Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE
|
|
|
- Cori Parrish
- 5 years ago
- Views:
Transcription

1 Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE
2 Objectives l Recognize that tuberculosis as a chronic disease mainly affecting the respiratory system. l Know the epidemiology of tuberculosis world wide and in the kingdom of Saudi Arabia. l Understand the methods of transmission of tuberculosis and people at risk.
3 Objectives l Know the causative agents, their characteristic and staining methods. l Understand the pathogenesis of tuberculosis. l Differentiate between primary and secondary tuberculosis and the clinical features of each.
4 Objectives l Understand the method of tuberculin skin test and result interpretation. l Know the laboratory diagnostic methods. l Know the chemotherapeutic agents and other methods of management. l Describe the methods of prevention and control of tuberculosis
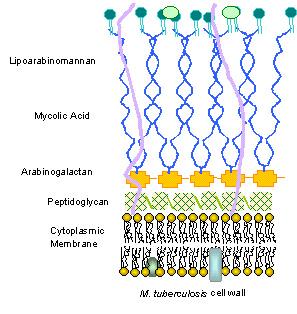
5 Characteristics of the Genus Mycobacteria Ø Slim, rod shaped, non-motile, do not form spores. Ø Do not stain by Gram stain. Why? Ø Cell wall contains high lipid concentration (Mycolic acid ) which resists staining by Gram stain. Ø Acid- Alcohol Fast Bacilli (AFB) : resist decolorization with up to 3% HCL, 5% ethanol or both.
6
7 Acid-Fast Bacilli (AFB) Ø Stains used : Ziehl-Neelsen stain (ZN stain) and Auramine Rhodamine stain. Ø Strict aerobes Ø Multiply intracellularily Ø Cause delayed hypersensitivity reaction type of immune response Ø Slowly growing ( between 2-8 wks.)
8

9
 cause infections in immunosuppressed patients.")
10 Species of Mycobacteria l Mycobacterium tuberculosis complex cause tuberculosis. l Mycobacterium leprae causes leprosy. l Atypical Mycobacteria / Mycobacteria other than tuberculosis ( MOTT) cause infections in immunosuppressed patients.
11 Mycobacterium tuberculosis complex 1- M.tuberculosis (Human type) 2- M. bovis (Bovine type) 3- M. Africanum 4- BCG strains All are called Mycobacterium tuberculosis complex and cause tuberculosis in human
12 Tuberculosis l Tuberculosis (TB) is an ancient chronic disease affects humans, caused by Mycobacterium tuberculosis complex. l A major cause of death worldwide. l Usually affects the lungs, other organs can be affected in one third of cases. l If properly treated is curable, but fatal if untreated in most cases.
