RECENT ADVANCES OF TUBERCULOSIS MANAGEMENT. Qais Abdulmajeed Haddad Consultant ID & IC Security Forces Hospital Program Riyadh - Saudi Arabia
|
|
|
- Caitlin Daniel
- 6 years ago
- Views:
Transcription
1 RECENT ADVANCES OF TUBERCULOSIS MANAGEMENT Qais Abdulmajeed Haddad Consultant ID & IC Security Forces Hospital Program Riyadh - Saudi Arabia
2 RECENT ADVANCES OF TUBERCULOSIS MANAGEMENT History Epidemiology Latent Tuberculosis Diagnosis Therapy Vaccine Infection Control Future Trends

3 1.5 m/year = 4110/day
4


5 Pulmoary Tuberculosis Extrapulmoary Tuberculosis TB Pleural effusion Tuberculous meningitis CNS Tuberculoma Milliary tuberculosis Renal & urogenital tuberculosis Bone & joint tuberculosis GIT tuberculosis TB Peritonitis Ileocecal TB Colonic TB Hepatic TB TB retinitis

6 Tuberculosis History Spinal TB After 1850 Laennec Neolithic skeleton (stone age) Pre-Columbian skeleton Early Egyptian remains Pulmonary & Extrapulmonary tuberculosis is one disease 1865 F. Villemin Tuberculosis transmitted to guinea pig by injecting diseased tissue 1882 Koch AFB & its pathogenicity
7 TB History Timeline 1993: TB cases decline due to increased funding and enhanced TB control efforts 1865: Jean-Antoine Villemin proved TB is contagious 1884: First TB sanatorium established in U.S. 1943: Streptomycin (SM) a drug used to treat TB is discovered Mid-1970s: Most TB sanatoriums in U.S. closed : Robert Koch discovers M. tuberculosis : Two more drugs are discovered to treat TB: INH and PAS Mid-1980s: Unexpected rise in TB cases Rifampicin introduced 1967
8 M. tuberculosis causes most TB cases in the world Mycobacteria that cause TB: M. tuberculosis M. bovis M. africanum M. microti M. canetti Types of Mycobacteria Mycobacteria that do not cause TB (NTM) e.g., M. avium complex, M. chelonae

9 TB TRANSMISSION Dots in air represent droplet nuclei containing M. tuberculosis
10 TB Transmission Probability that TB will be transmitted depends on: Infectiousness of person with TB disease Environment in which exposure occurred Length of exposure Virulence (strength) of the tubercle bacilli The best way to stop transmission is to: Isolate infectious persons Provide effective treatment to infectious persons as soon as possible
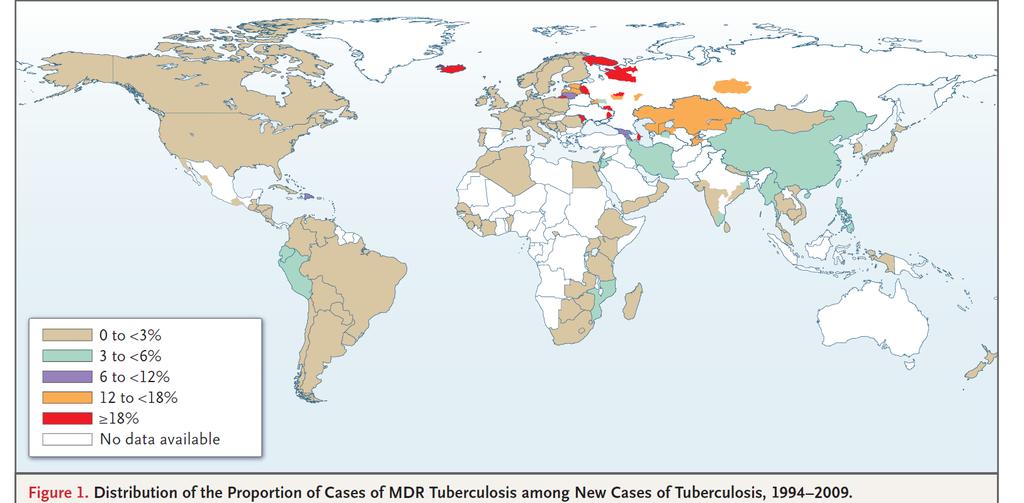
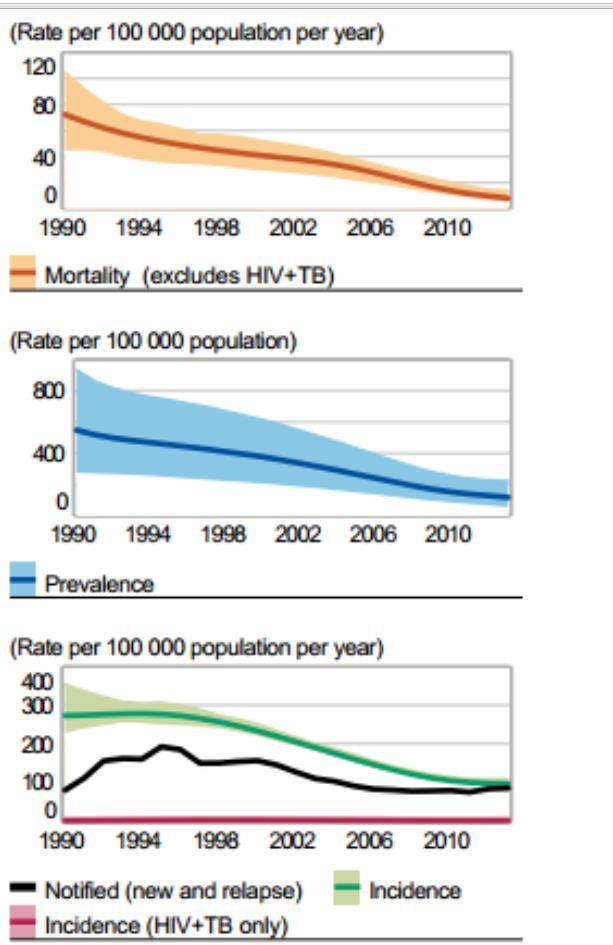
11 WHO Global TB Report 2014 Incidence: 9 million (2013) 95% occurs in low- and middle-income countries Alarming increase in the number of patients with MDR-TB and XDR-TB has been noted (East Europe & Africa) Globally, 45% drop in mortality between 1990 & 2012 Mortality: 1.5 million / year 0.5 million are children HIV co-infection with TB: 360,000 deaths / year 13% of total active TB infections

12 RR-TB (Rifampicin Resistant) MDR-TB (INH+Rifampicin Resistant)
13
14 Latent Tuberculosis
15 LTBI VS. TB DISEASE Latent TB Infection (LTBI) Inactive, contained tubercle bacilli in the body TST or blood test usually positive Chest x-ray usually normal Sputum smears and cultures negative No symptoms Not infectious Not a case of TB TB Disease (in the lungs) Active, multiplying tubercle bacilli in the body TST or blood test usually positive Chest x-ray usually abnormal Sputum smears and cultures may be positive Symptoms such as cough, fever, weight loss Often infectious before Rx A case of TB
