Core Curriculum on Tuberculosis: What the Clinician Should Know
|
|
|
- Laurence Marsh
- 6 years ago
- Views:
Transcription


1 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1
2 Chapters Content Core Curriculum Contents 1 Overview of Tuberculosis (TB) Epidemiology in the United States 2 Transmission and Pathogenesis of TB 3 Testing for TB Infection and Disease 4 Diagnosis of TB Disease 5 Treatment for Latent TB Infection 6 Treatment for TB Disease 7 TB Infection Control 8 Communit y TB Control 2
3 Chapter 1. Overview of TB Epidemiology in the United States 3
4 Progress Toward TB Elimination in the U.S. 1989: Release of A Strategic Plan for the Elimination of Tuberculosis in the United States, MMWR1989; 38 (Suppl. No. S-3), with goal of TB elimination in : Resurgence of TB in the United States, fueled by several factors In response to resurgence, U.S. renewed commitment and support for TB control In 1993, upward trend was reversed; that decline has continued 4
5 Factors Contributing to the Increase in TB Morbidit y: Emerging HIV/AIDS epidemic Immigration from countries where TB was common Transmission of TB in congregate settings Development of multidrug-resistant (MDR) TB Decades of funding cuts had impaired effectiveness of TB control programs 5
6 Factors Contributing to the Decrease in TB Morbidit y Since 1993 Success attributed to increased efforts to Promptly identify persons with TB Initiate appropriate treatment Ensure completion of therapy But TB elimination faces barriers 6
7 Areas of Concern Remain U.S. TB cases occur largely in high-risk populations In these populations, TB is difficult to detect, diagnose, and treat Global TB epidemic persists Current TB control measures are limited; new tests, vaccines, drugs needed 7
8 TB Disease Trends in the United States During resurgence, , reported TB cases increased every year : cases decreased : cases decreased 5%-7% annually : decreased at a more moderate 3%-5% 2009: declined 10.6% from : cases resumed moderate decreases (average 4.5% from 2009) 10,528 cases reported in
9 Reported TB Cases United States, * 9
10 TB Trends, United States While TB is declining overall, high rates persist among some groups Local epidemiology affects trends in individual areas 2011:total of 38 states reported a rate 3.4/100,000 (national average for the year) 12 states + D.C. reported a rate >3.4/100,000 These areas = 67% of the 2011 national total Also had substantial decreases in TB,

11 TB Case Rates,* United States,
12 Reported Cases of TB by Country of Origin, United States Cases among U.S.-born and foreign-born persons declining, but much less so in foreign born 2002: First year foreign-born persons accounted for majorit y of U.S. TB cases (51%) 2011, accounted for 62% In foreign-born persons, TB cases roughly level: : TB cases averaged 7,700/year : TB cases averaged 6,700/year In U.S.-born persons: , TB cases decreased from 17,438 to 3,981 12
13 Percentage of TB Cases Among Foreign-Born Persons in the U.S., 2001 and 2011 Number of states with <25% of cases in foreign-born: down from 13 to 6 Number of states with 25%-49% of cases in foreignborn: down from 14 to 11 N um ber of states w ith 50% of cases in foreign-born: up from 23 to 34 13

14 Percentage of TB Cases Among Foreign-Born Persons, United States* 14

15 Countries of Birth of Foreign-Born Persons Reported with TB, United States,
16 TB Case Rates by Race/Ethnicity* United States, ** 16
17 Factors Likely Contributing to Burden of TB in Minorities In foreign-born minorities, TB may result from infection in country of origin Some minority groups have unequal distribution of TB risk factors (e.g., HIV infection), contributing to increased exposure to TB or increased risk of developing disease once infected with M. tuberculosis Lower socioeconomic status and crowded housing are linked to increased TB risk 17
18 HIV-Infected Persons, United States, * Persons coinfected with HIV and M. tuberculosis are at high risk of developing TB disease In persons with TB, all ages, percentage of HIV coinfection decreased from 15% to 6% In age group 25 44, decreased from 29% to 10% 18
19 Estimated HIV Coinfection in Persons Reported with TB, United States, * 19
20 Multidrug-Resistant (MDR) TB Remains a Serious Public Health Concern in the United States MDR TB has decreased in foreign born and U.S. born, but decline greater in U.S. born , proportion of primary MDR TB in foreign born increased from 25% to 83% 20
21 Primary MDR TB in U.S.-Born vs. Foreign-Born Persons United States, * 21
22 Extensively Drug-Resistant (XDR) TB in the United States XDR TB is a rare type of MDR TB Resistant to INH,RIF,fluoroquinolones,and 1 of 3 injectable 2nd-line drugs No apparent trend for XDR TB in the U.S. 22
23 XDR TB Case Count Defined on Initial DST* by Year, ** 23
24 Persons at Higher Risk for Exposure to or Infection with TB Close contacts of person known or suspected to have active TB Foreign-born persons from areas where TB is common Persons who visit TB-prevalent countries Residents and employees of high-risk congregate settings 24
25 Persons at Higher Risk for Exposure to or Infection with TB (cont.) Health care workers (HCWs) who serve high-risk clients Populations defined locally as having increased incidence of latent M. tuberculosisinfection or TB disease, such as medically underserved, low-income persons who abuse drugs or alcohol Children and adolescents exposed to adults at increased risk for infection or disease 25
26 Chapter 2. Transmission and Pathogenesis of TB 26
27 Introduction Airborne disease caused by the bacterium Mycobacterium tuberculosis (M. tb) M. tb complex (M. tb, M. bovis, M. africanum, M. microti, M. canetti, M. caprae, M. pinnipedii, and M. mungi) can cause TB disease Majority of TB cases caused by M. tb M. tb organisms also called tubercle bacilli 27



28 Transmission of M. tuberculosis M. tb spread via airborne particles called droplet nuclei Expelled when person with infectious TB coughs, sneezes, shouts, or sings Transmission occurs when droplet nuclei inhaled and reach the alveoli of the lungs, via nasal passages, respiratory tract, and bronchi 28
29 Probability TB Will Be Transmitted Susceptibility of the exposed person Infectiousness of person with TB (i.e., number of bacilli TB patient expels into the air) Environmental factors that affect the concentration of M. tb organisms Proximity,frequency, and duration of exposure (e.g., close contacts) Can be transmitted from children, though less likely 29


30 Pathogenesis Droplet nuclei containing tubercle bacilli are inhaled, enter the lungs, and travel to the alveoli. Tubercle bacilli multiply in the alveoli. 30

31 Pathogenesis A small number of tubercle bacilli enter the bloodstream and spread throughout the body. The tubercle bacilli may reach any part of the body, including areas where TB disease is more likely to develop (such as the brain, larynx, lymph node, lung, spine, bone, or kidney). 31

.")
.")
32 Pathogenesis Within 2 to 8 weeks, special immune cells called macrophages ingest and surround the tubercle bacilli. The cells form a barrier shell, called a granuloma, that keeps the bacilli contained and under control (LTBI). If the immune system cannot keep the tubercle bacilli under control, the bacilli begin to multiply rapidly (TB disease). This process can occur in different areas in the body, such as the lungs, kidneys, brain, or bone. 32
33 Latent TB Infection (LTBI) Granulomas may persist (LTBI), or may break down to produce TB disease 2 to 8 weeks after infection, LTBI can be detected via TST or interferon-gamma release assay (IGRA) The immune system is usually able to stop the multiplication of bacilli Persons with LTBI are not infectious and do not spread organisms to others 33
34 TB Disease In some, the granulomas break down, bacilli escape and multiply, resulting in TB disease Can occur soon after infection, or years later Persons with TB disease are usually infectious and can spread bacteria to others Positive M. tb culture confirms TB diagnosis 34
35 Sites of Disease Lungs (pulmonary): most common site; usually infectious Miliary: occurs when bacilli spread to all parts of the body; rare, but fatal if untreated Central nervous system: usually occurs as meningitis, but can occur in brain or spine 35
36 Sites of Disease (cont.) Outside the lungs (extrapulmonary): usually not infectious, unless person has Concomitant pulmonary disease, Extrapulmonary disease in the oral cavity or larynx, or Extrapulmonary disease with open site, especially with aerosolized fluid. 36
37 Risk of Developing Disease Normal Immune System Untreated, 5% of infected persons with normal immunity develop TB in first 1 2 years post infection, another 5% later in life Thus, about 10% of infected persons with normal immunity will develop TB at some point in life if not treated 37
38 Risk of Developing Disease (cont.) Weak Immune System Persons with weak immunity at increased risk of progressing to TB disease Untreated HIV infection highest risk factor: risk of developing TB disease is 7% 10% each year; Children <5 years of age also at increased risk 38
39 LTBI vs. TB Disease Person with LTBI (Infected) Has a small amount of TB bacteria in his/her body that are alive, but inactive Cannot spread TB bacteria to others Does not feel sick, but may become sick if the bacteria become active in his/her body Usually has a TB skin test or TB blood test reaction indicating TB infection Radiograph is typically normal Sputum smears and cultures are negative Should consider treatment for LTBI to prevent TB disease Does not require respiratory isolation Not a TB case Person with TB Disease (Infectious) Has a large amount of active TB bacteria in his/her body May spread TB bacteria to others May feel sick and may have symptoms such as a cough, fever, and/or weight loss Usually has a TB skin test or TB blood test reaction indicating TB infection Radiograph may be abnormal Sputum smears and cultures may be positive Needs treatment for TB disease May require respiratory isolation A TB case 39
40 Drug-Resistant TB Caused by organisms resistant to one or more TB drugs Transmitted same way as drug-susceptible TB, and no more infectious Delay in detecting drug resistance may prolong period of infectiousness because of delay in starting correct treatment 40
41 Multidrug-Resistant (MDR) and Extensively Drug- Resistant (XDR) TB MDR TB caused by bacteria resistant to best TB drugs, isoniazid and rifampin XDR TB caused by organisms resistant to isoniazid and rifam pin,plus fluoroquinolones and 1 of the 3 injectable second-line drugs All TB TB with any drug resistance MDR TB* with drug resistance to at least the firstline drugs isoniazid and rifampin XDR TB** with drug resistance to the first-line drugs isoniazid and rifampin and to specific second-line drugs *Often resistant to additional drugs **Resistant to any fluoroquinolone and at least one of three injectable second-line drugs (i.e., amikacin, kanamycin, or capreomycin 41
42 Types of Drug Resistance Drug resistance develops in two ways: Primary resistance develops in persons initially infected with resistant organisms Secondary (acquired) resistance develops during TB therapy 42
43 Circumstances Increasing the Risk of Drug- Resistant TB Risk of drug-resistant TB is increased with exposure to a person who Has confirmed drug-resistant TB Had prior unsuccessful treatment for TB, and drug susceptibilit y results not known Originated in a drug-resistant TB prevalent country Has positive smear and culture 2 months after treatment start 43
44 Classification System for TB Based on TB pathogenesis (stage of disease) Helps clinician track the development of TB in patients Persons with class 3 or 5 TB should be reported to health department Patients should not have class 5 classification for more than 3 months 44
45 TB Classification System Class Stage of Disease 0 No exposure, no infection 1 Exposure, no evidence of infection 2 TB infection, no disease 3 TB, clinically active 4 TB, not clinically active 5 TB suspect 45
46 Chapter 3. Testing for TB Infection and Disease 46
47 Identifying High-Risk Groups for M. tb Testing Health-care providers should find and test Uninfected persons at high risk for LTBI, and/or Persons at high risk for progression to TB disease Flexibility needed in defining high-risk groups Risk for TB or LTBI in current high-risk groups may decrease over time, and groups currently not at risk may subsequently become high risk 47
48 Evaluation of Persons with Positive TB Tests Facilities should consult with local health department before starting testing program to ensure evaluation and treatment resources are available Persons with positive TST or IGRA should be evaluated for disease If disease is ruled out, consider for LTBI treatment If patient not willing or able to take treatment, educate on TB signs and symptoms 48
49 Methods for Detecting M. tb Infection in U.S. Mantoux tuberculin skin test (TST) IGRAs: QuantiFERON-TB Gold In-Tube (QFT-GIT), and T-Spot.TB These tests do not exclude LTBI or TB disease Decisions about medical/public health management should include other info/data, and not rely only on TST/IGRA results 49
50 Mantoux Tuberculin Skin Test (TST) Purified protein derivative (PPD), derived from tuberculin, is injected between skin layers using the Mantoux technique Infected person s immune cells recognize TB proteins in PPD, respond to site, causing wheal to rise Takes 2-8 weeks after exposure and infection for the immune system to react to PPD Reading and interpretation of TST reaction must be done within hours 50
 into forearm between skin layers Produce wheal (raised area) 6 10")
51 Administering the TST Inject 0.1 ml of PPD (5 tuberculin units) into forearm between skin layers Produce wheal (raised area) 6 10 mm in diameter Follow universal precautions for infection control 51

52 Reading the TST Trained health care worker assesses reaction hours after injection Palpate (feel) injection site to find raised area Measure diameter of induration across forearm; only measure induration, not redness Record size of induration in millimeters; record 0 if no induration found 52
53 Interpreting the TST Reaction 5 m m induration is classified as positive in HIV-infected persons Recent contacts of infectious TB Persons with fibrotic changes on chest radiograph consistent with prior TB Patients with organ transplants and other immunosuppressed patients 53
54 Interpreting the TST Reaction (cont.) 10 m m induration is classified as positive in Recent arrivals from high-prevalence countries Injection drug users Residents and employees of high-risk congregate settings 54
55 Interpreting the TST Reaction (cont.) 10 m m induration is classified as positive in Mycobacteriology laboratory personnel Persons with conditions that increase risk for progressing to TB Children <5 years of age, or children and youth exposed to adults at high risk 55
56 Interpreting the TST Reaction (cont.) 15 m m is classified as positive in Persons with no known risk factors for TB Targeted skin testing should only be conducted among high-risk groups 56
57 Factors that May Affect the Skin Test Reaction Type of Reaction False-positive False-negative Possible Cause Nontuberculous mycobacteria BCG vaccination Problems with TST administration Anergy Viral, bacterial, fungal coinfection Recent TB infection Very young age; advanced age Live-virus vaccination Overwhelming TB disease Renal failure/disease Lymphoid disease Low protein states Immunosuppressive drugs Problems with TST administration 57
58 Boosting Special Considerations When Using TST Some may have negative (waned) TST reaction when tested years after infection (e.g., older adults) Initial skin test may stimulate (boost) ability to react to PPD Subsequent positive boosted reaction may be misinterpreted as a new infection May still be considered for treatment if currently at high risk for TB disease 58
59 Special Considerations When Using TST (cont.) Two-Step Testing Used for initial skin testing of adults to be retested periodically, to reduce likelihood that boosted reaction will be misinterpreted as recent infection If 1st test positive, consider infected; if negative, give 2nd test 1 3 weeks later If 2nd test positive, consider infected; if negative, consider uninfected 59
60 Special Considerations When Using TST (cont.) Pregnant women TST is safe and reliable for mother and fetus throughout pregnancy Give TST to pregnant women who have risk factors for infection or disease 60
61 Special Considerations When Using TST (cont) Occupational Exposure to TB Cutoff for defining a positive TST reaction depends on Individual risk factors for TB Prevalence of TB in the facility High-risk sites should test residents and staff at entry and hire and at intervals determined by annual risk assessment 61
62 Interferon Gamma Release Assays (IGRAs) IGRAs detect M. tb infection by measuring immune response in blood Cannot differentiate between TB and LTBI; other tests needed May be used for surveillance/screening, or to find those who will benefit from treatment FDA-approved IGRAs are QFT Gold In-Tube and T- Spot.TBtest 62
63 General Recommendations for Using IGRAs May be used in place of, but not in addition to, TST Preferred when testing persons Who might not return for TST reading Who have received BCG vaccination Generally should not be used to test children <5 years of age, unless used in conjunction with TST 63
64 General Recommendations for Using IGRAs (cont.) May be used in place of TST to test recent contacts of infectious TB Detect M. tb infection with greater specificity than TST Data are limited on ability to predict subsequent TB In contact investigations, confirm negative via retest 8 10 weeks postexposure Use same test for repeat testing to reduce misclassification errors 64
65 General Recommendations for Using IGRAs (cont.) May be used for periodic screening, e.g., for health-care workers IGRAs do not boost subsequent test results; administered with one patient visit Results from both IGRA and TST may be useful when initial test is Negative, and patient has high risk of TB infection or disease Positive, and additional evidence is required/desired Unclear or indeterminate 65
66 BCG Vaccination Vaccine made from live, attenuated (weakened) strain of M. bovis Early version first given to humans in 1921 Many TB-prevalent countries vaccinate infants to prevent severe TB disease 66
67 Recommendations for BCG Vaccination BCG not generally recommended in the U.S. However, its use may be considered in very limited circumstances Use BCG only after consultation with local health department and TB experts 67
68 Recommendations for BCG Vaccination (cont.) Infants and Children Can be considered for infant or child with negative skin-test result who Is continually exposed to untreated or ineffectively treated adult Will be continually exposed to adult with MDR TB BCG vaccination not recommended for HIV-infected children 68
69 Recommendations for BCG Vaccination (cont.) Health-Care Workers Should be considered on individual basis for health-care workers in settings in which High percentage of MDR TB patients has been found, Transmission of drug-resistant TB strains and subsequent infection are likely, and Comprehensive TB infection-control precautions implemented but not successful. 69
70 BCG Contraindications Contraindicated in persons with impaired immune response from HIV infection, congenital immunodeficiency Leukemia, lymphoma, generalized malignancy High-dose steroid therapy Alkylating agents Antimetabolites Radiation therapy BCG vaccination should not be given to pregnant women 70
71 Interpretation of TB Test Results in BCG- Vaccinated Persons TST or IGRA not contraindicated for BCG-vaccinated persons Results used to support or exclude diagnosis of infection In BCG-vaccinated, interpret TST with same criteria used for non BCG-vaccinated Booster phenomenon may occur in BCG-vaccinated persons 71
72 Chapter 4. Diagnosis of TB Disease 72
73 Medical Evaluation for TB Medical history Physical examination Test for TB infection Chest radiograph Bacteriologic examination 73
74 Medical Evaluation for TB 1. Medical History Symptoms of disease; how long History of TB exposure, infection, or disease Past TB treatment Demographic risk factors for TB Medical conditions that increase risk for TB disease 74
75 Medical Evaluation for TB (cont.) 1. Medical History (cont.) Symptoms of pulmonary TB: Prolonged cough (3 weeks or longer), hemoptysis Chest pain Loss of appetite, unexplained weight loss Night sweats, fever Fatigue 75
76 Medical Evaluation for TB (cont.) 1. Medical History (cont.) Symptoms of possible extrapulmonary TB: Blood in the urine (TB of the kidney) Headache/confusion (TB meningitis) Back pain (TB of the spine) Hoarseness (TB of the larynx) Loss of appetite, unexplained weight loss Night sweats, fever Fatigue 76
77 Medical Evaluation for TB (cont.) 2. Physical Examination Provides valuable information about the patient s overall condition Cannot be used to confirm or rule out TB disease 77



78 Medical Evaluation for TB (cont.) 3. Test for M. tuberculosisinfection Two methods for detecting M. tb infection: TST and IGRAs TST and IGRAs help differentiate persons with M. tb infection from those not infected Negative reaction to either does not exclude diagnosis of TB or LTBI 78
79 Medical Evaluation for TB (cont.) 4. Chest Radiograph Chest abnormalities suggest, but do not confirm, TB disease Posterior-anterior view is standard Apical/posterior areas of upper lobe or superior areas of lower lobe often show abnormalities In immunosuppressed (e.g., HIV infected), lesions may have at ypical appearance 79

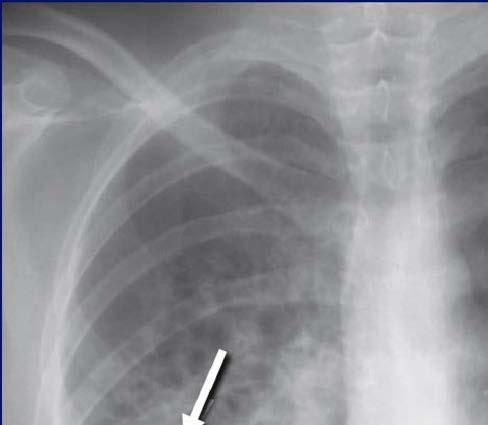

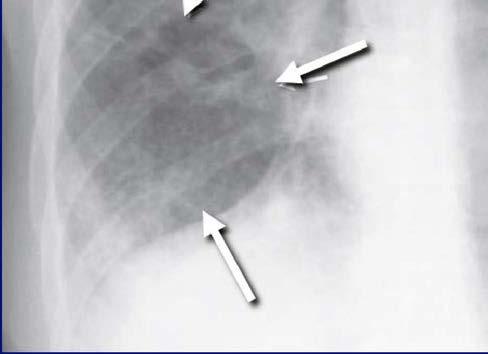

80 Chest Radiograph with Lower Lobe Cavit y 80
81 Medical Evaluation for TB (cont.) 4. Chest Radiograph (cont.) Old TB can produce dense, hard nodules or lesions containing live bacilli Fibrotic nodules/lesions from old TB + positive TB test = high-priority candidate for LTBI treatment Calcified lesions pose low risk for progressing to TB Active versus inactive disease cannot be determined from chest radiograph alone 81
82 Medical Evaluation for TB (cont.) 4. Chest Radiograph (cont.) In HIV infected, pulmonary TB may present atypical radiograph Less common: cavitary disease (with higher CD4 counts) More common: infiltrates, adenopathy, or normal radiograph (with lower CD4 counts) With signs/symptoms, negative radiograph does not rule out disease With no signs/symptoms and positive TB test, negative radiograph may rule out TB in HIV-negative person 82
 5. Bacteriologic Examination")


83 Medical Evaluation for TB (cont.) 5. Bacteriologic Examination of Specimens Specimen collection AFB smear classification NAA testing Culture and identification Drug-susceptibility testing 83
 Specimen collection, processing, and review All persons suspected of TB disease should have sputum")

84 Medical Evaluation for TB (cont.) 5. Bacteriologic Examination of Specimens (cont.) Specimen collection, processing, and review All persons suspected of TB disease should have sputum cultured Collect at least 3 sputum specimens at 8- to 24-hour intervals, at least 1 in the morning Follow infection control precautions during specimen collection Collection methods include coughing, sputum induction, bronchoscopy, gastric aspiration 84
85 Medical Evaluation for TB (cont.) 5. Bacteriologic Examination of Specimens (cont.) Specimen collection methods for extrapulmonary TB TB disease can occur in almost any site Variety of clinical specimens other than sputum can be submitted Before collection, ensure transport and processing procedures are in place 85
86 Medical Evaluation for TB (cont.) 5. Bacteriologic Examination of Specimens (cont.) Smear examination Detecting AFB in smears may be first evidence of mycobacteria Quickest (results within 24 hours) and easiest procedure Provides a preliminary presumptive diagnosis of TB AFB in a smear are counted and classified as 4+, 3+, 2+, or 1+ 86
 are tubercle bacilli")
87 AFB Smear AFB (shown in red) are tubercle bacilli 87
88 Direct Detection Using Nucleic Acid Amplification (NAA) NAA tests rapidly identify a specimen via DNA and RNA amplification Benefits may include Earlier lab confirmation of TB disease Earlier respiratory isolation and treatment initiation Improved patient outcomes; interruption of transmission Perform at least 1 NAA test on each pulmonary TB suspect A single negative NAA test does not exclude TB 88
")
89 Nucleic Acid Amplification (NAA) Test 89
90 Culture Remains gold standard for confirming diagnosis of TB Culture all specimens, even if smear or NAA negative Results in 4 14 days when liquid medium systems used Culture monthly until conversion, i.e., 2 consecutive negative cultures 90

91 Colonies of M. tuberculosisgrowing on Media 91
92 Drug-Susceptibilit y Testing Conduct drug-susceptibility testing on initial M. tb isolate Promptly forward results to the health department Repeat for patients who Do not respond to therapy or Have positive cultures despite 3months of therapy 92

