Common Variable ImmunoDeficiency
|
|
|
- Tracy Caldwell
- 5 years ago
- Views:
Transcription


1 Common Variable ImmunoDeficiency (CVID) Nima Rezaei, MD, PhD Deputy President of Research Center for Immunodeficiencies, Children s Medical Center, Pediatrics Center of Excellence, Associate Dean of International Affairs, School of Medicine Director of Global Academic Program Tehran University of Medical Sciences, Tehran, Iran
2 Case 1 A 14-year-old patient, who had liver granuloma, extranodal marginal zone B-cell lymphoma, and autoimmune neutropenia. The patient was born to first-degree consanguineous parents. He developed pneumonia as well as lymphoproliferative manifestations, including retroperitoneal para-aortic lymph node hyperplasia and hepatosplenomegaly, leading to pancytopenia. The immunologic profile of this patient showed hypogammaglobulinemia: IgG, 320 mg/dl IgM, 30 mg/dl IgA, 15 mg/dl blood type O yet with an absence of anti-a and anti-b isohemagglutinins CD3, 78.2% CD4, 55.2% CD8, 20.0% CD19, 5.7% CD16, 11.9%

3 What is the diagnosis of the patient?
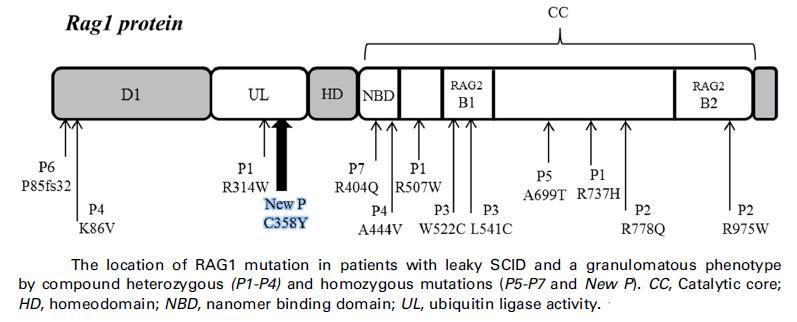
4 Mutations in all known gene defects associated with CVID (including CD19; CD20; CD21; CD81; ICOS; TACI; BAFFR; and LRBA) were ruled out by the exome sequencing data. Homozygosity mapping suggested one linkage to a Mb region on chromosome 11. We subsequently found a novel homozygous mutation (c. G1073A, p. C358Y) in the RAG1 gene, which is predicted to be probably damaging by using Polyphen 2. This mutation was confirmed by Sanger sequencing in the patient (homozygous form) and his parents (heterozygous form), who were asymptomatic. Furthermore, we performed a functional test for RAG1, and the results were consistent with a mild phenotype, atypical SCID with granuloma with a residual recombination activity of 48.8% 6 0.6% of wild-type protein, as measured by using an artificial green fluorescent protein substrate.
5
6 Case 2 A 14-month-old boy was admitted due to chronic diarrhea. He was the second child of consanguineous parents. He had a medical history of 4 previous hospitalizations because of pneumonia (at 7 months), febrile seizure (at 9 months), viral meningitis (at 11 months), and bronchiolitis and failure to thrive (at 12 months). The immunologic profile of this patient showed hypogammaglobulinemia: IgG, 100 mg/ dl IgA, 0 mg/dl IgM, 23 mg/dl isohemagglutinin titer, 0 White blood cells, 7700 cells/μl, lymphocytes, 2464 cells/μl CD3+, 1374 cells/ μl CD3+CD4+, 616 cells/ μl CD3+CD8+, 665 cells/μl CD19+, 714 cells/ μl CD16/56+, 167 cells/μl What is the diagnosis of the patient?

7 We found a known, homozygous mutation in p.v722i (c.2164g>a) in the JAK3 gene
8 Case 3 A 10-year-old boy is presented with recurrent infections and autoimmunity. His parents are cousins. He came with a history of an episode of severe upper respiratory infection and gastroenteritis leading to hospitalization at 2 years of age. Severe disseminated varicella infection occurred 8 months later and soon afterward he developed thrombocytopenia and splenomegaly The immunologic profile of this patient showed hypogammaglobulinemia: IgG, 47 mg/ dl IgA, 45 mg/dl IgM, 193 mg/dl White blood cells, 5800 cells/μl, lymphocytes, 1682 cells/μl CD3+, 1429 cells/ μl CD3+CD4+, 555 cells/ μl CD3+CD8+, 841 cells/μl CD19+, 134 cells/ μl CD16/56+, 176 cells/μl What is the diagnosis of the patient?


9 Bronchiolitis obliterans with organizing pneumonia (BOOP)
10
11
12 Primary antibody deficiencies (PAD) - The most common types of primary immunodeficiency diseases - Ranging from a severe reduction of all serum immunoglobulin classes and absent number of B cells to a selective antibody deficiency with normal serum immunoglobulin - Clinical manifestations: -Recurrent infections -Chronic inflammation -Autoimmunity -Cancers

13 Predominantly antibody deficiencies 2016 Recurrent bacterial infections e.g., Otitis media, pneumonia, sinusitis, diarrhea, sepsis
14 * X-linked Agammaglobulinemia Btk deficiency * AR-Agammaglobulinemia heavy chain deficiency 5 deficiency Ig deficiency Ig deficiency BLNK deficiency PI3KR1 deficiency * Other Forms of Agammaglobulinemia with Absent B-Cells TCF3 (E47) deficiency LRRC8 deficiency Thymoma with immunodeficiency and myelodysplasia with hypogammaglobulinemia
15 Immunoglobulin Class Switch Recombination Deficiencies CD40LG deficiency CD40 deficiency AICDA deficiency UNG deficiency INO80 deficiency MSH6 deficiency Other forms of CSR selective deficiency
16 * Selective IgA Deficiency * Other Immunoglobulin Isotypes or Light Chain Deficiencies Activated PI3K-delta PI3KR1 loss of function Isolated IgG subclass deficiency IgA with IgG subclass deficiency Ig heavy chain mutations/deletions IGKC deficiency light chain deficiency * Specific Antibody Deficiency with Normal Immunoglobulin Concentrations * Transient Hypogammaglobulinemia of Infancy * CARD11 gain of function
17 * Common Variable Immunodeficiency (CVID) * LRBA Deficiency * PI3KD Syndrome * CD19 Complex Deficiencies CD19 deficiency CD21 deficiency CD81 deficiency * CD20 Deficiency * Other Monogenic Defects Associated with Hypogammaglobulinemia ICOS deficiency TACI deficiency BAFF receptor deficiency TWEAK deficiency NFKB2 deficiency MOGS deficiency TRNT1 deficiency TTC37 deficiency




18 Definition CVID is a heterogeneous group of disorders characterized by Hypogammaglobulinemia Defective specific antibody production Recurrent and chronic infections Increased susceptibility to autoimmune disorders and cancers
19 - The most prevalent human PIDs requiring medical attention - Prevalence ranging from 1:10,000 to 1:50,000 - Affects males and females equally. - Broad clinical spectrum - Present at any age, but peaks of presentation is in childhood and early adult life - Average delay of 5 6 years between the onset of symptoms and diagnosis!

 was the main factor after diagnosis")

20 The total estimated cost of diagnosed CVID is US$274,200/patient annually and early diagnosis of the disease can save US$6500. Hospital admission cost (US$25,000/patient) accounts for the most important expenditure parameter before diagnosis, but medication cost (US$40,600/patients) was the main factor after diagnosis primarily due to monthly administration of immunoglobulin. The greatest cost-determining factor is the cost of treatment, spent mostly on immunoglobulin replacement therapy of the patients. CVID patients costs are reduced after diagnosis due to appropriate management.
21 Etiology - CVID was first described in 1953, but the basic molecular defect(s) is still unknown. - There is no single diagnostic immunological or genetic test for CVID - Its diagnosis relies on a decrease of immunoglobulins of at least two isotypes (serum IgG, IgA, and/or IgM), and genetic exclusion of other antibody deficiencies associated with well-defined single gene defects
22 Etiology Although the most CVID cases are sporadic, it has been estimated that 10 20% of the cases are familial. In multiple-case families, CVID is often present in one parent, accompanied by IgA deficiency (IgAD) in the descendants, and it has been estimated that about 15% of the patients with CVID have a first degree relative with either IgAD or CVID Some cases of IgAD, who progress to CVID, have been reported
23 Genetic Defects
24