16
17 PPD VS IGRA Latent TB infection (LTBI) diagnosis remained to be dependent on PPD (Mantoux test) which was first described by Robert Koch in 1890 PPD needs two patient visits and liable for observer error in reading Interferon-Gamma Release Assays (IGRAs) are whole-blood tests that can aid in diagnosing LTBI with one patient visit
18 Initial Process QFT-TB Gold T-Spot Process whole blood within 16 hours Process peripheral blood mononuclear cells (PBMCs) within 8 hours, or if T-Cell Xtend is used, within 30 hours M. Tuberculosis Antigen Single mixture of synthetic peptides representing ESAT-6, CFP-10 & TB7.7. Separate mixtures of synthetic peptides representing ESAT-6 & CFP-10 Measurement IFN-g concentration Number of IFN-g producing cells (spots) Possible Results Positive, negative, indeterminate Positive, negative, indeterminate, borderline
19
20
21 Isoniazid VS Isoniazid + Rifapentine Rates of Treatment completion Isoniazid only Isoniazid + Rifapentine P Value 69% 82% <0.001 Drug Discontinuation 3.7% 4.9% Doses
22
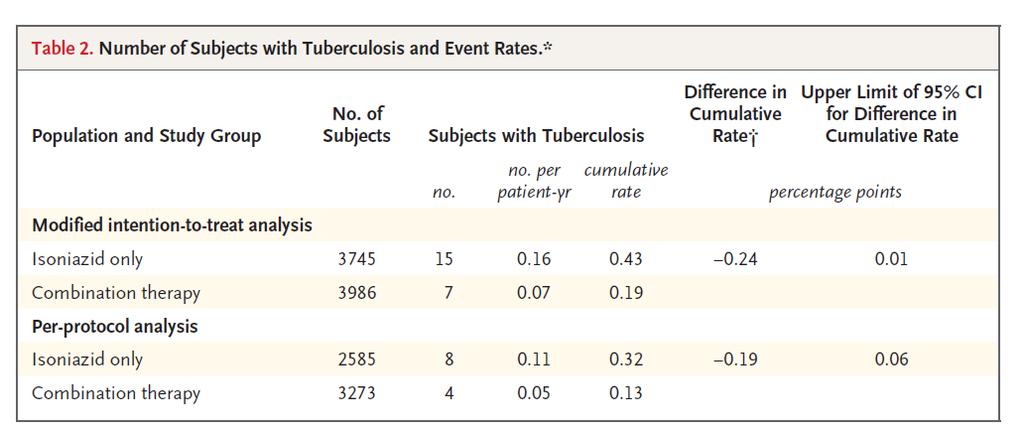
23 1148 patients had a median age of 30 years and a median CD4 cell count of 484/ml This was an open-label, randomized trial of LTBI in HIV patients (PPD 5mm or more) Divided in 4 blocks 2:2:2:1 rifapentine (900 mg) plus isoniazid (900 mg) once weekly for 12 weeks Rifampin (600 mg) plus isoniazid (900 mg) twice weekly for 12 weeks Isoniazid (300 mg) daily for duration of the study ( 6 yrs) Control regimen of isoniazid (300 mg) daily for 6 months
24 Conclusions The use of rifapentine plus isoniazid for 3 months was as effective as 9 months of isoniazid alone in preventing tuberculosis and had a higher treatment completion rate Neither a 3-month course of intermittent rifapentine or rifampin with isoniazid nor continuous isoniazid was superior to 6 months of isoniazid
25
26 A Trial of Mass Isoniazid Preventive Therapy for Tuberculosis Control In the intervention clusters, 27,126 miners (66.2%) underwent screening. Of these miners, 23,659 (87.2%) started taking isoniazid for 9 months If active tuberculosis was diagnosed, they were referred for treatment Conclusions: Mass screening and treatment for latent tuberculosis had no significant effect on tuberculosis control in South African gold miners, despite the successful use of isoniazid in preventing tuberculosis during treatment

27 Laboratory Diagnosis of Tuberculosis AFB smear by ZN stain and culture remain the gold standard in diagnosis
28 Detecting AFB by fluorochrome stain using fluorescence microscopy The smear may be stained by auramine-o dye. In this method the TB bacilli are stained yellow against dark background & easily visualized using florescent microscope Advantages: - More sensitive - Rapid Disadvantages: - Hazards of dye toxicity - more expensive - must be confirmed by Z-N stain
29 Cultures on L J media Lowenstein Jensen medium is an egg based media with addition of salts, 5 % glycerol, Malachite green & penicillin Advantages: - Specificity about 99 % - More sensitive (need lower no. of bacilli / ml) - Can differentiate between TB complex & NTM using biochemical reactions - Sensitivity tests for antituberculous drugs ( St, INH, Rif., E) Disadvantages: Slowly growing ( up to 8 weeks )
30 Rapid Radiometric Culture System BACTEC specimens are cultured in a liquid medium (Middle brook7h9 broth base ) containing C 14 labelled palmitic acid & PANTA antibiotic mixture Growing mycobacteria utilize the acid, releasing radioactive CO 2 which is measured as growth index (GI) in the BACTEC instrument The daily increase in GI output is directly proportional to the rate & amount of growth in the medium
31 Microscopic-Observation Drug-Susceptibility Assay for the Diagnosis of TB A single MODS culture of a sputum sample offers more rapid and sensitive detection of tuberculosis and multidrug-resistant tuberculosis than the existing gold-standard methods used Moore DA et al, N Engl J Med 2006;355:
32 Nucleic Acid Amplification (NAP) Test. A new molecular diagnostic test called Xpert MTB/RIF assay detects M. tuberculosis complex within 2 hours, with an assay sensitivity that is much higher than that of smear microscopy
33 Treatment of Tuberculosis
34 TB Drug Resistance Mono-resistance MDR-TB: Resistance to isoniazid and rifampicin XDR-TB: FLD: SLD: TDR: Resistance to at least isoniazid and rifampicin, and to any fluoroquinolone, and to any of the 3 2 nd line injectables (amikacin, capreomycin & kanamycin) CDC, Mortal Wkly Rep 2006; 55: Resistance to all first-line anti-tb drugs Resistance to second-line anti-tb drugs cohort of 15 patients in Iran was reported which were resistant to all anti-tb drugs tested Velayati AA et al, Chest 2009; 136: 420-5)
35 Major Problems in Treatment OF TB MDR-TB Paradoxical expansion of TB lesions (brain) Chronic Liver Disease Raised ALT Raised bilirubin Chronic Renal Disease Mild renal impairment ESRD
36 Group Anti-TB Drugs Group 1: First line Oral agents Anti-TB Drugs Isoniazid, Rifampicin, Pyrazinamide, ethambutol, Rifabutin, Rifapentin Group 2: Injectable agents Kanamycin, Amikacin, Capreomycin, Streptomycin Group 3: Fluoroquinolones Levofloxacin, Moxifloxacin, Ofloxacin Group 4: Oral Bacteriostatic Second Line Agents Group 5: Agents with an unclear role in the Rx of drug resistant TB Para aminosalicylic acid, Cycloserine, Terizidone, Ethionamide, Prothionamide, viomycin Clofazimine, Linezolid, Amoxicillin/clavulanate, Thioacetazone, Imipenem/cilastatin, high dose Isoniazid, Clarithromycin
37 CLINICAL TRIALS OF RECOMMENDED CHEMOTHERAPY REGIMENS 9 MONTHS DURATION REGIMENS Study Regimen PATIENTS ASSESSED Comp. N Failures N (%) Relapses N (%) 1 st BTA S(E)HR/7HR ND BTA EHR/7HR (1.5) 1 ST French EHR/7HR (2.4) 2 nd French E(S)HR/6HR (3.8) Arkansas HR/8H 2 R (2.8) 15 (2.1) San Francisco 88 2HRE/7HR (1.5) 4 (2)
38 CLINICAL TRIALS OF RECOMMENDED CHEMOTHERAPY REGIMENS FOR TUBERCULOSIS 6 MONTHS DURATION REGIMENS PATIENTS ASSESSED Study Regimen Comp. N Failures N (%) Relapses N (%) East Africa BMRC 2HRSZ/4HR (Z) (1.3) 1983 Singapore BMRC 2(H)HR(S)Z/HR (.3) 3 (1) 1985 Singapore BMRC 2HRSZ/4HR(Z) (1.9) nd BTA HRS(E)Z/4HR (1.6) Poland HRSZ/4HR Algeria EHRZ/2HR (3) Hongkong/BMRC 6HRZ(S) (E) (1.4) 1987 Germany HRSZ 95 2 (2.1) 0
39 BACTERIOLOGIC RELAPSE RATES IN SMEAR-POSITIVE & CULTURE POSITIVE DISEASE: HIGHLY EFFECTIVE SIX-MONTH REGIMENS WITH ISONIAZID & RIFAMPIN Study Regimen mo Follow-up mo Patients Assessed US Public Health Service study 20 Second East African-BMRC study East African- BMRC study Singapore- BMRC study Second BTA study Bacteriologic Relapses (%) HR (9) HR (7) 2 SHR/HRZ 2SHRZ/HR 2 SHRZ/HRZ 2 SHRZ/HR (2) (2) (2) 2 SHRZ/HR (1)
40 USPHS TUBERCULOSIS SHORT COURSE (1990) THERAPY TRIAL 21, RANDOMIZED, MULTI-CNTRE TRIAL Myco. tuberculosis, positive sputum culture All susceptible 617 pts. HRZ (2) / HR (4) 445 pts. HR (9) 6 months 9 months Sputum conversion (16 wks) 95% 90% Non-compliance Relapse (22 months) Completed therapy 61 51
41 TREATMENT ALTERNATIVES WITH SUSPECTED INITIAL DRUG RESISTANCE Beginning Regimens Continuing Regimens INH ( R ) OR INH ( R ) and SM (R) SM ( R ) (1) HRE (2) RE (10) HR (7) (2) HRZS (2) RE (10) HR (7) (3) HRZE (2) RE (10) HR (7)
42 SHORT COURSE FOR EXTRAPULMONARY TUBERCULOSIS 350 pts 402 sites Pleural (119), Disseminated (51), GU (51) Lymphatic (56), Bone/joints (26), Vertebral (21) Abdominal (21), Meningeal (18), Pericardial (12) Laryngeal (13), Misc (14) HR (1) daily/ HR (8) TW H (300mg), R (600mg) H (900mg), R (600mg) Mortality 5/297 = 1.7% Treatment failure 6/297 = 2.0% Late relapse 2/297 = 0.7% Ann Int. Med 1986 ASIM DUTT
43 Four-Month Moxifloxacin or Gatifloxacin Based Regimens for Drug-Sensitive TB Gillespie S et al, NEJM 2014 Merle CS et al, NEJM 2014 Fouad M, Ann Pharmacother 2011 Conde MB et al, Lancet 2009 Noninferiority of the 4-month regimen to the standard regimen with respect to the primary efficacy end point was not shown
44 THE IMPACT OF DOT ON EPIDEMIOLOGY The WHO-recommended Stop TB Strategy provides the framework for treating and caring for those who are sick and controlling the epidemic of drugsusceptible and drug-resistant disease The DOTS approach, which underpins the Stop TB Strategy, calls for political commitment to national programs designed to control disease by means of early diagnosis with the use of bacteriologic testing, standardized treatment with supervision and patient support, and provision and management of the drugs used in treatment
45 Where might new anti-tb drugs come from Repurposing of existing drugs used for other infections: Fluoroquinolnes, linezolid, clofazimine Improved use of existing TB drugs: Rifamycins Development of new chemical entities: Bedaquiline (TMC207) (Diaryquinoline) Delamanid (OPC67683) and Petomanid (Nitroimidazole) Sutezolid and AZD5847 (Oxazolidinone) SQ109 (Ethylene diamine)
46 FDA NEWS RELEASE For Immediate Release: Dec. 31, 2012 Media Inquiries: Sandy Walsh, , Consumer Inquiries: 888-INFO-FDA On Dec. 28, the U.S. Food and Drug Administration approved Sirturo (bedaquiline) as part of combination therapy to treat adults with multi-drug resistant pulmonary tuberculosis (TB) when other alternatives are not available.
47
48 BEDAQUILINE Bedaquiline fumarate is an oral diarylquinoline; it was approved by the United States Food and Drug Administration (FDA) in 2012 for treatment of multidrugresistant tuberculosis (MDR-TB) Provisional Centers for Disease Control and Prevention (CDC) guidelines have been issued for both approved and unapproved uses The World Health Organization (WHO) has also published recommendations on the use of bedaquiline
49 BEDAQUILINE Toxicity The FDA issued a black box warning to alert healthcare practitioners regarding an increased rate of death due to QT prolongation has been observed among patients treated with bedaquiline compared with patients treated with placebo (11.4 percent versus 2.5 percent, respectively). Bedaquiline may also result in increases in liver function tests
50
51 Delamanid (OPC-67683) Delamanid (OPC-67683), a new agent derived from the nitro-dihydroimidazooxazole class of compounds Inhibits mycolic acid synthesis, Has shown potent in vitro and in vivo activity Against both drug-susceptible and drug-resistant Administered at doses of 200 and 300 mg daily resulted in a decrease in the sputum M. tuberculosis burden that was similar to that of the potent antituberculosis drug rifampicin in previous studies of early bactericidal activity
52 TB Recurrences: Relapse vs Reinfection In a population based study in northern Malawi, tuberculosis patients diagnosed from were actively followed after the end of treatment Whole genome sequencing with approximately 100X coverage was carried out on all available cultures IS6110 Restriction Fragment Length Polymorphism (RFLP) was available on cultures up to 2008 a single nucleotide polymorphism (SNP) difference of: 10 SNPs was used to define relapse >100 SNPs for reinfection Guerra Assunção1 JA et al, J Infect Dis 2014
53 TB Recurrences: Relapse vs Reinfection Of 1471 patients 139 had laboratory-confirmed recurrences: 55 had relapse 20 had reinfection 64 type of recurrence was unclassified Almost all relapses occurred in the first 2 years HIV infection was associated with reinfection but not relapse Relapses were associated with: Isoniazid resistance Treatment before 2007 Lineage-3 strains Guerra Assunção1 JA et al, J Infect Dis 2014
54 TB Vaccine - BCG The protection conferred by the BCG vaccine is significantly greater when the vaccine is administered to neonates or school children and for miliary or meningeal TB Protection against pulmonary TB, which accounts for the majority of TB mortality and morbidity worldwide, is age dependent In children,protection against pulmonary TB can reach up to 80% [5]; however, only 50% of adults are protected, and some studies have reported no real preventive effects Previous exposure to environmental mycobacteria appears to be an important limiting factor for the BCG vaccine Subjects with latent TB infection are less protected and the vaccine efficacy has been shown N. Principi; Tuberculosis 2014 (in press)

55 N. Principi; Tuberculosis 2014 (in press)
56 TB Infection Control Negative pressure room Wear N95 mask Hand Hygiene Limit patient movement (put mask if patient moved to radiology, surgery, etc ) Investigate family contacts and close contacts No need for special hospital or sanatorium
57 WHO Ambitious Target Reducing TB incidence to 10 per 10 5 by year 2035 Aim at eliminating TB as a public health problem by 2050 (reducing TB incidence to 1 per 10 5 )


58
HA Convention 2016 : Special Topic Session 3 May 2016
 HA Convention 2016 : Special Topic Session 3 May 2016 Diagnosis and Management of TB in Adults Dr. Thomas Mok COS(RMD), KH Tuberculosis An airborne infectious disease caused by Mycobacterium tuberculosis
HA Convention 2016 : Special Topic Session 3 May 2016 Diagnosis and Management of TB in Adults Dr. Thomas Mok COS(RMD), KH Tuberculosis An airborne infectious disease caused by Mycobacterium tuberculosis
Tuberculosis. New TB diagnostics. New drugs.new vaccines. Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012
 Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
MULTIDRUG- RESISTANT TUBERCULOSIS. Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic
 MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Marcos Burgos, MD has the following disclosures to make:
 Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
TB Laboratory for Nurses
 TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Antimycobacterial drugs. Dr.Naza M.Ali lec Dec 2018
 Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE
 Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Frances Morgan, PhD October 21, Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS
 The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Newer anti-tb drugs and regimens. DM Seminar
 Newer anti-tb drugs and regimens DM Seminar 31-10-14 Why are newer drugs/regimens needed? Problems with current drugs/regimens Drug resistance Drug interaction of anti-tubercular drugs with ART Long duration
Newer anti-tb drugs and regimens DM Seminar 31-10-14 Why are newer drugs/regimens needed? Problems with current drugs/regimens Drug resistance Drug interaction of anti-tubercular drugs with ART Long duration
Ken Jost, BA, has the following disclosures to make:
 Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Management of MDR TB. Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore
 Management of MDR TB Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore Outline Global epidemiology of Tuberculosis Epidemiology of Tuberculosis
Management of MDR TB Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore Outline Global epidemiology of Tuberculosis Epidemiology of Tuberculosis
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
APSR RESPIRATORY UPDATES
 APSR RESPIRATORY UPDATES Volume 5, Issue 2 Newsletter Date: February 2013 APSR EDUCATION PUBLICATION Inside this issue: Tuberculosis Multidrug-resistant pulmonary tuberculosis treatment regimens and patient
APSR RESPIRATORY UPDATES Volume 5, Issue 2 Newsletter Date: February 2013 APSR EDUCATION PUBLICATION Inside this issue: Tuberculosis Multidrug-resistant pulmonary tuberculosis treatment regimens and patient
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health
 Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health C. Robert Horsburgh, Jr. Boston University School of Public Health Background Outline Why does drug resistance threaten
Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health C. Robert Horsburgh, Jr. Boston University School of Public Health Background Outline Why does drug resistance threaten
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist, NH GEISELMED.DARTMOUTH.EDU GEISELMED.DARTMOUTH.
 The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
Hot Issues in Tuberculosis: Treatment of Latent TB Infection and New TB Drugs
 Slide 1 Hot Issues in Tuberculosis: Treatment of Latent TB Infection and New TB Drugs Constance A. Benson, M.D. Professor of Medicine Division of Infectious Diseases University of California, San Diego
Slide 1 Hot Issues in Tuberculosis: Treatment of Latent TB Infection and New TB Drugs Constance A. Benson, M.D. Professor of Medicine Division of Infectious Diseases University of California, San Diego
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE MAY 8-11, 2018 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. List
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE MAY 8-11, 2018 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. List
Treatment of Tuberculosis
 Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Management of Drug-resistant Tuberculosis (DR-TB)
") Management of Drug-resistant Tuberculosis (DR-TB) Nitipatana Chierakul Division of Respiratory Disease & Tuberculosis Department of Medicine Faculty of Medicine Siriraj Hospital October 14 th, 2008 Tropical
Management of Drug-resistant Tuberculosis (DR-TB) Nitipatana Chierakul Division of Respiratory Disease & Tuberculosis Department of Medicine Faculty of Medicine Siriraj Hospital October 14 th, 2008 Tropical
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Global epidemiology of drug-resistant tuberculosis. Factors contributing to the epidemic of MDR/XDR-TB. CHIANG Chen-Yuan MD, MPH, DrPhilos
 Global epidemiology of drug-resistant tuberculosis Factors contributing to the epidemic of MDR/XDR-TB CHIANG Chen-Yuan MD, MPH, DrPhilos By the end of this presentation, participants would be able to describe
Global epidemiology of drug-resistant tuberculosis Factors contributing to the epidemic of MDR/XDR-TB CHIANG Chen-Yuan MD, MPH, DrPhilos By the end of this presentation, participants would be able to describe
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
MYCOBACTERIUM. Mycobacterium Tuberculosis (Mtb) nontuberculous mycobacteria (NTM) Mycobacterium lepray
 nontuberculous mycobacteria (NTM) Mycobacterium lepray") MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
The treatment of patients with initial isoniazid resistance
 The treatment of patients with initial isoniazid resistance 2011 INTERTB Meeting, St George s, London Patrick Phillips, MRC Clinical Trials Unit DA Mitchison, AJ Nunn. 21 st October 2011 Outline Background
The treatment of patients with initial isoniazid resistance 2011 INTERTB Meeting, St George s, London Patrick Phillips, MRC Clinical Trials Unit DA Mitchison, AJ Nunn. 21 st October 2011 Outline Background
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
New Tuberculosis Guidelines. Jason Stout, MD, MHS
 New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Tuberculosis. WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED
 Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
TB in the Correctional Setting Florence, Arizona October 7, 2014
 TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
Challenge in Lebanon as around the World
 OPL 22nd Pharmaceutical Congress 2014 Tuberculosis A Continuing i Public Health Challenge in Lebanon as around the World Myrna Germanos Haddad Hematology/Immunology Lab Hotel-Dieu de France Hospital Beirut
OPL 22nd Pharmaceutical Congress 2014 Tuberculosis A Continuing i Public Health Challenge in Lebanon as around the World Myrna Germanos Haddad Hematology/Immunology Lab Hotel-Dieu de France Hospital Beirut
Tuberculosis: update 2013
 Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
NEW DRUGS FOR TUBERCULOSIS: THE NEED, THE HOPE AND THE REALITY
 NEW DRUGS FOR TUBERCULOSIS: THE NEED, THE HOPE AND THE REALITY Neil W. Schluger, M.D. Professor of Medicine, Epidemiology and Environmental Health Sciences Columbia University Global tuberculosis incidence
NEW DRUGS FOR TUBERCULOSIS: THE NEED, THE HOPE AND THE REALITY Neil W. Schluger, M.D. Professor of Medicine, Epidemiology and Environmental Health Sciences Columbia University Global tuberculosis incidence
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Diagnosis of drug resistant TB
 Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
The ABC s of AFB s Laboratory Testing for Tuberculosis. Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory
 The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
TB 101 Disease, Clinical Assessment and Lab Testing
 TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Pharmacology and Pharmacokinetics of TB Drugs Part I
 Pharmacology and Pharmacokinetics of TB Drugs Part I Charles A. Peloquin, Pharm. D. Professor, and Director Infectious Disease Pharmacokinetics Laboratory College of Pharmacy and The Emerging Pathogens
Pharmacology and Pharmacokinetics of TB Drugs Part I Charles A. Peloquin, Pharm. D. Professor, and Director Infectious Disease Pharmacokinetics Laboratory College of Pharmacy and The Emerging Pathogens
Chapter 5 Treatment. 5.1 First-Line Antituberculous Treatment
 Chapter 5 Treatment Abstract In this chapter the treatment of drug sensitive and drug resistant TB and timing of antiretroviral treatment for HIV infected patients will be reviewed. Emphasis is placed
Chapter 5 Treatment Abstract In this chapter the treatment of drug sensitive and drug resistant TB and timing of antiretroviral treatment for HIV infected patients will be reviewed. Emphasis is placed
Management of Multidrug- Resistant TB in Children. Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building
 Management of Multidrug- Resistant TB in Children Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building Objectives To review data on best practices for diagnosis, treatment and prevention
Management of Multidrug- Resistant TB in Children Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building Objectives To review data on best practices for diagnosis, treatment and prevention
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis. Impact of TB. Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH)
") Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
Treatment of Tuberculosis
 Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
2016 Annual Tuberculosis Report For Fresno County
 206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!!
 Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
Tuberculosis Intensive November 17 20, 2015 San Antonio, TX
 Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer
 Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Pediatric TB Intensive San Antonio, Texas October 14, 2013
 Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
Dosage and Administration
 SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
Sirturo: a new treatment against multidrug resistant tuberculosis
 Sirturo: a new treatment against multidrug resistant tuberculosis TB is an on-going problem WHO estimated incidence of new TB cases 2009 Global Tuberculosis Control: WHO report 2010. Available at: http://www.who.int/tb/publications/global_report/2010/en/index.html
Sirturo: a new treatment against multidrug resistant tuberculosis TB is an on-going problem WHO estimated incidence of new TB cases 2009 Global Tuberculosis Control: WHO report 2010. Available at: http://www.who.int/tb/publications/global_report/2010/en/index.html
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Diagnosis of TB: Laboratory Ken Jost, BA November 12, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas November 11 14, 2014 Diagnosis of TB: Laboratory Ken Jost, BA November 12, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
TB IN EMERGENCIES. Disease Control in Humanitarian Emergencies (DCE)
") TB IN EMERGENCIES Department of Epidemic and Pandemic Alert and Response (EPR) Health Security and Environment Cluster (HSE) (Acknowledgements WHO Stop TB Programme WHO/STB) 1 Why TB? >33% of the global
TB IN EMERGENCIES Department of Epidemic and Pandemic Alert and Response (EPR) Health Security and Environment Cluster (HSE) (Acknowledgements WHO Stop TB Programme WHO/STB) 1 Why TB? >33% of the global
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Chapter 4 Diagnosis of Tuberculosis Disease
 Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Let s Talk TB. A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Abstract Nearly 50% of patients with
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Abstract Nearly 50% of patients with
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
Bedaquiline: 10 years later, the drug susceptibility testing protocol is still pending
 EDITORIAL TUBERCULOSIS Bedaquiline: 10 years later, the drug susceptibility testing protocol is still pending Max Salfinger 1 and Giovanni Battista Migliori 2 Affiliations: 1 Dept of Medicine, National
EDITORIAL TUBERCULOSIS Bedaquiline: 10 years later, the drug susceptibility testing protocol is still pending Max Salfinger 1 and Giovanni Battista Migliori 2 Affiliations: 1 Dept of Medicine, National
Tuberculosis Infection in the US Military
 Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
Research Methods for TB Diagnostics. Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012
 Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Treatment of Tuberculosis
 Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Tuberculosis: The Big Picture And Challenge of Drug-resistance
 5 th APHL National Conference on Laboratory Aspects of Tuberculosis August 11-13, 2008 San Diego, California Tuberculosis: The Big Picture And Challenge of Drug-resistance RADM Kenneth G. Castro, M.D.
5 th APHL National Conference on Laboratory Aspects of Tuberculosis August 11-13, 2008 San Diego, California Tuberculosis: The Big Picture And Challenge of Drug-resistance RADM Kenneth G. Castro, M.D.
Diagnosis & Management of Latent TB Infection
 Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
TB Intensive San Antonio, Texas May 7-10, 2013
 TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant