Contact Investigation and Prevention in the USA
|
|
|
- Nathaniel Short
- 5 years ago
- Views:
Transcription


1 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis Institute Annual Meeting of the Child and Adolescent TB working group The Hague, The Netherlands October 24, 2018
2 Control of Tuberculosis in the United States Case finding and treatment 2016: 9,272 cases: incidence 2.9 cases/100, % in children Contact investigations Source case investigations Targeted testing of persons with risk Diagnosis and treatment of LTBI is critical to control and elimination of TB in the U.S. Red Book 2012
3 Objectives of the Contact Investigation Identify all high and low risk contacts Medically evaluate all appropriate contacts Identify contacts diagnosed with LTBI and provide appropriate treatment to completion of therapy thus preventing future disease Identify contacts diagnosed with TB disease and provide appropriate treatment to completion of therapy thus preventing further transmission Identify contacts at high risk of developing TB disease (e.g., children, immunocompromised) and provide appropriate treatment until infection and disease is ruled out


4 Control of TB in the United States Case finding + treatment -> Contact investigations The most reliable TB control program is based upon aggressive and expedient contact investigations, rather than routine screening of large populations High priority contact: Household Age <5 yrs Med risk condition Procedure Congregate, Time Can be complex and may require lots of detective work Red Book 2009

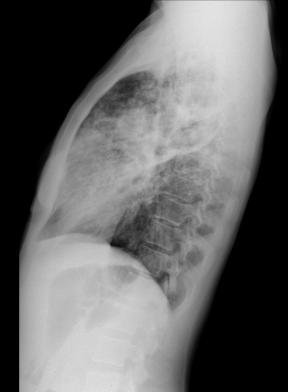
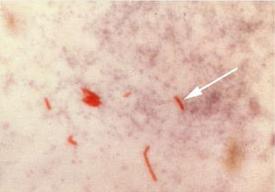
5 Contact Investigation A 39 year-old female was admitted to a New Jersey hospital with fever, decreased appetite, 11 kg weight loss, cough X 1-3 months, night sweats Chest radiographs were done Sputa were 4+ AFB, later identified as pansensitive M. tbc Presumptive case of TB reported to to local health department Place of employment-daycare Center Health department nurse contacted TB controller for the county


6 Daycare Contact (DCC) Investigation On-site assessment of DCC conducted by TB controller: High priority contacts: children attend: All <4 years of age 5 staff members: Adults and adolescents Daycare is in a church basement Index patient was secretary with little contact with the children Household and social contacts High priority contacts: 9; field staff felt index pt. did not reveal all contacts 4 are children: 2 are <1 year of age with recent history of pneumonia
7 Church Basement-Daycare
8 Contact Investigation Results: Totals After Initial Testing Daycare Center <4 yrs old (+) TST 14/35 (40%) (-) TST 21/35 (60%) TB disease 7/35 (20%) All <4 yrs old Household + Social 9 2 <4 yrs old (+) TST 5/9 (56%) (-) TST 4/9 (44%) TB disease 2/9 (22%) Both <1 yr old



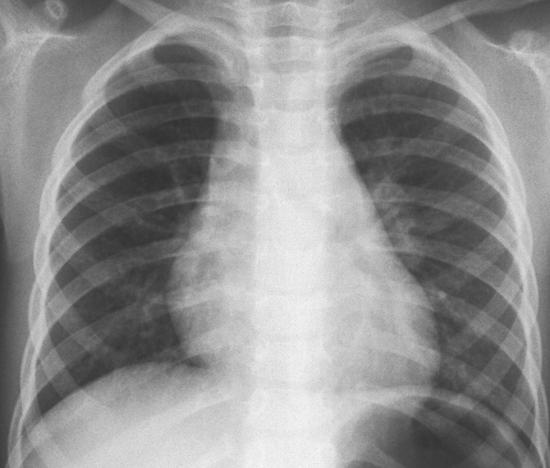
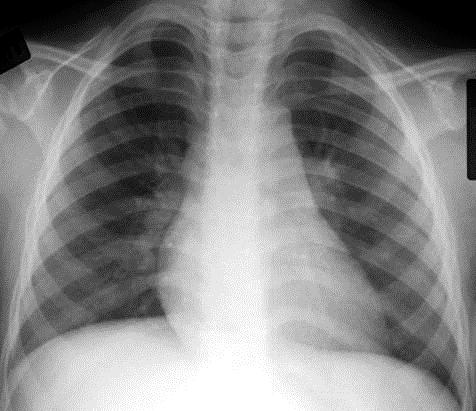
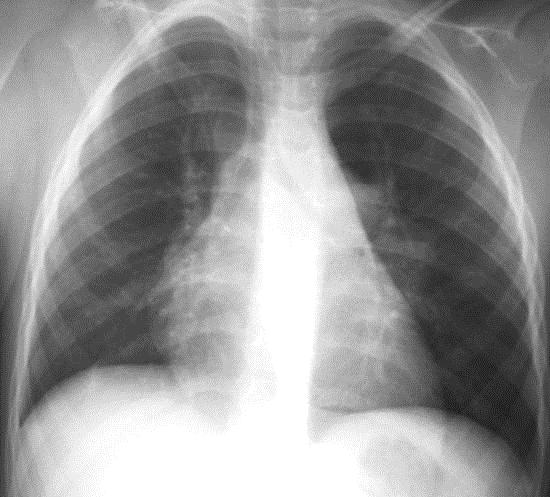

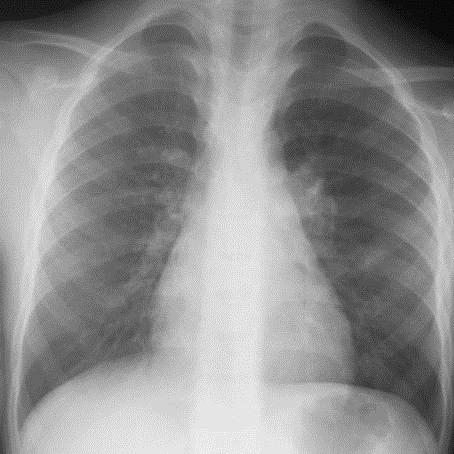
9 TB in 6 mo old 6 mo old 3 yr old Daycare 3 yr old 4 yr old 2 yr old 3 yr old 2 yr old 4 yr old
10 Contact vs. Source Case Investigation CONTACT INVESTIGATION LTBI INDEX PATIENT TRANSMISSION TB DISEASE SOURCE CASE INVESTIGATION TRANSMISSION LTBI TB DISEASE INDEX CASE



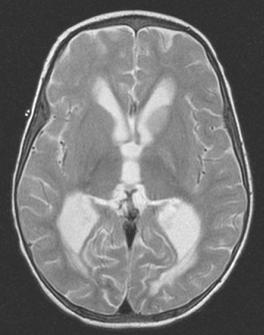

11 CT MRI

12

13
14 US Contact Investigations Outcomes - Sputum AFB Smear (+) Year # Cases Sputum sm (+) # Contacts ID Evaluation Indices National Objective Contact index No contacts ID 8% 8% 7% 7% 6% 5% 5% 5% 6% 6% Evaluated % Not evaluated TB disease 1% 1% 1% 1% 1% <1% <1% <1% <1% <1% Infected 24% 23% 23% 22% 20% 19% 19% 19% 19% 17% LTBI treatment 69% 72% 71% 74% 67% 74% 70% 68% 71% 72% 91% initiated LTBI treatment completed 63% 66% 68% 64% 67% 67% 66% 66% 71% 74% 81%
15 Targeted Testing for Tuberculosis in Children and Adolescents Children for whom immediate TST or IGRA is indicated: Contacts of people with confirmed or suspected contagious TB (contact investigation) Children with radiographic or clinical findings suggesting tuberculosis disease Children immigrating from high rates of infections (Asia, Middle East, Africa, Latin America, counties of the former Soviet Union) Children with history of significant travel to countries with endemic infection who have substantial contact with the resident population Children who should have annual TST or IGRA: Children with HIV infection Children at increased risk of progression of TBI to TB disease HIV infection, Hodgkin disease, lymphoma, diabetes mellitus, chronic renal failure, malnutrition, prolonged or high-dose corticosteroid therapy, chemotherapy, tumor necrosis factor (TNF-alpha) antagonists Red Book 2018
16 Changes in TB Diagnosis Tools in Children: IGRAs and the 2018 RED BOOK IGRAs recommended in immunocompetent children >2 years of age [previously >5 years of age] in all situations where a TST would be used Particularly useful for children who have received BCG vaccination Use with caution in immunocompromised children TST was acceptable for all age groups and remains the preferred test for those <2 years of age In evaluating children for TB disease neither IGRAs nor the TST are perfect; always need clinical judgement Red Book 2018
17 Treatment of Tuberculosis Infection in Children: 2018 Red Book and CDC Isoniazid + rifapentine (3HP)* Rifampin (4R) Isoniazid (9H) *Red Book does not state a preference but says that some experts think 3HP is the preferred regimen Borisov A, et al, MMWR 2018
18 LTBI treatment: 3HP for children As effective as 9H, shorter course, higher completion rates, safe, DOT or SAT, greater pill burden Children >12 years of age: Recommended as equal alternative to 9 months of INH Children 2-11 years of age: Recommended as equal alternative to 9 months of INH Children <2 years of age: INH-RPT: Not recommended: Lack of safety and pharmacokinetic data in this age group Villarino E, et al JAMA Pediatr 2015; Borisov A, et al, MMWR 2018
19 Dosing: 3HP INH (100 and 300 mg tabs): Children age 2-11 years: 25 mg/kg/dose [900 mg] Children older than 12 years of age: 15 mg/kg/dose [900 mg] Rifapentine (150 mg tabs): Weight (kgs) Dose (mg) Maximum (mg) >
20 Treatment of Latent Tuberculosis Infection Rifampin for mg/kg/day (max. 600 mg) po daily for 4 months (prior recommended dose mg/kg) Acceptable regimen for LTBI treatment As effective as 9H, shorter course, better adherence, higher dose safe INH not tolerated; index patient isolate INH-resistant Cruz & Starke, (IJTLD 2014): Rifampin mg/kg/day (max. 600 mg) po daily for 4 months: Safe, completion rates similar to 9H by DOPT Gaensbauer (PIDJ 2018): No treatment failures: 395 children; welltolerated; high completion rates Diallo (NEJM 2018): Rifampin mg/kg/day for 4 months: Effective and safe as 9H
21 Treatment of Latent Tuberculosis Infection INH mg/kg (max., 300 mg) PO daily for 270 doses Efficacy approaches 100%; prevents TB meningitis Poor completion rates due to treatment length Alternative: Twice weekly directly observed (DOT) INH mg/kg (max., 900 mg) PO for 72 doses Monitor index case isolate sensitivities Hepatotoxicity from INH is rare in children: Monthly assessment for clinical evidence of hepatotoxicity should be made: malaise, loss of appetite or weight, nausea, vomiting, abdominal pain, jaundice Routine monitoring of LFTs is not indicated, except: Concurrent liver disease Pregnancy or first 12 weeks postpartum Concurrently on other hepatotoxic medications Clinical evidence of heptatoxic effects
22 Summary of contact investigations and LTBI diagnosis and treatment in the U.S.: Contact investigations use the concentric circle model and target high priority/high risk contacts first Programs need to improve the number of contacts evaluated, started on and completing LTBI treatment Diagnosis and treatment of LTBI is critical to control and elimination of TB in the U.S. Short course treatment regimens (3HP and 4R) for LTBI are safe and effective in children and should lead to increased treatment completion rates which lead to: A decrease in active disease among children following recent infection A reduction of the reservoir of LTBI from which reactivation disease may develop in the future

23
24 Tuberculosis Exposure in Children <4 years of age and Window Prophylaxis History, PE, TST/IGRA, CXR are done CXR is done regardless of TST/IGRA result IF the child is: Asymptomatic and physical examination is normal TST is negative (<5 mm) or IGRA negative Chest X-ray is normal AND IF <4 years of age START: Isoniazid (INH) 10 mg/kg (max., 300 mg) PO once daily TST/IGRA repeated 8-10 weeks after contact broken with infectious adult: If TST/IGRA (-), discontinue INH If TST/IGRA (+), re-evaluate child and treat accordingly
25 Targeted TB Testing Risk-Assessment Questionnaire Has a family member or contact had TB disease? Has a family member had a positive TB test? Was your child born in a high-risk country (i.e. outside US, Canada, Australia, New Zealand, or Western European countries) Has your child traveled to a high-risk country and spent significant time with the resident population? Red Book 2018

26 Percentage of Pediatric TB Cases by Age Group,
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Jeffrey R. Starke, M.D. has the following disclosures to make:
 AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
Tuberculosis Screening Protocol For Use In Marin County School Settings
 Tuberculosis Screening Protocol For Use In Marin County School Settings New Student no known history of positive skin test Kindergarten or First Grade entry (whichever comes first) All students, countywide,
Tuberculosis Screening Protocol For Use In Marin County School Settings New Student no known history of positive skin test Kindergarten or First Grade entry (whichever comes first) All students, countywide,
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
Santa Clara County Tuberculosis Screening Requirement for School Entrance Effective June 1, 2014
 Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Disclosures. Current Issues and Controversies in Child and Adolescent Tuberculosis 02/24/2016. NSTC 2016 Annual Meeting
 Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Contact Investigation
 Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Pediatric Tuberculosis in Los Angeles County: An Update
 Pediatric Tuberculosis in Los Angeles County: An Update Julie Higashi, MD PhD Director, Tuberculosis Control Program March 2, 2019 0 Pediatricians will be the driving force of TB elimination in California
Pediatric Tuberculosis in Los Angeles County: An Update Julie Higashi, MD PhD Director, Tuberculosis Control Program March 2, 2019 0 Pediatricians will be the driving force of TB elimination in California
Latent TB Infection Treatment
 Latent TB Infection Treatment Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulmonary/Critical Care/Occ Med UI Carver College of Medicine 2014 MFMER slide-1 Disclosures: None
Latent TB Infection Treatment Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulmonary/Critical Care/Occ Med UI Carver College of Medicine 2014 MFMER slide-1 Disclosures: None
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
Tuberculosis in Children and Adolescents 2017
 Tuberculosis in Children and Adolescents 2017 George D. McSherry, MD Division of Infectious Diseases Penn State Children s Hospital and Pediatric Section Northeastern Regional Training and Medical Consultation
Tuberculosis in Children and Adolescents 2017 George D. McSherry, MD Division of Infectious Diseases Penn State Children s Hospital and Pediatric Section Northeastern Regional Training and Medical Consultation
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Screening and Treatment Recommendations for Persons Exposed to MDR TB
 Screening and Treatment Recommendations for Persons Exposed to MDR TB Although all persons at increased risk of tuberculosis (TB) infection should be screened for TB infection per USPTF/CDC guidelines
Screening and Treatment Recommendations for Persons Exposed to MDR TB Although all persons at increased risk of tuberculosis (TB) infection should be screened for TB infection per USPTF/CDC guidelines
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Tuberculosis: Where Are We Now?
 Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
2017/2018 Annual Volunteer Tuberculosis Notice
 Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal
 Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Latent Tuberculosis in Adults: From Testing TO Treatment
 Latent Tuberculosis in Adults: From Testing TO Treatment Sergio M. Borgia, MD, MSc., FRCP(C) Infectious Diseases Consultant, WOHS Medical Director, WOHS Tuberculosis Clinic Assistant Clinical Professor,
Latent Tuberculosis in Adults: From Testing TO Treatment Sergio M. Borgia, MD, MSc., FRCP(C) Infectious Diseases Consultant, WOHS Medical Director, WOHS Tuberculosis Clinic Assistant Clinical Professor,
Isoniazid Preventive Therapy (IPT)
") Isoniazid Preventive Therapy (IPT) Josefina Cadorna-Carlos, M.D. Professor of Pediatrics U E R M M M C Objectives 1. Define IPT. 2. Discuss the indications for IPT. 3. Present RCT s for IPT (6H vs 9H).
Isoniazid Preventive Therapy (IPT) Josefina Cadorna-Carlos, M.D. Professor of Pediatrics U E R M M M C Objectives 1. Define IPT. 2. Discuss the indications for IPT. 3. Present RCT s for IPT (6H vs 9H).
Utilizing All the Tools in the TB Toolbox
 Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
INDEX CASE INFORMATION
 Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
11/1/2017. Disclosures. Update In Tuberculosis, Indiana Outline/Objectives. Pathogenesis of M.tb Global/U.S. TB Burden, 2016
 Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Communicable Disease Control Manual Chapter 4: Tuberculosis. Assessment and Follow-Up of TB Contacts
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Assessment and Follow-Up of TB July, 2018 Page 1 TABLE OF CONTENTS 8.0 ASSESSMENT AND
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Assessment and Follow-Up of TB July, 2018 Page 1 TABLE OF CONTENTS 8.0 ASSESSMENT AND
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
TUBERCULOSIS CONTACT INVESTIGATION
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Latent tuberculosis infection
 EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
New Standards for an Old Disease:
 New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION
 TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
Preventing TB: Recent Research Results and Novel Short Course Therapy for LTBI
 Preventing TB: Recent Research Results and Novel Short Course Therapy for LTBI Constance A. Benson, M.D. Professor of Medicine Director, UCSD AntiViral Research Unit PI, CD4 Collaborative HIV Clinical
Preventing TB: Recent Research Results and Novel Short Course Therapy for LTBI Constance A. Benson, M.D. Professor of Medicine Director, UCSD AntiViral Research Unit PI, CD4 Collaborative HIV Clinical
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Sharing the Care: Working Together on LTBI Treatment and Management Webinar. September 24, Curry International Tuberculosis Center
 TB Infection Diagnostics and Treatment Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention 1 Curry International
TB Infection Diagnostics and Treatment Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention 1 Curry International
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
LTBI: Who to Test & When to Treat
 LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Tuberculosis Exposure, Infection, and Disease Among Children with Medical Comorbidities
 Tuberculosis Exposure, Infection, and Disease Among Children with Medical Comorbidities Andrea T. Cruz, MD, MPH, Omar Merchant, Affan Zafar, and Jeffrey R. Starke, MD Department of Pediatrics February
Tuberculosis Exposure, Infection, and Disease Among Children with Medical Comorbidities Andrea T. Cruz, MD, MPH, Omar Merchant, Affan Zafar, and Jeffrey R. Starke, MD Department of Pediatrics February
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015
 Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 Initiation Phase Part 1 Ginny Dowell, RN, BSN February 4, 2015 Ginny Dowell RN, BSN has the following disclosures to make:
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 Initiation Phase Part 1 Ginny Dowell, RN, BSN February 4, 2015 Ginny Dowell RN, BSN has the following disclosures to make:
Disclosures. Public Health Motivation 6/6/2012. The 12-Dose INH-Rifapentine Once-Weekly DOT Regimen: What Next?
 The 12-Dose INH-Rifapentine Once-Weekly DOT Regimen: What Next? NTCA Conference June 14, 2012 John Jereb, FSEB, DTBE, CDC Special thanks to Christine Ho, Elsa Villarino, and Andrey Borisov The findings
The 12-Dose INH-Rifapentine Once-Weekly DOT Regimen: What Next? NTCA Conference June 14, 2012 John Jereb, FSEB, DTBE, CDC Special thanks to Christine Ho, Elsa Villarino, and Andrey Borisov The findings
Pediatric Tuberculosis: The Essentials October 8, 2014
 Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
TB Contact Investigation
 Ann Raftery, RN, PHN, MS Curry International TB Center Overview Contact investigation as a core TB control and elimination activity Components of TB Contact Investigation TB Control Priority Strategies.
Ann Raftery, RN, PHN, MS Curry International TB Center Overview Contact investigation as a core TB control and elimination activity Components of TB Contact Investigation TB Control Priority Strategies.
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Ongoing Research on LTBI and Research priorities in India
 Ongoing Research on LTBI and Research priorities in India Dr. C.Padmapriyadarsini, MD, MS ICMR-National Institute for Research in Tuberculosis Chennai, India Technical Consultation Meeting on Programmatic
Ongoing Research on LTBI and Research priorities in India Dr. C.Padmapriyadarsini, MD, MS ICMR-National Institute for Research in Tuberculosis Chennai, India Technical Consultation Meeting on Programmatic
Latent TB Infection (LTBI) Strategies for Detection and Management
 Strategies for Detection and Management") Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Michael J. Huey, MD. NYSCHA Annual Meeting WE-2, October 19, 2016
 Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
Disclosures. Outline. No disclosures or conflicts of interest to report. Special LTBI situations. H t it d id ff t
 Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Programmatic management of LTBI : a two pronged approach for ending the TB epidemic. Haileyesus Getahun Global TB Programme WHO/HQ
 Programmatic management of LTBI : a two pronged approach for ending the TB epidemic Haileyesus Getahun Global TB Programme WHO/HQ What is latent TB infection? A state of persistent immune response to stimulation
Programmatic management of LTBI : a two pronged approach for ending the TB epidemic Haileyesus Getahun Global TB Programme WHO/HQ What is latent TB infection? A state of persistent immune response to stimulation
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges
 Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges David Karol, MD, MA Bureau of Prisons, FMC Butner Duke University Medical Center June 26, 2013 No Disclosures
Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges David Karol, MD, MA Bureau of Prisons, FMC Butner Duke University Medical Center June 26, 2013 No Disclosures
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Ian Kitai TB Specialist. Division of Infectious Diseases Sickkids
 Ian Kitai TB Specialist Division of Infectious Diseases Sickkids Review Clinical presentation of TB disease childhood How to assess risk for TB infection How to assess risk for disease if infected TST
Ian Kitai TB Specialist Division of Infectious Diseases Sickkids Review Clinical presentation of TB disease childhood How to assess risk for TB infection How to assess risk for disease if infected TST
A Mobile Health Intervention Utilizing Community Partnership to Improve Access to Latent Tuberculosis Infection Treatment
 A Mobile Health Intervention Utilizing Community Partnership to Improve Access to Latent Tuberculosis Infection Treatment Cassandra Garcia, MSN, RN, FNP-BC Mobile Clinic Provider Texas Children s Mobile
A Mobile Health Intervention Utilizing Community Partnership to Improve Access to Latent Tuberculosis Infection Treatment Cassandra Garcia, MSN, RN, FNP-BC Mobile Clinic Provider Texas Children s Mobile
TB Classification (ATS/CDC)
") bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
Screening and management of latent TB Infection Gerry Davies
 Screening and management of latent TB Infection Gerry Davies Reader in Infection Pharmacology Institutes of Infection and Global Health & Translational Medicine HIV Scientific Meeting Liverpool 21st July
Screening and management of latent TB Infection Gerry Davies Reader in Infection Pharmacology Institutes of Infection and Global Health & Translational Medicine HIV Scientific Meeting Liverpool 21st July
The Epidemiology of Tuberculosis in Minnesota,
 The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available