World Health Organization. Western Pacific Region
|
|
|
- Molly Gibbs
- 5 years ago
- Views:
Transcription
1 Standard modules for HBV 1
2 HBV Module 1 Hepatitis B serological markers and virology 2
3 Acute hepatitis HAV HBV HCV HDV HEV Case fatality Case fatality Uncommon increases with increases with age age Superinfection in HBV may lead to fulminant disease Higher case fatality in pregnant women Chronic No 5% (adults) 55 85% Very rare infection 90% (children) Complicates hepatitis B HCC* No Yes Yes No Route of transmission Waterborne Foodborne Person to person Main hepatitis viruses Perinatal Bloodborne Sexual Bloodborne Perinatal Sexual Bloodborne Waterborne Foodborne Vaccine Yes Yes No HBV vaccine No Treatment None options None Available Available Modified treatment of HBV *HCC; hepatocellular carcinoma 3
4 Populations at higher risk for hepatitis B and C HBV HCV Persons who injected drugs Sex workers Men who have sex with men Health care workers Persons in long term care facilities Persons on chronic dialysis treatment Prisoners and other persons in closed setting Persons who frequently receive blood/blood products Children born to mother infected with HBV / HCV 4 TECHNICAL CONSIDERATIONS AND CASE DEFINITIONS TO IMPROVE SURVEILLANCE FOR VIRAL HEPATITIS. (WHO 2016) P9
5 Who is at risk for chronic HBV infection? Age is a key factor in determining the risk of chronic hepatitis B infection 80 90% of infants infected during the first year of life 30 50% of children infected before the age of 6 years Less than 5% of otherwise healthy persons who are infected as adults 20 30% of adults who are chronically infected will develop cirrhosis and/or liver cancer. 5 WHO guideline 2015
6 Who is at risk for chronic HBV infection? 6 WHO guideline 2015
7 Who to test for chronic HBV and HCV infection There are several possible approaches to testing for HBV and HCV infection General population testing Focused or targeted testing of specific high risk groups Routine antenatal clinic (ANC) testing Birth cohort testing Blood donor screening 7 GUIDELINES ON HEPATITIS B AND C TESTING (WHO 2017) P38 39
8 Who to test for chronic HBV infection Testing approach and population General population testing Routine testing in pregnant women Focused testing in most affected populations Blood donors Recommendations In settings with a 2% or 5% HBsAg seroprevalence,all adults have routine access to and be offered HBsAg serological testing In settings with a 2% or 5% HBsAg seroprevalence, HBsAg serological testing be routinely offered to all pregnant women in antenatal clinics In all settings, HBsAg serological testing be offered to the following individuals Adults and adolescents from populations most affected by HBV infection Adults, adolescents and children with a clinical suspicion of chronic viral hepatitis Sexual partners, children and other family members, and close household contacts of those with HBV infection Health care workers In all settings, screening of blood donors should be mandatory 8 GUIDELINES ON HEPATITIS B AND C TESTING (WHO 2017) P36
9 Initial assessment for chronic hepatitis B and C HBV HCV Chronic infection HBsAg Anti HCV Acute infection Anti HBc IgM HCV RNA, HCcAg etc. (without anti HCV antibody, excluding other hepatitis viruses) 9
10 Additional assessment for chronic hepatitis Serological markers Severity Staging HBV Anti HBs/anti HBc antibodies HBe antigen, Anti HBe, HBV DNA HCV HCV RNA HCV genotype Aminotransferase (AST/ALT) Bilirubin, albumin, alkaline phosphatase (ALP) Liver biopsy Non invasive tests APRI, FIB 4, FibroTest, Transietn elastography 10
11 Serological pattern of chronic HBV infection 11 GUIDELINES ON HEPATITIS B AND C TESTING (WHO 2017) P22

 12 GUIDELINES ON HEPATITIS B AND C")
12 How to test for chronic HBV infection (A) Single assay (HBs seroprevalence 0.4%) (B) Two assays (HBs seroprevalence <0.4%) 12 GUIDELINES ON HEPATITIS B AND C TESTING (WHO 2017) P53
13 HBV Module 2 Hepatitis B transmission and prevention 13
14 Transmission routes of HBV Vertical: Mother to child Horizontal: Young children, household contacts Sexual Health care associated Blood products Unsafe injections Medical procedure (i.e. Needle stick injury) Persons who inject drugs (PWID) Organs and tissue transplantation 14
15 HBV infection and age at acquisition Infections during infancy and early childhood are particularly likely to lead to chronic infection, with risk of cirrhosis and death (a public health problem) 15
16 Prevention of HBV infection Vaccination* Childhood vaccination Primary 3-dose vaccination Timely birth dose High risk groups Catch up programs * Is the key intervention to prevent chronic HBV infection (occurs following infection during infancy and childhood) Other measures Screening of blood and blood products Injection safety Occupational safety Harm reduction interventions Safe sex 16
17 Infant and neonatal hepatitis B vaccination Vaccination is the mainstay of Hepatitis B prevention Infant and neonatal hepatitis B vaccination The hepatitis B vaccination is the mainstay of hepatitis B prevention WHO recommends birth dose (BD) and 3rd dose (B3) of hepatitis B vaccination The complete vaccine series induces protective antibody levels in >95% of infants and children. 17
18 Hepatitis B vaccine Contains a viral protein: HBsAg = Hepatitis B surface antigen Originally produced from plasma of persons with chronic HBV infection, but now only recombinant protein is used Recombinant vaccine Gene for HBsAg is inserted into yeast or mammalian cells The cells are cultured to produce an excess of protein The protein is purified and adsorbed on the surface of an adjuvant (alum) Used as intramuscular injection 18
19 Hepatitis B vaccines Storage at 2 8 C Stability and storage Relatively heat stable remains effective even after several days at room temperature However, very sensitive to freezing Avoid freezing at all costs 19
20 Protection* in Infants by HBV Vaccination Dose Dose Protection 1 16% 40% 2 80% 95% 3 98% 100% * Protection defined as anti HBs antibody titer of 10 miu/ml or higher Note: Preterm infants less than 2 kg respond to vaccination less often 20
21 Hepatitis B vaccine response rates A 3 dose series induces protective antibody concentrations in >95% of healthy infants, children and young adults (<40 years) Lower response rates in older adults (>40 years), obesity, smoking, chronic systemic illnesses Seroprotection rates following vaccination in older persons years >90% years >80% 21
22 Vaccine non responders 5 10% people may not respond to 3 dose schedule Most of the non responders do respond to an additional 3 dose vaccination series Alternative options for non responders Double dose Four dose schedule Intradermal administration Newer vaccines 22
23 Global health sector strategy on hepatitis Targets Interventions 2020 target 2030 target 1. Hep B3 vaccine 90% 90% 2. HBV PMTCT 50% 90% 1. Service coverage 2. Impact 3. Blood and injection safety 95 % screened donations 100 % screened donations 50% RUP devices 90% RUP devices 4. Harm reduction 200 injection sets / PWID 300 injection sets / PWID 5. Treatment A. Incidence 30% diagnosed 90% diagnosed 5M and 3M treated for HBV and HCV 30% (1% HBsAg in children ) 80% eligible treated 90% (0.1% HBsAg in children) B. Mortality 10% 65% 23 PMTCT: Prevention of mother to child transmission PWID: Person who injects drugs
24 Immunization coverage with 3 dose schedule of hepatitis B vaccine in infants in 2015 Coverage (%) African American Eastern Mediterranean European South East Asia Western Pacific Global Year Source: WHO AND UNICEF Joint Reporting
25 Immunization Coverage Coverage (%) African American Western Pacific Global Year 25 Source: WHO AND UNICEF Joint Reporting
26 Regional vaccination coverage Hepatitis B vaccine 3rd dose Hepatitis B vaccine birth dose Chronic infections 26 Eric Wiesen et al,vaccine 2016 WPRO
27 Catch up hepatitis B vaccination strategies All children and adolescents younger than 18 yearsold and not previously vaccinated should receive the vaccine if they live in countries where there is low or intermediate endemicity. Higher dose of vaccination might improve the lower response in persons with HIV or with a low CD4 count. Safer sex practices also protect against transmission including minimizing the number of partners and using barrier protective measures. 27
28 HBV Module 3 Natural history of Hepatitis B 28
29 Consequences of HBV infection Hepatitis B virus infection Acute infection (short duration: <6 mo) Chronic infection (duration >6 mo) Asymptomatic Chronic hepatitis B Acute viral hepatitis Cirrhosis: compensated Acute liver failure Cirrhosis: decompensated 29
30 Natural history of HBV infection (Acute phase) Acute HBV infection HBsAg (+) IgM anti HBc (+) HBV DNA(+), HBeAg(+/ ), Anti HBs( ) *: IgM anti HBc(+) can distinguish acute infection from chronic infection 95% in adults 5 30% in children Infection resolved HBsAg ( ), Anti HBs (+) IgM anti HBc( ), Anti HBc (+), HBV DNA( ), HBeAg( ) 3 5% (10% in Gt. A) in adults 70 95% in children Infection persistent HBsAg (+), Anti HBs ( ) IgM anti HBc( ), Anti HBc(+) HBV DNA(+), HBeAg(+/ ) Rare, but to take care Fulminant hepatitis *: Anti HBs (+) can distinguish resolved state from chronic infection next slide % Death 30

31 Serological pattern of acute HBV infection 31 GUIDELINES ON HEPATITIS B AND C TESTING (WHO 2017) P22
32 Natural history of HBV infection (chronic phase) Infection persistent HBe(+) chronic hepatitis HBsAg (+), Anti HBc (+) HBeAg (+), HBV DNA high ALT high HBe( ) chronic hepatitis HBsAg (+), Anti HBc (+) HBeAg ( ), HBV DNA low( high) ALT normal high Liver cirrhosis Liver failure Liver cancer Death Inactive carrier HBsAg (+), Anti HBc (+) HBeAg ( ), HBV DNA ( ) low ALT normal Clinical clearance HBsAg ( ), Anti HBs ( ) Anti HBc (+), HBV DNA ( ) ALT normal 32
33 Natural history of chronic hepatitis B Chronic hepatitis B Immunetolerant phase Immune active phase Immune control phase Immune clearance (cure) Reactivation phase 33
34 Natural history of chronic hepatitis B Chronic hepatitis B Immunetolerant phase Immune active phase Immune control phase Immune clearance (cure) Cirrhosis with any of the phases Phases that need anti viral drug treatment Phases that DO NOT need anti viral drug treatment Reactivation phase 34
35 Natural history of HBV infection (chronic phase) Infection persistent HBe(+) chronic hepatitis HBsAg (+), Anti HBc (+) HBeAg (+), HBV DNA high ALT high HBe( ) chronic hepatitis HBsAg (+), Anti HBc (+) HBeAg ( ), HBV DNA low( high) ALT normal high Liver cirrhosis Liver failure Liver cancer Death Inactive carrier HBsAg (+), Anti HBc (+) HBeAg ( ), HBV DNA ( ) low ALT normal Clinical clearance HBsAg ( ), Anti HBs ( ) Anti HBc (+), HBV DNA ( ) ALT normal 35
")
36 Serological pattern of chronic HBV infection 36 GUIDELINES ON HEPATITIS B AND C TESTING (WHO 2017) P22
37 Atypical clinical course of HBV infection HBeAg negative chronic hepatitis Seroconversion commonly means HBV replication Mutations in pre core or core promotor region Rapid progression to cirrhosis HBV reactivation in immuno deficient state De novo hepatitis Hematopoietic stem cell transplant, rituximab, Chronicity rate in new adults infection Difference in geographical distribution and chronicity 37
38 HBV Module 4 Assessment of liver fibrosis 38

39 Assessing the degree of liver fibrosis Non invasive tests Components Requirements Cost APRI AST, platelets Simple serum and FIB 4 Age, AST, ALT, Platelets hematology test FibroTest ggt, haptoglobin, bilirubin, A1apoprotein, α2 macroglobulin AST; aspartate aminotransferase ALT; alanine aminotransferase APRI; aspartate aminotransferase to platelet ratio index FIB 4; fibrosis 4 score Specialized tests at designed laboratories Fibroscan Transient elastography Dedicated equipment +++ Fibroscan (http.myliverexam.com/en/lexamen fibroscan.html) GUIDELINES FOR THE PREVENTION, CARE AND TREATMENT OF PERSONS WITH CHRONIC HEPATITIS B INFECTION (WHO 2015)
40 Assessing the degree of liver fibrosis by NITs Fibrosis stages assessed Cut off values for the detection of fibrosis Cirrhosis (METAVIR F4) Significant fibrosis (METAVIR F2) APRI F2, F4 High cut off 2.0 High cut off 1.5 FIB 4 F3 High cut off 3.25 FibroTest F2, F3, F Fibroscan F2, F3, F4 >11 14 kpa >7 8.5 kpa APRI = [ (AST(IU/L)/ AST_ULN(IU/L)) x 100 ] / platelet count (10 9 /L) ULN signifies the upper limit of normal for AST in the laboratory where these investigations were undertaken FIB 4 = age(yr) x AST(IU/L)/platelet count(10 9 /L) x [ALT(IU/L) 1/2 ] 40 GUIDELINES FOR THE PREVENTION, CARE AND TREATMENT OF PERSONS WITH CHRONIC HEPATITIS B INFECTION (WHO 2015)
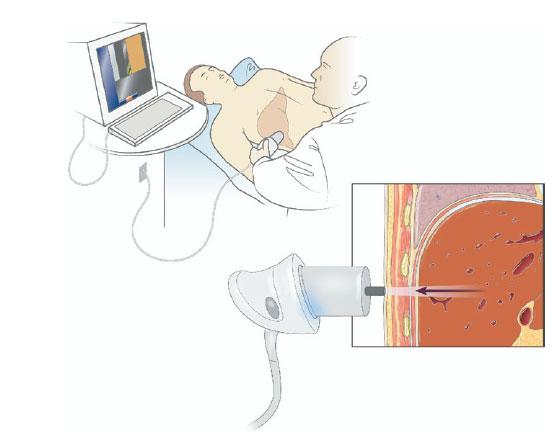

41 Transient elastography (Fibroscan) 41


42 Transient elastography (Fibroscan) Transducer sends a mechanical shearwave Monitor display of Fibroscan Large explored volume (at least 100 times more than biopsy) 42
43 Transient elastography (Fibroscan) Median Calculated from 10 valid measurement Is used as the final result Inter quartile range (IQR) Spread of the middle half of observations Should be small IQR/median Ratio of IQR to median Indicates variability in different reading High values means large variation If > 30%, implies no reliability 43
44 Fibroscan Advantages Easy, non invasive Can be done in outpatient or community settings Takes <10 minutes to perform Health care staff can be easily trained Limiting factors High cost of equipment Equipment needs regular maintenance/calibration by trained personnel No universal cut off values for specific stages of fibrosis Difficult to measure in very obese 44
45 The Child Turcotte Pugh Classification system Points Encephalopathy None Minimal (grade1 or 2) Advanced (grade 3 or 4) Ascites Absent Controlled Refractory Total bilirubin <34 (<2) (2 3) >51 (>3) (μmol/l)(mg/dl) Albumin(g/dL) > <2.8 Prothrombin time (seconds) or PT INR* Child Pugh Class A: 5 6 points Child Pugh Class B: 7 9 points Child Pugh Class C: points <4 or < or >6 or >2.3 *PT INR ; prothrombin time international normalized ratio 45
46 HBV Module 5 Treatment for Chronic Hepatitis B 46
47 WHO guidelines Assessment for treatment Monitoring Stopping treatment 47
48 Initial assessment for hepatitis B and C HBV HCV Chronic infection HBsAg Anti HCV Acute infection Anti HBc IgM HCV RNA, HCcAg etc. (without anti HCV antibody, excluding other hepatitis viruses) 48 MONITORING AND EVALUATION FOR VIRAL HEPATITIS B AND C: RECOMMENDED INDICATORS AND FRAMEWORK (WHO 2016)
49 Additional assessment for chronic hepatitis Serological markers Severity Staging HBV Anti HBs/anti HBc antibodies HBe antigen, Anti HBe, HBV DNA HCV HCV RNA Aminotransferase (AST/ALT) Bilirubin, albumin, alkaline phosphatase (ALP) Liver biopsy Non invasive tests APRI, FIB 4, FibroTest, Transietn elastography 49 GUIDELINES FOR THE PREVENTION, CARE AND TREATMENT OF PERSONS WITH CHRONIC HEPATITIS B INFECTION (WHO 2015) P17 19
50 Why should we treat HBV infection Delay the progression of cirrhosis (Improve liver fibrosis) Reduce the incidence of hepatocellular carcinoma Improve long term survival and QOL Key outcomes Sustained ALT normalization Sustained undetectable HBV DNA HBeAg seroconversion / HBsAg seroconversion Reversion of fibrosis stage 50 GUIDELINES FOR THE PREVENTION, CARE AND TREATMENT OF PERSONS WITH CHRONIC HEPATITIS B INFECTION (WHO 2015)
51 Clinical management of HBV infection 1. Natural history of HBV infection 2. Clinical assessment of persons with chronic hepatitis B 3. Why to treat for HBV 4. Who to treat for HBV 5. How to treat for HBV 6. How to monitor during treatment for HBV 7. When to stop treatment for HBV 51
52 Which patients should we treat for HBV HBV Cirrhosis High risk of disease progression to cirrhosis and hepatocellular carcinoma, such as Older than 30 years Persistently abnormal ALT levels High level HBV replication HCV All patients Optimal timing of treatment for HBV is still debated. 52 GUIDELINES FOR THE PREVENTION, CARE AND TREATMENT OF PERSONS WITH CHRONIC HEPATITIS B INFECTION (WHO 2015) P36 37
53 Summary of WHO Recommendation HBsAg CIRRHOSIS ALT HBV DNA Cirrhotic patients or APRI >2 Treatment Recommended >20,000 Treatment Recommended Persistently elevated 2,000 20,000 Treatment Deferred Non cirrhotic patients aged >30 <2,000 Treatment Deferred HBsAg+ Fluctuating Normal (<19 F, <30 M) Treatment Deferred Treatment Deferred Populaiton Non cirrhotic patients aged <30 Treatment Deferred HBsAg No Treatment Required 53
54 Clinical management of HBV infection 1. Natural history of HBV infection 2. Clinical assessment of persons with chronic hepatitis B 3. Why to treat for HBV 4. Who to treat for HBV 5. How to treat for HBV 6. How to monitor during treatment for HBV 7. When to stop treatment for HBV 54
55 How to treat HBV infection Antiviral agents Interferon (IFN), Pegylated (PEG) IFN Nucleos(t)ide analogue (NA) Tenofovir, Entecavir Lifelong treatment is generally required Clearance of HBsAg (=Cure) is rare High rate recurrence in treatment discontinuation Optimal timing of discontinuation remains unclear Patient s motivation is essential 55 GUIDELINES FOR THE PREVENTION, CARE AND TREATMENT OF PERSONS WITH CHRONIC HEPATITIS B INFECTION (WHO 2015)
56 Antiviral agents for HBV Antiviral agent Potency against HBV Resistance barrier Antivity against HIV Cost Interferons Moderate Not applicable Moderate High Tenofovir High High High Low (high in Hong Kong and other Asian countries) Entecavir High High Weak High Emtricitabine Moderate Low High Low Telbivudine High Low Unclear High Lamivudine Moderate high Low High Low Adefovir Low Moderate None (at 10mg dose) High 56 GUIDELINES FOR THE PREVENTION, CARE AND TREATMENT OF PERSONS WITH CHRONIC HEPATITIS B INFECTION (WHO 2015) P21
57 WHO recommendation: choice of drug In all adults, adolescents and children aged 12 years or older in whom antiviral therapy is indicated, the nucleos(t)ide analogues which have a high barrier to drug resistance (tenofovir or entecavir) are recommended. Entecavir is recommended in children 57 GUIDELINES FOR THE PREVENTION, CARE AND TREATMENT OF PERSONS WITH CHRONIC HEPATITIS B INFECTION (WHO 2015)

58 Drug dose Adults Entecavir 0.5 mg/day oral Tenofovir 300 mg/day oral Children need dose modification 58

59 Drugs need dose adjustment in renal disease 59
60 Duration of treatment Cirrhosis or APRI >2.0 Lifelong treatment Discontinuation may be considered exceptionally in those without cirrhosis (or APRI < 2.0 in adults) and all of the following: Can be followed carefully long term for reactivation If HBeAg loss and seroconversion to anti HBe, and maintained for one year Persistently normal ALT Persistently undetectable HBV DNA 60
61 HBV Module 6 Monitoring for Chronic Hepatitis B 61
")
62 Need for monitoring HBsAg +ve No treatment Defer treatment Start treatment All need monitoring (irrespective of need for treatment) 62
63 Who should we monitor and why All patients with chronic HBV and HCV infection More frequent monitoring is recommended for: Persons who do not yet meet the criteria for treatment Persons on treatment or following treatment cessation Monitoring is essential to confirm Adherence, toxicities Treatment effect ALT, HBsAg, HBeAg, HBV DNA Hepatocellular carcinoma Ultrasound and AFP testing 63 GUIDELINES FOR THE PREVENTION, CARE AND TREATMENT OF PERSONS WITH CHRONIC HEPATITIS B INFECTION (WHO 2015) P64
64 How to monitor? 64
65 How to monitor? At least annually: ALT HBsAg, HBeAg, HBV DNA level APRI Adherence to treatment Drug adverse events (renal function) More frequent In those who do not clearly meet criteria for treatment Following treatment discontinuation Surveillance for hepatocellular cancer 65
66 How to monitor HBV infected patients : every 12 mos Disease progression / treatment response : every 12 months Monitoring for treatment toxicities Adherence Renal function Ultrasound : every 6 months Detection of liver cancer (cirrhosis / family history) ALT, HBV DNA, HBeAg Risk factors for renal dysfunction α fetoprotein Non invasive test Baseline 6month 12month 18month 24month 66
67 Clinical management of HCV infection 1. Natural history of HBV infection 2. Clinical assessment of persons with chronic hepatitis B 3. Why to treat for HBV 4. Who to treat for HBV 5. How to treat for HBV 6. How to monitor during treatment for HBV 7. When to stop treatment for HBV 67
68 When to stop treatment of HBV Possible discontinuation (Persons without cirrhosis) who can be followed carefully long term for reactivation HBeAg seroconversion to anti HBe and after completion of at least one additional year of treatment in association with persistently normal ALT levels persistently undetectable HBV DNA levels Retreatment is recommended if there are consistent sign of reactivation (HBsAg / HBeAg becomes positive, ALT levels increase, or HBV DNA becomes detectable again) 68 GUIDELINES FOR THE PREVENTION, CARE AND TREATMENT OF PERSONS WITH CHRONIC HEPATITIS B INFECTION (WHO 2015) P64
69 HBV Practical session case based learning 69
70 A 52 year old male presents with malaise History: no previous hospitalization Social: 120g alcohol/day (30 years), no tobacco, no records of substance abuse Examination: unremarkable Laboratory data: AST 78 U/L (ULN 30), ALT 64 U/L HBsAg positive, Anti HCV negative Clinical Question What test do you order? Case study 1 70
71 What test do you order? HBV DNA 2.8 x10 8 IU/mL, HIV rapid diagnostic test negative Hb 11.8 g/dl, Neutrophil 2.5 x10 9 /L, PLT 98 x10 9 /L Alb 3.4 g/dl, T Bil 1.2 mg/dl, PT INR 1.6 Cre 1.0 mg/dl Ultrasound: chronic liver disease, mild splenomegaly Clinical Question What is the stage of liver disease? Is treatment recommended? Case study 1 What monitoring do you require? 71
72 What is the stage of liver disease? APRI 2.6; [78/30]x100/98 > 2.0; Liver cirrhosis (compensated) Is treatment recommended? Diagnosis: Liver cirrhosis B Select recommended preferred regimen: Tenofovir 300mg once daily or Entecavir 0.5mg once daily Lifelong treatment Case study 1 Assist for treatment: reduce alcohol intake What monitoring do you require? Monitor for efficacy and toxicity (baseline and every 12 months) Long life screening for HCC (every 6 months) 72
73 A 28 year old female presents for a health check up Complaints: not any symptoms History: no previous hospitalization Social: no records of alcohol, tobacco and substance Examination: unremarkable Laboratory data: She has found to be 24 weeks of gestation HBsAg positive, Anti HCV negative, HIV RDT negative Clinical Question What test do you order? Case study 2 73
74 What test do you order? HBV DNA 1.7 x10 8 IU/mL Hb 9.8 g/dl, Neutrophil 2.8 x10 9 /L, PLT 188 x10 9 /L AST 58 U/L (ULN 30), ALT 62 U/L Alb 4.0 g/dl, T Bil 0.9 mg/dl, PT INR 1.4 Cre 0.8 mg/dl, normal urine Ultrasound: normal liver, no ascites, no hepatoma Clinical Question What is the stage of liver disease? Is treatment recommended? Case study 2 74
75 What is the stage of liver disease? APRI 1.0; [58/30]x100/188 < 2.0; not liver cirrhosis Is treatment recommended? Diagnosis: chronic hepatitis B, 24 weeks of gestation Infant and neonatal hepatitis B vaccination: All infants should receive their first dose of hepatitis B vaccine as soon as possible after birth, preferably 24 hours, followed by two or three doses. Prevention of mother to child HBV transmission no recommendation Breast feeding is safe. Case study 2 75
76 A 45 year old female presents with insomnia History: no previous hospitalization Social: no records of alcohol, tobacco and substance Examination: unremarkable Laboratory data: Hb 12.6 g/dl, AST 34 U/L (ULN 30), ALT 40 U/L HBsAg positive, Anti HCV negative Clinical Question What test do you order? Case study 3 76
77 What test do you order? HBV DNA 1.2 x10 8 IU/mL Neutrophil 3.0 x10 9 /L, PLT 218 x10 9 /L Alb 4.0 g/dl, T Bil 0.8 mg/dl, PT INR 1.5 Cre 0.8 mg/dl Ultrasound: normal liver, no ascites, no hepatoma Clinical Question Case study 3 What is the stage of liver disease? Is treatment recommended? What monitoring do you require? 77
78 What is the stage of liver disease? APRI 0.5; [34/30]x100/218 < 2.0; not liver cirrhosis Is treatment recommended? Diagnosis: Chronic hepatitis B Select recommended preferred regimen: Tenofovir 300mg once daily or Entecavir 0.5mg once daily Lifelong treatment Case study 3 What monitoring do you require? Monitor for efficacy and toxicity (baseline and every 12 month) 78
79 A 26 year old male presents with low grade fever History: no previous hospitalization Social: 60g alcohol/day (6 years), there are records of substance abuse, Sexually active with several partners Examination: injection scar of arm Laboratory data: Hb 13.0 g/dl, Neutrophil 2.8 x10 9 /L, PLT 282 x10 9 /L AST 112 U/L (ULN 30), ALT 120 U/L, HBsAg positive Clinical Question What test do you order? Case study 4 79
80 What test do you order? HBV DNA 3.5 x10 8 IU/mL Alb 4.1 g/dl, T Bil 1.0 mg/dl, PT INR 1.4 Cre 0.8 mg/dl Anti HCV negative, HIV RDT negative Ultrasound: normal liver, no ascites, no hepatoma Clinical Question What is the stage of liver disease? Is treatment recommended? Case study 4 What monitoring do you require? 80
81 What is the stage of liver disease? APRI 1.3; [112/30]x100/282 < 2.0; not liver cirrhosis Is treatment recommended? Diagnosis: chronic hepatitis B Select recommended preferred regimen: Tenofovir 300mg once daily or Entecavir 0.5mg once daily Lifelong treatment Case study 4 Assist for treatment: alcohol sobriety, drug abstinence What monitoring do you require? Monitor for efficacy and toxicity (baseline and every 12 month) 81
82 Case study 5 52 year old man Planned for laparoscopic cholecystectomy Detected to have HBsAg positive on evaluation History No previous hospitalization No addiction Examination: unremarkable What tests should one order? 82
83 Case study 5: Test results Investigations Values Hemoglobin (g/dl) 11.8 Platelets (x 10 9 /L) 98 Total bilirubin (mg/dl) 1.2 Albumin (g/dl) 3.4 ALT (IU/L) AST (IU/L) 66 (<40 IU/L) 98 (<40 IU/L) Prothrombin time (INR) 1.6 HBV DNA (IU/L) 1,120 USG abdomen Coarse echo texture of liver Portal vein diameter = 14 mm Splenomegaly, no ascites 83
84 Case study 5: Issues in management What is the stage of liver disease? Cirrhosis versus no cirrhosis Compensated versus decompensated Is treatment recommended? What drug? How long? How would you monitor the person during treatment? 84
85 Case study 5: Questions What is the stage of liver disease? Is treatment recommended? What is the treatment? What is the monitoring required? 85
86 Case study 5: Questions What is the stage of liver disease? APRI = [98/40] x 100/98 = ~2.5 APRI > 2.0 Liver cirrhosis (compensated) Is treatment recommended? What is the treatment? What is the monitoring required? 86
87 Case study 5: Questions What is the stage of liver disease? APRI = [98/40] x 100/98 = ~2.5 APRI > 2.0 Liver cirrhosis (compensated) Is treatment recommended? HBV DNA is detectable: Those with cirrhosis need treatment (irrespective of DNA level) What is the treatment? What is the monitoring required? 87
88 Case study 5: Questions What is the stage of liver disease? APRI = [98/40] x 100/98 = ~2.5 APRI > 2.0 Liver cirrhosis (compensated) Is treatment recommended? HBV DNA is detectable: Those with cirrhosis need treatment (irrespective of DNA level) What is the treatment? Entecavir 0.5 mg, once daily, oral, life-long What is the monitoring required? 88
89 Case study 5: Questions What is the stage of liver disease? APRI = [98/40] x 100/98 = ~2.5 APRI > 2.0 Liver cirrhosis (compensated) Is treatment recommended? HBV DNA is detectable: Those with cirrhosis need treatment (irrespective of DNA level) What is the treatment? Entecavir 0.5 mg, once daily, oral, life-long What is the monitoring required? 89 Monitor for efficacy, decompensation and liver cancer Lifelong
90 Case study 5: Take home messages Cirrhosis must be looked for in all HBsAg positive patients In patients with cirrhosis and detectable HBV DNA Antiviral drugs should be started (regardless of HBV DNA level) Serum ALT level has no role in deciding the need for treatment In patients with cirrhosis, antiviral treatment 90 Should be continued for life Entecavir is preferred over tenofovir (the latter has renal toxicity) Usual dose of entecavir is 0.5 mg/d even in compensated cirrhosis, but is 1.0 mg/d in decompensated cirrhosis
91 Case study 6 25 y old woman Detected HBsAg positive during blood donation screening Asymptomatic, good health No previous hospitalization, no morbidity, no addiction Examination: unremarkable What test should one order? 91
92 Case study 6: Test results Investigations Values Hemoglobin (g/dl) 12.8 Platelets (x 10 9 /L) 218 Total bilirubin (mg/dl) 0.8 Albumin (g/dl) 4.0 ALT (IU/L) AST (IU/L) 34 (<40 IU/L) 28 (<40 IU/L) Prothrombin time (INR) 1.1 HBV DNA (copies/ml) 8000 USG abdomen Normal liver size and echotexture Portal vein diameter = 10 mm Normal spleen; no ascites 92
93 Case study 6: Questions What is the stage of liver disease? Is treatment recommended? What is the treatment? What is the monitoring required? 93
94 Case study 6: Questions What is the stage of liver disease? APRI = [28/30] x 100/218 = ~0.4 APRI < 2.0 No cirrhosis Is treatment recommended? What is the treatment? What is the monitoring required? 94
95 Case study 6: Questions What is the stage of liver disease? APRI = [28/30] x 100/218 = ~0.4 APRI < 2.0 No cirrhosis Is treatment recommended? ALT normal HBV DNA = 8000 copies/ml = ~ 8000/5 or 1600 IU/mL What is the treatment? What is the monitoring required? 95
96 Case study 6: Questions What is the stage of liver disease? APRI = [28/30] x 100/218 = ~0.4 APRI < 2.0 No cirrhosis Is treatment recommended? ALT normal HBV DNA = 8000 copies/ml = ~ 8000/5 or 1600 IU/mL What is the treatment? No treatment (immune control phase) What is the monitoring required? 96
97 Case study 6: Questions What is the stage of liver disease? APRI = [28/30] x 100/218 = ~0.4 APRI < 2.0 No cirrhosis Is treatment recommended? ALT normal HBV DNA = 8000 copies/ml = ~ 8000/5 or 1600 IU/mL What is the treatment? No treatment (immune control phase) What is the monitoring required? Monitor for disease activity and liver cancer 97
98 Case study 6: Take home messages In young patients without cirrhosis: No need for treatment, unless ALT as well as HBV DNA are high However, all patients need periodic monitoring or disease activity and for HCC HBV DNA levels should be expressed as IU/mL (if reported as copies/ml, convert before interpretation) 98
99 Case study 7 38 y old woman Incidentally detected HBsAg positive during treatment for primary infertility No previous hospitalization, other disease or addiction Examination: normal What tests should one order? 99
100 Case study 7: Test results Investigations Values Hemoglobin (g/dl) 10.8 Platelets (x 10 9 /L) 255 Total bilirubin (mg/dl) 1.2 Albumin (g/dl) 3.8 ALT (IU/L) AST (IU/L) 76 (<40 IU/L) 56 (<40 IU/L) Prothrombin time (INR) 1.2 HBV DNA (IU/ml) 123,000 USG abdomen Normal liver size and echotexture Portal vein diameter = 10 mm Normal spleen; no ascites 100
101 What test would you order? Case study Investigations Values Hemoglobin 10.8 g/dl Platelets 255 x 10 9/L Total bilirubin 1.2 mg/dl Albumin 3.8 g/dl ALT AST 76 IU/L (<30 IU/L) 56 Prothrombin time INR 1.2 HBV DNA quantitative 123,000 IU/mL USG abdomen Normal size liver Portal vein diameter 10 mm No splenomegaly or ascites
102 Case study 7: Questions What is the stage of liver disease? Is treatment recommended? What is the treatment? What is the monitoring required? 102
103 Case study 7: Questions What is the stage of liver disease? APRI = [56/40] x 100/255 = ~0.6 APRI < 0.6 No cirrhosis Is treatment recommended? What is the treatment? What is the monitoring required? 103
104 Case study 7: Questions What is the stage of liver disease? APRI = [56/40] x 100/255 = ~0.6 APRI < 0.6 No cirrhosis Is treatment recommended? ALT high HBV DNA = 123,000 IU/mL (>20,000 IU/mL) What is the treatment? What is the monitoring required? 104
105 Case study 7: Questions What is the stage of liver disease? APRI = [56/40] x 100/255 = ~0.6 APRI < 0.6 No cirrhosis Is treatment recommended? ALT high HBV DNA = 123,000 IU/mL (>20,000 IU/mL) What is the treatment? Tenofovir, 300 mg, once daily, oral What is the monitoring required? 105
106 Case study 7: Questions What is the stage of liver disease? APRI = [56/40] x 100/255 = ~0.6 APRI < 0.6 No cirrhosis Is treatment recommended? ALT high HBV DNA = 123,000 IU/mL (>20,000 IU/mL) What is the treatment? Tenofovir, 300 mg, once daily, oral What is the monitoring required? Monitor for response, drug toxicity and liver cancer 106
107 Take home messages: Case study 7 Patients with HBV infection, who have high ALT and high HBV DNA need treatment with antiviral drugs In absence of cirrhosis, either tenofovir or entecavir may be used, tenofovir is the preferred drug Such patients need periodic monitoring for drug response, toxicity and HCC 107
Module 1 Introduction of hepatitis
 Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
World Health Organization. Western Pacific Region
 Advanced modules for HBV 1 HBV Module 1 Hepatitis B serological markers and virology 2 Acute hepatitis HAV HBV HCV HDV HEV Case fatality Case fatality Uncommon increases with increases with age age Superinfection
Advanced modules for HBV 1 HBV Module 1 Hepatitis B serological markers and virology 2 Acute hepatitis HAV HBV HCV HDV HEV Case fatality Case fatality Uncommon increases with increases with age age Superinfection
Management of Chronic Hepatitis B in Asian Americans
 Management of Chronic Hepatitis B in Asian Americans Myron J Tong; UCLA, CA Calvin Q. Pan; Mount Sinai, NY Hie-Won Hann; Thomas Jefferson, PA Kris V. Kowdley; Virginia Mason, WA Steven Huy B Han; UCLA,
Management of Chronic Hepatitis B in Asian Americans Myron J Tong; UCLA, CA Calvin Q. Pan; Mount Sinai, NY Hie-Won Hann; Thomas Jefferson, PA Kris V. Kowdley; Virginia Mason, WA Steven Huy B Han; UCLA,
World Health Organization. Western Pacific Region
 Advanced modules for HCV 1 HCV Module 1 Hepatitis C serological markers and virology 2 HCV Markers 3 Test Anti HCV (Anti hepatitis C virus antibody) HCV RNA (quantitative or qualitative) (Nucleic acid
Advanced modules for HCV 1 HCV Module 1 Hepatitis C serological markers and virology 2 HCV Markers 3 Test Anti HCV (Anti hepatitis C virus antibody) HCV RNA (quantitative or qualitative) (Nucleic acid
Viral Hepatitis. Dr. Abdulwahhab S. Abdullah CABM, FICMS-G&H PROF. DR. SABEHA ALBAYATI CABM,FRCP
 Viral Hepatitis Dr. Abdulwahhab S. Abdullah CABM, FICMS-G&H PROF. DR. SABEHA ALBAYATI CABM,FRCP Viral hepatitis Viral hepatitis must be considered in any patient presenting with hepatitis on LFTs (high
Viral Hepatitis Dr. Abdulwahhab S. Abdullah CABM, FICMS-G&H PROF. DR. SABEHA ALBAYATI CABM,FRCP Viral hepatitis Viral hepatitis must be considered in any patient presenting with hepatitis on LFTs (high
Who to Treat? Consider biopsy Treat. > 2 ULN Treat Treat Treat Treat CIRRHOTIC PATIENTS Compensated Treat HBV DNA detectable treat
 Who to Treat? Parameter AASLD US Algorithm EASL APASL HBV DNA CRITERIA HBeAg+ >, IU/mL > 2, IU/mL > 2, IU/mL >, IU/mL HBeAg- > 2, IU/mL > 2, IU/mL > 2, IU/mL > 2, IU/mL ALT CRITERIA PNALT 1-2 ULN Monitor
Who to Treat? Parameter AASLD US Algorithm EASL APASL HBV DNA CRITERIA HBeAg+ >, IU/mL > 2, IU/mL > 2, IU/mL >, IU/mL HBeAg- > 2, IU/mL > 2, IU/mL > 2, IU/mL > 2, IU/mL ALT CRITERIA PNALT 1-2 ULN Monitor
Outline. Updates in the Clinical Management of Hepatitis B and C. Who should be screened for HBV? Chronic Hepatitis B 10/7/2018
 Outline Updates in the Clinical Management of Hepatitis B and C Jennifer C. Lai, MD, MBA Transplant Hepatologist Associate Professor of Medicine In Residence University of California, San Francisco Initial
Outline Updates in the Clinical Management of Hepatitis B and C Jennifer C. Lai, MD, MBA Transplant Hepatologist Associate Professor of Medicine In Residence University of California, San Francisco Initial
Toronto Declaration: Strategies to control and eliminate viral hepatitis globally. A call for coordinated action
 Toronto Declaration: Strategies to control and eliminate viral hepatitis globally A call for coordinated action Hepatitis B National Action Plan All countries should develop a national and/or regional
Toronto Declaration: Strategies to control and eliminate viral hepatitis globally A call for coordinated action Hepatitis B National Action Plan All countries should develop a national and/or regional
Chronic Hepatitis B Infection
 Chronic Hepatitis B Infection Mohssen Nassiri Toosi, MD Imam Khomeinin Hospital Tehran University of Medical Sciences Chronic Hepatitis B Infection Virus : HBs Ag Positive Host Liver Health Chronic Hepatitis
Chronic Hepatitis B Infection Mohssen Nassiri Toosi, MD Imam Khomeinin Hospital Tehran University of Medical Sciences Chronic Hepatitis B Infection Virus : HBs Ag Positive Host Liver Health Chronic Hepatitis
EAST LONDON INTEGRATED CARE
 CITY & HACKNEY ELIC EAST LONDON INTEGRATED CARE MANAGEMENT OF CHRONIC HEPATITIS B IN PRIMARY CARE Chronic Hepatitis B virus (HBV) is an important public health problem globally and a leading cause of liver
CITY & HACKNEY ELIC EAST LONDON INTEGRATED CARE MANAGEMENT OF CHRONIC HEPATITIS B IN PRIMARY CARE Chronic Hepatitis B virus (HBV) is an important public health problem globally and a leading cause of liver
World Health Organization. Western Pacific Region
 Basic modules for HCV 1 HCV Module 1 Hepatitis C serological markers and virology 2 HCV Markers 3 Test Anti HCV (Anti hepatitis C virus antibody) HCV RNA (quantitative or qualitative) (Nucleic acid test)
Basic modules for HCV 1 HCV Module 1 Hepatitis C serological markers and virology 2 HCV Markers 3 Test Anti HCV (Anti hepatitis C virus antibody) HCV RNA (quantitative or qualitative) (Nucleic acid test)
Viral Hepatitis. Dr Melissa Haines Gastroenterologist Waikato Hospital
 Viral Hepatitis Dr Melissa Haines Gastroenterologist Waikato Hospital Viral Hepatitis HAV HBV HCV HDV HEV Other viral: CMV, EBV, HSV Unknown Hepatitis A Hepatitis A Transmitted via the faecal-oral route
Viral Hepatitis Dr Melissa Haines Gastroenterologist Waikato Hospital Viral Hepatitis HAV HBV HCV HDV HEV Other viral: CMV, EBV, HSV Unknown Hepatitis A Hepatitis A Transmitted via the faecal-oral route
Clinical Case Maria Butí, MD, PhD
 Clinical Case Maria Butí, MD, PhD Liver Unit, Internal Medicine Department Vall d Hebron Hospital 1 Clinical Case 70 year-old male Smoker, no alcohol intake No risk factors Diabetes Mellitus treated with
Clinical Case Maria Butí, MD, PhD Liver Unit, Internal Medicine Department Vall d Hebron Hospital 1 Clinical Case 70 year-old male Smoker, no alcohol intake No risk factors Diabetes Mellitus treated with
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Hepatitis B (chronic): diagnosis and management of chronic hepatitis B in children, young
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Hepatitis B (chronic): diagnosis and management of chronic hepatitis B in children, young
March 29, :15 PM 1:15 PM San Diego, CA Convention Center Ballroom 20D
 March 29, 2017 12:15 PM 1:15 PM San Diego, CA Convention Center Ballroom 20D Provided by #IM2017 This lunch symposium is not part of the official Internal Medicine Meeting 2017 Education Program. #IM2017
March 29, 2017 12:15 PM 1:15 PM San Diego, CA Convention Center Ballroom 20D Provided by #IM2017 This lunch symposium is not part of the official Internal Medicine Meeting 2017 Education Program. #IM2017
Hepatitis B screening and surveillance in primary care
 Hepatitis B screening and surveillance in primary care Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures
Hepatitis B screening and surveillance in primary care Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures
Management of Hepatitis B - Information for primary care providers
 Management of Hepatitis B - Information for primary care providers July 2018 Chronic hepatitis B (CHB) is often a lifelong condition. Not everyone infected needs anti-viral therapy. This document outlines
Management of Hepatitis B - Information for primary care providers July 2018 Chronic hepatitis B (CHB) is often a lifelong condition. Not everyone infected needs anti-viral therapy. This document outlines
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Hepatitis B (chronic): diagnosis and management of chronic hepatitis B in children, young
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Hepatitis B (chronic): diagnosis and management of chronic hepatitis B in children, young
HBV in HIV Forgotten but not Gone
 Activity Code FA376 HBV in HIV Forgotten but not Gone Richard K. Sterling, MD, MSc VCU Hepatology Professor of Medicine Chief, Section of Hepatology Virginia Commonwealth University Learning Objectives
Activity Code FA376 HBV in HIV Forgotten but not Gone Richard K. Sterling, MD, MSc VCU Hepatology Professor of Medicine Chief, Section of Hepatology Virginia Commonwealth University Learning Objectives
Hepatitis B. What's the impact on the risk? Dr Himanshu Bhatia, Asia Chief Medical Officer ALUCA, Brisbane, Sept 2013
 Hepatitis B What's the impact on the risk? Dr Himanshu Bhatia, Asia Chief Medical Officer ALUCA, Brisbane, Sept 2013 Some quick facts about Hepatitis B Worldwide: 350-400 Million are chronic infections
Hepatitis B What's the impact on the risk? Dr Himanshu Bhatia, Asia Chief Medical Officer ALUCA, Brisbane, Sept 2013 Some quick facts about Hepatitis B Worldwide: 350-400 Million are chronic infections
Chronic Hepatitis B: management update.
 Chronic Hepatitis B: management update. E.O.Ogutu Department of clinical medicine & therapeutics, University of Nairobi. Physicians meeting,kisumu 2011. Background epidemiology Chronic hepatitis B (CHB)
Chronic Hepatitis B: management update. E.O.Ogutu Department of clinical medicine & therapeutics, University of Nairobi. Physicians meeting,kisumu 2011. Background epidemiology Chronic hepatitis B (CHB)
Considerations for Antiretroviral Use in Patients with Hepatitis B Virus & Human Immunodeficiency Syndrome Coinfection
 Considerations for Antiretroviral Use in Patients with Hepatitis B Virus & Human Immunodeficiency Syndrome Coinfection Mahnaz Arian, MD Assistant Professor in infectious Disease Mashhad university of Medical
Considerations for Antiretroviral Use in Patients with Hepatitis B Virus & Human Immunodeficiency Syndrome Coinfection Mahnaz Arian, MD Assistant Professor in infectious Disease Mashhad university of Medical
Hepatitis B Virus. Taylor Page PharmD Candidate 2019 February 1, 2019
 Hepatitis B Virus Taylor Page PharmD Candidate 2019 February 1, 2019 Epidemiology 3218 cases of acute HBV reported in 2016 847,000 non-institutionalized persons living with chronic HBV in 2011-2012 Viral
Hepatitis B Virus Taylor Page PharmD Candidate 2019 February 1, 2019 Epidemiology 3218 cases of acute HBV reported in 2016 847,000 non-institutionalized persons living with chronic HBV in 2011-2012 Viral
CITY & HACKNEY ELIC EAST LONDON INTEGRATED CARE MANAGEMENT OF CHRONIC HEPATITIS B IN PRIMARY CARE
 CITY & HACKNEY ELIC EAST LONDON INTEGRATED CARE MANAGEMENT OF CHRONIC HEPATITIS B IN PRIMARY CARE Chronic Hepatitis B virus (HBV) is an important public health problem globally and a leading cause of liver
CITY & HACKNEY ELIC EAST LONDON INTEGRATED CARE MANAGEMENT OF CHRONIC HEPATITIS B IN PRIMARY CARE Chronic Hepatitis B virus (HBV) is an important public health problem globally and a leading cause of liver
S401- Updates in the Treatments of Hepatitis B & C
 S401- Updates in the Treatments of Hepatitis B & C Ruben Gonzalez-Vallina, MD Director of Gastroenterology Outpatient Initiatives Miami Children s Hospital Miami, Florida Disclosure of Relevant Relationship
S401- Updates in the Treatments of Hepatitis B & C Ruben Gonzalez-Vallina, MD Director of Gastroenterology Outpatient Initiatives Miami Children s Hospital Miami, Florida Disclosure of Relevant Relationship
Viral hepatitis Blood Born hepatitis. Dr. MONA BADR Assistant Professor College of Medicine & KKUH
 Viral hepatitis Blood Born hepatitis Dr. MONA BADR Assistant Professor College of Medicine & KKUH Outline Introduction to hepatitis Characteristics of viral hepatitis Mode of transmission Markers of hepatitis
Viral hepatitis Blood Born hepatitis Dr. MONA BADR Assistant Professor College of Medicine & KKUH Outline Introduction to hepatitis Characteristics of viral hepatitis Mode of transmission Markers of hepatitis
Viral hepatitis. Supervised by: Dr.Gaith. presented by: Shaima a & Anas & Ala a
 Viral hepatitis Supervised by: Dr.Gaith presented by: Shaima a & Anas & Ala a Etiology Common: Hepatitis A Hepatitis B Hepatitis C Hepatitis D Hepatitis E Less common: Cytomegalovirus EBV Rare: Herpes
Viral hepatitis Supervised by: Dr.Gaith presented by: Shaima a & Anas & Ala a Etiology Common: Hepatitis A Hepatitis B Hepatitis C Hepatitis D Hepatitis E Less common: Cytomegalovirus EBV Rare: Herpes
Viral Hepatitis Diagnosis and Management
 Viral Hepatitis Diagnosis and Management CLINICAL BACKGROUND Viral hepatitis is a relatively common disease (25 per 100,000 individuals in the United States) caused by a diverse group of hepatotropic agents
Viral Hepatitis Diagnosis and Management CLINICAL BACKGROUND Viral hepatitis is a relatively common disease (25 per 100,000 individuals in the United States) caused by a diverse group of hepatotropic agents
Dr David Rowbotham NHS. The Leeds Teaching Hospitals. NHS Trust
 Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Nurses Update June 2010 Chronic Hepatitis HBV / HCV David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Nurses Update June 2010 Chronic Hepatitis HBV / HCV David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Media centre. WHO Hepatitis B. Key facts. 1 of :12 AM.
 1 of 5 2013-08-02 7:12 AM Media centre Hepatitis B Share Print Fact sheet N 204 Updated July 2013 Key facts Hepatitis B is a viral infection that attacks the liver and can cause both acute and chronic
1 of 5 2013-08-02 7:12 AM Media centre Hepatitis B Share Print Fact sheet N 204 Updated July 2013 Key facts Hepatitis B is a viral infection that attacks the liver and can cause both acute and chronic
Global reporting system for hepatitis (GRSH) project description
 project description") Global reporting system for hepatitis (GRSH) project description Contents 1. Background... 2 2. Target audience for this document... 2 3. Data to be reported through the Global Reporting System for Hepatitis...
Global reporting system for hepatitis (GRSH) project description Contents 1. Background... 2 2. Target audience for this document... 2 3. Data to be reported through the Global Reporting System for Hepatitis...
Bible Class: Hepatitis B Virus Infection
 Bible Class: Hepatitis B Virus Infection Nasser Semmo UVCM, Hepatology What is the HBV prevalence? 2 Hepatitis B Worldwide approx. 350 Mio. chronically infected with HBV Approx. 40% of the world population:
Bible Class: Hepatitis B Virus Infection Nasser Semmo UVCM, Hepatology What is the HBV prevalence? 2 Hepatitis B Worldwide approx. 350 Mio. chronically infected with HBV Approx. 40% of the world population:
Emerging Challenges In Primary Care: Chronic Hepatitis B: Guidelines for Screening, Clinical Management, Whether to Follow or Treat, and How
 Emerging Challenges In Primary Care: 2015 Chronic Hepatitis B: Guidelines for Screening, Clinical Management, Whether to Follow or Treat, and How 1 Faculty Christopher O'Brien, MD, AGAF, FRCMI Professor
Emerging Challenges In Primary Care: 2015 Chronic Hepatitis B: Guidelines for Screening, Clinical Management, Whether to Follow or Treat, and How 1 Faculty Christopher O'Brien, MD, AGAF, FRCMI Professor
Emerging Challenges In Primary Care: 2015
 Emerging Challenges In Primary Care: 2015 Chronic Hepatitis B: Guidelines for Screening, Clinical Management, Whether to Follow or Treat, 1 Faculty Christopher O'Brien, MD, AGAF, FRCMI Professor of Clinical
Emerging Challenges In Primary Care: 2015 Chronic Hepatitis B: Guidelines for Screening, Clinical Management, Whether to Follow or Treat, 1 Faculty Christopher O'Brien, MD, AGAF, FRCMI Professor of Clinical
GUIDELINES ON HEPATITIS B AND C TESTING POLICY BRIEF
 NOVEMBER 2016 GUIDELINES ON HEPATITIS B AND C TESTING POLICY BRIEF NOVEMBER 2016 GUIDELINES ON HEPATITIS B AND C TESTING POLICY BRIEF WHO Library Cataloguing-in-Publication Data Guidelines on hepatitis
NOVEMBER 2016 GUIDELINES ON HEPATITIS B AND C TESTING POLICY BRIEF NOVEMBER 2016 GUIDELINES ON HEPATITIS B AND C TESTING POLICY BRIEF WHO Library Cataloguing-in-Publication Data Guidelines on hepatitis
The Impact of HBV Therapy on Fibrosis and Cirrhosis
 The Impact of HBV Therapy on Fibrosis and Cirrhosis Jordan J. Feld, MD, MPH Associate Professor of Medicine University of Toronto Hepatologist Toronto Centre for Liver Disease Sandra Rotman Centre for
The Impact of HBV Therapy on Fibrosis and Cirrhosis Jordan J. Feld, MD, MPH Associate Professor of Medicine University of Toronto Hepatologist Toronto Centre for Liver Disease Sandra Rotman Centre for
Emerging Challenges In Primary Care: 2015
 Emerging Challenges In Primary Care: 2015 Chronic Hepatitis B: Guidelines for Screening, Clinical Management, Whether to Follow or Treat, 1 Faculty Christopher O'Brien, MD, AGAF, FRCMI Professor of Clinical
Emerging Challenges In Primary Care: 2015 Chronic Hepatitis B: Guidelines for Screening, Clinical Management, Whether to Follow or Treat, 1 Faculty Christopher O'Brien, MD, AGAF, FRCMI Professor of Clinical
Hepatitis C Virus (HCV) & Infectious Disease 101 for Hubs & Spokes April 24, :00 pm 1:00 pm
 & Infectious Disease 101 for Hubs & Spokes April 24, :00 pm 1:00 pm") Hepatitis C Virus (HCV) & Infectious Disease 101 for Hubs & Spokes April 24, 2018 12:00 pm 1:00 pm Presenters: Thomas E. Freese, PhD, Larissa Mooney, MD, & Rachel McLean, MPH, Chief, Office of Viral Hepatitis
Hepatitis C Virus (HCV) & Infectious Disease 101 for Hubs & Spokes April 24, 2018 12:00 pm 1:00 pm Presenters: Thomas E. Freese, PhD, Larissa Mooney, MD, & Rachel McLean, MPH, Chief, Office of Viral Hepatitis
World Health Organization. Western Pacific Region
 Basic modules for hepatitis 1 Basic Module 1 Liver anatomy and physiology 2 Position of liver Midline Located in right upper abdomen Protected by the right rib cage Right upper Measures: 12 15 cm in vertical
Basic modules for hepatitis 1 Basic Module 1 Liver anatomy and physiology 2 Position of liver Midline Located in right upper abdomen Protected by the right rib cage Right upper Measures: 12 15 cm in vertical
Hepatitis C Update on New Treatments
 Hepatitis C Update on New Treatments Kevork M. Peltekian, MD, FRCPC 44th Annual Dalhousie Spring Refresher Course - Therapeutics April 5 - April 7, 2018 Halifax Convention Centre Disclosures Conflicts
Hepatitis C Update on New Treatments Kevork M. Peltekian, MD, FRCPC 44th Annual Dalhousie Spring Refresher Course - Therapeutics April 5 - April 7, 2018 Halifax Convention Centre Disclosures Conflicts
HBV : Structure. HBx protein Transcription activator
 Hepatitis B Virus 1 Hepatitis B Virus 2 Properties of HBV a member of the hepadnavirus group Enveloped, partially double-stranded DNA viruses, smallest DNA virus Replication involves a reverse transcriptase
Hepatitis B Virus 1 Hepatitis B Virus 2 Properties of HBV a member of the hepadnavirus group Enveloped, partially double-stranded DNA viruses, smallest DNA virus Replication involves a reverse transcriptase
GAZETTE COMMON GROUND. CHB: A significant and prevalent disease in the US and worldwide. Inside. Screening, diagnosis, and evaluation
 VOL III/III COMMON GROUND GAZETTE Inside CASE 1: Screening, diagnosis, and evaluation P. 1 CASE 2: Initiating treatment P. 4 CASE 3: Managing antiviral resistance P. 5 CASE 4: Achieving the maximum effect
VOL III/III COMMON GROUND GAZETTE Inside CASE 1: Screening, diagnosis, and evaluation P. 1 CASE 2: Initiating treatment P. 4 CASE 3: Managing antiviral resistance P. 5 CASE 4: Achieving the maximum effect
Clinical dilemmas in HBeAg-negative CHB
 Clinical dilemmas in HBeAg-negative CHB George V. Papatheodoridis Professor in Medicine & Gastroenterology Medical School of National & Kapodistrian University of Athens Director of Academic Department
Clinical dilemmas in HBeAg-negative CHB George V. Papatheodoridis Professor in Medicine & Gastroenterology Medical School of National & Kapodistrian University of Athens Director of Academic Department
Lifetime risk of infection >60% Early childhood infections common
 Hepatitis Community Medicine HBV Public health sig HBV is 100 times more infectious than HIV. >350 million chronically infected worldwide. >1 million people die annually of HBV- related chronic liver disease.
Hepatitis Community Medicine HBV Public health sig HBV is 100 times more infectious than HIV. >350 million chronically infected worldwide. >1 million people die annually of HBV- related chronic liver disease.
Hepatitis B infection
 Hepatitis B infection Kenneth Kabagambe Executive Director The National Organization for People Living with Hepatitis B (NOPLHB Uganda General introduction: Viral hepatitis in Uganda Viruses that affect
Hepatitis B infection Kenneth Kabagambe Executive Director The National Organization for People Living with Hepatitis B (NOPLHB Uganda General introduction: Viral hepatitis in Uganda Viruses that affect
Updates in the Treatment of Hepatitis C
 Disclosures Updates in the Treatment of Hepatitis C Arslan Kahloon M.D Assistant Professor of Medicine University of Tennessee, Chattanooga I have no conflicts of interest or financial sponsorship to disclose
Disclosures Updates in the Treatment of Hepatitis C Arslan Kahloon M.D Assistant Professor of Medicine University of Tennessee, Chattanooga I have no conflicts of interest or financial sponsorship to disclose
HBV Diagnosis and Treatment
 HBV Diagnosis and Treatment Anna S. F. Lok, MD Alice Lohrman Andrews Professor in Hepatology Director of Clinical Hepatology Assistant Dean for Clinical Research University of Michigan Ann Arbor, MI, USA
HBV Diagnosis and Treatment Anna S. F. Lok, MD Alice Lohrman Andrews Professor in Hepatology Director of Clinical Hepatology Assistant Dean for Clinical Research University of Michigan Ann Arbor, MI, USA
Learning Objectives: Hepatitis Update. Primary Causes of Chronic Liver Disease in the U.S. Hepatitis Definition. Hepatitis Viruses.
 Learning Objectives: Hepatitis Update ASCLS-Michigan March 31, 2016 Dr. Kathleen Hoag Upon attendance of this seminar and review of material provided, the attendees will be able to: 1. List hepatitis viruses
Learning Objectives: Hepatitis Update ASCLS-Michigan March 31, 2016 Dr. Kathleen Hoag Upon attendance of this seminar and review of material provided, the attendees will be able to: 1. List hepatitis viruses
Hepatitis C Virus (HCV)
") Clinical Practice Guidelines Hepatitis C Virus (HCV) OBJECTIVE The purpose is to guide the appropriate diagnosis and management of Hepatitis C Virus (HCV). GUIDELINE These are only guidelines, and are
Clinical Practice Guidelines Hepatitis C Virus (HCV) OBJECTIVE The purpose is to guide the appropriate diagnosis and management of Hepatitis C Virus (HCV). GUIDELINE These are only guidelines, and are
Hepatitis B Update. Jorge L. Herrera, M.D. University of South Alabama Mobile, AL. Gastroenterology
 Hepatitis B Update Jorge L. Herrera, M.D. University of South Alabama Mobile, AL Deciding Who to Treat Is hepatitis B a viral disease or a liver disease? Importance of HBV-DNA Levels in the Natural History
Hepatitis B Update Jorge L. Herrera, M.D. University of South Alabama Mobile, AL Deciding Who to Treat Is hepatitis B a viral disease or a liver disease? Importance of HBV-DNA Levels in the Natural History
Confirmed (Laboratory Tests) Serum positive for IgM anti-hbc or, hepatitis B surface antigen (HbsAg).
 Serum positive for IgM anti-hbc or, hepatitis B surface antigen (HbsAg).") Hepatitis B Hepatitis B is a liver disease that results from infection with the Hepatitis B virus. It can range in severity from a mild illness lasting a few weeks to a serious, lifelong illness. Hepatitis
Hepatitis B Hepatitis B is a liver disease that results from infection with the Hepatitis B virus. It can range in severity from a mild illness lasting a few weeks to a serious, lifelong illness. Hepatitis
CASES FOR DISCUSSION. Yohannes B
 CASES FOR DISCUSSION Yohannes B HCV CASE-1 A 34 years old apparently healthy lady who came to us after being told to have HCV infection on medical checkup done as part of a visa approval process to travel
CASES FOR DISCUSSION Yohannes B HCV CASE-1 A 34 years old apparently healthy lady who came to us after being told to have HCV infection on medical checkup done as part of a visa approval process to travel
WHEN HCV TREATMENT IS DEFERRED WV HEPC ECHO PROJECT
 WHEN HCV TREATMENT IS DEFERRED WV HEPC ECHO PROJECT October 13, 2016 Reminder - treatment is recommended for all patients with chronic HCV infection Except short life expectancies that cannot be remediated
WHEN HCV TREATMENT IS DEFERRED WV HEPC ECHO PROJECT October 13, 2016 Reminder - treatment is recommended for all patients with chronic HCV infection Except short life expectancies that cannot be remediated
Dr. John C Rwegasha.FRCP(Lond),MSc, Muhimbili National Hospital Dar es Salaam Tanzania 15/09/2018 1
,MSc, Muhimbili National Hospital Dar es Salaam Tanzania 15/09/2018 1") Dr. John C Rwegasha.FRCP(Lond),MSc, Muhimbili National Hospital Dar es Salaam Tanzania 15/09/2018 1 No disclosures. 15/09/2018 2 Sub-Saharan Africa (SSA) has a high burden of morbidity and mortality resulting
Dr. John C Rwegasha.FRCP(Lond),MSc, Muhimbili National Hospital Dar es Salaam Tanzania 15/09/2018 1 No disclosures. 15/09/2018 2 Sub-Saharan Africa (SSA) has a high burden of morbidity and mortality resulting
Hepatitis B: A Preventable Cause of Liver Cancer. Saira Khaderi MD, MPH Assistant Professor of Surgery Associate Director, Project ECHO June 17, 2016
 Hepatitis B: A Preventable Cause of Liver Cancer Saira Khaderi MD, MPH Assistant Professor of Surgery Associate Director, Project ECHO June 17, 2016 Overview Epidemiology HBV and cancer Screening, Diagnosis
Hepatitis B: A Preventable Cause of Liver Cancer Saira Khaderi MD, MPH Assistant Professor of Surgery Associate Director, Project ECHO June 17, 2016 Overview Epidemiology HBV and cancer Screening, Diagnosis
The ABCs of Viral Hepatitis Diagnosis. Ila Singh, M.D., Ph.D. P & S Viral Hepatitis. Hepatitis A, B, C, D, E and G viruses
 The ABCs of Viral Hepatitis Diagnosis Ila Singh, M.D., Ph.D. P & S 14-453 is132@columbia.edu Viral Hepatitis Hepatotropic viruses Hepatitis A, B, C, D, E and G viruses Generalized infection plus infection
The ABCs of Viral Hepatitis Diagnosis Ila Singh, M.D., Ph.D. P & S 14-453 is132@columbia.edu Viral Hepatitis Hepatotropic viruses Hepatitis A, B, C, D, E and G viruses Generalized infection plus infection
Viral Hepatitis: Dr Erana Gray General and Infectious Diseases Physician
 Viral Hepatitis: Dr Erana Gray General and Infectious Diseases Physician Outline: Virology HBV + pregnancy HCV + new treatments Cases Hepatitis Foundation HBV: virus HBsAg far in excess of complete virions,
Viral Hepatitis: Dr Erana Gray General and Infectious Diseases Physician Outline: Virology HBV + pregnancy HCV + new treatments Cases Hepatitis Foundation HBV: virus HBsAg far in excess of complete virions,
Hepatitis B Treatment Pearls. Agenda
 Hepatitis B Treatment Pearls Fredric D. Gordon, MD Vice Chair Dept. of Transplantation and Hepatobiliary Diseases Lahey Hospital & Medical Center Associate Professor of Medicine Tufts Medical School Boston,
Hepatitis B Treatment Pearls Fredric D. Gordon, MD Vice Chair Dept. of Transplantation and Hepatobiliary Diseases Lahey Hospital & Medical Center Associate Professor of Medicine Tufts Medical School Boston,
NH2 N N N O N O O P O O O O O
 N N NH 2 N N O O P O O O O O O James Watson and Francis Crick Double Helix 1953 Baruch Blumberg, MD, PhD 1925-2011 Australia Antigen 1965 Hepatitis B Virus (HBV) Hepadnaviridae member that primarily infects
N N NH 2 N N O O P O O O O O O James Watson and Francis Crick Double Helix 1953 Baruch Blumberg, MD, PhD 1925-2011 Australia Antigen 1965 Hepatitis B Virus (HBV) Hepadnaviridae member that primarily infects
Update on Hepatitis B and Hepatitis C
 Update on Hepatitis B and Hepatitis C Catherine Stedman Department of Gastroenterology, Christchurch Hospital and University of Otago, Christchurch Disclosures I have the following financial relationships
Update on Hepatitis B and Hepatitis C Catherine Stedman Department of Gastroenterology, Christchurch Hospital and University of Otago, Christchurch Disclosures I have the following financial relationships
Patients must have met all of the following inclusion criteria to be eligible for participation in this study.
 Supplementary Appendix S1: Detailed inclusion/exclusion criteria Patients must have met all of the following inclusion criteria to be eligible for participation in this study. Inclusion Criteria 1) Willing
Supplementary Appendix S1: Detailed inclusion/exclusion criteria Patients must have met all of the following inclusion criteria to be eligible for participation in this study. Inclusion Criteria 1) Willing
Maitines septiembre de 2011 Francisco Jorquera Plaza
 Bringing Into Focus: A Practical Guide to Using Virologic and Serologic Tests in the Management of Hepatitis B Maitines septiembre de 2011 Francisco Jorquera Plaza 2.000 millones de personas infectadas
Bringing Into Focus: A Practical Guide to Using Virologic and Serologic Tests in the Management of Hepatitis B Maitines septiembre de 2011 Francisco Jorquera Plaza 2.000 millones de personas infectadas
HEPATITIS B INFECTION and Pregnancy. Caesar Mensah Communicable Diseases & Infection Control Specialist, UK June 2011
 HEPATITIS B INFECTION and Pregnancy Caesar Mensah Communicable Diseases & Infection Control Specialist, UK June 2011 HEPATITIS B 26/07/2011 What is Hepatitis B? It is inflammation (infection) of the liver
HEPATITIS B INFECTION and Pregnancy Caesar Mensah Communicable Diseases & Infection Control Specialist, UK June 2011 HEPATITIS B 26/07/2011 What is Hepatitis B? It is inflammation (infection) of the liver
EASL Clinical Practice Guidelines: Management of chronic hepatitis B virus infection
 EASL Clinical Practice Guidelines: Management of chronic hepatitis B virus infection European Association for the Study of the Liver Introduction Our understanding of the natural history of hepatitis B
EASL Clinical Practice Guidelines: Management of chronic hepatitis B virus infection European Association for the Study of the Liver Introduction Our understanding of the natural history of hepatitis B
Hepatitis B. ECHO November 29, Joseph Ahn, MD, MS Associate Professor of Medicine Director of Hepatology Oregon Health & Science University
 Hepatitis B ECHO November 29, 2017 Joseph Ahn, MD, MS Associate Professor of Medicine Director of Hepatology Oregon Health & Science University Disclosures Advisory board Gilead Comments The speaker Joseph
Hepatitis B ECHO November 29, 2017 Joseph Ahn, MD, MS Associate Professor of Medicine Director of Hepatology Oregon Health & Science University Disclosures Advisory board Gilead Comments The speaker Joseph
Treatment of chronic hepatitis delta Case report
 Treatment of chronic hepatitis delta Case report George Papatheodoridis Professor in Medicine & Gastroenterology Medical School of National and Kapodistrian University of Athens, Director of Academic Department
Treatment of chronic hepatitis delta Case report George Papatheodoridis Professor in Medicine & Gastroenterology Medical School of National and Kapodistrian University of Athens, Director of Academic Department
Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER
 Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER Objective Epidemiology Screening criteria Appropriate work up Treatment Guidelines
Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER Objective Epidemiology Screening criteria Appropriate work up Treatment Guidelines
Global Reporting System for Hepatitis (GRSH) An introduction. WHO Global Hepatitis Programme
 An introduction. WHO Global Hepatitis Programme") Global Reporting System for Hepatitis (GRSH) An introduction WHO Global Hepatitis Programme 2018 Objectives 1. Explain the role of the new reporting system 2. Outline the reporting required from countries
Global Reporting System for Hepatitis (GRSH) An introduction WHO Global Hepatitis Programme 2018 Objectives 1. Explain the role of the new reporting system 2. Outline the reporting required from countries
Hepatitis B. Epidemiology and Natural History and Implications for Treatment
 Hepatitis B Epidemiology and Natural History and Implications for Treatment Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco
Hepatitis B Epidemiology and Natural History and Implications for Treatment Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco
Hepadnaviridae family (DNA) Numerous antigenic components Humans are only known host May retain infectivity for more than 7 days at room temperature
 Numerous antigenic components Humans are only known host May retain infectivity for more than 7 days at room temperature") Hepatitis B Epidemic jaundice described by Hippocrates in 5th century BC Jaundice reported among recipients of human serum and yellow fever vaccines in 1930s and 1940s Australia antigen described in 1965
Hepatitis B Epidemic jaundice described by Hippocrates in 5th century BC Jaundice reported among recipients of human serum and yellow fever vaccines in 1930s and 1940s Australia antigen described in 1965
ACTIVITY DISCLAIMER. Kurt Cook, MD, MSc DISCLOSURE. Audience Engagement System. Learning Objectives
 On the Liver Disease Front Lines: Hepatitis A, B and C Prevention and Treatment Kurt Cook, MD, MSc ACTIVITY DISCLAIMER The material presented here is being made available by the American Academy of Family
On the Liver Disease Front Lines: Hepatitis A, B and C Prevention and Treatment Kurt Cook, MD, MSc ACTIVITY DISCLAIMER The material presented here is being made available by the American Academy of Family
Delta hepatitis: How to manage and optimize therapy? Dominique ROULOT Unité d Hépatologie, Hôpital Avicenne
 Delta hepatitis: How to manage and optimize therapy? Dominique ROULOT Unité d Hépatologie, Hôpital Avicenne Delta hepatitis treatment in 2018 Currently, Peg-IFNα 180 µg/wk is the only effective treatment
Delta hepatitis: How to manage and optimize therapy? Dominique ROULOT Unité d Hépatologie, Hôpital Avicenne Delta hepatitis treatment in 2018 Currently, Peg-IFNα 180 µg/wk is the only effective treatment
Commonly Asked Questions About Chronic Hepatitis C
 Commonly Asked Questions About Chronic Hepatitis C From the American College of Gastroenterology 1. How common is the hepatitis C virus? The hepatitis C virus is the most common cause of chronic viral
Commonly Asked Questions About Chronic Hepatitis C From the American College of Gastroenterology 1. How common is the hepatitis C virus? The hepatitis C virus is the most common cause of chronic viral
IN THE NAME OF GOD. D r. MANIJE DEZFULI AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL INFECTIOUS DISEASES SPECIALIST
 IN THE NAME OF GOD AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL D r. MANIJE DEZFULI INFECTIOUS DISEASES SPECIALIST Acute Viral Hepatitis The Anatomy of the Liver Hepatic Physiology Liver: Largest solid organ
IN THE NAME OF GOD AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL D r. MANIJE DEZFULI INFECTIOUS DISEASES SPECIALIST Acute Viral Hepatitis The Anatomy of the Liver Hepatic Physiology Liver: Largest solid organ
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
End Stage Liver Disease & Disease Specific Indications for Liver Transplant. Susan Kang, RN, MSN, ANP-BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
Hepatitis B Virus therapy. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 Hepatitis B Virus therapy Maria Buti Hospital Universitario Valle Hebron Barcelona Spain Disclosures Advisor: AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck Sharp &
Hepatitis B Virus therapy Maria Buti Hospital Universitario Valle Hebron Barcelona Spain Disclosures Advisor: AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck Sharp &
Sandi Mitchell Nurse Educator Clinical Prevention Services BCCDC
 Sandi Mitchell Nurse Educator Clinical Prevention Services BCCDC sandi.mitchell@bccdc.ca Hepatitis A, B and C Testing Transmission Treatment What Is Hepatitis? Hepatitis means inflammation of the liver
Sandi Mitchell Nurse Educator Clinical Prevention Services BCCDC sandi.mitchell@bccdc.ca Hepatitis A, B and C Testing Transmission Treatment What Is Hepatitis? Hepatitis means inflammation of the liver
Viral Hepatitis in Children DR. HOSSAIN IBRAHIM AGEEL PEDIATRIC GASTROENTEROLOGIST PEDIATRIC DEPARTMENT KFCH JAZAN
 Viral Hepatitis in Children DR. HOSSAIN IBRAHIM AGEEL PEDIATRIC GASTROENTEROLOGIST PEDIATRIC DEPARTMENT KFCH JAZAN General Concepts Hepatitis = 'inflammation of the liver'. Virus causes: Hepatotropic and
Viral Hepatitis in Children DR. HOSSAIN IBRAHIM AGEEL PEDIATRIC GASTROENTEROLOGIST PEDIATRIC DEPARTMENT KFCH JAZAN General Concepts Hepatitis = 'inflammation of the liver'. Virus causes: Hepatotropic and
DISCLOSURES. This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea
 DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
Chronic hepatitis B: diagnosis, monitoring and management
 PRESCRIBING IN PRACTICE n Chronic hepatitis B: diagnosis, monitoring and management Ben Hudson MRCP and Peter Collins MD, FRCP Hepatitis B is a blood-borne DNA virus and chronic disease is defined as failure
PRESCRIBING IN PRACTICE n Chronic hepatitis B: diagnosis, monitoring and management Ben Hudson MRCP and Peter Collins MD, FRCP Hepatitis B is a blood-borne DNA virus and chronic disease is defined as failure
Community/GP based screening & management of HBV & HCV
 Community/GP based screening & management of HBV & HCV Catherine Stedman Department of Gastroenterology, Christchurch Hospital and University of Otago, Christchurch Disclosures I have the following financial
Community/GP based screening & management of HBV & HCV Catherine Stedman Department of Gastroenterology, Christchurch Hospital and University of Otago, Christchurch Disclosures I have the following financial
ESCMID Online Lecture Library. by author
 Hepatitis B virus and solid organ transplantation Prof. Hakan Leblebicioglu Department of Clinical Microbiology and Infectious Diseases Ondokuz Mayis University, Samsun, Turkey Conflict of interest Outline
Hepatitis B virus and solid organ transplantation Prof. Hakan Leblebicioglu Department of Clinical Microbiology and Infectious Diseases Ondokuz Mayis University, Samsun, Turkey Conflict of interest Outline
Liver Disease. By: Michael Martins
 Liver Disease By: Michael Martins Recently I have been getting a flurry of patients that have some serious liver complications. This week s literature review will be the dental management of the patients
Liver Disease By: Michael Martins Recently I have been getting a flurry of patients that have some serious liver complications. This week s literature review will be the dental management of the patients
HEPATITIS VIRUSES. Other causes (not exclusively hepatitis v.)also called sporadic hepatitis: HEPATITIS A(infectious hepatitis)
also called sporadic hepatitis: HEPATITIS A(infectious hepatitis)") Dept.of Microbiology/Virology Assist.prof. Shatha F. Abdullah HEPATITIS VIRUSES Medically important hepatitis v. (liver)are: 1.HAV 2.HBV 3.HCV 4.HDV 5.HEV 6.HGV Other causes (not exclusively hepatitis
Dept.of Microbiology/Virology Assist.prof. Shatha F. Abdullah HEPATITIS VIRUSES Medically important hepatitis v. (liver)are: 1.HAV 2.HBV 3.HCV 4.HDV 5.HEV 6.HGV Other causes (not exclusively hepatitis
Hepatology for the Nonhepatologist
 Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
CURRENT TREATMENT. Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, Virginia
 CURRENT TREATMENT OF HBV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, Virginia CHRONIC HBV INFECTION DEMOGRAPHICS IN THE USA Estimated
CURRENT TREATMENT OF HBV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, Virginia CHRONIC HBV INFECTION DEMOGRAPHICS IN THE USA Estimated
Hepatitis A-E Viruses. Dr Nemes Zsuzsanna
 Hepatitis A-E Viruses Dr Nemes Zsuzsanna Viral Hepatitis - Historical Perspectives Infectious A E Enterically transmitted Viral hepatitis NANB Serum B D C Parenterally transmitted HGV, TTV, SEN, other
Hepatitis A-E Viruses Dr Nemes Zsuzsanna Viral Hepatitis - Historical Perspectives Infectious A E Enterically transmitted Viral hepatitis NANB Serum B D C Parenterally transmitted HGV, TTV, SEN, other
Drug Class Monograph
 Drug Class Monograph Class: Chronic Hepatitis B Drug: Baraclude (entecavir), Epivir (lamivudine), Hepsera (adefovir), Intron A (interferon alfa- 2b), Pegasys (peginterferon alfa-2a), Tyzeka (telbivudine),
Drug Class Monograph Class: Chronic Hepatitis B Drug: Baraclude (entecavir), Epivir (lamivudine), Hepsera (adefovir), Intron A (interferon alfa- 2b), Pegasys (peginterferon alfa-2a), Tyzeka (telbivudine),
Uses and Misuses of Viral Hepatitis Testing. Origins of Liver Science
 Uses and Misuses of Viral Hepatitis Testing Richard S Lang, MD, MPH, FACP Chairman, Preventive Medicine Vice-Chair, Wellness Institute Raul J Seballos, MD, FACP Vice-Chair, Preventive Medicine Wellness
Uses and Misuses of Viral Hepatitis Testing Richard S Lang, MD, MPH, FACP Chairman, Preventive Medicine Vice-Chair, Wellness Institute Raul J Seballos, MD, FACP Vice-Chair, Preventive Medicine Wellness
Hepatitis Case Investigation
 * indicates required fields Does patient also have: Hepatitis Case Investigation West Virginia Electronic Disease Surveillance System Division of Surveillance and Disease Control Infectious Disease Epidemiology
* indicates required fields Does patient also have: Hepatitis Case Investigation West Virginia Electronic Disease Surveillance System Division of Surveillance and Disease Control Infectious Disease Epidemiology
Management of Acute HCV Infection
 Management of Acute HCV Infection This section provides guidance on the diagnosis and medical management of acute HCV infection, which is defined as presenting within 6 months of the exposure. During this
Management of Acute HCV Infection This section provides guidance on the diagnosis and medical management of acute HCV infection, which is defined as presenting within 6 months of the exposure. During this
Choice of Oral Drug for Hepatitis B: Status Asokananda Konar
 Choice of Oral Drug for Hepatitis B: Status 2011 Asokananda Konar Chronic hepatitis B (CHB) is a global public health challenge with an estimated 350 to 400 million people with chronic HBV infection, despite
Choice of Oral Drug for Hepatitis B: Status 2011 Asokananda Konar Chronic hepatitis B (CHB) is a global public health challenge with an estimated 350 to 400 million people with chronic HBV infection, despite
KASL Clinical Practice Guidelines: Management of chronic hepatitis B
 pissn 2287-2728 eissn 2287-285X Review Clinical and Molecular Hepatology 2012;18:109-162 KASL Clinical Practice Guidelines: Management of chronic hepatitis B The Korean Association for the Study of the
pissn 2287-2728 eissn 2287-285X Review Clinical and Molecular Hepatology 2012;18:109-162 KASL Clinical Practice Guidelines: Management of chronic hepatitis B The Korean Association for the Study of the
Hepatitis B Prior Authorization Policy
 Hepatitis B Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Hepatitis B Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Management of Hepatitis B
 Management of Hepatitis B Background HBV is contracted either sexually or by blood to blood transmission. The combined prevalence of HBV and HCV is just over 2% in the UK. More than 95% of immune competent
Management of Hepatitis B Background HBV is contracted either sexually or by blood to blood transmission. The combined prevalence of HBV and HCV is just over 2% in the UK. More than 95% of immune competent
9/12/2018. Hepatitis B Virus Infection. Hepatitis B Infection
 Centers for Disease Control and Prevention National Center for Immunization and Respiratory Diseases Hepatitis B and Hepatitis B Vaccine Adult Track Chapter 10 Photographs and images included in this presentation
Centers for Disease Control and Prevention National Center for Immunization and Respiratory Diseases Hepatitis B and Hepatitis B Vaccine Adult Track Chapter 10 Photographs and images included in this presentation
ARTICLE IN PRESS. A Treatment Algorithm for the Management of Chronic Hepatitis B Virus Infection in the United States: An Update
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:xxx REVIEW A Treatment Algorithm for the Management of Chronic Hepatitis B Virus Infection in the United States: An Update EMMET B. KEEFFE,* DOUGLAS T. DIETERICH,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:xxx REVIEW A Treatment Algorithm for the Management of Chronic Hepatitis B Virus Infection in the United States: An Update EMMET B. KEEFFE,* DOUGLAS T. DIETERICH,
The Alphabet Soup of Viral Hepatitis Testing
 The Alphabet Soup of Viral Hepatitis Testing August 18, 2011 Patricia Slev, PhD, DABCC Medical Director, Serologic Hepatitis and Retrovirus Laboratory, ARUP Laboratories Assistant Professor of Pathology,
The Alphabet Soup of Viral Hepatitis Testing August 18, 2011 Patricia Slev, PhD, DABCC Medical Director, Serologic Hepatitis and Retrovirus Laboratory, ARUP Laboratories Assistant Professor of Pathology,