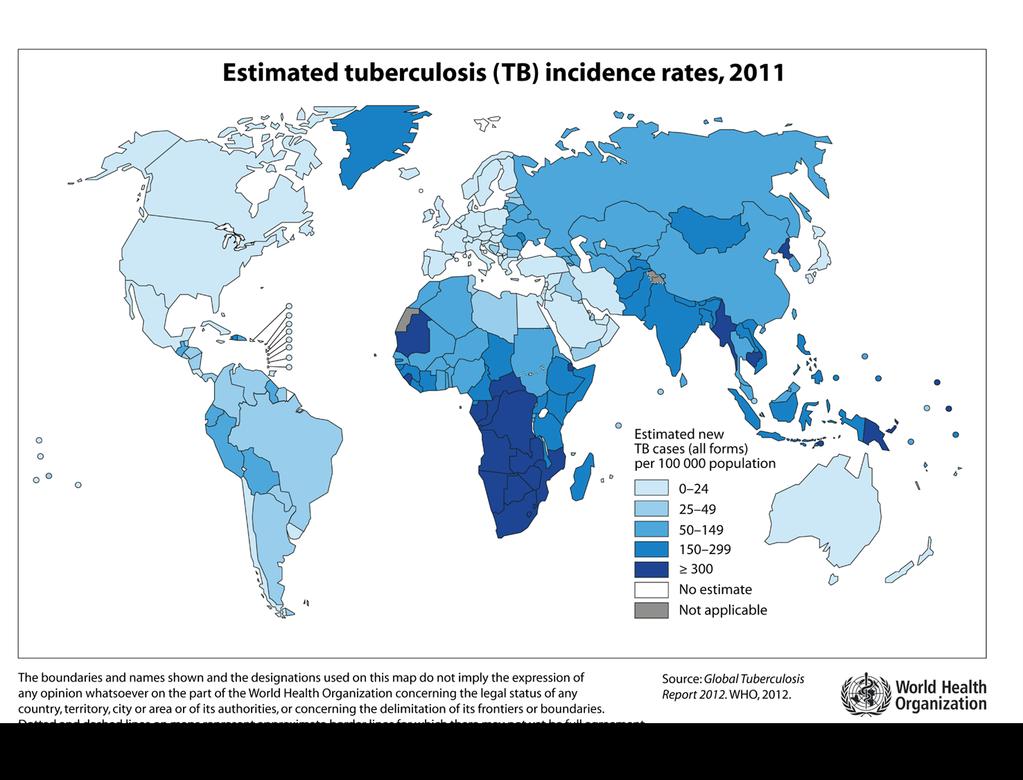
13 Epidemiology Ø TB affects 1/3 of human race as a latent dormant tuberculosis. Ø WHO estimated 8.9 million new cases and 2-4 million death in 2014 Ø Incidence: a world wide disease, more common in developing countries ( see diagram). Ø Affects all age groups who are subject to get the infection. Ø
14
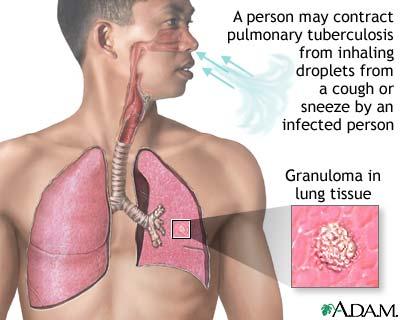
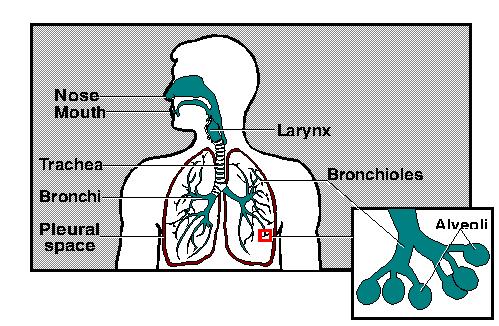
15 Epidemiology Ø Transmission mainly through inhalation of airborne droplet nuclei ( < 5 µm) in pulmonary diseases cases, rarely through GIT & skin Ø Reservoir: patients with open TB. Ø Age: young children & adults Ø People at risk : include ;lab technicians, immunosuppressed patients,workers in mines and contacts with index case.
16 Pathogenesis of Tuberculosis l Mycobacteria is acquired by airborne droplet which reach the alveolar macrophages and are able to survive their (main virulence factor). l Simulates cell mediated immune response which controls the multiplication of the organism but does not kill it. l Granuloma formed and organism lives in dormant state ( latent tuberculosis infection)
17 Pathogenesis of TB
18 Pathogenesis of Tuberculosis l Patient show evidence of delayed cell mediated immunity ( CMI ). l Disease results due to destructive effect of CMI. l Clinically the disease is divided into primary or secondary.
19 Pathogenesis of Tuberculosis Ø Primary Tuberculosis Occurs in patients not previously infected. Inhalation of bacilli Phagocytosis lymph nodes calcify to produce GHON Focus (or Primary Complex) at the periphery of mid zone of lung.
20
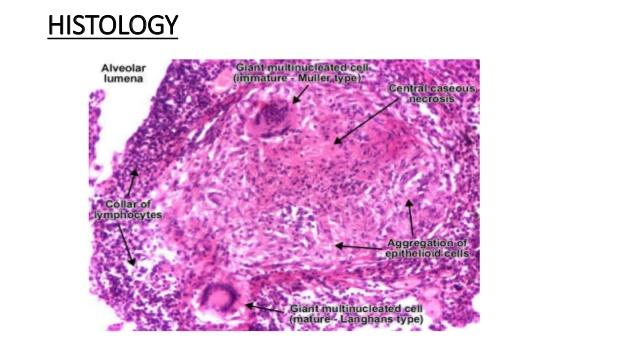
21 Primary Tuberculosis Ø Microscopy of lesion shows Granuloma. Ø Clinically: primary TB usually asymptomatic or / minor illness. Ø Non-pulmonary TB: may spreads from pulmonary infections to other organs eg.: TB of lymph nodes ( cervical, mesenteric). TB meningitis TB bone & joint
22 Primary Tuberculosis Ø Genitourinary TB Ø Miliary TB (blood) Ø Soft tissue (cold abscess): lack of inflammation with caseation. Caseation: due to delayed hypersensitivity reaction. Contains many bacilli,enzymes, O 2,N 2 intermediates, necrotic center of granuloma (cheezy material).
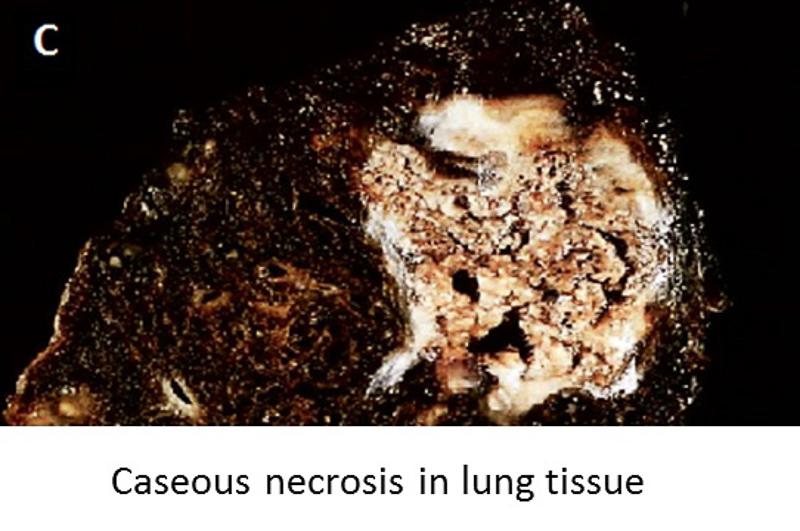
23 CASEATION
")
24 Secondary TB (reactivation) Ø Occurs later in life Ø Lung more common site Ø Immunocompromised patients. Ø Lesion localized in apices Ø Infectious & symptomatic Ø Microscopy: many bacilli, large area of caseous necrosis cavity (open TB) with granuloma and caseation.
25 Secondary TB Ø Clinically: fever, cough, hemoptysis,weight loss & weakness. Sources of secondary TB : - Endogenous (reactivation of an old TB) or - Exogenous (re-infection with new strain)
26 Immunity to Tuberculosis Ø CMI associated with delayed hypersensitivity reaction. Ø Detected by tuberculin skin test. Ø Tuberculin test takes 2-10 weeks to react to tuberculin and becomes positive.
27 Tuberculin Test Ø Uses purified protein derivative (PPD). Ø Activity expressed by Tuberculin unit. Ø Activates synthesized lymphocytes to produce CMI which appear as skin induration. Ø May not distinguish between active and past infection except in an individual with recent contact with infected case. Ø Low level activity induced by environmental mycobacteria.
, 5 tuberculin units.")
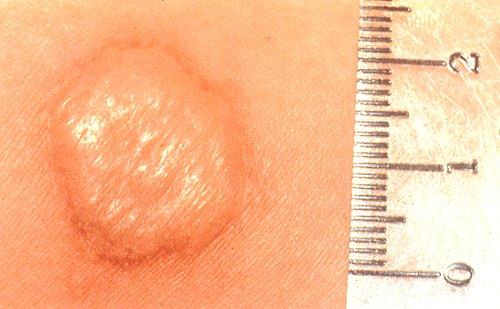
28 Method of Tuberculin Skin Test Mantoux test: Ø Intradermal inoculation of 0.1 ml of PPD ( purified protein derivative), 5 tuberculin units. Ø Read after 48-72hrs.
29 Positive Tuberculin Skin Test Ø >5mm induration : Recent contact with active TB. HIV or high risk for HIV Chest X-ray consistent with healed TB. Organ transplant Ø > 10mm induration: IV drugs user, HIV seronegative patient. Medical conditions eg. diabetes, malignancy.
30 Positive Tuberculin Test Residents & employee at high risk Patients from country with high incidence. Children < 4yrs or exposed to adult high risk group. Mycobacteriology lab. personnel. Ø >15 mm induration: Considered positive in any persons including those with no risk factors for TB.

31

32 Summary interpretation of positive tuberculin test
33 Negative Tuberculin Skin Test Ø No induration, either due to: No previous infection Pre-hypersensitivity stage Lost TB sensitivity with loss of antigen. Ø AIDS patients are anergic and susceptible to the infection.
34 Laboratory Diagnosis of TB specimens: ØPulmonary TB: Three early morning sputum samples,or bronchial lavage, or gastric washing (infants). Ø Cerebrospinal fluid ( CSF) ( TB meningitis) Ø Three early morning urine Ø Bone, joint aspirate Ø Lymph nodes, pus or tissues NOT swab. Repeat sample as required.
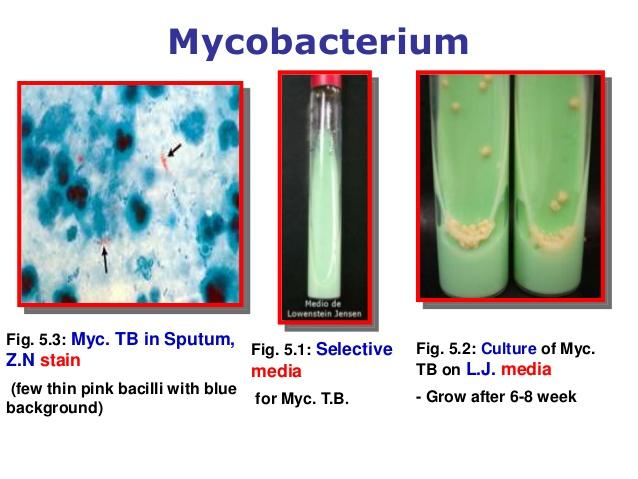
35 Laboratory Diagnosis of TB Direct microscopy of specimen : Z-N or (Auramine ) stain. Culture is the gold standard. Important for identification and sensitivity. Media used: Lowenstein-Jensen media (L J). Contains: eggs, asparagine, glycerol, pyruvate / malachite green.
36 Laboratory Diagnosis of TB Colonies appear in LJ media after 2-8 weeks as eugenic, raised, buff, adherent growth enhanced by glycerol (MTB) or by pyruvate (M.bovis). Ø Other media and methods plus LJ media used,eg: Automated methods : Bactec MGIT ( Mycobacterium Growth Indicator Test). Measurement of interferon -gamma release assay ( IF-γ) : positive in latent TB. Molecular methods : eg. ProbTech detects nucleic acid directly from respiratory samples. Xpert MTB/RIF detects nucleic acid and resistance to rifampicin
37

38 Growth of MTB on LJ media
39 Identification & Susceptibility Testing Ø Morphological characteristics, growth at 37C % CO 2 Ø Biochemical tests : Niacin production & Nitrate test. Ø Susceptibility testing: to detect resistance to anti-tuberculosis agents.
40 Management of a TB case Ø Isolation of the patient for days (smear positive cases contain > 1000 organisms / ml of sputum and considered infectious). Ø Triple regimen of therapy.why? To prevent resistant mutants To prevent relapse Ø Treatment must be guided by sensitivity testing.
41 First Line Treatment Ø Isoniazide Ø Rifampicin Ø Ethmbutol (INH) (RIF) (E) Ø Pyrazinamide (P) Ø Streptomycin (S) Combination therapy :INH+ RIF +P for 2 months then continue with INH+RIF for 4-6 months. Ø Directly Observed Therapy (DOT).
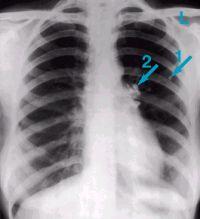
 Chest X-ray of the same patient 10 months after antituberculous therapy. (Courtesy of Dr.")
42 Tuberculosis: (a) Chest X-ray of a patient with tuberculosis bronchopneumonia. (b) Chest X-ray of the same patient 10 months after antituberculous therapy. (Courtesy of Dr. R.S.Kennedy)
43 Second Line Used for the bacteria resistant to first line drugs. More toxic than the first line drugs. Ø PAS ( Para-Amino Salicylic acid) Ø Ethionamide Ø Cycloserine, Ø Kanamycin, Ø Fluroquiolones
44 Prevention of TB Ø Tuberculin testing of herds. Ø Slaughter of infected animals. Ø Pasteurization of milk to prevent bovine TB Ø Recognition of new cases. Ø Prophylaxis with INH of contacts. Ø Follow up cases. Ø Immunization with BCG ( live attenuated ) to all new borne.
45 Reference book Ryan, Kenneth J.. Sherris Medical Microbiology, Latest Edition. McGraw-Hill Education.
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
Mycobacterium tuberculosis. Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology
 Dr.Baha, AL-Amiedi Ph. D.Microbiology") Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Medical Bacteriology- Lecture 10. Mycobacterium. Actinomycetes. Nocardia
 Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
MYCOBACTERIA. Pulmonary T.B. (infect bird)
") MYCOBACTERIA SPP. Reservoir Clinical Manifestation Mycobacterium tuberculosis Human Pulmonary and dissem. T.B. M. lepra Human Leprosy M. bovis Human & cattle T.B. like infection M. avium Soil, water, birds,
MYCOBACTERIA SPP. Reservoir Clinical Manifestation Mycobacterium tuberculosis Human Pulmonary and dissem. T.B. M. lepra Human Leprosy M. bovis Human & cattle T.B. like infection M. avium Soil, water, birds,
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Medical Bacteriology- lecture 13. Mycobacterium Actinomycetes
 Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Mycobacteriaceae
 Mycobacteriaceae 9.04.2018 1 Classification Kingdom: Bacteria Phylum: Actinobacteria Order: Actinomycetales Family: Mycobacteriaceae Genus: Mycobacterium 9.04.2018 2 The properties of Mycobacterium genus
Mycobacteriaceae 9.04.2018 1 Classification Kingdom: Bacteria Phylum: Actinobacteria Order: Actinomycetales Family: Mycobacteriaceae Genus: Mycobacterium 9.04.2018 2 The properties of Mycobacterium genus
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS. Famous victims in their intellectual prime: Chopin, Paganini, Thoreau, Keats, Elizabeth Browning, Brontës
 TUBERCULOSIS GENERAL Tuberculosis (TB) kills 1,700,000 annually worldwide. "The Captain of all the men of death that came to take him away was the consumption, for it was that which brought him down to
TUBERCULOSIS GENERAL Tuberculosis (TB) kills 1,700,000 annually worldwide. "The Captain of all the men of death that came to take him away was the consumption, for it was that which brought him down to
MYCOBACTERIUM. Mycobacterium Tuberculosis (Mtb) nontuberculous mycobacteria (NTM) Mycobacterium lepray
 nontuberculous mycobacteria (NTM) Mycobacterium lepray") MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
PEDIATRIC TB. Modified PPT from group A seminar (F)
") PEDIATRIC TB Modified PPT from group A seminar (F) objectives the epidemiology of pediatric TB. TB Mycobacteriology. pediatric TB presentations compared to adults TB. Know the differences between, and
PEDIATRIC TB Modified PPT from group A seminar (F) objectives the epidemiology of pediatric TB. TB Mycobacteriology. pediatric TB presentations compared to adults TB. Know the differences between, and
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
number Done by Corrected by Doctor Hamid Al Zoubi
 number 15 Done by أبو عجمي ة مها Corrected by Waseem Abu Obeida Doctor Hamid Al Zoubi In case you don t know - (Bacillus = rod) and (bacilli = rods) - hypersensitivity tests can be either immediate (within
number 15 Done by أبو عجمي ة مها Corrected by Waseem Abu Obeida Doctor Hamid Al Zoubi In case you don t know - (Bacillus = rod) and (bacilli = rods) - hypersensitivity tests can be either immediate (within
TB Laboratory for Nurses
 TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
Tuberculosis. Impact of TB. Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH)
") Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
MO TASEM AJ Nader Alaridah
 22 MO TASEM AJ...... Nader Alaridah Mycobacterium ** Mycobacterium is a class of Actinobacteria, which are non-spore forming, non-motile and acid-fast bacilli ( they remain stained with the red dye carbofuchsin
22 MO TASEM AJ...... Nader Alaridah Mycobacterium ** Mycobacterium is a class of Actinobacteria, which are non-spore forming, non-motile and acid-fast bacilli ( they remain stained with the red dye carbofuchsin
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Frances Morgan, PhD October 21, Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS
 The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Mycobacteriology William H. Benjamin, Jr.
 Mycobacteriology William H. Benjamin, Jr. William H. Benjamin, PhD Department of Pathology UAB 1 Mycobacteria sp. Acid Fast Bacilli (AFB) Mycolic acids (C78-91) Waxes Obligate aerobes Slow growing days
Mycobacteriology William H. Benjamin, Jr. William H. Benjamin, PhD Department of Pathology UAB 1 Mycobacteria sp. Acid Fast Bacilli (AFB) Mycolic acids (C78-91) Waxes Obligate aerobes Slow growing days
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Respiratory System الفريق الطبي االكاديمي
 Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
HISTORY TB = 25% ADULT DEATHS EGYPTIAN MUMMIES: SPINAL TB. 17 th -18th CENTURIES- URBANIZATION MID 24
 HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS
HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
A retrospective evaluation study of diagnostic accuracy of Xpert MTB/RIF assay, used for detection of Mycobacterium tuberculosis in Greece
 Örebro University School of Health and Medical Science Biomedical Laboratory Science Programme 180 credits Degree project in biomedical laboratory science, advanced course, 15 credits May 21, 2015 A retrospective
Örebro University School of Health and Medical Science Biomedical Laboratory Science Programme 180 credits Degree project in biomedical laboratory science, advanced course, 15 credits May 21, 2015 A retrospective
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Mycobacterial cell wall. Cell Cycle Lengths. Outline of Laboratory Methods. Laboratory Methods
 Laboratory Methods Cell Cycle Lengths Generation time (hrs) Days needed for 26 generations (colony) E. coli 0.33 0.36 Nancy Connell, PhD Professor, nfectious Disease Department of Medicine Center for Emerging
Laboratory Methods Cell Cycle Lengths Generation time (hrs) Days needed for 26 generations (colony) E. coli 0.33 0.36 Nancy Connell, PhD Professor, nfectious Disease Department of Medicine Center for Emerging
HISTORY TB = 25% ADULT DEATHS MID 24 PRE-ANTIBIOTIC ERA
 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
Order: Actinomycetales. Family: Mycobactericeae. Some are parasitic to cold blooded animal, others are saprophytic in nature.
 Order: Actinomycetales Family: Mycobactericeae They are widely distributed in nature. Few no is pathogenic for man & animal. Some are parasitic to cold blooded animal, others are saprophytic in nature.
Order: Actinomycetales Family: Mycobactericeae They are widely distributed in nature. Few no is pathogenic for man & animal. Some are parasitic to cold blooded animal, others are saprophytic in nature.
TB/HIV 2 sides of the same coin. Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai
 TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LESSON ASSIGNMENT. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 6 Tuberculosis. TEXT ASSIGNMENT Paragraphs 6-1 through 6-11. LESSON OBJECTIVES After completing this lesson, you should be able to: 6-1. Identify the characteristics, signs/ symptoms,
LESSON ASSIGNMENT LESSON 6 Tuberculosis. TEXT ASSIGNMENT Paragraphs 6-1 through 6-11. LESSON OBJECTIVES After completing this lesson, you should be able to: 6-1. Identify the characteristics, signs/ symptoms,
Chapter 4 Diagnosis of Tuberculosis Disease
 Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
TB 101 Disease, Clinical Assessment and Lab Testing
 TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit
 MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit Topics to be covered What is Tuberculosis? TB bacteria and what is unique about it. How is TB different from HIV? How is TB
MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit Topics to be covered What is Tuberculosis? TB bacteria and what is unique about it. How is TB different from HIV? How is TB
TOG The Way Forward
 TOG 2016- The Way Forward Main Changes in Diagnostic algorithm Definition (Type, Classification, Outcome) Registration at the time of Diagnosis (PHI level Notification Register) Long term follow up (till
TOG 2016- The Way Forward Main Changes in Diagnostic algorithm Definition (Type, Classification, Outcome) Registration at the time of Diagnosis (PHI level Notification Register) Long term follow up (till
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
Transmission and Pathogenesis of Tuberculosis. Transmission and Pathogenesis of Tuberculosis. Mycobacteria. Introduction to the pathogen Transmission
 Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Assistant Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Assistant Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Transmission and Pathogenesis of Tuberculosis
 Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Associate Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Associate Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Ken Jost, BA, has the following disclosures to make:
 Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Why need to havetb Clearance. To Control and Prevent Tuberculosis
 Why need to havetb Clearance To Control and Prevent Tuberculosis How to ID Tuberculosis There are two kinds of tests that are used to determine if a person has been infected with TB bacteria: the tuberculin
Why need to havetb Clearance To Control and Prevent Tuberculosis How to ID Tuberculosis There are two kinds of tests that are used to determine if a person has been infected with TB bacteria: the tuberculin
TB, BCG and other things. Chris Conlon Infectious Diseases Oxford
 TB, BCG and other things Chris Conlon Infectious Diseases Oxford Epidemiology Latent TB IGRA BCG >50/100000
TB, BCG and other things Chris Conlon Infectious Diseases Oxford Epidemiology Latent TB IGRA BCG >50/100000
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
56% of these were in south east Asia and west pacific region.
 Tuberc ulosis Dr. ASAAD FARHAN ASSIST. PROF.PEDS. Learning objectives epidemiology Tuberculosis remains worlds deadliest communicable disease. TB is present in all regions of the world. WHO estimates that
Tuberc ulosis Dr. ASAAD FARHAN ASSIST. PROF.PEDS. Learning objectives epidemiology Tuberculosis remains worlds deadliest communicable disease. TB is present in all regions of the world. WHO estimates that
Tuberculosis 6/7/2018. Objectives. What is Tuberculosis?
 Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Antimycobacterial drugs. Dr.Naza M.Ali lec Dec 2018
 Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
HIV prevalance in TB cases
 TUBERCULOSIS HIV prevalance in TB cases Top 5 AIDS indicative diseases; EUR, 2003 58% 35% 25% 11% 7% TB HIV wasting s. Candidiasis Rec. pneumonia HIV encephal. 26% 25% 31% 31% 16% 8% 7% 16% 14% 10% TB
TUBERCULOSIS HIV prevalance in TB cases Top 5 AIDS indicative diseases; EUR, 2003 58% 35% 25% 11% 7% TB HIV wasting s. Candidiasis Rec. pneumonia HIV encephal. 26% 25% 31% 31% 16% 8% 7% 16% 14% 10% TB
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Laboratory Diagnostic Techniques. Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust
 Laboratory Diagnostic Techniques Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust Learning Objectives 1) When to consider a diagnosis of TB 2) When to consider a referral
Laboratory Diagnostic Techniques Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust Learning Objectives 1) When to consider a diagnosis of TB 2) When to consider a referral
Public Health Mycobacteriology (TB) Laboratory Testing Services
 Laboratory Testing Services") Public Health Mycobacteriology (TB) Laboratory Testing Services Gary Budnick Supervising Microbiologist Connecticut Department of Public Health Laboratory Branch Hartford, Connecticut Specimen Collection
Public Health Mycobacteriology (TB) Laboratory Testing Services Gary Budnick Supervising Microbiologist Connecticut Department of Public Health Laboratory Branch Hartford, Connecticut Specimen Collection
TB infection control: overview and importance
 TB infection control: overview and importance John Ferguson, Newcastle, NSW Infectious Diseases & Microbiology jferguson@hnehealth.nsw.gov.au Goroka Hospital, September 2014 Patterns of TB disease Latent
TB infection control: overview and importance John Ferguson, Newcastle, NSW Infectious Diseases & Microbiology jferguson@hnehealth.nsw.gov.au Goroka Hospital, September 2014 Patterns of TB disease Latent
The ABC s of AFB s Laboratory Testing for Tuberculosis. Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory
 The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!!
 Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Learning Objectives: Case 1 11/12/2015. Tuberculosis: Focus on Transmission and Pathogenesis. TB: Some Important Terms
 A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
Tuberculosis Part 1. Some useful truths
 Tuberculosis Part 1 Some useful truths Tuberculosis will be dealt with in detail in chapter 9 in a few week s time when we deal with the air borne bacterial diseases and the diseases of the lower respiratory
Tuberculosis Part 1 Some useful truths Tuberculosis will be dealt with in detail in chapter 9 in a few week s time when we deal with the air borne bacterial diseases and the diseases of the lower respiratory
HISTORY TB = 25% ADULT DEATHS PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA
 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
INDUSTRIALIZATION TB = 25% ADULT DEATHS
 HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS 1 GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM
HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS 1 GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
TB: A Supplement to GP CLINICS
 TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Tuberculosis. New TB diagnostics. New drugs.new vaccines. Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012
 Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally