) Latent TB")
 Treated Die within 2 years Survive")
41 Natural History of TB Infection Exposure to TB No infection Infection (70-90%) (10-30%) Latent TB (90%) Never develop Active disease Untreated Active TB (10%) Treated Die within 2 years Survive Die Cured
42 LTBI vs. TB Disease Latent t TB Infection (LTBI) TB Disease (in the lungs) Inactive, contained tubercle bacilli in the body TST or blood test results usually positive Chest x-ray usually normal Active, multiplying tubercle bacilli in the body TST or blood test results usually positive Chest x-ray usually abnormal Sputum smears and cultures negative No symptoms Not infectious Not a case of TB Sputum smears and cultures may be positive Symptoms such as cough, fever, weight loss Often infectious before treatment A case of TB
 (Goal = prevent")

 = TB Infection which hhas")
 = NOT")
43 Latent TB vs. Active TB Latent TB (LTBI) (Goal = prevent future active disease) = TB Infection = No Disease = NOT SICK = NOT INFECTIOUS Active TB (Goal = treat to cure, prevent transmission) = TB Infection which hhas progressed to TB Disease = SICK (usually) = INFECTIOUS if PULMONARY (usually) = NOT INFECTIOUS if not PULMONARY (usually)
44 TB Pathogenesis Progression from LTBI to TB Disease
45 Progression to TB Disease (1) Risk of developing TB diseaseis highest the first2 years after infection People with LTBI can be given treatment to prevent them from developing TB disease Detecting TB infection early and providing treatment helps prevent new cases of TB disease 45
46 Progression to TB Disease (2) Some conditions increase probability of LTBI progressing to TB disease Infection with HIV Organ transplant Chest x ray findings suggestive of previous TB Substance abuse Recent TB infection Prolonged therapy with corticosteroids and other immunosuppressive therapy, such as prednisone and tumor necrosis factor alpha [TNF α] antagonists Silicosis Diabetes mellitus Severe kidney disease Certain types of cancer Certain intestinal conditions Low body weight
47 Progression to TB Disease (3) People Exposed to TB Not TB Infected Latent TB Infection (LTBI) Not Infectious Not Infectious Negative TST or QFT-G test result No TB Infection Positive TST or QFT G test result Latent TB Infection May go on to develop TB disease



48 Progression to TB Disease (4) Inan HIV infected person, TB can develop in one of two ways: Person with LTBI becomes infected with HIV and then develops TB disease as the immune system is weakened TB and HIV Person with HIV infection becomes infected with M. tuberculosis and then rapidly develops TB disease Image credit: Mississippi State Department of Health
49 Progression to TB Disease (5) TB and HIV People who are infected with both M. tuberculosis and HIV are much more lk likely l to develop TB disease TB infection and NO risk factors TB infection and dhivi infection (pre-highly Active Antiretroviral Treatment [HAART]) Risk is about 5% in the Risk is about 7% to 10% first 2 years after PER YEAR, a very high infection and about 10% risk over a lifetime over a lifetime
50 TB Pathogenesis Sites of TB Disease 50
51 Sites of TB Disease (1) Bacilli may reach any part of the body, but common sites include: Brain Larynx Bone Kidney Lymph node Pleura Lung Spine
52 Sites of TB Disease (2) Location Frequency Pulmonary TB Lungs Most TB cases are pulmonary Extrapulmonary TB Places other than lungs such as: Larynx Lymph nodes Pleura Brain Kidneys Bones and joints Found more often in: HIV-infected or other immunosuppressed persons Young children Miliary TB Carried to all parts of body, through bloodstream Rare

")

53 Sites of TB Disease (2)
54 Diagnosis of LTBI Available testing methods for M. tuberculosis infection: Mantoux tuberculin skin test (TST) Blood tests known as interferon gamma release assays (IGRAs): QuantiFERON TB Gold test (QFT G) QuantiFERON TB Gold In Tube (QFT GIT) T SPOT TB 54
55 Mantoux Tuberculin Skin Test (1) TST is administered by injection Tuberculin is made from proteins derived from inactive tubercle bacilli Most people p who have TB infection will have a reaction at injection site Syringe being filled with 0.1 ml of liquid tuberculin 55
56 Mantoux Tuberculin Skin Test (2) 0.1 ml of 5 tuberculin units of liquid tuberculin are injected between the layers of skin on forearm HCW administering i i Mantoux TST 56
57 Mantoux Tuberculin Skin Test (3) Forearm should be examined within hours by HCW Reaction is an area of induration (swelling) around injection site Induration is measured in millimeters Erythema (redness) )is not measured Only the induration is measured
58 Mantoux Tuberculin Skin Test (5) Interpreting the Reaction Induration of > 5 mm is considered positive for: People living with HIV Recent close contacts of people with infectious TB People with chest x ray findings suggestive of previous TB disease People with organ transplants Other immunosuppressed patients 58
59 Mantoux Tuberculin Skin Test (6) Interpreting the Reaction Induration of > 10 mm is considered a positive reaction for: People who have recently come from areas where TB is common People who inject drugs People who live or work in high risk congregate settings Mycobacteriology lb laboratory workers
60 Mantoux Tuberculin Skin Test (7) Interpreting the Reaction Induration of > 10 mm is considered d a positive reaction for: People with certain medical conditions that increase risk for TB Children younger than 4 years old Infants, children, or adolescents exposed to adults in high risk categories
61 Mantoux Tuberculin Skin Test (8) Interpreting the Reaction Induration of > 15 mm is considered a positive reaction for people who have no known risk factors for TB 61
62 IGRA guidelines consensus Guidelines on IGRAs are now published across much of Europe The newest are the UK NICE guidelines issued 23 rd March 2011, which reflect the most up todate data on IGRAs General consensus on features of IGRA vs TST IGRAs are more specific than the TST Hence preferred in BCG vaccinated persons and all positive TSTs should be confirmed with an IGRA IGRAs detect infected persons that the TST does not Hence IGRAs should be used instead of, or in addition to, the TST in immunosuppressed persons IGRAs bring bi logistical i ladvantages of only one patient visit ii Hence IGRA use is recommended in hard to reach populations Using IGRAs is more cost effective than not using them Using only the TST is the most expensive strategy IGRA use in children is still an area under debate National Institute for Health and Clinical Excellence (NICE) Tuberculosis. NICE Clinical Guideline 117. March 2011
63 / Health In the last few years a new DNA detection technique called GeneXpert has been endorsed by the WHO From a sample of sputum it can detect whether a sample contains TB and whether it is resistant to rifampicin in about three hours But for full drug resistance information the patient has to wait longer.
64 / Health 24 September 2014 Last updated at 09:37 GMT Breath test for TB developed By Michael Eyre Science reporter
65 /Health: Breath test for TB developed d It provides rapid information on drug resistance that takes up to six weeks using standard methods, US scientists report in the journal, Nature Communications. The bacteria emit nitrogen gas signature within 10 minutes of exposure to isoniazid in rabbits. Gas detected by a mass spectrometer
66 Rapid tuberculosis tests Blood Non accurate Non FDA approved False negative results
67 Diagnosis of TB Disease 1. Medical history 2. Physical examination 3. Test for TB infection 4. Chest x ray 5. Bacteriologic examinations : Acid fast bacilli (AFB), Nucleic Acid Amplification Tests (NAA) Culturing and Identifying Specimen Drug Susceptibility Testing
68 Patients who have any tubercle bacilli seen in their sputum have a positive smear. Patients who have positive smears areconsidered infectious because they can cough tubercle bacilli into the air.
69 Treatment of TB disease Most TB is curable, but Four or more drugs required for the simplest regimen 6 9 or more months of treatment required Person must be isolated until non infectious Directly observed therapy to assure adherence/completion is recommended Side effects and toxicity of drugs common May prolong treatment t t May prolong infectiousness Other medical and psychosocial py conditions complicate therapy TB may be more severe Drug drug interactions common
70 Treatment of LTBI (1) LTBI is treated to prevent the development of TB disease 70
71 High Priority for LTBI Treatment (2) High priority groups for LTBI treatment if positive IGRA or TST result of >10 mm: People who have come within last 5 years from countries where TB is common People who inject drugs People who live or work in high risk facilities People who work in mycobacteriology laboratories
72 High Priority for LTBI Treatment (3) High priority groups for LTBI treatment if positive IGRA or TST result of > 10 mm: (cont.): People with medical conditions that increase risk of TB disease Children younger than 4 years old Infants, children, and adolescents exposed to adults in high risk groups 72
73 Low Priority for LTBI Treatment Individuals without any risk factors generally should not be tested for TB infection However, individuals with no risk factors who are tested and have a positive IGRA or TST result of >15 mm should be evaluated for LTBI treatment
74 Treatment tof LTB What is the preferred LTBI treatment regimen? INH given daily for 9 months. 74
75 Treatment of TB Disease Initial regimen should contain the following four drugs: Isoniazid (INH) Rifampin (RIF) Pyrazinamide (PZA) INH RIF Ethambutol (EMB) PZA EMB 75
76 Treatment of TB Disease Treatment must contain multiple drugs to which organisms are susceptible Treatment with a single drug can lead to the development of drug resistant resistant TB 76
77 Special Considerations for LTBI (1) Directly Observed Therapy (DOT) DOT is when a health care worker (HCW) or another designated person watches a patient swallow each dose of medication Used to hl help patients adhere to treatment Should be considered for people who are at high risk for TB or suspected to be non adherent 77
78 Drug Resistant TB 78
79 Drug Resistant TB (1) To at least one TB treatment drug Isoniazid (INH) Rifampin (RIF) Pyrazinamide (PZA) Ethambutol (EMB) d Resistant means drugs can no longer kill the bacteria
80 Primary Resistance Drug Resistant TB (2) Caused by person-to-person transmission i of drug-resistant t organisms Secondary Develops during TB treatment: t t Resistance Patient was not given appropriate treatment regimen OR Patient did not follow treatment regimen as prescribed
81 Drug Resistant TB (3) Mono-resistant Poly-resistant Multidrug resistant (MDR TB) Extensively drug resistant (XDR TB) Resistant to any one TB treatment drug Resistant to at least any 2 TB drugs (but not both isoniazid and rifampin) Resistant to at least isoniazid and rifampin, the 2 best first-line TB treatment drugs Resistant to isoniazid and rifampin, PLUS resistant to any fluoroquinolone AND at least 1 of the 3 injectable second-line drugs (e.g., amikacin, kanamycin, or capreomycin)




82 BCG No longer in use in many countries except in exposed children
83 Epidemiology
84 TB: the disease in Lebanon cases Smear positive: 251 cases (39.7%) Smear negative: 131 cases (20.8%) Extra pulmonary: 250 cases (39.5%) MDR TB : 7 cases TB HIV: 3 cases Children: 45 cases (7%)
85 Incidence in the origin countries of non national patients living in Lebanon Incidence in: Lebanon: 15/ Syria: 19/ Sri Lanka: 66/ Sudan: 117/ Bengladesh: 225/ Ethiopia: 258/ Philippines : 270/100 00
86 Trend of Tuberculosis incidence in Lebanon Had been declining till the year In 2012, the National TB Programme (NTP) observed that 48% of all notified cases were among non Lebanese. The 27% increase in TB incidence in 2012 is attributed to Syrian refugees population
87 Trend of TB cases notification in national and non national population by years.
88 Before the Syrian crisis, in 2011, the estimated prevalence of TB : in Syria was 23 per 100,000 population in Lebanon Lb 19 per 100, population
89 NTP indicates that currently over half of the people referred to the programme for investigations and treatment are non Lebanese nationals. As of August 2013, according to the NTP, 100 Syrian refugees have been diagnosed with TB in Lebanon, including three cases of multi drug resistant (MDR) TB.
90 There has been Syrian and Lebanese returnees TB patients who were forced to interrupt their treatment because of the worsening security situation inside Syria. This interrupted TB treatment can lead to weaker identification of TB in the communities, low cure rate and potentially increase in multidrug resistant (MDR) TB, which is difficult and expensive to treat
91 The National Tuberculosis Programme (NTP) in Lebanon follows (Directly Observed Treatment Strategy), High treatment success rate of 87% among Lebanese nationals.
