TB Intensive Houston, Texas
|
|
|
- Adela Stanley
- 5 years ago
- Views:
Transcription
1 TB Intensive Houston, Texas October 15-17, Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to make: No conflict of interests No relevant financial relationships with any commercial companies pertaining to this educational activity 1
2 Diagnosis of Tuberculosis Radiology Rosa M Estrada Y Martin, MD MSc FCCP Associate Professor Pulmonary, Critical Care and Sleep Medicine Divisions The University of Texas Health Science Center at Houston Primary tuberculosis Outline Reactivation tuberculosis (post primary) Tuberculosis in HIV infected adults and immunocompromised patients Extrapulmonary tuberculosis CT scanning 2
3 Primary Tuberculosis TB is divided into primary and post primary (or reactivation) 20 30% of the new cases are primary TB in adults (prevalence of TB has decreased in developed countries) Confirmation of TB is more important Most resolve spontaneously, but reactivation may occurs without t treatmentt t Smears are positive in < 20% Cultures are positive in 50% Primary Tuberculosis Most pts are asymptomatic; fever and nonproductive cough may occur Symptoms are due to progression to active disease Opacities are seen in middle and lower lungs Commonly unilateral Lymph node enlargement often occurs, and may cause bronchial compression 3
4 Primary Tuberculosis Seen in pts not previously exposed to M tuberculosis, infants and children (especially under 5 yrs of age) There are four main radiologic presentations: parenchymal disease, lymphadenopathy, miliary disease, and pleural effusion Primary Tuberculosis Parenchymal disease: dense, homogeneous consolidation of any lobe; predominance in the lower and middle lobes 2/3 of cases: resolve without consequences 1/3 of cases: scar persists, up to 15% scar can calcify; called a Ghon focus Other calcification can be seen as calcified nodules 4
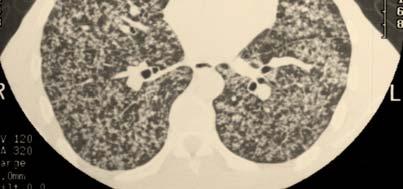
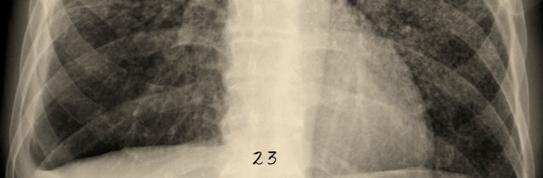
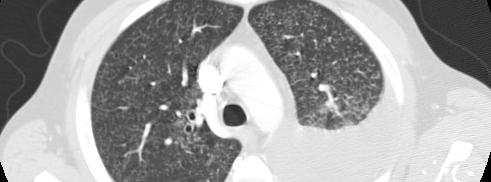
5 Primary Tuberculosis Lymphadenopathy: Seen up to 95% of children and 40% ofadults Typically, unilateral and right sided, involving the hilum and right paratracheal region (1/3 of cases have bilateral involvement) The combination of calcified hilar nodes and a Ghon focus is called a Ranke complex, (not unique to TB, can be seen with histoplasmosis) Primary Tuberculosis Miliary disease: more commonly seen in the elderly, l infants, and immunocompromisedi host. Usually seen within 6 months of the initial exposure Classically is evenly distributed diffuse small 2 3 mm nodules, with a slight lower lobe predominance 5
6 Primary Tuberculosis Pleural Effusion: Seen in ¼ of pts with primary TB. Often is the only manifestation. ti It is seen 3 to 7 months after initial exposure Uncommon in infants Usually unilateral, complications are rare Residual pleural thickening and calcification can occur PPD test can be initially negative Primary Tuberculosis The natural history of TB pleuritis is spontaneous resolution over 2 to 4 mo There is a high risk of reactivation if not treated 6
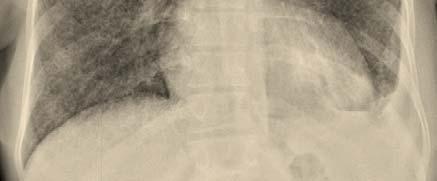
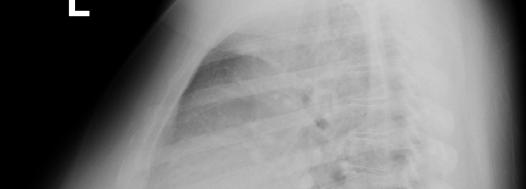
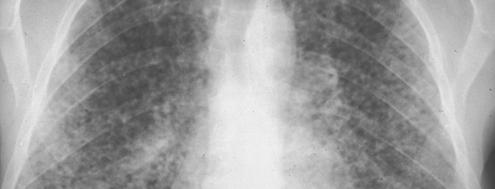
7 Primary Tuberculosis Primary Tuberculosis 7
 Most commonly affects infants and")

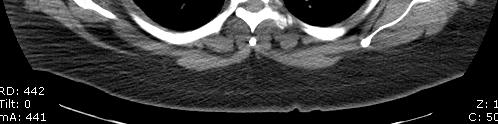
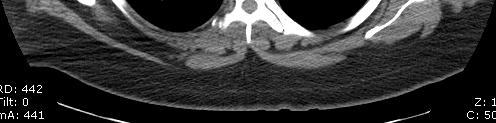
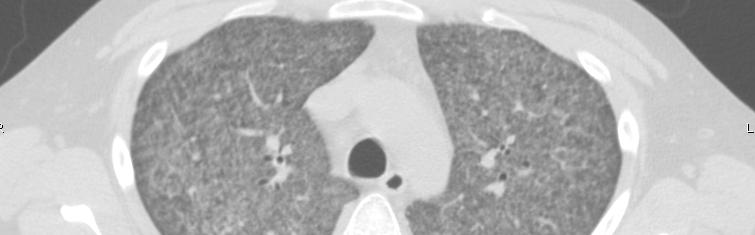
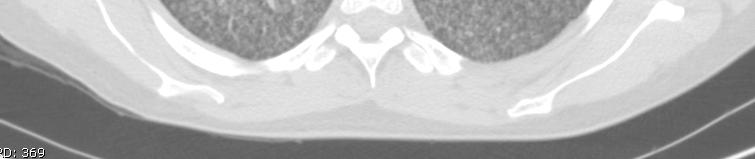
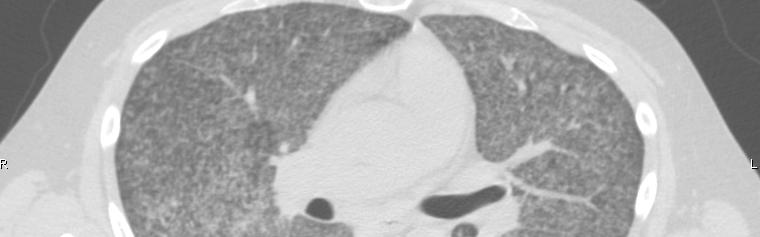
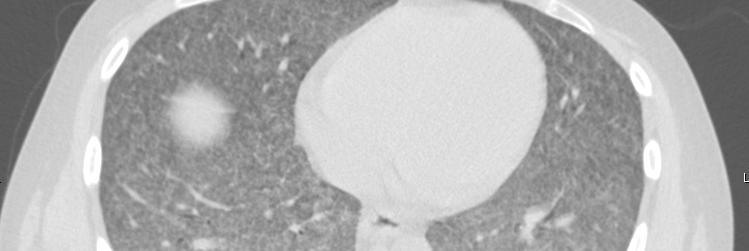
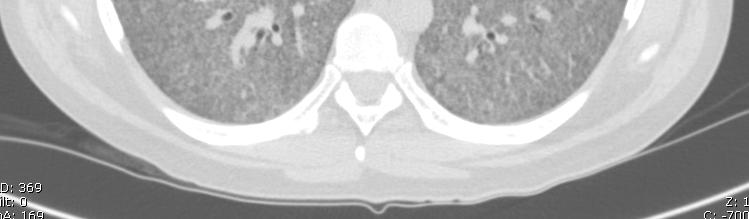
8 Primary Tuberculosis Miliary TB may develop as a result of primary or reactivation TB (post primary) Most commonly affects infants and children (< 5 yr old), the elderly, alcohol abusers, pts with neoplasm, HIV infected pts, and other immunocompromised pts Primary Tuberculosis 8



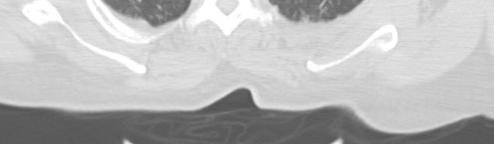
9 Primary Tuberculosis Primary Tuberculosis 9



10 Primary Tuberculosis Primary Tuberculosis 10
11 Primary Tuberculosis Primary Tuberculosis 11
12 Post primary or reactivation tuberculosis Primary TB is usually self limiting Postprimary TB is progressive: cavitation is the hallmark, hematogenous dissemination (miliary), and bronchogenic spread (tree in bud) Fibrosis and calcification are seen after healing Characterized by upper lobes predilection, cavitation and absence of lymphadenopathy Manifestations are: parenchymal disease, airway involvement, and pleural extension Post primary or reactivation tuberculosis Parenchymal disease: Early is patchy, poorly defined consolidation, mainly apical and posterior segments of the upper lobes. More than one segment is involved in the majority of cases; bilateral disease in 1/3 to 2/3 of pts Cavitation is the hallmark and occurs in 50% of cases. Typically have thick, irregular walls, usually multiple cavities within areas of consolidation 12
13 Post primary or reactivation tuberculosis With airway disease, endobronchial spread of infection, tree in bud opacities may develop (suggesting active TB) Lymphadenopathy and pneumothoraces described in 5% of pts Post primary or reactivation tuberculosis Airway involvement: Characterized by bronchial stenosis, leading to lobar collapse or hyperinflation, obstructive pneumonia, and mucoid impaction Bronchial stenosis is seen in 10% 40% of pts with active TB Tree in bud opacities and bronchiectasis can be seen 13
14 Post primary or reactivation tuberculosis Post primary or reactivation tuberculosis Pleural extension: Pleural effusions are more commonin primary TB. Pleural effusion in postprimary TB is usually small and associated with parenchymal disease. Seen up to 18% of cases Effusions are typically septated, can be stable for yrs Pleura may become thickened, tuberculous empyema and risk of bronchopleural fistula. Residual pleural thickening and calcification 14

15 Post primary or reactivation tuberculosis Hemoptysis is common. Hemoptysis due to bleeding from dilated d vessels in bronchiectatic ti areas related to infection or from mycetoma formation in an old cavity Severe hemoptysis can be sec to erosion of an expanding cavity into a pulmonary artery called Rasmussen aneurysm Post primary or reactivation tuberculosis 15


16 Post primary or reactivation tuberculosis Post primary or reactivation tuberculosis 16


17 Post primary or reactivation tuberculosis Post primary or reactivation tuberculosis 17
18 Post primary or reactivation tuberculosis Post primary or reactivation tuberculosis 18




19 Post primary or reactivation tuberculosis Post primary or reactivation tuberculosis 19
20 Post primary or reactivation tuberculosis Post primary or reactivation tuberculosis 20


21 Post primary or reactivation tuberculosis Post primary or reactivation tuberculosis 21
22 Post primary or reactivation tuberculosis Post primary or reactivation tuberculosis 22
23 Post primary or reactivation tuberculosis Tuberculosis and Immunocompromised Host Higher prevalence of extrapulmonary involvement 38% of immunocompromised pts with TB have pulmonary involvement only, but up to 30% have only extrapulmonary involvement May have a normal chest radiograph due to limited immune response 23


24 Tuberculosis and HIV Manifestations depend on the degree of immunodeficiency Higher CD4 count behaves like TB reactivation Lower CD4 count behaves like primary tuberculosis Up to 40% suffer disseminated TB disease The majority of pts show a typical chest radiographic appearance but normal CXR are not unusual Tuberculosis and HIV 24



25 Tuberculosis and HIV Tuberculosis and HIV 25


26 Tuberculosis and HIV Tuberculosis and HIV 26




27 Tuberculosis and HIV Tuberculosis and HIV 27



28 Tuberculosis and HIV Tuberculosis and Immunocompromised Host (ESRD) 28


29 Tuberculosis and EtOH abuse Extrapulmonary Tuberculosis Hematogenous seeding of nonpulmonary organs by the tuberculous bacillus is common About 50% pts with active tuberculosis have extrapulmonary involvement, (in order of frequency): lymph nodes, pleural space, GU tract, bone and joint sites, meninges, and peritoneum GI tract 29
30 Extrapulmonary Tuberculosis The likelihood of extrapulmonary involvement increases in immunocompromisedi pts Laryngeal tuberculosis is an uncommon but highly infectious form of extrapulmonary TB, usually the result of lower airway disease (probably due to hematogenous spread) Extrapulmonary Tuberculosis 30
31 Extrapulmonary Tuberculosis can affect any organ Cardiac: pericarditis, pericardial effusion, myocarditis CNS: meningitis, tuberculomas, tuberculous abscesses, cerebritis, and miliary TB Head and neck: lymphadenitis (scrofula), less common sinonasal, thyroid, skull base Musculoskeletal: spinal column, pelvis, hip, and knee (spondilytis, osteomyelitis, arthritis) Abdominal: lymphadenopathy, p y, peritonitis, ileocecal region, hepatosplenic, adrenal Genitourinary: renal, ureters, bladder, genital (fallopian tubes in women and seminal or prostate gland in men) Extrapulmonary Tuberculosis 31

32 Extrapulmonary Tuberculosis Pott s Disease Extrapulmonary Tuberculosis Pott s Disease 32


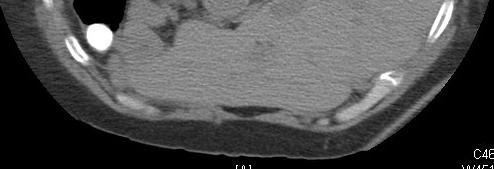
33 Extrapulmonary Tuberculosis Pott s Disease Extrapulmonary Tuberculosis Pott s Disease 33
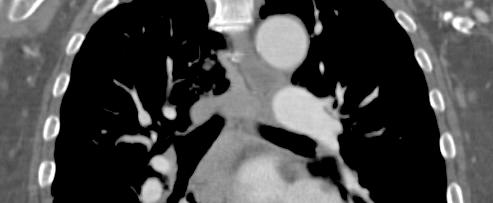
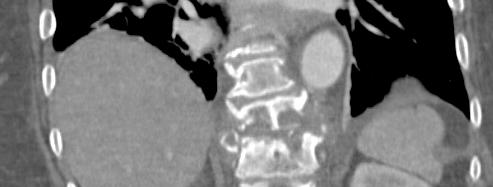
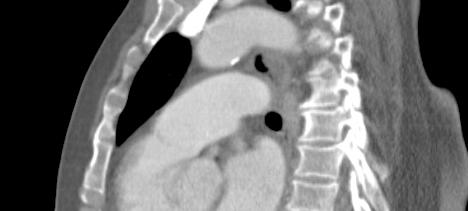

34 Extrapulmonary Tuberculosis Pott s Disease Extrapulmonary Tuberculosis Pott s Disease 34

35 CT scanning for optimal radiology evaluation Do you need a Chest CT to diagnose pulmonary tuberculosis? Probably no, more useful in extrapulmonary, immunocompromised pts with normal CXR, apical disease, and associated lung masses HIV with LAD 35


36 HIV with LAD HIV with LAD 36



37 HIV with LAD EtOH abuse and RUL opacity 37




38 EtOH abuse and RUL opacity EtOH abuse and RUL opacity 38



39 Miliary opacities and EtOH abuse EtOH abuse and miliary opacities 39


40 EtOH abuse and miliary opacities EtOH abuse and miliary opacities 40


41 EtOH abuse and miliary opacities EtOH abuse and miliary opacities 41



42 EtOH abuse and miliary opacities EtOH abuse and miliary opacities 42

43 Miliary tuberculosis Miliary tuberculosis 43


44 Miliary tuberculosis Tuberculosis with bronchogenic spread 44

45 RUL cavity Primary Tuberculosis 45
46 Primary Tuberculosis Biapical Involvement 46
47 Biapical Involvement? masses 47


48 RUL nodule RUL nodular opacities 48


49 Plombage and thoracoplasty Thank you 49
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
David E. Griffith, MD has the following disclosures to make:
 Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Radiographic Manifestations of Pediatric TB Susan D. John, MD, FACR November 13, 2009 Radiologic Presentation of Childhood TB Susan D. John, MD,
Pediatric TB Intensive Houston, Texas November 13, 2009 Radiographic Manifestations of Pediatric TB Susan D. John, MD, FACR November 13, 2009 Radiologic Presentation of Childhood TB Susan D. John, MD,
Tanya Van, M.D. has the following disclosures to make:
 Imaging of Pulmonary Mycobacterial TB Infection Tanya Van, M.D. April6, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Tanya Van, M.D. has the following disclosures to
Imaging of Pulmonary Mycobacterial TB Infection Tanya Van, M.D. April6, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Tanya Van, M.D. has the following disclosures to
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Radiological Features of Mycobacterium tuberculosis TUBERCULE BACILLUS TUBERCULE BACILLUS DIAGNOSIS. Guy Richards. PATHOGENESIS of TUBERCULOSIS
 Radiological Features of Guy Richards Department of critical care Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand, Johannesburg, South Africa TUBERCULE BACILLUS Discovery
Radiological Features of Guy Richards Department of critical care Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand, Johannesburg, South Africa TUBERCULE BACILLUS Discovery
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Original Article. Section: Radiology INTRODUCTION MATERIALS AND METHODS
 DOI: 10.21276/aimdr.2016.2.6.RD4 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 To Compare the Diagnostic Efficacy of HRCT Lung with Chest Radiographic Findings and Clinical Correlation with Microbiological
DOI: 10.21276/aimdr.2016.2.6.RD4 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 To Compare the Diagnostic Efficacy of HRCT Lung with Chest Radiographic Findings and Clinical Correlation with Microbiological
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Extrapulmonary Manifestations of Tuberculosis: A Radiologic Review
 Extrapulmonary Manifestations of Tuberculosis: A Radiologic Review Poster No.: C-1958 Congress: ECR 2014 Type: Authors: Educational Exhibit J. Isern 1, S. Llaverias Borrell 1, A. Olarte 1, E. Grive 1,
Extrapulmonary Manifestations of Tuberculosis: A Radiologic Review Poster No.: C-1958 Congress: ECR 2014 Type: Authors: Educational Exhibit J. Isern 1, S. Llaverias Borrell 1, A. Olarte 1, E. Grive 1,
Role of imaging (images) in my practice. Dr P Senthur Nambi Consultant Infectious Diseases
 in my practice. Dr P Senthur Nambi Consultant Infectious Diseases") Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Tuberculosis in Patients with End-Stage Renal Disease 1
 Tuberculosis in Patients with End-Stage Renal Disease 1 Hyo-Cheol Kim, M.D., Jin Mo Goo, M.D., Myung Jin Chung, M.D., Min Hoan Moon, M.D., Young Hwan Koh, M.D., and Jung-Gi Im, M.D. Purpose: The purpose
Tuberculosis in Patients with End-Stage Renal Disease 1 Hyo-Cheol Kim, M.D., Jin Mo Goo, M.D., Myung Jin Chung, M.D., Min Hoan Moon, M.D., Young Hwan Koh, M.D., and Jung-Gi Im, M.D. Purpose: The purpose
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Extraordinary Patterns of Tuberculosis
 Extraordinary Patterns of Tuberculosis E. Kadakovska Infectology Center of Latvia, Clinic of Tuberculosis and Lung Diseases, Diagnostics and Radiology Department 1 Target Importance of recognizing of tuberculosis
Extraordinary Patterns of Tuberculosis E. Kadakovska Infectology Center of Latvia, Clinic of Tuberculosis and Lung Diseases, Diagnostics and Radiology Department 1 Target Importance of recognizing of tuberculosis
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining
 Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Atypical radiologic appearances of pulmonary tuberculosis in non-hiv adult patients
 Atypical radiologic appearances of pulmonary tuberculosis in non-hiv adult patients Poster No.: R-0200 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: K. N. Jeon, K. Bae, M. J. Park Keywords:
Atypical radiologic appearances of pulmonary tuberculosis in non-hiv adult patients Poster No.: R-0200 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: K. N. Jeon, K. Bae, M. J. Park Keywords:
RADPrimer Curriculum Breast Topics Covered Basic Intermediate 225
 Breast Anatomy & Normal Variants 11 Breast Imaging Modalities 13 BI RADS Lexicon 3 Mammography: Masses 9 Mammography: Calcifications 17 Mammography: Additional Findings 8 Ultrasound Features 10 Ultrasound
Breast Anatomy & Normal Variants 11 Breast Imaging Modalities 13 BI RADS Lexicon 3 Mammography: Masses 9 Mammography: Calcifications 17 Mammography: Additional Findings 8 Ultrasound Features 10 Ultrasound
Tuberculosis of the chest
 European Journal of Radiology 55 (2005) 158 172 Tuberculosis of the chest Luís Curvo-Semedo,Luísa Teixeira, Filipe Caseiro-Alves Department of Radiology, Hospitais da Universidade de Coimbra, Praceta Mota
European Journal of Radiology 55 (2005) 158 172 Tuberculosis of the chest Luís Curvo-Semedo,Luísa Teixeira, Filipe Caseiro-Alves Department of Radiology, Hospitais da Universidade de Coimbra, Praceta Mota
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
Respiratory System الفريق الطبي االكاديمي
 Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code
 Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT
 Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer
 Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer Poster No.: C-2297 Congress: ECR 2012 Type: Educational Exhibit Authors: Y.
Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer Poster No.: C-2297 Congress: ECR 2012 Type: Educational Exhibit Authors: Y.
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Primary tuberculosis in a malnourished adolescent
 Primary tuberculosis in a malnourished adolescent Mazen Zawaideh 1*, Cherng Chao 2, Patricia Poole 2, John Naheedy 3 1. School of Medicine, University of California, San Diego, La Jolla, USA 2. Radiology
Primary tuberculosis in a malnourished adolescent Mazen Zawaideh 1*, Cherng Chao 2, Patricia Poole 2, John Naheedy 3 1. School of Medicine, University of California, San Diego, La Jolla, USA 2. Radiology
Key messages. CXR interpretation in TB/HIV setting. Training course
 Key messages CXR interpretation in TB/HIV setting Training course Normal CXR Front view and lateral view Good notions of technical conditions to obtain a good CXR Good knowledge of criteria for quality
Key messages CXR interpretation in TB/HIV setting Training course Normal CXR Front view and lateral view Good notions of technical conditions to obtain a good CXR Good knowledge of criteria for quality
Primary and reactivation pulmonary tuberculosis: Up-to date imaging an management
 Primary and reactivation pulmonary tuberculosis: Up-to date imaging an management Poster No.: C-0894 Congress: ECR 2016 Type: Educational Exhibit Authors: A. P. Salazar Gomez, C. Montealegre Angarita,
Primary and reactivation pulmonary tuberculosis: Up-to date imaging an management Poster No.: C-0894 Congress: ECR 2016 Type: Educational Exhibit Authors: A. P. Salazar Gomez, C. Montealegre Angarita,
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
Pulmonary Aspergillosis
 May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
INTRATHORACIC TUBERCULOSIS IN CHILDREN
 DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS IN CHILDREN A Guide For Low Income Countries 2003 International Union Against Tuberculosis and Lung Disease DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS
DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS IN CHILDREN A Guide For Low Income Countries 2003 International Union Against Tuberculosis and Lung Disease DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS
1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive abdominal distension 3 months Failure
 Dr Rajasree S Dr Srinivas S, Dr Bagdi RK, Dr Satheesh C Apollo Childrens Hospital, Chennai 1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive
Dr Rajasree S Dr Srinivas S, Dr Bagdi RK, Dr Satheesh C Apollo Childrens Hospital, Chennai 1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive
Radiological spectrum of Thoracic Sequelae and Complications of Tuberculosis
 Radiological spectrum of Thoracic Sequelae and Complications of Tuberculosis Poster No.: P-0013 Congress: ESTI 2014 Type: Educational Poster Authors: B. Alami, O. Addou, M. Jaffal, M. Y. Alaoui Lamrani,
Radiological spectrum of Thoracic Sequelae and Complications of Tuberculosis Poster No.: P-0013 Congress: ESTI 2014 Type: Educational Poster Authors: B. Alami, O. Addou, M. Jaffal, M. Y. Alaoui Lamrani,
TB Classification (ATS/CDC)
") bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Congenital Lung Malformations: Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Introduction to Radiology for TB Nurses
 Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Computed Tomography (CT) Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients
 Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients") Cronicon OPEN ACCESS EC BACTERIOLOGY AND VIROLOGY Research Article Computed Tomography (CT) Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients Ehsan Shahverdi 1 *, Ashkan
Cronicon OPEN ACCESS EC BACTERIOLOGY AND VIROLOGY Research Article Computed Tomography (CT) Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients Ehsan Shahverdi 1 *, Ashkan
100 Chest X Rays for Study Group. by Dr. Suneet Khurana
 100 Chest X Rays for Study Group by Dr. Suneet Khurana Approach to - Chest X Ray (shadow of the viscera on a photographic plate) Gas appears Black Fat appears Dark Grey Water Appears as Light Grey Bone
100 Chest X Rays for Study Group by Dr. Suneet Khurana Approach to - Chest X Ray (shadow of the viscera on a photographic plate) Gas appears Black Fat appears Dark Grey Water Appears as Light Grey Bone
Excavated pulmonary nodule: steps to diagnosis?
 Excavated pulmonary nodule: steps to diagnosis? Poster No.: C-1044 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit W. Mnari, M. MAATOUK, A. Zrig, B. Hmida, M. GOLLI; Monastir/ TN Metastases,
Excavated pulmonary nodule: steps to diagnosis? Poster No.: C-1044 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit W. Mnari, M. MAATOUK, A. Zrig, B. Hmida, M. GOLLI; Monastir/ TN Metastases,
Pediatric TB Intensive Houston, Texas October 14, Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Pulmonary Sarcoidosis - Radiological Evaluation
 Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Community-Acquired Acinetobacter baumannii Pneumonia: Initial Chest Radiographic Findings and Follow-up CT Findings in Helping Predict Patient Outcome
 Community-Acquired Acinetobacter baumannii Pneumonia: Initial Chest Radiographic Findings and Follow-up CT Findings in Helping Predict Patient Outcome Jeong Joo Woo, Dong Hyun Lee, Jin Kyung An Department
Community-Acquired Acinetobacter baumannii Pneumonia: Initial Chest Radiographic Findings and Follow-up CT Findings in Helping Predict Patient Outcome Jeong Joo Woo, Dong Hyun Lee, Jin Kyung An Department
Pulmonary TB aspects
 Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
The use of advanced imaging in the diagnosis of TB. Pierre Goussard, Robert Gie Tygerberg Children`s Hospital and University of Stellenbosch
 The use of advanced imaging in the diagnosis of TB Pierre Goussard, Robert Gie Tygerberg Children`s Hospital and University of Stellenbosch Imaging Bronchoscopy Tracheo-bronchograms Chest CT-scan Ultrasound
The use of advanced imaging in the diagnosis of TB Pierre Goussard, Robert Gie Tygerberg Children`s Hospital and University of Stellenbosch Imaging Bronchoscopy Tracheo-bronchograms Chest CT-scan Ultrasound
UERMMMC Department of Radiology. Basic Chest Radiology
 UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
TUBERCULOSIS. Year: Vol: Page: HOME HELP FEEDBACK SUBSCRIPTIONS ARCHIVE SEARCH SEARCH RESULT
 QUICK SEARCH: [advanced] Go Author: Keyword(s): TUBERCULOSIS Year: Vol: Page: HOME HELP FEEDBACK SUBSCRIPTIONS ARCHIVE SEARCH SEARCH RESULT (Radiographics. 2000;20:449-470.) RSNA, 2000 This Article SCIENTIFIC
QUICK SEARCH: [advanced] Go Author: Keyword(s): TUBERCULOSIS Year: Vol: Page: HOME HELP FEEDBACK SUBSCRIPTIONS ARCHIVE SEARCH SEARCH RESULT (Radiographics. 2000;20:449-470.) RSNA, 2000 This Article SCIENTIFIC
9 month old with stridor, cough, low-grade fever, mild hypoxia
 9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Nurse Case Management Waukesha, Wisconsin March 31 April 2, Pediatric TB Michelle Hulse, MD April 1, 2009
 TB Nurse Case Management Waukesha, Wisconsin March 31 April 2, 2009 Pediatric TB Michelle Hulse, MD April 1, 2009 Pediatric Tuberculosis HNTC Nurse Case Management Course April 1, 2009 Waukesha, Wisconsin
TB Nurse Case Management Waukesha, Wisconsin March 31 April 2, 2009 Pediatric TB Michelle Hulse, MD April 1, 2009 Pediatric Tuberculosis HNTC Nurse Case Management Course April 1, 2009 Waukesha, Wisconsin
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Lecture 3. Inflammatory Processes
 Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
X-Rays. Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady
 X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
Chapter 135 Tuberculosis
 Chapter 135 Tuberculosis Episode overview Core questions: 1. Describe the 4 phases of TB infection 2. For how long is a patient with active TB considered infectious? What isolation measures are necessary
Chapter 135 Tuberculosis Episode overview Core questions: 1. Describe the 4 phases of TB infection 2. For how long is a patient with active TB considered infectious? What isolation measures are necessary
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
Imaging of cardio-pulmonary treatment related damage. Radiotheraphy and Lung
 Imaging of cardio-pulmonary treatment related damage Dr. Andrea Borghesi Dr. Emanuele Gavazzi Department of Radiology 2 University of Brescia Radiotheraphy and Lung The goal of radiation therapy (RT) is
Imaging of cardio-pulmonary treatment related damage Dr. Andrea Borghesi Dr. Emanuele Gavazzi Department of Radiology 2 University of Brescia Radiotheraphy and Lung The goal of radiation therapy (RT) is
General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
 General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
A case of pulmonary tuberculosis presenting as a large pseudo-tumour
 CASE REPORT A case of pulmonary tuberculosis presenting as a large pseudo-tumour Abdulhalim Ibrahim 1, Mozafar Khalid 2, Mohammed KM Ali 3 1. Manchester Royal infirmary, Manchester, UK. 2. North Tees University
CASE REPORT A case of pulmonary tuberculosis presenting as a large pseudo-tumour Abdulhalim Ibrahim 1, Mozafar Khalid 2, Mohammed KM Ali 3 1. Manchester Royal infirmary, Manchester, UK. 2. North Tees University
Diagnosis of Tuberculosis Infection and Disease
 Diagnosis of Tuberculosis Infection and Disease David E. Griffith, M.D. Assistant Medical Director Heartland National TB Center The Medical Evaluation for Diagnosing Tuberculosis Traditional Approach Patient
Diagnosis of Tuberculosis Infection and Disease David E. Griffith, M.D. Assistant Medical Director Heartland National TB Center The Medical Evaluation for Diagnosing Tuberculosis Traditional Approach Patient
An Image Repository for Chest CT
 An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Web Chapter 3. Image Gallery: Lesion detection on low dose chest CT
 Web Chapter 3 Image Gallery: Lesion detection on low dose chest CT Sarabjeet Singh, MD Mannudeep K. Kalra, MD *Eugene J. Mark, MD *James Stone, MD James H. Thrall, MD Department of Radiology and *Department
Web Chapter 3 Image Gallery: Lesion detection on low dose chest CT Sarabjeet Singh, MD Mannudeep K. Kalra, MD *Eugene J. Mark, MD *James Stone, MD James H. Thrall, MD Department of Radiology and *Department
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
COMPUTED TOMOGRAPHY DEMONSTRATION OF THE COMPLICATIONS AND ASSOCIATIONS OF LYMPHOBRONCHIAL TUBERCULOSIS IN CHILDREN
 COMPUTED TOMOGRAPHY DEMONSTRATION OF THE COMPLICATIONS AND ASSOCIATIONS OF LYMPHOBRONCHIAL TUBERCULOSIS IN CHILDREN Dr Susan Lucas A research report submitted to the Faculty of Health Sciences, University
COMPUTED TOMOGRAPHY DEMONSTRATION OF THE COMPLICATIONS AND ASSOCIATIONS OF LYMPHOBRONCHIAL TUBERCULOSIS IN CHILDREN Dr Susan Lucas A research report submitted to the Faculty of Health Sciences, University
Pediatric Drug-Resistant TB in China
 Pediatric Drug-Resistant TB in China Shuihua Lu,Tao Li Shanghai Public Health Clinical Center Jan.18,2013 A MDR-TB CASE A four and a half years old boy, spent 4 yeas of his life in hospital. His childhood
Pediatric Drug-Resistant TB in China Shuihua Lu,Tao Li Shanghai Public Health Clinical Center Jan.18,2013 A MDR-TB CASE A four and a half years old boy, spent 4 yeas of his life in hospital. His childhood
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant