Medicine, Stanford University School of Medicine, Stanford, CA, USA.
|
|
|
- Teresa Hensley
- 5 years ago
- Views:
Transcription
1 JCM Accepted Manuscript Posted Online 13 January 2016 J. Clin. Microbiol. doi: /jcm Copyright 2016, American Society for Microbiology. All Rights Reserved. 1 2 Interferon-γ release assays for latent tuberculosis: what are the sources of variability? Niaz Banaei a,b,c#, Rajiv L. Gaur a, and Madhukar Pai d a Department of Pathology, Stanford University School of Medicine, Stanford, CA, USA. b Department of Medicine, Division of Infectious Diseases and Geographic Medicine, Stanford University School of Medicine, Stanford, CA, USA. c Clinical Microbiology Laboratory, Stanford University School of Medicine, Stanford, CA, USA. d McGill International TB Centre & Department of Epidemiology & Biostatistics, McGill University, Montreal, Quebec, Canada. # Corresponding author Niaz Banaei, MD 3375 Hillview Ave, Room 1106 Palo Alto, CA Phone: Fax: nbanaei@stanford.edu 1
2 Abstract Interferon-γ release assays (IGRAs) are blood-based tests intended for diagnosis of latent tuberculosis infection (LTBI). IGRAs offer logistical advantages and are supposed to offer improved specificity over the tuberculin skin test (TST). However, recent serial testing studies in low risk individuals have revealed higher false conversion rates with IGRAs compared with TST. Reproducibility studies have identified various sources of variability that contribute to non-reproducible results. Sources of variability can be broadly classified as pre-analytical, analytical, post-analytical, manufacturing, and immunological. In this review, we summarize known sources of variability and their impact on IGRA results. We also provide recommendations on how to minimize sources of IGRA variability. 2
3 Introduction Interferon gamma (IFN-γ) release assays (IGRAs) are laboratory alternatives to tuberculin skin test (TST) for diagnosis of latent tuberculosis infection (LTBI) (1). IGRAs are ex vivo assays that measure T-cell response after over-night stimulation with relatively Mycobacterium tuberculosis (MTB)-specific antigens. IGRAs are increasingly replacing TST for annual screening of U.S. health care workers and are also utilized in student/employee health and public health programs, and in screening of patients prior to immunosuppression (1). In addition, IGRA conversion rate is now being used as a measure of vaccine efficacy in TB vaccine trials (2). IGRAs are supposed to offer improved specificity over the TST (1). By and large, this advantage holds true in populations that receive BCG vaccination after infancy (one year of age) or receive multiple doses; specificity of TST is compromised in such settings (1). However, in practice, IGRAs have proved less specific in low risk North American health care workers and college students (1). Furthermore, several studies have raised concerns over high rates of IGRA reversions (1). Given the growing use of IGRAs, it is imperative that we identify the underlying sources of variability and understand their impact on IGRA accuracy. The two most widely used IGRAs include the QuantiFERON-TB Gold In-Tube (QFT-GIT) assay (Cellestis/Qiagen, Carnegie, Australia), and the T-SPOT.TB (T- 3
4 SPOT) assay (Oxford Immunotec, Abingdon, United Kingdom). Although a new, 4-tube version of QFT (called QFT-Plus) has been launched by Qiagen, this version is currently not approved in the US. The QFT-GIT assay, the FDAapproved version, is an enzyme-linked immunosorbent assays (ELISA)-based, whole-blood test that uses peptides from the two RD1 antigens (ESAT-6 and CFP-10) as well as peptides from a one additional antigen (TB7.7 [Rv2654c]) in an in-tube format. The assay consists of three tubes: the negative control (nil) tube that measures background IFN-γ response, the antigen tube that measures antigen-specific response, and the positive control (mitogen) tube that measures non-specific T-cell response. The qualitative result (negative, positive, or indeterminate) is interpreted from quantification of IFN-γ in international units (IU) per milliliter (ml). An individual is considered positive for MTB infection if the TB response (IFN-γ response to TB antigens minus the background IFN-γ response) is above the test cut-off. The T-SPOT is an enzyme-linked immunospot (ELISPOT) assay performed on separated and counted peripheral blood mononuclear cells (PBMC) after incubation with ESAT-6 and CFP-10 peptides in separate wells. The assay consists of four wells: the negative control (nil) well that measures background IFN-γ producing T-cells (spot forming cells [SFC]), the two antigen wells that measure MTB-specific SFC to ESAT-6 and CFP-10, and the positive control (mitogen) well that measures non-specific SFC. The qualitative result (negative, positive, or indeterminate) is interpreted from number of SFC. An individual is 4
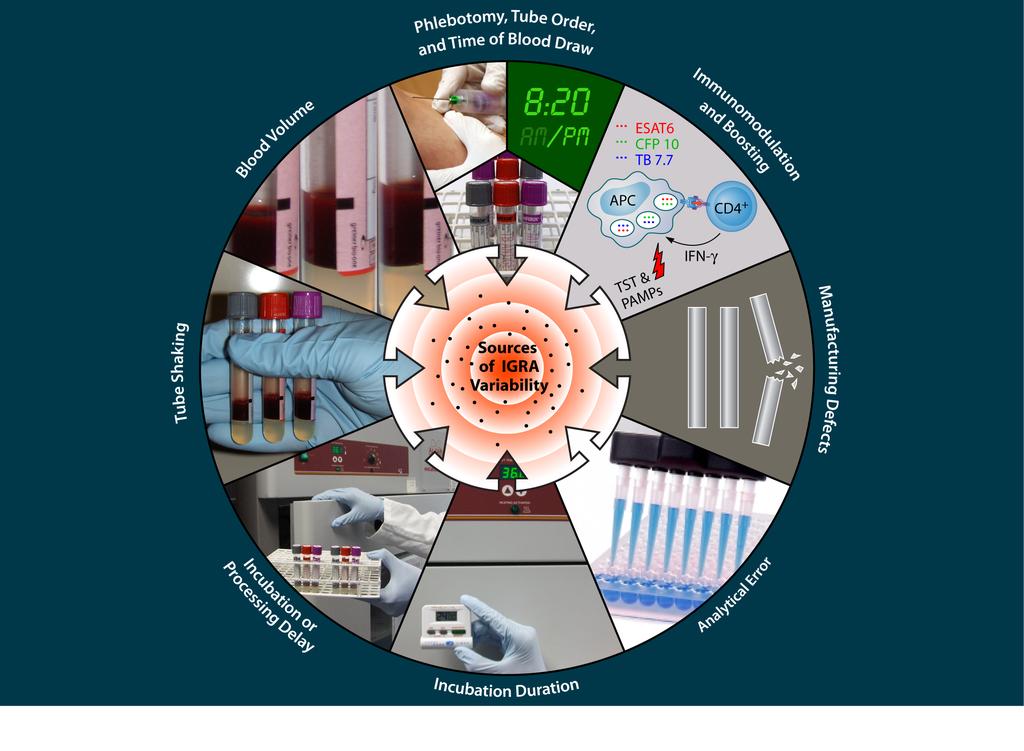
5 considered positive for MTB infection if the spot counts in the TB antigen wells exceed a specific threshold after subtracting the spots in the negative control well. Oxford Immunotec offers T-SPOT testing in the U.S. via its own national reference laboratory called Oxford Diagnostic Laboratories (Memphis, TN). Given the multiple steps involved in IGRAs, error can be introduced at any point during testing. In addition, because IGRAs are functional assays, they are susceptible to modulation by different factors. In recent years, studies have identified and characterized various sources of variability. Most of these studies have investigated variability in the QFT-GIT assay because it is more widely used for on-site testing than the T-SPOT assay. In a previous analysis (1), we broadly classified the sources of variability as pre-analytical, analytical, manufacturing and immunological (Figure 1). In the ensuing sections we update our previous review, and describe each source of variability and the potential impact it may have on results (Table 1). Sources of Variability Pre-analytical. Pre-analytical sources of variability are numerous and represent some of the more important sources of IGRA variability (3). The time of blood collection might make a difference. Mazurek et al. reported significantly higher TB response values with the QFT-GIT assay when blood was collected in the evening as compared to the morning (4). Phlebotomy is the first window of opportunity for introduction of predictable variability. Inadequate disinfection of 5
6 the skin and the rubber septum of blood collection tubes may introduce microbial contaminants into the blood sample. The immunomodulatory effect of microbes is discussed below under immunological sources of variability. Blood collection in the correct order of QFT-GIT tubes (starting with the nil and ending with the mitogen) might matter. Contamination of the antigen tube with mitogen can cause a false positive result and contamination of the nil tube with mitogen can cause a false negative result. Next, the volume of blood drawn into the QFT-GIT antigen tube can alter results. The blood volume drawn into the vacutainer tubes can range from 0.8 to 1.2 ml according to the package insert and a published study (5). Gaur et al. investigated the impact of 0.8, 1.0 and 1.2 ml blood added to the antigen tube and showed that blood volume inversely correlates with TB response in infected individuals and results in false-negative results in some individuals (5). Lastly, vigorous shaking of QFT-GIT tubes can non-specifically increase IFN-γ response in the nil and the antigen tube and lead to either a false-positive or a falsenegative result depending on which tube is shaken excessively (5). Amongst the potential sources of variability shown in Figure 1, processing delay between blood collection and incubation of cells is an important variable (3). According to the package inserts, incubation of the QFT-GIT tubes can be delayed for up to 16 hours and processing of a blood sample for the T-SPOT assay can be delayed for up to 8 hours. However, studies using ELISPOT and 6
7 non-commercial whole-blood assays have shown a processing delay of 1 to 4 hours before stimulation with MTB antigens results in a lower number of IFN-γproducing T cells (6). Doberne et al. investigated the impact of incubation delay on QFT-GIT and showed a significant decline in TB response when incubation was delayed by 6 and 12 hours, resulting in 19% (5/26) and 22% (5/23) falsenegative rates, respectively (7). Incubation delay has also been shown to increase the indeterminate rate due to reduction of the mitogen response below the assay threshold in the QFT-GIT assay (7-9). Jarvis et al. showed lower mitogen responses when QFT tubes are kept at room temperature (as suggested by the manufacturer) or lower temperatures, which may explain the higher indeterminate rate observed with incubation delay (10). The impact of processing delay (immediately after blood collection vs. delayed) on the T-SPOT assay has not been studied in individuals with MTB infection. Beffa et al. showed a higher rate of T-SPOT indeterminate results during autumn and winter than in spring and summer, suggesting that transport of blood specimen at lower ambient temperatures may negatively impact the assay (11). The manufacturer of the T-SPOT assay offers the T-Cell Xtend to extend processing time up to 32 hours. The T-Cell Xtend is an antibody complex added to the blood sample in the laboratory to deplete inhibitory neutrophils. Although several groups have investigated the impact of the T-Cell Xtend (12-14), none has compared immediate processing to delayed processing with and without the T-Cell Xtend. Therefore, the potential utility of the T-Cell Xtend remains to be 7
8 demonstrated. This is crucial, because nearly all T-SPOT testing in the U.S. is currently outsourced (personal communication with laboratory directors) and thus, processing delay may lead to reproducibly false-negative results in a low risk population (15). The length of time T-cells are stimulated with TB antigen in IGRAs also can vary between runs. According to package inserts, the length of incubation can range from 16 to 24 hours for the QFT-GIT assay and hours for the T-SPOT assay. It is reasonable to expect longer incubations to give rise to higher concentration of IFN-γ and larger number of SFC. However, Gaur et al. showed that incubation of QFT-GIT tubes for 16, 20 and 24 hours does not increase TB response in infected individuals and does not cause false-positive results in uninfected individuals (5). Studies have also shown plasma storage at 4 C and - 80 C for 4 weeks or PBMC storage at -80 C for 4 weeks does not have a major effect on QFT-GIT and ELISPOT results, respectively (6, 16). Analytical. Analytical sources of variability refer to unpredictable fluctuations in assay measurements due to uncontrolled factors in biological fluids (matrix effects); to imprecision of pipetting; manipulation errors in centrifugation, decantation, and washing steps; and to imprecision of measurement of final signal by the operator or the instrument (17). Much effort has been invested by the manufacturers to improve the analytical reproducibility of enzyme-linked immunoassays (17). Still, considerable analytical variability occurs and clinical 8
9 assays typically deal with this through adoption of an indeterminate range. To illustrate analytical variability with the QFT-GIT assay, we took a sample with borderline-negative TB response (Figure 2A) and another sample with a borderline-positive TB response (Figure 2B) and measured TB response by an automated ELISA instrument over 20 consecutive ELISA runs. Not only did the TB response fluctuate quantitatively, giving a CV of 14% and 11%, respectively, two (10%) and four (20%) times, respectively, they crossed the assay cut-off giving rise to discrepant results. Studies investigating between-run reproducibility of the QFT-GIT assay have shown while there is a high degree of agreement between dichotomous results, there is considerable variability in quantitative results which leads to discordant results when TB response is bordering the assay cut-off (16, 18-20). Metcalfe et al. used a model to estimate between-run CV for 366 samples retested by two technicians after 2-3 days of storage at 4 C (18). They showed ±0.6 IU/mL (CV 14%) between-run variability for all individuals and ±0.24 IU/mL (CV 27%) variability for subjects with initial response in the borderline range of 0.25 to 0.8 IU/mL. They reported a conversion and reversion rate of 9% and 7%, respectively; 86% (24/28) of discordant results occurred among samples with borderline TB response. Withworth et al. reported between-laboratory standard deviation of 0.16 IU/ml when blood was tested in three laboratories using automated ELISA instruments (19). Discordant results were reported in 7.7%, 85.7% of which had responses ±0.25 IU/mL of the assay cut-off. Whitworth et al. 9
10 also showed greater between-run variability when ELISA was performed manually vs. automated (21). Tuuminen et al. measured within-run and between-run variability for the QFT-GIT and the T-SPOT assays showing that between-run variability exceeded within-run variability for both assays (20). Analytical error originating from ELISPOT and ELISA readers has been investigated for commercial IGRAs. Franken et al. assessed inter-reader variability for spot counting (22) with 4 different observers and two automated readers. The proportion of positive results varied between readers by maximally 15%. Some individuals were found to systematically count more spots than others. In another study, Van Zyl-Smit et al reported no more than 1 spot variability at counts of 0 to 10 spots per well and no significant variability in optical density values for the ELISA plates reread over 2 hours (23). Post-analytical. Clerical error during manual data entry can culminate in false results (19). Clerical error can be avoided by interfacing the ELISA system with the laboratory information system. Manufacturing. Manufacturing defects can cause non-reproducible IGRA results. False positive QFT-GIT results related to faulty antigen tubes have been documented. Slater et al. reported an incident of sudden increase in daily QFT- GIT positivity rate from 10% to 31% (24). Paired testing of 463 subjects with the suspect antigen tube lot and a new lot confirmed a manufacturing defect causing 10
11 false positive results. Although the manufacturer could not identify the cause of the defect, in 2013 the manufacturer issued a market withdrawal for another faulty antigen tube lot causing false-positive results. Review of their manufacturing process identified a potential bacterial contamination. The manufacturer reported implementing corrective measures to prevent reoccurrence of this problem. Since then, there have been two other reports of faulty antigen tubes causing false-positive results (25, 26). Indeterminate QFT-GIT results due to faulty mitogen tubes have also been reported. In 2013 the manufacturer of the QFT-GIT assay reported increased rates of indeterminate results with the introduction of a new lot of the mitogen tube. Interestingly, not all users were equally affected which suggests varied pre-analytical practices, such as time to incubation, might have contributed to the problem. Immunological. Two immunological sources of IGRA variability have been described to date: in vivo immune boosting by the TST and ex vivo immunomodulation by microbial products. Van Zyl-Smit et al. and other investigators have reported a significant increase in TB response with the QFT- GIT and the T-SPOT assays when these assays follow a TST by more than 3 days (27). This boosting effect can result in a conversion in a previously IGRAnegative individuals. It is not clear how long the boosting persists and whether the purified protein derivative (PPD) formulation contributes to boosting. The 11
12 mechanism of TST boosting is thought to be through an immune recall of memory T-cells to RD1 antigens (and TB7.7 for QFT-GIT) that are present in the PPD extract. Although IGRA boosting is predominantly observed in MTBinfected individuals (27), few studies have reported few conversions after TST testing in individuals with no risk factors for MTB infection (28-31). IGRAs are susceptible to modulation by endogenous and exogenous factors. Microbe-associated molecular patterns (MAMPs), such as peptidoglycan and lipopolysaccharide (LPS), are potent modulators of innate and adaptive immunity through activation of pathogen recognition receptors on immune cells (32). It is well known that skin and environmental microorganisms can be introduced into the blood specimen during phlebotomy. It has also been shown that systemic circulation contains peptidoglycan originating from the gut microbiota (33). Thus, it is plausible that microbial contaminants and circulating MAMPs could modulate IGRAs to cause non-reproducible results. Gaur et al. showed that LPS added to QFT-GIT tubes at 10 ng/ml could non-specifically increase the TB response and cause false-positive results (34). Gaur et al. also showed that as few as 10 colony forming units of Staphylococcus aureus, a skin colonizer, spiked into the antigen tube alone or into both the nil and the antigen tubes is sufficient to cause false-positive results in 6.9% of 58 uninfected individuals tested (35). Although not shown in that study, it is possible that S. aureus could also cause falsenegative results if added to the nil tube alone. 12
13 Eliminating sources of variability While variability caused by random sources is unavoidable and can only be addressed through adoption of an indeterminate range (variation attributed to random error), systematic sources of variability can be minimized through standardization of laboratory procedures and quality assurance of reagents. In the ensuing section we describe best practices for IGRAs based on lessons learned from reproducibility studies. 1. Disinfection. IGRA package inserts currently lack specific instructions on the choice of disinfectant and the method of skin and tube septum disinfection to minimize introduction of microbial contaminants into the blood sample during phlebotomy. Standardize skin and tube septum disinfection, akin to that done for blood cultures. 2. Tube order. Standardize the order of the QFT-GIT tubes during phlebotomy per the package insert (purge tube - nil tube - antigen tube - mitogen tube). 3. Blood volume. Standardize blood volume drawn into the QFT-GIT tubes, particularly for the antigen tube. Filling the tubes up to the 1 ml mark is practical. Collecting blood using a syringe and transferring 1 ml to each of the tubes is more accurate. 4. Tube shaking. Standardize gentle shaking of the QFT-GIT tubes per the package insert. Avoid separate shaking of the nil and antigen tubes as differential shaking can result in a false-positive or a false-negative result. 5. Processing delay. Minimize delays in incubation of cells. For the QFT-GIT 13
14 assay, this can be achieved by placing an incubator at the collection site (8) or by using a portable incubator to transport the tubes from the field to the laboratory. Further studies are needed to determine whether the T-Cell Xtend reagent can prolong processing time for the T-SPOT assay. 6. Analytical error. Use automated ELISA and ELISPOT instruments to reduce analytical variability. 7. Manufacturing defect. Institute a quality assurance program to monitor positivity and indeterminate rates. When rates cross a preset threshold and persist (24), halt utilization of potentially faulty lots and alert the manufacturer. 8. Immune boosting. When a two-step testing procedure (TST followed by IGRA) is used, TST boosting of the IGRA result can be avoided by drawing the blood sample for IGRA within 72 hours of TST placement (27). Summary IGRAs are functional assays that are susceptible to variability from various sources. Different sources of variability have different effects with the net sum of all sources resulting in either no change, increase or decrease in assay response. The impact of variability sources becomes most noticeable when TB response is bordering the assay cut-off. While systematic sources of variability can be minimized through assay standardization and quality assurance, random sources are unavoidable and can only be addressed through adoption of an indeterminate range, which is currently lacking for the QFT-GIT assay. Further studies are needed, particularly for the T-SPOT assay, to better define the extent 14
15 of variability attributed to each source. With the launch of the newer generation QFT-Plus assay, there is a need for reproducibility data on the newer version, especially since additional tubes and mechanisms are involved Reference 1. Pai M, Denkinger CM, Kik SV, Rangaka MX, Zwerling A, Oxlade O, Metcalfe JZ, Cattamanchi A, Dowdy DW, Dheda K, Banaei N Gamma interferon release assays for detection of Mycobacterium tuberculosis infection. Clin Microbiol Rev 27: Tameris MD, Hatherill M, Landry BS, Scriba TJ, Snowden MA, Lockhart S, Shea JE, McClain JB, Hussey GD, Hanekom WA, Mahomed H, McShane H, the MVA85A 020 Trial Study Team Safety and efficacy of MVA85A, a new tuberculosis vaccine, in infants previously vaccinated with BCG: a randomised, placebo-controlled phase 2b trial. Lancet 381: Tagmouti S, Slater M, Benedetti A, Kik SV, Banaei N, Cattamanchi A, Metcalfe J, Dowdy D, van Zyl Smit R, Dendukuri N, Pai M, Denkinger C Reproducibility of interferon gamma (IFN-gamma) release Assays. A systematic review. Ann Am Thorac Soc 11: Mazurek H, Whitworth WC, Goodwin DJ Affect Of Blood Collection Time On Quantiferon -Tb Gold In-Tube Test Variability. Am J Respir Crit Care Med 185:A Gaur RL, Pai M, Banaei N Impact of blood volume, tube shaking, and incubation time on reproducibility of QuantiFERON-TB gold in-tube assay. J Clin 15
16 Microbiol 51: Smith SG, Joosten SA, Verscheure V, Pathan AA, McShane H, Ottenhoff TH, Dockrell HM, Mascart F Identification of major factors influencing ELISpot-based monitoring of cellular responses to antigens from Mycobacterium tuberculosis. PLoS One 4:e Doberne D, Gaur RL, Banaei N Preanalytical delay reduces sensitivity of QuantiFERON-TB gold in-tube assay for detection of latent tuberculosis infection. J Clin Microbiol 49: Herrera V, Yeh E, Murphy K, Parsonnet J, Banaei N Immediate incubation reduces indeterminate results for QuantiFERON-TB Gold in-tube assay. J Clin Microbiol 48: Yun JW, Chung HS, Koh WJ, Chung DR, Kim YJ, Kang ES Significant reduction in rate of indeterminate results of the QuantiFERON-TB Gold In-Tube test by shortening incubation delay. J Clin Microbiol 52: Jarvis J, Gao Y, de Graaf H, Hughes S, Allan RN, Williams A, Marshall B, Elkington P, Faust SN, Tebruegge M Environmental temperature impacts on the performance of QuantiFERON-TB Gold In-Tube assays. J Infect 71: Beffa P, Zellweger A, Janssens JP, Wrighton-Smith P, Zellweger JP Indeterminate test results of T-SPOT.TB performed under routine field conditions. Eur Respir J 31: Wang SH, Stew SS, Cyktor J, Carruthers B, Turner J, Restrepo BI Validation of increased blood storage times with the T-SPOT.TB assay with T- 16
17 Cell Xtend reagent in individuals with different tuberculosis risk factors. J Clin Microbiol 50: Bouwman JJ, Thijsen SF, Bossink AW Improving the timeframe between blood collection and interferon gamma release assay using T-Cell Xtend(R). J Infect 64: Lenders LM, Meldau R, van Zyl-Smit RN, Woodburne V, Maredza A, Cashmore TJ, Semple PL, Badri M, Zumla A, Dheda K Comparison of same day versus delayed enumeration of TB-specific T cell responses. J Infect 60: King TC, Upfal M, Gottlieb A, Adamo P, Bernacki E, Kadlecek CP, Jones JG, Humphrey-Carothers F, Rielly AF, Drewry P, Murray K, DeWitt M, Matsubara J, O'Dea L, Balser J, Wrighton-Smith P T-SPOT.TB Interferon-gamma Release Assay Performance in Healthcare Worker Screening at Nineteen U.S. Hospitals. Am J Respir Crit Care Med 192: Detjen, AK, Loebenberg, L, Grewal, HM, Stanley, K, Gutschmidt, A, Kruger, C, Du Plessis, N, Kidd, M, Beyers, N, Walzl, G, Hesseling, AC Short-term reproducibility of a commercial interferon gamma release assay. Clin. Vaccine Immunol. 16: Wild, D The immunoassay handbook. Elsevier, Amsterdam ; Boston. 18. Metcalfe, JZ, Cattamanchi, A, McCulloch, CE, Lew, JD, Ha, NP, Graviss, EA Test variability of the QuantiFERON-TB gold in-tube assay in clinical practice. Am. J. Respir. Crit. Care Med. 187: Whitworth, WC, Hamilton, LR, Goodwin, DJ, Barrera, C, West, KB, 17
18 Racster, L, Daniels, LJ, Chuke, SO, Campbell, BH, Bohanon, J, Jaffar, AT, Drane, W, Maserang, D, Mazurek, GH Within-subject interlaboratory variability of QuantiFERON-TB gold in-tube tests. PLoS One. 7:e Tuuminen, T, Tavast, E, Vaisanen, R, Himberg, JJ, Seppala, I Assessment of Imprecision in gamma interferon release assays for the detection of exposure to Mycobacterium tuberculosis. Clin. Vaccine Immunol. 17: Whitworth, WC, Goodwin, DJ, Racster, L, West, KB, Chuke, SO, Daniels, LJ, Campbell, BH, Bohanon, J, Jaffar, AT, Drane, W, Sjoberg, PA, Mazurek, GH Variability of the QuantiFERON(R)-TB gold in-tube test using automated and manual methods. PLoS One. 9:e Franken, WP, Thijsen, S, Wolterbeek, R, Bouwman, JJ, el Bannoudi, H, Kik, SV, van Dissel, JT, Arend, SM Variation in T-SPOT.TB spot interpretation between independent observers from different laboratories. Clin. Vaccine Immunol. 16: van Zyl-Smit, RN, Pai, M, Peprah, K, Meldau, R, Kieck, J, Juritz, J, Badri, M, Zumla, A, Sechi, LA, Bateman, ED, Dheda, K Within-subject variability and boosting of T-cell interferon-gamma responses after tuberculin skin testing. Am. J. Respir. Crit. Care Med. 180: Slater, M, Parsonnet, J, Banaei, N Investigation of false-positive results given by the QuantiFERON-TB Gold In-Tube assay. J. Clin. Microbiol. 50: Slater, M, Dubose, A, Banaei, N False-positive quantiferon results at a large healthcare institution. Clin. Infect. Dis. 58:
19 Couturier, MR, Myatt, R, Dorn, D, Yang, DT, Pitstick, N Defective antigen tubes generate false-positive QuantiFERON tuberculosis test results. Clin. Infect. Dis. 59: van Zyl-Smit, RN, Zwerling, A, Dheda, K, Pai, M Within-subject variability of interferon-γ assay results for tuberculosis and boosting effect of tuberculin skin testing: a systematic review. PLoS One. 4:e Naseer, A, Naqvi, S, Kampmann, B Evidence for boosting Mycobacterium tuberculosis-specific IFN-gamma responses at 6 weeks following tuberculin skin testing. Eur. Respir. J. 29: Baker, CA, Thomas, W, Stauffer, WM, Peterson, PK, Tsukayama, DT Serial testing of refugees for latent tuberculosis using the QuantiFERONgold in-tube: effects of an antecedent tuberculin skin test. Am. J. Trop. Med. Hyg. 80: Igari, H, Watanabe, A, Sato, T Booster phenomenon of QuantiFERON-TB Gold after prior intradermal PPD injection. Int. J. Tuberc. Lung Dis. 11: Perry, S, Sanchez, L, Yang, S, Agarwal, Z, Hurst, P, Parsonnet, J Reproducibility of QuantiFERON-TB gold in-tube assay. Clin. Vaccine Immunol. 15: Mogensen, TH Pathogen recognition and inflammatory signaling in innate immune defenses. Clin. Microbiol. Rev. 22: Clarke, TB, Davis, KM, Lysenko, ES, Zhou, AY, Yu, Y, Weiser, JN Recognition of peptidoglycan from the microbiota by Nod1 enhances systemic 19
20 innate immunity. Nat. Med. 16: Gaur, RL, Suhosk, MM, Banaei, N In Vitro Immunomodulation of a Whole Blood IFN-γ Release Assay Enhances T Cell Responses in Subjects with Latent Tuberculosis Infection. PLoS One. 7:e Gaur, RL, Banaei, N Inoculation of QuantiFERON-TB tubes with skin microbiota causes false-positive results. Am. J. Respir. Crit. Care Med. 190: Downloaded from on August 31, 2018 by guest 20
21 434 Figure Legends Figure 1. Major sources of variability in IGRA results. Source: Pai M et al. Clin Micro Rev 2014 (1) (reproduced with permission) Figure 2. Between-run reproducibility of QFT-GIT assay. The TB response (IFN-γ concentration in antigen tube minus nil tube) was measured from a sample with borderline negative result (A) and another sample with borderline positive result (B) by an automated ELISA instrument over 20 consecutive runs. Samples were stored at 4 C between runs. Two to four ELISA runs were performed each day. The cut-off value for the standard QFT-GIT assay (dashed line) is shown for reference. Positive results are shown in red. Coefficient of variance (CV) and conversion and reversion rates are shown. 21
22 Table 1. Potential sources of variability in IGRAs and their impact on assay response. Impact on Assay Response Source of Variability QFT-GIT T-SPOT Manufacturing Between-lot variability? Pre-analytical Time of blood draw (am vs. pm) pm? Skin disinfection? Traumatic blood draw?? Blood volume ( mL) 1.2mL NA Shaking of blood tubes? T-cell and APC count?? a Transportation temperature? Incubation delay <30 C? Incubation time No effect? Plasma separation delay? b NA Plasma / PBMC storage No effect No effect Analytical Within-run imprecision Between-run imprecision Between-operator imprecision Between-laboratory imprecision Automation Immunological Boosting by TST c c Modulation by PAMP? a The mononuclear input is normalized b According to manufacturer delay after plasma separation contributes to ELISA variability c Particularly in individuals infected with MTB. Less proven in uninfected individuals. NA, not applicable; APC, antigen presenting cell, PAMP, pathogen-associated molecular pattern Source: Adapted from Pai M et al. Clin Micro Rev 2014 (reproduced with permission) 22
23
24
Investigation of false-positive results by the QuantiFERON-TB Gold In-Tube assay
 JCM Accepts, published online ahead of print on 11 July 2012 J. Clin. Microbiol. doi:10.1128/jcm.00730-12 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Investigation of false-positive
JCM Accepts, published online ahead of print on 11 July 2012 J. Clin. Microbiol. doi:10.1128/jcm.00730-12 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Investigation of false-positive
Impact of blood volume, tube shaking, and incubation time on the reproducibility
 JCM Accepts, published online ahead of print on 21 August 2013 J. Clin. Microbiol. doi:10.1128/jcm.01627-13 Copyright 2013, American Society for Microbiology. All Rights Reserved. 1 2 Impact of blood volume,
JCM Accepts, published online ahead of print on 21 August 2013 J. Clin. Microbiol. doi:10.1128/jcm.01627-13 Copyright 2013, American Society for Microbiology. All Rights Reserved. 1 2 Impact of blood volume,
Effect of prolonged incubation time on the results of the QuantiFERON TB Gold In-Tube assay for the diagnosis of latent tuberculosis infection
 CVI Accepts, published online ahead of print on 3 July 2013 Clin. Vaccine Immunol. doi:10.1128/cvi.00290-13 Copyright 2013, American Society for Microbiology. All Rights Reserved. 1 2 3 Effect of prolonged
CVI Accepts, published online ahead of print on 3 July 2013 Clin. Vaccine Immunol. doi:10.1128/cvi.00290-13 Copyright 2013, American Society for Microbiology. All Rights Reserved. 1 2 3 Effect of prolonged
Testing for TB. Bart Van Berckelaer Territory Manager Benelux. Subtitle
 Testing for TB Bart Van Berckelaer Territory Manager Benelux Subtitle Agenda TB infection pathway TB immunisation Testing options Pre lab considerations of the whole blood ELISA test The T-SPOT.TB test
Testing for TB Bart Van Berckelaer Territory Manager Benelux Subtitle Agenda TB infection pathway TB immunisation Testing options Pre lab considerations of the whole blood ELISA test The T-SPOT.TB test
Detecting latent tuberculosis using interferon gamma release assays (IGRA)
") Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
Immediate Incubation Reduces Indeterminate Results for QuantiFERON-TB Gold In-Tube Assay
 JOURNAL OF CLINICAL MICROBIOLOGY, Aug. 2010, p. 2672 2676 Vol. 48, No. 8 0095-1137/10/$12.00 doi:10.1128/jcm.00482-10 Copyright 2010, American Society for Microbiology. All Rights Reserved. Immediate Incubation
JOURNAL OF CLINICAL MICROBIOLOGY, Aug. 2010, p. 2672 2676 Vol. 48, No. 8 0095-1137/10/$12.00 doi:10.1128/jcm.00482-10 Copyright 2010, American Society for Microbiology. All Rights Reserved. Immediate Incubation
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
Evaluation of QuantiFERON -TB Gold-Plus in Healthcare Workers in a Low- Incidence Setting
 JCM Accepted Manuscript Posted Online 15 March 2017 J. Clin. Microbiol. doi:10.1128/jcm.02498-16 Copyright 2017 American Society for Microbiology. All Rights Reserved. 1 2 Evaluation of QuantiFERON -TB
JCM Accepted Manuscript Posted Online 15 March 2017 J. Clin. Microbiol. doi:10.1128/jcm.02498-16 Copyright 2017 American Society for Microbiology. All Rights Reserved. 1 2 Evaluation of QuantiFERON -TB
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Variation in T-SPOT.TB spot interpretation between independent observers of different laboratories
 8 Variation in T-SPOT.TB spot interpretation between independent observers of different laboratories Willeke P.J. Franken 1, Steven Thijsen 2, Ron Wolterbeek 3, John J.M. Bouwman 2, Hanane el Bannoudi
8 Variation in T-SPOT.TB spot interpretation between independent observers of different laboratories Willeke P.J. Franken 1, Steven Thijsen 2, Ron Wolterbeek 3, John J.M. Bouwman 2, Hanane el Bannoudi
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Conflict of Interest Disclosures:
 Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
TB Intensive Tyler, Texas December 2-4, 2008
 TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Interferon-gamma release assay for treatment monitoring of active tuberculosis
 JCM Accepts, published online ahead of print on 21 November 2012 J. Clin. Microbiol. doi:10.1128/jcm.02278-12 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Interferon-gamma
JCM Accepts, published online ahead of print on 21 November 2012 J. Clin. Microbiol. doi:10.1128/jcm.02278-12 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Interferon-gamma
Richard N. van Zyl-Smit 1, Rannakoe J. Lehloenya 1,2, Richard Meldau 1, Keertan Dheda 1,3,4. Introduction
 Original Article Impact of correcting the lymphocyte count to improve the sensitivity of TB antigen-specific peripheral blood-based quantitative T cell assays (T-SPOT. TB and QFT-GIT) Richard N. van Zyl-Smit
Original Article Impact of correcting the lymphocyte count to improve the sensitivity of TB antigen-specific peripheral blood-based quantitative T cell assays (T-SPOT. TB and QFT-GIT) Richard N. van Zyl-Smit
Keywords: tuberculosis; IFN-g release assays; diagnostics; reproducibility
 Reproducibility of Interferon Gamma (IFN-g) Release Assays A Systematic Review Saloua Tagmouti 1, Madeline Slater 2, Andrea Benedetti 3,4, Sandra V. Kik 3,4, Niaz Banaei 5, Adithya Cattamanchi 6, John
Reproducibility of Interferon Gamma (IFN-g) Release Assays A Systematic Review Saloua Tagmouti 1, Madeline Slater 2, Andrea Benedetti 3,4, Sandra V. Kik 3,4, Niaz Banaei 5, Adithya Cattamanchi 6, John
Using Interferon Gamma Release Assays for Diagnosis of TB Infection
 Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Technical Bulletin No. 172
 CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
Peggy Leslie-Smith, RN
 Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
IGRA Test Reliability. How Test Design and Lab Control Impact Results
 IGRA Test Reliability How Test Design and Lab Control Impact Results IGRA Test Reliability Background Why IGRAs are uniquely challenging to both test manufacturers and labs Why complexity exists with both
IGRA Test Reliability How Test Design and Lab Control Impact Results IGRA Test Reliability Background Why IGRAs are uniquely challenging to both test manufacturers and labs Why complexity exists with both
Laboratory Updates on IGRA Testing
 Laboratory Updates on IGRA Testing Edward A. Graviss, PhD, MPH, FIDSA August 18, 2017 EXCELLENCE EXPERTISE INNOVATION Edward A. Graviss, PhD, MPH, FIDSA, has the following disclosures to make: No conflict
Laboratory Updates on IGRA Testing Edward A. Graviss, PhD, MPH, FIDSA August 18, 2017 EXCELLENCE EXPERTISE INNOVATION Edward A. Graviss, PhD, MPH, FIDSA, has the following disclosures to make: No conflict
Testing & Treatment for TB Infection: Blood Tests, Skin Tests, Who to Screen & Who to Treat?
 NECHA 11/4/2016 Testing & Treatment for TB Infection: Blood Tests, Skin Tests, Who to Screen & Who to Treat? E. Jane Carter, M.D. Immediate Past President International Union Against TB and Lung Disease
NECHA 11/4/2016 Testing & Treatment for TB Infection: Blood Tests, Skin Tests, Who to Screen & Who to Treat? E. Jane Carter, M.D. Immediate Past President International Union Against TB and Lung Disease
QuantiFERON-TB Gold Plus
 QuantiFERON-TB Gold Plus A New Interferon-γ Release Assay (IGRA) for the Indirect Detection of Mycobacterium tuberculosis HOT TOPIC / 2018 Presenter: Elitza S. Theel, PhD, D(ABMM) Director of Infectious
QuantiFERON-TB Gold Plus A New Interferon-γ Release Assay (IGRA) for the Indirect Detection of Mycobacterium tuberculosis HOT TOPIC / 2018 Presenter: Elitza S. Theel, PhD, D(ABMM) Director of Infectious
Journal of Infectious Diseases Advance Access published August 2, 2013
 Journal of Infectious Diseases Advance Access published August 2, 2013 1 Reversion and Conversion of Interferon-gamma Release Assay Results in HIV-1 Infected Individuals Maximilian C. Aichelburg 1,*, Thomas
Journal of Infectious Diseases Advance Access published August 2, 2013 1 Reversion and Conversion of Interferon-gamma Release Assay Results in HIV-1 Infected Individuals Maximilian C. Aichelburg 1,*, Thomas
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Literature Overview. Health Economics. Experience with QuantiFERON -TB Gold. Cellestis Clinical Guide series
 Literature Overview Experience with QuantiFERON -TB Gold Health Economics Cellestis Clinical Guide series 2008 www.cellestis.com This literature overview is intended to provide healthcare professionals
Literature Overview Experience with QuantiFERON -TB Gold Health Economics Cellestis Clinical Guide series 2008 www.cellestis.com This literature overview is intended to provide healthcare professionals
Qualitative and quantitative results of interferon-γ release assays for monitoring the response to anti-tuberculosis treatment
 ORIGINAL ARTICLE Korean J Intern Med 217;32:32-38 https://doi.org/1.394/kjim.216.199 Qualitative and quantitative results of interferon-γ release assays for monitoring the response to anti-tuberculosis
ORIGINAL ARTICLE Korean J Intern Med 217;32:32-38 https://doi.org/1.394/kjim.216.199 Qualitative and quantitative results of interferon-γ release assays for monitoring the response to anti-tuberculosis
Richard O Brien, Consultant, FIND 3 rd Global Symposium on IGRAs Waikoloa, Hawaii, 13 January 2012
 Global l Applications of IGRAs Richard O Brien, Consultant, FIND 3 rd Global Symposium on IGRAs Waikoloa, Hawaii, 13 January 2012 Disclosure I have no personal financial conflicts of I have no personal
Global l Applications of IGRAs Richard O Brien, Consultant, FIND 3 rd Global Symposium on IGRAs Waikoloa, Hawaii, 13 January 2012 Disclosure I have no personal financial conflicts of I have no personal
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
QFT-Plus: a plus in variability? Evaluation of new generation IGRA in serial testing of students with a migration background in Germany
 Knierer et al. Journal of Occupational Medicine and Toxicology (2017) 12:1 DOI 10.1186/s12995-016-0148-z RESEARCH Open Access QFT-Plus: a plus in variability? Evaluation of new generation IGRA in serial
Knierer et al. Journal of Occupational Medicine and Toxicology (2017) 12:1 DOI 10.1186/s12995-016-0148-z RESEARCH Open Access QFT-Plus: a plus in variability? Evaluation of new generation IGRA in serial
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Indeterminate test results of T-SPOT TM.TB performed under routine field conditions
 Eur Respir J 2008; 31: 842 846 DOI: 10.1183/09031936.00117207 CopyrightßERS Journals Ltd 2008 Indeterminate test results of T-SPOT TM.TB performed under routine field conditions P. Beffa*, A. Zellweger
Eur Respir J 2008; 31: 842 846 DOI: 10.1183/09031936.00117207 CopyrightßERS Journals Ltd 2008 Indeterminate test results of T-SPOT TM.TB performed under routine field conditions P. Beffa*, A. Zellweger
The Direct Comparison of Two Interferon-gamma Release Assays in the Tuberculosis Screening of Japanese Healthcare Workers
 ORIGINAL ARTICLE The Direct Comparison of Two Interferon-gamma Release Assays in the Tuberculosis Screening of Japanese Healthcare Workers Masaki Tanabe 1, Akiko Nakamura 1, Akie Arai 1, Daisuke Yamasaki
ORIGINAL ARTICLE The Direct Comparison of Two Interferon-gamma Release Assays in the Tuberculosis Screening of Japanese Healthcare Workers Masaki Tanabe 1, Akiko Nakamura 1, Akie Arai 1, Daisuke Yamasaki
LTBI-Tuberculin skin test. T-Spot.TB Technology. QuantiFERON -TB Gold In Tube T-SPOT.TB ELISA ELISA
 LTBI-Tuberculin skin test QuantiFERON -TB Gold In Tube ELISA PPD ~200 antigens 3 ml blood ESAT-6 TB 7.7 16-24 hour incubation Nil Negative control PHA Positive control Andersen et al Lancet 2000;356:1099-1104
LTBI-Tuberculin skin test QuantiFERON -TB Gold In Tube ELISA PPD ~200 antigens 3 ml blood ESAT-6 TB 7.7 16-24 hour incubation Nil Negative control PHA Positive control Andersen et al Lancet 2000;356:1099-1104
Category Description / Key Findings Publication
 PUBLICATIONS Selected T-SPOT.TB test publications, by area of interest, up to 31 th August 2016. Category Description / Key Findings Publication Background A useful primer on the evolution, administration
PUBLICATIONS Selected T-SPOT.TB test publications, by area of interest, up to 31 th August 2016. Category Description / Key Findings Publication Background A useful primer on the evolution, administration
Thorax Online First, published on December 8, 2009 as /thx
 Thorax Online First, published on December 8, 2009 as 10.1136/thx.2009.119677 Title Page Cost effectiveness of the NICE guidelines for screening for latent tuberculosis infection: the Quantiferon-TB gold
Thorax Online First, published on December 8, 2009 as 10.1136/thx.2009.119677 Title Page Cost effectiveness of the NICE guidelines for screening for latent tuberculosis infection: the Quantiferon-TB gold
BMC Infectious Diseases QuantiFERON conversion following tuberculin administration is common in HIV infection. Should cut-off be lower?
 BMC Infectious Diseases QuantiFERON conversion following tuberculin administration is common in HIV infection. Should cut-off be lower? --Manuscript Draft-- Manuscript Number: Full Title: Article Type:
BMC Infectious Diseases QuantiFERON conversion following tuberculin administration is common in HIV infection. Should cut-off be lower? --Manuscript Draft-- Manuscript Number: Full Title: Article Type:
Utility of PPD or IGRA to answer the age old question of "TB or not TB
 Utility of PPD or IGRA to answer the age old question of "TB or not TB Thomas S. Alexander, Ph.D., D(ABMLI) Immunologist Summa Health alexandt@summahealth.org Yes, The reservation is in the name of Dr.
Utility of PPD or IGRA to answer the age old question of "TB or not TB Thomas S. Alexander, Ph.D., D(ABMLI) Immunologist Summa Health alexandt@summahealth.org Yes, The reservation is in the name of Dr.
Use of an Interferon- Release Assay To Diagnose Latent Tuberculosis Infection in Foreign-Born Patients*
 Original Research MYCOBACTERIAL DISEASE Use of an Interferon- Release Assay To Diagnose Latent Tuberculosis Infection in Foreign-Born Patients* Daniel Brodie, MD; David J. Lederer, MD, MS; Jade S. Gallardo,
Original Research MYCOBACTERIAL DISEASE Use of an Interferon- Release Assay To Diagnose Latent Tuberculosis Infection in Foreign-Born Patients* Daniel Brodie, MD; David J. Lederer, MD, MS; Jade S. Gallardo,
ORIGINAL ARTICLE. Clinical evaluation of QuantiFERON TB-2G test for immunocompromised patients
 ERJ Express. Published on July 25, 2007 as doi: 10.1183/09031936.00040007 ORIGINAL ARTICLE Clinical evaluation of QuantiFERON TB-2G test for immunocompromised patients Yoshihiro Kobashi, Keiji Mouri, Yasushi
ERJ Express. Published on July 25, 2007 as doi: 10.1183/09031936.00040007 ORIGINAL ARTICLE Clinical evaluation of QuantiFERON TB-2G test for immunocompromised patients Yoshihiro Kobashi, Keiji Mouri, Yasushi
Within-Subject Variability of Mycobacterium tuberculosis-specific Gamma Interferon Responses in German Health Care Workers
 CLINICAL AND VACCINE IMMUNOLOGY, July 2011, p. 1176 1182 Vol. 18, No. 7 1556-6811/11/$12.00 doi:10.1128/cvi.05058-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Within-Subject
CLINICAL AND VACCINE IMMUNOLOGY, July 2011, p. 1176 1182 Vol. 18, No. 7 1556-6811/11/$12.00 doi:10.1128/cvi.05058-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Within-Subject
questions Frequently asked General tuberculosis information T-SPOT.TB Test description and performance T-SPOT.TB Test performance characteristics
 General tuberculosis information Frequently asked questions T-SPOT.TB Test description and performance T-SPOT.TB Test performance characteristics T-SPOT.TB advantages over tuberculin skin test T-SPOT.TB
General tuberculosis information Frequently asked questions T-SPOT.TB Test description and performance T-SPOT.TB Test performance characteristics T-SPOT.TB advantages over tuberculin skin test T-SPOT.TB
Short-Term Reproducibility of a Commercial Interferon Gamma Release Assay
 CLINICAL AND VACCINE IMMUNOLOGY, Aug. 2009, p. 1170 1175 Vol. 16, No. 8 1556-6811/09/$08.00 0 doi:10.1128/cvi.00168-09 Copyright 2009, American Society for Microbiology. All Rights Reserved. Short-Term
CLINICAL AND VACCINE IMMUNOLOGY, Aug. 2009, p. 1170 1175 Vol. 16, No. 8 1556-6811/09/$08.00 0 doi:10.1128/cvi.00168-09 Copyright 2009, American Society for Microbiology. All Rights Reserved. Short-Term
No, not these...or these.
 Interpretation of IGRA Results - Session Commentary - Matthew J. Binnicker, Ph.D., D(ABMM) The Big Three: No, not these...or these. The Big Three: Commonly asked questions when interpreting IGRA results:
Interpretation of IGRA Results - Session Commentary - Matthew J. Binnicker, Ph.D., D(ABMM) The Big Three: No, not these...or these. The Big Three: Commonly asked questions when interpreting IGRA results:
borderline range for Quantiferon Gold In-Tube Tube results Abstract Objective Methods Results Conclusions
 RESEARCH ARTICLE A borderline range for Quantiferon Gold In- Tube results Jerker Jonsson 1,2, Anna Westman 3,4, Judith Bruchfeld 2,5, Erik Sturegård 6, Hans Gaines 1,2,5, Thomas Schön 7,8 * a1111111111
RESEARCH ARTICLE A borderline range for Quantiferon Gold In- Tube results Jerker Jonsson 1,2, Anna Westman 3,4, Judith Bruchfeld 2,5, Erik Sturegård 6, Hans Gaines 1,2,5, Thomas Schön 7,8 * a1111111111
Update on IGRA Predictive Value
 Update on IGRA Predictive Value Sandra Kik, PhD Molebogeng Rangaka, MD, PhD Madhukar Pai, MD, PhD McGill International TB Centre, McGill University University of Cape Town & London School of Hygiene and
Update on IGRA Predictive Value Sandra Kik, PhD Molebogeng Rangaka, MD, PhD Madhukar Pai, MD, PhD McGill International TB Centre, McGill University University of Cape Town & London School of Hygiene and
Clinical evaluation of QuantiFERON TB-2G test for immunocompromised patients
 Eur Respir J 2007; 30: 945 950 DOI: 10.1183/09031936.00040007 CopyrightßERS Journals Ltd 2007 Clinical evaluation of QuantiFERON TB-2G test for immunocompromised patients Y. Kobashi, K. Mouri, Y. Obase,
Eur Respir J 2007; 30: 945 950 DOI: 10.1183/09031936.00040007 CopyrightßERS Journals Ltd 2007 Clinical evaluation of QuantiFERON TB-2G test for immunocompromised patients Y. Kobashi, K. Mouri, Y. Obase,
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA)
 and Interferon-gamma Release Assays (IGRA)") Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2019 Bob Belknap M.D. Director, Denver Metro TB Program Disclosures No relevant financial relationships Objectives Be able to
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2019 Bob Belknap M.D. Director, Denver Metro TB Program Disclosures No relevant financial relationships Objectives Be able to
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Time interval to conversion of interferon-c release assay after exposure to tuberculosis
 Eur Respir J 2011; 37: 1447 1452 DOI: 10.1183/09031936.00089510 CopyrightßERS 2011 Time interval to conversion of interferon-c release assay after exposure to tuberculosis S.W. Lee*,#, D.K. Oh ", S.H.
Eur Respir J 2011; 37: 1447 1452 DOI: 10.1183/09031936.00089510 CopyrightßERS 2011 Time interval to conversion of interferon-c release assay after exposure to tuberculosis S.W. Lee*,#, D.K. Oh ", S.H.
The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over?
 The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over? ROY F. CHEMALY, MD, MPH, FIDSA, FACP PROFESSOR OF MEDICINE DIRECTOR, INFECTION CONTROL SECTION
The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over? ROY F. CHEMALY, MD, MPH, FIDSA, FACP PROFESSOR OF MEDICINE DIRECTOR, INFECTION CONTROL SECTION
Mædica - a Journal of Clinical Medicine
 Mædica - a Journal of Clinical Medicine ORIGINAL PAPERS Prospective Comparison of Two Brands of Tuberculin Skin Tests and Quantiferon-TB Gold in-tube Assay Performances for Tuberculosis Infection in Hospitalized
Mædica - a Journal of Clinical Medicine ORIGINAL PAPERS Prospective Comparison of Two Brands of Tuberculin Skin Tests and Quantiferon-TB Gold in-tube Assay Performances for Tuberculosis Infection in Hospitalized
IGRAs for Diagnosis of Tuberculosis: 2010 Update
 IGRAs for Diagnosis of Tuberculosis: 2010 Update Nira Pollock, M.D., Ph.D. Division of Infectious Diseases Beth Israel Deaconess Medical Center Boston, MA May 1, 2010 Problems with the PPD False positives
IGRAs for Diagnosis of Tuberculosis: 2010 Update Nira Pollock, M.D., Ph.D. Division of Infectious Diseases Beth Israel Deaconess Medical Center Boston, MA May 1, 2010 Problems with the PPD False positives
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Use of Interferon-γ Release Assays (IGRAs) in TB control in low and middle-income settings - EXPERT GROUP MEETING -
 in TB control in low and middle-income settings - EXPERT GROUP MEETING -") Use of Interferon-γ Release Assays (IGRAs) in TB control in low and middle-income settings - EXPERT GROUP MEETING - Date and time: 20-21 July 2010, 09:00 18:00 Venue: Salle B, WHO-HQ, Geneva, Switzerland
Use of Interferon-γ Release Assays (IGRAs) in TB control in low and middle-income settings - EXPERT GROUP MEETING - Date and time: 20-21 July 2010, 09:00 18:00 Venue: Salle B, WHO-HQ, Geneva, Switzerland
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
A Clinician s Perspective: Improving Rheumatology Patient Care Using the T-SPOT.TB Test
 A Clinician s Perspective: Improving Rheumatology Patient Care Using the T-SPOT.TB Test Solomon Forouzesh, MD, FACD, FACR Medical Director Arthritis Care & Treatment Center Clinical Associate Professor
A Clinician s Perspective: Improving Rheumatology Patient Care Using the T-SPOT.TB Test Solomon Forouzesh, MD, FACD, FACR Medical Director Arthritis Care & Treatment Center Clinical Associate Professor
Identifying TB co-infection : new approaches?
 Identifying TB co-infection : new approaches? Charoen Chuchottaworn MD. Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH Primary tuberculosis Natural history
Identifying TB co-infection : new approaches? Charoen Chuchottaworn MD. Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH Primary tuberculosis Natural history
[DOI] /j.issn
![[DOI] /j.issn](/thumbs/93/114201584.jpg "[DOI] /j.issn") 56 2018 1 1431 - [ ]- - T- SPOT.TB 5638 18T-SPOT.TB T-SPOT.TB86.5%(95%CI 71.2%~95.5%) 100%(95%CI 90.5%~100%) 52.9%(95%CI 27.8%~77.0%) 35.3%(95%CI 14.2%~61.7%) 80.0%(95%CI 64.4%~90.9%) 77.1%(95%CI 62.7%~88.0%)
56 2018 1 1431 - [ ]- - T- SPOT.TB 5638 18T-SPOT.TB T-SPOT.TB86.5%(95%CI 71.2%~95.5%) 100%(95%CI 90.5%~100%) 52.9%(95%CI 27.8%~77.0%) 35.3%(95%CI 14.2%~61.7%) 80.0%(95%CI 64.4%~90.9%) 77.1%(95%CI 62.7%~88.0%)
Evidence on IGRAs in Low & Middle Income Countries. Madhukar Pai, MD, PhD McGill University, Montreal
 Evidence on IGRAs in Low & Middle Income Countries Madhukar Pai, MD, PhD McGill University, Montreal Madhukar.pai@mcgill.ca Disclosure No industry/financial conflicts I co-chair the Stop TB Partnership
Evidence on IGRAs in Low & Middle Income Countries Madhukar Pai, MD, PhD McGill University, Montreal Madhukar.pai@mcgill.ca Disclosure No industry/financial conflicts I co-chair the Stop TB Partnership
Screening for Tuberculosis Infection. Harlingen, TX. Linda Dooley, MD has the following disclosures to make:
 TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
Interpretation of TST & IGRA results. Objectives
 Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Evidence-based use of the new diagnostic tools for TB-infection
 Evidence-based use of the new diagnostic tools for TB-infection Roland Diel, MD, MPH German Central Committee against Tuberculosis, Germany 20. Tuberkulose-Symposium in Münchenwiler, 24 th March 2011 1
Evidence-based use of the new diagnostic tools for TB-infection Roland Diel, MD, MPH German Central Committee against Tuberculosis, Germany 20. Tuberkulose-Symposium in Münchenwiler, 24 th March 2011 1
Diagnosis of tuberculosis
 Diagnosis of tuberculosis Madhukar Pai, MD, PhD Assistant Professor, Epidemiology McGill University, Montreal, Canada madhukar.pai@mcgill.ca Global TB Case Detection A major concern 2.6 million new smear
Diagnosis of tuberculosis Madhukar Pai, MD, PhD Assistant Professor, Epidemiology McGill University, Montreal, Canada madhukar.pai@mcgill.ca Global TB Case Detection A major concern 2.6 million new smear
Dimitrios Vassilopoulos,* Stamatoula Tsikrika, Chrisoula Hatzara, Varvara Podia, Anna Kandili, Nikolaos Stamoulis, and Emilia Hadziyannis
 CLINICAL AND VACCINE IMMUNOLOGY, Dec. 2011, p. 2102 2108 Vol. 18, No. 12 1556-6811/11/$12.00 doi:10.1128/cvi.05299-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Comparison
CLINICAL AND VACCINE IMMUNOLOGY, Dec. 2011, p. 2102 2108 Vol. 18, No. 12 1556-6811/11/$12.00 doi:10.1128/cvi.05299-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Comparison
LIAISON QuantiFERON -TB Gold Plus Solution
 Tuberculosis LIAISON QuantiFERON -TB Gold Plus Solution Let TB testing flow FOR OUTSIDE THE US AND CANADA ONLY LIAISON QuantiFERON -TB Gold Plus Solution A new fully automated CLIA assay to aid in the
Tuberculosis LIAISON QuantiFERON -TB Gold Plus Solution Let TB testing flow FOR OUTSIDE THE US AND CANADA ONLY LIAISON QuantiFERON -TB Gold Plus Solution A new fully automated CLIA assay to aid in the
IGRAs evolution. José Domínguez
 MESA: Novedades en métodos diagnósticos y en tratamiento Moderadores: Fernando Alcaide. Hospital Universitari de Bellvitge. L Hospitalet de Llobregat. Julià González. Hospital Clínic i Provincial de Barcelona.
MESA: Novedades en métodos diagnósticos y en tratamiento Moderadores: Fernando Alcaide. Hospital Universitari de Bellvitge. L Hospitalet de Llobregat. Julià González. Hospital Clínic i Provincial de Barcelona.
These recommendations will remain in effect until the national shortage of PPD solution has abated.
 Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
COMPARISON OF TWO INTERFERON-G ASSAYS AND
 3 COMPARISON OF TWO INTERFERON-G ASSAYS AND CONTACTS Sandra M. Arend 1, Steven F.T. Thijsen 2, Eliane M.S. Leyten 1, John J.M. Bouwman 2, Willeke P.J. Franken 1 3, Frank G.J. Cobelens 4,5, Arend-Jan van
3 COMPARISON OF TWO INTERFERON-G ASSAYS AND CONTACTS Sandra M. Arend 1, Steven F.T. Thijsen 2, Eliane M.S. Leyten 1, John J.M. Bouwman 2, Willeke P.J. Franken 1 3, Frank G.J. Cobelens 4,5, Arend-Jan van
Title: Response to M. tuberculosis selected RD1 peptides in Ugandan HIV-infected patients with smear positive pulmonary tuberculosis: a pilot study
 Author's response to reviews Title: Response to M. tuberculosis selected RD1 peptides in Ugandan HIV-infected patients with smear positive pulmonary tuberculosis: a pilot study Authors: Delia Goletti (d.goletti@tiscali.it)
Author's response to reviews Title: Response to M. tuberculosis selected RD1 peptides in Ugandan HIV-infected patients with smear positive pulmonary tuberculosis: a pilot study Authors: Delia Goletti (d.goletti@tiscali.it)
Tuberculosis (TB) remains a major global. Are interferon-c release assays useful for diagnosing active tuberculosis in a high-burden setting?
 remains a major global. Are interferon-c release assays useful for diagnosing active tuberculosis in a high-burden setting?") Eur Respir J 2011; 38: 649 656 DOI: 10.1183/09031936.00181610 CopyrightßERS 2011 Are interferon-c release assays useful for diagnosing active tuberculosis in a high-burden setting? D.I. Ling*, M. Pai*,
Eur Respir J 2011; 38: 649 656 DOI: 10.1183/09031936.00181610 CopyrightßERS 2011 Are interferon-c release assays useful for diagnosing active tuberculosis in a high-burden setting? D.I. Ling*, M. Pai*,
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA)
 and Interferon-gamma Release Assays (IGRA)") Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2018 Bob Belknap M.D. Director, Denver Metro TB Program No Disclosures Objectives be able to describe: 1. Who should get tested
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2018 Bob Belknap M.D. Director, Denver Metro TB Program No Disclosures Objectives be able to describe: 1. Who should get tested
Clinical Study Consistency of Mycobacterium tuberculosis-specific Interferon-Gamma Responses in HIV-1-Infected Women during Pregnancy and Postpartum
 Infectious Diseases in Obstetrics and Gynecology Volume 2012, Article ID 950650, 7 pages doi:10.1155/2012/950650 Clinical Study Consistency of Mycobacterium tuberculosis-specific Interferon-Gamma Responses
Infectious Diseases in Obstetrics and Gynecology Volume 2012, Article ID 950650, 7 pages doi:10.1155/2012/950650 Clinical Study Consistency of Mycobacterium tuberculosis-specific Interferon-Gamma Responses
The Most Widely Misunderstood Test of All
 The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Diagnosis and Medical Case Management of Latent TB. Bryan Rock, MD April 27, 2010
 TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
Incidence of occupational latent tuberculosis infection in South African healthcare workers
 ORIGINAL ARTICLE TUBERCULOSIS Incidence of occupational latent tuberculosis infection in South African healthcare workers Shahieda Adams 1,2, Rodney Ehrlich 2, Roslynn Baatjies 3, Richard N. van Zyl-Smit
ORIGINAL ARTICLE TUBERCULOSIS Incidence of occupational latent tuberculosis infection in South African healthcare workers Shahieda Adams 1,2, Rodney Ehrlich 2, Roslynn Baatjies 3, Richard N. van Zyl-Smit
Received 8 February 2007/Returned for modification 20 March 2007/Accepted 10 April 2007
 CLINICAL AND VACCINE IMMUNOLOGY, June 2007, p. 714 719 Vol. 14, No. 6 1556-6811/07/$08.00 0 doi:10.1128/cvi.00073-07 Copyright 2007, American Society for Microbiology. All Rights Reserved. Comparison of
CLINICAL AND VACCINE IMMUNOLOGY, June 2007, p. 714 719 Vol. 14, No. 6 1556-6811/07/$08.00 0 doi:10.1128/cvi.00073-07 Copyright 2007, American Society for Microbiology. All Rights Reserved. Comparison of
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines
 Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
T-Cell Assays for Tuberculosis Infection: Deriving Cut- Offs for Conversions Using Reproducibility Data
 T-Cell Assays for Tuberculosis Infection: Deriving Cut- Offs for Conversions Using Reproducibility Data Anandharaman Veerapathran 1,2, Rajnish Joshi 1,2,3, Kalyan Goswami 1,2, Sandeep Dogra 4, Erica E.
T-Cell Assays for Tuberculosis Infection: Deriving Cut- Offs for Conversions Using Reproducibility Data Anandharaman Veerapathran 1,2, Rajnish Joshi 1,2,3, Kalyan Goswami 1,2, Sandeep Dogra 4, Erica E.
Juzar Ali, MD, FRCP(C) FCCP has the following disclosures to make:
 FCCP has the following disclosures to make:") Interferon Gamma Release Assays (IGRA) Juzar Ali, MD, FRCP(C) FCCP June 27, 2018 TB Intensive June 26-29, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Juzar Ali, MD, FRCP(C) FCCP has the following
Interferon Gamma Release Assays (IGRA) Juzar Ali, MD, FRCP(C) FCCP June 27, 2018 TB Intensive June 26-29, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Juzar Ali, MD, FRCP(C) FCCP has the following
Diagnosis of tuberculosis: principles and practice of using interferon- release assays (IGRAs)
") Diagnosis of tuberculosis: principles and practice of using interferon- release assays (IGRAs) Educational aims To provide an overview of interferon- release assays (IGRAs) used for detection of tuberculosis
Diagnosis of tuberculosis: principles and practice of using interferon- release assays (IGRAs) Educational aims To provide an overview of interferon- release assays (IGRAs) used for detection of tuberculosis
RESEARCH NOTE QUANTIFERON -TB GOLD IN-TUBE TEST FOR DIAGNOSING LATENT TUBERCULOSIS INFECTION AMONG CLINICAL-YEAR THAI MEDICAL STUDENTS
 Southeast Asian J Trop Med Public Health RESEARCH NOTE QUANTIFERON -TB GOLD IN-TUBE TEST FOR DIAGNOSING LATENT TUBERCULOSIS INFECTION AMONG CLINICAL-YEAR THAI MEDICAL STUDENTS Benjawan Phetsuksiri 1, Somchai
Southeast Asian J Trop Med Public Health RESEARCH NOTE QUANTIFERON -TB GOLD IN-TUBE TEST FOR DIAGNOSING LATENT TUBERCULOSIS INFECTION AMONG CLINICAL-YEAR THAI MEDICAL STUDENTS Benjawan Phetsuksiri 1, Somchai
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Comparison of Quantiferon-TB Gold With Tuberculin Skin Test for Detecting Latent Tuberculosis Infection Prior to Liver Transplantation
 American Journal of Transplantation 2007; 7: 2797 2801 Blackwell Munksgaard C 2007 The Authors Journal compilation C 2007 The American Society of Transplantation and the American Society of Transplant
American Journal of Transplantation 2007; 7: 2797 2801 Blackwell Munksgaard C 2007 The Authors Journal compilation C 2007 The American Society of Transplantation and the American Society of Transplant
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
2016 OPAM Mid-Year Educational Conference, Sponsored by AOCOPM Sunday, March 13, 2016
 Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
Evaluation of Mycobacterium tuberculosis specific T cell response to ESAT-6 and PPD antigen with ELISPOT assay
 In the name of God Evaluation of Mycobacterium tuberculosis specific T cell response to ESAT-6 and PPD antigen with ELISPOT assay presented by: M. Taheri Symptoms of TB Cough for more than two week Bloody
In the name of God Evaluation of Mycobacterium tuberculosis specific T cell response to ESAT-6 and PPD antigen with ELISPOT assay presented by: M. Taheri Symptoms of TB Cough for more than two week Bloody
Report on WHO Policy Statements
 Report on WHO Policy Statements Christopher Gilpin TB Diagnostics and Laboratory Strengthening Unit Secretariat, Global Laboratory Initiative Stop TB Department, WHO Geneva New Diagnostics Working Group
Report on WHO Policy Statements Christopher Gilpin TB Diagnostics and Laboratory Strengthening Unit Secretariat, Global Laboratory Initiative Stop TB Department, WHO Geneva New Diagnostics Working Group
Title: Comparison of an ESAT-6/ CFP-10 Peptide-Based ELISPOT Assay to Tuberculin. Skin Test for Tuberculosis Screening in a Moderate Risk Population
 CVI Accepts, published online ahead of print on 18 April 2007 Clin. Vaccine Immunol. doi:10.1128/cvi.00073-07 Copyright 2007, American Society for Microbiology and/or the Listed Authors/Institutions. All
CVI Accepts, published online ahead of print on 18 April 2007 Clin. Vaccine Immunol. doi:10.1128/cvi.00073-07 Copyright 2007, American Society for Microbiology and/or the Listed Authors/Institutions. All
Interferon-gamma release assays for the tuberculosis serial testing of health care workers: a systematic review
 Ringshausen et al. Journal of Occupational Medicine and Toxicology 2012, 7:6 RESEARCH Open Access Interferon-gamma release assays for the tuberculosis serial testing of health care workers: a systematic
Ringshausen et al. Journal of Occupational Medicine and Toxicology 2012, 7:6 RESEARCH Open Access Interferon-gamma release assays for the tuberculosis serial testing of health care workers: a systematic
University of Groningen
 University of Groningen Positive predictive value of ELISpot in BAL and pleural fluid from patients with suspected pulmonary tuberculosis Hofland, Regina W.; Thijsen, Steven F. T.; van Lindert, Anne S.
University of Groningen Positive predictive value of ELISpot in BAL and pleural fluid from patients with suspected pulmonary tuberculosis Hofland, Regina W.; Thijsen, Steven F. T.; van Lindert, Anne S.