Tuberculosis. Anne Dunleavy. Excellence in specialist and community healthcare
|
|
|
- Dennis Phelps
- 6 years ago
- Views:
Transcription


1 Tuberculosis Anne Dunleavy Excellence in specialist and community healthcare
2 Overview Epidemiology Illustrative cases Treatment Priorities Conclusion Presentation title / St George s University Hospitals NHS Foundation Trust


3 The White Plague

4 WHO /3 infected (2 billion) 10.4 million new cases 1.8 million deaths Tuberculosis/ St George s University Hospitals NHS Foundation Trust
5 Number of cases Rate (per 100,000) TB case notifications and rates, England, , , ,000 7, , , , ,000 2, , Year Number of cases Rate per 100,000 I 95% CI Tuberculosis in England: 2016 report Source: Enhanced Tuberculosis Surveillance system (ETS), Office for National Statistics (ONS) Data extracted: April 2016 Prepared by: TB Section, National Infection Service, Public Health England 6

6 Three-year average TB rates by local authority district, England, London Tuberculosis rate (per 100,000) >50.0 Tuberculosis in England: 2016 report Contains Ordnance Survey data Crown copyright and database right 2015 Contains National Statistics data Crown copyright and database right 2015 Source: Enhanced Tuberculosis Surveillance system (ETS), Office for National Statistics (ONS) Data extracted: April 2016 Prepared by: TB Section, National Infection Service, Public Health England 7
7 8
8 9
 North East, Yorkshire & the Humber (n=569, rate=7.1*) East Midlands (n=354, rate=7.6*) Lowest number of TB cases Lowest TB burden control board West Midlands (n=708, rate=12.")
9 TB case notifications and rates by TB control board, England, 2015 TB Number burden of TB cases Highest number of TB cases Highest TB burden control board North West (n=570, rate=7.9*) North East, Yorkshire & the Humber (n=569, rate=7.1*) East Midlands (n=354, rate=7.6*) Lowest number of TB cases Lowest TB burden control board West Midlands (n=708, rate=12.3*) East of England (n=393, rate=6.2*) South of England (n=893, rate=6.3*) London (n=2,269, rate=26.2*) * per 100,000 Contains Ordnance Survey data Crown copyright and database right 2015 Tuberculosis in England: 2016 report, version 1.2 Source: Enhanced Tuberculosis Surveillance system (ETS) Data extracted: April 2016 Prepared by: TB Section, National Infection Service, Public Health England 10

