Tuberculosis in Children and Adolescents 2017
|
|
|
- Kristian Russell
- 5 years ago
- Views:
Transcription


1 Tuberculosis in Children and Adolescents 2017 George D. McSherry, MD Division of Infectious Diseases Penn State Children s Hospital and Pediatric Section Northeastern Regional Training and Medical Consultation Center Rutgers Global Tuberculosis Institute Tuberculosis Educational Conference Breathe Pennsylvania March 24, 2017
2 Objectives Utilize a risk assessment tool to identify children and adolescents for targeted testing and evaluation for TB infection Apply current recommendations for management of TB infection and TB disease in children and adolescents Understand the difficulties in the diagnosis of TB disease in children and adolescents
3 Tuberculosis in Children and Adolescents Classification system for tuberculosis Epidemiology: Global, national, state Transmission of tuberculosis to children and its significance Public Health Aspects of Tuberculosis Control Targeted Tuberculosis Testing: Why and how to Use of a Risk Assessment Questionnaire Contact Investigations Management of the TB-exposed child Missed opportunities and their effects Latent TB Infection: Diagnosis and treatment The tests BCG vaccine and the TST Difficulties in the diagnosis and treatment of tuberculosis disease in children Clinical presentation and radiographic appearances Mycobacteriology and culture confirmation Barriers to adherence and the importance of DOT Medication: dosages, preparations, administration, Monitoring
4 Class Type Description Classification System for TB No TB exposure Not infected TB exposure No evidence of infection TB infection No disease No history of exposure. Negative reaction to tuberculin skin test or IGRA. History of exposure Negative tuberculin skin test or IGRA.. Positive reaction to tuberculin skin test or IGRA. No clinical, bacteriological, or radiographic evidence of active TB TB, clinically active TB Not clinically active TB suspected M. tuberculosis cultured (if done). Clinical, bacteriological, or radiographic evidence of current disease. History of episode(s) of TB or Abnormal but stable radiographic findings. Positive reaction to a TST or IGRA. Negative bacteriologic studies (if done). and No clinical or radiographic evidence of current disease Diagnosis pending
5 Epidemiology Tuberculosis remains the leading infectious disease in the world Approximately 1/3 of the world s population (>1.9 billion people) is infected with M. tuberculosis In the 2000s: 90 million new cases 30 million deaths Among children <15 years of age: Approximately 13 million cases 5 million deaths 10.4 million of new TB cases in 2015 globally 1 million of these were in children (approx. 10% of total cases) Approx. 3% of these cases likely have MDR-TB and 40,000 are HIV-infected 136,000 children <15 years old died in 2014 from TB Account for 25-40% of severe morbidity, mortality, and sequelae WHO Global TB Report
6 Definition of pediatric tuberculosis (TB): TB disease in a person < 15 years old In 2015: Background: Pediatric Tuberculosis 9,557 TB cases were reported among all age groups 440 (4.6%) were pediatric Age group N Percent out of all age groups 0-4 years % 5-14 years %
7 Pennsylvania TB Cases 2015 All ages: years of age: 3 <5 years of age: years of age: 12

8 Number and Percentage of Pediatric TB Cases by U.S. and Foreign Birth,

9 Percentage of Pediatric TB Cases with Foreign Birth by Birth Country, 1993 and 2015 Ethiopia 6% Ethiopia 2% Philippines 6% Honduras 5% Philippines 10%
10 Epidemiology: United States TB case rates for all ages are higher in urban, lowincome areas, and in nonwhite racial and ethnic minorities Specific groups with high LTBI and TB disease rates: Immigrants and refugees from high-prevalence regions (Asia, Africa, Latin America, countries of the former Soviet Union) International adoptees Travelers to countries with high-prevalence Homeless people Residents of correctional facilities
11 Transmission of M. tuberculosis to Children Children are usually infected by an adult or adolescent in the immediate household Casual extra-familial contact is less often the source of infection Children rarely infect other children or adults: Tubercle bacilli are relatively sparse in secretions Children with pulmonary TB rarely cough Cough, when present, lacks the tussive force needed to aerosolize bacilli
12

13


14 CT chest, cavitary TB adult CT chest, primary TB child
15 Significance of Tuberculosis in Children Public Health: Diagnosis of LTBI or tuberculosis disease in a child is considered a sentinel public health event usually representing recent transmission of TB within a community Personal Health: High rates of morbidity and mortality Red Book 2009 American Academy of Pediatrics
16 Risk of Progression to TB Disease Immunocompetent adults: 5-10% lifetime risk of developing disease after infection Adults with TB infection and HIV infection: 5-10% annual risk of developing disease Children and the risk of TB disease:

17 Risk of Tuberculosis Disease by Age Newton S, et al Lancet ID 2008 after Marais BJ, et al. Int J Tuberc Lung Dis 2004
18 Increased Risk of Progression of LTBI to TB Disease Age groups: Infants and young children Post pubertal adolescents Recent infection: Highest risk in first 6 months after infection Remains high for 2 years Recent immigration Immunodeficiency: HIV infection, Hodgkin disease, lymphoma, diabetes mellitus, chronic renal failure, malnutrition Immunosuppressive drugs: prolonged or high-dose corticosteroid therapy, chemotherapy, tumor necrosis factor (TNF-alpha) antagonists used to treat rheumatoid arthritis and Crohn disease
19 Control of Tuberculosis in the United States Targeted testing of persons with risk Case finding and treatment Contact investigations Red Book 2012
20 TB Control: Targeted TB Testing What is Targeted TB Testing? Identifies persons at high risk of infection with M. tuberculosis Identifies persons at high risk of progressing to disease should they be infected Reduces unnecessary testing, evaluations and treatment CDC, AAP
21 Why Use Risk-Based Targeted TB Testing? Why not use routine, universal, administratively mandated TB testing? Why not use the TST or IGRA as a screening tool? Daycare Schools Colleges Summer camps Answer: Limitations of the TST/IGRA Universal testing means that large numbers of low risk children will be tested: Inefficient use of healthcare resources Even if the specificity of the test approaches 99%, testing of persons in low-prevalence groups would result in mostly false-positives IGRA specificity reduces but does not eliminate false positives in low risk population MMWR 2010;59(No. RR-5)
22 Targeted TB Testing Risk assessment: >1 risk factor identified on screening riskassessment questionnaire General pediatric practice School-based healthcare Contact and source-case investigations Signs and symptoms consistent with TB disease High risk of progression due to underlying conditions: HIV infection, Hodgkin disease, lymphoma, diabetes mellitus, chronic renal failure, malnutrition, prolonged or high-dose corticosteroid therapy, chemotherapy, tumor necrosis factor (TNF-alpha) antagonists
23 Targeted TB Testing Risk-Assessment Questionnaire Has a family member or contact had TB disease? Has a family member had a positive TB test? Was your child born in a high-risk country (i.e. outside US, Canada, Australia, New Zealand, or Western European countries) Has your child traveled to a high-risk country and spent >1 week with the resident population? Red Book 2012
24 Using the Risk Assessment Questionnaire At first contact with child and every 6 months until age 2 years After age 2 years, ask risk assessment questions every year if possible Anytime a risk factor is identified, a TST or IGRA should be performed Red Book 2009
25
26 Diagnosis of TB infection in children Tuberculin skin test (TST) Interferon-γ release assays (IGRAs)


27 Mantoux test Tuberculin skin tests (TST) 5 TU of purified protein derivative (PPD) or 2 TU of PPD-RT23 PPD tuberculin solution contains dozens of TB antigens, exact composition varies from batch to batch Can be difficult to place and interpret properly: Intradermal injection by an experienced provider Requires second visit for interpretation Interpretation requires careful measurement of induration at the site of injection by a provider experienced in this measurement
28 Tuberculin skin tests (TST) False negative results: Improper handling of PPD solution Improper placement of the test Incorrect interpretation of results Immunosuppression: Disease: HIV, early or advanced TB disease, cancer, malnutrition, viral illness (measles, varicella, influenza) Medications: Corticosteroids Cancer chemotherapy Immunomodulating biologic agents (tumor necrosis factor-α inhibitors) Live viral vaccines (measles, perhaps varicella) Positive test can be due to: Infection with M. tuberculosis Infection with nontuberculous mycobacteria (NTM) Receipt of bacille Calmette-Guerin (BCG) vaccine Cannot distinguish LTBI from TB disease
29 Summary: Tuberculin skin tests (TST) There are limitations to both the sensitivity and specificity of the TST PPV is much greater when patients with risk factors for LTBI are tested When used in patients without risk factors, most positive results are false positives This is accentuated among children who have received the BCG vaccine
30 BCG Vaccine and Tuberculin Skin Testing History of BCG is never a contraindication to TST Interpretation of TST results in BCG recipients is the same as for people who have not received the vaccine Difficult to distinguish between (+) TST caused by M.tuberculosis infection and those caused by BCG Reactivity does not occur in some children after BCG vaccination If BCG does cause a (+) TST, the reaction is generally negative by 5 years of age If child is from a high-burden country, (+) TST is almost always due to LTBI Therefore, management of children with a history of BCG and a (+) TST includes: IGRA if >5 years of age, perhaps down to age 2 years, lower if you call me If IGRA positive: Diagnostic evaluation including a chest radiograph and appropriate treatment
31 Interferon-γ Release Assays (IGRAs) Detect interferon-γ release ex vivo from CD4+ lymphocytes stimulated by antigens found on the M. tuberculosis complex Two assays are available: QuantiFERON-TB Gold In-Tube assay (QFT) T-SPOT.TB assay (T-SPOT) Both assays use ESAT-6 and CFP-10 QFT uses a third antigen TB7.7 These antigens are not encoded in the genomes of M bovis-bcg or Mycobacterium avium intracellulare Similar to the TST, IGRAs do not distinguish between TB infection and TB disease Negative IGRA does not rule out either in child with suspicious findings No cross reactivity with M. bovis (BCG vaccine) nor with M. avium complex (MAC) Specificity >TST May cross react with M. kansasi, M. fortuitum, M. marinum
32 Interferon gamma release assays (IGRA): Use in children TST preferred, IGRA acceptable Children <5 years of age Positive IGRA likely indicates infection with M. tuberculosis Negative IGRA does not rule infection with M. tuberculosis Increasing evidence that IGRAs are reliable down to 2 years of age and below IGRA preferred, TST acceptable Children >5 years of age who have received BCG vaccine Children >5 years of age unlikely to return for TST reading AAP Technical Report. Pediatrics 2014;134(6)e1763.
33 Interferon gamma release assays: Use in children Both TST and IGRA should be considered when: Initial and repeat IGRA are indeterminate Initial test (TST or IGRA) is negative and: Clinical suspicion for TB disease is moderate to high Risk of progression and poor outcome is high Initial TST is positive and: Child healthy and at low risk Additional evidence needed to increase adherence Nontuberculous mycobacterial infection suspected Interpretation of (-) IGRA in child with (+) TST: Child unlikely to have LTBI (not universal, depends on clinical situation) Red Book 2015
34 TB Screening: IGRA QuantiFERON Gold in-tube Company: Cellestis, Australia US FDA approved Method: Enzyme linked immunosorbant assay (EIA) Whole blood Incubated with MTB antigens (ESAT-6, CFP-10, TB7.7 ) T-Cells produce INF- γ Supernatant removed INF- γ measured by ELISA reader T-Spot.TB Company: Oxford Immunotec, UK US FDA approved o Method: o Enzyme linked immunospot test (Elispot) PBMC/T-cells Incubated with MTB antigens (ESAT-6 & CFP-10) T-Cells produce INF- γ IFN- γ binds to antibody in wells Spots develop and are counted manually or by reader