25 Clinical Manifestations The main clinical symptoms associated with CVID patients are recurrent infections, autoimmune manifestations, lymphoma and other selected cancers. - Acute sino-pulmonary infections: pneumonia, sinusitis, and otitis - Chronic pulmonary disease: bronchiectasis, lymphoid interstitial pneumonitis, non-caseating granulomatous infiltrations PULMONARY Asthma or non-smoker s COPD LIP GLILD COP Follicular bronchiolitis /respiratory bronchiolitis (DIP) LIVER, BILE DUCTS Nodular lymphoid hyperplasia (Sclerosing Cholangitis Primary Biliary Cirrhosis Autoimmune Hepatitis GASTROINTESTINAL Malabsorption -B12 (parietal cell ab neg, C+A atrophy) - Vitamin A, D, E (zinc, iron) Celiac disease /autoimmune enteropathy -biopsy: often no plasma cells Inflammatory bowel disease -Crohn -like, CU-like, GVHD-like and their combinations, lymphocytic colitis SICCA -common w/o Sjogren THYROID -TPOAb LYMPHOID TISSUE &BLOOD -enlarged spleen -clinically benign clonality -Malignancy: B-nHL, others ITP AIHA Evans AINP, other neutropenias Pancytopenia, BM aplasia SKIN Psoriasis (+arthritis) Vitiligo, alopecia JOINTS JIA Rheumatoid arthritis Sjögren SLE Reactive arthritis - Gastrointestinal disease: nodular lymphoid hyperplasia, inflammatory bowel disease, sprue-like illness with flat villi, giardiasis and nonspecific malabsorption -Autoimmune diseases: autoimmune hemolytic anemia, thrombocytopenia, rheumatoid arthritis, pernicious anemia -Lymphoma and cancers: gastrointestinal tract adenocarcinoma, non-hodgkin lymphoma

26

27
28
 * Decreased levels of")
29 Clinical Characteristics of CVID * Recurrent pyogenic infections with extracellular encapsulated organisms, such as Streptococcus pneumoniae, Haemophilus influenzae type b, and group A Streptococcus * Otitis, sinusitis, recurrent pneumonia, bronchiectasis, and conjunctivitis * Few problems with fungal or viral infections (except enterovirus encephalitis and poliomyelitis) * Decreased levels of immunoglobulins in serum and secretions RHINOSINUSITIS Pneumococci, Haemophilus sp. Moraxella Tendency to need long ab courses and to recur LUNG INFECTIONS Pneumococci Haemophilus sp. S.aureus BRONCHIECTASIS recur GI INFECTIONS H.pylori: screen and treat!! Giardia: screen and treat Campylobacter Salmonella: MENINGITIS S.pneum, N.meningitidis purulent OTITIS CONJUCTIVITIS Purulent Often recur and together with sinusitis Sicca contributes SEPSIS ARTHRITIS -Mycoplasma (SKIN ABSCESSES) Sialadenitis * Diarrhea common, especially secondary to infection with Giardia lamblia * Growth retardation not striking * Compatible with survival to adulthood or for several years after onset unless complications occur
30 Immunological Defects - The core defect seems to be in late B cell differentiation, but the nature is unknown. - Other components of the immune system such as T cells or dendritic cells could also be involved. - Although most CVID patients have normal numbers of B cells, their B cells fail to differentiate into immunoglobulin-secreting plasma cells. - Consequently, CVID patients have reduced levels of serum immunoglobulin and respond abnormally to immunization with protein and polysaccharide antigens. - Reduced number of switched CD27+ memory B cells in CVID patients has been considered as a basis for sub-classification of CVID % have increased numbers of CD8+ T cells and a reduced CD4/CD8 ratio (<1).
31
32
33

34

35
36 Diagnosis The most important laboratory criterion for establishing the diagnosis of CVID is a low serum IgG concentration, ranging from profoundly reduced (<100 mg/dl) to just 2 SDs below the normal values for age Flow cytometry is important in evaluating numbers of peripheral B cells in patients with profound hypogammaglobulinemia. Numbers of B cells in the peripheral blood may be normal or reduced and approximately 13% of patients will have a B cell count of less than 3% in peripheral blood. Approximately half of the patients with CVID may have reduced T cell numbers and diminished lymphocyte proliferative responses to mitogens and antigens. Documenting impaired production of specific antibodies (isohemagglutinins and/or poor responses to one or more vaccines) is valuable for the diagnosis of CVID.
 Polysaccharide antigens: S.")
37 Tests for Antibody-Mediated Immunity * Quantitative immunoglobulin levels: IgG, IgA, IgM, IgE * Isohemagglutinin titers (anti-a, anti-b): measures IgM. function * Specific antibody levels: Protein antigens: diphtheria, tetanus Protein-conjugated antigens: Haemophilus influenzae, Streptococcus pneumoniae (conjugate vaccine) Polysaccharide antigens: S. pneumoniae (unconjugated vaccine) * B-cell numbers and subsets by flow cytometry

38 Approach to a patient with hypogammaglobulinemia
39 Management The mainstay of treatment for CVID is immunoglobulin replacement therapy. Intravenous (IVIG) or subcutaneous (SCIG) immunoglobulin prophylaxis can be used on a regular basis to maintain a trough level of at least mg/dl. The prognosis for patients with CVID depends on the frequency of infections, structural lung damage and concomitant presence of autoimmune disease. Other major factors in determining the prognosis is the extent of end-organ damage and the success of prophylaxis against infections. Patients and their families should thus be educated about early signs of infection in order not to delay treatment. Other forms of supportive care, such use of prophylactic antibiotics and good pulmonary hygiene, are important as bacterial infections may continue, albeit at a reduced rate, even with appropriate immunoglobulin replacement
40
41

