Role of the Laboratory in TB Diagnosis and Management
|
|
|
- Erik Grant
- 6 years ago
- Views:
Transcription
1 Role of the Laboratory in TB Diagnosis and Management Michael Pentella, Ph.D., D(ABMM), CIC Associate Director University Hygienic Lab Clinical Associate Professor, College of Public Health, University of Iowa
2 Objectives At the completion of this TB webinar, participants will: Be familiar with the tests to diagnose latent tuberculosis and active tuberculosis Recognize the tests available to detect Mycobacterium tuberculosis in clinical specimens Understand the value of molecular tests to detect TB

3 History of TB Diagnostics Robert Koch announced in 1882 that he had found a microbe, Mycobacterium tuberculosis, that was the cause of "White Death", a disease responsible for one-seventh of all deaths in Europe in the late part of the 1800's.
4 Timeline of TB Infection Exposure 4-6 wks Adaptive T cell response Latent TB (LTBI)* Yrs-decades Lifelong Containment Active TB *Prevention efforts focus on detecting LTBI, most LTBI do not advance to active disease but those patients are at high risk particularly if they become immunocompromised.
5 TB Infection vs. TB Disease TB in the body Chest X-ray normal Sputum not done No symptoms Not infectious Not a case of TB TB in the body Chest X-ray abnormal Sputum smear and culture positive Symptoms: cough, fever, weight loss Infectious Case of TB
6 TB Algorithm Collect sputum specimens at 3 different times and 8 hours apart (at least one must be a first morning specimen) for AFB smear and mycobacterial culture. Perform MTD or NAAT test on the first smear positive sputum specimen
 Blood Test (IGRA) AFB (Acid Fast Bacilli) microscopy of sputum")
 Molecular probes PCR Sensitivity Testing")
7 Diagnosis of TB Clinical picture History and symptoms Chest XRay Antigen Test Skin test (TST) Blood Test (IGRA) AFB (Acid Fast Bacilli) microscopy of sputum NAAT Testing Culture (up to 6 weeks) Solid medium Liquid (MGIT) Nucleic Acid Amplification Testing (NAAT) Molecular probes PCR Sensitivity Testing Genotyping
8 Requirements to get a high quality specimen to the laboratory Collect specimens before therapy started Even after a few days of therapy, AFB may be killed or numbers decreased to longer be detectable Specimens must be handled properly to guarantee successful cultures Promptly transport specimens
9 Specimen Type: Varies with Pulmonary symptoms Sputum (spontaneous, induced) Bronchoalveolar Lavage Gastric Lavage (children) Tissue and Body fluids (CSF, pleural, blood) Wounds, skin lesions (exudates)
10 Specimen Collection and Processing: special considerations Biohazard Aerosol transmission Prevent contamination of specimen Slow growth rate of TB Evaluate at least 3 specimens per patient
11 Sputum collection considerations Instruct patients that nasopharyngeal discharge and saliva are not sputum Sputum = thick, yellowish (sometimes blood-tinged) exudative material brought up from the lungs after a deep, productive cough First rinse mouth with mouthwash to decrease bacterial contamination Collect specimen into appropriate container
12 Sputum cont About 10 ml of sputum is sufficient If patient cannot provide an adequate specimen then sputum induction is acceptable Warm, aerosolized hypertonic salt solution Be certain to label the specimen as induced sputum
13 Specimen Transport From the time of collection until the specimen is processed, the other bacteria present will over grow (contaminate) the slower growing Mycobacteria sp. Speed is important Courier Ship cold when possible Shipping cold slows bacterial growth
14 Specimen Processing If collected from a non-sterile site (sputum), then digest and decontaminate before culture Kill off other microbes Liquefy mucin Remove organic debris Homogenize tissue N-acetyl-L-cysteine (NALC)-NaOH method Concentrate specimen
15 Summary of Standard Diagnostic Techniques Direct from specimen AFB Smear cold kinyoun and fluorescent Culture in broth and on solid media Direct detection by NAAT From growth of organism Probe (accuprobe) Biochemicals 16S ribosomal RNA Sensitivity Testing
16 TB Specimen Processing Specimen Culture Smear Positive Probe Biochemical Sensitivity Genotyping NAAT
17 Laboratory Tests: Non-specific AFB smear Semi-quantitative as a measure of patient infectiousness Culture Liquid and solid media (up to 6 weeks) Automated commercial systems widely used Semi-quantitative