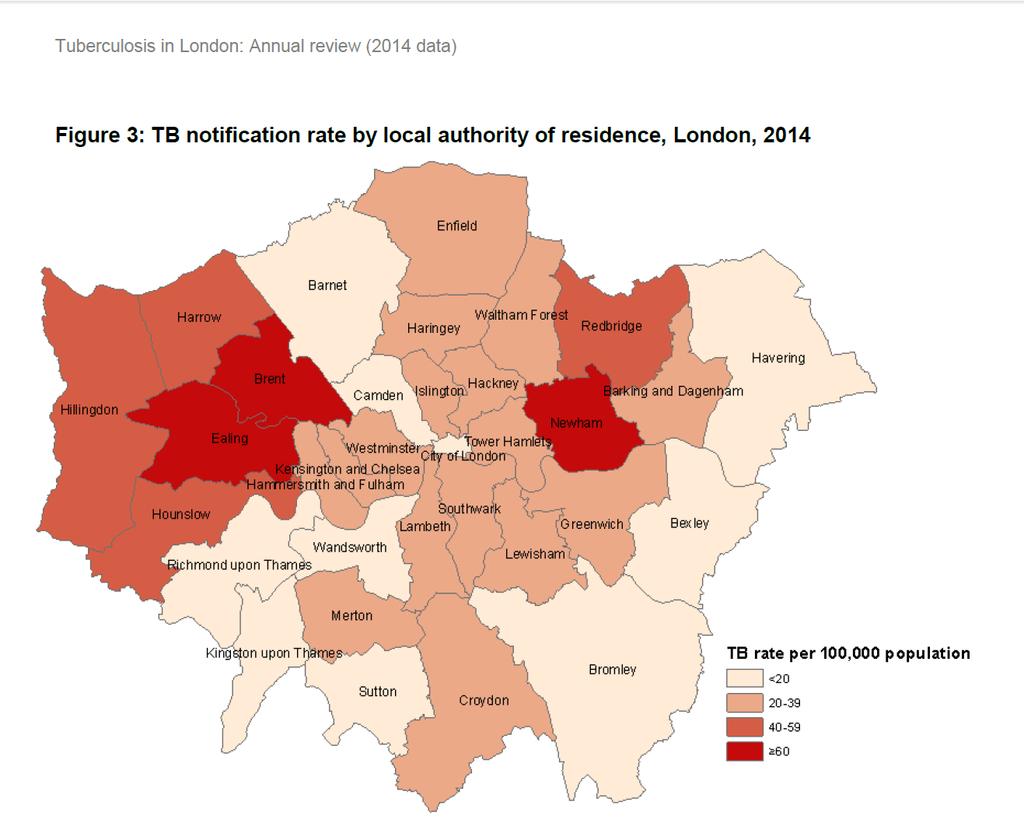
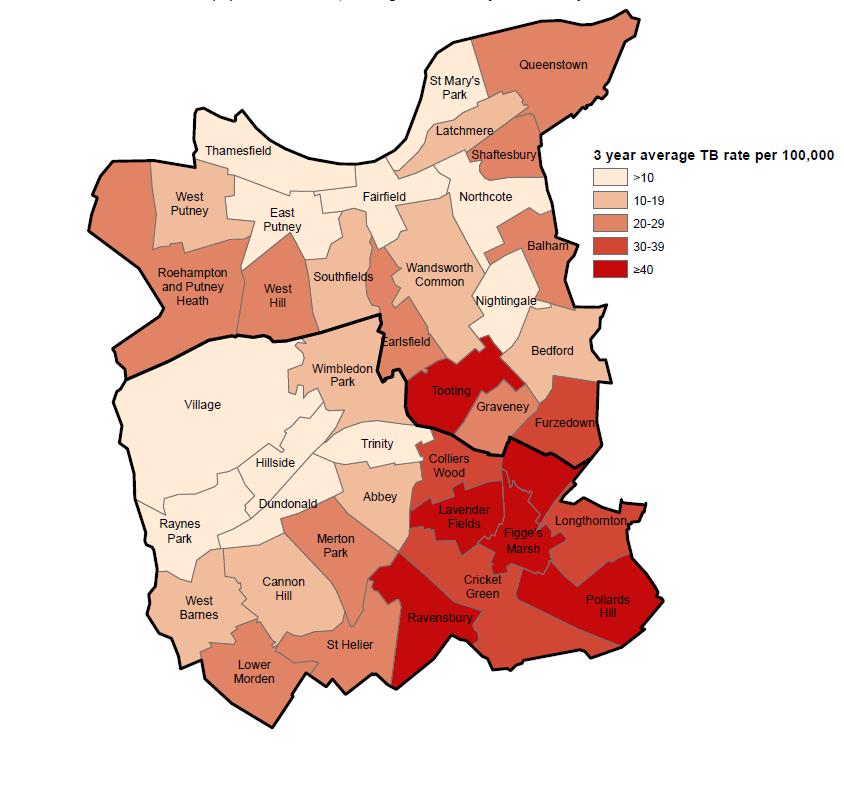
10 TB London 11
11 Number of cases Rate (per 100,000) TB case notifications and rates by place of birth, England, ,000 6,000 5,000 4,000 3,000 2,000 1, Year UK born Non-UK born Rate UK born Rate Non-UK born I 95% CI (too narrow to be visible) I 95% CI Tuberculosis in England: 2016 report Source: Enhanced Tuberculosis Surveillance system (ETS), Labour Force Survey (LFS) Data extracted: April 2016 Prepared by: TB Section, National Infection Service, Public Health England 12
12 Number of cases Rate (per 100,000) TB case notifications and rates by age group and place of birth, England, , Age group (years) UK born Non-UK born Rate in UK born Rate in Non-UK born I 95% CI (too narrow to be visible) I 95% CI Tuberculosis in England: 2016 report Source: Enhanced Tuberculosis Surveillance system (ETS), Labour Force Survey (LFS) Data extracted: April 2016 Prepared by: TB Section, National Infection Service, Public Health England 13
13 Number of cases Trend in TB case notifications for the top five countries of birth* of non-uk born cases, England, ,800 1,600 1,400 1,200 1, Year India Pakistan Somalia Bangladesh Nepal * Five most frequent countries of birth in 2015 Tuberculosis in England: 2016 report Source: Enhanced Tuberculosis Surveillance system (ETS) Data extracted: April 2016 Prepared by: TB Section, National Infection Service, Public Health England 14
14 Case 1 SM 29 yo Black African male From South Africa and in UK for 4 years April 2016 presented to GP with a 3 week history of cough No response to antibiotics 2 weeks later no response, new haemoptysis Further course of antibiotics Tuberculsosis/ St George s University Hospitals NHS Foundation Trust
15 Case 1 3 rd trip to the GP Further course of antibiotics 4 th trip CXR not reported June 2016 presented to A&E large haemoptysis Tuberculosis/ St George s University Hospitals NHS Foundation Trust
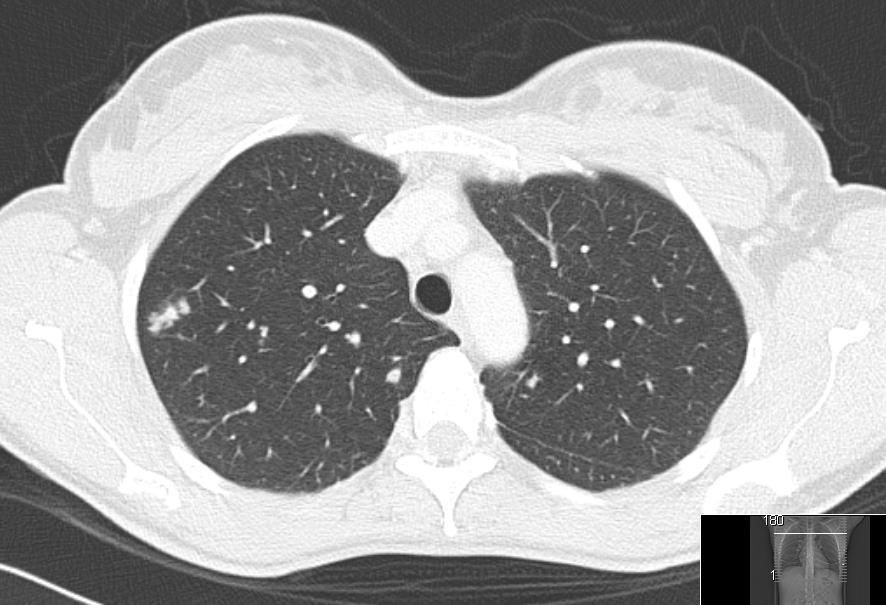
16

17 Cavitation LUL Consolidation throughout left lung
18 What do you do next? Presentation title / St George s University Hospitals NHS Foundation Trust
19 What do you do next? Isolate in a cubicle FFP3 masks Countries at risk of MDRTB Tuberculosis/ St George s University Hospitals NHS Foundation Trust
20 What tests? Interferon Gamma Release Assay (IGRA) eg QUANTIferon GOLD Mantoux Sputum MC&S Sputum AFBs TB PCR Presentation title / St George s University Hospitals NHS Foundation Trust
21 What tests? Interferon Gamma Release Assay (IGRA) eg QUANTIferon GOLD Mantoux Sputum MC&S Sputum AFBs TB PCR Presentation title / St George s University Hospitals NHS Foundation Trust
22 Case 1 Sputum AFB smear positive
23 Case 1 Sputum AFB smear positive Rifampicin resistance PCR negative Mycobacterium tuberculosis on PCR

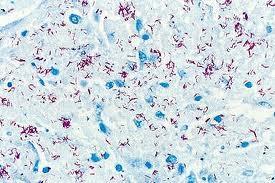
24 Acid fast bacilli Lowenstein-Jensen culture medium
25 Rapid diagnostic tests (PCR) For MTB complex (M tuberculosis, M bovis, M africanum) If: Rapid confirmation would alter care Before large contact-tracing initiative Consider TB even if rapid diagnostic tests negative in pleural fluid, CSF, urine Especially in TB meningitis (risk of not treating severe)
26 Other tests FBC LFTs U&Es Vitamin D Hep B/C HIV
27 Case 1 Sputum AFB smear positive Rifampicin resistance PCR negative Commenced on treatment
28 Medications Rifampicin 6 months Isoniazid 6 months Pyrazinamide Induction, first 2 months Ethambutol Induction, first 2 months
29 Side Effects
30 Side Effects Abnormal LFTs Itchy rashes Gastritis Urine & tears pinky Arthralgias SLE Gout Peripheral Neuropathy Optic neuritis Flu-like symptoms Neutropenia etc
31 Case 1 Screening Wife
32 Inhalation of MTB Immediate killing of MTB (PPD-) Primary Infection (PPD+)
33 Inhalation of MTB Immediate killing of MTB (PPD-) Primary Infection (PPD+) Stabilization (latency) Active disease
34 Inhalation of MTB Immediate killing of MTB (PPD-) Primary Infection (PPD+) Stabilization (latency) +/- Suppressed immunity Active disease
35 Inhalation of MTB Immediate killing of MTB (PPD-) Primary Infection (PPD+) Stabilization (latency) +/- Suppressed immunity Active disease Chemoprophylaxis Chemotherapy Lifelong Latency Cure
36 Inhalation of MTB Immediate killing of MTB (PPD-) Primary Infection (PPD+) Stabilization (latency) +/- Suppressed immunity Active disease Chemotherapy Chemotherapy Lifelong Latency Cure Lifelong Latency
37 Diagnosis Latent TB Active TB Mantoux (skin test) Interferon Gamma Release Assays (IGRA) Latent TB = positive skin test or IGRA + normal CXR + no symptoms Imaging (CXR, CT, MRI, USG) Microscopic staining (AFB) TB culture Histology caseating granuloma
 Standard dose 5TU (0.")
38 Mantoux test Purified protein derivative tuberculin (glycerol extract of tubercle bacillus) Standard dose 5TU (0.1 ml of 1:1000 solution) intradermally Read at hours
39 Interferon Gamma tests T-SPOT.TB QuantiFERON-TB Gold Detect interferon-gamma released by T cells in response to MTB T-SPOT counts individual T cells (ELISpot) Quantiferon measures total IFNγ (ELISA) ESAT-6 and CFP10 (proteins unique for MTB) Advantages: No return visit Result next day No boosting More specific (BCG/ atypicals/ More sensitive than skin test in children, and HIV positive patients Venous, heparinised, room temp, 6-8 hours
40 Active TB cough, fever, night sweats, fatigue, anorexia, weight loss, haemoptysis requires urgent treatment with at least 6 months of anti-tuberculous treatment may be an infection risk dependent on site and progression of disease close contacts are screened notifiable disease asymptomatic Latent TB can be treated with 3 to 6 months of anti-tuberculous treatment to reduce 5-10% lifetime risk of reactivation never infectious contacts do not require screening not notifiable 41
41 Wife Positive Mantoux 15mm Dry cough for 3 weeks No other symptoms Presentation title / St George s University Hospitals NHS Foundation Trust
42 Case 1

43 Case 1 Multiple coworkers exposed PHE incident Fully sensitive
44 Delay from symptom onset 2015 median time 72 days 28% pulmonary delay > 4 months 33% UK born cases experience a delay Tuberculosis/ St George s University Hospitals NHS Foundation Trust
45 Case 2 A 23 yo Indian man in outpatients 3/12 hx of tiredness, weight loss and a dry cough BCG in childhood TB contact 1 year ago had a Mantoux test that was 10mm and a negative interferon gamma release assay (IGRA). On this occasion examination and chest x-ray is normal. Repeat Mantoux test is 20mm and he has a positive IGRA. He is unable to produce sputum spontaneously.

46 What do you do next?
47 Case 2 Commence treatment for latent TB infection Commence a standard four drug regimen for TB Follow-up with a repeat chest x-ray in 6 weeks Perform a CT scan and obtain appropriate specimens Perform a bronchoscopy or induced sputum
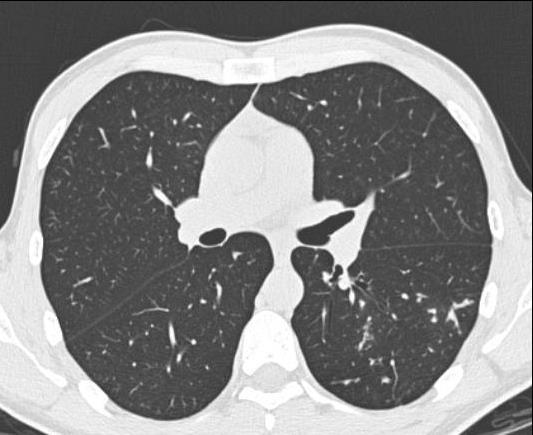
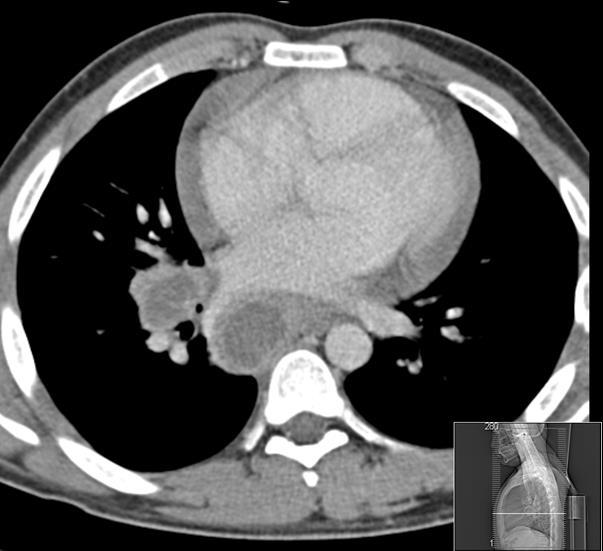
48 CT scan
49 Next steps Directed bronchoscopy and BAL
50 Next steps Directed bronchoscopy What bloods?
51 Next steps Directed bronchoscopy What bloods? FBC, LFTs, U&Es HIV, Hep B&C Vitamin D
52 Next steps Directed bronchoscopy What bloods? FBC, LFTs, U&Es HIV, Hep B&C Vitamin D What treatment?

53 Medications Rifampicin 6 months Isoniazid 6 months Pyrazinamide Induction, first 2 months Ethambutol Induction, first 2 months
54 Bronchoalveolar lavage Initially AFB smear positive 3 weeks later culture positive 6 weeks in MDRTB
55 Bronchoalveolar lavage Initially AFB smear positive 3 weeks later culture positive 6 weeks in MDRTB Aaaaaaaaaaaaaaaaaagh!
56 What do you do? 1. Perform a repeat CT to ensure resolution of the initial subtle left changes 2. Stop the isoniazid and rifampicin and continue with ethambutol and pyrazinamide and review with a CT in one month 3. Stop isoniazid and rifampicin and add moxifloxacin and streptomycin 4. Refer him to a specialist 5. Stop isoniazid and rifampicin and add amikacin, moxifloxacin and cyloserine
57 Management of MDRTB By clinicians with the expertise to do so! NO NEW DRUGS WITHOUT SENSITIVITIES Should be on 3 5 drugs to which the bug is sensitive At least 18 months and follow-up for 2 years after Brilliant case management by nurses and outreach team
58 Pulmonary TB again 32 yo man Presents to A&E 2 month history of 2 stone weight loss, cough, sputum, sweats and tiredness Homeless O/E spiking temps, thin, crackles Chest x-ray
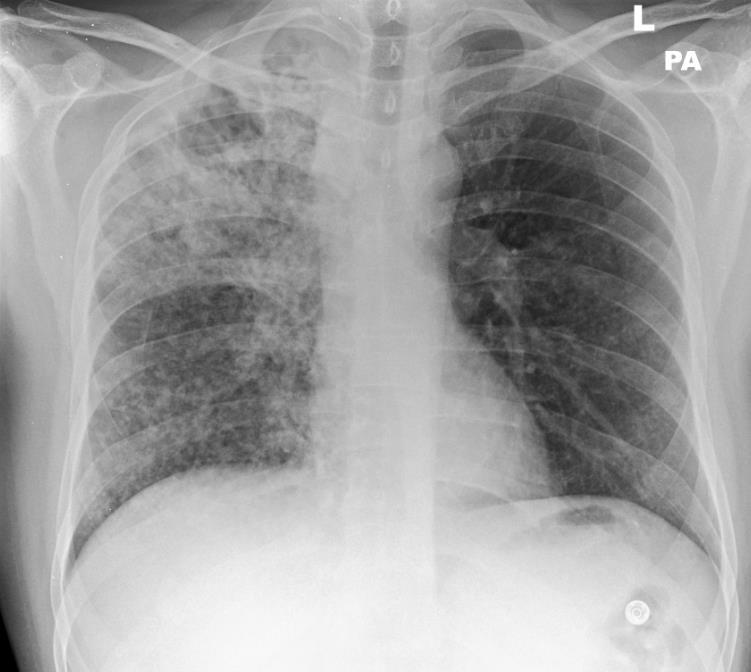
59
60 What are you going to do next? Admit to side room Masks? 3 x sputa Bloods CSF Discharge?
61 Sputum smear positive Extra test? Other considerations?
62 Sputum smear positive Extra test? PCR Rif probe Other considerations? Infectivity 6 months treatment to complete DOT Homelessness
63 DOT?
64 Directly Observed Therapy (DOT) All patients should be risk assessed Previous history of treatment Current poor adherence Homelessness Drug or alcohol misuse Cognitive or psychiatric disorders Denial History of imprisonment
65 Barriers to treatment Social risk factors Minimum 6 months treatment Side effects Brilliant case management key
66
67 Pericardial Disease Lymphocytosis Prednisolone 60mg At risk of restrictive pericarditis Consider operative treatment

68
69 TB meningitis High protein and low glucose Polymorphonuclear cells do not exclude Not usually AFB smear positive Repeat samples MRI with contrast best Always perform a CXR
70 TB Meningitis High mortality 1 year treatment 2 month induction phase Prolonged induction phase Prednisolone 40mg Monitor carefully
71 Common symptoms Cough Fever Sweats Weightt loss Fatigue Lymphadenopathy Haemoptysis
72 Uncommon symptoms Headaches Abdominal pain Back pain Depression Thirst Clear sputum Pallor Cold extremities
73 Uncommon symptoms Headaches Abdominal pain Back pain Depression Thirst Clear sputum ANY OTHER SYMPTOM! Pallor Cold extremities
74 Remember Only 50% of cases are pulmonary You need prolonged contact to catch it It is treatable The more you think TB the more you ll diagnose it early BCG does not prevent TB Tuberculosis/ St George s University Hospitals NHS Foundation Trust
75 Beth Villanueva TB Nurse Lead Dr Anne Dunleavy TB Resp Cons Dr Catherine Cosgrove TB ID Cons Dr Angela Houston TB ID Consultant Prof. Tom Harrison TB ID Consultant Dr Derek Macallan TB ID Consultant lead Dr Amber Arnold - Locum ID Consultant Gale TB service administrator Veera Pavlova Senior TB nurse specialist Innocent Dunstan TB nurse specialist Csaba Koczkas TB nurse specialist Marcos TB nurse specialist Michael Nayagam TB outreach worker Presentation title / St George s University Hospitals NHS Foundation Trust




76 HoHow to Refer et TB Nurses Tel: , bleep: 8481 MON FRI 09:00 17:00 excl. public holidays For out-of-hours urgent queries please contact: on-call ID registrar on bleep: 7568 or
77 Thank you Any questions? Excellence in specialist and community healthcare
78 Divider title Arial Bold 30pt
79 Presentation title / St George s University Hospitals NHS Foundation Trust
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
TB, BCG and other things. Chris Conlon Infectious Diseases Oxford
 TB, BCG and other things Chris Conlon Infectious Diseases Oxford Epidemiology Latent TB IGRA BCG >50/100000
TB, BCG and other things Chris Conlon Infectious Diseases Oxford Epidemiology Latent TB IGRA BCG >50/100000
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial update) 1.1 Short title Tuberculosis
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial update) 1.1 Short title Tuberculosis
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Tuberculosis in England 2018 report (presenting data to end of 2017) Tables and figures slide set
 Tables and figures slide set") Tuberculosis in England 2018 report (presenting data to end of 2017) Tables and figures slide set Number of TB notifications and rates, England, 1971-2017 2 Tuberculosis in England: 2018 report, Office
Tuberculosis in England 2018 report (presenting data to end of 2017) Tables and figures slide set Number of TB notifications and rates, England, 1971-2017 2 Tuberculosis in England: 2018 report, Office
New Entrant Screening and Latent TB Get screened and find out if you have TB infection before you develop TB disease!
 New Entrant Screening and Latent TB Get screened and find out if you have TB infection before you develop TB disease! Screening and treatment for TB are free. What does this leaflet cover? What is Tuberculosis
New Entrant Screening and Latent TB Get screened and find out if you have TB infection before you develop TB disease! Screening and treatment for TB are free. What does this leaflet cover? What is Tuberculosis
Tuberculosis 6/7/2018. Objectives. What is Tuberculosis?
 Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service
 Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service North Central London TB Service TBService@nhs.net After Action Review Could we have
Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service North Central London TB Service TBService@nhs.net After Action Review Could we have
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
New NICE guideline updates recommendations for diagnosing latent tuberculosis
 Tel: 0845 003 7782 www.nice.org.uk Ref: 2011/053 PRESS RELEASE New NICE guideline updates recommendations for diagnosing latent tuberculosis The National Institute for Health and Clinical Excellence (NICE)
Tel: 0845 003 7782 www.nice.org.uk Ref: 2011/053 PRESS RELEASE New NICE guideline updates recommendations for diagnosing latent tuberculosis The National Institute for Health and Clinical Excellence (NICE)
TB Clinical Guidelines: Revision Highlights March 2014
 TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Tuberculosis. New TB diagnostics. New drugs.new vaccines. Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012
 Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!!
 Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
The diagnosis of active TB
 The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
PEDIATRIC TB. Modified PPT from group A seminar (F)
") PEDIATRIC TB Modified PPT from group A seminar (F) objectives the epidemiology of pediatric TB. TB Mycobacteriology. pediatric TB presentations compared to adults TB. Know the differences between, and
PEDIATRIC TB Modified PPT from group A seminar (F) objectives the epidemiology of pediatric TB. TB Mycobacteriology. pediatric TB presentations compared to adults TB. Know the differences between, and
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE
 Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks
 1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On
1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On
Tuberculosis. Impact of TB. Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH)
") Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
UCLH Members Event: Tuberculosis
 UCLH Members Event: Tuberculosis 22 nd June 2015 Dave Moore, London School of Hygiene & Tropical Medicine & UCLH Phil Gothard, Hospital for Tropical Diseases, UCLH Al Story, TB Find & Treat Service, UCLH
UCLH Members Event: Tuberculosis 22 nd June 2015 Dave Moore, London School of Hygiene & Tropical Medicine & UCLH Phil Gothard, Hospital for Tropical Diseases, UCLH Al Story, TB Find & Treat Service, UCLH
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
South West. Tuberculosis Treatment Outcome Surveillance for the South West
 South West Tuberculosis Treatment Outcome Surveillance for the South West 2001-2004 Outcome Surveillance 2001-2004 TB Outcome Surveillance 2001-2004 Data for the South West Region, England A report from
South West Tuberculosis Treatment Outcome Surveillance for the South West 2001-2004 Outcome Surveillance 2001-2004 TB Outcome Surveillance 2001-2004 Data for the South West Region, England A report from
Case presentation. Dr REESAUL R
 Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
TB: A Supplement to GP CLINICS
 TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
2017/2018 Annual Volunteer Tuberculosis Notice
 Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis Infection in the US Military
 Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
Annual surveillance report 2015
 Annual surveillance report 215 Acknowledgements The Public Health Agency Northern Ireland gratefully acknowledges all those who contributed to this report, including; physicians, nurses, microbiologists,
Annual surveillance report 215 Acknowledgements The Public Health Agency Northern Ireland gratefully acknowledges all those who contributed to this report, including; physicians, nurses, microbiologists,
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Tuberculosis in South West Centre: Annual review (2014 data) Data from 2000 to 2014
 Data from 2000 to 2014") Tuberculosis in South West Centre: Annual review (2014 data) Data from 2000 to 2014 2 About Public Health England Public Health England exists to protect and improve the nation's health and wellbeing,
Tuberculosis in South West Centre: Annual review (2014 data) Data from 2000 to 2014 2 About Public Health England Public Health England exists to protect and improve the nation's health and wellbeing,
Childhood Tuberculosis Some Basic Issues. Jeffrey R. Starke, M.D. Baylor College of Medicine
 Childhood Tuberculosis Some Basic Issues Jeffrey R. Starke, M.D. Baylor College of Medicine TUBERCULOSIS IS A SOCIAL DISEASE WITH MEDICAL IMPLICATIONS THE GREAT PARADOX OF TUBERCULOSIS A CAUTIONARY TALE
Childhood Tuberculosis Some Basic Issues Jeffrey R. Starke, M.D. Baylor College of Medicine TUBERCULOSIS IS A SOCIAL DISEASE WITH MEDICAL IMPLICATIONS THE GREAT PARADOX OF TUBERCULOSIS A CAUTIONARY TALE
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
2016 OPAM Mid-Year Educational Conference, Sponsored by AOCOPM Sunday, March 13, 2016
 Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Audit of management of TB in HIV co-infected patients: survey of clinic arrangements
 Audit of management of TB in HIV co-infected patients: survey of clinic arrangements Please complete this questionnaire if your clinic/department provides TB treatment and care for adult patients, but
Audit of management of TB in HIV co-infected patients: survey of clinic arrangements Please complete this questionnaire if your clinic/department provides TB treatment and care for adult patients, but
Tuberculosis Procedure ICPr016. Table of Contents
 Tuberculosis Procedure ICPr016 Table of Contents Tuberculosis Procedure ICPr016... 1 What is Tuberculosis?... 2 Any required definitions/explanations... 2 NHFT... 2 Tuberculosis (TB)... 3 Latent TB...
Tuberculosis Procedure ICPr016 Table of Contents Tuberculosis Procedure ICPr016... 1 What is Tuberculosis?... 2 Any required definitions/explanations... 2 NHFT... 2 Tuberculosis (TB)... 3 Latent TB...
Annual surveillance report 2016
 Annual surveillance report 216 Acknowledgements The Public Health Agency Northern Ireland gratefully acknowledges all those who contributed to this report, including; physicians, nurses, microbiologists,
Annual surveillance report 216 Acknowledgements The Public Health Agency Northern Ireland gratefully acknowledges all those who contributed to this report, including; physicians, nurses, microbiologists,
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
In our paper, we suggest that tuberculosis and sarcoidosis are two ends of the same spectrum. Given the pathophysiological and clinical link between
 In our paper, we suggest that tuberculosis and sarcoidosis are two ends of the same spectrum. Given the pathophysiological and clinical link between the two, we also propose a classification system for
In our paper, we suggest that tuberculosis and sarcoidosis are two ends of the same spectrum. Given the pathophysiological and clinical link between the two, we also propose a classification system for
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
Tuberculosis What you need to know. James Zoretic M.D., M.P.H. Regions 2 and 3 Director
 Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Diagnosis & Management of Latent TB Infection
 Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
Thorax Online First, published on December 8, 2009 as /thx
 Thorax Online First, published on December 8, 2009 as 10.1136/thx.2009.119677 Title Page Cost effectiveness of the NICE guidelines for screening for latent tuberculosis infection: the Quantiferon-TB gold
Thorax Online First, published on December 8, 2009 as 10.1136/thx.2009.119677 Title Page Cost effectiveness of the NICE guidelines for screening for latent tuberculosis infection: the Quantiferon-TB gold
Tuberculosis in Wales Annual Report 2014
 Tuberculosis in Wales Annual Report 2014 Author: Communicable Disease Surveillance Centre Date: 20/03/2015 Version: 1 Status: Final Intended Audience: Health Purpose and Summary of Document: This report
Tuberculosis in Wales Annual Report 2014 Author: Communicable Disease Surveillance Centre Date: 20/03/2015 Version: 1 Status: Final Intended Audience: Health Purpose and Summary of Document: This report
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Tuberculosis. WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED
 Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Tuberculosis in North East England: Annual review (2015 data) Data from 2000 to 2015
 Data from 2000 to 2015") Tuberculosis in North East England: Annual review (2015 data) Data from 2000 to 2015 Tuberculosis in North East Centre (2015) About Public Health England Public Health England exists to protect and improve
Tuberculosis in North East England: Annual review (2015 data) Data from 2000 to 2015 Tuberculosis in North East Centre (2015) About Public Health England Public Health England exists to protect and improve
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
UC DavisTB Screening Requirement: How to submit your TB Health Assessment Form
 UC DavisTB Screening Requirement: How to submit your TB Health Assessment Form Step 1 If after completing the TB Risk Screening you are found to be at high risk, you must complete the Tuberculosis (TB)
UC DavisTB Screening Requirement: How to submit your TB Health Assessment Form Step 1 If after completing the TB Risk Screening you are found to be at high risk, you must complete the Tuberculosis (TB)
Respiratory Tuberculosis (TB)
") Respiratory Tuberculosis (TB) Information Leaflet For Patients and Visitors Please follow this guidance from the Infection Prevention and Control Team What is Respiratory Tuberculosis (TB)? Pulmonary/respiratory
Respiratory Tuberculosis (TB) Information Leaflet For Patients and Visitors Please follow this guidance from the Infection Prevention and Control Team What is Respiratory Tuberculosis (TB)? Pulmonary/respiratory
Chapter 4 Diagnosis of Tuberculosis Disease
 Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
TB Data Quality Assurance: United Kingdom
 TB Data Quality Assurance: United Kingdom Ibrahim Abubakar, MBBS, PhD, FFPH Tuberculosis Section HPA Centre for Infections 8,655 cases in 2008 14.1 per 100,000 Increase over last 2 decades TB Surveillance
TB Data Quality Assurance: United Kingdom Ibrahim Abubakar, MBBS, PhD, FFPH Tuberculosis Section HPA Centre for Infections 8,655 cases in 2008 14.1 per 100,000 Increase over last 2 decades TB Surveillance
Trust Guideline for the Prevention of Tuberculosis and Management of Tuberculosis Exposure in Health Care Workers
 A Clinical Guideline For Use in: By: For: Division responsible for document: Key words: Name and job title of document author: Name and job title of document author s Line Manager: Supported by: Assessed
A Clinical Guideline For Use in: By: For: Division responsible for document: Key words: Name and job title of document author: Name and job title of document author s Line Manager: Supported by: Assessed
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
New Tuberculosis Guidelines. Jason Stout, MD, MHS
 New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Symptoms Latent TB Active TB
 1 Tuberculosis Tuberculosis (TB) is a disease that can spread through the air. It is caused by a bacterium called Mycobacterium tuberculosis. It usually affect the lungs. However, it can also affect other
1 Tuberculosis Tuberculosis (TB) is a disease that can spread through the air. It is caused by a bacterium called Mycobacterium tuberculosis. It usually affect the lungs. However, it can also affect other
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has