42 Case 4 - A 2-year-old boy - History of recurrent respiratory infections - Absent tonsils with no lymphadenopathy - Low serum immunoglobulin levels (IgG: 90 mg/dl, IgA: 5 mg/dl, IgM: 10 mg/dl) Q1. Which of the following test could make a diagnosis? A- Nitro blue tetrazolium (NBT) test B- Lymphocyte subpopulation (B- and T- cell) enumeration C- Specific antibody responses D- Delayed cutaneous hypersensitivity
 B- Hyper IgM syndrome (HIGM) C- X-linked agammaglobulinemia (XLA) D- Severe")
43 Flow cytometry: CD3: 82%, CD4: 50%, CD8: 32%, CD19: 1% Q2. What is the most likely diagnosis? A- Common variable immunodeficiency (CVID) B- Hyper IgM syndrome (HIGM) C- X-linked agammaglobulinemia (XLA) D- Severe combined immunodeficiency (SCID)
44 Q3. Which gene defect is responsible for the disease? A- CD40LG B- BTK C- AID D- TACI Q4. What is the treatment of choice for this patient? A- Bone marrow transplantation B- Gene therapy C- Immunoglobulin replacement therapy D- Interferon-γ therapy
45 Case 5 A 12-year-old male patient with splenomegaly and otitis media and sinusitis. Immunological work-up showed WBC: 4,240/mm 3 lymphocytes: 42.4% IgG: 487 mg/dl (normal values for age: mg/dl) IgA: 29 mg/dl (normal values for age: mg/dl) IgM: 35 mg/dl (normal values for age: mg/dl) Antibody response to tetanus toxoid and hepatitis B were absent CD3: 73.5%, CD4: 30.5%, CD8: 35.5%, CD19: 11.6%, CD16: 15.1%. Proliferative response to mitogens was normal. Q1. Which is the most likely diagnosis? A- CVID B- X-linked HIGM C- Agammaglobulinemia D- XLP
46 The patient returned to our attention for the presence of jaundice. Additional laboratory findings included Red blood cell: 2,540,000/mm 3 haemoglobin: 8.1 g/dl hematocrit: 23.5% MCV: 92.7 fl bilirubin total: 18.8 mg/dl (direct: 0.84 mg/dl, indirect: mg/dl) Coombs test: positive Q2: What is the most likely diagnosis is? A- Autoimmune haemolytic anemia (AIHA) B- Leukemia C- Bone marrow failure D- Post-infectious anemia
47 The patient performed chest CT scan and abdominal sonography. Both imaging showed nodular lesions in the lung and spleen. Clinical examination was negative. Laboratory exams were negative. Q3. What could be the possible diagnosis? A- Lymphoma B- Neoplasia C- Metastatic lesions D- Granulomas Q4. Which of the following strategies could be used to evaluate the carrier status of the patient's mother or siblings for genetic counseling and family planning? A- Analysis of memory B cells B- TACI mutations analysis C- BAFF mutations analysis D- None
48 Q5. Which of the following is false about CVID? A- The patients usually, but not always, develop recurrent bacterial infections B- The minimum age used to diagnose a patient with CVID is 2 years C- Chest CT scan should be performed for older patients to exclude the presence of a thymoma D- Lymphoid malignancies should be excluded before the diagnosis of CVID is secured. Q6. What is the treatment of choice for CVID patients? A- Bone marrow transplantation B- GCSF therapy C- IVIG therapy D- IFN-g therapy.
49 Q7. All of the following can be the probable cause of adverse reactions following the administration of IVIG in this patient, except: A- Fast infusion rate B- Anti-IgA antibodies C- Intercurrent infection D- Autoimmunity Q8. If a patient with CVID receiving IVIG develops mild and minor adverse reactions, what would be the best step to take? A- Slowing the infusion rate of IVIG B- Discontinuing the infusion of IVIG C- Discontinuing the infusion of IVIG and administration of epinephrine E- Recommending longer interval between IVIG infusion




50 References * Picard C, et al. Primary Immunodeficiency Diseases: an Update on the Classification from the International Union of Immunological Societies Expert Committee for Primary Immunodeficiency J Clin Immunol Oct 19. * Bpusfiha A, et al. The 2015 IUIS Phenotypic Classification for Primary Immunodeficiencies. J Clin Immunol Oct 7.

51 Thank you for your attention
PRIMARY IMMUNODEFICIENCIES CVID MANAGEMENT CVID MANAGEMENT
 PRIMARY IMMUNODEFICIENCIES CVID MANAGEMENT CVID MANAGEMENT 1 PRIMARY IMMUNODEFICIENCIES KEY ABBREVIATIONS CVID CT IgA IgG IgM IPOPI IVIG SCIG PID Common Variable Immune Deficiency Computerised tomography
PRIMARY IMMUNODEFICIENCIES CVID MANAGEMENT CVID MANAGEMENT 1 PRIMARY IMMUNODEFICIENCIES KEY ABBREVIATIONS CVID CT IgA IgG IgM IPOPI IVIG SCIG PID Common Variable Immune Deficiency Computerised tomography
A heterogeneous collection of diseases characterised by hypogammaglobulinemia.
 1 Common variable immunodeficiency () A heterogeneous collection of diseases characterised by hypogammaglobulinemia. Although is the most common primary immune deficiency (PID) symptomatic in adults, it
1 Common variable immunodeficiency () A heterogeneous collection of diseases characterised by hypogammaglobulinemia. Although is the most common primary immune deficiency (PID) symptomatic in adults, it
Autoimmunity and Primary Immune Deficiency
 Autoimmunity and Primary Immune Deficiency Mark Ballow, MD Division of Allergy & Immunology USF Morsani School of Medicine Johns Hopkins All Children s Hospital St Petersburg, FL The Immune System What
Autoimmunity and Primary Immune Deficiency Mark Ballow, MD Division of Allergy & Immunology USF Morsani School of Medicine Johns Hopkins All Children s Hospital St Petersburg, FL The Immune System What
COMMON VARIABLE IMMUNODEFICIENCY
 COMMON VARIABLE IMMUNODEFICIENCY This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 COMMON VARIABLE IMMUNODEFICIENCY Also available
COMMON VARIABLE IMMUNODEFICIENCY This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 COMMON VARIABLE IMMUNODEFICIENCY Also available
Primary Immunodeficiency
 Primary Immunodeficiency DiGeorge Syndrome Severe Combined Immunodeficiency SCID X-Linked Agammaglobulinemia Common variable immunodeficiency (CVID) IgA deficiency Hyper- IgM Syndrome Wiskott-Aldrich syndrome
Primary Immunodeficiency DiGeorge Syndrome Severe Combined Immunodeficiency SCID X-Linked Agammaglobulinemia Common variable immunodeficiency (CVID) IgA deficiency Hyper- IgM Syndrome Wiskott-Aldrich syndrome
Is it CVID? Not Necessarily HAIG TCHEUREKDJIAN, MD
 Is it CVID? Not Necessarily HAIG TCHEUREKDJIAN, MD Current Paradigm of Pathogenesis Genetic defect(s) Molecular defect(s) Cellular defect(s) Clinical disease Current Paradigm of Pathogenesis Genetic defect(s)
Is it CVID? Not Necessarily HAIG TCHEUREKDJIAN, MD Current Paradigm of Pathogenesis Genetic defect(s) Molecular defect(s) Cellular defect(s) Clinical disease Current Paradigm of Pathogenesis Genetic defect(s)
Chapter 11. Hyper IgM Syndromes
 Chapter 11 Hyper IgM Syndromes Patients with Hyper-IgM (HIGM) syndrome are susceptible to recurrent and severe infections and in some types of HIGM syndrome opportunistic infections and an increased risk
Chapter 11 Hyper IgM Syndromes Patients with Hyper-IgM (HIGM) syndrome are susceptible to recurrent and severe infections and in some types of HIGM syndrome opportunistic infections and an increased risk
HYPER IgM SYNDROME This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist.
 HYPER IgM SYNDROME This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 HYPER IgM SYNDROME Also available : COMMON VARIABLE IMMUNODEFICIENCY
HYPER IgM SYNDROME This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 HYPER IgM SYNDROME Also available : COMMON VARIABLE IMMUNODEFICIENCY
X-linked agammaglobulinemia (XLA)
") X-linked agammaglobulinemia (XLA) hello@piduk.org 0800 987 898 www.piduk.org About this booklet This booklet provides information on X-linked agammaglobulinemia (XLA). It has been produced by the PID UK
X-linked agammaglobulinemia (XLA) hello@piduk.org 0800 987 898 www.piduk.org About this booklet This booklet provides information on X-linked agammaglobulinemia (XLA). It has been produced by the PID UK
When should a Primary Immunodeficiency be Suspected?
 When should a Primary Immunodeficiency be Suspected? Ricardo U Sorensen. MD Head, Jeffrey Modell Diagnostic Center for Primary Immunodeficiencies. LSUHSC, New Orleans Learning Objectives Define Primary
When should a Primary Immunodeficiency be Suspected? Ricardo U Sorensen. MD Head, Jeffrey Modell Diagnostic Center for Primary Immunodeficiencies. LSUHSC, New Orleans Learning Objectives Define Primary
New proposals for partial antibody deficiencies
 New proposals for partial antibody deficiencies Helen Chapel, Janne Bjorkander,, Mary-Ellen Conley, Teresa Espanol,, Amos Etzioni, Bodo Grimacher, Lennart Hammarstrom,, Maria Kanariou,, Luigi Notarangelo,,
New proposals for partial antibody deficiencies Helen Chapel, Janne Bjorkander,, Mary-Ellen Conley, Teresa Espanol,, Amos Etzioni, Bodo Grimacher, Lennart Hammarstrom,, Maria Kanariou,, Luigi Notarangelo,,
Problem 7 Unit 6 Clinical: Primary immunodeficiency
 Problem 7 Unit 6 Clinical: Primary immunodeficiency THE IMMUNE SYSTEM - Function: recognizing pathogens (foreign non-self antigens) and organizing a defense response against them by facilitating destruction
Problem 7 Unit 6 Clinical: Primary immunodeficiency THE IMMUNE SYSTEM - Function: recognizing pathogens (foreign non-self antigens) and organizing a defense response against them by facilitating destruction
Immunodeficiency. (1 of 2)
") Immunodeficiency (1 of 2) Primary immunodeficiency diseases Innate or adaptive Most are detected in infancy (6 months 2 years) Rare but some mild genetic forms exist in many individuals Defects in Innate
Immunodeficiency (1 of 2) Primary immunodeficiency diseases Innate or adaptive Most are detected in infancy (6 months 2 years) Rare but some mild genetic forms exist in many individuals Defects in Innate
3/29/2011. Algorithms for Diagnosis of Suspected Immunodeficiency. Overview. Case #1. Case #2. Primary Immunodeficiency (PID) Case #3
 Case #3") Overview Algorithms for Diagnosis of Immuno Susan M. Orton, PhD, D(ABMLI), MT(ASCP) Associate Professor Four major categories of primary immuno (PID) Clinical conditions associated with PID and organisms
Overview Algorithms for Diagnosis of Immuno Susan M. Orton, PhD, D(ABMLI), MT(ASCP) Associate Professor Four major categories of primary immuno (PID) Clinical conditions associated with PID and organisms
IgG subclass deficiencies
 IgG subclass deficiencies hello@piduk.org 0800 987 8986 www.piduk.org About this booklet This booklet provides information on IgG subclass deficiencies. It has been produced by the PID UK Medical Advisory
IgG subclass deficiencies hello@piduk.org 0800 987 8986 www.piduk.org About this booklet This booklet provides information on IgG subclass deficiencies. It has been produced by the PID UK Medical Advisory
Updated data of a nation-wide study of clinical phenotypes and TACI mutations in patients with common variable immunodeficiency (CVID).
.") University of Thessaly School of Health Sciences Faculty of Medicine Department of Immunology-Histocompatibility Οn behalf of the Study Group of Primary Immunodeficiencies of the Hellenic Hematology Association.
University of Thessaly School of Health Sciences Faculty of Medicine Department of Immunology-Histocompatibility Οn behalf of the Study Group of Primary Immunodeficiencies of the Hellenic Hematology Association.
ESIM: Winter School in Riga Case report
 ESIM: Winter School in Riga 2015 Case report Imanta Ozola Zālīte Pauls Stradins Clinical University Hospital Latvia 29.01.2015. January, 2006 32 y., man 2-3 weeks fatigue fluidal stool 2 times per day
ESIM: Winter School in Riga 2015 Case report Imanta Ozola Zālīte Pauls Stradins Clinical University Hospital Latvia 29.01.2015. January, 2006 32 y., man 2-3 weeks fatigue fluidal stool 2 times per day
WISKOTT-ALDRICH SYNDROME. An X-linked Primary Immunodeficiency
 WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
Form 2033 R3.0: Wiskott-Aldrich Syndrome Pre-HSCT Data
 Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Has this patient's data been previously reported to USIDNET? USIDNET ID: Today's Date: - - Date of HSCT for which
Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Has this patient's data been previously reported to USIDNET? USIDNET ID: Today's Date: - - Date of HSCT for which
Case Presentations in Primary Immune Deficiency Diseases. John W. Sleasman, M.D. St Petersburg, FL Mark Ballow, M.D. Buffalo NY & Sarasota, FL
 Case Presentations in Primary Immune Deficiency Diseases John W. Sleasman, M.D. St Petersburg, FL Mark Ballow, M.D. Buffalo NY & Sarasota, FL COPD and recurrent infections 42 WF non- smoker with diagnosis
Case Presentations in Primary Immune Deficiency Diseases John W. Sleasman, M.D. St Petersburg, FL Mark Ballow, M.D. Buffalo NY & Sarasota, FL COPD and recurrent infections 42 WF non- smoker with diagnosis
Luke Droney IMMUNOGLOBULIN LEVELS AND FUNCTION
 IMMUNOGLOBULIN LEVELS AND FUNCTION Interpret changes in immunoglobulin levels within the clinical context including - Immunodeficiency - Disorders characterised by hypergammaglobulinaemia, rheumatoid arthritis,
IMMUNOGLOBULIN LEVELS AND FUNCTION Interpret changes in immunoglobulin levels within the clinical context including - Immunodeficiency - Disorders characterised by hypergammaglobulinaemia, rheumatoid arthritis,
What is your diagnosis? a. Lymphocytic colitis. b. Collagenous colitis. c. Common variable immunodeficiency (CVID) associated colitis
 associated colitis") Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
Immune Deficiency Primary and Secondary. Dr Liz McDermott Immunology Department NUH
 Immune Deficiency Primary and Secondary Dr Liz McDermott Immunology Department NUH Summary Different types of Immune Deficiency Why it is important to identify immune deficiency? Diagnostic delay Antibody
Immune Deficiency Primary and Secondary Dr Liz McDermott Immunology Department NUH Summary Different types of Immune Deficiency Why it is important to identify immune deficiency? Diagnostic delay Antibody
Patient Identification: Patient Name (first, middle, last)
") Patient Identification: Patient Name (first, middle, last) Patient s USIDNET Registry Number assigned after online enrollment Date of Birth / / (mm/dd/yyyy) or Year of Birth Gender: male [ ], female [
Patient Identification: Patient Name (first, middle, last) Patient s USIDNET Registry Number assigned after online enrollment Date of Birth / / (mm/dd/yyyy) or Year of Birth Gender: male [ ], female [
Wiskott-Aldrich Syndrome
 chapter 7 Wiskott-Aldrich Syndrome Wiskott-Aldrich syndrome is a primary immunodeficiency disease involving both T- and B-lymphocytes. In addition, the blood cells that help control bleeding, called platelets
chapter 7 Wiskott-Aldrich Syndrome Wiskott-Aldrich syndrome is a primary immunodeficiency disease involving both T- and B-lymphocytes. In addition, the blood cells that help control bleeding, called platelets
Wiskott-Aldrich Registry Data Collection Form Patient Identification: Patient Name (first, middle, last)
") Patient Identification: Patient Name (first, middle, last) Patient s USIDNET Registry Number assigned after online enrollment Date of Birth / / (mm/dd/yyyy) or Year of Birth Gender: male [ ], female [
Patient Identification: Patient Name (first, middle, last) Patient s USIDNET Registry Number assigned after online enrollment Date of Birth / / (mm/dd/yyyy) or Year of Birth Gender: male [ ], female [
Approach to a child with recurrent infections. Dave le Roux 9 March 2012
 Approach to a child with recurrent infections Dave le Roux 9 March 2012 Jeffrey Modell Foundation http://www.info4pi.org Primary immune deficiencies: myths PID s are very very rare Selective IgA 1:333
Approach to a child with recurrent infections Dave le Roux 9 March 2012 Jeffrey Modell Foundation http://www.info4pi.org Primary immune deficiencies: myths PID s are very very rare Selective IgA 1:333
Support for Immune Globulin Replacement Therapy in IgG Subclass Deficiency. Michelle Huffaker, MD Stanford University
 Support for Immune Globulin Replacement Therapy in IgG Subclass Deficiency Michelle Huffaker, MD Stanford University Disclosures I have nothing to disclose What is an IgG subclass? Subclass IgG1 IgG2 IgG3
Support for Immune Globulin Replacement Therapy in IgG Subclass Deficiency Michelle Huffaker, MD Stanford University Disclosures I have nothing to disclose What is an IgG subclass? Subclass IgG1 IgG2 IgG3
Recurrent Infection, Pulmonary Disease, and Autoimmunity as Manifestations of Immune Deficiency
 Recurrent Infection, Pulmonary Disease, and Autoimmunity as Manifestations of Immune Deficiency Erwin W. Gelfand, M.D. Professor, Department of Pediatrics National Jewish Health Professor of Immunology
Recurrent Infection, Pulmonary Disease, and Autoimmunity as Manifestations of Immune Deficiency Erwin W. Gelfand, M.D. Professor, Department of Pediatrics National Jewish Health Professor of Immunology
Osteosclerotic Myeloma (POEMS Syndrome)
") Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Immunology and the middle ear Andrew Riordan
 Immunology and the middle ear Andrew Riordan The Immune system is NOT there; To baffle medical students To keep Immunologists in a job To encourage experiments on mice The Immune system IS there as a defence
Immunology and the middle ear Andrew Riordan The Immune system is NOT there; To baffle medical students To keep Immunologists in a job To encourage experiments on mice The Immune system IS there as a defence
IgA: Biology and deficiency
 Introduction to IgA First described in 1953 IgA: Biology and deficiency Dr Sarah Sasson SydPATH Registrar 14 th July 2014 Most abundant and heterogeneous antibody isotype produced in the body 66mg/kg/day-
Introduction to IgA First described in 1953 IgA: Biology and deficiency Dr Sarah Sasson SydPATH Registrar 14 th July 2014 Most abundant and heterogeneous antibody isotype produced in the body 66mg/kg/day-
Immunodeficiency. By Dr. Gouse Mohiddin Shaik
 Immunodeficiency By Dr. Gouse Mohiddin Shaik Immunodeficieny Immunodeficiency is failure of immune system to protect against disease or malignency Immunodeficiency is of two types Primary Secondary immunodeficiency
Immunodeficiency By Dr. Gouse Mohiddin Shaik Immunodeficieny Immunodeficiency is failure of immune system to protect against disease or malignency Immunodeficiency is of two types Primary Secondary immunodeficiency
Common variable immunodeficiency: familial inheritance and autoimmune manifestations in two siblings
 The Turkish Journal of Pediatrics 2010; 52: 89-93 Case Common variable immunodeficiency: familial inheritance and autoimmune manifestations in two siblings Neslihan Edeer-Karaca, Nesrin Gülez, Güzide Aksu,
The Turkish Journal of Pediatrics 2010; 52: 89-93 Case Common variable immunodeficiency: familial inheritance and autoimmune manifestations in two siblings Neslihan Edeer-Karaca, Nesrin Gülez, Güzide Aksu,
Predominantly Antibody Deficiencies
 Immunology and Genetics Journal (2018) 1:52-80 Doi: 10.22034/igj.2018.80253 Review Predominantly Antibody Deficiencies Gholamreza Azizi 1, Reza Yazdani 2 * Received: 17 July 2018/ Accepted: 20 November
Immunology and Genetics Journal (2018) 1:52-80 Doi: 10.22034/igj.2018.80253 Review Predominantly Antibody Deficiencies Gholamreza Azizi 1, Reza Yazdani 2 * Received: 17 July 2018/ Accepted: 20 November
New Diagnosis of Common Variable Immunodeficiency in a 12-Year-Old With Pneumonia: An Illustrative Case
 ILLUSTRATIVE CASE New Diagnosis of Common Variable Immunodeficiency in a 12-Year-Old With Pneumonia: An Illustrative Case AUTHORS Stefani Samples, MD, 1 Nirupma Sharma, MD, 2 and Dennis Ownby, MD 3 1 Department
ILLUSTRATIVE CASE New Diagnosis of Common Variable Immunodeficiency in a 12-Year-Old With Pneumonia: An Illustrative Case AUTHORS Stefani Samples, MD, 1 Nirupma Sharma, MD, 2 and Dennis Ownby, MD 3 1 Department
Clinical Immunology of Immunodeficiencies: More than Just Recurrent Infections. Disclosure. Lecture Objectives
 Clinical Immunology of Immunodeficiencies: More than Just Recurrent Infections New England Allergy Society 2018 Annual Meeting Plymouth, MA Thomas A. Fleisher, MD, FAAAAI, FACAAI Executive Vice President,
Clinical Immunology of Immunodeficiencies: More than Just Recurrent Infections New England Allergy Society 2018 Annual Meeting Plymouth, MA Thomas A. Fleisher, MD, FAAAAI, FACAAI Executive Vice President,
Immunodeficiency and Skin (September 21, 2018) By (Arti Nanda, MD, DNBE [Kuwait])