18 Diagnosis of TB: AFB Smear Microscopy Make a smear on a slide Stain for acid-fast bacteria Cold Kinyoun Ziehl Neelsen Fluorochrome (Auramine-Rhodamine)
19 Diagnosis of TB: AFB Smear Strengths Microscopy Easy, fast, cheap (ZN) Weakness 50-60% of TB patients are smear negative Need at least 10,000 CFU/ml sputum for positive result Cannot differentiate Mycobacteria species
20 Importance of acid-fast bacilli smear microscopy as a primary diagnostic tool Initial diagnosis Monitoring treatment Determination of time to release from isolation
21 How sensitive is the smear? Peterson et. al. JCM 1999 vol. 37: Number of specimens Direct AFB smear sensitivity Concentrated AFB smear sensitivity Comment 353 culture positive for Mycobacteria 208 cultures positive for M. tuberculosis Analysis of 3 specimens per patient 34% 58% Direct smear cannot be relied on 42% 74% Concentrated smear most reliable 81% 91% Concentrated smear is still the most reliable
 GeneXpert")
22 Direct detection of TB in the specimen MTD test Genprobe transcription mediated amplification In house developed Nucleic Acid Amplification test (NAAT) GeneXpert Cepheid NAAT
23 Interpretation of NAAT Result Smear NAAT Interpretation + + Presumed Positive TB, No Additional Testing + -- If first sputum specimen: smear positive and NAAT-negative, repeat on one additional specimens, if negative then presume negative for TB Additional specimens (limit 2). Presumptive positive for TB if the subsequent specimen positive Presumptive negative for TB. Two specimens recommended.
24 TB NAAT Algorithm Respiratory Specimen Smear Positive Smear Negative NAAT NAAT Positive: Presumed TB, pending culture results Negative Use clinical judgment to determine whether to begin therapy while awaiting culture results and determine if additional diagnostic testing is needed. Consider testing another specimen (not to exceed a total of two). If a second specimen is smear positive, NAAT negative, the patient is presumed to have an infection with non-tuberculous mycobacteria, pending culture results. Inhibitors Detected: Test result is of no diagnostic help. Consider testing second specimen (not to exceed a total of two). Positive Use clinical judgment to determine whether to begin therapy while awaiting culture results and determine if additional diagnostic testing is needed. Consider testing another specimen (not to exceed a total of two). NAAT Positive: A patient can be presumed to have tuberculosis, pending culture results, if two specimens are NAA positive. Negative Use clinical judgment to determine whether to begin therapy while awaiting results of culture and other diagnostic tests. Currently available NAA tests are not sufficiently sensitive to exclude the diagnosis of TB in AFB smear negative patients suspected of having TB.

25 Diagnosis of TB: Culture Solid Media Culutre Agar Middlebrook 7H10/7H11 Egg based Lowenstein-Jensen Liquid Broth Culture 7H9 Commercial broth and monitoring systems Becton Dickinson MGIT ThermoScientific, TREK Diagnostic Systems,Versa TREK Myco Use a solid and a liquid media
 of cell wall mycolic acids Molecular probes Culture")
26 Laboratory Tests: Specific Biochemical tests Require sub-culture Ex. Niacin, Nitrate, Tween 80 Hydrolysis, 68 Catalase High performance liquid chromatography (HPLC) of cell wall mycolic acids Molecular probes Culture confirmation Direct from growth in broth or on slant DNA sequence analysis 16S rrna gene
27 Molecular Probes for Mycobacteria identification MYCOBACTERIUM TUBERCULOSIS Complex Culture Identification Test For identification of M. tuberculosis, M. bovis, M. bovis (BCG), M. africanum, M. canetti, M. microti etc. isolated from culture. MYCOBACTERIUM AVIUM Culture Identification Test - For the identification of Mycobacterium avium isolated from culture. MYCOBACTERIUM INTRACELLULARE Culture Identification Test - For the identification of Mycobacterium intracellulare isolated from culture. MYCOBACTERIUM AVIUM Complex Culture Identification Test - For the identification of Mycobacterium avium complex (M. avium, M. intracellulare, and other members) isolated from culture. MYCOBACTERIUM GORDONAE Culture Identification Test - For the identification of Mycobacterium gordonae isolated from culture. MYCOBACTERIUM KANSASII Culture Identification Test - For the identification of Mycobacterium kansasii isolated from culture.

28 Molecular Probe Performance Characteristics Organism Sensitivity Specificity M avium 99.3% 100% M intracellulare 100% 100% M avium complex 99.9% 100% M gordonae 98.8% 99.7% M kansasii 92.8% 100% M tuberculosis complex 99.2% 99.0%
")
29 Biochemical tests for M. tuberculosis complex 8 species make up the complex Mycobacterium tuberculosis Mycobacterium africanum Mycobacterium bovis Mycobacterium bovis (BCG) Mycobacterium microti Mycobacterium canettii Mycobacterium pinnipedii Mycobacterium mungi Differentiate by biochemical testing Niacin Nitrate Others
30 Antimicrobial susceptibility testing Required for all MTB complex patients Absolute concentration Resistance ratio Proportion Recommended for some NTM species
31 Drug susceptibility testing of M. tuberculosis Culture based DST remains the gold std Reliable for INH & Rif, inconsistent for Ethambutol resistance Genotypic methods Sequencing Line probe hybridization assays (commercial) Molecular beacons (GeneXpert) Loop mediated isothermal amplification
32
33 Genotyping MMWR Controlling TB in the US Nov skforceplan/strategies_accelerate.htm Refers to procedures to identify M. tuberculosis isolates that are identical in specific parts of the genome Along with epi investigation, genotype used to confirm transmission