93 Drug-Susceptibilit y Testing 93
94 Second-line Drug-Susceptibilit y Testing Limit to persons at increased risk for drug resistance: Have history of treatment with TB drugs Had contact with a person with drug-resistant TB Demonstrated resistance to first-line drugs Has positive smears or cultures despite 3 months of TB treatment 94
95 Molecular Detection of Drug Resistance Drug resistance is caused by mutations in specific M. tb genes Several molecular assays and tests can detect mutations Molecular detection should be used for patients with high risk for rifampin resistance (MDR TB) Conventional drug susceptibility testing should be done in conjunction with molecular tests 95
96 Genot yping Laboratory-based approach that analyzes the genetic material of patient isolates Different strains of M. tb have different genotype patterns M. tb isolates with identical genotypes often indicates recent transmission Main purpose of genotyping: add to TB controllers understanding of TB transmission in their communit y 96
97 Genot yping (cont.) Used with traditional epi investigations, genot yping has Confirmed/detected transmission Identified risk factors for recent infection Demonstrated re-infection with different strains Identified weaknesses in conventional contact investigations Documented lab cross-contamination Identified outbreaks not previously recognized 97
98 Chapter 5. Treatment for Latent Tuberculosis Infection 98
99 Treatment for Latent TB Infection (LTBI) Over 11 million persons in U.S. estimated to have LTBI (4% of population) 5%-10% will develop TB disease if untreated Treatment of LTBI essential to controlling and eliminating TB disease Reduces risk of LTBI to TB disease progression Use targeted testing to find persons at high risk for TB who would benefit from LTBI treatment Several treatment regimens available 99
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Chapter 4 Diagnosis of Tuberculosis Disease
 Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014
 TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Tuberculosis What you need to know. James Zoretic M.D., M.P.H. Regions 2 and 3 Director
 Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Core Curriculum on Tuberculosis: What the Clinician Should Know DR.RUPNATHJI( DR.RUPAK NATH )
") Core Curriculum on Tuberculosis: What the Clinician Should Know Introduction to the Core Curriculum on Tuberculosis: What the Clinician Should Know i Introduction to the Core Curriculum on Tuberculosis:
Core Curriculum on Tuberculosis: What the Clinician Should Know Introduction to the Core Curriculum on Tuberculosis: What the Clinician Should Know i Introduction to the Core Curriculum on Tuberculosis:
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Why need to havetb Clearance. To Control and Prevent Tuberculosis
 Why need to havetb Clearance To Control and Prevent Tuberculosis How to ID Tuberculosis There are two kinds of tests that are used to determine if a person has been infected with TB bacteria: the tuberculin
Why need to havetb Clearance To Control and Prevent Tuberculosis How to ID Tuberculosis There are two kinds of tests that are used to determine if a person has been infected with TB bacteria: the tuberculin
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Tuberculin Skin Testing
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Learning Objectives: Case 1 11/12/2015. Tuberculosis: Focus on Transmission and Pathogenesis. TB: Some Important Terms
 A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Primer on Tuberculosis (TB) in the United States
 in the United States") Primer on Tuberculosis (TB) in the United States The purpose of this primer is to provide instructors who have no prior background in TB research or clinical care with basic knowledge that they may find
Primer on Tuberculosis (TB) in the United States The purpose of this primer is to provide instructors who have no prior background in TB research or clinical care with basic knowledge that they may find
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Community pharmacy-based tuberculosis skin testing
 Community pharmacy-based tuberculosis skin testing Shanna K. O Connor, PharmD ISU KDHS Spring CE Seminar 2018 In support of improving patient care, Idaho State University Kasiska Division of Health Sciences
Community pharmacy-based tuberculosis skin testing Shanna K. O Connor, PharmD ISU KDHS Spring CE Seminar 2018 In support of improving patient care, Idaho State University Kasiska Division of Health Sciences
TB Transmission, Pathogenesis & Infection Control
 TB Transmission, Pathogenesis & Infection Control Bradley Allen, MD, PhD, FACP, FIDSA. 2014 MFMER slide-1 Disclosures Medical Consultant, TB Control Program Indiana State Department of Health Past clinical
TB Transmission, Pathogenesis & Infection Control Bradley Allen, MD, PhD, FACP, FIDSA. 2014 MFMER slide-1 Disclosures Medical Consultant, TB Control Program Indiana State Department of Health Past clinical
Chapter 1 Overview of Tuberculosis Epidemiology in the United States
 Chapter 1 Overview of Tuberculosis Epidemiology in the United States Table of Contents Chapter Objectives.... 1 Progress Toward TB Elimination in the United States... 3 TB Disease Trends in the United
Chapter 1 Overview of Tuberculosis Epidemiology in the United States Table of Contents Chapter Objectives.... 1 Progress Toward TB Elimination in the United States... 3 TB Disease Trends in the United
These recommendations will remain in effect until the national shortage of PPD solution has abated.
 Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
Peggy Leslie-Smith, RN
 Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer
 Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis. WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED
 Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
Frances Morgan, PhD October 21, Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS
 The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Tuberculosis Infection in the US Military
 Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
INDEX CASE INFORMATION
 Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
Replaces: 02/11/16. Formulated: 7/95 EMPLOYEE TB TESTING
 Effective : 02/09/17 Page 1 of 4 PURPOSE: To describe the process where by employees may obtain routine TB skin testing by facility medical staff. POLICY: Employees of the Texas Department of Criminal
Effective : 02/09/17 Page 1 of 4 PURPOSE: To describe the process where by employees may obtain routine TB skin testing by facility medical staff. POLICY: Employees of the Texas Department of Criminal
Tuberculosis. Impact of TB. Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH)
") Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
The Air We Share: Principles and Practices of TB Infection Control
 The Air We Share: Principles and Practices of TB Infection Control Session Four of a Four-Part Webinar Series Presented in Partnership with the BC Lung Association January 10, 2014 Facilitators: Nash Dhalla,
The Air We Share: Principles and Practices of TB Infection Control Session Four of a Four-Part Webinar Series Presented in Partnership with the BC Lung Association January 10, 2014 Facilitators: Nash Dhalla,
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Yakima Health District BULLETIN
 Yakima Health District BULLETIN Summary Volume 13, Issue 1 February, 2014 Tuberculosis in Yakima County The rate of active tuberculosis (TB) in Yakima County has declined by about two-thirds over the past
Yakima Health District BULLETIN Summary Volume 13, Issue 1 February, 2014 Tuberculosis in Yakima County The rate of active tuberculosis (TB) in Yakima County has declined by about two-thirds over the past
CUSOM Student Health Immunization Requirements
 CUSOM Student Health Immunization Requirements Regulatory and legislative authorities require that students demonstrate immunization, immunity and/or protection from multiple contagious diseases before
CUSOM Student Health Immunization Requirements Regulatory and legislative authorities require that students demonstrate immunization, immunity and/or protection from multiple contagious diseases before
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
2017/2018 Annual Volunteer Tuberculosis Notice
 Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
Advanced Concepts in Pediatric Tuberculosis
 Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks
 1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On
1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On
Tuberculosis & Refugees in Philadelphia
 Tuberculosis & Refugees in Philadelphia Philadelphia TB Control Program Daniel P. Dohony, MPH Philadelphia TB Control Program Health Information Portal Website: hip.phila.gov Contains Information On» Disease
Tuberculosis & Refugees in Philadelphia Philadelphia TB Control Program Daniel P. Dohony, MPH Philadelphia TB Control Program Health Information Portal Website: hip.phila.gov Contains Information On» Disease
TUBERCULOSIS TODAY WORLD-WIDE, UNITED STATES, TEXAS J O R D A N C O U L S O N, R. N. S N S C O O R D I N A T O R, P H E P / H S R 1
 TUBERCULOSIS TODAY WORLD-WIDE, UNITED STATES, TEXAS J O R D A N C O U L S O N, R. N. S N S C O O R D I N A T O R, P H E P / H S R 1 WHAT IS TB? TB is a disease caused by a bacterium called Mycobacterium
TUBERCULOSIS TODAY WORLD-WIDE, UNITED STATES, TEXAS J O R D A N C O U L S O N, R. N. S N S C O O R D I N A T O R, P H E P / H S R 1 WHAT IS TB? TB is a disease caused by a bacterium called Mycobacterium
HEALTHWEST PROCEDURE. No Revised by: Effective: December 1, 1995 Revised: April 19, 2017 Environment of Care Committee
 HEALTHWEST PROCEDURE Revised by: Effective: December 1, 1995 Revised: April 19, 2017 Environment of Care Committee Approved by: Subject: Tuberculosis Infection Control Julia Rupp, Executive Director I.
HEALTHWEST PROCEDURE Revised by: Effective: December 1, 1995 Revised: April 19, 2017 Environment of Care Committee Approved by: Subject: Tuberculosis Infection Control Julia Rupp, Executive Director I.
FLORIDA DEPARTMENT OF JUVENILE JUSTICE DETENTION SERVICES FACILITY MEDICAL POLICIES
 FLORIDA DEPARTMENT OF JUVENILE JUSTICE DETENTION SERVICES FACILITY MEDICAL POLICIES Superintendent Signature Designated Health Authority Signature Effective Date: November 1, 2016 Subject: TUBERCULOSIS
FLORIDA DEPARTMENT OF JUVENILE JUSTICE DETENTION SERVICES FACILITY MEDICAL POLICIES Superintendent Signature Designated Health Authority Signature Effective Date: November 1, 2016 Subject: TUBERCULOSIS
TB Laboratory for Nurses
 TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
Advanced Concepts in Pediatric TB: Latent TB Infection
 Welcome to the second of eight sessions on Advanced Concepts in Pediatric TB, sponsored by the Southeastern National Tuberculosis Center. Today we present the in Pediatric TB. Today s presenter is Dr.
Welcome to the second of eight sessions on Advanced Concepts in Pediatric TB, sponsored by the Southeastern National Tuberculosis Center. Today we present the in Pediatric TB. Today s presenter is Dr.
Tuberculosis 6/7/2018. Objectives. What is Tuberculosis?
 Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
CDC IMMIGRATION REQUIREMENTS:
 CDC IMMIGRATION REQUIREMENTS: Technical Instructions for Tuberculosis Screening and Treatment Using Cultures and Directly Observed Therapy October 1, 2009 Table of Contents Preface...i Tuberculosis Screening...1
CDC IMMIGRATION REQUIREMENTS: Technical Instructions for Tuberculosis Screening and Treatment Using Cultures and Directly Observed Therapy October 1, 2009 Table of Contents Preface...i Tuberculosis Screening...1
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
(a) Infection control program. The facility must establish an infection control program under which it--
 Infection control program. The facility must establish an infection control program under which it--") 420-5-10-.17 Infection Control. (1) The facility must establish and maintain an infection control program designed to provide a safe, sanitary, and comfortable environment and to help prevent the development
420-5-10-.17 Infection Control. (1) The facility must establish and maintain an infection control program designed to provide a safe, sanitary, and comfortable environment and to help prevent the development
Stop TB Poster (laminated copies are available from TB Control: )
") Tuberculosis Prevention and Control Recommendations For Homeless Shelters in Maine Tool Kit What Your Shelter Can Do to Prevent TB Assessing Your Shelter Guests Risk for TB Cough Alert Policy Think TB
Tuberculosis Prevention and Control Recommendations For Homeless Shelters in Maine Tool Kit What Your Shelter Can Do to Prevent TB Assessing Your Shelter Guests Risk for TB Cough Alert Policy Think TB
Symptoms Latent TB Active TB
 1 Tuberculosis Tuberculosis (TB) is a disease that can spread through the air. It is caused by a bacterium called Mycobacterium tuberculosis. It usually affect the lungs. However, it can also affect other
1 Tuberculosis Tuberculosis (TB) is a disease that can spread through the air. It is caused by a bacterium called Mycobacterium tuberculosis. It usually affect the lungs. However, it can also affect other
SWABCHA Fact Sheet: Tuberculosis (TB)
") SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
The Most Widely Misunderstood Test of All
 The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Student Health Requirements Master of Arts, Biomedical Sciences Program
 Student Health Requirements Master of Arts, Biomedical Sciences Program All students in medically related programs, just as physicians in practice, are required to be current with required immunizations
Student Health Requirements Master of Arts, Biomedical Sciences Program All students in medically related programs, just as physicians in practice, are required to be current with required immunizations
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
Mycobacterium tuberculosis. Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology
 Dr.Baha, AL-Amiedi Ph. D.Microbiology") Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
Investigation of Contacts of Persons with Infectious Tuberculosis, 2005
 1 Investigation of Contacts of Persons with Infectious Tuberculosis, 2005 Daniel P. Dohony, MPH Division of Tuberculosis Elimination Centers for Disease Control and Prevention and Philadelphia TB Control
1 Investigation of Contacts of Persons with Infectious Tuberculosis, 2005 Daniel P. Dohony, MPH Division of Tuberculosis Elimination Centers for Disease Control and Prevention and Philadelphia TB Control
Asking the Right Questions. A Visual Guide to Tuberculosis Case Management for Nurses. Reference Guide
 Asking the Right Questions A Visual Guide to Tuberculosis Case Management for Nurses Reference Guide The Francis J. Curry National Tuberculosis Center is a joint project of the San Francisco Department
Asking the Right Questions A Visual Guide to Tuberculosis Case Management for Nurses Reference Guide The Francis J. Curry National Tuberculosis Center is a joint project of the San Francisco Department
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
Block Grant Requirements and Tuberculosis in Substance Abusing Populations
 Block Grant Requirements and Tuberculosis in Substance Abusing Populations Christine Pickens RNBC,M.Ed. Operation Par, Inc. This product is supported by Florida Department of Children and Families Substance
Block Grant Requirements and Tuberculosis in Substance Abusing Populations Christine Pickens RNBC,M.Ed. Operation Par, Inc. This product is supported by Florida Department of Children and Families Substance
What Drug Treatment Centers Can do to Prevent Tuberculosis
 What Drug Treatment Centers Can do to Prevent Tuberculosis Tuberculosis (TB) is alive and well Learn what you can do to prevent TB among your clients and protect yourself! Transmission TB is spread through
What Drug Treatment Centers Can do to Prevent Tuberculosis Tuberculosis (TB) is alive and well Learn what you can do to prevent TB among your clients and protect yourself! Transmission TB is spread through
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
"GUARDING AGAINST TUBERCULOSIS IN INSTITUTIONAL FACILITIES"
 MAJOR PROGRAM POINTS "GUARDING AGAINST TUBERCULOSIS IN INSTITUTIONAL FACILITIES" Training For THE CDC "TUBERCULOSIS PREVENTION GUIDELINES" "Quality Safety and Health Products, for Today...and Tomorrow"
MAJOR PROGRAM POINTS "GUARDING AGAINST TUBERCULOSIS IN INSTITUTIONAL FACILITIES" Training For THE CDC "TUBERCULOSIS PREVENTION GUIDELINES" "Quality Safety and Health Products, for Today...and Tomorrow"
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
TB and Respiratory Protection
 Slide 1 TB and Respiratory Protection Tuberculosis (TB) is a disease present throughout the United States. Lehigh Valley Health Network is concerned about your health and needs your help to prevent the
Slide 1 TB and Respiratory Protection Tuberculosis (TB) is a disease present throughout the United States. Lehigh Valley Health Network is concerned about your health and needs your help to prevent the
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers. Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program
 Transmission in Ambulatory Surgery Centers. Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program") Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program Topics of Discussion TB Overview Epidemiology of TB in Oregon Annual Facility
Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program Topics of Discussion TB Overview Epidemiology of TB in Oregon Annual Facility
Appendix B. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial update) 1.1 Short title Tuberculosis
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial update) 1.1 Short title Tuberculosis
Chapter 7 Tuberculosis Infection Control
 Chapter 7 Tuberculosis Infection Control Table of Contents Chapter Objectives.... 187 Introduction.... 189 Infectiousness.... 190 TB Infection Control Measures... 194 TB Infection Control Program................................................
Chapter 7 Tuberculosis Infection Control Table of Contents Chapter Objectives.... 187 Introduction.... 189 Infectiousness.... 190 TB Infection Control Measures... 194 TB Infection Control Program................................................
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening