Tuberculosis: Where Are We Now?
|
|
|
- Amie Terry
- 5 years ago
- Views:
Transcription

1 Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey
2 Learning Objectives Understand the current epidemiologic state of TB globally and in the United States Discuss current diagnostics and treatment options for persons with TB infection Understand the basics of TB disease
3 Outline Epidemiology Global Domestic Tuberculosis infection versus disease Diagnosing TB infection Treatment of TB infection Basics of TB disease Resources

4 Source: WHO Global Tuberculosis Report 2016

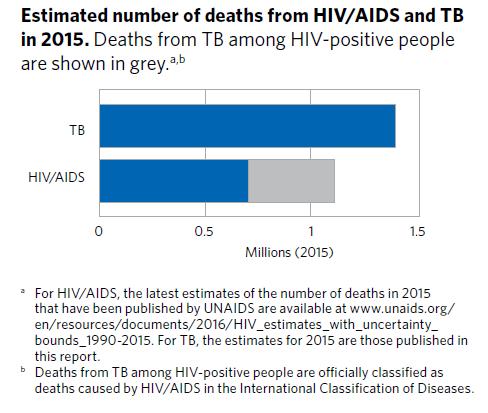
5 Source: WHO Global Tuberculosis Report 2016


6 1/3 of world s population has latent TB infection
7


8 Reported Tuberculosis (TB) Cases United States, * No. of cases *As of June 9, Year Schmit KM, Wansaula Z, Pratt R, Price SF, Langer AJ. Tuberculosis United States, MMWR Morb Mortal Wkly Rep 2017;66:

9 TB Case Rates,* United States, 2015 *Cases per 100,000 population; as of June 9, 2016.

10 TB Case Rates by Race/Ethnicity,* United States, Cases per 100,000 population * All races are non-hispanic. As of June 9, 2016.

11 TB Case Rates, by Age Group and Race/Ethnicity,* United States, 2015 Cases per 100,000 population * All races are non-hispanic; multiple race indicates two or more races reported for a person, but does not include persons of Hispanic/Latino origin. As of June 9, 2016.

12 Number of TB Cases Among U.S.-Born versus Foreign-Born Persons, United States, * No. of cases * As of June 9, % of cases are in minorities 68% of all cases are in foreign-born Case rate in foreign-born is 14x higher than US-born

13 Reported TB Cases, by Origin and Race/Ethnicity, United States, 2015* U.S.-born persons Foreign-born persons All races are non-hispanic; multiple race indicates two or more races reported for a person, but does not include persons of Hispanic/Latino origin. * As of June 9, American Indian/Alaska Native and Native Hawaiian/Other Pacific Islander accounted for <1% of cases among foreign-born persons and are not shown.


14 Percentage of Foreign-Born Persons Among TB Cases, United States,* 2005 and 2015 * As of June 9, 2016.

15 Percentage of Foreign-Born Persons with TB, by Time of Residence in U.S. Before Diagnosis, 2015* Percentage * As of June 9, Foreign-born TB patients for whom information on length of residence in the United States before diagnosis is unknown or missing.

16 Number of tuberculosis cases diagnosed among foreignborn persons <10 years and 10 years after arrival in the United States, Tsang CA, Langer AJ, Navin TR, Armstrong LR. Tuberculosis Among Foreign-Born Persons Diagnosed 10 Years After Arrival in the United States, MMWR 2017


17 TB in Pennsylvania cases cases 2016 Case rate 1.4 Pennsylvania 2015 State Health Profile; CDC
18 Summary of Trends in US Number of cases increased in 2015, but down in 2016; case rate similar 2/3 of all cases are in people born outside the US, the majority of whom have been residing in US > 5 years HIV coinfection has decreased to < 6% TB cases among homeless individuals has also declined (<5%) Resuming and intensifying progress to TB elimination ( 1 case/million) requires Existing priorities - case identification, early treatment, contact tracing needed to prevent resurgence Tb elimination requires new strategies especially to detect and treat latent TB infection in at-risk groups
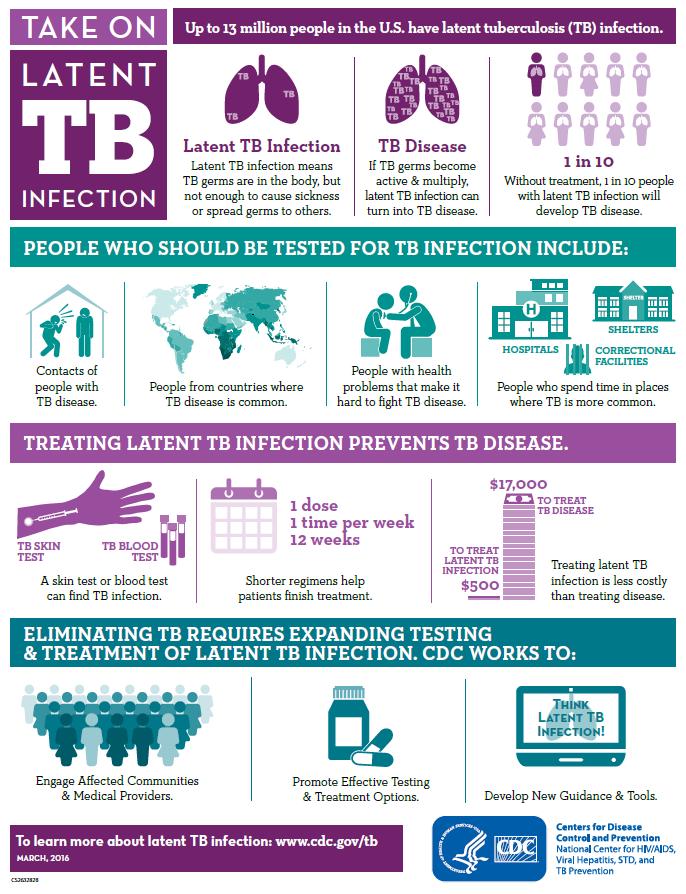
19 TB Infection (LTBI) in the US Up to 13 million people in US infected; ~ 4.5% 5-10% may go on to have active TB if untreated ~ 70% of LTBI in foreign born individuals 19% of US born with LTBI treated; 10% of foreign born Treatment 90% effective 80% active cases arise from prior infection No significant decline in TST or IGRA positivity over past decade Mancuso et al, AJRCCM, 2016
20 TB Infection in US Mancuso et al, AJRCCM, 2016
21 TB Infection in the US Up to 13 million people in US infected; ~ 4.5% 5-10% may go on to have active TB if untreated 80% active cases arise from prior infection ~ 70% of LTBI in foreign born individuals No significant decline in TST or IGRA positivity over past decade A large reservoir of LTBI remains, and continues to be a barrier to TB elimination Ramping up targeted testing and treatment is the path to TB elimination Clinicians, health care agencies, community organizations, esp those serving at-risk patients, are critical to success

 Before starting medications such as TNFα blocker Clinicians and community organizations critical to TB elimination Many at high risk not seen")
22 CDC & USPSTF Targeted testing and treatment CDC and USPSTF recommend testing in those at increased risk USPSTF Those from countries with increased TB prevalence, regardless of time in US Those in high risk congregate settings Consult with L/SHD about populations at risk CDC still recommends testing HCW Close contacts Certain medical illnesses (HIV, DM,etc.) Before starting medications such as TNFα blocker Clinicians and community organizations critical to TB elimination Many at high risk not seen by HD TB disease often missed by today s clinician TB education/outreach needed
23 Tuberculosis (LTBI) Definitions Diagnosis Treatment
24 TB Infection vs. TB Disease A Person with Latent TB Infection A Person with Active TB Disease Has no symptoms Does not feel sick Cannot spread TB to others Usually has a positive skin test or Interferon Gamma Release Assay (IGRA) Has a normal CXR and sputum test Has symptoms that may include: a bad cough that lasts longer than 2 weeks pain in the chest coughing up blood or sputum weakness or fatigue weight loss no appetite chills fever night sweats May spread TB to others Usually has a positive skin test or IGRA May have an abnormal chest x-ray, or positive sputum smear or culture

25 Who do we test? High risk of infection Close contacts Work/live high-risk settings Those from countries where TB is common High risk of progression HIV infection Recently infected Young children IDU Immunocompromised Those not properly treated for TB disease in past
26 Diagnosis of TB Infection No definitive or gold standard test Tests do not distinguish latent from active TB Tuberculin Skin Testing (in use > 100 years) Interferon Gamma Release Assays (IGRA) Quanti-FERON TB Gold In Tube T-SPOT.TB Testing goal is to identify those who will most benefit from treatment Likelihood of infection Risk of progression and morbidity Lower the risk of future transmission

27 TST Limitations Cross reacts with BCG and non-tuberculous mycobacteria Limited sensitivity, especially in immunosuppressed Poor positive predictive value: Very few will go on to develop TB disease Requires technical expertise for administration and test interpretation Patient must return for 2 nd visit

28 Interferon Gamma Release Assays (IGRAs) In-vitro blood tests Measure interferon gamma release from T-cells stimulated by specific antigens

29 Quanti-FERON Gold In Tube Method Tubes: Nil TB Antigen Mitogen Measure IFN - gamma

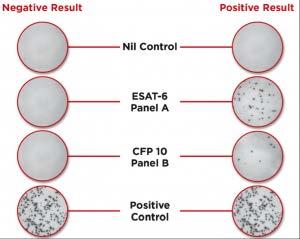
30 T-SPOT.TB Test
31 Interferon Gamma Release Assays (IGRAs) Andersen et al., Lancet, 2000.
32 Overall Test Performance More specific Sensitivity** Specificity (BCG vaccinated population) TST 71-82% *60% 97% QFT 81-86% > 95% > 95% T-SPOT.TB 90-95% 98% * Variable, depends on when and how often BCG was given **Sensitivity wanes in HIV or young children Specificity (non- BCG vaccinated population) Advantages: one visit, blood test, more specific Pai, M etal. Clinical Microbiology Reviews, 2014 King et al., AJRCCM, 2015
33 IGRA Interpretation QFT-GIT Result Nil TB Ag Nil (IU/ml) Mitogen Nil (IU/ml) Interpretation Positive and 25% nil Any M.tb infection likely Negative 8.0 <0.35 or < 25% nil 0.5 M.tb infection unlikely Indeterminate 8.0 > 8.0 <0.35 or < 25% nil Any <0.5 Any Uncertain likelihood of infection TB-SPOT.TB Result Nil TB Response Mitogen Interpretation Positive 10 spots 8 spots Any M.tb infection likely Borderline 10 spots 5, 6, 7 spots Any Uncertain likelihood of infection Negative 10 spots 4 spots 20 spots M.tb infection unlikely Indeterminate > spots Any 4 spots Any < 20 spots Uncertain likelihood of infection
 Borderline (T-SPOT ) In borderline zone close to cut point If result borderline, invalid or indeterminate and reason to test still exists, can repeat")
34 Indeterminate and Borderline Tests Indeterminate Poor response to mitogen (+ control), may improve with repeat test Delay in processing Technical errors Patient factors: immunocompromised High background IFN gamma in nil (- control) Borderline (T-SPOT ) In borderline zone close to cut point If result borderline, invalid or indeterminate and reason to test still exists, can repeat test

35 Pai M et al. Clin. Microbiol. Rev. 2014;27:3-20 Sources of variability in IGRAs

36 Clinical Infectious Diseases (2017): Vol 64 Prior Guidelines from 1999 and 2003.

37 LTBI Diagnostic Approach Lewinsohn et al. ATS/IDSA/CDC: Diagnosis of TB in Adults and Children. CID 2017:64

38 LTBI Diagnostic Approach Lewinsohn et al. ATS/IDSA/CDC: Diagnosis of TB in Adults and Children. CID 2017:64
39 Testing in Health Care Workers Serial testing can result in conversions, reversions, boosting, random variability Criteria for conversion and boosting have been established for TST Definite criteria for conversions and reversions with IGRA not clear yet Some studies show quite a bit of variability around the IGRA cut point with serial testing true infection/conversion versus false positive In one large HCW study, IGRA conversion was seen more frequently then TST conversion
40 A 45 y.o. health care worker who works in a TB clinic, and is otherwise healthy, has an indeterminate QFT GIT test. What should be done next? Repeat IGRA and try to avoid delays in processing
41 A college s student health service is developing a policy on testing for TB infection. In the past, the clinic has had < 50% students return after their initial visit. Some of their students are international exchange students from South Asia and Central America. If you were asked to choose an IGRA or TST for this clinic s mode of LTBI diagnosis, which would you choose? IGRA is the better choice given difficulty getting students back as well as students who have likely had BCG vaccine
42 Diagnosis of LTBI - Summary TST and IGRA are imperfect tests for identifying TB infection; IGRA more specific Neither rules out TB Disease Neither differentiates TB Disease from TB infection Avoid testing in low risk people All tests have lower sensitivity in immunocompromised patients IGRA is preferred in BCG vaccinated individuals and in those unlikely to return for 2 nd visit, who are likely to have M.tb infection and have low/intermed risk of progression (2017 guidelines - strong recommendation) Both IGRA and TST may be helpful in certain populations (2017 guidelines conditional recommendations) Retesting may be indicated in borderline or indeterminate results
43 Treatment of TB Infection Rule out TB disease History, exam, chest radiograph, bacteriology if needed Assess risks and benefits of treatment Educate and counsel patient Why treatment is indicated Potential side effects Duration of therapy Completion of treatment is low Maximize with shorter regimen, selecting right population
44 Treatment Regimens for LTBI Drugs Months of Duration Interval Minimum Doses INH 9* Daily 270 2x wkly** 76 INH 6 Daily 180 2x wkly** 52 RIF 4 Daily 120 INH-RPT 3 Weekly** 12 *Preferred ** Intermittent treatment only with directly observed therapy (DOT)
45 TB Infection Treatment Completion of Isoniazid for 9 months (9H) is variable, but poor even in controlled situations 52%-69% (latter in a controlled study) Why? Hepatotoxicity Provider preferences Duration and pill burden
46 TBTC Study 26: PREVENT TB Patients with LTBI at high risk for reactivation (mainly close contacts of active cases) 9 months of daily INH, selfadministered (270 doses) 3 months of once weekly INH and rifapentine by DOT (12 doses) Study endpoint: development of active TB at 33 months
47 INH and Rifapentine for 12 weeks (3HP) Efficacy was similar 82% in INH-RPT vs. 69% completion in standard therapy group Fewer adverse events in INH-RPT arm More hepatotoxicity in INH alone group More possible hypersensitivity reactions in INH- RPT
48 INH-RPT Recommendations Equal alternative to 9 months INH in otherwise healthy individuals 12 years old + high risk for TB disease: Close contact Converter Fibrotic changes on CXR HIV not on ART, otherwise healthy Others are considered on an individual basis Main limitation: Need for directly observed therapy
49 INH-RPT NOT Recommended Children < 2 years old HIV on ART Pregnancy, or likely to become pregnant during treatment Presumed INH or RIF resistance Prior adverse effects with INH or rifamycins

50 Self Administration or Modified DOT iadhere Study: Directly observed therapy (DOT) v self administered (SAT) v self administered with weekly text reminders (esat) Completion rates were measured in multiple countries SAT in the US was non-inferior to DOT Discontinuation due to adverse events was similar among groups Video DOT Use of recorded or video visits being studied at several sites Convenient, well accepted Awaiting CDC recommendation on SAT and modified DOT Such strategies may improve initiation and adherence to therapy Belknap et al., CROI, 2015 Gold et al., Open Forum Infectious Diseases, 2016
51 RPT Adverse Effects Reddening of secretions Uncommon Hepatotoxicity (0.4%) Leukopenia Thrombocytopenia Hypersensitivity seen with other rifamycins (3.8%) Fever, flu-like, pruritus, hypotension, headache, petechiae Hepatic induction of drug metabolism Be observant of other potential adverse effects as regimen more widely used Report: MedWatch
52 Other Short-Course Regimens for TB Infection RIF daily for 4 months (4R) INH resistant or intolerant Patient unlikely to be adherent for longer treatment period 80-85% treatment completion rates In situations where Rifampin cannot be used (e.g., HIVinfected persons receiving protease inhibitors), Rifabutin may be substituted Increases completion rate, lessens burden on public health clinic Caveats Be aware of drug interactions Methadone, Prednisone, Protease Inhibitors, Oral contraceptives, Many others
53 Treatment of LTBI: Comparison of INH vs. RIF Comparison of Regimen Features: 9H and 4R Regimen Feature 9H 4R High efficacy X X* Lower hepatotoxicity X Lower overall cost X Higher adherence X More effective against INH-resistant strains X (e.g., among foreign-born persons) Shorter duration X Fewer drug-drug interactions X * Good evidence that 3R is at least as efficacious as 6H. Inferential reasoning from other evidence suggests that efficacy of 4R may approach that of 9H. AJRCCM 170; , 2004
54 A 47 y.o. household contact to a patient with active TB is found to be QFT GIT positive. She is known to be TST negative in the past. She is on no medications and is otherwise healthy. She works from home and lives with the index case. Which regimen is best for this patient? Short course INH + Rifapentine weekly for 12 weeks via DOT No other interfering medications Index case also getting home DOT convenient Fits study population
55
56 TB Infection: Future Directions Emphasize use of short-course rifamycin containing regimens Ongoing trials 9H v 4R 9H v 1 month daily INH and Rifapentine Self-administered weekly INH and Rifapentine with text messaging reminders (iadhere) Role of Rifabutin
57 Advances in TB Disease Diagnosis GeneXpert Line probe assays Urine LAM Treatment New uses for known drugs New drugs Short course and novel regimens

58 TB Disease Maintain a high index of suspicion especially in highrisk groups Transplant, patients on TNF blockers, patients receiving chemotherapy, dialysis patients Consult with local health department to understand who is atrisk in your community Diagnostic tools are only useful if disease is suspected New diagnostics allow for more rapid identification AND treatment of TB preventing transmission Prevention (by identifying and treating LTBI) is the key
59
60

61 Summary Unite to End TB Demographics of TB in US are changing USPSTF policy + advances in diagnosing (IGRA) + treating (3HP and other short course regimens) TB infection will help get us to TB elimination New strategies and partnerships between public health and other health care providers key Newer, faster diagnostics for TB disease, but need to think TB There are many resources available in different formats; know your local and regional experts
62 globaltb.njms.rutgers.edu

 482 3627 mc_gtbi@njms.")
63 Northeastern Regional Training and Medical Consultation Center Global TB Institute 1 (800) mc_gtbi@njms.rutgers.edu
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Latent TB Infection (LTBI)
") Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Sharing the Care: Working Together on LTBI Treatment and Management Webinar. September 24, Curry International Tuberculosis Center
 TB Infection Diagnostics and Treatment Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention 1 Curry International
TB Infection Diagnostics and Treatment Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention 1 Curry International
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Peggy Leslie-Smith, RN
 Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
LTBI: Who to Test & When to Treat
 LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
The Most Widely Misunderstood Test of All
 The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Pediatric Tuberculosis in Los Angeles County: An Update
 Pediatric Tuberculosis in Los Angeles County: An Update Julie Higashi, MD PhD Director, Tuberculosis Control Program March 2, 2019 0 Pediatricians will be the driving force of TB elimination in California
Pediatric Tuberculosis in Los Angeles County: An Update Julie Higashi, MD PhD Director, Tuberculosis Control Program March 2, 2019 0 Pediatricians will be the driving force of TB elimination in California
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Latent TB Infection (LTBI) Strategies for Detection and Management
 Strategies for Detection and Management") Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Conflict of Interest Disclosures:
 Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Advanced Concepts in Pediatric Tuberculosis
 Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
Screening for Tuberculosis Infection. Harlingen, TX. Linda Dooley, MD has the following disclosures to make:
 TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
Revised Technical Instructions for Civil Surgeons. October 9, 2018
 Revised Technical Instructions for Civil Surgeons October 9, 2018 Speakers Joanna Regan Centers for Disease Control and Prevention Shereen Katrak California Department of Public Health Pennan Barry California
Revised Technical Instructions for Civil Surgeons October 9, 2018 Speakers Joanna Regan Centers for Disease Control and Prevention Shereen Katrak California Department of Public Health Pennan Barry California
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Tyler, Texas December 2-4, 2008
 TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Using Interferon Gamma Release Assays for Diagnosis of TB Infection
 Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
Latent tuberculosis infection
 EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
ATS/CDC Guidelines for Treating Latent TB Infection
 TB Intensive Tyler, Texas June 2-4, 2010 ATS/CDC Guidelines for Treating Latent TB Infection Timothy R. Aksamit, MD June 2, 2010 ATS/CDC Guidelines for Treating LTBI Tuberculosis Intensive University of
TB Intensive Tyler, Texas June 2-4, 2010 ATS/CDC Guidelines for Treating Latent TB Infection Timothy R. Aksamit, MD June 2, 2010 ATS/CDC Guidelines for Treating LTBI Tuberculosis Intensive University of
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines
 Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal
 Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Diagnosis and Medical Case Management of Latent TB. Bryan Rock, MD April 27, 2010
 TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
TB Intensive. San San Antonio, Texas. December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 ATS/CDC Guidelines for Treating Latent TB Infection Timothy Aksamit, MD; Mayo Clinic December 1, 2010 ATS/CDC Guidelines for Treating LTBI Tuberculosis
TB Intensive San Antonio, Texas December 1-3, 2010 ATS/CDC Guidelines for Treating Latent TB Infection Timothy Aksamit, MD; Mayo Clinic December 1, 2010 ATS/CDC Guidelines for Treating LTBI Tuberculosis
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Michael J. Huey, MD. NYSCHA Annual Meeting WE-2, October 19, 2016
 Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination
 IUATLD North American Region Conference February 24, 2017 Vancouver, BC Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
IUATLD North American Region Conference February 24, 2017 Vancouver, BC Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
11/1/2017. Disclosures. Update In Tuberculosis, Indiana Outline/Objectives. Pathogenesis of M.tb Global/U.S. TB Burden, 2016
 Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Programmatic management of LTBI : a two pronged approach for ending the TB epidemic. Haileyesus Getahun Global TB Programme WHO/HQ
 Programmatic management of LTBI : a two pronged approach for ending the TB epidemic Haileyesus Getahun Global TB Programme WHO/HQ What is latent TB infection? A state of persistent immune response to stimulation
Programmatic management of LTBI : a two pronged approach for ending the TB epidemic Haileyesus Getahun Global TB Programme WHO/HQ What is latent TB infection? A state of persistent immune response to stimulation
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014
 TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Community pharmacy-based tuberculosis skin testing
 Community pharmacy-based tuberculosis skin testing Shanna K. O Connor, PharmD ISU KDHS Spring CE Seminar 2018 In support of improving patient care, Idaho State University Kasiska Division of Health Sciences
Community pharmacy-based tuberculosis skin testing Shanna K. O Connor, PharmD ISU KDHS Spring CE Seminar 2018 In support of improving patient care, Idaho State University Kasiska Division of Health Sciences
Jeffrey R. Starke, M.D. has the following disclosures to make:
 AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
Interpretation of TST & IGRA results. Objectives
 Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
TB Infection: The Old and The New
 TB Infection: The Old and The New Ellen R. Murray, PhD, BSN, RN Southeast National TB Center ellen.murray@medicine.ufl.edu Objectives At the completion of this session, participants will be able to: Select
TB Infection: The Old and The New Ellen R. Murray, PhD, BSN, RN Southeast National TB Center ellen.murray@medicine.ufl.edu Objectives At the completion of this session, participants will be able to: Select
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2, 2011 ATS/CDC Guidelines for Treating LTBI Timothy Aksamit, MD April 6, 2011 Timothy Aksamit, MD has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 2, 2011 ATS/CDC Guidelines for Treating LTBI Timothy Aksamit, MD April 6, 2011 Timothy Aksamit, MD has the following disclosures to make: No conflict of interests
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION
 TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
The Elimination of Tuberculosis. Richard E. Chaisson, MD. Center for TB Research Center for AIDS Research Johns Hopkins University
 The Elimination of Tuberculosis Richard E. Chaisson, MD Center for TB Research Center for AIDS Research Johns Hopkins University Disclosures Spouse owns Merck stock Consultant: Merck Research funding:
The Elimination of Tuberculosis Richard E. Chaisson, MD Center for TB Research Center for AIDS Research Johns Hopkins University Disclosures Spouse owns Merck stock Consultant: Merck Research funding:
TB Intensive San Antonio, Texas May 7-10, 2013
 TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis. WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED
 Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
New Standards for an Old Disease:
 New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
The Role of Rifampin for the Treatment of Latent TB Infection. Introduction. Introduction
 The Role of Rifampin for the Treatment of Latent TB Infection March 26, 2008 Alfred A. Lardizabal, MD Associate Professor of Medicine New Jersey Medical School Global Tuberculosis institute Treatment of
The Role of Rifampin for the Treatment of Latent TB Infection March 26, 2008 Alfred A. Lardizabal, MD Associate Professor of Medicine New Jersey Medical School Global Tuberculosis institute Treatment of
Coordinating with Public Health on Tuberculosis Testing & Treatment
 Coordinating with Public Health on Tuberculosis Testing & Treatment Bernadette Jakeman, PharmD, PhC, BCPS, AAHIVP Associate Professor University of New Mexico College of Pharmacy Objectives 1. Identify
Coordinating with Public Health on Tuberculosis Testing & Treatment Bernadette Jakeman, PharmD, PhC, BCPS, AAHIVP Associate Professor University of New Mexico College of Pharmacy Objectives 1. Identify
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination
 Four Corners TB and HIV Conference November 3, 2015 Durango, CO The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
Four Corners TB and HIV Conference November 3, 2015 Durango, CO The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011 Douglas Hornick, MD has the following disclosures to
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011 Douglas Hornick, MD has the following disclosures to
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 ATS/CDC Guidelines for Treating Latent TB Infection Timothy Aksamit, MD August 7, 2012 Timothy Aksamit, MD has the following disclosures to make: No conflict
TB Intensive San Antonio, Texas August 7-10, 2012 ATS/CDC Guidelines for Treating Latent TB Infection Timothy Aksamit, MD August 7, 2012 Timothy Aksamit, MD has the following disclosures to make: No conflict
Tuberculosis Infection in the US Military
 Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army