35 QuantiFERON -TB Gold IT: ELISA Interpretation of test result Antige n From: QuantiFERON -TB Gold IT product insert

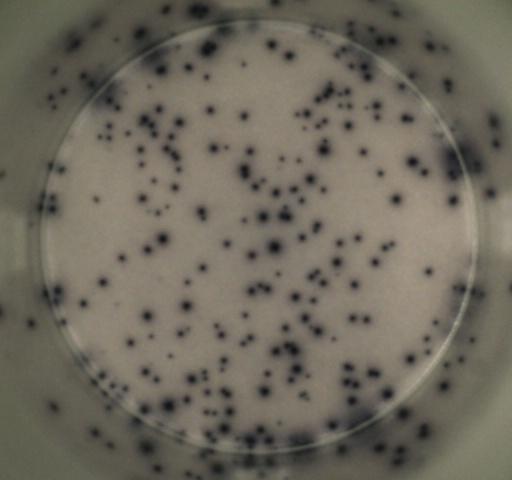

36 Positive T-Spot Negative T-Spot
37 Indeterminate results: Test vs. host failure High background gamma interferon (abnormal negative control) Concurrent illness Mitogen put in the wrong well (nil) Defective tubes Low mitogen (abnormal positive control) Transient or chronic immune suppression QFT-G or T-spot: no mitogen in control well QFT-GIT: defective tubes, overfilling, or inadequate shaking
38 Interferon-γ Release Assays (IGRAs) Standard instructions are provided for performing IGRAs but concerns have been raised about the reproducibility of results on serial performance Serial testing of healthcare workers at low risk of TB infection has shown unexplained conversion of IGRA to positive and then reversion to negative 79/405 Ugandan children tested at age 5 years had positive T-SPOT but only 38 (30%) remained positive when tested 3 weeks later IGRA results are susceptible to variability due to a number of factors: Manufacturing issues, inconsistencies in specimen collection, inadequate blood volume, time of collection, delays in isolation and incubation of cells, inadequate mixing of QFT blood, laboratory error Nkurunungi PLoS One 2012
39 New York City Experience Enhanced LTBI treatment outcomes IGRAs reliable tests for TB infection (risk factors) Contact investigations: One stop testing Fewer false positives (BCG) No need for evaluation and treatment Costs Training of staff Logistics Phlebotomy in infants
40 AAP Technical Report 2014 (Starke)
41 Evaluation of the child with a positive TB test (TST, IGRA) Evaluation of all children with a positive TB test should include: A careful history for symptoms of disease Physical examination Chest radiographs (PA & lateral) Household investigation


42 Control of TB in the United States Contact investigations The most reliable TB control program is based upon aggressive and expedient contact investigations, rather than routine screening of large populations High priority contact: Household Age <5 yrs Med risk condition Procedure Congregate, Time Can be complex and may require lots of detective work Red Book 2009
43 Prevention of TB in Children: Potential Missed Opportunities Failure to find and appropriately manage adult source cases (case finding) Delay in reporting the initial diagnosis of TB Contact investigation interview failure Delay in evaluation of exposed children Failure to completely evaluate exposed children Failure to prescribe INH window prophylaxis Failure to maintain a contact under surveillance LTBI diagnosed; treatment not prescribed Failure to complete treatment for LTBI
 Chest X-ray is normal AND IF <4 years of age START: Isoniazid (INH) 10 mg/kg (max.")
44 Tuberculosis Exposure in Children <4 years of age and Window Prophylaxis History, PE, TST, CXR are done CXR is done regardless of TST result IF the child is: Asymptomatic and physical examination is normal TST is negative (<5 mm) Chest X-ray is normal AND IF <4 years of age START: Isoniazid (INH) 10 mg/kg (max., 300 mg) PO once daily
45 Tuberculosis Exposure in Children Why is INH given as Window Prophylaxis even if there is no evidence of TB infection or disease at the initial visit? Child may already be infected Infection more likely to progress to disease Infants and younger children are more likely to develop disseminated disease or meningitis TST repeated 8-10 weeks after contact broken with infectious adult: If TST (-), discontinue INH If TST (+), re-evaluate child and treat accordingly

46 Timetable of TB in Children after Walgren Tuberculosis. Starke JR, in Feigin, Cherry, Demmler, Kaplan, ed: Textbook of Pediatric ID 2009
47 Case #2: Three generations, two families and a pediatrician Or, source cases, index cases, and contact investigations you never know what you ll get if you keep your eyes open and keep asking questions. Clinicians were asking Could this child have TB? THE IMPORTANCE OF EPIDEMIOLOGY in childhood TB If we could only find an adult source case



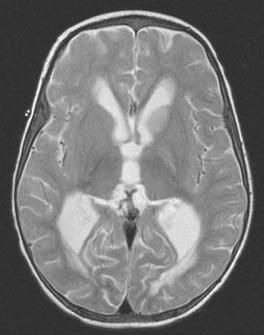

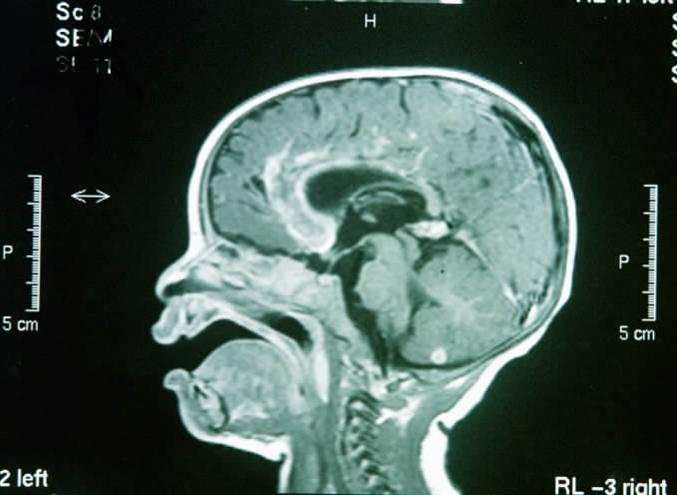
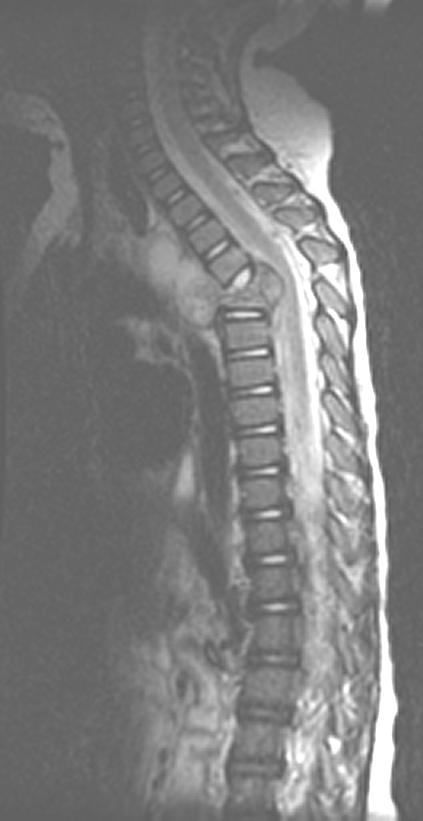
48 CT MRI
49
50

51
52
53
54 Potential Missed Opportunities in TB Control Initially, 5/18 children are diagnosed as TBexposed Two (Ages 6 & 28 months) identified in the contact investigation have 0.0 mm TSTs and normal CXRS at the health department Mother says at the health department that she would like to them to be seen by their private pediatrician No PE done No INH window prophylaxis given




55
56 Potential Missed Opportunities in TB Control Two other children from the same family who have LTBI are referred to the same pediatrician for evaluation and management at mother s request: Receive prescriptions for INH plus 8 refills No follow-up appointments are given Social history: Homeless, 5 children, mother with her own serious health problems, holding down a full-time job Set-up for another missed opportunity? Strong probability Will therapy for LTBI be completed? Was it? Yes, why? DOT of infection (DOTI)








57 6 mo old 7 yr old 11 mo old 17 mo old 5 yr old 2 yr old 2 yr old 2 yr old 6 mo old

58
59 Case History: Final Numbers Eighteen children were exposed to a 26-year old woman with bilateral cavitary pulmonary tuberculosis: 15/18 (83%) children are infected 9/15 (60%) develop TB disease Two after initial negative TST (Missed opportunity) 1 TB meningitis, 2 miliary 6/15 (40%) have LTBI 3/18 (17%) are TB-exposed but not infected Through 3 generations: All 2 nd and 3 rd generation cases preventable TB-infected child of today may become the index pt. of tomorrow without treatment for LTBI
60 The High Cost of Missed Opportunities Missed opportunities documented: Failure to find and appropriately manage adult source cases (Case finding) Contact investigation interview failure Delay in evaluation of exposed children Failure to completely evaluate exposed children Failure to prescribe prophylactic INH Failure to complete treatment for LTBI (Adherence)
61 Evaluation of the Child with a positive TST or IGRA Evaluation of all children with a positive TB test should include: A careful history for symptoms of disease Physical examination Chest radiographs (PA & lateral) Household investigation
62 Treatment of Latent Tuberculosis Infection INH mg/kg (max., 300 mg) PO daily for 270 doses Efficacy approaches 100% Alternative: Twice weekly directly observed (DOT) INH mg/kg (max., 900 mg) PO for 72 doses Monitor index case isolate sensitivities Hepatotoxicity from INH is rare in children: Monthly assessment for clinical evidence of hepatotoxicity should be made: malaise, loss of appetite or weight, nausea, vomiting, abdominal pain, jaundice Routine monitoring of LFTs is not indicated, except: Concurrent liver disease Pregnancy or first 12 weeks postpartum Concurrently on other hepatotoxic medications Clinical evidence of hepatoxic effects
63 Treatment of Latent Tuberculosis Infection Rifampin mg/kg/day (max. 600 mg) po daily for 6 months is an alternative INH not tolerated Index patient isolate INH-resistant Cruz & Starke, (IJTLD 2014) : Rifampin mg/kg/day (max. 600 mg) po daily for 4 months: Safe, completion rates similar to 9INH by DOPT Additional regimens for LTBI treatment: 3 months of INH + rifampin 2 months of rifampin + PZA (When given as part of regimen: H, R, Z, E to treat TB disease and child subsequently found to have LTBI only)
64 What about the 12-dose, intermittent INH-RPT regimen for children? Children >12 years of age: Recommended as equal alternative to 9 months of INH Children 2-11 years of age: INH for 9 months recommended INH-RPT: Insufficient safety and efficacy data to recommend universal use in this age group INH-RPT: An option if completion of 9H unlikely and likelihood or hazard of TB is great Children <2 years of age: INH for 9 months recommended INH-RPT: Not recommended: Lack of safety and pharmacokinetic data in this age group
65 How Children with Tuberculosis are Identified Presentation with a symptomatic illness Discovery of a child with pulmonary tuberculosis during contact investigation of an adult with tuberculosis Few or no symptoms Evaluation: (+) TST/IGRA and abnormal CXR In some areas of U.S. up to 50% of children with TB are discovered in this manner Before significant symptoms have developed
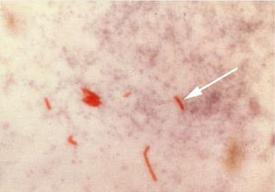
66 Mycobacteriologic Diagnosis of Tuberculosis Adults: 70-90% have a sputum that is (+) for M. tuberculosis Children: Tubercle bacilli are relatively few in number Sputum generally cannot be obtained from children <10 yrs old Gastric aspirates in children with PTB % sensitive in children 60-70% sensitive in infants Bronchoalveolar lavage (BAL): Sensitivity may be less than gastric aspirates

67 Pediatric TB Cases by Case Verification Criteria*, N= 21,223 Lab Confirmed 26% Clinical Case 52% Provider Diagnosis 22% *Based on the public health surveillance definition for TB [MMWR 1997:46(No. RR-10):40-41]
 Pulmonary 71% Miliary (1.3) Bone & Joint (1.5) Other (4.3) *Any extrapulmonary involvement which includes cases that are extrapulmonary only and both.")
68 Pediatric TB Cases by Site of Disease, Extrapulmonary 22% Both 7% Any extrapulmonary involvement* (totaling 29.5%) Extrapulmonary site (%) Lymphatic (18.8) Meningeal (3.6) Pulmonary 71% Miliary (1.3) Bone & Joint (1.5) Other (4.3) *Any extrapulmonary involvement which includes cases that are extrapulmonary only and both. Patients may have more than one disease site but are counted in mutually exclusive categories for surveillance purposes.
69 Difficulties in the Diagnosis of Tuberculosis in Children Children are often asymptomatic or symptoms are nonspecific: Fever, poor appetite, poor weight gain or weight loss Approximately 22-30% of disease is extrapulmonary Meningitis and miliary disease tend to develop soon after infection 70-80% occur in children 0-4 years of age Epidemiologic link (the adult source case) Crucial to identify the adult source case for the child Provides strong evidence that the child suspected of having TB disease actually has TB May be the only isolate available for susceptibility testing
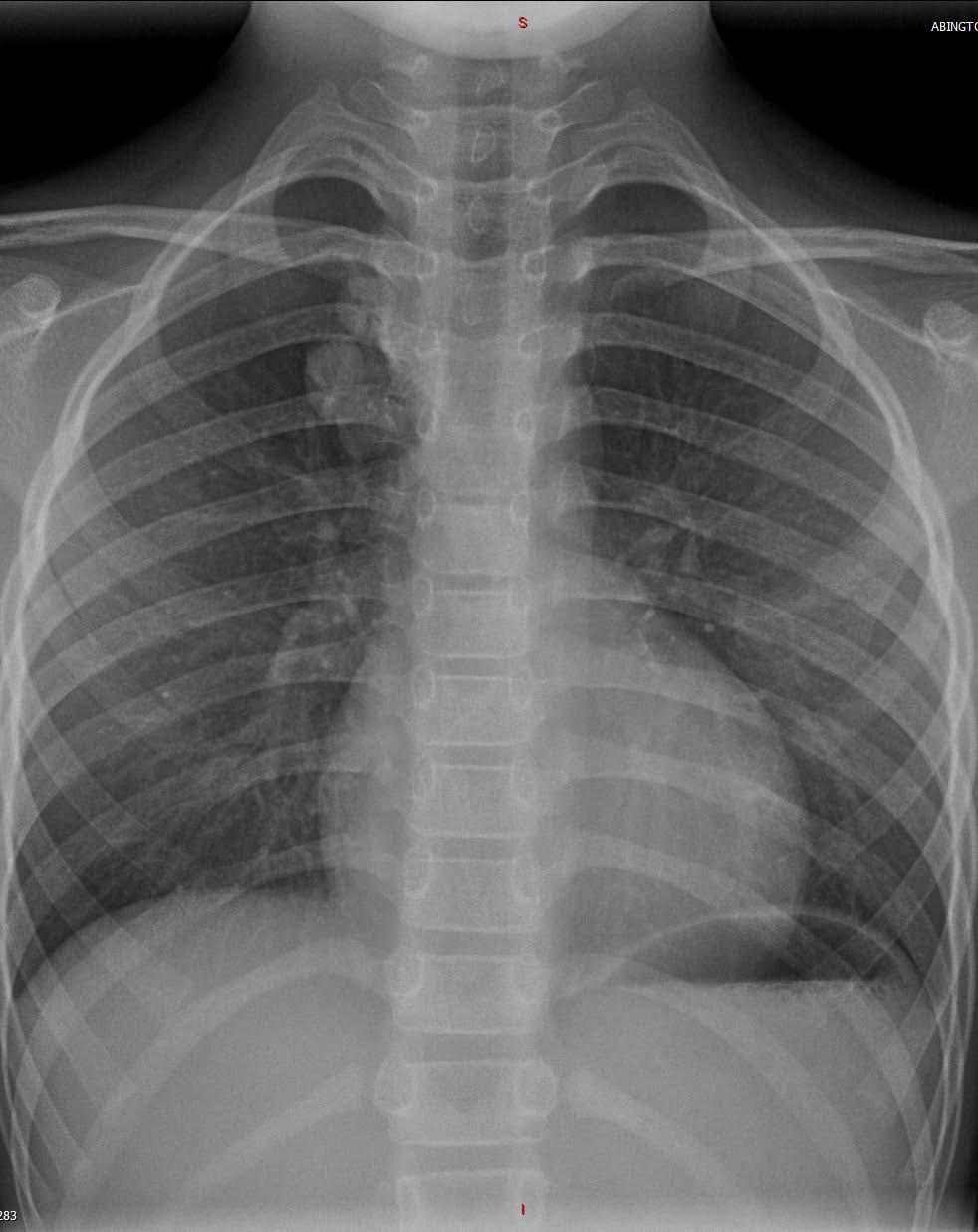
70 Difficulties in the Diagnosis of Tuberculosis in Children Physical examination may be normal TST may be negative (10-40%). IGRA? Chest radiograph: Any lobe of the lung may be involved Good technique/experience with children Two views Careful interpretation
71
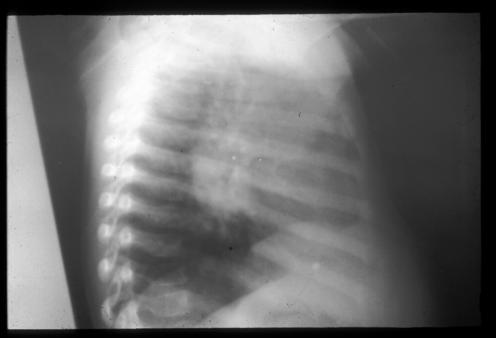
72

73
74
75

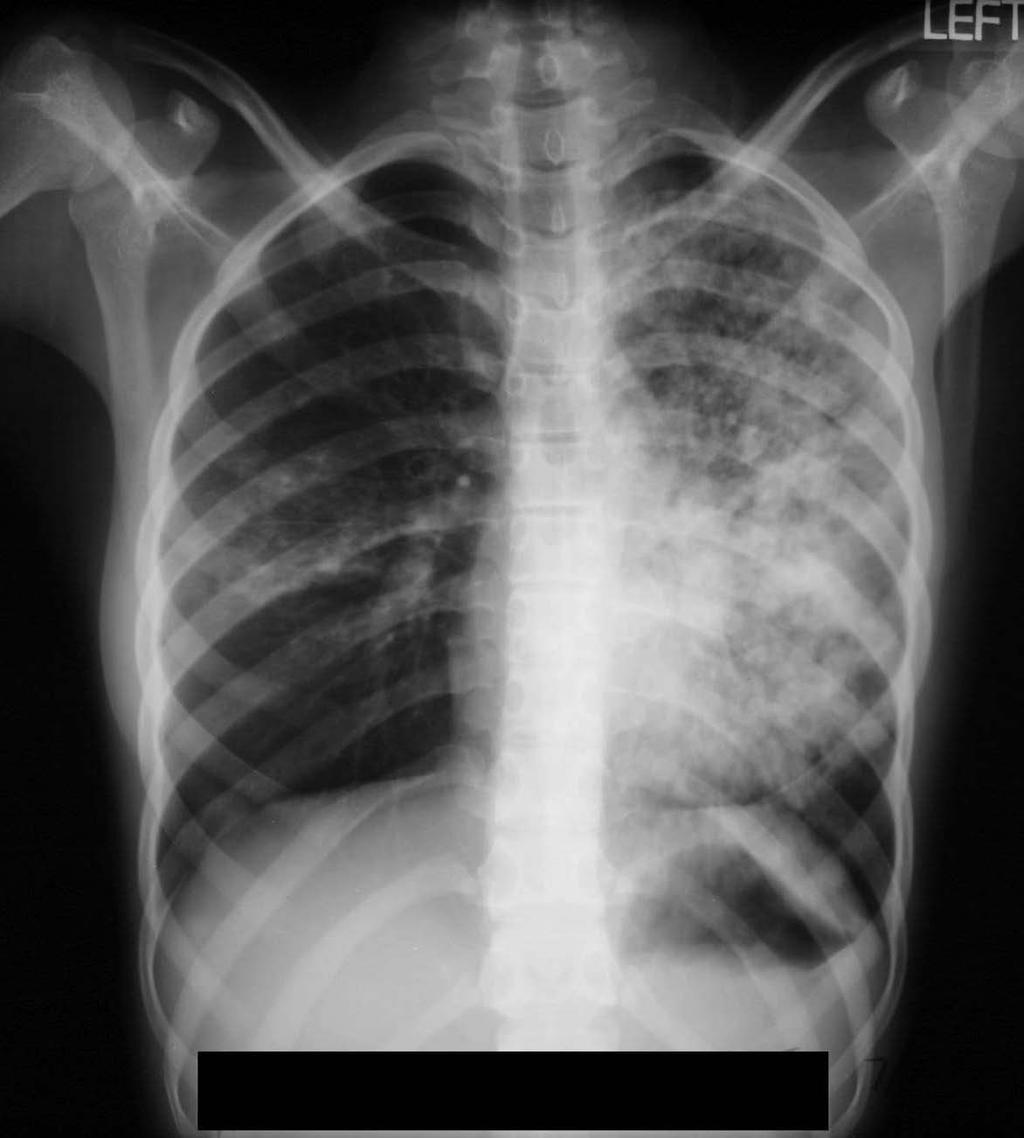
76


77

78


79
80 Tuberculosis in Adolescents Adolescents develop tuberculosis in one of two ways: Reactivation of infection acquired during childhood The closer to puberty at the time of infection the greater the risk of reactivation Chronic pulmonary tuberculosis Progression of infection acquired during adolescence to disease: Classic primary disease Progressive primary pulmonary tuberculosis Chronic pulmonary tuberculosis


81 Adolescents: Reactivation Tuberculosis Constitutional symptoms often more prominent than respiratory symptoms Weight loss and fever are very common Drenching night sweats occur several times per week Cough, chest pain, hemoptysis Cavitary lesions frequently seen


82
83 Case #7: Another missed opportunity: Just how bad can this get? OR Can you die from TB if you are a teenager? AND Why LTBI is important!

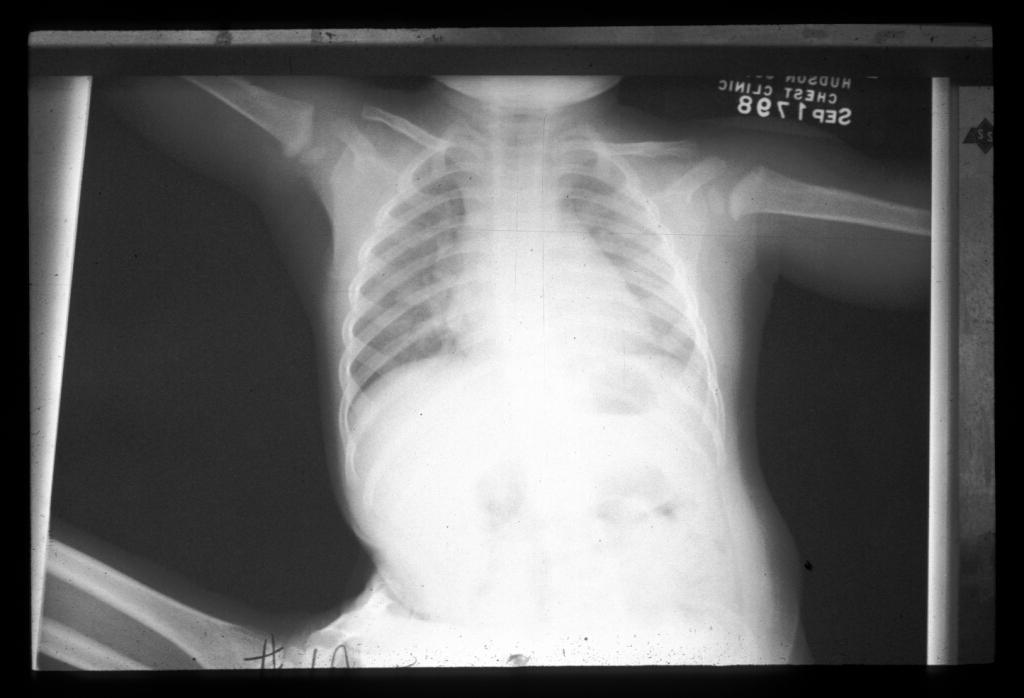
84 Case #21 8-year old girl, recently arrived from Haiti was evaluated at the DOH for a 12 mm TST reaction There were no symptoms of TB disease and PE was normal A chest radiograph was done: INH 200 mg po once daily; #30 tabs dispensed 6 months later the chart reads: Overdue for medication refill. There were no further notes.until 5 years later.
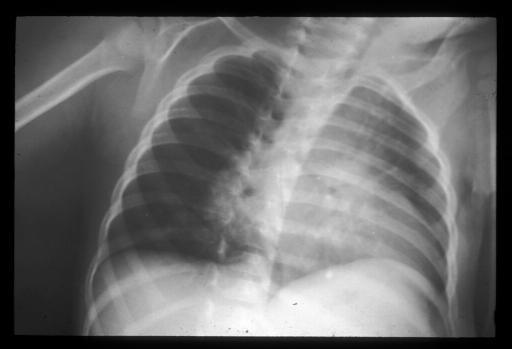
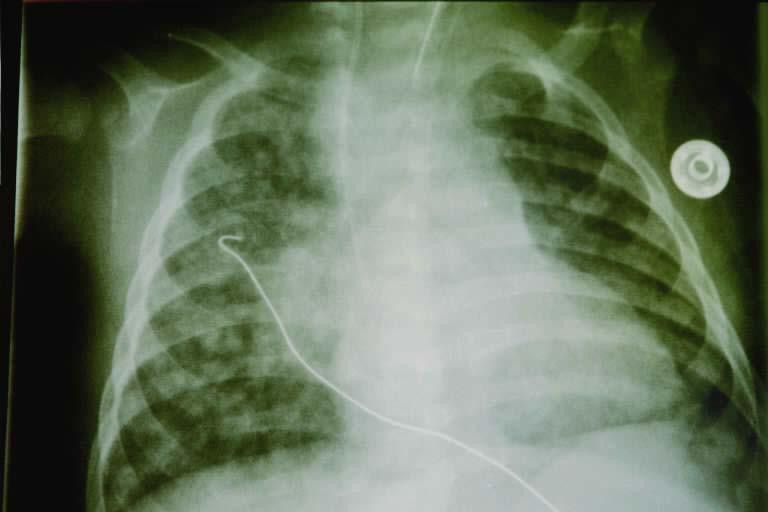
85 Hospital Admission The patient, now 13-years of age, was admitted to a local hospital with a 3 week history of fever, cough, increasing dyspnea, and weakness She had been sent home by the school nurse on 4 occasions over the previous 2 months for the fever and cough and then for weight loss and weakness She was seen on 2 occasions by her PCP and was given antibiotics (azithromycin) and twice in EDs of local hospitals: The last ED visit was 9 days PTA when chest radiographs were done and amoxicillin-clavulanate (Augmentin) was given There was no improvement with antibiotic A chest x-ray was done in the last ED:
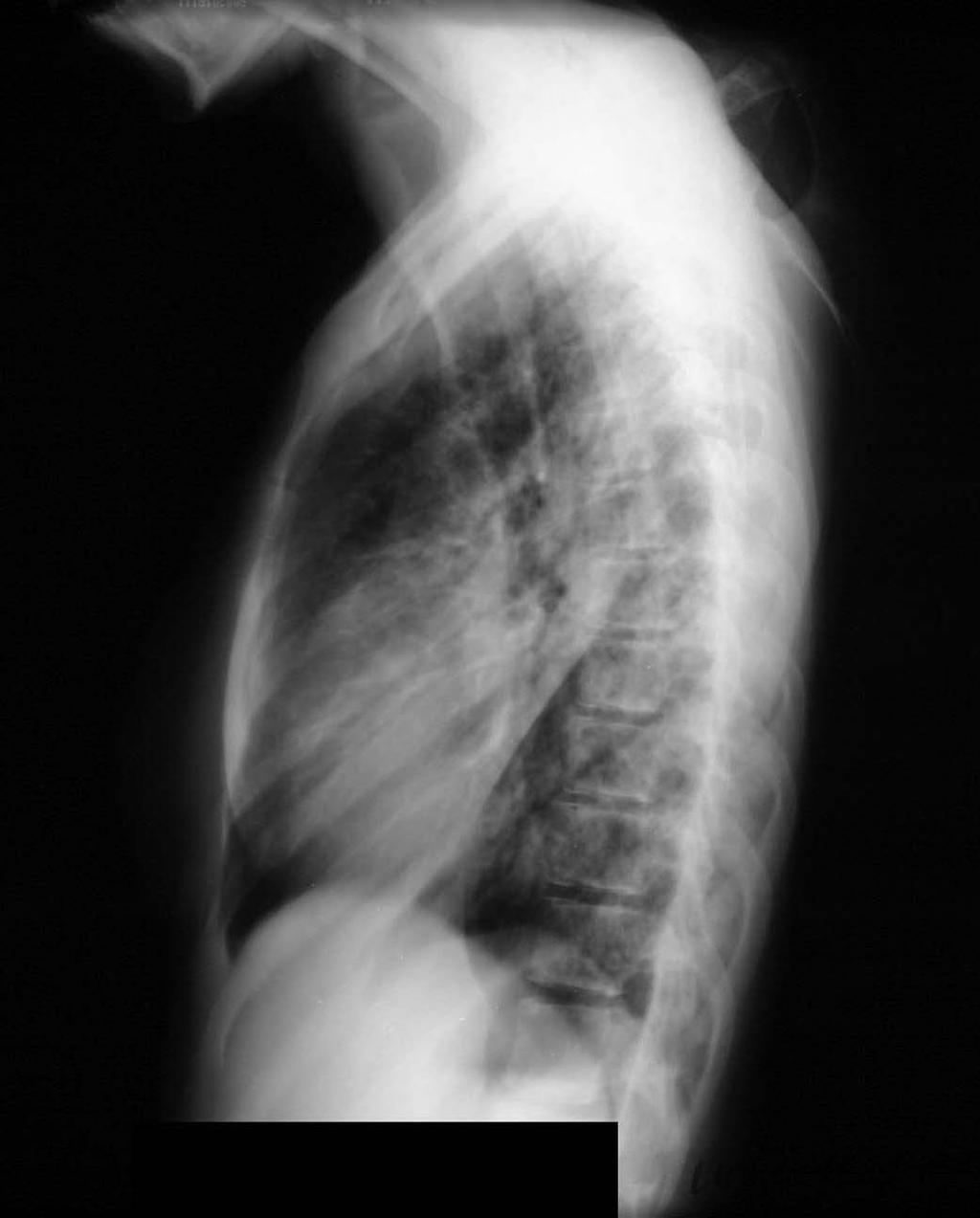
86
87 Case PE: Cachetic, weak appearing female with flat affect in mild respiratory distress T F HR 160 RR 22 O 2 sat = 92% Wt: 78.7 lbs UBWt.: 96.7 lbs Treatment IV ceftriaxone and oral azithromycin Infectious Diseases consultation: Sputa: AFB smear: (+), few AFB; culture (+): pansensitive MTB Anti-TB medications started: INH 300 mg po daily RIF 600 mg po daily PZA 500 mg po, three times a day (?) Emb 400 mg po, twice daily (?)


88 102 0 F Vital Sign Graphic Sheets
89 Case 7/12: At hospital discharge Remains febrile Came directly to Hudson County Chest Clinic with driven by her brother and sister with TB escort Cachetic, weak with unsteady gate Continued treatment added supplement, ibuprofen DOT by RN Home visit by CRNP (PED) Weak, tires easily, bed ridden, bed-bathroom, bedroom had no windows, home was very warm (no AC) Poor oral intake Tachypneic, tachycardic


90 Hospitalized 7/24-8/17: Weaker, hypoxemic, cachectic with weight down to 66 lbs RR sat 90% Continued TB meds; oxygen NGT placed for continuous nutritional supplementation

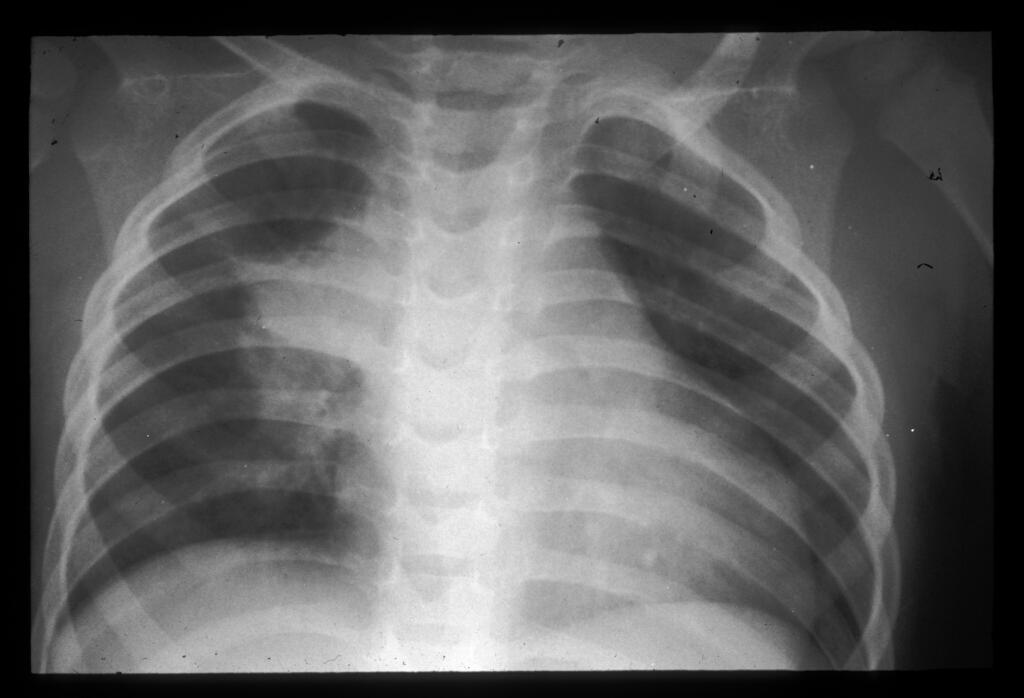
91 Case Gradually regained strength and began to walk Discharge: 8/17 RR 20 on 1L oxygen; Wt 76 lbs TB meds and supplement AC purchased and placed in home 8/23: Wt. 88 lbs; RR = 18 O 2 sat 97% on RA 9/20: Wt. 97 lbs; RR = 18 11/1: Wt. 99 lbs 12/13: Wt 102 lbs 12/13 CXR:
92 Treatment of TB in Children & Adolescents If INH resistance rate >4% or if other risk for resistance include four drugs in initial regimen: Isoniazid (10 mg/kg/day, range 10-20, max. 300) Rifampin (15 mg/kg/day, range 10-20, max. 600) Pyrazinamide (20-30 mg/kg/day) Ethambutol (15-25 mg/kg/day) Treatment complicated by child unfriendly preparations of the medications Directly observed therapy (DOT) Monitor liver transaminases? Depends on severity of disease Follow susceptibility studies of Mtbc isolate (index and/or child isolate) Important to be familiar with resistance patterns in the community
93 Summary Reported cases of tuberculosis in the U.S.: More than 2/3 occurs in nonwhite racial and ethnic groups More than 50% occur in foreign born persons Among children case rates are highest in infants and postpubertal adolescents Children are usually: Infected by adult or adolescent household contacts Not infectious (contagious) Tuberculosis or LTBI in a child is a sentinel public health event Contact investigations and targeted TB testing are mainstays of TB control in the U.S. Evaluation of TB-exposed child: TB test, CXR, window prophylaxis Risk assessment questionnaires are the most effective screening tool to detect children at risk for LTBI TB diagnosis in young children requires a high index of suspicion DOT is key to successful treatment
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
Peggy Leslie-Smith, RN
 Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
TB Intensive Tyler, Texas December 2-4, 2008
 TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
The Origin of Swine Flu
 How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
These recommendations will remain in effect until the national shortage of PPD solution has abated.
 Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
Advanced Concepts in Pediatric Tuberculosis
 Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Using Interferon Gamma Release Assays for Diagnosis of TB Infection
 Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Technical Bulletin No. 172
 CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Jeffrey R. Starke, M.D. has the following disclosures to make:
 AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
New Standards for an Old Disease:
 New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Latent TB Infection (LTBI)
") Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Tuberculosis 6/7/2018. Objectives. What is Tuberculosis?
 Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
Contact Investigation
 Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Diagnosis and Medical Case Management of Latent TB. Bryan Rock, MD April 27, 2010
 TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
2017/2018 Annual Volunteer Tuberculosis Notice
 Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
The Epidemiology of Tuberculosis in Minnesota,
 The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
Disclosures. Current Issues and Controversies in Child and Adolescent Tuberculosis 02/24/2016. NSTC 2016 Annual Meeting
 Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Interpretation of TST & IGRA results. Objectives
 Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
TB Clinical Guidelines: Revision Highlights March 2014
 TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines
 Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Tuberculin Skin Testing
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Tuberculosis Education for the Medical Professional
 Tuberculosis Education for the Medical Professional North Dakota Diagnosis and Medical Management of Latent TB Infection Dawn Farrell, RN, BSN, PHN Maria Robles, BSN July 10, 2007 Tuberculosis Education
Tuberculosis Education for the Medical Professional North Dakota Diagnosis and Medical Management of Latent TB Infection Dawn Farrell, RN, BSN, PHN Maria Robles, BSN July 10, 2007 Tuberculosis Education
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Santa Clara County Tuberculosis Screening Requirement for School Entrance Effective June 1, 2014
 Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011 Douglas Hornick, MD has the following disclosures to
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011 Douglas Hornick, MD has the following disclosures to
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Tuberculosis: Where Are We Now?
 Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic