TB Intensive San Antonio, Texas May 7-10, 2013
|
|
|
- Coral O’Neal’
- 6 years ago
- Views:
Transcription
1 TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant financial relationships with any commercial companies pertaining to this educational activity 1
2 Tuberculosis in the HIV Patient Lisa Y. Armitige, MD, PhD Medical Consultant Heartland TB Center Associate Professor of Medicine/Pediatrics University of Texas HSC at Tyler Effect of HIV on Tuberculosis Epidemiology 2

3 Estimated Incidence of TB per 100,000 Population in African Countries in 1990 and 2005 Chaisson R and Martinson N. N Engl J Med 2008;358: Newly reported cases of tuberculosis per persons by year in the United States, 1980 to 1995 Snider, G. L. Ann Intern Med 1997;126:

4 % Coinfection Estimated HIV Coinfection in Persons Reported with TB, United States, * Aged All Ages *Updated as of July 21, 2011 Note: Minimum estimates based on reported HIV-positive status among all TB cases in the age group Outcomes of Exposure to M. tuberculosis Inhalation of Droplet Nuclei Regional replication in lungs, dissemination ~90% ~5% ~5% Killing, clearance of organisms Latent disease Active disease 4
5 Outcomes of Exposure to M. tuberculosis in HIV-negative and HIV-positive patients Inhalation of Droplet Nuclei Regional replication in lungs, dissemination ~90% 10% reactivation ~5% reactivation per year lifetime Up to 36% active disease ~5% Killing, clearance of organisms Latent disease Active disease Signs & Symptoms - Pulmonary TB Pulmonary Symptoms: Productive, prolonged cough of over 3 weeks duration Chest pain Hemoptysis Systemic Symptoms: Fever Chills Night sweats Appetite loss Weight loss Easy fatigability 5
6 An Algorithm for Tuberculosis Screening and Diagnosis in People with HIV N Engl J Med 2010;362: An Algorithm for Tuberculosis Screening and Diagnosis in People with HIV N Engl J Med 2010;362:
7 Clinical Presentation HIV-positive vs. HIV-negative patients Driven mostly by degree of immunity HIV-positive patients are more likely to have: Isolated extrapulmonary localization (53-63% in some studies) Primary infection Pulmonary basilar involvement Tuberculous pneumonia Hilar or mediastinal lymphadenopathies Miliary or disseminated TB Normal CXR (8-20% in some studies) Clinical Microbiology and Infection, Volume 10 Number 5, May 2004 Testing for TB Infection -TST The tuberculin skin test (TST) may help differentiate infected from uninfected people with signs and symptoms A negative TST does not exclude the diagnosis of TB (especially for patient s with severe TB illness or infection with HIV) 7
8 Classifying the Tuberculin Reaction 5 mm is classified as positive in HIV-positive persons Recent contacts of TB case Persons with fibrotic changes on chest radiograph consistent with old healed TB Patients with organ transplants and other immunosuppressed patients Diagnosis * * Clinical Microbiology and Infection, Volume 10 Number 5, May



9 IFN-γ (gamma) release assays (IGRAs) Antigens for Gamma-Release Assays 9
 T-SPOT.")
10 FDA-approved IGRAs Quantiferon-Gold In-Tube (IT) T-SPOT.TB Quantiferon Gold In-Tube 10
11 ELISPOT S. A. Clark et al Clinical and Experimental Immunology Poor concordance between interferon-γ release assays and tuberculin skin tests in diagnosis of latent tuberculosis infection among HIV-infected individuals BMC Infectious Diseases 2009, 9:15 Cross sectional study in 2 HIV clinics in Atlanta, Georgia (n= 336), 85% black, 65% male, 91% US-born, 69% on HAART, 60% with a history of an OI. Median CD4 = 334, median viral load 400 copies/ml Conclusion: We found a low prevalence of LTBI and poor concordance between all 3 diagnostic tests (TST, QF-IT, T-SPOT.TB). 11
12 Role of Interferon Gamma Release Assay in Active TB Diagnosis among HIV Infected Individuals PLoS ONE May vol 4(5) 105 HIV/TB patients in India 50% were culture positive 31% were TST positive Sensitivity decreased with declining CD4 count 65% were positive by Quantiferon-IT More indeterminate results with CD4 <200 Role of interferon-gamma release assays in the diagnosis of pulmonary tuberculosis in patients with advanced HIV infection Cattamanchi et al. BMC Infectious Diseases 2010, 10:75 ** 12
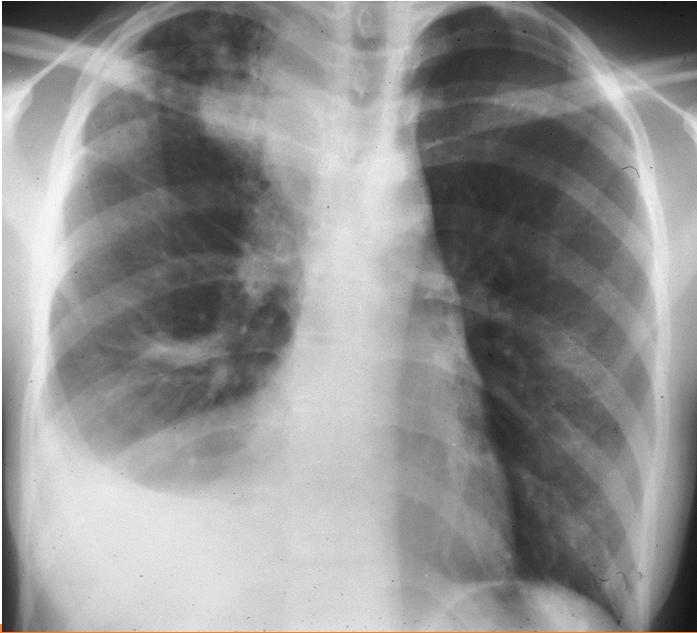
13 CXR HIV infected persons In HIV-infected persons almost any abnormality on CXR may indicate TB May cause infiltrates without cavities in any lung zone May cause mediastinal or hilar lymphadenopathy with or without infiltrates or cavities Clinical Presentation HIV-positive vs. HIV-negative patients Driven mostly by degree of immunity HIV-positive patients are more likely to have: Isolated extrapulmonary localization (53-63% in some studies) Primary infection Pulmonary basilar involvement Tuberculous pneumonia Hilar or mediastinal lymphadenopathies Miliary or disseminated TB Normal CXR (8-20% in some studies) Clinical Microbiology and Infection, Volume 10 Number 5, May
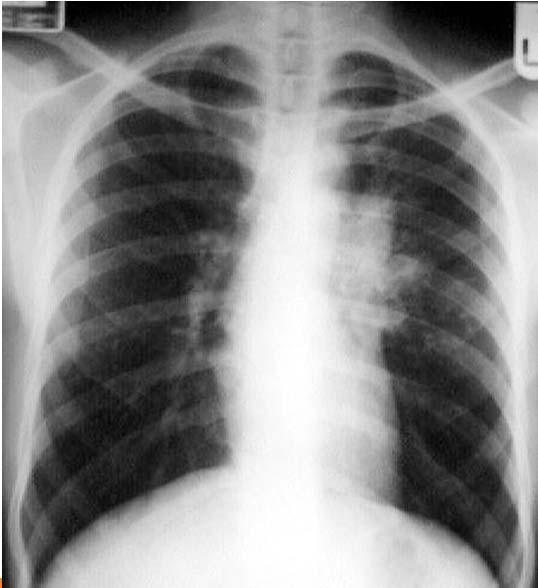
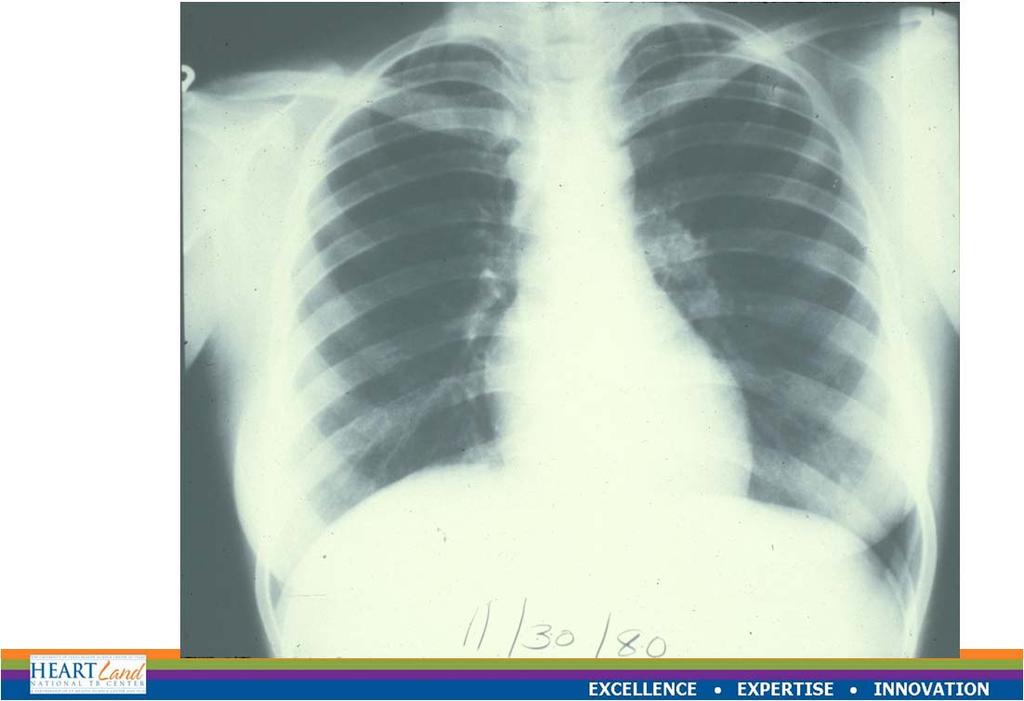
14 Primary Tuberculosis 14
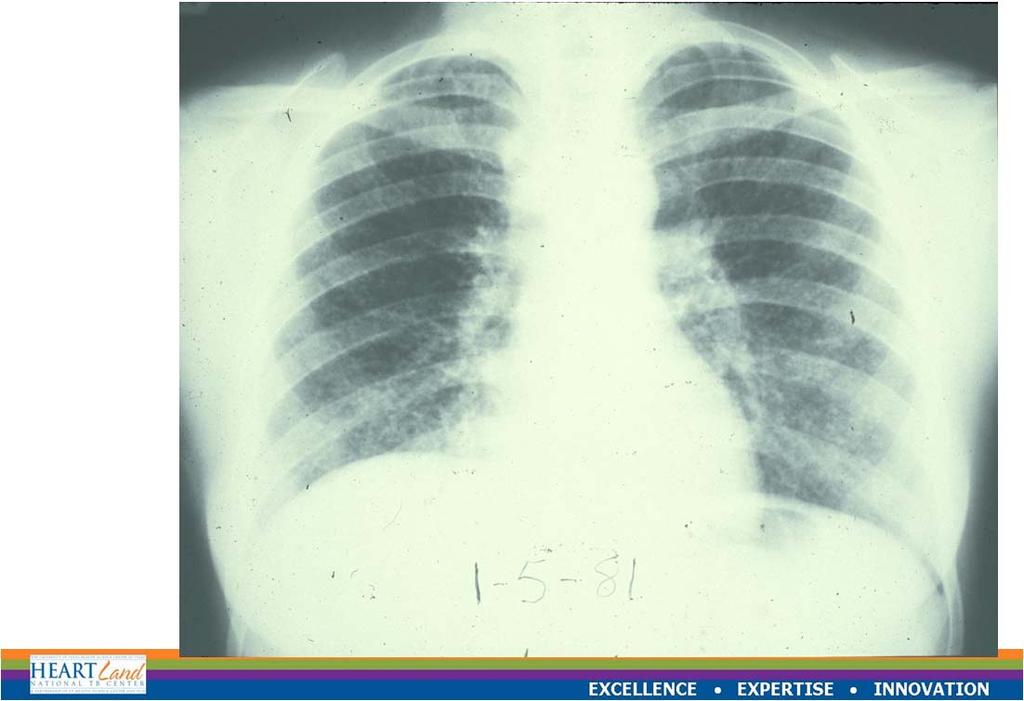
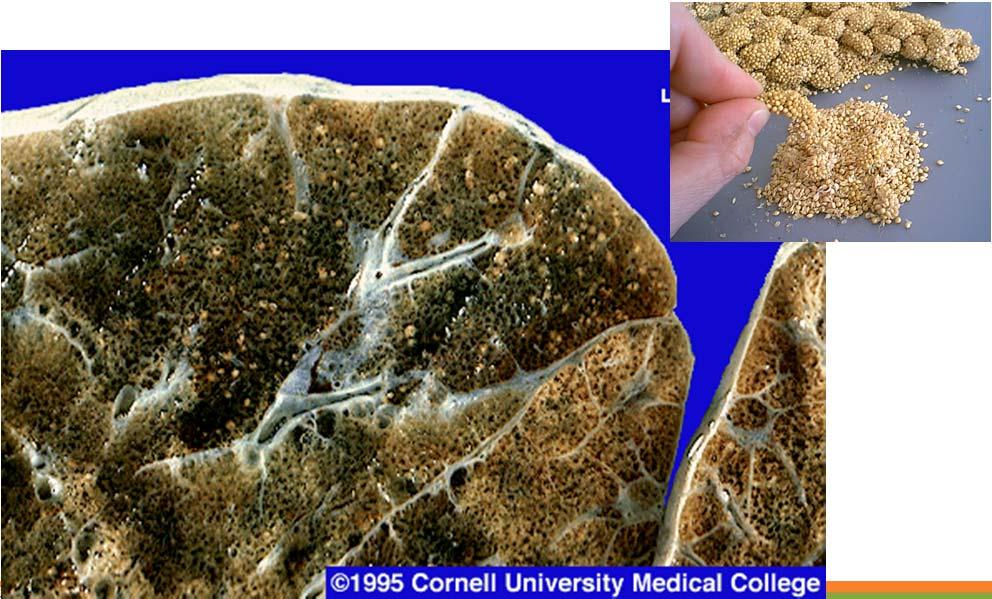
15 Miliary Tuberculosis 15
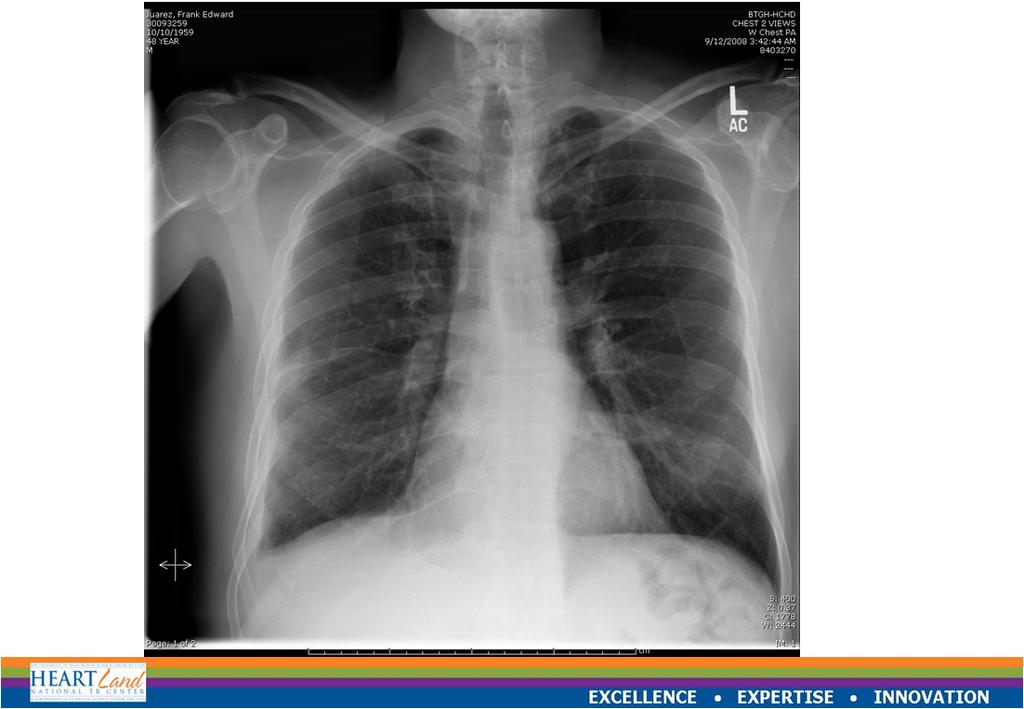
16 Tuberculosis and HIV 16
17 CXR Special Situations Pregnant women who are highly suspicious and being evaluated for active disease should undergo a CXR without delay, even during the first trimester Patients suspected of extrapulmonary TB should have a CXR to rule out pulmonary TB Bacteriologic or histologic exam Sputum Three (8-24 hours apart, at least one first thing in the morning) Tissue Lymph node biopsy Bone marrow biopsy Other specimens Urine CSF Peritoneal fluid Pleural fluid (pleural biopsy) 17

18 Diagnosis * * * Clinical Microbiology and Infection, Volume 10 Number 5, May 2004 An Algorithm for Tuberculosis Screening and Diagnosis in People with HIV N Engl J Med 2010;362:
19 Diagnosis Summary Must have a high index of suspicion Must utilize many pieces of information in making the diagnosis TB can present very differently in HIVinfected patients when compared to HIVnegative patients Case Scenario #1 A 35 year old HIV+ man (A.G.) is referred to you for a TST measuring 12 mm. On questioning, the patient states he was skin tested because one of his roommates was diagnosed with pulmonary cavitary TB. How should you approach this patient? 19
20 Classifying the Tuberculin Reaction 5 mm is classified as positive in HIV-positive persons Recent contacts of TB case Persons with fibrotic changes on chest radiograph consistent with old healed TB Patients with organ transplants and other immunosuppressed patients Case Scenario # 1 (cont) A.G. reveals his TST 3 years ago was negative. He currently takes Atripla (efavirenz-based treatment), his CD4 count is 453 and his viral load is <40. He has HCV and hypertension managed with HCTZ. 20
21 Case Scenario #1 (cont) He has 2 other roommates who will see you later this week. They are also HIV+ but were TST-negative. How would you evaluate these individuals? Case Scenario #1 (cont) Roommate #1 only recently moved into the home. He has a CD4 count of 638, takes no meds, has no significant health issues and denies any current symptoms. Roommate #2 was recently diagnosed with HIV and is not currently on medications. His CD4 count is 45 and he has a cough he attributes to post-nasal drip. He feels well, denies weight loss or other suggestive symptoms. 21
22 Testing for TB Infection - Principles Individuals who have a + TST result, a + IGRA result or symptoms suggestive of TB (regardless of TST/IGRA results) should be evaluated with an chest x-ray Patients with HIV who may not react to testing by TST or IGRA should have a chest x-ray if TB is suspected or if exposed to an active TB case If abnormalities are noted, or the client has symptoms suggestive of extrapulmonary TB, additional diagnostic tests should be conducted CXR HIV infected persons In HIV-infected persons almost any abnormality on CXR may indicate TB May cause infiltrates without cavities in any lung zone May cause mediastinal or hilar lymphadenopathy with or without infiltrates or cavities 22
23 Case Scenario #1 (cont) Assuming a negative CXR in all three, how would you approach each patient? A.G. (TST 12 mm, CD4 453, HCV, denies symptoms) Roommate #1 (TST 0mm, CD4 638, no symptoms) Roommate #2 (TST 0mm, CD4 45, cough, no symptoms) Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents, MMWR 2009 HIV-infected persons, regardless of age, should be treated for LTBI if they have no evidence of active TB and exhibit the following characteristics: 1) a positive diagnostic test for LTBI and no prior history of treatment for active or latent TB (AI); 2) a negative diagnostic test for LTBI but are close contacts of persons with infectious pulmonary TB (AII); and 3) a history of untreated or inadequately treated healed TB (i.e., old fibrotic lesions on chest radiography) regardless of diagnostic tests for LTBI (AII) 23
24 Risk reduction by treatment of Latent TB Infection (LTBI) in HIV-infected patients Churchyard et al. JID 2007:196 (Suppl 1) S52 Initiating Treatment for LTBI Before initiating treatment for LTBI Rule out TB disease i.e. wait for culture results if specimen obtained Determine prior history of treatment for LTBI or TB disease Assess risks and benefits of treatment Determine current and previous drug therapy 24
25 Isoniazid Regimens for LTBI 9-month regimen of isoniazid (INH) is the preferred regimen 6-month regimen is less effective but may be used if unable to complete 9 months May be given daily or intermittently (twice weekly) Use directly observed therapy (DOT) for intermittent regimen Persons with the following conditions need special precautions while on isoniazid a. Age 35 years and over b. Taking other medications on a long term basis c. Alcohol abusers d. History of previous discontinuation of isoniazid because of toxicity/adverse reactions e. Chronic liver disease f. Peripheral neuropathy g. Pregnancy 25
26 Rifampin Regimens for LTBI Rifampin (RIF) given daily for 4 months is an acceptable alternative when treatment with INH is not feasible. In situations where RIF cannot be used (e.g., HIV-infected persons receiving protease inhibitors), rifabutin may be substituted. RIF and PZA for 2 months should generally not be offered due to risk of severe adverse events 6 6 MMWR August 8, 2003; 52 (31): LTBI treatment MMWR August 8, 2003 / Vol. 52 / No
27 3HP Regimen and HIV patients 12 week regimen of INH and Rifapentine dosed once a week Contraindicated in patients on ANY antiretrovirals Acceptable if not on HIV medications Case Scenario #1 (cont) Assuming a negative CXR in all three, how would you approach each patient? A.G. (TST 12 mm, CD4 453, HCV, denies symptoms) Roommate #1 (TST 0mm, CD4 638, no symptoms) Roommate #2 (TST 0mm, CD4 45, cough, no symptoms) 27
28 Case Scenario #2 A 28 year old Latino male with HIV presents with a 2 ½ month history of productive cough, night sweats, fevers, fatigue and 30 lb weight loss. The patient has been under the care of an ID physician for his HIV and has been stable on a protease inhibitor (PI)- containing regimen. The patient has been working construction out of state and has not been able to visit his doctor until now. He has been compliant with his HIV meds and his current laboratory studies show a CD4 count of 281 and viral load <50. Two of 3 sputums collected on consecutive days are positive for AFB Which anti-tb regimen do you start him on? What do you do with his HIV meds? Anti-Tuberculosis drugs (ATS/CDC/IDSA) First-Line drugs Isoniazid Rifampin Rifapentine Rifabutin* Ethambutol Pyrazinamide *Not FDA approved for TB Second-Line Drugs Cylcoserine Ethionamide Levofloxacin* Moxifloxacin* PAS Streptomycin Amikacin/Kanamycin Capreomycin 28
29 Purpose 1 5. Recommended Treatment Regimens 36 What s New In this Document 1 CONTENTS OF 6. Practical Aspects of Treatment 42 Summary 1 THE 80 Page 7. Drug Interactions Introduction and Background 13 Document 8. Treatment in Special Situations Organization and Supervision of Treatment Management of Relapse, Treatment Failure, and 66 Drug Resistance 3. Drugs in Current Use Treatment of Tuberculosis in Low Income Countries: Recommendations and Guidelines of the WHO and the IUATLD Principles of Antituberculosis Chemotherapy Research Agenda for Tuberculosis Treatment 74 Updates and Changes in Therapy Changes in dosing schedules: HIV + individuals with low CD4 counts should NOT be given twice weekly therapy Daily therapy can be 7 days per week OR can be 5 days per week IF given by DOT and the Mtb is drug susceptible 29
30 Role of New Agents Rifabutin (RBT): May be used as a primary drug for patients (especially HIV+) receiving medications having unacceptable interactions with rifampin (e.g. Protease Inhibitors, methadone) Fluoroquinolones: May be used when first line drugs are not tolerated or the organism is resistant Moxifloxacin is rapidly becoming the agent of choice ATS recommendations for treatment of tuberculosis * * Morbidity and Mortality Weekly Report June 20, 2003 / Vol. 52 / No. RR 11 30

31 Rifamycins Have significant interaction with all ARVs except nucleoside analogues (other than AZT) and enfuvirtide Once or twice weekly regimens show high rate of rifampin resistance in HIV patients with CD4 cell count <100 Most common locus of interaction is the cytochrome P450 system As inducers, rifampin > rifapentine > rifabutin Effect of efavirenz dosing with rifampin on treatment outcomes Manosuthi et al AIDS 2005, 19: Manosuthi et al AIDS 2006, Vol 20 No 1 31
32 Rifampin and PIs Note: Decrease in serum protease inhibitor level is NOT overcome by low dose ritonavir Clinical Microbiology and Infection, Volume 10 Number 5, May 2004 Rifabutin Has much less effect than rifampin on drugs metabolized by CYP3A Requires dosage adjustment due to effects by many other drugs (such as ritonavir). PIs (especially if boosted with ritonavir) cause a marked increase in serum rifabutin serum concentrations and toxicity Rifabutin dose should be decreased when using PI-based regimens. Concerns regarding adequate dosing if patient is not compliant with PI medication 32
")
33 Rifabutin Good virological and immunological outcomes when administered with PI-based HAART Treatment of choice when pt cannot tolerate NNRTIbased treatment (though no head-to-head studies) Expensive 33
 Rifampin (no change)")
34 Commonly used HIV medications and rifamycins Efavirenz (Sustiva/Atripla) Rifampin (no change) Rifabutin mg Protease Inhibitors Rifampin contraindicated Rifabutin 150 mg daily or 300 mg TIW 34

35 Treatment - Summary Every effort should be made to treat within the CDC guidelines to increase the chances of treatment success, decrease the chances of relapse and minimize the length of time with toxicities. Rifamycins can be safely added to almost any regimen. TB treatment regimens that do not contain rifampin have an unacceptably high failure rate Overall Treatment Outcomes * * Ronan. A. M. JID 2006:193 (15 May)


36 When should treatment be started when patient is being treated for TB? Considerations Treatment of HIV improves outcomes in patients with TB Decreased death or relapse Multiple medications with multiple potential toxicities that are overlapping 36
37 Initiation of ART in patients with HIV/TB In patients with CD4 counts <50 cells/mm 3, ART should be initiated within 2 weeks of starting TB treatment (AI) In patients with CD4 counts 50 cells/mm 3 who present with clinical disease of major severity as indicated by clinical evaluation, ART should be initiated within 2 to 4 weeks of starting TB treatment. The strength of this recommendation varies on the basis of CD4 cell count: CD4 count 50 to 200 cells/mm3 (BI) CD4 count >200 cells/mm3 (BIII) In patients with CD4 counts 50 cells/mm 3 who do not have severe clinical disease, ART can be delayed beyond 2 to 4 weeks of starting TB therapy but should be started within 8 to 12 weeks of TB therapy initiation. The strength of this recommendation also varies on the basis of CD4 cell count: CD4 count 50 to 500 cells/mm3 (AI) CD4 count >500 cells/mm3 (BIII) Additional recommendations for patients with HIV/TB Despite pharmacokinetic drug interactions, a rifamycin (rifampin or rifabutin) should be included in TB regimens for patients receiving ART, with dosage adjustment if necessary (AII). Rifapentine (RPT) is NOT recommended in HIV-infected patients receiving ART for treatment of latent TB infection (LTBI) or active TB, unless in the context of a clinical trial (AIII). Immune reconstitution inflammatory syndrome (IRIS) may occur after initiation of ART. Both ART and TB treatment should be continued while managing IRIS (AIII). Treatment support, which can include directly observed therapy (DOT) of TB treatment, is strongly recommended for HIV-infected patients with active TB disease (AII). 37

38 Case Scenario #3 A 30 year old black woman presents with fever, chills, night sweats and a 20 lb weight loss over the past month. She has large anterior cervical lymph nodes and a left lower lobe infiltrate. Biopsy of one of the lymph nodes reveals granulomas and AFB which are probe positive for Mtb. After further testing, the patient is found to be HIV positive with a CD4 count of 80. The patient is started on 4 drug therapy and, once stable on anti-tb drugs, is started on HAART with efavirenz. Two months into treatment, the patient has worsening cough, a return of fevers, night sweats and worsening LAD. How do you proceed with this patient? IRIS Meintjes et al Lancet ID 8:

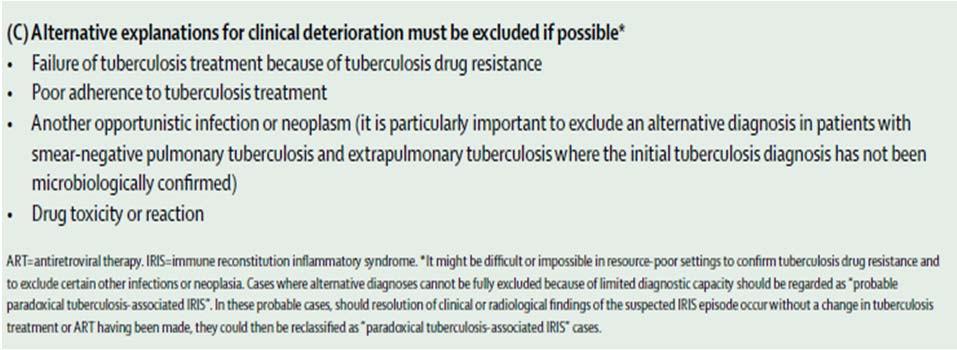
39 IRIS Meintjes et al Lancet ID 8: IRIS Meintjes et al Lancet ID 8:

40 One more thing Co-trimoxazole prophylaxis Nunn et al. BMJ 2008;337;a257 40
41 THEY ALWAYS COME BACK Do It Right The First Time! Barbara Seaworth Thanks!! Questions? Heartland National Tuberculosis Center TEX-LUNG 41
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas. TB/HIV Co-Infection. Lisa Armitige, MD, PhD has the following disclosures to make:
 TB Intensive San Antonio, Texas August 2-5, 2011 TB/HIV Co-Infection Lisa Armitige, MD, PhD August 4, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas August 2-5, 2011 TB/HIV Co-Infection Lisa Armitige, MD, PhD August 4, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB Intensive Tyler, Texas December 2-4, Tuberculosis and HIV Co-Infection. Lisa Y. Armitige, MD, PhD. December 4, 2008.
 TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
TB/HIV Co-Infection. Tuberculosis and HIV
 TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
TB and Co-Morbidities Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 TB and Co-Morbidities Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 TB and Co-Morbidities Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Co-morbidities that Impact Managing TB Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Co-morbidities that Impact Managing TB Lisa Armitige, MD, PhD November 17, 2010 Co-morbidities in Substance Abuse that Impact
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Co-morbidities that Impact Managing TB Lisa Armitige, MD, PhD November 17, 2010 Co-morbidities in Substance Abuse that Impact
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD
 Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J. Regional Chest Clinic New Jersey State TB Physician Advisory Board Cooper Univ. Hospital EIP Program TB and HIV
Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J. Regional Chest Clinic New Jersey State TB Physician Advisory Board Cooper Univ. Hospital EIP Program TB and HIV
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Treatment of Tuberculosis
 TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
8/28/2017. Learning Objectives. After attending this presentation, learners will be able to:
 New and Noteworthy in Tuberculosis Diagnostics and Treatment Susan Swindells, MBBS Professor of Internal Medicine University of Nebraska Medical Center Omaha, Nebraska San Antonio, Texas: August 21 to
New and Noteworthy in Tuberculosis Diagnostics and Treatment Susan Swindells, MBBS Professor of Internal Medicine University of Nebraska Medical Center Omaha, Nebraska San Antonio, Texas: August 21 to
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
TB and Comorbidities Adriana Vasquez, MD April 12, 2018
 TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
Clinical Vignette: Patient 1. Approach to Co-infection with TB. TB and HIV Co-infection: Some Resources. Objectives.
 TB and HIV Co-infection: Some Resources http://www.cdc.gov/tb AETC Natl Resource Center: http://www.aidsetc.org Approach to Co-infection with TB and HIV: 2012 Henry Fraimow, MD Consultant, Southern N.J.
TB and HIV Co-infection: Some Resources http://www.cdc.gov/tb AETC Natl Resource Center: http://www.aidsetc.org Approach to Co-infection with TB and HIV: 2012 Henry Fraimow, MD Consultant, Southern N.J.
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
CLINICAL VIGNETTE: Patient 1. Approach to Co-infection with TB and HIV: TB and HIV Co-infection: Some Resources. Goals and Objectives
 TB and HIV Co-infection: Some Resources http://www.cdc.gov/tb http://www.umdnj.edu/globaltb/coretbresources.htm Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J.
TB and HIV Co-infection: Some Resources http://www.cdc.gov/tb http://www.umdnj.edu/globaltb/coretbresources.htm Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J.
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Treatment of Tuberculosis
 Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Tuberculosis: Where Are We Now?
 Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
TB in the Correctional Setting Florence, Arizona October 7, 2014
 TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012
 TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)
") Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
Latent TB Infection (LTBI) Strategies for Detection and Management
 Strategies for Detection and Management") Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Tuberculosis, HIV, and Corrections James B. McAuley, MD, MPH April 22, 2009
 TB in the Correctional Setting Collinsville, Illinois April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD, MPH April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD
TB in the Correctional Setting Collinsville, Illinois April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD, MPH April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
Tuberculosis Intensive November 17 20, 2015 San Antonio, TX
 Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Treatment of Tuberculosis
 Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
Latent tuberculosis infection
 EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
Non-rifampin rifamycins in TB/HIV
 Non-rifampin rifamycins in TB/HIV Richard E. Chaisson, MD Johns Hopkins University Center for TB Research Consortium to Respond Effectively to the AIDS-TB Epidemic Rifamycins for TB Inhibit bacterial DNA-dependent
Non-rifampin rifamycins in TB/HIV Richard E. Chaisson, MD Johns Hopkins University Center for TB Research Consortium to Respond Effectively to the AIDS-TB Epidemic Rifamycins for TB Inhibit bacterial DNA-dependent
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB Clinical Guidelines: Revision Highlights March 2014
 TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Immune Reconstitution Inflammatory Syndrome. Dr. Lesego Mawela
 Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
11/3/2009 SECOND EDITION Madhukar Pai McGill University. ISTC Training Modules Introduction
 SECOND EDITION 2009 Madhukar Pai McGill University Introduction 1 Purpose of ISTC ISTC Version 2: Key Points 21 Standards Differ from existing guidelines: standards present what should be done, whereas,
SECOND EDITION 2009 Madhukar Pai McGill University Introduction 1 Purpose of ISTC ISTC Version 2: Key Points 21 Standards Differ from existing guidelines: standards present what should be done, whereas,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011
 ART Treatment Guideline Training 31 st January to 4 th February, 2011") TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis 6/7/2018. Objectives. What is Tuberculosis?
 Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE MAY 8-11, 2018 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. List
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE MAY 8-11, 2018 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. List
Tuberculosis and Diabetes Dec. 10, 2009 Dean Schillinger, M.D. and Gisela Schecter, M.D., M.P.H. 1 of 18
 Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Tuberculosis. WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED
 Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
Treatment of Tuberculosis
 Recommendations and Reports June 20, 2003 / 52(RR11);1-77 Recommendations and Reports June 20, 2003 / 52(RR11);1-77 Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society
Recommendations and Reports June 20, 2003 / 52(RR11);1-77 Recommendations and Reports June 20, 2003 / 52(RR11);1-77 Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000