92 The NTP in Lebanon has eight TB control centers across the country.
93 WHO Lebanon is ensuring the provision of anti TB medication for 200 Syrian refugees/year in addition to the 600 Lebanese cases. TB as an airborne disease spreads especially in congested and unhygienic i living i conditions, i such as the ones many Syrian refugees in Lebanon as well as returning Lb Lebanese families from Syriaare exposed to. One important issue in TB control is the provision of TB services in remote areas and among mobile populations. p Weakened or disrupted services for these communities can complicate diagnosis and treatment potentially can complicate diagnosis and treatment, potentially leading to an increase in MDR TB.
94 LTBI: To treat or not to treat? 3 to home workers tested for TST Very High rate of positive cases for TST Prophylactic treatment of LTBI not supported by WHO Heavy financial burden Prophylaxic treatment failed to lower the % of TBI in african fi countries ti LTBI treatment advised only in chidren
95 LTBI: To treat or not to treat? TBI : the disease has a huge cost on the Lebanese government (sana, drugs ) LTBI :decision for prophylactic treatment depends on the decision of the Minister of PH Under study by a committee
96 TB: What are the Challenges Guidelines, Laws andregulations Guidelines treatment, contact investigation, prevention data driven/expert opinion Laws case reporting, isolation of infectious individuals id Laws/regulations travel restrictions, entry into the country International travel regulations WHO
97 TB : Prevention and Control latiiti Activities Identification and treatment of TB cases Identification, evaluation and treatment of high risk close contacts of cases Surveillance/case reporting TB laboratory services Targeted testing and LTBI treatment for high risk populations Training/continuing i i i education for health h care providers Program evaluation
98 TB continues as a public health issue many problems to face: Old public health concepts (isolation of infectious individuals, closely monitored treatment, recognition and preventive treatment for infected contacts) are still critical, but will not eradicate TB Care providers not familiar with signs/symptoms of TB Diagnosis i delayed dl d Inappropriate treatment Drug resistance due to improper use of drugs Must address both nationals and newcomer populations Older, remote exposure Incarcerated, homeless, history of drug, alcohol use Newcomers from high TB prevalence areas
99 Challenges to Public Health System Public health workers must: Educate Identify support services (food, housing) Treat TB in geriatric populations Treat TB in children Deal with alcohol, drug abusing, incarcerated patients Manage TB in patients with underlying medical conditions Provide culturally appropriate care for non Lebanese /nonliterate populations Treat TB cases with drug resistant TB
100 Tuberculosis Key facts in 2013 Second only to HIV/AIDS as the greatest killer worldwide 9 million people infected (1/3) 1.5 million died from the disease. > 95% of TB deaths in low and middle income countries children became ill with TB HIV negative e children died of TB. Globally in 2013, an estimated people developed multidrug resistant TB (MDR TB). The Millennium Development Goal : to reverse the spread of TB by Between 1990 and 2013,: 37 million lives were saved through TB diagnosis and treatment between 2000 and 2013 (45%)
101
102
103 World TB Day, 24 March 2014 To raise awareness about the burden of (TB) prevention and control efforts worldwide. Of the 9 million people a year who get sick ikwith ihtb, 3 million of them are "missed" by health systems. World TB Day provides the opportunity to call for further action to reach the 3 million.
104
105 The Stop TB Strategy WHO has developed da new six point Stop TB Strategy its goal: to dramatically reduce the global burden of tuberculosis by 2015 To ensure all TB patients benefit from universal access to high quality diagnosis and patient centered treatment. The development of new and effective tools to prevent, detect and treat TB. The engagement of all care providers
106 The Stop TB Strategy The Global Drug Facility GDF (created 2001) : TB treatments & diagnostics to population p in need. In 2014 > 24 million treatment courses to 133 countries Provides technical assistance and innovative tools to countries, and supports key projects like TB REACH, Expand TB,TBExpert in thediagnostic field.
107
108 A new vaccine development of shorter, simpler treatment regimens faster more accurate diagnostic tools(genexpert device) reduce the cost of innovative technologies and accelerate their adoption. Research
109 Theguardian.com, Monday 23 june 2014 «Genetictest for TB could dramatically improve diagnosis in children» Reports an article il published in the «NEJM» Identifies specific gene sequences that appear more frequently in TB infection I th f di i f i f t d Improve the accuracy of diagnosisof infected children in developing countries more difficult to diagnose thanadults
110 TB? STILL MILESTONES TO GO
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Primer on Tuberculosis (TB) in the United States
 in the United States") Primer on Tuberculosis (TB) in the United States The purpose of this primer is to provide instructors who have no prior background in TB research or clinical care with basic knowledge that they may find
Primer on Tuberculosis (TB) in the United States The purpose of this primer is to provide instructors who have no prior background in TB research or clinical care with basic knowledge that they may find
Tuberculosis 6/7/2018. Objectives. What is Tuberculosis?
 Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014
 TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
Tuberculosis What you need to know. James Zoretic M.D., M.P.H. Regions 2 and 3 Director
 Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Why need to havetb Clearance. To Control and Prevent Tuberculosis
 Why need to havetb Clearance To Control and Prevent Tuberculosis How to ID Tuberculosis There are two kinds of tests that are used to determine if a person has been infected with TB bacteria: the tuberculin
Why need to havetb Clearance To Control and Prevent Tuberculosis How to ID Tuberculosis There are two kinds of tests that are used to determine if a person has been infected with TB bacteria: the tuberculin
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
Running head: TUBERCULOSIS 1
 Running head: TUBERCULOSIS 1 Tuberculosis Erin Burdi Ferris State University TUBERCULOSIS 2 Abstract Tuberculosis is one of the world s oldest infectious diseases. It is a disease that continues to affect
Running head: TUBERCULOSIS 1 Tuberculosis Erin Burdi Ferris State University TUBERCULOSIS 2 Abstract Tuberculosis is one of the world s oldest infectious diseases. It is a disease that continues to affect
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
TUBERCULOSIS TODAY WORLD-WIDE, UNITED STATES, TEXAS J O R D A N C O U L S O N, R. N. S N S C O O R D I N A T O R, P H E P / H S R 1
 TUBERCULOSIS TODAY WORLD-WIDE, UNITED STATES, TEXAS J O R D A N C O U L S O N, R. N. S N S C O O R D I N A T O R, P H E P / H S R 1 WHAT IS TB? TB is a disease caused by a bacterium called Mycobacterium
TUBERCULOSIS TODAY WORLD-WIDE, UNITED STATES, TEXAS J O R D A N C O U L S O N, R. N. S N S C O O R D I N A T O R, P H E P / H S R 1 WHAT IS TB? TB is a disease caused by a bacterium called Mycobacterium
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Learning Objectives: Case 1 11/12/2015. Tuberculosis: Focus on Transmission and Pathogenesis. TB: Some Important Terms
 A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
What is tuberculosis? What causes tuberculosis?
 What is tuberculosis? What causes tuberculosis? Last updated: Thursday 4 September 2014 Tuberculosis Infectious Diseases / Bacteria / Viruses Respiratory / Asthma Some may see Tuberculosis as a historical
What is tuberculosis? What causes tuberculosis? Last updated: Thursday 4 September 2014 Tuberculosis Infectious Diseases / Bacteria / Viruses Respiratory / Asthma Some may see Tuberculosis as a historical
TB IN EMERGENCIES. Disease Control in Humanitarian Emergencies (DCE)
") TB IN EMERGENCIES Department of Epidemic and Pandemic Alert and Response (EPR) Health Security and Environment Cluster (HSE) (Acknowledgements WHO Stop TB Programme WHO/STB) 1 Why TB? >33% of the global
TB IN EMERGENCIES Department of Epidemic and Pandemic Alert and Response (EPR) Health Security and Environment Cluster (HSE) (Acknowledgements WHO Stop TB Programme WHO/STB) 1 Why TB? >33% of the global
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Tuberculosis. Impact of TB. Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH)
") Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Tuberculosis. New TB diagnostics. New drugs.new vaccines. Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012
 Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
What Drug Treatment Centers Can do to Prevent Tuberculosis
 What Drug Treatment Centers Can do to Prevent Tuberculosis Tuberculosis (TB) is alive and well Learn what you can do to prevent TB among your clients and protect yourself! Transmission TB is spread through
What Drug Treatment Centers Can do to Prevent Tuberculosis Tuberculosis (TB) is alive and well Learn what you can do to prevent TB among your clients and protect yourself! Transmission TB is spread through
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Descriptive Epidemiology Project: Tuberculosis in the. United States. MPH 510: Applied Epidemiology. Summer A 2014
 Descriptive Epidemiology Project: Tuberculosis in the United States MPH 510: Applied Epidemiology Summer A 2014 June 1, 2014 1 The white plague affected thousands upon thousands of people in the 18 th
Descriptive Epidemiology Project: Tuberculosis in the United States MPH 510: Applied Epidemiology Summer A 2014 June 1, 2014 1 The white plague affected thousands upon thousands of people in the 18 th
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Frances Morgan, PhD October 21, Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS
 The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
All you need to know about Tuberculosis
 All you need to know about Tuberculosis What is tuberculosis? Tuberculosis is an infectious disease that usually affects the lungs. Doctors make a distinction between two kinds of tuberculosis infection:
All you need to know about Tuberculosis What is tuberculosis? Tuberculosis is an infectious disease that usually affects the lungs. Doctors make a distinction between two kinds of tuberculosis infection:
2016 Annual Tuberculosis Report For Fresno County
 206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
Questions and Answers Press conference - Press Centre Room 3 Wednesday 16 August 2006, 14.00hrs
 Questions and Answers Press conference - Press Centre Room 3 Wednesday 16 August 2006, 14.00hrs What causes TB? TB is caused by the bacterium Mycobacterium tuberculosis. Although it can cause disease in
Questions and Answers Press conference - Press Centre Room 3 Wednesday 16 August 2006, 14.00hrs What causes TB? TB is caused by the bacterium Mycobacterium tuberculosis. Although it can cause disease in
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
TB 2015 burden, challenges, response. Dr Mario RAVIGLIONE Director
 TB 2015 burden, challenges, response Dr Mario RAVIGLIONE Director Addis Ababa, Ethiopia 11-13 November 2015 Overview TB basics TB burden & challenges Response: End TB Strategy DAY 1 What is TB? Definition
TB 2015 burden, challenges, response Dr Mario RAVIGLIONE Director Addis Ababa, Ethiopia 11-13 November 2015 Overview TB basics TB burden & challenges Response: End TB Strategy DAY 1 What is TB? Definition
4/25/2012. The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB
 Sindy M. Paul, MD, MPH, FACPM May 1, 2012 The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB morbidity, including resistance Identifying people
Sindy M. Paul, MD, MPH, FACPM May 1, 2012 The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB morbidity, including resistance Identifying people
Chapter 7 Tuberculosis (TB)
") Chapter 7 Tuberculosis (TB) TB infection vs. TB disease Information about TB TB skin testing Active TB disease TB risk factors Role of Peel Public Health in TB prevention and control Environmental and
Chapter 7 Tuberculosis (TB) TB infection vs. TB disease Information about TB TB skin testing Active TB disease TB risk factors Role of Peel Public Health in TB prevention and control Environmental and
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
What Is TB? 388 How TB Is Spread 388 How to Know if a Person Has TB 389 How to Treat TB 389 Resistance to TB medicines 390
 386 Chapter 25 In this chapter: What Is TB? 388 How TB Is Spread 388 How to Know if a Person Has TB 389 How to Treat TB 389 Resistance to TB medicines 390 Preventing TB 391 Working for Change 391 387 (TB)
386 Chapter 25 In this chapter: What Is TB? 388 How TB Is Spread 388 How to Know if a Person Has TB 389 How to Treat TB 389 Resistance to TB medicines 390 Preventing TB 391 Working for Change 391 387 (TB)
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Symptoms Latent TB Active TB
 1 Tuberculosis Tuberculosis (TB) is a disease that can spread through the air. It is caused by a bacterium called Mycobacterium tuberculosis. It usually affect the lungs. However, it can also affect other
1 Tuberculosis Tuberculosis (TB) is a disease that can spread through the air. It is caused by a bacterium called Mycobacterium tuberculosis. It usually affect the lungs. However, it can also affect other
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
TB Transmission, Pathogenesis & Infection Control
 TB Transmission, Pathogenesis & Infection Control Bradley Allen, MD, PhD, FACP, FIDSA. 2014 MFMER slide-1 Disclosures Medical Consultant, TB Control Program Indiana State Department of Health Past clinical
TB Transmission, Pathogenesis & Infection Control Bradley Allen, MD, PhD, FACP, FIDSA. 2014 MFMER slide-1 Disclosures Medical Consultant, TB Control Program Indiana State Department of Health Past clinical
New Standards for an Old Disease:
 New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
Tuberculosis & Refugees in Philadelphia
 Tuberculosis & Refugees in Philadelphia Philadelphia TB Control Program Daniel P. Dohony, MPH Philadelphia TB Control Program Health Information Portal Website: hip.phila.gov Contains Information On» Disease
Tuberculosis & Refugees in Philadelphia Philadelphia TB Control Program Daniel P. Dohony, MPH Philadelphia TB Control Program Health Information Portal Website: hip.phila.gov Contains Information On» Disease
Mycobacterium tuberculosis. Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology
 Dr.Baha, AL-Amiedi Ph. D.Microbiology") Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
Contact Investigation
 Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis. WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED
 Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
CDC IMMIGRATION REQUIREMENTS:
 CDC IMMIGRATION REQUIREMENTS: Technical Instructions for Tuberculosis Screening and Treatment Using Cultures and Directly Observed Therapy October 1, 2009 Table of Contents Preface...i Tuberculosis Screening...1
CDC IMMIGRATION REQUIREMENTS: Technical Instructions for Tuberculosis Screening and Treatment Using Cultures and Directly Observed Therapy October 1, 2009 Table of Contents Preface...i Tuberculosis Screening...1
Questions and Answers About
 Questions and Answers About TB 2005 DEPARTMENT OF HEALTH AND HUMAN SERVICES TB Elimination Questions and Answers About TB 2005 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention
Questions and Answers About TB 2005 DEPARTMENT OF HEALTH AND HUMAN SERVICES TB Elimination Questions and Answers About TB 2005 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Proposed Regs.pdf
 Kansas Wesleyan University TB testing Policy In Compliance with Kansas Statue KSA 2009 Supp. 65-129, all Kansas Wesleyan University students who have traveled, resided in for more than three months, or
Kansas Wesleyan University TB testing Policy In Compliance with Kansas Statue KSA 2009 Supp. 65-129, all Kansas Wesleyan University students who have traveled, resided in for more than three months, or
TB and Respiratory Protection
 Slide 1 TB and Respiratory Protection Tuberculosis (TB) is a disease present throughout the United States. Lehigh Valley Health Network is concerned about your health and needs your help to prevent the
Slide 1 TB and Respiratory Protection Tuberculosis (TB) is a disease present throughout the United States. Lehigh Valley Health Network is concerned about your health and needs your help to prevent the
TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks
 1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On
1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On
MULTIDRUG- RESISTANT TUBERCULOSIS. Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic
 MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
The Air We Share: Principles and Practices of TB Infection Control
 The Air We Share: Principles and Practices of TB Infection Control Session Four of a Four-Part Webinar Series Presented in Partnership with the BC Lung Association January 10, 2014 Facilitators: Nash Dhalla,
The Air We Share: Principles and Practices of TB Infection Control Session Four of a Four-Part Webinar Series Presented in Partnership with the BC Lung Association January 10, 2014 Facilitators: Nash Dhalla,
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE MAY 8-11, 2018 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. List
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE MAY 8-11, 2018 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. List
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TUBERCULOSIS CONTACT INVESTIGATION
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Nguyen Van Hung (NTP, Viet Nam)
") Technical Consultation Meeting on the Programmatic Management of Latent Tuberculosis Infection 31 August-1 September 2017, Seoul, Republic Korea Adopting new LTBI diagnostics at country level: perspective
Technical Consultation Meeting on the Programmatic Management of Latent Tuberculosis Infection 31 August-1 September 2017, Seoul, Republic Korea Adopting new LTBI diagnostics at country level: perspective
MODULE SIX. Global TB Institutions and Policy Framework. Treatment Action Group TB/HIV Advocacy Toolkit
 MODULE SIX Global TB Institutions and Policy Framework Treatment Action Group TB/HIV Advocacy Toolkit 1 Topics to be Covered Global TB policy and coordinating structures The Stop TB Strategy TB/HIV collaborative
MODULE SIX Global TB Institutions and Policy Framework Treatment Action Group TB/HIV Advocacy Toolkit 1 Topics to be Covered Global TB policy and coordinating structures The Stop TB Strategy TB/HIV collaborative
Replaces: 02/11/16. Formulated: 7/95 EMPLOYEE TB TESTING
 Effective : 02/09/17 Page 1 of 4 PURPOSE: To describe the process where by employees may obtain routine TB skin testing by facility medical staff. POLICY: Employees of the Texas Department of Criminal
Effective : 02/09/17 Page 1 of 4 PURPOSE: To describe the process where by employees may obtain routine TB skin testing by facility medical staff. POLICY: Employees of the Texas Department of Criminal
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
TB Laboratory for Nurses
 TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
Asking the Right Questions. A Visual Guide to Tuberculosis Case Management for Nurses. Reference Guide
 Asking the Right Questions A Visual Guide to Tuberculosis Case Management for Nurses Reference Guide The Francis J. Curry National Tuberculosis Center is a joint project of the San Francisco Department
Asking the Right Questions A Visual Guide to Tuberculosis Case Management for Nurses Reference Guide The Francis J. Curry National Tuberculosis Center is a joint project of the San Francisco Department
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Diagnosis & Management of Latent TB Infection
 Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
INTENSIFIED TB CASE FINDING
 INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
Tuberculosis Infection in the US Military
 Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
Core Curriculum on Tuberculosis: What the Clinician Should Know DR.RUPNATHJI( DR.RUPAK NATH )
") Core Curriculum on Tuberculosis: What the Clinician Should Know Introduction to the Core Curriculum on Tuberculosis: What the Clinician Should Know i Introduction to the Core Curriculum on Tuberculosis:
Core Curriculum on Tuberculosis: What the Clinician Should Know Introduction to the Core Curriculum on Tuberculosis: What the Clinician Should Know i Introduction to the Core Curriculum on Tuberculosis:
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Stop TB Poster (laminated copies are available from TB Control: )
") Tuberculosis Prevention and Control Recommendations For Homeless Shelters in Maine Tool Kit What Your Shelter Can Do to Prevent TB Assessing Your Shelter Guests Risk for TB Cough Alert Policy Think TB
Tuberculosis Prevention and Control Recommendations For Homeless Shelters in Maine Tool Kit What Your Shelter Can Do to Prevent TB Assessing Your Shelter Guests Risk for TB Cough Alert Policy Think TB
"GUARDING AGAINST TUBERCULOSIS IN INSTITUTIONAL FACILITIES"
 MAJOR PROGRAM POINTS "GUARDING AGAINST TUBERCULOSIS IN INSTITUTIONAL FACILITIES" Training For THE CDC "TUBERCULOSIS PREVENTION GUIDELINES" "Quality Safety and Health Products, for Today...and Tomorrow"
MAJOR PROGRAM POINTS "GUARDING AGAINST TUBERCULOSIS IN INSTITUTIONAL FACILITIES" Training For THE CDC "TUBERCULOSIS PREVENTION GUIDELINES" "Quality Safety and Health Products, for Today...and Tomorrow"
Tuberculosis Facts. TB is not spread by: Sharing food and drink Shaking someone s hand Touching bed lines or toilet seats
 Tuberculosis Facts Below are frequently asked questions about TB, and their answers. If you have additional questions you may contact the City of Ennis Department of Health Services at 972-875-1234 or
Tuberculosis Facts Below are frequently asked questions about TB, and their answers. If you have additional questions you may contact the City of Ennis Department of Health Services at 972-875-1234 or