Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches
|
|
|
- Warren York
- 5 years ago
- Views:
Transcription
1 Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor of Clinical Medicine, UCSF April 30, 2015
2 Faculty and Planning Committee Disclosures Please consult your program book. Off-Label Disclosure The following off-label/investigational uses will be discussed in this presentation: none
3 Learning Objectives Upon completion of this presentation, learners should be better able to: Describe the efficacy of class sparing strategies in treatment naïve and experienced patients Discuss the risks and benefits of switching ARV therapy in patients receiving suppressive ARV therapy Devise and modify ARV regimens in treatmentexperienced patients
4 Outline Class sparing approaches Recent switch studies How to assess potential risks and benefits of switching ARV regimens in treatment-experienced patients
5 Case 1 53 yo man with HIV (CD4 nadir 250 in 1996, current CD4 700, VL < 40 copies/ml) requests treatment simplification Comorbidities: osteopenia with metatarsal stress fractures, on Ca, Vit D, alendronate recently started after fractures healed Hyperlipidemia, on atorvastatin and fenofibrate Obesity, on disability for stress fractures in metatarsal bones Current regimen: maraviroc, atazanavir/r, TDF/FTC, nevirapine
6 ARV History : D4T, 3TC, indinavir. Had virologic failure but no GT available : DDI, nevirapine, lopinavir/ritonavir : Treatment Interruption 2008: R5 virus, enrolled in MVC study, started on maraviroc 150 mg BID, r/atz 400 mg QD, NVP 400 mg QD, TDF/FTC one QD Since 2008: Excellent adherence and virologic suppression since 2008; chronic diarrhea for which he takes imodium
7 What would you start him on? A. maraviroc, rilpivirine, dolutegravir B. maraviroc, etravirine, raltegravir C. check HLA B5701, if negative, start on abacavir/lamivudine, rilpvirine, dolutegravir D. Something else
8 What would you start him on? A. maraviroc, rilpivirine, dolutegravir B. maraviroc, etravirine, raltegravir C. check HLA B5701, if negative, start on abacavir/lamivudine, rilpvirine, dolutegravir D. Something else Outcome: pt starts on regimen A, has maintained suppression after 6 mos, and loves his new regimen. Fenofibrate has been discontinued with good control of lipids
9 DHHS Guidelines 2015: What to Start Recommended regimens Alternative regimens* NNRTI EFV/TDF/FTC RPV/TDF/FTC Boosted PI DRV/RTV + TDF/FTC ATV + RTV or COBI + TDF/FTC DRV + RTV or COBI + ABC/3TC DRV/COBI + TDF/FTC INSTI DTG + ABC/3TC DTG + TDF/FTC EVG/COBI/TDF/FTC RAL + TDF/FTC DHHS Guidelines, April 8, 2015 *DRV/r + RAL AND LPV/r + 3TC for pts who cannot take TDF or ABC For pts with VL < 100K: ATV/r or EFV + ABC/3TC; RPV/TDF/FTC For pts who are HLA-B*5701 positive, avoid abacavir
10 Current options for NRTI sparing regimens: IAS-USA guidelines 2014 Regimen Raltegravir plus darunavir/r Lopinavir/r plus lamivudine Lopinavir/r plus raltegravir Caveats Raltegravir given BID, DRV/r QD; Inferior results with CD4 < 200 and HIV PCR > 100,000 Single study LPV/r not standard first line PI/r in US BID dosing for both PI/r and RAL LPV/r not standard first line PI/r in US Gunthard HF et al, JAMA 2014; 312:410-25
11 NRTI-sparing in treatment-naïve 3TC + LPV/r (GARDEL): encouraging results Studies with DRV/r + RAL (NEAT-1): equivocal results MVC + DRV/r (MODERN): poor results, leading to early trial discontinuation
12 GARDEL: Study Design Randomized, international, open label phase III study Included ARV naïve adults (HIV-1 RNA > 1000 copies/ml; no IAS defined NRTI or PI resistance) Randomized to LPV/r 400 mg/100 mg BID + 3TC (n=217) vs LPV/r 400 mg/100 mg BID + investigatorselected 2NRTI fixed dose combination (n=209) Primary endpoint: HIV RNA < 50 copies/ml (ITT) at week 48 Approximately 80% from Latin America Cahn P et al, Lancet Infect Dis 2014; 14:578-80
13 GARDEL: Results For primary endpoint, 2D combo non-inferior to 3D combo at wk 48 (VL < 50 2D 88% vs 3D 83%) Similar results for pts with baseline VL > 100K 10 discontinuations in 3D vs 1 in 2D arm Drugs used reflect availability in developing world?what would results be with DRV/r or DOL with either 3TC or FTC? Cahn P et al, Lancet Infect Dis 2014; 14:578-80
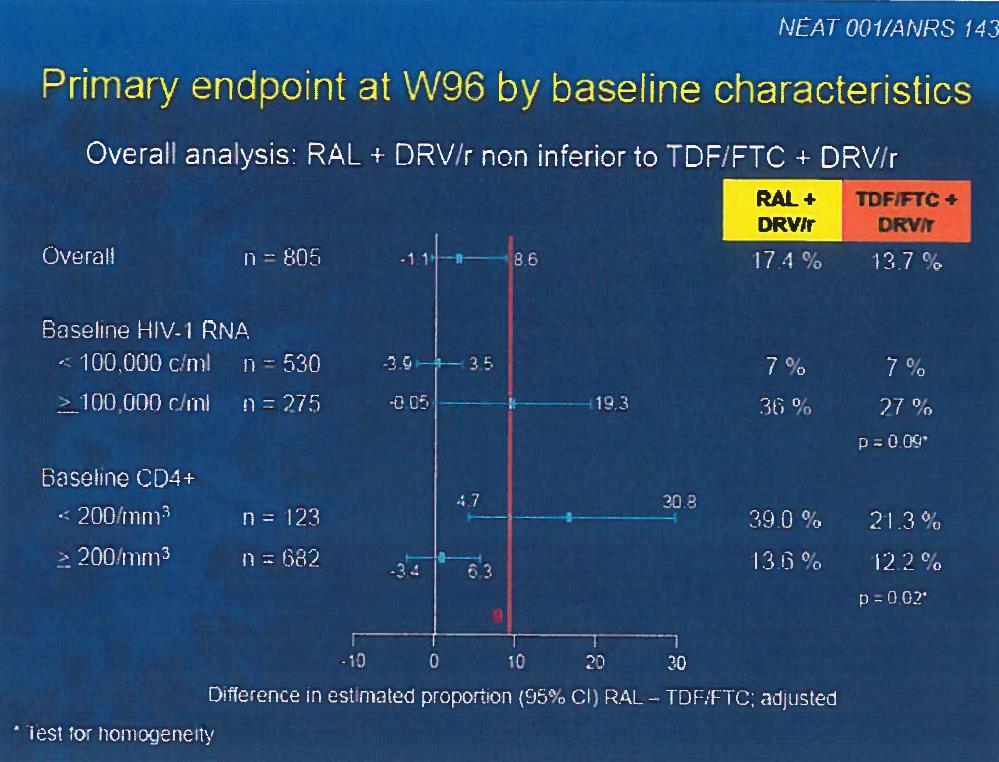
14 NEAT 001/ANRS 143: DRV/r + RAL vs. DRV/r + TDF/FTC in ARV Naïve Pts Randomized, open label phase 3 study 805 ARV-naïve patients randomized in 15 European countries Primary (composite) endpoint: Virologic: change of rx prior to week 32 because of inadequate response OR VL > 50 copies/ml after week 32 Clinical: Death, new AIDS-defining events, new non-aids defining events Raffi F, et al. CROI Abstract 84LB

15 RAL + DRV/RTV Noninferior to TDF/FTC + DRV/RTV at 96 Wks Similar numbers of pts with PDVF (RAL: n = 66; TDF/FTC: n = 52) No pts with resistance in TDF/FTC arm vs 5 with integrase mutations and 1 with K65R Raffi F, et al. 21st CROI Abstract 84LB.
16
17 Switching ART in suppressed patients: potential benefits Convenience Stigma Pill burden Lack of food restrictions Tolerability Lipid sparing, cardiovascular risk Psychiatric comorbidities/suicidality Renal and bone disease Drug-drug interactions Cost DHHS Guidelines, May 1, 2014
18 Switching ART in suppressed patients: potential risks New toxicities Some newer agents may be less potent Continuing partially active or inactive agents may lead to functional monotherapy Food requirements Drug interactions DHHS Guidelines, May 1, 2014
19 Case 2 37 yo male, intermittent meth use, depression, CD4 nadir 50, EGFR 80, no other comorbidities ARV history : AZT, 3TC, NVP 2003 present: TDF, FTC, ATZ/r Current CD4 300, has VL blips from time to time in copies/ml range, never high enough to genotype He insists on switching to STR, insists he will be 100% adherent You prescribe EVG/COBI/FTC/TDF After 6 mos, CD4 is 200, HIV PCR is 2500

20 HIV Genotype* *No PI mutations
21 Encouraging adherence, what regimen do you suggest?? A. TDF/FTC, ATZ/r B. TDF/FTC, DRV/r C. Continue EVG/COBI/TDF/FTC D. TDF/FTC, DRV/r, dolutegravir 50 mg qd E. TDF/FTC, DRV/r, dolutegravir 50 mg BID
22 Encouraging adherence, what regimen do you suggest?? A. TDF/FTC, ATZ/r B. TDF/FTC, DRV/r C. Continue EVG/COBI/TDF/FTC D. TDF/FTC, DRV/r, dolutegravir 50 mg qd E. TDF/FTC, DRV/r, dolutegravir 50 mg BID Outcome: you switch him back to choice A, and he continues to blip in copies/ml range
23 Recent switch studies: what have we learned? From PI/r based ART to RAL SWITCHMRK and Spiral Studies From PI/r based ART to TDF/FTC/RPV Spirit Study From TDF/FTC/EVG/COBI to: STRATEGY NNRTI STRATEGY PI
24 SWITCHMRK vs. Spiral: Conflicting Results switch studies to RAL from r/pi based ART in suppressed pts SWITCHMRK (double blind) Suppressed pts on 2n + LPV/r randomized switch to 2n/RAL vs continue 2n/LPV/r After 24 weeks switch NOT noninferior Duration of previous suppression on LPV/r 2n: 6 months Most failures in patients on multiple prior regimens SPIRAL (open label) Suppressed pts on 2n/PI/r randomized switch to 2n/RAL vs. continue 2n/PI/r After 48 weeks noninferior Duration of previous suppression on PI/r + 2n: 6 years Eron J et al, Lancet 2010; 375:396; Martinez E et al, AIDS 2010; 24:1697
25 STRATEGY Trials: switch to EVG/COBI/TDF/FTC in Suppressed Pts STRATEGY NNRTI: randomize 2:1 switch to EVG/COBI/TDF/FTC qd vs continue TDF/FTC NNRTI in suppressed patients STRATEGY PI: randomize 2:1 switch to EVG/COBI/TDF/FTC vs. continue TDF/FTC/PI/r in suppressed pts Approximately 330 pts randomized in each study Primary endpoint: HIV RNA < 50 copies/ml at wk 48 Pozniak A et al. Lancet Infect Dis 2014; 14: ; Arribas JR et al, Lancet Infect Dis 2014; 14:581-89
26 STRATEGY-NNRTI: Change to EVG/COBI Noninferior to Stable NNRTIs at Wk 48 Results for primary endpoint: 93% achieved HIV VL < 50 copies/ml in switch group vs 88% in no switch group Regimens: EFV, 78%; NVP, 17%; RPV, 4%; ETR, < 1%; 74% on EFV/TDF/FTC; 91% on first regimen Results similar across all baseline virologic and demographic subgroups 3 pts with VF in switch arm vs 1 in no switch arm 5 in switch arm vs 1 in the NNRTI arm discontinued due to AE Similar results in STRATEGY-PI study Pozniak A et al. Lancet Infect Dis 2014; 14:
27 Canadian National Cohort: Switching After Suppression Associated With Risk of VF Retrospective analysis of factors associated with VF among suppressed pts who switched (N = 2807) Initiated first-line ART with 3 agents between 1/1/2005 and 6/30/2012 In multivariate model Switching ART associated with increased risk of VF (P <.001) Females and pts with IDU history at increased risk of VF with switch (P <.001) Would be interesting to speculate who was advocating the switch: patient or provider? Hull M, et al. 20th IAC Abstract TUAB0103..
28 Efavirenz as initial therapy and increased risk for suicidal ideation Review of 4 ACTG studies in ARV naïve patients Compared 3241 pts starting EFV vs 2091 pts starting non EFV-based ART Average duration f/u 96 mos First suicidal ideation OR attempted OR completed suicide in each group: 8.08 events per 1000 PY in EFV group (47 events) 3.66 events per 1000 PY in EFV-free group (5 events) Mollan KR et al, Ann Intern Med 2014; 161:1 10
29 Rather than d/c TDF/FTC/EFV, what about reducing EFV dose to minimize toxicity?
30 ENCORE1: EFV 400 vs 600 mg QD + TDF/FTC in Treatment-Naive Pts Randomized, double-blind, noninferiority study performed in Europe, Asia, Central America Primary endpoint: HIV-1 RNA < 200 c/ml at Wk 96 ART naive pts randomized to EFV 400 mg/d plus TDF/FTC (n = 321) vs EFV 600 mg/d plus TDF/FTC (n = 309) Primary endpoint: HIV RNA<200 copies/ml at week 48 % suppressed at wk 48: 94% EFV 400 mg vs 92% EFV 600 mg Puls R et al, Lancet 2014; 383:
31 ENCORE1: EFV 400 vs 600 mg QD + TDF/FTC in Treatment-Naïve Patients Mean change in CD4+ cell count from BL greater with 400-mg vs 600-mg EFV (P =.03) Rate of EFV-related AEs lower with 400-mg vs 600-mg dose: 37.7% vs 47.9% (P =.01) Trend toward lower rate of discontinuation for EFVrelated AEs with 400-mg vs 600-mg dose: 8.3% vs 15.5% (P =.07) Frequency of treatment emergent NNRTI resistance similar in both arms Puls R et al, Lancet 2014; 383:
32 Conclusions Most NRTI sparing regimens in treatment-naïve patients have suboptimal outcomes Selected patients with HIV can have treatment simplification with excellent outcomes Multiple prior ARV regimens and poor patient adherence may affect efficacy of switch regimens
33 Thank you for your attention!!
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD
 More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
Antiretroviral Therapy: What to Start
 FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
Are the current doses of ARV correct. Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine
 Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Disclosures. Update on HIV Drug Therapy: A Case based Discussion. Case # 1: Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv
 Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Treating HIV: When the Guidelines Don t Fit. Joel Gallant, MD, MPH. Southwest CARE Center Santa Fe, New Mexico
 Treating HIV: When the Guidelines Don t Fit Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, New Mexico Johns Hopkins University School of Medicine University of New Mexico School of Medicine Disclosures
Treating HIV: When the Guidelines Don t Fit Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, New Mexico Johns Hopkins University School of Medicine University of New Mexico School of Medicine Disclosures
Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary?
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
HIV Treatment Update. Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London
 HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
Didactic Series. CROI 2014 Update. March 27, 2014
 Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi
 6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
Simplifying Antiretroviral Therapy Regimens: It s not so simple
 Simplifying Antiretroviral Therapy Regimens: It s not so simple Jonathan Colasanti, MD, MSPH Division of Infectious Diseases Emory University School of Medicine Disclosures No Financial Disclosures Parts
Simplifying Antiretroviral Therapy Regimens: It s not so simple Jonathan Colasanti, MD, MSPH Division of Infectious Diseases Emory University School of Medicine Disclosures No Financial Disclosures Parts
Reduced Drug Regimens
 Dr. Jose R Arribas @jrarribas Financial disclosures JOSE R ARRIBAS Research Support: Speaker s Bureau: Viiv, Janssen, Abbvie, BMS, Gilead, MSD Board Member/Advisory Panel: Merck, Gilead Stock/Shareholder:
Dr. Jose R Arribas @jrarribas Financial disclosures JOSE R ARRIBAS Research Support: Speaker s Bureau: Viiv, Janssen, Abbvie, BMS, Gilead, MSD Board Member/Advisory Panel: Merck, Gilead Stock/Shareholder:
The next generation of ART regimens
 The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
Switching antiretroviral therapy to safer strategies based on integrase inhibitors
 Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
2-Drug regimens in HIV Anton Pozniak MD FRCP
 2-Drug regimens in HIV Anton Pozniak MD FRCP Advantages Cost Dual Therapy Toxicities of Nukes CV risk, bone, renal disease Smaller STRs Keep drugs for later etc. Dual Therapy-Talking Points - What are
2-Drug regimens in HIV Anton Pozniak MD FRCP Advantages Cost Dual Therapy Toxicities of Nukes CV risk, bone, renal disease Smaller STRs Keep drugs for later etc. Dual Therapy-Talking Points - What are
Case # 1. Case #1 (cont d)
") Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
HIV Update Allegra CPD Day Program Port Elizabeth Dr L E Nojoko
 HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
Switching antiretroviral therapy to safer strategies based on integrase inhibitors. Pedro Cahn
 Switching antiretroviral therapy to safer strategies based on integrase inhibitors Pedro Cahn Disclosures Research Grants: Abbvie-Merck-Richmond-ViiV Advisory boards: Merck-Sandoz-ViiV Switching in Virologically
Switching antiretroviral therapy to safer strategies based on integrase inhibitors Pedro Cahn Disclosures Research Grants: Abbvie-Merck-Richmond-ViiV Advisory boards: Merck-Sandoz-ViiV Switching in Virologically
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
The Use of Integrase Inhibitors In Latin America: From Guidelines to the Real World Ernesto Martínez B., MD Internal Medicine, Infectious Diseases
 De afbeelding kan niet worden weergegeven. The Use of Integrase Inhibitors In Latin America: From Guidelines to the Real World Ernesto Martínez B., MD Internal Medicine, Infectious Diseases DISCLOSURE
De afbeelding kan niet worden weergegeven. The Use of Integrase Inhibitors In Latin America: From Guidelines to the Real World Ernesto Martínez B., MD Internal Medicine, Infectious Diseases DISCLOSURE
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
HIV Treatment Update 8/3/2015. When to Start. Disclosures
 8/3/215 HIV Treatment Update Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
8/3/215 HIV Treatment Update Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
Antiretroviral Treatment 2014
 Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
11/7/2016. Antiretroviral Therapy Strategies. Learning Objectives. After attending this presentation, participants will be able to:
 Antiretroviral Therapy Strategies FORMATTED: 1/14/16 Joel E. Gallant, MD, MPH Medical Director of Specialty Services Southwest CARE Center Santa Fe, New Mexico Adjunct Professor of Medicine The Johns Hopkins
Antiretroviral Therapy Strategies FORMATTED: 1/14/16 Joel E. Gallant, MD, MPH Medical Director of Specialty Services Southwest CARE Center Santa Fe, New Mexico Adjunct Professor of Medicine The Johns Hopkins
Bon Usage des Antirétroviraux dans l Infection par le VIH
 Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
Antiretroviral Therapy: Panel Discussion
 disclosures Antiretroviral Therapy: Panel Discussion Medical Management of HIV December 9, 217 Panelists: Harry Lampiris, MD; Annie Luetkemeyer, MD; Carina Marquez, MD Moderator: Oliver Bacon, MD none
disclosures Antiretroviral Therapy: Panel Discussion Medical Management of HIV December 9, 217 Panelists: Harry Lampiris, MD; Annie Luetkemeyer, MD; Carina Marquez, MD Moderator: Oliver Bacon, MD none
HIV Treatment: State of the Art 2013
 HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
Qué anuncian los nuevos trials?
 Qué anuncian los nuevos trials? XVII Curso Nacional VIH/SIDA Sociedad Chilena de Infectología Agosto 2014 Dr. Carlos Beltrán Hospital Barros Luco Trudeau Universidad de Santiago Grupo SidaChile El presente
Qué anuncian los nuevos trials? XVII Curso Nacional VIH/SIDA Sociedad Chilena de Infectología Agosto 2014 Dr. Carlos Beltrán Hospital Barros Luco Trudeau Universidad de Santiago Grupo SidaChile El presente
HIV - Therapy Principles
 HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
Cases from the Clinic(ians): Case-Based Panel Discussion
: Case-Based Panel Discussion") Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Case 1 continued. Case 1 (cont) 12/8/16. MMAH Debate Panel Thursday, December 8, Case 1
 12/8/16. MMAH Debate Panel Thursday, December 8, Case 1") MMAH Debate Panel Thursday, December 8, 2016 Case 1 HPI 55 yo man with newly diagnosed HIV initiates care in your clinic. His CD4+ cell count is 600, with HIV VL=90,000 copies/ml. He is asymptomatic at
MMAH Debate Panel Thursday, December 8, 2016 Case 1 HPI 55 yo man with newly diagnosed HIV initiates care in your clinic. His CD4+ cell count is 600, with HIV VL=90,000 copies/ml. He is asymptomatic at
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Third Agent Advantages Disadvantages. Component Tenofovir/emtricitabine (TDF/FTC) 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily
 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily") Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Clinical support for reduced drug regimens. David A Cooper The University of New South Wales Sydney, Australia
 Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
Antiretroviral Therapy in 2016
 Antiretroviral Therapy in 2016 Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
Antiretroviral Therapy in 2016 Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
L infettivologia del 3 millennio: AIDS ed altro
 L infettivologia del 3 millennio: AIDS ed altro VI Convegno Nazionale 15-16 -17 maggio 2014 Centro Congressi Hotel Ariston Paestum (SA) Nuove molecole ad azione anti-hiv Annalisa Saracino Clinica Malattie
L infettivologia del 3 millennio: AIDS ed altro VI Convegno Nazionale 15-16 -17 maggio 2014 Centro Congressi Hotel Ariston Paestum (SA) Nuove molecole ad azione anti-hiv Annalisa Saracino Clinica Malattie
Drug toxicities: Safest PIs. Michelle Moorhouse 14 Apr 2016
 Drug toxicities: Safest PIs Michelle Moorhouse 14 Apr 2016 Impact of PIs on AIDS mortality CDC.gov. Epidemiology of HIV infection. Evolution of PIs http://www.clinicaloptions.com/hiv/treatment%20updates/boosted%20pis/interactive%20virtual%20presentation/slideset.aspx
Drug toxicities: Safest PIs Michelle Moorhouse 14 Apr 2016 Impact of PIs on AIDS mortality CDC.gov. Epidemiology of HIV infection. Evolution of PIs http://www.clinicaloptions.com/hiv/treatment%20updates/boosted%20pis/interactive%20virtual%20presentation/slideset.aspx
Optimizing Clinical Utility of Integrase Inhibitors. Anton Pozniak MD FRCP
 Optimizing Clinical Utility of Integrase Inhibitors Anton Pozniak MD FRCP INSTIs-Characteristics Rapid viral load decline Low rates resistance/ Transmitted Resistance Less chance of side effects Less pills,
Optimizing Clinical Utility of Integrase Inhibitors Anton Pozniak MD FRCP INSTIs-Characteristics Rapid viral load decline Low rates resistance/ Transmitted Resistance Less chance of side effects Less pills,
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
ART: The New, The Old and The Ugly
 ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
12th European AIDS Conference / EACS ARV Therapies and Therapeutic Strategies A CME Newsletter
 EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
Professor José Arribas
 19 th Annual Conference of the British HIV Association (BHIVA) Professor José Arribas Hospital La Paz, Madrid, Spain 16-19 April 2013, Manchester Central Convention Complex Can we live without nucleosides?
19 th Annual Conference of the British HIV Association (BHIVA) Professor José Arribas Hospital La Paz, Madrid, Spain 16-19 April 2013, Manchester Central Convention Complex Can we live without nucleosides?
BHIVA antiretroviral treatment guidelines 2015
 BHIVA antiretroviral treatment guidelines 2015 Duncan Churchill Brighton & Sussex University Hospitals NHS Trust Laura Waters Mortimer Market Centre, CNWL Duncan Churchill GENERAL POINTS & WHEN TO START
BHIVA antiretroviral treatment guidelines 2015 Duncan Churchill Brighton & Sussex University Hospitals NHS Trust Laura Waters Mortimer Market Centre, CNWL Duncan Churchill GENERAL POINTS & WHEN TO START
Starting and Switching ART: 2016
 Starting and Switching ART: 2016 Luke Jerram Rajesh T. Gandhi, M.D. Massachusetts General Hospital Harvard Medical School Disclosures: grant support from EBSCO, Gilead, Merck, Viiv Thanks to Henry Sunpath,
Starting and Switching ART: 2016 Luke Jerram Rajesh T. Gandhi, M.D. Massachusetts General Hospital Harvard Medical School Disclosures: grant support from EBSCO, Gilead, Merck, Viiv Thanks to Henry Sunpath,
SELECTING THE BEST ART FOR EACH PATIENT
 SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
Disclosures. Goals/Format. Patient 1 12/8/18. Antiretroviral Therapy Management. Harry Lampiris: None. Gabriel Chamie: None.
 Disclosures Antiretroviral Therapy Management Panel Discussion & Debate Medical Management of AIDS & Hepatitis December 6, 2018 Harry Lampiris, MD, 1 Gabriel Chamie, MD, MPH 2 Susa Coffey, MD, 2 and Vivek
Disclosures Antiretroviral Therapy Management Panel Discussion & Debate Medical Management of AIDS & Hepatitis December 6, 2018 Harry Lampiris, MD, 1 Gabriel Chamie, MD, MPH 2 Susa Coffey, MD, 2 and Vivek
Update on HIV Drug Resistance. Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School
 Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies. Joel Gallant, MD, MPH Johns Hopkins University School of Medicine
 Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies Joel Gallant, MD, MPH Johns Hopkins University School of Medicine Initial Regimen: DHHS Guidelines 3/27/2012 Preferred Regimens
Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies Joel Gallant, MD, MPH Johns Hopkins University School of Medicine Initial Regimen: DHHS Guidelines 3/27/2012 Preferred Regimens
Second-Line Therapy NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
How to best manage HIV patient?
 How to best manage HIV patient? 1 2 Treatment Treatment Failure success HIV therapy = a long life therapy Why do we want to change a suppressive ART? Side effect Comorbidities Reduce drug burden How to
How to best manage HIV patient? 1 2 Treatment Treatment Failure success HIV therapy = a long life therapy Why do we want to change a suppressive ART? Side effect Comorbidities Reduce drug burden How to
2/16/2017. Management and Prevention of HIV Infection: Case Discussion. Case 1. Case 1
 Management and Prevention of HIV Infection: Case Discussion Eric S. Daar, M.D. Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Grant
Management and Prevention of HIV Infection: Case Discussion Eric S. Daar, M.D. Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Grant
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
What is the magic number? Clinical perspective
 What is the magic number? Clinical perspective Andrea De Luca Dipartimento Biotecnologie Mediche Università di Siena UOC Malattie Infettive AOU Senese Outline Regimens with reduced number of drugs Use
What is the magic number? Clinical perspective Andrea De Luca Dipartimento Biotecnologie Mediche Università di Siena UOC Malattie Infettive AOU Senese Outline Regimens with reduced number of drugs Use
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
 Initial Therapy for Antiretroviral Naïve HIV Infected Patients Michelle Cespedes, MD, MS Associate Professor of Medicine Division of Infectious Disease Icahn School of Medicine at Mount Sinai Disclosures
Initial Therapy for Antiretroviral Naïve HIV Infected Patients Michelle Cespedes, MD, MS Associate Professor of Medicine Division of Infectious Disease Icahn School of Medicine at Mount Sinai Disclosures
INTERGRASE INHIBITORS- WHAT S NEW?
 INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
State of the ART: Integrase Inhibitors Clinical Data. Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain
 Madrid, Spain") State of the ART: Integrase Inhibitors Clinical Data Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain Disclosures Consulting fees and honoraria Gilead, Janssen, MSD,
State of the ART: Integrase Inhibitors Clinical Data Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain Disclosures Consulting fees and honoraria Gilead, Janssen, MSD,
Single Pill Combinations Versus Generics: Prescribing Practices in a New Healthcare Era
 Activity Code FM285 Single Pill Combinations Versus Generics: Prescribing Practices in a New Healthcare Era Monica Gandhi MD, MPH Clinic Director, Ward 86 HIV Clinic, SFGH/UCSF Learning Objectives Upon
Activity Code FM285 Single Pill Combinations Versus Generics: Prescribing Practices in a New Healthcare Era Monica Gandhi MD, MPH Clinic Director, Ward 86 HIV Clinic, SFGH/UCSF Learning Objectives Upon
Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use
 Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use Calvin Cohen MD Harvard Vanguard Medical Associates CRI New England Vice Chair, Science Steering Cmte, INSIGHT Boston MA Learning
Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use Calvin Cohen MD Harvard Vanguard Medical Associates CRI New England Vice Chair, Science Steering Cmte, INSIGHT Boston MA Learning
Simplified regimens: Pros and Cons
 Rio de Janeiro, 2018 Simplified regimens: Pros and Cons Pedro Cahn Treatment Strategies: A long way Monotherapy Dual therapy STIs Triple therapy Non daily regimens Simplification Mega HAART Long Acting/Extended
Rio de Janeiro, 2018 Simplified regimens: Pros and Cons Pedro Cahn Treatment Strategies: A long way Monotherapy Dual therapy STIs Triple therapy Non daily regimens Simplification Mega HAART Long Acting/Extended
Pediatric HIV Update NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
Two Drug Regimens Pros and Cons. Jürgen Rockstroh Department of Medicine I University Hospital Bonn, Bonn, Germany
 Two Drug Regimens Pros and Cons Jürgen Rockstroh Department of Medicine I University Hospital Bonn, Bonn, Germany HIV Clinical Forum, Moscow, Russia, Friday 23 rd November 2018 Conflict of Interest: JKR
Two Drug Regimens Pros and Cons Jürgen Rockstroh Department of Medicine I University Hospital Bonn, Bonn, Germany HIV Clinical Forum, Moscow, Russia, Friday 23 rd November 2018 Conflict of Interest: JKR
Antiretroviral Drugs
 Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
Dr Carole Wallis, PhD Medical Director, BARC-SA Head of the Specialty Molecular Division, Lancet Laboratories, South Africa
 Dr Carole Wallis, PhD Medical Director, BARC-SA Head of the Specialty Molecular Division, Lancet Laboratories, South Africa Transmitted drug resistance Resistance patterns in first-line failures in adults
Dr Carole Wallis, PhD Medical Director, BARC-SA Head of the Specialty Molecular Division, Lancet Laboratories, South Africa Transmitted drug resistance Resistance patterns in first-line failures in adults
TDF containing ART: Efficacy and Safety. Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia
 TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
Management of ART Failure. EACS Advanced HIV Course 2015 Dr Nicky Mackie
 Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
STRIBILD (aka. The Quad Pill)
") NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
REASONS FOR DISCONTINUATION OF DUAL THERAPY WITH DOLUTEGRAVIR AND RILPIVIRINE
 REASONS FOR DISCONTINUATION OF DUAL THERAPY WITH DOLUTEGRAVIR AND RILPIVIRINE R. Montejano, N. Stella-Ascariz, S. Garcia-Bujalance, JI. Bernardino, V. Hontañon, R. Mican, Montes M, E. Valencia, J. González,
REASONS FOR DISCONTINUATION OF DUAL THERAPY WITH DOLUTEGRAVIR AND RILPIVIRINE R. Montejano, N. Stella-Ascariz, S. Garcia-Bujalance, JI. Bernardino, V. Hontañon, R. Mican, Montes M, E. Valencia, J. González,
New HIV EACS and Italian Guidelines
 Original Article HIV correlated pathologies and other infections Marco Borderi New HIV EACS and Italian Guidelines Infectious Disease Unit - S. Orsola-Hospital - University of Bologna Corresponding author:
Original Article HIV correlated pathologies and other infections Marco Borderi New HIV EACS and Italian Guidelines Infectious Disease Unit - S. Orsola-Hospital - University of Bologna Corresponding author:
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
What are the most promising opportunities for dose optimisation?
 What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
Updates to the HHS Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents Living with HIV Updated October 17, 2017
 Mountain West AIDS Education and Training Center Updates to the HHS Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents Living with HIV Updated October 17, 2017 26 October 2017 Hillary
Mountain West AIDS Education and Training Center Updates to the HHS Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents Living with HIV Updated October 17, 2017 26 October 2017 Hillary
HIV: Approach to the Treatment-Naïve Patient
 HIV: Approach to the Treatment-Naïve Patient Paul E. Sax, M.D. Clinical Director, Division of Infectious Diseases Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Approach
HIV: Approach to the Treatment-Naïve Patient Paul E. Sax, M.D. Clinical Director, Division of Infectious Diseases Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Approach
BHIVA guidelines on the treatment of HIV-1-positive adults with antiretroviral therapy. START & other changes
 BHIVA guidelines on the treatment of HIV-1-positive adults with antiretroviral therapy START & other changes Contents Introduction & treatment aims Major changes When to start What to start BHIVA: what
BHIVA guidelines on the treatment of HIV-1-positive adults with antiretroviral therapy START & other changes Contents Introduction & treatment aims Major changes When to start What to start BHIVA: what
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort
 Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Disclosures. Introduction to ARV Drug Resistance New Clinicians Workshop 12/9/16. Introduction. ARS Question
 Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
D:A:D: Cumulative Exposure to DRV/r Increase MI Risk
 D:A:D: Cumulative Exposure to DRV/r Increase MI Risk 20.0-15.0-10.0-5.0-4.0-3.0-2.0-1.0- Unadjusted CVD rate ratios per 5 years additional exposure: ATV/r 1.25 [1.10-1.43] and DRV/r 1.93 [1.63-2.28] Adjusted*
D:A:D: Cumulative Exposure to DRV/r Increase MI Risk 20.0-15.0-10.0-5.0-4.0-3.0-2.0-1.0- Unadjusted CVD rate ratios per 5 years additional exposure: ATV/r 1.25 [1.10-1.43] and DRV/r 1.93 [1.63-2.28] Adjusted*
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Kiat Ruxrungtham. Professor of Medicine Chulalongkorn University, and HIV-NAT, Thai Red Cross AIDS Research Centre
 Kiat Ruxrungtham Professor of Medicine Chulalongkorn University, and HIV-NAT, Thai Red Cross AIDS Research Centre www.iasusa.org; www.aidsinfo.nih.gov; www.clinicaloptions.com; www.clinicaloptions.com/hiv
Kiat Ruxrungtham Professor of Medicine Chulalongkorn University, and HIV-NAT, Thai Red Cross AIDS Research Centre www.iasusa.org; www.aidsinfo.nih.gov; www.clinicaloptions.com; www.clinicaloptions.com/hiv
CROI 2017 Review: Novel ART Strategies
 Mountain West AIDS Education and Training Center CROI 2017 Review: Novel ART Strategies Brian R. Wood, MD Assistant Professor of Medicine Medical Director, Mountain West AETC ECHO Telehealth March 2, 2017
Mountain West AIDS Education and Training Center CROI 2017 Review: Novel ART Strategies Brian R. Wood, MD Assistant Professor of Medicine Medical Director, Mountain West AETC ECHO Telehealth March 2, 2017
Second and third line paediatric ART strategies
 Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
What next? Francois Venter. ART new drugs, new studies. Wits Reproductive Health & HIV Institute
 Thanks: Polly Clayden, Francesca Conradie, Loyd Mulenga, Gary Maartens, Andrew Hill, David Ripin, Elli Katabira, Chris Duncombe, Nathan Ford, Marco Vitoria, WHO Industry: Gilead, Janssen, ViivV Abbott,
Thanks: Polly Clayden, Francesca Conradie, Loyd Mulenga, Gary Maartens, Andrew Hill, David Ripin, Elli Katabira, Chris Duncombe, Nathan Ford, Marco Vitoria, WHO Industry: Gilead, Janssen, ViivV Abbott,
Terapia del paciente naive con un régimen de Inhibidor de la proteasa Dr. Jose R Arribas IX Curso de avances en Infección VIH y hepatitis virales
 Terapia del paciente naive con un régimen de Inhibidor de la proteasa Dr. Jose R Arribas IX Curso de avances en Infección VIH y hepatitis virales clinicaloptions.com/hiv Eficacia en Ensayos Clínicos pivotales
Terapia del paciente naive con un régimen de Inhibidor de la proteasa Dr. Jose R Arribas IX Curso de avances en Infección VIH y hepatitis virales clinicaloptions.com/hiv Eficacia en Ensayos Clínicos pivotales
Disclosures. Introduction to ARV Drug Resistance New Clinicians Workshop. Introduction. ARS Question 12/6/2017
 Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
Didactic Series. Update: 2012 HIV Treatment Guidelines. Daniel Lee, MD August 30, 2012
 Didactic Series Update: 2012 HIV Treatment Guidelines Daniel Lee, MD August 30, 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
Didactic Series Update: 2012 HIV Treatment Guidelines Daniel Lee, MD August 30, 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
Josep Mallolas Hospital Clínic Barcelona
 Nuevos paradigmas en la infección VIH Josep Mallolas Hospital Clínic Barcelona 1. Do you believe, I have to start ARV therapy? Incidence and Mortality of AIDS in Spain HIV and NON-AIDS complications HIV
Nuevos paradigmas en la infección VIH Josep Mallolas Hospital Clínic Barcelona 1. Do you believe, I have to start ARV therapy? Incidence and Mortality of AIDS in Spain HIV and NON-AIDS complications HIV
The Integrase Inhibitor Drug Class: A Comparative Clinical Review
 The Integrase Inhibitor Drug Class: A Comparative Clinical Review Ian Frank Professor of Medicine University of Pennsylvania Philadelphia, PA USA franki@pennmedicine.upenn.edu Disclosure Gilead, ViiV/GlaxoSmithKline:
The Integrase Inhibitor Drug Class: A Comparative Clinical Review Ian Frank Professor of Medicine University of Pennsylvania Philadelphia, PA USA franki@pennmedicine.upenn.edu Disclosure Gilead, ViiV/GlaxoSmithKline:
CNS Toxicity of Integrase Inhibitors Myth or Reality? Ignacio Pérez Valero Unidad de VIH. Hospital U. La Paz
 CNS Toxicity of Integrase Inhibitors Myth or Reality? Ignacio Pérez Valero Unidad de VIH. Hospital U. La Paz Question for the audience Do you think that any integrase inhibitor drug produce CNS adverse
CNS Toxicity of Integrase Inhibitors Myth or Reality? Ignacio Pérez Valero Unidad de VIH. Hospital U. La Paz Question for the audience Do you think that any integrase inhibitor drug produce CNS adverse
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents
 Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents Victor Musiime, MBChB, MMED, PhD Senior Lecturer, Makerere University Investigator, Joint Clinical Research Centre (JCRC)
Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents Victor Musiime, MBChB, MMED, PhD Senior Lecturer, Makerere University Investigator, Joint Clinical Research Centre (JCRC)
Antiretroviral Therapy: When and What to Start. Joe Eron, MD University of North Carolina at Chapel Hill School of Medicine
 Antiretroviral Therapy: When and What to Start Joe Eron, MD University of North Carolina at Chapel Hill School of Medicine Learning Objectives As a results of participating in this activity participants
Antiretroviral Therapy: When and What to Start Joe Eron, MD University of North Carolina at Chapel Hill School of Medicine Learning Objectives As a results of participating in this activity participants
The ART of Managing Drug-Drug Interactions in Patients with HIV
 The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies. Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine
 Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
What is the Virologic Support for Two-Drug Regimens?
 What is the Virologic Support for Two-Drug Regimens? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker has received consulting
What is the Virologic Support for Two-Drug Regimens? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker has received consulting
INDUCTION/MAINTENANCE Clinical Case
 INDUCTION/MAINTENANCE Clinical Case Dr. Jose R Arribas @jrarribas INDUCTION/MAINTENANCE (more or less) Dr. Jose R Arribas @jrarribas Disclosures Speaker s Bureau: Viiv, Janssen, Abbvie, BMS, Gilead, MSD
INDUCTION/MAINTENANCE Clinical Case Dr. Jose R Arribas @jrarribas INDUCTION/MAINTENANCE (more or less) Dr. Jose R Arribas @jrarribas Disclosures Speaker s Bureau: Viiv, Janssen, Abbvie, BMS, Gilead, MSD
Didactic Series. Switching Regimens in the Setting of Virologic Suppression
 Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Virological suppression and PIs. Diego Ripamonti Malattie Infettive - Bergamo
 Virological suppression and PIs Diego Ripamonti Malattie Infettive - Bergamo Ritonavir-boosted PIs Boosted PIs: 3 drugs in one The intrinsic antiretroviral activity Viral suppression and high baseline
Virological suppression and PIs Diego Ripamonti Malattie Infettive - Bergamo Ritonavir-boosted PIs Boosted PIs: 3 drugs in one The intrinsic antiretroviral activity Viral suppression and high baseline