Diagnosis of tuberculosis
|
|
|
- Rosa Gregory
- 6 years ago
- Views:
Transcription



1 Diagnosis of tuberculosis Madhukar Pai, MD, PhD Assistant Professor, Epidemiology McGill University, Montreal, Canada Global TB Case Detection A major concern 2.6 million new smear + cases notified in million new cases overall notified in % of the estimated 4.1 million cases 57% of the estimated 9.3 million cases WHO Report 2009 Global Tuberculosis Control 1



2 Why is diagnosis the Achilles heel of TB control? 3 Diagnostic tools that Koch used Microscopy Culture Tuberculin test 4 2
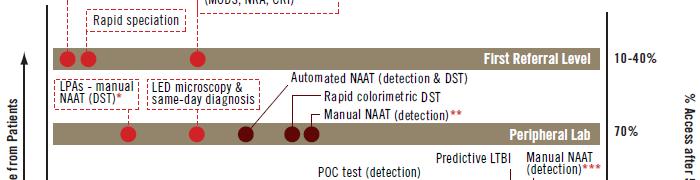
3 are still in use today! Active TB Sputum microscopy [1882] Mycobacterial culture [1882] Chest X-rays [1896] Latent t TB (LTBI) Tuberculin skin test [1890] 5 The landscape in 2010 is much improved Surveillance Reference methods Network supervision Resolution testing (screening-test negative drug resistance) Regional Labs Reference Labs LC / DST 15d/ 30d SC / DST LC / DST 30d / 15d 60d/ 30d In house DST (MODS, NRA, CRI) Special settings and conditions LPA Rif / INH 2d District Level Screening Passive case finding Detect and treat SubDistrict Level ZN 2-3d Integrated NAAT +40% /2h Microscopy Level LED FM +10% Manual NAAT+25% Clinical Screening Primary care Community Level RDT Gen1 / Gen 2 3
4 Diagnosis of latent tuberculosis infection (LTBI) Importance of LTBI It is estimated that nearly one-third of the world s population is infected with M. tuberculosis In most individuals, M. tuberculosis infection is contained initially by host defences, and infection remains latent. However, latent TB infection (LTBI) has the potential to develop into active disease at any time. Identification and treatment of latent tuberculosis infection can reduce the risk of development of disease by as much as percent, and so has potential to protect the health of the individuals as well as the public by reducing the number of potential sources of infection 4
5 Indications for LTBI testing The goal of testing for LTBI is to identify individuals who are at increased risk for the development of tuberculosis and therefore would benefit from treatment of latent TB infection. Only those who would benefit from treatment should be tested So a decision to test presupposes a decision to treat if the test is positive. In general, testing for LTBI is warranted to identify individuals who are at risk of new infection, and to identify individuals at increased risk of reactivation due to associated conditions However, LTBI testing is a challenge There is no definite method to confirm or rule out LTBI LTBI: a diagnostic challenge [case #1] My 19 year old son is being worked up for his 2nd kidney transplant and is currently on hemodialysis. He has been through numerous drug reactions (some of them extremely rare) and he is not too keen on the skin test. The TB skin test is a part of the protocol of the Ottawa Hospital as there were two people last year who died of TB post renal transplant. From the studies I have found on the internet it appears that the TB skin test is not a very accurate method of detection of LTBI in hemodialysis patients. Is there anyone in Canada who is using this test and would it be possible to bring it to Ottawa? We are told that the Ottawa hospitals have a great concern about TB as they service the Inuit population. That said, I would assume that employing a TB blood test would be of great benefit to our renal patient population. 10 5
![LTBI: a diagnostic challenge [case #2] I am a healthcare worker, and have just had a positive TB skin test.](/docs-images/77/75437432/images/6-0.jpg "It's only been one year since my last skin test which was negative.")


6 LTBI: a diagnostic challenge [case #2] I am a healthcare worker, and have just had a positive TB skin test. It's only been one year since my last skin test which was negative. My primary care doctor read my chest x-ray as negative and did not recommend INH, but the Health Dept. here recommends taking INH for 6-9 months. Doctors and nurses whom I work with say that false positives happen all the time and to not worry about it. I have read about the side effects of this drug, and want to be sure that I actually am a carrier before taking it. I have been reading about the QFT-G and am wondering if it will help resolve my dilemma about taking INH? 11 Who should be tested? Pai & Menzies. UpToDate
; in other regions, PPD RT-23 is used at the standard dose of 2 TU Interferon-gamma release assays (IGRAs) QuantiFERON-TB Gold In Tube T-SPOT.TB TB Both tests are imperfect!")
7 How do we test for LTBI? Tuberculin skin test Mantoux method, using purified protein derivative (PPD) at the recommend dose of 5 tuberculin units (0.1 ml); in other regions, PPD RT-23 is used at the standard dose of 2 TU Interferon-gamma release assays (IGRAs) QuantiFERON-TB Gold In Tube T-SPOT.TB TB Both tests are imperfect! Tuberculin skin test TST Measures cell-mediated immune response (CMI) Uses PPD: a crude antigenic mixture Limitations of TST: false positives and false negatives are possible technical issues in administration and interpretation difficulty in separating true infection from the effects of BCG and non-tuberculous mycobacteria (NTM) repeated TST boosts the immune response requires a 3-dimensional interpretation 14 7


8 Administering the TST Inject 0.1 ml of 5 TU PPD tuberculin solution intradermally on volar surface of lower arm using a 27-gauge needle Produce a wheal 6 to 10 mm in diameter Source: US CDC Reading the TST Measure reaction in 48 to 72 hours Measure induration, not erythema Record reaction in millimeters, not negative or positive Ensure trained health care professional measures and interprets the TST Self reading is not accurate Source: US CDC 8


9 TST Interpretation Pai & Menzies. UpToDate 2009 Factors That May Cause False-Positive TST Reactions Nontuberculous mycobacteria Reactions caused by nontuberculous mycobacteria are usually 10 mm of induration BCG vaccination Reactivity in BCG vaccine recipients generally wanes over time; positive TST result is likely due to TB infection if risk factors are present Source: US CDC 9





10 Factors That May Cause False-Negative TST Reactions Pai & Menzies. UpToDate 2009 TST requires a 3-dimensional interpretation 10




11 When BCG is given after infancy or repeated many times, it can affect TST results Analysis of 24 studies with N = 240,243 subjects When BCG is given in infancy, false-positive TST results due to BCG occur in 6% of vaccinated subjects When BCG is given after infancy, false-positive TST results due to BCG occur in 40% of vaccinated subjects In India, BCG has limited effect on TST 11





12 In Uganda, BCG has limited effect on TST In Japan, BCG has a major effect on TST 12






13 In Ukraine, BCG has a major effect on TST IGRAs T-SPOT.TB [Oxford Immunotec, UK] QuantiFERON-TB Gold In Tube [Cellestis Ltd, Australia] 13
14 Quick Summary of Evidence TST specificity is high in BCG non-vaccinated; but lower and variable in BCG vaccinated IGRAs (especially QFT) have very high specificity (>95%) IGRA specificity is higher than TST IGRAs are not affected by BCG vaccination Maybe very helpful in settings that give BCG after infancy or give multiple vaccinations Sensitivity of IGRAs and TST is not consistent across tests and populations Overall, IGRAs are ~80% sensitive in culture+ TB patients Sensitivity is lower in high incidence countries QFT is as sensitive as TST (~80%) QFT sensitivity is higher in low incidence than high incidence countries T-SPOT.TB appears to be more sensitive (~90%) than both QuantiFERON tests and TST But this may partly be because of cut-offs used for T-SPOT vs QFT In low-incidence settings, IGRAs correlate well with markers of exposure Pai et al. Annals Int Med 2008 Countries that may benefit from IGRAs Zwerling A et al. 14
15 IGRAs in immunocompromised Immunocompromised groups are highly variable, and most studies are small: All tests underperform in severely immunocompromised patients Using both TST and IGRA might help increase sensitivity IGRA sens in HIV+ is lower (~60 65%) than HIV- (~80 90%) About 15% of HIV+ TB patients have indeterminate IGRA results Indeterminate IGRA results increase with level of immunosuppression (i.e. low CD4 counts) Very limited data on predictive value Utility as rule out test for active TB is not well established Unlikely to have a rule out value, given the modest sensitivity 29 IGRAs for active TB diagnosis No role in adults Cannot distinguish between latent and active TB Sensitivity is not high Cannot rule out Specificity will always be low in high TB incidence settings Cannot rule in No evidence that IGRAs offer any added value over conventional microbiological tests In children Cannot be used in isolation A negative IGRA does not rule out active TB at any age. Cannot replace microbiological investigations Useful as evidence of infection which should be interpreted with other information (e.g. contact, symptoms, radiological findings) 30 15
16 Predictive value: Incidence rates of TB by IGRA status Rangaka M et al. Incidence rate per 1000 person-years 31 Rates of disease progression in IGRA+ in the largest high burden country studies Country N Test Incidence of active TB in IGRA+ groups The Gambia [Hill et al. 2008] Turkey [Bakir et al. 2008] 2348 ELISPOT (inhouse) 908 ELISPOT (T-SPOT.TB) 9/1000 person-yr 21/1000 person-yr S Africa [Mahomed et al (abstract)] Colombia [del Corral et al. 2009] Senegal [Lienhardt et al. PLoS One 2010] 5248 QFT 6/1000 person-yr 2060 In-house whole-blood CFP-10 assay 2679 ELISPOT (inhouse) 11/1000 person-yr 14/1000 person-yr 16
17 Results: IGRA vs TST: Which has greater predictive ability? Rangaka M et al. 33 Conclusions on predictive value Incidence rates of TB, even in IGRA positive individuals, are low, suggesting that a vast majority (>95%) of IGRA+ individuals do not progress to TB disease during follow-up. This is similar to the TST. All existing LTBI tests (TST and IGRAs) have only modest predictive value and may not help identify those who are at highest risk of progression to disease. Based on the evidence thus far, IGRAs appear to have similar predictive value as the TST. In some settings, the % IGRA+ will be less than % TST+, reducing the number needed for IPT The search for highly predictive biomarkers must continue 34 17
.")
18 USA: CDC Guidelines, 2010 IGRAs can be used in place of (but not in addition to) TST in all situations in which CDC recommends TST as an aid in diagnosing LTBI (contact investigations, testing during pregnancy, and screening of health care workers and others undergoing serial evaluation for LTBI). IGRAs are preferred over TST in individuals who have received BCG and individuals from groups that have poor rates of return for TST reading. TST is preferred over IGRAs for testing children less than 5 years of age. Canadian IGRA guidelines For persons with a positive TST and low pretest probability of recently acquired LTBI, as well as no other risk factors for progression to active disease, IGRAs may be used as a confirmatory test to exclude the possibility of a false positive TST. For persons with high risk of progression to active disease if infected, a TST should be used; if this is positive the person should be considered to have LTBI. If negative, an IGRA could be done; if positive the person should be considered to have LTBI


19 Canadian IGRA guidelines In immunocompromised individuals, the TST should be the initial test used to detect LTBI. If the TST is positive, the person should be considered to have LTBI. However, given the rate of false-negative TST results in immunocompromised populations, IGRA testing is appropriate in the setting of negative TST results. If the IGRA result is positive, the person may be considered to have LTBI. In children, IGRAs may be used as a supplementary diagnostic tool, together with clinical specimens for definitive microbiologic diagnosis, TST and other investigations. However, IGRA should not be a substitute for, or obviate the need for, appropriate microbiologic specimen collection. A negative IGRA (or TST) does NOT rule out active TB at any age. 37 Diagnosis of active TB and drug-resistance 19

20 Diagnostic options Smear microscopy Culture NAAT Drug Susceptibility Testing Smear Microscopy 50-70% sensitive, very specific Quick, cheap, relatively easy Stains take advantage of mycolic acid in cell walls of Mycobacteria Acid Fast Bacilli Stain Decolorize Counterstain 20


21 LIGHT MICROSCOPY Traditional method More experienced microscopists Tedious FLUORESCENT MICROSCOPY Need lower magnification 45% less time to examine slides 10% more sensitive Easier staining procedure WHO policies on Smear Microscopy LED microscopy



22 Commercial LED Microscopes Minion et al. Exp Rev Med Dev 2009 Culture-based diagnostics Gold Standard High Sensitivity, Isolate Available for DST and molecular typing Slow Turnaround, Biosafety Issues, Requires Specimen Processing, Relatively Expensive 22



23 Policy on Culture-based Diagnostics 2007 Conventional NAATs High specificity and PPV Sensitivity is lower and highly variable Especially in extrapulmonary specimens Especially in smear negative specimens (>95% smear + vs % smear -) Expensive Should not be used on follow-up specimens In house assays Roche Cobas Amplicor Gen-Probe AMTD BD ProbeTec ET Ling D et al. 23




 [3 specimens increases to 90.")
24 Newer NAAT: Cepheid Xpert MTB/RIF Automated nested RT- PCR Simple 1-step specimen preparation Can be used at the pointof-treatment Results in 2 hours Detects TB and RIF resistance Equipment ~$20k; ~$20/test 1462 symptomatic patients (4386 samples) 50.7% culture positivity Sensitivity: 98.2% in smear (+) 72.5% in smear (-) [3 specimens increases to 90.2%] Specificity 99.2% 97.6% accurate for Rif-R 98.1% accurate for Rif-S Results in <2hrs 24





25 Upcoming WHO Policy Raviglione M et al. Detecting Drug Resistance Multidrug and extensively drug-resistant TB (M/XDR-TB): 2010 global report on surveillance and response 25


26 Conventional Drug Susceptibility Testing Agar Proportion Method Plate isolate onto drug-free and drug-containing media Count colonies on each if >1% of drug-free growth present on drugcontaining growth = Resistant BACTEC 460/MGIT Inoculate drug-containing bottles Inoculate drug-free bottle with 1: diluted d isolate Growth Index (growth units) compared Line Probe Assays Detection of MTB & RIFresistance (rpob) Requires extraction, amplification Colorimetric development using immobilized probes Innogenetics, INNO-LiPA Rif TB Hain, GenoType MTBDRplus Inno-LiPA Rif.TB assay Innogenetics, Belgium GenoType MTBDRplus assay Hain Lifescience GmbH, Germany 26


27 Policy on Line Probe Assays 2008 Rapid rifampin resistance detection using Xpert MTB/RIF Boehme C et al. NEJM


28 In conclusion, much progress has been made in improving TB diagnosis, but 55 We still do not have a good point of care test 56 28




29 Global Plan to Stop TB 29
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
Update on IGRA Predictive Value
 Update on IGRA Predictive Value Sandra Kik, PhD Molebogeng Rangaka, MD, PhD Madhukar Pai, MD, PhD McGill International TB Centre, McGill University University of Cape Town & London School of Hygiene and
Update on IGRA Predictive Value Sandra Kik, PhD Molebogeng Rangaka, MD, PhD Madhukar Pai, MD, PhD McGill International TB Centre, McGill University University of Cape Town & London School of Hygiene and
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Intensive Tyler, Texas December 2-4, 2008
 TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
INTENSIFIED TB CASE FINDING
 INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
How best to structure a laboratory network with new technologies
 How best to structure a laboratory network with new technologies Cristina Gutierrez, MD, PhD Uniting to scale up TB care in Central Asia 14 and 15 April 2011 Tashkent, Uzbekistan New laboratory diagnostics
How best to structure a laboratory network with new technologies Cristina Gutierrez, MD, PhD Uniting to scale up TB care in Central Asia 14 and 15 April 2011 Tashkent, Uzbekistan New laboratory diagnostics
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Research Methods for TB Diagnostics. Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012
 Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Peggy Leslie-Smith, RN
 Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
TB Laboratory for Nurses
 TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
TB 101 Disease, Clinical Assessment and Lab Testing
 TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
POSITIONING OF TB DX : TIERED SYSTEM, INTEGRATED APPROACH
 POSITIONING OF TB DX : TIERED SYSTEM, INTEGRATED APPROACH Akos Somoskövi, M.D., Ph.D. and Giorgio Roscigno, M.D. ANNUAL GLI MEETING, 4 th OCTOBER 2010 MERIEUX FOUNDATION, ANNECY Integrated Laboratory Network
POSITIONING OF TB DX : TIERED SYSTEM, INTEGRATED APPROACH Akos Somoskövi, M.D., Ph.D. and Giorgio Roscigno, M.D. ANNUAL GLI MEETING, 4 th OCTOBER 2010 MERIEUX FOUNDATION, ANNECY Integrated Laboratory Network
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Testing for TB. Bart Van Berckelaer Territory Manager Benelux. Subtitle
 Testing for TB Bart Van Berckelaer Territory Manager Benelux Subtitle Agenda TB infection pathway TB immunisation Testing options Pre lab considerations of the whole blood ELISA test The T-SPOT.TB test
Testing for TB Bart Van Berckelaer Territory Manager Benelux Subtitle Agenda TB infection pathway TB immunisation Testing options Pre lab considerations of the whole blood ELISA test The T-SPOT.TB test
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines
 Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
Ken Jost, BA, has the following disclosures to make:
 Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
New Standards for an Old Disease:
 New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
Evidence on IGRAs in Low & Middle Income Countries. Madhukar Pai, MD, PhD McGill University, Montreal
 Evidence on IGRAs in Low & Middle Income Countries Madhukar Pai, MD, PhD McGill University, Montreal Madhukar.pai@mcgill.ca Disclosure No industry/financial conflicts I co-chair the Stop TB Partnership
Evidence on IGRAs in Low & Middle Income Countries Madhukar Pai, MD, PhD McGill University, Montreal Madhukar.pai@mcgill.ca Disclosure No industry/financial conflicts I co-chair the Stop TB Partnership
Detecting latent tuberculosis using interferon gamma release assays (IGRA)
") Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
Predictive Value of interferon-gamma release assays for incident active TB disease: A systematic review
 Predictive Value of interferon-gamma release assays for incident active TB disease: A systematic review Lele Rangaka University of Cape Town, South Africa mxrangaka@yahoo.co.uk 1 The 3 I s Isoniazid preventive
Predictive Value of interferon-gamma release assays for incident active TB disease: A systematic review Lele Rangaka University of Cape Town, South Africa mxrangaka@yahoo.co.uk 1 The 3 I s Isoniazid preventive
TB/HIV 2 sides of the same coin. Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai
 TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
Role of the Laboratory in TB Diagnosis and Management
 Role of the Laboratory in TB Diagnosis and Management Michael Pentella, Ph.D., D(ABMM), CIC Associate Director University Hygienic Lab Clinical Associate Professor, College of Public Health, University
Role of the Laboratory in TB Diagnosis and Management Michael Pentella, Ph.D., D(ABMM), CIC Associate Director University Hygienic Lab Clinical Associate Professor, College of Public Health, University
Latent Tuberculosis in Adults: From Testing TO Treatment
 Latent Tuberculosis in Adults: From Testing TO Treatment Sergio M. Borgia, MD, MSc., FRCP(C) Infectious Diseases Consultant, WOHS Medical Director, WOHS Tuberculosis Clinic Assistant Clinical Professor,
Latent Tuberculosis in Adults: From Testing TO Treatment Sergio M. Borgia, MD, MSc., FRCP(C) Infectious Diseases Consultant, WOHS Medical Director, WOHS Tuberculosis Clinic Assistant Clinical Professor,
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Receipt within 1 day of specimen collection. Report AFB b smear result within 1 day from receipt of specimen
 Recommendation Promote rapid delivery of specimens to the laboratory Use fluorescent acid-fast staining and promptly transmit results by phone, FAX, or electronically Identify growth as acid-fast and use
Recommendation Promote rapid delivery of specimens to the laboratory Use fluorescent acid-fast staining and promptly transmit results by phone, FAX, or electronically Identify growth as acid-fast and use
NOLA TB TIMES. TB Diagnostics A Special Issue. on TB Diagnosis 101. Diagnostic Discrepancy Data. Comprehensive Approach
 NOLA TB TIMES Volume 1, No 3 February 2016 TB Diagnostics A Special Issue on TB Diagnosis 101 Happy New Year and Happy Mardi Gras to everyone! We already have seven presumptive cases of tuberculosis (TB)
NOLA TB TIMES Volume 1, No 3 February 2016 TB Diagnostics A Special Issue on TB Diagnosis 101 Happy New Year and Happy Mardi Gras to everyone! We already have seven presumptive cases of tuberculosis (TB)
Using Interferon Gamma Release Assays for Diagnosis of TB Infection
 Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Modeling LTBI What are the key issues to consider? Dr Dick Menzies, Montreal Chest Institute, McGill International TB Centre
 Modeling LTBI What are the key issues to consider? Dr Dick Menzies, Montreal Chest Institute, McGill International TB Centre Overview The problem Treating active TB does not seem to be enough The solution:
Modeling LTBI What are the key issues to consider? Dr Dick Menzies, Montreal Chest Institute, McGill International TB Centre Overview The problem Treating active TB does not seem to be enough The solution:
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Community pharmacy-based tuberculosis skin testing
 Community pharmacy-based tuberculosis skin testing Shanna K. O Connor, PharmD ISU KDHS Spring CE Seminar 2018 In support of improving patient care, Idaho State University Kasiska Division of Health Sciences
Community pharmacy-based tuberculosis skin testing Shanna K. O Connor, PharmD ISU KDHS Spring CE Seminar 2018 In support of improving patient care, Idaho State University Kasiska Division of Health Sciences
Report on WHO Policy Statements
 Report on WHO Policy Statements Christopher Gilpin TB Diagnostics and Laboratory Strengthening Unit Secretariat, Global Laboratory Initiative Stop TB Department, WHO Geneva New Diagnostics Working Group
Report on WHO Policy Statements Christopher Gilpin TB Diagnostics and Laboratory Strengthening Unit Secretariat, Global Laboratory Initiative Stop TB Department, WHO Geneva New Diagnostics Working Group
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Nguyen Van Hung (NTP, Viet Nam)
") Technical Consultation Meeting on the Programmatic Management of Latent Tuberculosis Infection 31 August-1 September 2017, Seoul, Republic Korea Adopting new LTBI diagnostics at country level: perspective
Technical Consultation Meeting on the Programmatic Management of Latent Tuberculosis Infection 31 August-1 September 2017, Seoul, Republic Korea Adopting new LTBI diagnostics at country level: perspective
2016 OPAM Mid-Year Educational Conference, Sponsored by AOCOPM Sunday, March 13, 2016
 Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
TB Nurse Case Management Davenport, Iowa September 27 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Role of the Laboratory in the TB Diagnosis and Management Michael Pentella, PhD, MS, SM(ASCP), CIC, D(ABMM) September 27, 2011 Michael Pentella,
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Role of the Laboratory in the TB Diagnosis and Management Michael Pentella, PhD, MS, SM(ASCP), CIC, D(ABMM) September 27, 2011 Michael Pentella,
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Use of Interferon-γ Release Assays (IGRAs) in TB control in low and middle-income settings - EXPERT GROUP MEETING -
 in TB control in low and middle-income settings - EXPERT GROUP MEETING -") Use of Interferon-γ Release Assays (IGRAs) in TB control in low and middle-income settings - EXPERT GROUP MEETING - Date and time: 20-21 July 2010, 09:00 18:00 Venue: Salle B, WHO-HQ, Geneva, Switzerland
Use of Interferon-γ Release Assays (IGRAs) in TB control in low and middle-income settings - EXPERT GROUP MEETING - Date and time: 20-21 July 2010, 09:00 18:00 Venue: Salle B, WHO-HQ, Geneva, Switzerland
Revised Technical Instructions for Civil Surgeons. October 9, 2018
 Revised Technical Instructions for Civil Surgeons October 9, 2018 Speakers Joanna Regan Centers for Disease Control and Prevention Shereen Katrak California Department of Public Health Pennan Barry California
Revised Technical Instructions for Civil Surgeons October 9, 2018 Speakers Joanna Regan Centers for Disease Control and Prevention Shereen Katrak California Department of Public Health Pennan Barry California
Richard O Brien, Consultant, FIND 3 rd Global Symposium on IGRAs Waikoloa, Hawaii, 13 January 2012
 Global l Applications of IGRAs Richard O Brien, Consultant, FIND 3 rd Global Symposium on IGRAs Waikoloa, Hawaii, 13 January 2012 Disclosure I have no personal financial conflicts of I have no personal
Global l Applications of IGRAs Richard O Brien, Consultant, FIND 3 rd Global Symposium on IGRAs Waikoloa, Hawaii, 13 January 2012 Disclosure I have no personal financial conflicts of I have no personal
TB Diagnostics: Global Market Analysis and Potential
 TB Diagnostics: Global Market Analysis and Potential Madhukar Pai, MD, PhD McGill University, Montreal, Canada madhukar.pai@mcgill.ca September 2012 Market analyses are important and necessary To support
TB Diagnostics: Global Market Analysis and Potential Madhukar Pai, MD, PhD McGill University, Montreal, Canada madhukar.pai@mcgill.ca September 2012 Market analyses are important and necessary To support
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
Conflict of Interest Disclosures:
 Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Advanced Concepts in Pediatric Tuberculosis
 Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
PCR and direct amplification for tuberculosis diagnosis. Emmanuelle CAMBAU University Paris Diderot, APHP, Saint Louis-Lariboisière Hospital,
 PCR and direct amplification for tuberculosis diagnosis Emmanuelle CAMBAU University Paris Diderot, APHP, Saint Louis-Lariboisière Hospital, Paris, France Educational Workshop 05- ECCMID 2015 Copenhagen
PCR and direct amplification for tuberculosis diagnosis Emmanuelle CAMBAU University Paris Diderot, APHP, Saint Louis-Lariboisière Hospital, Paris, France Educational Workshop 05- ECCMID 2015 Copenhagen
The ABC s of AFB s Laboratory Testing for Tuberculosis. Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory
 The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
The Origin of Swine Flu
 How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
T-CELL RESPONSES ASSESSED USING IGRA AND TST ARE NOT CORRELATED WITH AFB GRADE AND CHEST RADIOGRAPH IN PULMONARY TUBERCULOSIS PATIENTS
 T-CELL RESPONSES ASSESSED USING IGRA AND TST ARE NOT CORRELATED WITH AFB GRADE AND CHEST RADIOGRAPH IN PULMONARY TUBERCULOSIS PATIENTS Kiatichai Faksri 1, 4, Wipa Reechaipichitkul 2, 4, Wilailuk Pimrin
T-CELL RESPONSES ASSESSED USING IGRA AND TST ARE NOT CORRELATED WITH AFB GRADE AND CHEST RADIOGRAPH IN PULMONARY TUBERCULOSIS PATIENTS Kiatichai Faksri 1, 4, Wipa Reechaipichitkul 2, 4, Wilailuk Pimrin
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
AT HIGH RISK OF PROGRESSING TO ACTIVE TB? Senior Lecturer and Consultant Physician University Hospitals of Leicester UK
 HOW WELL DO IGRAS PERFORM IN THE IDENTIFICATION OF PERSONS WHO ARE AT HIGH RISK OF PROGRESSING TO ACTIVE TB? Dr Pranab Haldar MD MRCP Senior Lecturer and Consultant Physician University Hospitals of Leicester
HOW WELL DO IGRAS PERFORM IN THE IDENTIFICATION OF PERSONS WHO ARE AT HIGH RISK OF PROGRESSING TO ACTIVE TB? Dr Pranab Haldar MD MRCP Senior Lecturer and Consultant Physician University Hospitals of Leicester
Tuberculosis Infection in the US Military
 Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Rapid PCR TB Testing Results in 68.5% Reduction in Unnecessary Isolation Days in Smear Positive Patients.
 Rapid PCR TB Testing Results in 68.5% Reduction in Unnecessary Isolation Days in Smear Positive Patients. Item Type Thesis Authors Patel, Ravikumar Publisher The University of Arizona. Rights Copyright
Rapid PCR TB Testing Results in 68.5% Reduction in Unnecessary Isolation Days in Smear Positive Patients. Item Type Thesis Authors Patel, Ravikumar Publisher The University of Arizona. Rights Copyright
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Diagnosis of drug resistant TB
 Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
Technical Bulletin No. 172
 CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculin Skin Testing
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
2. Methods of Tuberculosis Screening
 2. Methods of Tuberculosis Screening Diagnosis of active or latent TB involves a number of tests. There is no gold standard for determining whether a person is infected with M. tuberculosis but in practice
2. Methods of Tuberculosis Screening Diagnosis of active or latent TB involves a number of tests. There is no gold standard for determining whether a person is infected with M. tuberculosis but in practice
Title: Role of Interferon-gamma Release Assays in the Diagnosis of Pulmonary Tuberculosis in Patients with Advanced HIV infection
 Author's response to reviews Title: Role of Interferon-gamma Release Assays in the Diagnosis of Pulmonary Tuberculosis in Patients with Advanced HIV infection Authors: Adithya Cattamanchi (acattamanchi@medsfgh.ucsf.edu)
Author's response to reviews Title: Role of Interferon-gamma Release Assays in the Diagnosis of Pulmonary Tuberculosis in Patients with Advanced HIV infection Authors: Adithya Cattamanchi (acattamanchi@medsfgh.ucsf.edu)
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Identifying TB co-infection : new approaches?
 Identifying TB co-infection : new approaches? Charoen Chuchottaworn MD. Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH Primary tuberculosis Natural history
Identifying TB co-infection : new approaches? Charoen Chuchottaworn MD. Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH Primary tuberculosis Natural history
Clinical and Public Health Impact of Nucleic Acid Amplification Tests (NAATs) for Tuberculosis
 for Tuberculosis") Clinical and Public Health Impact of Nucleic Acid Amplification Tests (NAATs) for Tuberculosis Amit S. Chitnis, MD, MPH; Pennan M. Barry, MD, MPH; Jennifer M. Flood, MD, MPH. California Tuberculosis Controllers
Clinical and Public Health Impact of Nucleic Acid Amplification Tests (NAATs) for Tuberculosis Amit S. Chitnis, MD, MPH; Pennan M. Barry, MD, MPH; Jennifer M. Flood, MD, MPH. California Tuberculosis Controllers
Evidence-based use of the new diagnostic tools for TB-infection
 Evidence-based use of the new diagnostic tools for TB-infection Roland Diel, MD, MPH German Central Committee against Tuberculosis, Germany 20. Tuberkulose-Symposium in Münchenwiler, 24 th March 2011 1
Evidence-based use of the new diagnostic tools for TB-infection Roland Diel, MD, MPH German Central Committee against Tuberculosis, Germany 20. Tuberkulose-Symposium in Münchenwiler, 24 th March 2011 1
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Diagnosis of TB: Laboratory Ken Jost, BA November 12, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas November 11 14, 2014 Diagnosis of TB: Laboratory Ken Jost, BA November 12, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
Screening and management of latent TB Infection Gerry Davies
 Screening and management of latent TB Infection Gerry Davies Reader in Infection Pharmacology Institutes of Infection and Global Health & Translational Medicine HIV Scientific Meeting Liverpool 21st July
Screening and management of latent TB Infection Gerry Davies Reader in Infection Pharmacology Institutes of Infection and Global Health & Translational Medicine HIV Scientific Meeting Liverpool 21st July
Clinical Policy Title: Interferon-gamma release assays for tuberculosis screening
 Clinical Policy Title: Interferon-gamma release assays for tuberculosis screening Clinical Policy Number: 07.01.06 Effective Date: March 1, 2014 Initial Review Date: November 20, 2013 Most Recent Review
Clinical Policy Title: Interferon-gamma release assays for tuberculosis screening Clinical Policy Number: 07.01.06 Effective Date: March 1, 2014 Initial Review Date: November 20, 2013 Most Recent Review
Frances Morgan, PhD October 21, Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS
 The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Laboratory Diagnosis of Tuberculosis: State-of-the-art
 World Clin Pulm Crit Care Med. 2014;3(1):66-78. Laboratory Diagnosis of Tuberculosis: State-of-the-art Madhukar Pai MD PhD Department of Epidemiology and Biostatistics, McGill International TB Center,
World Clin Pulm Crit Care Med. 2014;3(1):66-78. Laboratory Diagnosis of Tuberculosis: State-of-the-art Madhukar Pai MD PhD Department of Epidemiology and Biostatistics, McGill International TB Center,
CULTURE OR PCR WHAT IS
 CULTURE OR PCR WHAT IS BEST FOR AFRICA? Peter R Mason BRTI TB IN AFRICA GLOBAL 9 MILLION NEW CASES/YR 1.5 MILLION TB DEATHS AFRICA 95% TB DEATHS IN LMIC 9/22 HIGH BURDEN COUNTRIES IN AFRICA STRONG LINK
CULTURE OR PCR WHAT IS BEST FOR AFRICA? Peter R Mason BRTI TB IN AFRICA GLOBAL 9 MILLION NEW CASES/YR 1.5 MILLION TB DEATHS AFRICA 95% TB DEATHS IN LMIC 9/22 HIGH BURDEN COUNTRIES IN AFRICA STRONG LINK
WELCOME. Lab Talk: What a Nurse Hears. April 18, NTNC Annual Meeting Lab Talk: What a Nurse Hears
 Lab Talk: What a Lab Talk: What a Max Salfinger, MD, FIDSA, FAAM Executive Director, Advanced Diagnostic Laboratories Laboratory Director, Mycobacteriology & Pharmacokinetics National Jewish Health Lisa
Lab Talk: What a Lab Talk: What a Max Salfinger, MD, FIDSA, FAAM Executive Director, Advanced Diagnostic Laboratories Laboratory Director, Mycobacteriology & Pharmacokinetics National Jewish Health Lisa
Diagnostic challenges of active childhood TB in Tanzania. Michala Vaaben Rose, MD, Ph.D Department of Infectious Diseases, Hvidovre
 Diagnostic challenges of active childhood TB in Tanzania Michala Vaaben Rose, MD, Ph.D Department of Infectious Diseases, Hvidovre 1 Diagnosis of Childhood Tuberculosis Muheza hospital, TZ Hilleroedhospital.dk
Diagnostic challenges of active childhood TB in Tanzania Michala Vaaben Rose, MD, Ph.D Department of Infectious Diseases, Hvidovre 1 Diagnosis of Childhood Tuberculosis Muheza hospital, TZ Hilleroedhospital.dk
Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011 Douglas Hornick, MD has the following disclosures to
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011 Douglas Hornick, MD has the following disclosures to
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA)
 and Interferon-gamma Release Assays (IGRA)") Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2019 Bob Belknap M.D. Director, Denver Metro TB Program Disclosures No relevant financial relationships Objectives Be able to
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2019 Bob Belknap M.D. Director, Denver Metro TB Program Disclosures No relevant financial relationships Objectives Be able to