![Immunodeficiency and Skin (September 21, 2018) By (Arti Nanda, MD, DNBE [Kuwait])](/thumbs/90/103062332.jpg "Immunodeficiency and Skin (September 21, 2018) By (Arti Nanda, MD, DNBE [Kuwait])") Immunodeficiency and Skin (September 21, 2018) By (Arti Nanda, MD, DNBE [Kuwait]) Immune deficiency refers to a state in which part of immune system is missing or defective resulting into an inability
Immunodeficiency and Skin (September 21, 2018) By (Arti Nanda, MD, DNBE [Kuwait]) Immune deficiency refers to a state in which part of immune system is missing or defective resulting into an inability
Thrombocytopenia in common variable immunodeficiency patients clinical course, management, and effect of immunoglobulins
 Clinical immunology DOI: 10.5114/ceji.2015.50838 Thrombocytopenia in common variable immunodeficiency patients clinical course, management, and effect of immunoglobulins ANNA PITUCH-NOWOROLSKA 1, MACIEJ
Clinical immunology DOI: 10.5114/ceji.2015.50838 Thrombocytopenia in common variable immunodeficiency patients clinical course, management, and effect of immunoglobulins ANNA PITUCH-NOWOROLSKA 1, MACIEJ
Agammaglobulinemia. Vilnius University Children s s Hospital Pediatric Center, R.Duobiene
 Agammaglobulinemia Vilnius University Children s s Hospital Pediatric Center, R.Duobiene Case report R.B., male, born on February 1997. The parents are consanguineous. Eyes pathology in fathers family
Agammaglobulinemia Vilnius University Children s s Hospital Pediatric Center, R.Duobiene Case report R.B., male, born on February 1997. The parents are consanguineous. Eyes pathology in fathers family
IVIG (intravenous immunoglobulin) Bivigam, Carimune NF, Flebogamma, Gammagard, Gammagard S/D, Gammaked, Gammaplex, Gamunex-C, Octagam, Privigen
 Bivigam, Carimune NF, Flebogamma, Gammagard, Gammagard S/D, Gammaked, Gammaplex, Gamunex-C, Octagam, Privigen") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following documented indications: 1. Primary Immunodeficiency Disease (PID) with ONE of the a. Hypogammaglobulinemia,
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following documented indications: 1. Primary Immunodeficiency Disease (PID) with ONE of the a. Hypogammaglobulinemia,
Pneumococcal meningitis in a young adult female with common variable immunodeficiency
 ISSN 1507-6164 DOI: 10.12659/AJCR.889617 Received: 2013.07.26 Accepted: 2013.08.06 Published: 2013.11.12 Pneumococcal meningitis in a young adult female with common variable immunodeficiency Authors Contribution:
ISSN 1507-6164 DOI: 10.12659/AJCR.889617 Received: 2013.07.26 Accepted: 2013.08.06 Published: 2013.11.12 Pneumococcal meningitis in a young adult female with common variable immunodeficiency Authors Contribution:
IMMU 7630 Fall 2011 IMMUNODEFICIENCY
 IMMUNODEFICIENCY CATEGORIES OF IMMUNODEFICIENCY STATES. Immunodeficiency can be primary or secondary. Primary immunodeficiency means a disease with a genetic cause, while secondary implies that some known
IMMUNODEFICIENCY CATEGORIES OF IMMUNODEFICIENCY STATES. Immunodeficiency can be primary or secondary. Primary immunodeficiency means a disease with a genetic cause, while secondary implies that some known
Approaching Neutropenia in Children. SW Florida Osteopathic Medical Society: 39 th Annual Seminars in Family Practice
 Approaching Neutropenia in Children SW Florida Osteopathic Medical Society: 39 th Annual Seminars in Family Practice Approaching Neutropenia in Children Emad Salman M.D Golisano Children s Hospital of
Approaching Neutropenia in Children SW Florida Osteopathic Medical Society: 39 th Annual Seminars in Family Practice Approaching Neutropenia in Children Emad Salman M.D Golisano Children s Hospital of
Primary Immunodeficiency Disease: Underdiagnosed at any age. Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc.
 Primary Immunodeficiency Disease: Underdiagnosed at any age Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc. Learning Objectives Identify the difference between primary and secondary
Primary Immunodeficiency Disease: Underdiagnosed at any age Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc. Learning Objectives Identify the difference between primary and secondary
Pathogenesis, Diagnosis, and Management of Primary Antibody Deficiencies and Infections
 CLINICAL MICROBIOLOGY REVIEWS, July 2009, p. 396 414 Vol. 22, No. 3 0893-8512/09/$08.00 0 doi:10.1128/cmr.00001-09 Copyright 2009, American Society for Microbiology. All Rights Reserved. Pathogenesis,
CLINICAL MICROBIOLOGY REVIEWS, July 2009, p. 396 414 Vol. 22, No. 3 0893-8512/09/$08.00 0 doi:10.1128/cmr.00001-09 Copyright 2009, American Society for Microbiology. All Rights Reserved. Pathogenesis,
References and supporting documents 9 Roles and responsibilities 10
 Common Variable Immunodeficiency (CVID) - diagnosis and Classification: Protocol Lead Author: Dr Hana Alachkar Additional author(s): Dr Archana Herwadkar Authors Division: CSS, Renal and Tertiary Medicine
Common Variable Immunodeficiency (CVID) - diagnosis and Classification: Protocol Lead Author: Dr Hana Alachkar Additional author(s): Dr Archana Herwadkar Authors Division: CSS, Renal and Tertiary Medicine
Infectious and Non Infectious Complications among Undiagnosed Patients with Common Variable Immunodeficiency
 Original Article Iran J Pediatr Dec 2009; Vol 19 (No 4), Pp:367-375 Infectious and Non Infectious Complications among Undiagnosed Patients with Common Variable Immunodeficiency Asghar Aghamohammadi* 1,2,
Original Article Iran J Pediatr Dec 2009; Vol 19 (No 4), Pp:367-375 Infectious and Non Infectious Complications among Undiagnosed Patients with Common Variable Immunodeficiency Asghar Aghamohammadi* 1,2,
Clinical Cases: Diagnosis and Management of Primary Immunodeficiency Around the World
 Primary Immune Deficiency: A Global Perspective Friday, February 28, 2014: 2:00 PM-5:00 PM Clinical Cases: Diagnosis and Management of Primary Immunodeficiency Around the World Elham Hossny, MD, PhD, FAAAAI
Primary Immune Deficiency: A Global Perspective Friday, February 28, 2014: 2:00 PM-5:00 PM Clinical Cases: Diagnosis and Management of Primary Immunodeficiency Around the World Elham Hossny, MD, PhD, FAAAAI
Rituximab for granulomatous lymphocytic interstitial lung disease in a patient with common variable immunodeficiency. Is single therapy enough?
 International Journal of Clinical Rheumatology Rituximab for granulomatous lymphocytic interstitial lung disease in a patient with common variable immunodeficiency. Is single therapy enough? bstract: Granulomatous
International Journal of Clinical Rheumatology Rituximab for granulomatous lymphocytic interstitial lung disease in a patient with common variable immunodeficiency. Is single therapy enough? bstract: Granulomatous
Secondary Immunodeficiency
 A guide for patients, their families, friends and healthcare professionals Raising awareness and supporting patients with immunodeficiencies in Australia. Secondary Immunodeficiency Edition 1 Date 15 th
A guide for patients, their families, friends and healthcare professionals Raising awareness and supporting patients with immunodeficiencies in Australia. Secondary Immunodeficiency Edition 1 Date 15 th
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Severe Congenital Neutropenia in Iran
 Severe Congenital Neutropenia in Iran Nima Rezaei, MD Department of Allergy and Clinical Immunology of Children's Medical Center, Immunology, Asthma and Allergy Research Institute, Tehran University of
Severe Congenital Neutropenia in Iran Nima Rezaei, MD Department of Allergy and Clinical Immunology of Children's Medical Center, Immunology, Asthma and Allergy Research Institute, Tehran University of
Clinical Immunodeficiency. Dr Claire Bethune Consultant Immunologist
 Clinical Immunodeficiency Dr Claire Bethune Consultant Immunologist Peninsula Specialist Immunodeficiency and Allergy service Eden Unit, Derriford https://www.plymouthhospitals.nhs. uk/eden Or Google Immunology
Clinical Immunodeficiency Dr Claire Bethune Consultant Immunologist Peninsula Specialist Immunodeficiency and Allergy service Eden Unit, Derriford https://www.plymouthhospitals.nhs. uk/eden Or Google Immunology
Advanced Laboratory studies for Primary Immunodeficiency Disorders
 4813: Problem-based Learning Workshop Advanced Laboratory studies for Primary Immunodeficiency Disorders Moderator: Richard Wasserman, MD, PhD Discussion Leader: Roshini Abraham, PhD Understand B cell
4813: Problem-based Learning Workshop Advanced Laboratory studies for Primary Immunodeficiency Disorders Moderator: Richard Wasserman, MD, PhD Discussion Leader: Roshini Abraham, PhD Understand B cell
Immunodeficiency and Autoimmunity
 Immunodeficiency and Autoimmunity JOCELYN JIANG WESTMEAD HOSPITAL ICPMR Case 1 42 year old woman referred for investigation for lymphopenia Incidental finding on routine bloods Lymphocyte count 0.5 x 10^9/L
Immunodeficiency and Autoimmunity JOCELYN JIANG WESTMEAD HOSPITAL ICPMR Case 1 42 year old woman referred for investigation for lymphopenia Incidental finding on routine bloods Lymphocyte count 0.5 x 10^9/L
International Conference on Parasitology August 24-26, 2015 Philadelphia, Pennsylvania, USA
 International Conference on Parasitology August 24-26, 2015 Philadelphia, Pennsylvania, USA SYMPOSIA THE CHALLENGE OF PARASITES AND IMMUNOSUPRESSION: FROM DIAGNOSIS TO TREATMENT from the bench to the bed
International Conference on Parasitology August 24-26, 2015 Philadelphia, Pennsylvania, USA SYMPOSIA THE CHALLENGE OF PARASITES AND IMMUNOSUPRESSION: FROM DIAGNOSIS TO TREATMENT from the bench to the bed
World Allergy Congress Dec. 4-8, condi5ons that effect long term survival
 Common Variable Immunodeficiency - Co- morbid Condi4ons Mark Ballow, MD Division of Allergy & Immunology, School of Medicine and Biomedical Sciences Women & Children s Hospital of Buffalo Mark Ballow:
Common Variable Immunodeficiency - Co- morbid Condi4ons Mark Ballow, MD Division of Allergy & Immunology, School of Medicine and Biomedical Sciences Women & Children s Hospital of Buffalo Mark Ballow:
Case #1. Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute
 Case #1 Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute Patient History Part I 76 year-old man 1997 diagnosed with MGUS (biclonal) during evaluation of (self-limited) anemia.
Case #1 Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute Patient History Part I 76 year-old man 1997 diagnosed with MGUS (biclonal) during evaluation of (self-limited) anemia.
IMMUNODEFICIENCIES CLASSIFICATION OF PIDS PRIMARY IMMUNODEFICIENCIES CLASSIFIED?
 PRIMARY IMMUNODEFICIENCIES CLASSIFICATION OF PIDS HOW ARE PRIMARY IMMUNODEFICIENCIES CLASSIFIED? 1 PRIMARY IMMUNODEFICIENCIES KEY ABBREVIATIONS CGD CVID IBD IgA/D/E/G/M IPOPI PID SCID Chronic granulomatous
PRIMARY IMMUNODEFICIENCIES CLASSIFICATION OF PIDS HOW ARE PRIMARY IMMUNODEFICIENCIES CLASSIFIED? 1 PRIMARY IMMUNODEFICIENCIES KEY ABBREVIATIONS CGD CVID IBD IgA/D/E/G/M IPOPI PID SCID Chronic granulomatous
Immunodeficiency: Recognizing Subtle Signs, Diagnosis & Referral
 Immunodeficiency: Recognizing Subtle Signs, Diagnosis & Referral Michael Daines, M.D. Associate Professor, Pediatric Allergy and Immunology Division director, Pediatric Allergy, Immunology, and Rheumatology
Immunodeficiency: Recognizing Subtle Signs, Diagnosis & Referral Michael Daines, M.D. Associate Professor, Pediatric Allergy and Immunology Division director, Pediatric Allergy, Immunology, and Rheumatology
Reports of efficacy and safety studies of primary immunodeficiency
 2. SYNOPSIS TITLE OF STUDY: Clinical Study to Evaluate the Safety, Efficacy, and Pharmacokinetics of IGIV3I GRIFOLS [Immune Globulin Intravenous (Human)] for Replacement Therapy in Primary Immunodeficiency
2. SYNOPSIS TITLE OF STUDY: Clinical Study to Evaluate the Safety, Efficacy, and Pharmacokinetics of IGIV3I GRIFOLS [Immune Globulin Intravenous (Human)] for Replacement Therapy in Primary Immunodeficiency
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
How the Immune System Works (and Fails) in 45 Minutes or Less. Disclosures. Learning Objectives 10/15/2014. Nothing to Disclose
 in 45 Minutes or Less. Disclosures. Learning Objectives 10/15/2014. Nothing to Disclose") How the Immune System Works (and Fails) in 45 Minutes or Less Christina Ciaccio MD, MSc Assistant Professor of Medicine and Pediatrics Nothing to Disclose Disclosures Learning Objectives List s involved
How the Immune System Works (and Fails) in 45 Minutes or Less Christina Ciaccio MD, MSc Assistant Professor of Medicine and Pediatrics Nothing to Disclose Disclosures Learning Objectives List s involved
Vitamin D Assay Testing For services performed on or after
 2018 MEDICARE LOCAL COVERAGE DETERMINATION (LCD) - L36692 CPT CODES: 82306, 82652 Vitamin D Assay Testing For services performed on or after 2-3-2017 DLS TEST CODE AND NAME 49907 (1,25 DIHYDROXY) (CPT
2018 MEDICARE LOCAL COVERAGE DETERMINATION (LCD) - L36692 CPT CODES: 82306, 82652 Vitamin D Assay Testing For services performed on or after 2-3-2017 DLS TEST CODE AND NAME 49907 (1,25 DIHYDROXY) (CPT
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Primary Immunodeficiencies and Sinusitis. Disclosure. Learning Objectives 3/31/2014. none
 Primary Immunodeficiencies and Sinusitis Hey Jin Chong MD PhD Assistant Professor Of Pediatrics Children s Hospital Of Pittsburgh Division of Pulmonary Medicine, Allergy & Immunology none Disclosure Learning
Primary Immunodeficiencies and Sinusitis Hey Jin Chong MD PhD Assistant Professor Of Pediatrics Children s Hospital Of Pittsburgh Division of Pulmonary Medicine, Allergy & Immunology none Disclosure Learning
SCID:failing the final exam on day 1
 SCID:failing the final exam on day 1 Michael Daines, M.D. Associate Professor, Pediatric Allergy and Immunology Division director, Pediatric Allergy, Immunology, and Rheumatology Disclosures Nothing relevant
SCID:failing the final exam on day 1 Michael Daines, M.D. Associate Professor, Pediatric Allergy and Immunology Division director, Pediatric Allergy, Immunology, and Rheumatology Disclosures Nothing relevant
Helminth worm, Schistosomiasis Trypanosomes, sleeping sickness Pneumocystis carinii. Ringworm fungus HIV Influenza
 Helminth worm, Schistosomiasis Trypanosomes, sleeping sickness Pneumocystis carinii Ringworm fungus HIV Influenza Candida Staph aureus Mycobacterium tuberculosis Listeria Salmonella Streptococcus Levels
Helminth worm, Schistosomiasis Trypanosomes, sleeping sickness Pneumocystis carinii Ringworm fungus HIV Influenza Candida Staph aureus Mycobacterium tuberculosis Listeria Salmonella Streptococcus Levels
PROBLEMS WITH THE IMMUNE SYSTEM. Blood Types, Transplants, Allergies, Autoimmune diseases, Immunodeficiency Diseases
 PROBLEMS WITH THE IMMUNE SYSTEM Blood Types, Transplants, Allergies, Autoimmune diseases, Immunodeficiency Diseases Antigens on red blood cells determine whether a person has type A, B, AB, or O blood
PROBLEMS WITH THE IMMUNE SYSTEM Blood Types, Transplants, Allergies, Autoimmune diseases, Immunodeficiency Diseases Antigens on red blood cells determine whether a person has type A, B, AB, or O blood
CPT Codes: The following ICD-10-CM codes support the medical necessity of CPT code 82306:
 CPT s: 82306 Vitamin D; 25 hydroxy, includes fraction(s), if performed 82652 Vitamin D; 1, 25 dihydroxy, includes fraction(s), if performed The following ICD-10-CM codes support the medical necessity of
CPT s: 82306 Vitamin D; 25 hydroxy, includes fraction(s), if performed 82652 Vitamin D; 1, 25 dihydroxy, includes fraction(s), if performed The following ICD-10-CM codes support the medical necessity of
A Case of Monogenic Immune Deficiency and Autoimmunity. The Canberra Hospital Immunology Department Dr Phillippa Pucar - Immunology Registrar
 A Case of Monogenic Immune Deficiency and Autoimmunity The Canberra Hospital Immunology Department Dr Phillippa Pucar - Immunology Registrar Initial Presentation A 40 year old F was referred for investigation
A Case of Monogenic Immune Deficiency and Autoimmunity The Canberra Hospital Immunology Department Dr Phillippa Pucar - Immunology Registrar Initial Presentation A 40 year old F was referred for investigation
Immunological disturbances in Good s syndrome
 CLINICAL REPORT Immunological disturbances in Good s syndrome Justyna Fijolek * MD PhD Elzbieta Wiatr * Urszula Demkow ** Tadeusz Maria Orlowski * * Institute of Tuberculosis and Lung Diseases Warsaw Poland.
CLINICAL REPORT Immunological disturbances in Good s syndrome Justyna Fijolek * MD PhD Elzbieta Wiatr * Urszula Demkow ** Tadeusz Maria Orlowski * * Institute of Tuberculosis and Lung Diseases Warsaw Poland.
Elements for a Public Summary
 VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Nanogam is intended to be used for the treatment of diseases in patients who are suffering from a shortage of immunoglobulins
VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Nanogam is intended to be used for the treatment of diseases in patients who are suffering from a shortage of immunoglobulins
Study Events 2. Consent Information 3. Family History 5. Registry Visit 8. Visit Information 11. Vitals / Measures 13. Clinical History 15
 Study Events 2 Consent Information 3 Family History 5 Registry Visit 8 Visit Information 11 Vitals / Measures 13 Clinical History 15 Immunizations, Infusions, Transfusions 31 Medications & Supplements
Study Events 2 Consent Information 3 Family History 5 Registry Visit 8 Visit Information 11 Vitals / Measures 13 Clinical History 15 Immunizations, Infusions, Transfusions 31 Medications & Supplements
Name of Primary Immune Deficiency: Patient/Applicant Name: Parent/Carer Name (if child under 16): Address: Phone: GP: Immunologist:
: Address: Phone: GP: Immunologist:") Name of Primary Immune Deficiency: Patient/Applicant Name: Parent/Carer Name (if child under 16): Address: Phone: GP: Immunologist: Date: To whom it may concern: A Primary Immune Deficiency (PI) is a genetic
Name of Primary Immune Deficiency: Patient/Applicant Name: Parent/Carer Name (if child under 16): Address: Phone: GP: Immunologist: Date: To whom it may concern: A Primary Immune Deficiency (PI) is a genetic
Approach to the Patient With Suspected Immunodeficiency
 Merck Manual Professional Version PROFESSIONAL VERSION Professional / Immunology; Allergic Disorders / Immunodeficiency Disorders Approach to the Patient With Suspected Immunodeficiency By James Fernandez,
Merck Manual Professional Version PROFESSIONAL VERSION Professional / Immunology; Allergic Disorders / Immunodeficiency Disorders Approach to the Patient With Suspected Immunodeficiency By James Fernandez,
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Immunodeficiency. Most are detected in infancy (6 months 2 years) >> because it s genetic not acquired
 >> because it s genetic not acquired") The sheet include slide in bold Immunodeficiency Mohammad Jomaa Primary immunodeficiency diseases The primary immunodeficiency is genetic disorder Innate or adaptive Most are detected in infancy (6 months
The sheet include slide in bold Immunodeficiency Mohammad Jomaa Primary immunodeficiency diseases The primary immunodeficiency is genetic disorder Innate or adaptive Most are detected in infancy (6 months
Understanding Diagnostic Tests for Immunodeficiency
 Understanding Diagnostic Tests for Immunodeficiency Manish J. Butte, M.D. Ph.D. Assistant Professor mjbutte@stanford.edu http://tcell.stanford.edu September 21, 2013 PEDIATRICS What are we testing for?
Understanding Diagnostic Tests for Immunodeficiency Manish J. Butte, M.D. Ph.D. Assistant Professor mjbutte@stanford.edu http://tcell.stanford.edu September 21, 2013 PEDIATRICS What are we testing for?
Subcutaneous ImmunoglobulinTherapy A New Way of Permanent Treatment in Primary Immunodeficiencies Gaby Strotmann
 Subcutaneous ImmunoglobulinTherapy A New Way of Permanent Treatment in Primary Immunodeficiencies Gaby Strotmann Immunodeficiency Department University Children s Hospital Dr. von Haunersches Kinderspital
Subcutaneous ImmunoglobulinTherapy A New Way of Permanent Treatment in Primary Immunodeficiencies Gaby Strotmann Immunodeficiency Department University Children s Hospital Dr. von Haunersches Kinderspital
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS
 QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016
 Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Primary Immunodeficiency Program at AUBMC (In collaboration with Children's Hospital in Boston and Four Regional Hospitals in the Middle East):
:") Primary Immunodeficiency Program at AUBMC (In collaboration with Children's Hospital in Boston and Four Regional Hospitals in the Middle East): Studies of Immunological Deficiency Syndromes Congenital
Primary Immunodeficiency Program at AUBMC (In collaboration with Children's Hospital in Boston and Four Regional Hospitals in the Middle East): Studies of Immunological Deficiency Syndromes Congenital
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
The broad spectrum of lung diseases in primary antibody deficiencies
 REVIEW PRIMARY ANTIBODY DEFICIENCIES The broad spectrum of lung diseases in primary antibody deficiencies Francesco Cinetto 1,2, Riccardo Scarpa 1,2, Marcello Rattazzi 1,2 and Carlo Agostini 1,2 Affiliations:
REVIEW PRIMARY ANTIBODY DEFICIENCIES The broad spectrum of lung diseases in primary antibody deficiencies Francesco Cinetto 1,2, Riccardo Scarpa 1,2, Marcello Rattazzi 1,2 and Carlo Agostini 1,2 Affiliations:
Autoimmunity and autoinflammation
 Autoimmunity and autoinflammation Primary immunodeficiencies Autoimmunity and autoinflammation 1 Primary immunodeficiencies List of some common abbreviations APECED CAPS CGD CINCA CRMO CVID FCAS FMF HIDS
Autoimmunity and autoinflammation Primary immunodeficiencies Autoimmunity and autoinflammation 1 Primary immunodeficiencies List of some common abbreviations APECED CAPS CGD CINCA CRMO CVID FCAS FMF HIDS
ACCME/Disclosures 4/13/2016. Clinical History
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
Epstein-Barr Virus in a Toddler. Elaine Bullock, MD Pediatrics LSU Health Shreveport Louisiana Chapter AAP Pediatric Potpourri on the Bayou
 Epstein-Barr Virus in a Toddler Elaine Bullock, MD Pediatrics LSU Health Shreveport Louisiana Chapter AAP Pediatric Potpourri on the Bayou Disclosure Presenter: Elaine Bullock, MD I have nothing to disclose
Epstein-Barr Virus in a Toddler Elaine Bullock, MD Pediatrics LSU Health Shreveport Louisiana Chapter AAP Pediatric Potpourri on the Bayou Disclosure Presenter: Elaine Bullock, MD I have nothing to disclose
Common Variable Immune Deficiency & Granulomatous Lymphocytic Interstitial Lung Disease
 Common Variable Immune Deficiency & Granulomatous Lymphocytic Interstitial Lung Disease Evans Fernández, M.D., M.S. Associate Professor, Interstitial Lung Disease Program & Autoimmune Lung Center National
Common Variable Immune Deficiency & Granulomatous Lymphocytic Interstitial Lung Disease Evans Fernández, M.D., M.S. Associate Professor, Interstitial Lung Disease Program & Autoimmune Lung Center National
1 Immunodeficiencies. Wojciech Feleszko MD
 1 Immunodeficiencies Wojciech Feleszko MD 100 90 80 70 60 50 40 WHY TODAY? WHY WE? 2 30 Respiratory 20 10 0 Gastrointestinal CNS Urinary Tract Bones Skin 3 Immunodeficiencies Congenital/Primary genetic
1 Immunodeficiencies Wojciech Feleszko MD 100 90 80 70 60 50 40 WHY TODAY? WHY WE? 2 30 Respiratory 20 10 0 Gastrointestinal CNS Urinary Tract Bones Skin 3 Immunodeficiencies Congenital/Primary genetic
B cell activation and antibody production. Abul K. Abbas UCSF
 1 B cell activation and antibody production Abul K. Abbas UCSF 2 Lecture outline B cell activation; the role of helper T cells in antibody production Therapeutic targeting of B cells 3 Principles of humoral
1 B cell activation and antibody production Abul K. Abbas UCSF 2 Lecture outline B cell activation; the role of helper T cells in antibody production Therapeutic targeting of B cells 3 Principles of humoral
2. Clinical Manifestations (Pediatric HIV Infection)
") Page 1 of 6 HOUSTON ROMANIA SOUTHERN AFRICA MEXICO HOME CONTACT Friday, July 25, 2003 Pediatric HIV Infection by Mark W. Kline, M.D. 1. Introduction 2. Clinical Manifestations 3. Diagnosis 2. Clinical
Page 1 of 6 HOUSTON ROMANIA SOUTHERN AFRICA MEXICO HOME CONTACT Friday, July 25, 2003 Pediatric HIV Infection by Mark W. Kline, M.D. 1. Introduction 2. Clinical Manifestations 3. Diagnosis 2. Clinical
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Chapter 24 The Immune System
 Chapter 24 The Immune System The Immune System Layered defense system The skin and chemical barriers The innate and adaptive immune systems Immunity The body s ability to recognize and destroy specific
Chapter 24 The Immune System The Immune System Layered defense system The skin and chemical barriers The innate and adaptive immune systems Immunity The body s ability to recognize and destroy specific
An Intriguing Case of Meningitis. Tiffany Mylius MLS (ASCP)
") An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later