34 CDC program for genotyping M. tuberculosis isolates DNA Fingerprinting Restriction Fragment Length Polymorphism (RFLP)
35
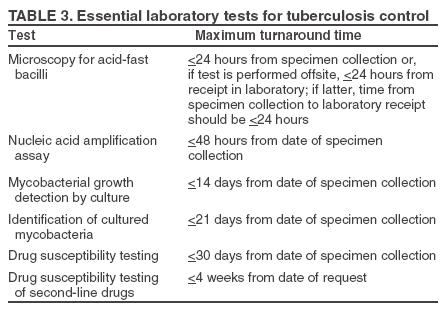
36 What are the expected TAT? Test Standard SHL AFB smear <24 h 7 h NAAT <48 h <24 h Growth in culture <14 d NA ID of culture <21 d 14 d Sensitivity Testing <30 d 21 d

37 Tuberculin Skin Test (TST) In routine use since 1910 TST is the most used test for M. tuberculosis infection in U.S. Delayed type hypersensitivity reaction to PPD, a polyvalent mycobacterial antigen mixture
38 TST Pro s Con s Advantages Inexpensive Good performance No special equipment Long history of experience Limitations Reader variability Boost response Low specificity Cross reaction with BCG and NTM Low sensitivity Need for 2 visits

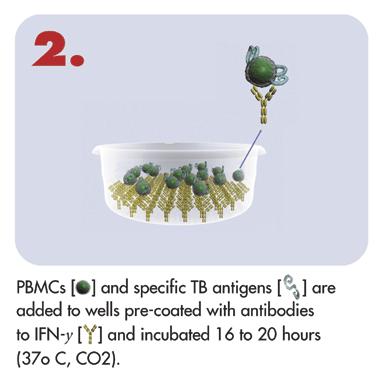
39 Interferon Gamma Release Assays: Principle: Persons exposed to M. tuberculosis develop T-cells (lymphocytes that recognize and respond to TB-specific antigens Dendritic cell processes antigen and presents antigen to T Cell
 Antigens ESAT 6 & CFP 10 T cell")
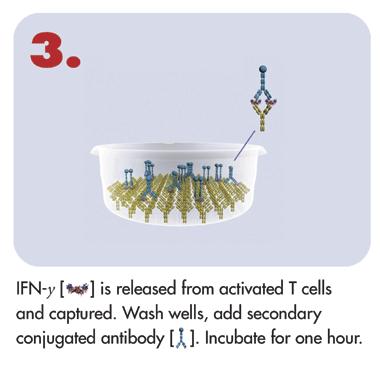
40 IGRA (continued) When stimulated with TB-specific antigens, these primed T-cells release the cytokine, interferon-gamma (IFN- γ) Antigens ESAT 6 & CFP 10 T cell releases IFN- γ

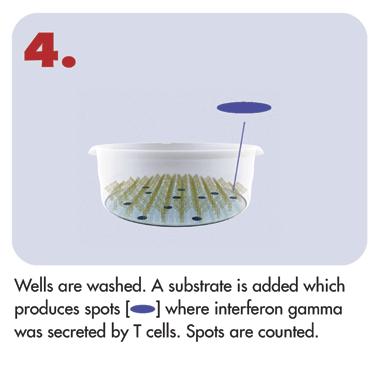
41 IGRA (continued) The released IFN- γ can then be detected and serves as an indirect indicator of exposure to TB.


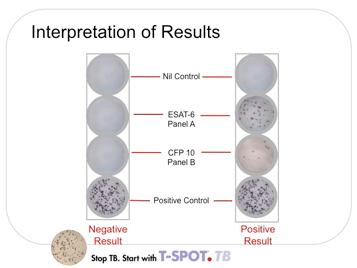
42 T-SPOT FDA approved August
43 mmunotec.com/ho w_it_works_north _America

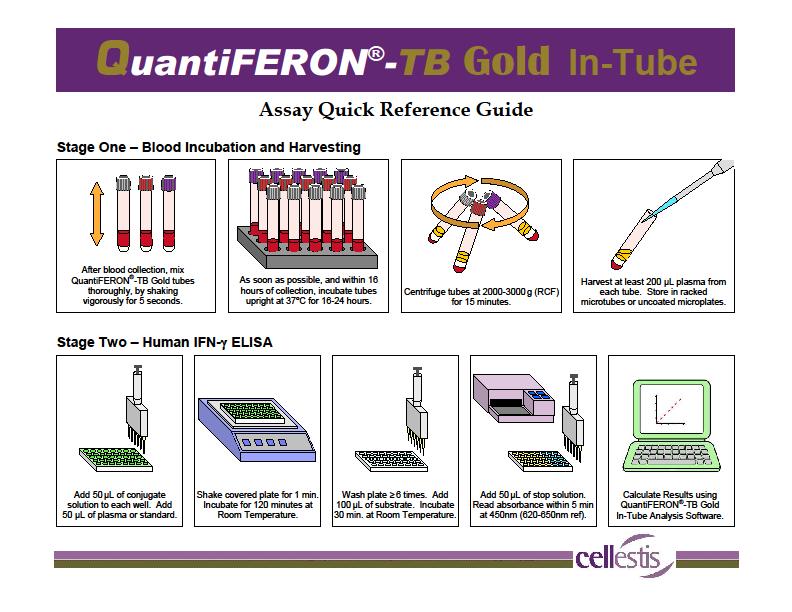
44 QuantiFERON TB- Gold In-Tube Blood test that measures and compares amount of interferon-gamma (IFN-γ) released by blood cells in response to antigens FDA approved in May 2005 Cellestis, Carnegie, Australia TB


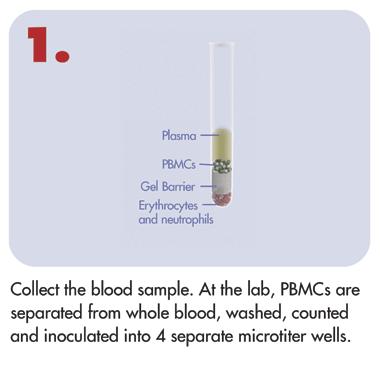
45 QFT Procedure Clinic and Lab Procedures in Clinic Blood Collection Shaking of Tubes Blood Incubation Plasma Separation Procedures in Lab ELISA Data Analysis
46
47 Data Analysis and Results Results are reported as Positive Negative Indeterminate Indeterminate Low mitogen CMI response High Nil live vaccines secondary infection
48 Technology Comparison T-SPOT QFTB In Tube TST Antigens ESAT-6 & CFP10 ESAT-6, CFP10, TB7.7 Boosting effect with repeat tests PPD No No Yes TAT h h h Readout units IFN-Gamma spot forming cells International units of IFN-Gamma Technology ELISpot ELISA NA Readout system Count of spots Measurement of optical density values using an automated reader Subjective Reading Yes No Yes Millimeters of induration Palpable induration
49
50 CDC advises that IGRA s can be used in all circumstances in which the TST is used, including Contact investigations Evaluation of recent immigrants who have had BCG vaccination TB screening of health care workers and other individuals in high risk settings IGRA is in place of (not an addition to) TST
51 General Benefits of IGRA over TST Requires only one patient visit Assesses responsiveness to M. tuberculosis antigens Does not boost previous responses Interpretation less subjective than for TST
52 Limitations of IGRAs Cross-reactivity is possible with some atypical Mycobacteria infections: M. kansasii, M.szulgai, and M. marinum Testing logistics: Specimen transport time Requirement for specialized testing equipment Additional data needed in certain patient populations Children, Immunocompromised, Pregnancy
53 BCG Vaccinated Patients IGRA benefit the BCG vaccinated patient Many false positive TST due to vaccination status Treatment is costly, carries risk of significant side effects Treatment is not always needed since most do not have LTBI


54 Performance of IGRAs and the TST: An up-to-date TB Test Meta-Analysis R Diel, R Loddenkemper and A Nienhaus Evidence based comparison of commercial interferon-gamma release assays for detecting active tuberculosis a meta-analysis. Chest, 2009, Published on Dec 18, 2009 in electronic format; Chest April : ; doi: /chest
55 Contact Investigations For persons with recent TB exposure, negative IGRA results should be confirmed with a repeat test 8-10 weeks after exposure (end of window period) per CDC. This is the same as for a negative TST. Yoshiyama, et al. Timing of Quantiferon TB-G test for the contact examination of tuberculosis. Kekkaku Aug;82(8): months interval from the diagnosis of the index case will be enough for the final decision of the infection of contacts. N=25, 8 positive QFTB-G
56 For high risk contacts When window prophylaxis has been started for high-risk contacts exposed to an infectious TB patient, a negative IGRA result at the end of the window period should be interpreted in light of all other clinical and epi data A full course of LTBI TX should be considered even with a negative result when the rate of TB transmission to other contacts is high or when a false-negative is suspected because of immune status.
57 Use of IGRA Baseline and Serial Testing Baseline testing with IGRA Establish baseline with single negative IGRA HCWs with positive IGRA result should be referred for diagnostic evaluation Serial testing for infection control A conversion is a change from negative to positive


58 Cost Barrier? Cost-effective alternative to TST Reduction in false positive test results No second visit needed to complete testing Two-step testing not needed Reduction in rates of CXR (due to higher specificity for M. tuberculosis)
59 Are IGRAs cost effective? DePerio et al: Arch Intern Med Use of IGRA leads to superior clinical outcomes and lower costs than the TST and should be considered in screening non-bcgvaccinated and BCG vaccinated new HCWs for LTBI. Marra et al: Int J Tuberc Lung Dis Selected use of QFT-G appears to be cost effective if used in targeted fashion.

60 IGRA Summary IGRAs are more specific than TST and are not confounded by previous BCG vaccination Less unnecessary preventive treatment IGRA are more sensitive than TST
61 TB antibody tests Tests that detect IgG antibody to TB Highly variable results for sensitivity and specificity Do not have a roll in the diagnosis of TB Not FDA approved Recently confused with IGRA in the news.
62 Take Home Message Culture of TB remains the gold standard AFB smears are the most cost effective NAAT are sensitive and rapid but cannot differentiate between dead and viable TB IGRA do not differentiate between active and latent TB There are new tests on the horizon

63 Let s not forget
64 Bibliography Requirements to get a high quality specimen to the laboratory Salfinger, M, and AJ Morris The role of the microbiology laboratory in diagnosing mycobacterial diseases. American Journal of Clinical Pathology. 101: S6-13. Standard diagnostic techniques for the detection and identification of Mycobacteria Chegou, NN, et.al Tuberculosis assays: past, present and future. Expert Reviews in Anti Infective Therapy. 9(4): Importance of acid-fast bacilli smear microscopy as a primary diagnostic tool Peterson, EM, et.al Comparison of direct and concentrated acid-fast smears to identify specimens culture positive for Mycobacterium species. Journal of Clinical Microbiology. 37(11): Drug susceptibility testing of M. tuberculosis O Grady, J. et.al New and improved diagnostics for detection of drug-resistant pulmonary tuberculosis. Current Opinion in Pulmonary Medicine. 17(3): Rapid methods for the identification and drug susceptibility testing of M. tuberculosis as they compare to the traditional methods Lalvani A Diagnosing tuberculosis infection in the 21st century: new tools to tackle an old enemy. Chest 131: CDC program for genotyping M. tuberculosis isolates Kato-Maeda, M, JZ Metcalfe, and L Flores Genotyping of Mycobacterium tuberculosis: application in epidemiologic studies. Future Microbiology (2): Interferon Gamma Assays (IGRA) Pro s and Con s Diel, R. et.al Evidence-based comparison of commercial interferon-gamma release assays for detecting active TB: a metaanalysis. Chest. 137:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Role of the Laboratory in the TB Diagnosis and Management Michael Pentella, PhD, MS, SM(ASCP), CIC, D(ABMM) September 27, 2011 Michael Pentella,
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Role of the Laboratory in the TB Diagnosis and Management Michael Pentella, PhD, MS, SM(ASCP), CIC, D(ABMM) September 27, 2011 Michael Pentella,
TB Laboratory for Nurses
 TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Ken Jost, BA, has the following disclosures to make:
 Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
TB 101 Disease, Clinical Assessment and Lab Testing
 TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
TB Intensive Tyler, Texas December 2-4, 2008
 TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
The ABC s of AFB s Laboratory Testing for Tuberculosis. Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory
 The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Frances Morgan, PhD October 21, Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS
 The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
CDPH - CTCA Joint Guidelines Guideline for Micobacteriology Services In California
 CDPH - CTCA Joint Guidelines Guideline for Micobacteriology Services In California These guidelines are intended to be used as an educational aid to help clinicians make informed decisions about patient
CDPH - CTCA Joint Guidelines Guideline for Micobacteriology Services In California These guidelines are intended to be used as an educational aid to help clinicians make informed decisions about patient
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014
 TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
Overview of Mycobacterial Culture, Identification, and Drug Susceptibility Testing
 Overview of Mycobacterial Culture, Identification, and Drug Susceptibility Testing 1. Essentials for the Mycobacteriology Laboratory: Promoting Quality Practices 1.1 Overview: Mycobacterial Culture, Identification,
Overview of Mycobacterial Culture, Identification, and Drug Susceptibility Testing 1. Essentials for the Mycobacteriology Laboratory: Promoting Quality Practices 1.1 Overview: Mycobacterial Culture, Identification,
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Stacy White, PhD May 12, TB for Community Providers. Phoenix, Arizona
 Role of the Laboratory in TB Diagnosis Stacy White, PhD May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Stacy White, PhD has the following disclosures
Role of the Laboratory in TB Diagnosis Stacy White, PhD May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Stacy White, PhD has the following disclosures
Diagnosis of TB: Laboratory Ken Jost Tuesday April 9, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 Diagnosis of TB: Laboratory Ken Jost Tuesday April 9, 2013 Ken Jost has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 Diagnosis of TB: Laboratory Ken Jost Tuesday April 9, 2013 Ken Jost has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Diagnosis of TB: Laboratory Ken Jost, BA November 12, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas November 11 14, 2014 Diagnosis of TB: Laboratory Ken Jost, BA November 12, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
Receipt within 1 day of specimen collection. Report AFB b smear result within 1 day from receipt of specimen
 Recommendation Promote rapid delivery of specimens to the laboratory Use fluorescent acid-fast staining and promptly transmit results by phone, FAX, or electronically Identify growth as acid-fast and use
Recommendation Promote rapid delivery of specimens to the laboratory Use fluorescent acid-fast staining and promptly transmit results by phone, FAX, or electronically Identify growth as acid-fast and use
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Public Health Mycobacteriology (TB) Laboratory Testing Services
 Laboratory Testing Services") Public Health Mycobacteriology (TB) Laboratory Testing Services Gary Budnick Supervising Microbiologist Connecticut Department of Public Health Laboratory Branch Hartford, Connecticut Specimen Collection
Public Health Mycobacteriology (TB) Laboratory Testing Services Gary Budnick Supervising Microbiologist Connecticut Department of Public Health Laboratory Branch Hartford, Connecticut Specimen Collection
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
Nucleic Acid Amplification Testing for the Diagnosis of TB
 Roche Nucleic Acid Amplification Testing for the Diagnosis of TB David Warshauer, PhD Deputy Director, Communicable Diseases Wisconsin State Laboratory of Hygiene 19 th /20 th Century Traditional Algorithm
Roche Nucleic Acid Amplification Testing for the Diagnosis of TB David Warshauer, PhD Deputy Director, Communicable Diseases Wisconsin State Laboratory of Hygiene 19 th /20 th Century Traditional Algorithm
Technical Bulletin No. 172
 CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
Peggy Leslie-Smith, RN
 Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
A Clinician s Guide to the TB Laboratory
 A Clinician s Guide to the TB Laboratory EXCELLENCE EXPERTISE INNOVATION Dear Healthcare Professional, This book provides basic information on the use of the public health and clinical laboratories in
A Clinician s Guide to the TB Laboratory EXCELLENCE EXPERTISE INNOVATION Dear Healthcare Professional, This book provides basic information on the use of the public health and clinical laboratories in
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Mycobacterial cell wall. Cell Cycle Lengths. Outline of Laboratory Methods. Laboratory Methods
 Laboratory Methods Cell Cycle Lengths Generation time (hrs) Days needed for 26 generations (colony) E. coli 0.33 0.36 Nancy Connell, PhD Professor, nfectious Disease Department of Medicine Center for Emerging
Laboratory Methods Cell Cycle Lengths Generation time (hrs) Days needed for 26 generations (colony) E. coli 0.33 0.36 Nancy Connell, PhD Professor, nfectious Disease Department of Medicine Center for Emerging
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Research Methods for TB Diagnostics. Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012
 Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Diagnosis of tuberculosis
 Diagnosis of tuberculosis Madhukar Pai, MD, PhD Assistant Professor, Epidemiology McGill University, Montreal, Canada madhukar.pai@mcgill.ca Global TB Case Detection A major concern 2.6 million new smear
Diagnosis of tuberculosis Madhukar Pai, MD, PhD Assistant Professor, Epidemiology McGill University, Montreal, Canada madhukar.pai@mcgill.ca Global TB Case Detection A major concern 2.6 million new smear
Conflict of Interest Disclosures:
 Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
TB Nurse Case Management. March 7-9, Diagnosis of TB: Ken Jost Wednesday March 7, 2012
 TB Nurse Case Management San Antonio, Texas March 7-9, 2012 Diagnosis of TB: Laboratory Ken Jost Wednesday March 7, 2012 Ken Jost has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7-9, 2012 Diagnosis of TB: Laboratory Ken Jost Wednesday March 7, 2012 Ken Jost has the following disclosures to make: No conflict of interests No relevant
Objectives. TB Laboratory Methods
 TB Laboratory Methods Beverly Metchock, Dr.P.H., D(ABMM) Team Leader, Reference Laboratory, Mycobacteriology Laboratory Branch February 2011 Objectives General overview of mycobacteriology (TB) lab practices
TB Laboratory Methods Beverly Metchock, Dr.P.H., D(ABMM) Team Leader, Reference Laboratory, Mycobacteriology Laboratory Branch February 2011 Objectives General overview of mycobacteriology (TB) lab practices
NOLA TB TIMES. TB Diagnostics A Special Issue. on TB Diagnosis 101. Diagnostic Discrepancy Data. Comprehensive Approach
 NOLA TB TIMES Volume 1, No 3 February 2016 TB Diagnostics A Special Issue on TB Diagnosis 101 Happy New Year and Happy Mardi Gras to everyone! We already have seven presumptive cases of tuberculosis (TB)
NOLA TB TIMES Volume 1, No 3 February 2016 TB Diagnostics A Special Issue on TB Diagnosis 101 Happy New Year and Happy Mardi Gras to everyone! We already have seven presumptive cases of tuberculosis (TB)
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
TB is Local. Barry Chin, Boston Globe, 10/15/2008. * BUT only in appropriate setting
 Diagnosis of Tuberculosis 2012 New Tools, Tricks, Thinking? John Bernardo, M.D. Pulmonary Section, Boston University School of Medicine Massachusetts Department of Public Health Objectives To review the
Diagnosis of Tuberculosis 2012 New Tools, Tricks, Thinking? John Bernardo, M.D. Pulmonary Section, Boston University School of Medicine Massachusetts Department of Public Health Objectives To review the
WELCOME. Lab Talk: What a Nurse Hears. April 18, NTNC Annual Meeting Lab Talk: What a Nurse Hears
 Lab Talk: What a Lab Talk: What a Max Salfinger, MD, FIDSA, FAAM Executive Director, Advanced Diagnostic Laboratories Laboratory Director, Mycobacteriology & Pharmacokinetics National Jewish Health Lisa
Lab Talk: What a Lab Talk: What a Max Salfinger, MD, FIDSA, FAAM Executive Director, Advanced Diagnostic Laboratories Laboratory Director, Mycobacteriology & Pharmacokinetics National Jewish Health Lisa
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Using Interferon Gamma Release Assays for Diagnosis of TB Infection
 Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
MYCOBACTERIUM. Mycobacterium Tuberculosis (Mtb) nontuberculous mycobacteria (NTM) Mycobacterium lepray
 nontuberculous mycobacteria (NTM) Mycobacterium lepray") MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Chapter 4 Diagnosis of Tuberculosis Disease
 Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE
 Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Principles of laboratory diagnosis of M. tuberculosis. Anne-Marie Demers, MD, FRCPC 11 September 2017
 Principles of laboratory diagnosis of M. tuberculosis Anne-Marie Demers, MD, FRCPC 11 September 2017 QUESTION Which statement is false? 1) A smear can only be on a concentrated specimen 2) It is normal
Principles of laboratory diagnosis of M. tuberculosis Anne-Marie Demers, MD, FRCPC 11 September 2017 QUESTION Which statement is false? 1) A smear can only be on a concentrated specimen 2) It is normal
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Guidelines for Tuberculosis Control in New Zealand 2010 Chapter 11: Mycobacteriology: Laboratory Methods and Standards
 Guidelines for Tuberculosis Control in New Zealand 2010 Chapter 11: Mycobacteriology: Laboratory Methods and Standards Ministry of Health. 2010. Guidelines for Tuberculosis Control in New Zealand 2010.
Guidelines for Tuberculosis Control in New Zealand 2010 Chapter 11: Mycobacteriology: Laboratory Methods and Standards Ministry of Health. 2010. Guidelines for Tuberculosis Control in New Zealand 2010.
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Detecting latent tuberculosis using interferon gamma release assays (IGRA)
") Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
Testing for TB. Bart Van Berckelaer Territory Manager Benelux. Subtitle
 Testing for TB Bart Van Berckelaer Territory Manager Benelux Subtitle Agenda TB infection pathway TB immunisation Testing options Pre lab considerations of the whole blood ELISA test The T-SPOT.TB test
Testing for TB Bart Van Berckelaer Territory Manager Benelux Subtitle Agenda TB infection pathway TB immunisation Testing options Pre lab considerations of the whole blood ELISA test The T-SPOT.TB test
Nucleic Acid Amplification Test for Tuberculosis. Heidi Behm, RN, MPH Acting TB Controller HIV/STD/TB Program Oregon, Department of Health Services
 Nucleic Acid Amplification Test for Tuberculosis Heidi Behm, RN, MPH Acting TB Controller HIV/STD/TB Program Oregon, Department of Health Services What is this test? Nucleic Acid Amplification Test (NAAT)
Nucleic Acid Amplification Test for Tuberculosis Heidi Behm, RN, MPH Acting TB Controller HIV/STD/TB Program Oregon, Department of Health Services What is this test? Nucleic Acid Amplification Test (NAAT)
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Use of the Cepheid GeneXpert to Release Patients from Airborne Isolation
 Use of the Cepheid GeneXpert to Release Patients from Airborne Isolation Dave Warshauer, PhD, D(ABMM) Deputy Director, Communicable Diseases Wisconsin State Laboratory of Hygiene WISCONSIN STATE LABORATORY
Use of the Cepheid GeneXpert to Release Patients from Airborne Isolation Dave Warshauer, PhD, D(ABMM) Deputy Director, Communicable Diseases Wisconsin State Laboratory of Hygiene WISCONSIN STATE LABORATORY
New Standards for an Old Disease:
 New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
AFB Identification Texas Approach
 AFB Identification Texas Approach Ken Jost Texas Department of State Health Services 6th National Conference on Laboratory Aspects of TB June 21, 2010 DSHS-Austin TB Lab Customers & Samples Year 2009 175
AFB Identification Texas Approach Ken Jost Texas Department of State Health Services 6th National Conference on Laboratory Aspects of TB June 21, 2010 DSHS-Austin TB Lab Customers & Samples Year 2009 175
The Origin of Swine Flu
 How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Laboratory Diagnostic Techniques. Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust
 Laboratory Diagnostic Techniques Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust Learning Objectives 1) When to consider a diagnosis of TB 2) When to consider a referral
Laboratory Diagnostic Techniques Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust Learning Objectives 1) When to consider a diagnosis of TB 2) When to consider a referral
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Appendix B. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
MYCOBACTERIOLOGY SERVICE MANUAL
 MYCOBACTERIOLOGY SERVICE MANUAL The Office of Laboratory Services (OLS) provides primary isolation and identification of Mycobacterium species in human diagnostic specimens. Reference specimens of AFB
MYCOBACTERIOLOGY SERVICE MANUAL The Office of Laboratory Services (OLS) provides primary isolation and identification of Mycobacterium species in human diagnostic specimens. Reference specimens of AFB
Identifying TB co-infection : new approaches?
 Identifying TB co-infection : new approaches? Charoen Chuchottaworn MD. Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH Primary tuberculosis Natural history
Identifying TB co-infection : new approaches? Charoen Chuchottaworn MD. Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH Primary tuberculosis Natural history
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
WSLH Testing and Surveillance Updates
 WSLH Testing and Surveillance Updates Wisconsin Mycobacteriology Laboratory Network annual conference November 4, 2015, Madison, WI Updates Outline Collection and Transport Smear and Culture Nucleic Acid
WSLH Testing and Surveillance Updates Wisconsin Mycobacteriology Laboratory Network annual conference November 4, 2015, Madison, WI Updates Outline Collection and Transport Smear and Culture Nucleic Acid
2016 OPAM Mid-Year Educational Conference, Sponsored by AOCOPM Sunday, March 13, 2016
 Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
Xpert MTB/RIF Training. Indira Soundiram 2012
 Xpert MTB/RIF Training Indira Soundiram 2012 A Better Way to Platform Design GeneXpert Infinity-48 GeneXpert Module GX-I GX-II GX-IV GX-XVI 2 Defining Molecular Diagnostics Any Test Any Time Any Sample
Xpert MTB/RIF Training Indira Soundiram 2012 A Better Way to Platform Design GeneXpert Infinity-48 GeneXpert Module GX-I GX-II GX-IV GX-XVI 2 Defining Molecular Diagnostics Any Test Any Time Any Sample
The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over?
 The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over? ROY F. CHEMALY, MD, MPH, FIDSA, FACP PROFESSOR OF MEDICINE DIRECTOR, INFECTION CONTROL SECTION
The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over? ROY F. CHEMALY, MD, MPH, FIDSA, FACP PROFESSOR OF MEDICINE DIRECTOR, INFECTION CONTROL SECTION
IGRAs for Diagnosis of Tuberculosis: 2010 Update
 IGRAs for Diagnosis of Tuberculosis: 2010 Update Nira Pollock, M.D., Ph.D. Division of Infectious Diseases Beth Israel Deaconess Medical Center Boston, MA May 1, 2010 Problems with the PPD False positives
IGRAs for Diagnosis of Tuberculosis: 2010 Update Nira Pollock, M.D., Ph.D. Division of Infectious Diseases Beth Israel Deaconess Medical Center Boston, MA May 1, 2010 Problems with the PPD False positives
TB NAAT testing at the Los Angeles County Public Health Laboratory
 TB NAAT testing at the Los Angeles County Public Health Laboratory Hector Rivas Public Health Microbiology Supervisor II Los Angeles County Public Health Laboratory hrivas@ph.lacounty.gov April 2012 1
TB NAAT testing at the Los Angeles County Public Health Laboratory Hector Rivas Public Health Microbiology Supervisor II Los Angeles County Public Health Laboratory hrivas@ph.lacounty.gov April 2012 1
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Diagnosis and Management of Active Tuberculosis
 Diagnosis and Management of Active Tuberculosis Zelalem Temesgen, MD FIDSA AAHIVS 2013 MFMER slide-1 Disclosures None 2013 MFMER slide-2 Objectives By the end of this session, participants should be able
Diagnosis and Management of Active Tuberculosis Zelalem Temesgen, MD FIDSA AAHIVS 2013 MFMER slide-1 Disclosures None 2013 MFMER slide-2 Objectives By the end of this session, participants should be able
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
결핵노출접촉자감염관리 서울아산병원감염내과 김성한
 결핵노출접촉자감염관리 서울아산병원감염내과 김성한 TB incidence (2012) TB incidence South Korea 108 China 73 Taiwan 68 Portucal 26 Japan 19 Spain 14 US 3.6 * unit- per 100,000 population Adapted from WHO Adapted from WHO Emerg
결핵노출접촉자감염관리 서울아산병원감염내과 김성한 TB incidence (2012) TB incidence South Korea 108 China 73 Taiwan 68 Portucal 26 Japan 19 Spain 14 US 3.6 * unit- per 100,000 population Adapted from WHO Adapted from WHO Emerg
QuantiFERON-TB Gold Plus
 QuantiFERON-TB Gold Plus A New Interferon-γ Release Assay (IGRA) for the Indirect Detection of Mycobacterium tuberculosis HOT TOPIC / 2018 Presenter: Elitza S. Theel, PhD, D(ABMM) Director of Infectious
QuantiFERON-TB Gold Plus A New Interferon-γ Release Assay (IGRA) for the Indirect Detection of Mycobacterium tuberculosis HOT TOPIC / 2018 Presenter: Elitza S. Theel, PhD, D(ABMM) Director of Infectious
INTENSIFIED TB CASE FINDING
 INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
Microscopic Morphology in Smears Prepared from MGIT Broth Medium for Rapid Presumptive Identification of Mycobacterium tuberculosis
 Annals of Clinical & Laboratory Science, vol. 33, no. 2, 2003 179 Microscopic Morphology in Smears Prepared from MGIT Broth Medium for Rapid Presumptive Identification of Mycobacterium tuberculosis complex,
Annals of Clinical & Laboratory Science, vol. 33, no. 2, 2003 179 Microscopic Morphology in Smears Prepared from MGIT Broth Medium for Rapid Presumptive Identification of Mycobacterium tuberculosis complex,
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
New Tuberculosis Guidelines. Jason Stout, MD, MHS
 New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
THE ROLE OF THE LABORATORY
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 THE ROLE OF THE LABORATORY LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe three
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 THE ROLE OF THE LABORATORY LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe three
THE ROLE OF THE LABORATORY
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE THE ROLE OF THE LABORATORY LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe three laboratory methods
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE THE ROLE OF THE LABORATORY LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe three laboratory methods