Treatment of Tuberculosis. Dr Sarabjit Chadha The Union
|
|
|
- Gabriella Summers
- 5 years ago
- Views:
Transcription

1 Treatment of Tuberculosis Dr Sarabjit Chadha The Union
 describes pulmonary consumption with cervical lymphnodes surgical")
2 History of treatment of TB. Believed to be as old as mankind Spinal TB has been diagnosed in Egyptian mummies dating 2400 BC Egyptian medical treatise (1500 BC) describes pulmonary consumption with cervical lymphnodes surgical lancing of the cyst application of mixture of acacia, peas, fruits, animal blood, insect blood, honey and salt In India Yakshma (resembles TB) finds a mention in scriptures dated 1500 BC to be treated with Breast milk, meat, alcohol and rest Move to higher altitudes

3 History of treatment of TB Hippocrates (460 BC)- gave the name Pthisis Nurse the patient in temple, good food and asses milk Galen (200 AD) Opium, blood letting; barley water, fish and fruit In 1600s Henry IV started the practice of Royal touch Unfortunately Henry IV himself died of TB


4 History of treatment of TB. In 1854 Hermann Brehmer build the first sanatorium
")
5 History of treatment of TB. Sanatorium Rest Good food Milk (Calcium) Sunlight High altitude


")
6 History of treatment of TB.. Surgical treatment Pneumothorax Carlo Forlanini Thoracoplasty Rib resection (Quincke) Total (Sauerbruch) Plombage


7 The advent of chemotherapy Dr. Selman A. Waksman - Discovered STREPTOMYCIN in Together with his laboratory assistant A. Schatz
8 Streptomycin.the wonder drug Treatment of TB started in 1946, with streptomycin First clinical trial by BMRC Dramatic reduction in immediate mortality Bed rest and Sm (27% vs 7%) Striking improvement in chest radiology and bacteriology
9 Sm resistance 5-year assessment showed that Sm did not improve outcomes due to emergence of Sm resistance Days since Start of Treatment
10 Other anti-tb drugs In 1949 PAS was introduced BMRC trial using Sm+PAS showed reduced incidence of resistance to SM S SP 60 % resistant cultures Months of treatment
11 Other anti TB drugs INH, R and Z INH introduced in 1952; Several studies with INH +Sm/PAS Sir John Crofton 3 SPH/9PH with no failures 1 year of hospitalisation/sanatorium - Very expensive Famous trial at TRC in India Domiciliary treatment as effective as sanatorium treatment Z in 1954 and Rif in 1963 addition of R and Z reduce the relapse rate when added to INH+Sm Short course therapy
12 Other anti TB drugs Clinical trials in various countries bactericidal synergism between R and Z R an effective sterilising drug throughout treatment, Z only in IP Initial intensive phase should last 2 months Treatment regimens 2RHZE/4RH were extensively trialled in Singapore 2 RHZE/6 TH (trialled in East Africa) HIV infection made Thioacetazone unusable Replaced with Ethambutol 6-month regimen - 2HRZE/4RH 8-month regimen 2 HRZE/6HE
13 Fundamentals of TB treatment Drug combinations Long term treatment Single dose administration

14 Drug Combinations Used mainly to prevent drug resistance as it prevents selection of resistant mutants The fall and rise mechanism
15 An unselected population of Mycobacterium tuberculosis S H E R S E E H
16 Selecting resistance by INH monotherapy H H H H H H H H H H H H H H H H H H H H H H H H
17 Long term treatment Allows action on different bacterial populations Rapidly multiplying bacteria Extracellular with maximum oxygenation Slowly multiplying bacteria Intramacrophagic location; acidic ph Intermittently growing bacteria Solid caseum Bacteria in latent/dormant stage Relapses and reactivation INH PZA RIF No drugs

18 Single dose administration Achieve peak blood levels Facilitate supervision Fixed dose combinations
19 Objectives of treatment To make the patient non-infectious as early as possible Early bactericidal activity of drugs To prevent relapse Sterilising action To prevent selection of resistance Combination of drugs Minimal side effects
20 Early bactericidal activity (EBA) Fall in viable CFU of M. TB /ml sputum per day During first few days of treatment with a drug EBA does not tell us anything about sterilization An agent with a good EBA may be a poor sterilizing agent INH has the maximum EBA Therapeutic margin Therapeutic dose/minimal effective dose INH 20; Rif - 4; Sm-1.5 High therapeutic margin indicates that the drug can penetrate large necrotic lesions
21 Anti-TB Drugs. Early Bactericidal Activity (EBA, 2 Days), measured for the reduction in the CFU in Sputum Edited: HL Rieder
22 Sterilisation The ability to kill the persisting, dormant or intermittently active bacilli, responsible for relapses Rapid sterilization will lead to the shortening of treatment R and Z are responsible for most of the killing of persisting bacilli Z may have a better sterilising action as compared to other drugs

23 Chemotherapy in TB
24 Principles for designing TB regimen At least 3 new or probably effective drugs At least 1 bactericidal and 1 sterilising drug to be continued through out the treatment H bactericidal R and Z are the sterilising drugs H and R continued throughout the treatment Z is stopped after Intensive Phase Regimen could be RHZ/RH
25 Why do we need a fourth drug? The fourth drug is given to protect against possible initial resistance to INH, not to kill bacilli Streptomycin is probably a better drug higher bactericidal activity In most countries more than the 50% of the strains with initial resistance to INH have also resistance to SM
26 Which is a better regimen? 2RHZE/4RH or 2RHZE/6HE
27
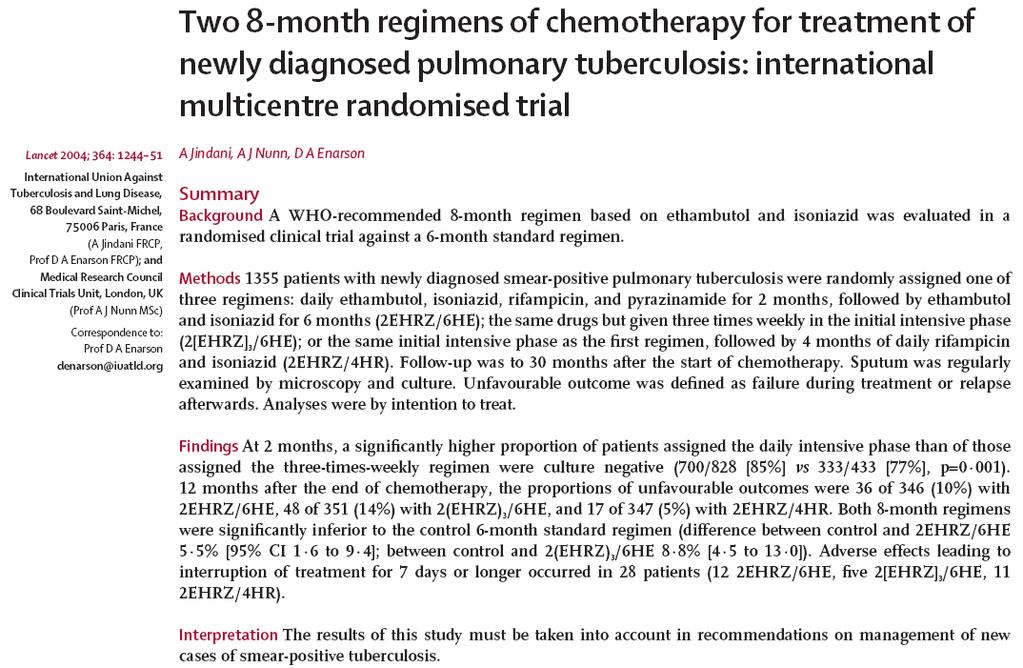
28 The Union Study A Outcome at 12 and 30 months after stopping treatment Regimen Unfavourable outcome at 12 mths 30 mths Failure Relapse Total Total 2EHRZ/6EH 5.5% 4.9% 10.4% 11.7% 2(EHRZ)3/6EH 6.3% 7.4% 13.7% 15.3% 2EHRZ/4HR 3.5% 1.4% 4.9% 6% Lancet 2004;364:
29 The Union study A Unfavourable outcomes at 12 mths (H res) Regimen INH susc INH -resist 2EHRZ/6EH 9.3% 38.5% 2(EHRZ)3/6EH 10.2% 27.3% 2EHRZ/4HR 3.7% 4.3% Lancet 2004;364:
30 How long to give rifampicin? 2 Months or 6 Months

31 - 57 trials with 312 arms and 21,472 participants were included - Regimens utilizing rifampin only for the first 1 2 m had significantly higher rates of failure, relapse, and acquired drug resistance, as compared to regimens that used rifampin for 6 m. - This was particularly evident when there was initial drug resistance to isoniazid, streptomycin, or both. - On the other hand, there was little evidence of difference in failure or relapse with daily or intermittent schedules of treatment administration
32 Ideal treatment regimen 2 HRZE / 4 HR
33 Intermittent regimen Rationale behind intermittent regimen Lag phase Easy to supervise Cost effective How does intermittent regimen work? Is it as effective as daily regimen?
34 Toman s, 2004 Lag phase
35 Bacteriopausal Effects during re-growth Number of viable bacilli Susceptible to Drug A Mutants resistant to A Lag due to drug A Lag due to drug B Regrowth starting Killing phase Regrowth Mitchison DA. In J Tuberc Lung Dis 1998;2:10-15
36 Toman s, 2004
37 Toman s, 2004
38 Is intermittent regimen recommended now?

39 - A total of 32 articles were included after excluding 331 ineligible articles, 42 non analytical studies, 22 narrative reviews or expert opinions and 44 articles embedded in systematic reviews. - These included 9 systematic reviews, 8 controlled studies, 9 pharmacokinetic-pharmacodynamic studies, 5 mouse studies and 1 article about guinea pig experiments. - Findings suggest high levels of evidence for using daily dosing schedules, especially during the initial phase in the presence of cavitation, isoniazid resistance and advanced HIV co-infection, to reduce the risk of treatment failure, recurrence and acquired drug resistance including acquired rifamycin resistance

40 HIV-infected patients treated with rifampin-based regimens alone had a higher risk for relapse and development of rifampin resistance if intermittent dosing of rifampin was started during the intensive phase of treatment, compared with patients who did not receive intermittent dosing (hazard ratio [HR] for relapse, 6.7 [95% CI, ]; HR for adquired rifampin resistance ARR-, 6.4 [95% CI, ]). This association remained when confined to patients with a CD4+ T lymphocyte count of < 100 lymphocytes/mm3. Intermittent dosing started only after the intensive phase of treatment did not increase the risks of relapse and ARR among HIV-infected patients with TB.
 than with regimens using rifamycin for at least 8 months.")
41 citations (6 randomized trials and 21 cohort studies) - Relapse was more common with regimens using 2 months rifamycin (ARR, 3.6; 95% CI, ) than with regimens using rifamycin for at least 8 months. - Compared with daily therapy in the initial phase (3352 patients from 35 study arms), thrice-weekly therapy (211 patients from 5 study arms) was associated with higher rates of failure (ARR, 4.0; 95% CI, ) and relapse [ARR, 4.8; 95% CI, ). - There were trends toward higher relapse rates if rifamycins were used for only 6 months, compared with 8 months, or if antiretroviral therapy was not used.
, whereas prolonging both intensive phase and overall treatment by 50% or more protected against relapse (OR 0.24, 95% CI 0.08 0.")
42 - Thrice-weekly treatment increased the risk of relapse in comparison with daily treatment (OR 3.92, 95% CI ), whereas prolonging both intensive phase and overall treatment by 50% or more protected against relapse (OR 0.24, 95% CI ) - When pretreatment culture was positive and cavitation was absent, the 30-month relapse rate for standard thrice-weekly regimen was 1.1% (95% CI %) - The corresponding rates in the presence of cavitation were 7.8% (95% CI %) for standard thrice-weekly regimen; 3.3% (95% CI %) for standard daily regimen; 0.5% (95% CI %) for extended thrice-weekly regimen; and 0.4% (95% CI %) for extended daily regimen

43 Only six cohort studies were identified, in which failure rates were 18% 44% in those with isoniazid resistance. In nine trials, using very different regimens in previously treated patients with mono-resistance to isoniazid, the combined failure and relapse rates ranged from 0% to over 75%. From pooled analysis of 33 trials in 1,907 patients with monoresistance to isoniazid, lower failure, relapse, and acquired drug resistance rates were associated with longer duration of rifampin, use of streptomycin, daily therapy initially, and treatment with a greater number of effective drugs
44 Intermittent regimen - Conclusions - Inspite of the limited evidence, it seems the daily treatment (at least in the Intensive phase) can reduce the rate of relapses, specially in patients HIV+, with Cavitary TB and with INH Resistance - As these patients are very frequent, perhaps the NTP should evaluate to introduce daily regimens
45 Important questions Follow up of patients on treatment How frequently? Does sputum monitoring predict outcome? Does extending IP improve outcomes? Can we reduce the duration of treatment? Is the current retreatment regimen rational?
46 Response to treatment Sputum examination is done End of intensive phase Mid of the continuation phase End of the treatment Assess response to treatment Identify those at risk of failure Identify those who are at risk of relapse??

47 Lancet Infect Dis 2010, 10:
![PREDICTING RELAPSES - The pooled SENSITIVITY for both 2-month SMEAR (24% [95% CI 12 42%], 6 Studies) and CULTURE (40% [95% CI 25 56%], 4](/docs-images/85/91917974/images/48-2.jpg "studies) were low. -Corresponding SPECIFICITY (85% [95% CI 72 90%] and 85% [95% CI 77 91%])were higher, but modest.")
48 PREDICTING RELAPSES - The pooled SENSITIVITY for both 2-month SMEAR (24% [95% CI 12 42%], 6 Studies) and CULTURE (40% [95% CI 25 56%], 4 studies) were low. -Corresponding SPECIFICITY (85% [95% CI 72 90%] and 85% [95% CI 77 91%])were higher, but modest. Lancet Infect Dis 2010, 10:
49 PREDICTING FAILURES - 2-month smear (seven studies) had low SENSITIVITY (57% [95% CI 41 73%]) and higher, although modest, SPECIFICITY (81% [95% CI 72 87%]). - Sensitivity is the proportion of patients who experienced treatment failure and had a positive sputum examination. - Specificity is the proportion of patients who did not experience treatment failure and had a negative sputum examination Lancet Infect Dis 2010, 10:


50
 and 2.0% (95%CI 1.4 2.8) smear- and culture-positive failures, and 1.2% (95%CI 1.0 1.4), 2.6% (95%CI 1.9 3.4) and 0.9% (95%CI 0.5 1.4) relapses were detected.")
51 Of patients evaluated, were smear-negative at 2 months (2M ); 1871 and 1870 (2M+) were randomised to no extension or extension (1M). Respectively 0.3% (95%CI ), 1.2% (95%CI ) and 2.0% (95%CI ) smear- and culture-positive failures, and 1.2% (95%CI ), 2.6% (95%CI ) and 0.9% (95%CI ) relapses were detected. Extension significantly reversed the relative risk (RR) of relapse of 2M+ vs. 2M patients from 2.2 (95%CI ) to 0.7 (95%CI ). The RR for failure remained high, at 7.3 (95%CI ) with and 4.2 (95% CI ) without extension.
52 Conclusions: Treatment failure and acquired RMP resistance cannot be prevented by a 1-month extension of the intensive phase It is possible that the reduced relapse rate could also have been obtained by extending the continuation phase. This would reduce costs, adverse events and the risk of amplifying resistance by continued use of EMB and PZA if MDR-TB is present
53 Conclusion Historically extension was recommended when Rif was used only for 2 months (4RHZE/6HE) Based on only 1 study In 1000 TB patients with a 7% risk of relapse, extending the treatment of 183 patients would avert 16 of the 70 expected relapses To achieve this 23% reduction in relapses, 158 patients per 1000 would be incorrectly predicted to relapse; their treatment would be extended unnecessarily
54 Shorter regimens 4 months OFLOTUB trial- completed REMOX trial- completed 3 months PaMZ- ongoing
55 Non-inferiority, randomised trial New, Smear+, Rif sensitive cases Control arm- 2HRZE/4HR Experimental arm- 2HRZG/2HRG The standard regimen compared with the 4-month regimen Higher dropout rate during treatment (5.0% vs. 2.7%) more treatment failures (2.4% vs. 1.7%) fewer recurrences (7.1% vs. 14.6%). No evidence of increased risks of prolongation of the QT interval or dysglycemia with the 4-month regimen Non-inferiority of the 4-month regimen to the standard regimen not shown
56 Randomised, double blinded, placebo controlled trials Compare 2 Moxifloxacin containing regimens with a control regimen Group 1 (Control): HRZE (8 weeks)/hr (18 weeks) Group 2: Ethambutol replaced by Moxifloxacin (17 weeks) Group 3: INH replaced by Moxifloxacin (17 weeks) The Moxi regimens showed more rapid initial decline in bacterial load (culture conversion) Favourable outcome in control group (92%) was better than the INH group (85%) and Emb group (80%) Non-inferiority for Moxi regimens was not demonstrated Shortening of treatment to 4 months was not effective
57 Re-treatment regimen 2RHZES/1RHZE/5RHE Indications- Relapses Treatment after LFU (TAD) Failures In case of relapse and TAD most of the patients are susceptible so Cat I should work as well In case of failures where the prevalence of MDR TB is higher retreatment regimen will only amplify resistance It may be beneficial in INH resistant cases protecting rifampicin resistance????



58 Amplification of resistance in case of initial INH resistance 2 HRZE/4 H R FAILURE Initial Resistance to H 2 HRZE/4 H R MDR, but suscpt. Z+E 2HRZES/1HRZE/5H R E Risk of Amplifying Resistance E (Avoidable if DST before 3rd Month)


59 Amplification Amplification of of resistance resistance of resistance in in case case of in of initial case initial INH of INH resistance resistance initial MDR TB 2 HRZE/4 H R FAILURE Initial M.D.R. 2 HRZE/4 H R Resistance to HR+E+Z 2HRZES/1HRZE/5H R E Risk of Amplifying Resistance to S


60 WHO guidelines 2017
61 Regimens included 4MfxHRZ, 4MfxRZE, 2MfxRZE/2(Mfx+RFP)2, 2MfxRZE/4(Mfx+RFP)1, 2(MfxHRZ)3/2(MfxHR)3 2GfxHRZ/2GfxHR, 2(GfxHRZ)3/2(GfxHR)3, Shorter FQ containing regimens of 4 months are associated with significantly higher rates of relapse at 18 months No reduction of adverse events with the fluoroquinolone containing regimen May lead to a rise in FQ resistance
62 Test non-inferiority of 4 month FQ containing regimens in Body mass index (BMI) greater than 18 nonsevere non-cavitary disease Extra-pulmonary disease The optimal dosing of fluoroquinolone needs to be determined To determine why certain groups are more likely to do worse with a 4-month FQ containing regimen.
63 FDCs are non-inferior and as effective as separate drug formulations in terms of treatment failure, death, treatment adherence and adverse events Patient satisfaction was higher with FDCs Slightly higher rate of relapse and acquired drug resistance with FDCs Bioavailability of the drugs in the FDCs were not evaluated
64 Additional research on the reasons why FDC formulations did not show a clear benefit over separate drug formulations Pharmacokinetic studies of the bioavailability of FDCs versus separate drug formulations
65 Thrice-weekly dosing had a higher risk of treatment failure, disease relapse and acquired drug resistance in DS-TB and unknown susceptibility More vulnerable populations are at risk of missing medication doses or not absorbing the doses (HIV) well with intermittent regimen increased risk of unfavourable outcomes. Requirements for different drug manufacturing and packaging and a reduced drug supply buffer and risk of stock-outs Adherence to treatment was not addressed adequately enough in the reviewed studies to be included as an outcome The data used in this review examined only patients with DS pulm TB and had no adverse reactions requiring modification of the dosing schedule
66 The utility and efficacy of 5 days per week versus 7 days of treatment per week in the intensive phase of therapy The optimal duration of the intensive phase of therapy. Additional research on the benefit of thrice-weekly dosing in the continuation phase
 showed that across CD4 strata, earlier and early ART is associated with a reduction in overall mortality compared to delayed ART Similar grade 3/4 non-iris events in early and delayed ART")
67 The review focused on the relative benefits of ART within 2 weeks ("earlier initiation ) or 8 weeks ( early initiation ) compared to ART after 8 weeks ( delayed initiation ) High-quality evidence (8 trials) showed that across CD4 strata, earlier and early ART is associated with a reduction in overall mortality compared to delayed ART Similar grade 3/4 non-iris events in early and delayed ART Higher incidence of IRIS in early ART Higher mortality but absolute number of deaths was small
68 PLHIV responding to ART need not expect a more unfavourable outcome to TB treatment than HIV neg Rates of failure and death did not differ between persons treated with 6 months rifampicin vs those treated for 8 months or later with or without ART Relapse rate was higher in 6 months regimen if patient was not on ART Ensuring the early start of ART should be prioritized
69 What are the factors that may cause PLHIV to not respond well to TB treatment starting ART late, low CD4 cell counts, drug resistance, cumulative drug toxicity, drug-drug interaction Explore and describe etiological factors leading to higher death rates and rates of adverse events in HIV-positive TB patients.
70 RCTs showed lower mortality, death, severe disability and relapse when patients treated with steroids in addition to anti- TB treatment Steroids should be given regardless of the severity of meningitis In TB pericarditis, benefit of steroid treatment with regard to death and constrictive pericarditis and treatment adherence Steroids may increase risk of HIV related cancers (non-hodgkins lymphoma and Kaposi sarcoma) Individually, the largest study (n=1400) and IMPI study showed no benefit of steroids
71 The optimal steroid dose and duration for TB meningitis (including different drug formulations and for different severities) The different effects of steroids on people who are HIVpositive or HIV-negative, or who are being treated with ART or not The relationship between steroid treatment and cancer risk with reference to the Mayosi et al. study on pericarditis

72 Standard of care is to do DST in all retreatment cases and treat accordingly Failures, interrupted treatment, relapse have higher risk of drug resistance Cat II adds single drug (Sm) to an unsuccessful regimen?? Streptomycin causes a high rate of adverse events, including ototoxicity and nephrotoxicity INH resistant patients are at higher risk of amplifying drug resistance Xpert does not detect H resistance The systematic review found had only indirect evidence from observational studies and no RCTs What to give in place of Cat II??? Mono or poly non MDR drug resistance RHZE through out

73

74
75 Thank You
The treatment of patients with initial isoniazid resistance
 The treatment of patients with initial isoniazid resistance 2011 INTERTB Meeting, St George s, London Patrick Phillips, MRC Clinical Trials Unit DA Mitchison, AJ Nunn. 21 st October 2011 Outline Background
The treatment of patients with initial isoniazid resistance 2011 INTERTB Meeting, St George s, London Patrick Phillips, MRC Clinical Trials Unit DA Mitchison, AJ Nunn. 21 st October 2011 Outline Background
Global epidemiology of drug-resistant tuberculosis. Factors contributing to the epidemic of MDR/XDR-TB. CHIANG Chen-Yuan MD, MPH, DrPhilos
 Global epidemiology of drug-resistant tuberculosis Factors contributing to the epidemic of MDR/XDR-TB CHIANG Chen-Yuan MD, MPH, DrPhilos By the end of this presentation, participants would be able to describe
Global epidemiology of drug-resistant tuberculosis Factors contributing to the epidemic of MDR/XDR-TB CHIANG Chen-Yuan MD, MPH, DrPhilos By the end of this presentation, participants would be able to describe
Improving Translation in TB Drug Development Through Quantitative Modeling. CPTR Workshop 2016, Washington DC
 Improving Translation in TB Drug Development Through Quantitative Modeling Lessons from Recent Phase III TB Trials CPTR Workshop 2016, Washington DC Christian Lienhardt Global TB Programme WHO, Geneva,
Improving Translation in TB Drug Development Through Quantitative Modeling Lessons from Recent Phase III TB Trials CPTR Workshop 2016, Washington DC Christian Lienhardt Global TB Programme WHO, Geneva,
Issues in TB Drug Development for Sensitive Disease - Clinical Development
 Issues in TB Drug Development for Sensitive Disease - Clinical Development GATB Open Forum New Delhi, 5-6 May 2008 Christian Lienhardt, MD, DTM, MSc, PhD IRD, Paris, France & International Union Against
Issues in TB Drug Development for Sensitive Disease - Clinical Development GATB Open Forum New Delhi, 5-6 May 2008 Christian Lienhardt, MD, DTM, MSc, PhD IRD, Paris, France & International Union Against
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Management of MDR TB. Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore
 Management of MDR TB Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore Outline Global epidemiology of Tuberculosis Epidemiology of Tuberculosis
Management of MDR TB Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore Outline Global epidemiology of Tuberculosis Epidemiology of Tuberculosis
NEW DRUGS FOR TUBERCULOSIS: THE NEED, THE HOPE AND THE REALITY
 NEW DRUGS FOR TUBERCULOSIS: THE NEED, THE HOPE AND THE REALITY Neil W. Schluger, M.D. Professor of Medicine, Epidemiology and Environmental Health Sciences Columbia University Global tuberculosis incidence
NEW DRUGS FOR TUBERCULOSIS: THE NEED, THE HOPE AND THE REALITY Neil W. Schluger, M.D. Professor of Medicine, Epidemiology and Environmental Health Sciences Columbia University Global tuberculosis incidence
Development of New Regimens for Tuberculosis Zhenkun Ma, Ph.D.
 Development of New Regimens for Tuberculosis Chief Scientific Officer Global Alliance for TB Drug Development 40 Wall Street, 24th Floor New York, NY 10005 USA 1 Outline What are the unmet needs in TB
Development of New Regimens for Tuberculosis Chief Scientific Officer Global Alliance for TB Drug Development 40 Wall Street, 24th Floor New York, NY 10005 USA 1 Outline What are the unmet needs in TB
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Guidelines for treatment of drug-susceptible tuberculosis and patient care
 TREATMENT OF TUBERCULOSIS Guidelines for treatment of drug-susceptible tuberculosis and patient care 2017 UPDATE Annex 4 EVIDENCE-TO-DECISION TABLES TREATMENT OF TUBERCULOSIS Guidelines for treatment
TREATMENT OF TUBERCULOSIS Guidelines for treatment of drug-susceptible tuberculosis and patient care 2017 UPDATE Annex 4 EVIDENCE-TO-DECISION TABLES TREATMENT OF TUBERCULOSIS Guidelines for treatment
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
Principles and practice of treating drug-sensitive TB
 Principles and practice of treating drug-sensitive TB Brian Eley Paediatric Infectious Diseases Unit Red Cross War Memorial Children s Hospital Department of Paediatrics and Child Health University of
Principles and practice of treating drug-sensitive TB Brian Eley Paediatric Infectious Diseases Unit Red Cross War Memorial Children s Hospital Department of Paediatrics and Child Health University of
Title: Meta-analysis of Individual patient Data (IPD) of Patients with INH (mono or poly-drug) Resistant Tuberculosis.
 of Patients with INH (mono or poly-drug) Resistant Tuberculosis.") Title: Meta-analysis of Individual patient Data (IPD) of Patients with INH (mono or poly-drug) Resistant Tuberculosis. Principal Investigator: Dick Menzies, MD Evidence base for treatment of INH resistant
Title: Meta-analysis of Individual patient Data (IPD) of Patients with INH (mono or poly-drug) Resistant Tuberculosis. Principal Investigator: Dick Menzies, MD Evidence base for treatment of INH resistant
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Tuberculosis
 Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist, NH GEISELMED.DARTMOUTH.EDU GEISELMED.DARTMOUTH.
 The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
The shorter regimen for MDR-TB: evidence and pitfalls
 The shorter regimen for MDR-TB: evidence and pitfalls Helen Cox 10 November 2017 What is the shortened regimen? Current conventional regimen (SA): Intensive Phase (at least 6 months): PZA / (EMB) / Kana
The shorter regimen for MDR-TB: evidence and pitfalls Helen Cox 10 November 2017 What is the shortened regimen? Current conventional regimen (SA): Intensive Phase (at least 6 months): PZA / (EMB) / Kana
Tuberculosis. New TB diagnostics. New drugs.new vaccines. Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012
 Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
Annex 1. Methods for evidence reviews and modelling
 WHO/HTM/TB/2011.6a. Methods for evidence reviews and modelling Questions for the 2011 update of the Guidelines for the programmatic management of drug-resistant tuberculosis (for Outcomes please see Table
WHO/HTM/TB/2011.6a. Methods for evidence reviews and modelling Questions for the 2011 update of the Guidelines for the programmatic management of drug-resistant tuberculosis (for Outcomes please see Table
WHO treatment guidelines for isoniazidresistant
 WHO treatment guidelines for isoniazidresistant tuberculosis Online Annexes: Supplement to the WHO treatment guidelines for drug-resistant tuberculosis WHO treatment guidelines for isoniazid-resistant
WHO treatment guidelines for isoniazidresistant tuberculosis Online Annexes: Supplement to the WHO treatment guidelines for drug-resistant tuberculosis WHO treatment guidelines for isoniazid-resistant
Tuberculosis Intensive November 17 20, 2015 San Antonio, TX
 Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Sirturo: a new treatment against multidrug resistant tuberculosis
 Sirturo: a new treatment against multidrug resistant tuberculosis TB is an on-going problem WHO estimated incidence of new TB cases 2009 Global Tuberculosis Control: WHO report 2010. Available at: http://www.who.int/tb/publications/global_report/2010/en/index.html
Sirturo: a new treatment against multidrug resistant tuberculosis TB is an on-going problem WHO estimated incidence of new TB cases 2009 Global Tuberculosis Control: WHO report 2010. Available at: http://www.who.int/tb/publications/global_report/2010/en/index.html
HA Convention 2016 : Special Topic Session 3 May 2016
 HA Convention 2016 : Special Topic Session 3 May 2016 Diagnosis and Management of TB in Adults Dr. Thomas Mok COS(RMD), KH Tuberculosis An airborne infectious disease caused by Mycobacterium tuberculosis
HA Convention 2016 : Special Topic Session 3 May 2016 Diagnosis and Management of TB in Adults Dr. Thomas Mok COS(RMD), KH Tuberculosis An airborne infectious disease caused by Mycobacterium tuberculosis
Predicting outcomes and drug resistance with standardised treatment of active tuberculosis
 Eur Respir J 21; 36: 87 877 DOI: 1.1183/931936.15179 CopyrightßERS 21 Predicting outcomes and drug resistance with standardised treatment of active tuberculosis O. Oxlade*,#, K. Schwartzman*,#, M. Pai*,#,
Eur Respir J 21; 36: 87 877 DOI: 1.1183/931936.15179 CopyrightßERS 21 Predicting outcomes and drug resistance with standardised treatment of active tuberculosis O. Oxlade*,#, K. Schwartzman*,#, M. Pai*,#,
Newer anti-tb drugs and regimens. DM Seminar
 Newer anti-tb drugs and regimens DM Seminar 31-10-14 Why are newer drugs/regimens needed? Problems with current drugs/regimens Drug resistance Drug interaction of anti-tubercular drugs with ART Long duration
Newer anti-tb drugs and regimens DM Seminar 31-10-14 Why are newer drugs/regimens needed? Problems with current drugs/regimens Drug resistance Drug interaction of anti-tubercular drugs with ART Long duration
Therapeutic TB vaccines Shortening Treatment for (DS- and) DR-TB?
 DR-TB?") Therapeutic TB vaccines Shortening Treatment for (DS- and) DR-TB? Mark Hatherill South African Tuberculosis Vaccine Initiative (SATVI) University of Cape Town, South Africa 1 1. The need for a therapeutic
Therapeutic TB vaccines Shortening Treatment for (DS- and) DR-TB? Mark Hatherill South African Tuberculosis Vaccine Initiative (SATVI) University of Cape Town, South Africa 1 1. The need for a therapeutic
Marcos Burgos, MD has the following disclosures to make:
 Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Certainty assessment of patients Effect Certainty Importance. a standardised 9 month shorter MDR-TB regimen. e f
 Author(s): STREAM Stage 1 Trial investigators reported for the Guideline Development Group for the WHO treatment guidelines on MDR/RR-TB, 2018 update (6 July 2018) - FINAL RESULTS Question: PICO 1. In
Author(s): STREAM Stage 1 Trial investigators reported for the Guideline Development Group for the WHO treatment guidelines on MDR/RR-TB, 2018 update (6 July 2018) - FINAL RESULTS Question: PICO 1. In
ACCESS TO MEDICINES. Update on tuberculosis field activities
 ACCESS TO MEDICINES Update on tuberculosis field activities Update on clinical activities 1/3 Latent TB Prevent study (S26) main study (8053 patients) PK substudy construction of a POPPK model Paediatric
ACCESS TO MEDICINES Update on tuberculosis field activities Update on clinical activities 1/3 Latent TB Prevent study (S26) main study (8053 patients) PK substudy construction of a POPPK model Paediatric
PHARMACOTHERAPY OF TUBERCULOSIS MANAGEMENT
 PHARMACOTHERAPY OF TUBERCULOSIS MANAGEMENT Rahela Ambaras Khan BPharm (USM), MPharm (Clin.)(UKM), BCPS(US) PhD Student Faculty of Medicine University Malaya OUTLINE Introduction to Tuberculosis Management
PHARMACOTHERAPY OF TUBERCULOSIS MANAGEMENT Rahela Ambaras Khan BPharm (USM), MPharm (Clin.)(UKM), BCPS(US) PhD Student Faculty of Medicine University Malaya OUTLINE Introduction to Tuberculosis Management
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Evidence review for Intermittent therapy for drug-susceptible TB: Questions addressed: intermittent therapy
 Evidence review for Intermittent therapy for drug-susceptible TB: Dr. Dick Menzies Montreal Chest Institute, McGill University Montreal, Canada Questions addressed: intermittent therapy 1: Does intermittent
Evidence review for Intermittent therapy for drug-susceptible TB: Dr. Dick Menzies Montreal Chest Institute, McGill University Montreal, Canada Questions addressed: intermittent therapy 1: Does intermittent
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Standard TB Treatment
 Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
What is drug resistance? Musings of a clinician
 What is drug resistance? Musings of a clinician William Burman MD Denver Public Health Tuberculosis Trials Consortium Financial disclosures Tibotec (developer of TMC207 and several antiretroviral drugs)
What is drug resistance? Musings of a clinician William Burman MD Denver Public Health Tuberculosis Trials Consortium Financial disclosures Tibotec (developer of TMC207 and several antiretroviral drugs)
TB Updates for the Physician Rochester, Minnesota June 19, 2009
 TB Updates for the Physician Rochester, Minnesota June 19, 2009 Recent Findings & Activities of the Tuberculosis Trials Consortium (TBTC) Bill Burman Denver TBTC Unit & Denver Public Health Recent findings
TB Updates for the Physician Rochester, Minnesota June 19, 2009 Recent Findings & Activities of the Tuberculosis Trials Consortium (TBTC) Bill Burman Denver TBTC Unit & Denver Public Health Recent findings
Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health
 Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health C. Robert Horsburgh, Jr. Boston University School of Public Health Background Outline Why does drug resistance threaten
Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health C. Robert Horsburgh, Jr. Boston University School of Public Health Background Outline Why does drug resistance threaten
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Let s Talk TB. A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Abstract Nearly 50% of patients with
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Abstract Nearly 50% of patients with
Treatment: First Line Drugs TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS TREATMENT: GENERAL PRINCIPLES MECHANISM OF ACTION MID 27
 TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
Problems, progress and evaluation of agents in clinical development ACCEPTED. Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands
 AAC Accepts, published online ahead of print on 15 December 2008 Antimicrob. Agents Chemother. doi:10.1128/aac.00749-08 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions.
AAC Accepts, published online ahead of print on 15 December 2008 Antimicrob. Agents Chemother. doi:10.1128/aac.00749-08 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions.
Global Perspective on Transmission: Value in Genotype Mapping of Disease Transmission Dynamics
 Global Perspective on Transmission: Value in Genotype Mapping of Disease Transmission Dynamics Neel R. Gandhi, MD Emory Rollins School of Public Health January 17, 2013 Medical Research Council BMJ 1948
Global Perspective on Transmission: Value in Genotype Mapping of Disease Transmission Dynamics Neel R. Gandhi, MD Emory Rollins School of Public Health January 17, 2013 Medical Research Council BMJ 1948
Shorter TB regimens What is in de pipeline? Martin Boeree, Associate Professor Radboudumc, Nijmegen, the Netherlands Tuesday, 23 September, 2014
 Shorter TB regimens What is in de pipeline? Martin Boeree, Associate Professor Radboudumc, Nijmegen, the Netherlands Tuesday, 23 September, 2014 Disclosures Clinical trials and studies funded by EDCTP,
Shorter TB regimens What is in de pipeline? Martin Boeree, Associate Professor Radboudumc, Nijmegen, the Netherlands Tuesday, 23 September, 2014 Disclosures Clinical trials and studies funded by EDCTP,
A NOVEL PHARMACODYNAMIC MODEL FOR TREATMENT OF TUBERCULOSIS USING DAYS TO POSITIVITY IN AUTOMATED LIQUID MYCOBACTERIAL CULTURE
 A NOVEL PHARMACODYNAMIC MODEL FOR TREATMENT OF TUBERCULOSIS USING DAYS TO POSITIVITY IN AUTOMATED LIQUID MYCOBACTERIAL CULTURE Emmanuel Chigutsa 1, Kashyap Patel 2, Marianne Visser 3, Gary Maartens 1,
A NOVEL PHARMACODYNAMIC MODEL FOR TREATMENT OF TUBERCULOSIS USING DAYS TO POSITIVITY IN AUTOMATED LIQUID MYCOBACTERIAL CULTURE Emmanuel Chigutsa 1, Kashyap Patel 2, Marianne Visser 3, Gary Maartens 1,
Hot Issues in Tuberculosis: Treatment of Latent TB Infection and New TB Drugs
 Slide 1 Hot Issues in Tuberculosis: Treatment of Latent TB Infection and New TB Drugs Constance A. Benson, M.D. Professor of Medicine Division of Infectious Diseases University of California, San Diego
Slide 1 Hot Issues in Tuberculosis: Treatment of Latent TB Infection and New TB Drugs Constance A. Benson, M.D. Professor of Medicine Division of Infectious Diseases University of California, San Diego
Author s response to reviews Title: Bacterial risk factors for treatment failure and relapse among patients with isoniazid resistant tuberculosis
 Author s response to reviews Title: Bacterial risk factors for treatment failure and relapse among patients with isoniazid resistant tuberculosis Authors: Phan Thai (phanvuongkhacthai@yahoo.com) Dang Ha
Author s response to reviews Title: Bacterial risk factors for treatment failure and relapse among patients with isoniazid resistant tuberculosis Authors: Phan Thai (phanvuongkhacthai@yahoo.com) Dang Ha
TB Nurse Case Management San Antonio, Texas April 9-11, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
XDR TUBERCULOSIS IN EUROPE EPIDEMIOLOGICAL ASPECTS. Enrico Girardi Unità di Epidemiologia Clinica INMI Spallanzani, Roma. Pag. 1
 XDR TUBERCULOSIS IN EUROPE EPIDEMIOLOGICAL ASPECTS Enrico Girardi Unità di Epidemiologia Clinica INMI Spallanzani, Roma Pag. 1 TB estimated incidence in EUR, 2004 Russian Fed. 12 th among the 22 TB high-burden
XDR TUBERCULOSIS IN EUROPE EPIDEMIOLOGICAL ASPECTS Enrico Girardi Unità di Epidemiologia Clinica INMI Spallanzani, Roma Pag. 1 TB estimated incidence in EUR, 2004 Russian Fed. 12 th among the 22 TB high-burden
Application for addition of 3-FDC rifampicin 150/isoniazid 75/ethambutol 275 mg (RHE) to the WHO model list of essential medicines
 to the WHO model list of essential medicines") Application for addition of 3-FDC rifampicin 150/isoniazid 75/ethambutol 275 mg (RHE) to the WHO model list of essential medicines Geneva, 10 August 2006 Focal Point: Hugo Vrakking Global Drug Facility
Application for addition of 3-FDC rifampicin 150/isoniazid 75/ethambutol 275 mg (RHE) to the WHO model list of essential medicines Geneva, 10 August 2006 Focal Point: Hugo Vrakking Global Drug Facility
Multidrug-resistant tuberculosis in children
 Multidrug-resistant tuberculosis in children James Seddon Clinical Lecturer Imperial College London UCL-TB and LSHTM TB Centre World TB Day 2015 24th March 2015 Outline Burden Recent studies Preventive
Multidrug-resistant tuberculosis in children James Seddon Clinical Lecturer Imperial College London UCL-TB and LSHTM TB Centre World TB Day 2015 24th March 2015 Outline Burden Recent studies Preventive
Treatment of INH Resistant-TB An aggregate data, and an Individual Patient Data (IPD) meta-analyses
 meta-analyses") Treatment of INH Resistant-TB An aggregate data, and an Individual Patient Data (IPD) meta-analyses Dick Menzies Montreal Chest Institute, McGill International TB Centre NAR Meeting Chicago, March 1-3,
Treatment of INH Resistant-TB An aggregate data, and an Individual Patient Data (IPD) meta-analyses Dick Menzies Montreal Chest Institute, McGill International TB Centre NAR Meeting Chicago, March 1-3,
Outline 8/2/2013. PK/PD PK/PD first-line drug กก PK/PD กก
 Pharmacokinetic and pharmacodynamic of anti- tuberculosis drugs Outline PK/PD PK/PD first-line drug กก PK/PD กก Concentration vs time in tissue and other body fluids Pharmacologic or toxicologic effect
Pharmacokinetic and pharmacodynamic of anti- tuberculosis drugs Outline PK/PD PK/PD first-line drug กก PK/PD กก Concentration vs time in tissue and other body fluids Pharmacologic or toxicologic effect
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf
 Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
SA TB Guidelines The interface with Advanced Clinical Care
 SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
TB and Comorbidities Adriana Vasquez, MD April 12, 2018
 TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Lancelot Pinto is a
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Lancelot Pinto is a
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
Clinical Trials Lecture 4: Data analysis
 Clinical Trials Lecture 4: Data analysis Dick Menzies, MD Respiratory Epidemiology and Clinical Research Unit Montreal Chest Institute TB Research methods course July 17, 2014 Lecture 4: Data analysis
Clinical Trials Lecture 4: Data analysis Dick Menzies, MD Respiratory Epidemiology and Clinical Research Unit Montreal Chest Institute TB Research methods course July 17, 2014 Lecture 4: Data analysis
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
MULTIDRUG- RESISTANT TUBERCULOSIS. Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic
 MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
TB in the Correctional Setting Florence, Arizona October 7, 2014
 TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
6/8/2018 TB TREATMENT. Bijan Ghassemieh, MD Seattle TB Clinical Intensive Disclosures. None
 TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Clinical spectrum and standard treatment of tuberculosis
 Clinical spectrum and standard treatment of tuberculosis Graham Bothamley Homerton University Hospital, London, UK 2 nd European Advanced Course in Clinical Tuberculosis 1 Plan of talk Why is there a clinical
Clinical spectrum and standard treatment of tuberculosis Graham Bothamley Homerton University Hospital, London, UK 2 nd European Advanced Course in Clinical Tuberculosis 1 Plan of talk Why is there a clinical
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
Phase III Clinical Trial Results at the 48 th Union World Conference on Lung Health: Implications for the Field 1
 Phase III Clinical Trial Results at the 48 th Union World Conference on Lung Health: Implications for the Field 1 Preliminary results from two phase III drug-resistant TB (DR-TB) clinical trials were presented
Phase III Clinical Trial Results at the 48 th Union World Conference on Lung Health: Implications for the Field 1 Preliminary results from two phase III drug-resistant TB (DR-TB) clinical trials were presented
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
What He Said: Rifampin versus Rifapentine
 What He Said: Rifampin versus Rifapentine Charles A. Peloquin, Pharm.D. Director Infectious Disease Pharmacokinetics Laboratory Professor, College of Pharmacy & The Emerging Pathogens Institute University
What He Said: Rifampin versus Rifapentine Charles A. Peloquin, Pharm.D. Director Infectious Disease Pharmacokinetics Laboratory Professor, College of Pharmacy & The Emerging Pathogens Institute University
NATIONAL TUBERCULOSIS CONTROL PROGRAMME- SCC AREA Quarterly Report on New and Retreatment Cases of Tuberculosis
 NATIONAL TUBERCULOSIS CONTROL PROGRAMME- SCC AREA Quarterly Report on New and Retreatment Cases of Tuberculosis Patients registered during quarter* of 20 Name of area No.# Name of the Reporter Signature:
NATIONAL TUBERCULOSIS CONTROL PROGRAMME- SCC AREA Quarterly Report on New and Retreatment Cases of Tuberculosis Patients registered during quarter* of 20 Name of area No.# Name of the Reporter Signature:
"Sterilization of TB disease in
 11/1/1 "Sterilization of TB disease in mice " Jacques Grosset Pharmacodynamics of daily rifapentine and rifampin in mice Free rifam mycin Concentrati ion/mic 1 1 Rifapentine (1mg/kg) Free rifam mycin Concentrati
11/1/1 "Sterilization of TB disease in mice " Jacques Grosset Pharmacodynamics of daily rifapentine and rifampin in mice Free rifam mycin Concentrati ion/mic 1 1 Rifapentine (1mg/kg) Free rifam mycin Concentrati
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Management of Multidrug- Resistant TB in Children. Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building
 Management of Multidrug- Resistant TB in Children Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building Objectives To review data on best practices for diagnosis, treatment and prevention
Management of Multidrug- Resistant TB in Children Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building Objectives To review data on best practices for diagnosis, treatment and prevention
New Drugs, New Treatments, Shorter Regimens
 New Drugs, New Treatments, Shorter Regimens Sarah K. Brode, MD MPH FRCP(C) West Park Healthcare Centre, University Health Network, University of Toronto TB Elimination: Back to Basics November 16, 2016
New Drugs, New Treatments, Shorter Regimens Sarah K. Brode, MD MPH FRCP(C) West Park Healthcare Centre, University Health Network, University of Toronto TB Elimination: Back to Basics November 16, 2016
Short Course Treatment for MDR TB
 Objectives Short Course Treatment for MDR TB Barbara J Seaworth M.D. Medical Director Heartland National TB Center Professor of Medicine, University of Texas Health Northeast Participants will utilize
Objectives Short Course Treatment for MDR TB Barbara J Seaworth M.D. Medical Director Heartland National TB Center Professor of Medicine, University of Texas Health Northeast Participants will utilize
Upcoming TB Alliance Studies. CPRT DST Review September, 2014
 Upcoming TB Alliance Studies CPRT DST Review September, 2014 STAND PaMZ Ph 3 STAND: Phase 3 Trial of the Pa-M-Z Regimen Participants with newly diagnosed smear positive DS- and MDR-TB DS Pa(100mg)-M-Z
Upcoming TB Alliance Studies CPRT DST Review September, 2014 STAND PaMZ Ph 3 STAND: Phase 3 Trial of the Pa-M-Z Regimen Participants with newly diagnosed smear positive DS- and MDR-TB DS Pa(100mg)-M-Z
APSR RESPIRATORY UPDATES
 APSR RESPIRATORY UPDATES Volume 5, Issue 2 Newsletter Date: February 2013 APSR EDUCATION PUBLICATION Inside this issue: Tuberculosis Multidrug-resistant pulmonary tuberculosis treatment regimens and patient
APSR RESPIRATORY UPDATES Volume 5, Issue 2 Newsletter Date: February 2013 APSR EDUCATION PUBLICATION Inside this issue: Tuberculosis Multidrug-resistant pulmonary tuberculosis treatment regimens and patient
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
TB-CHAMP A PHASE 3 CLUSTER RANDOMIZED TRIAL FOR PREVENTION OF TB IN CHILD HOUSEHOLD CONTACTS
 TB-CHAMP A PHASE 3 CLUSTER RANDOMIZED TRIAL FOR PREVENTION OF TB IN CHILD HOUSEHOLD CONTACTS ANNEKE C. HESSELING RESIST TB WEBINAR 20 APRIL 2017 DESMOND TUTU TB CENTRE PROFESSOR IN PAEDIATRICS AND CHILD
TB-CHAMP A PHASE 3 CLUSTER RANDOMIZED TRIAL FOR PREVENTION OF TB IN CHILD HOUSEHOLD CONTACTS ANNEKE C. HESSELING RESIST TB WEBINAR 20 APRIL 2017 DESMOND TUTU TB CENTRE PROFESSOR IN PAEDIATRICS AND CHILD
Draft agreed by Efficacy Working Party (EWP) April Adoption by CHMP for release for consultation April 2008
 April Adoption by CHMP for release for consultation April 2008") 20 July 2017 EMA/CHMP/EWP/14377/2008 Rev. 1 Committee for Medicinal Products for Human Use (CHMP) Addendum to the guideline on the evaluation of medicinal products indicated for treatment of bacterial
20 July 2017 EMA/CHMP/EWP/14377/2008 Rev. 1 Committee for Medicinal Products for Human Use (CHMP) Addendum to the guideline on the evaluation of medicinal products indicated for treatment of bacterial
What more is required to use rifamycin regimens to prevent TB in people living with HIV in resource constrained settings?
 What more is required to use rifamycin regimens to prevent TB in people living with HIV in resource constrained settings? Gary Maartens Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI
What more is required to use rifamycin regimens to prevent TB in people living with HIV in resource constrained settings? Gary Maartens Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
TB IN EMERGENCIES. Disease Control in Humanitarian Emergencies (DCE)
") TB IN EMERGENCIES Department of Epidemic and Pandemic Alert and Response (EPR) Health Security and Environment Cluster (HSE) (Acknowledgements WHO Stop TB Programme WHO/STB) 1 Why TB? >33% of the global
TB IN EMERGENCIES Department of Epidemic and Pandemic Alert and Response (EPR) Health Security and Environment Cluster (HSE) (Acknowledgements WHO Stop TB Programme WHO/STB) 1 Why TB? >33% of the global
The Role of Rifampin for the Treatment of Latent TB Infection. Introduction. Introduction
 The Role of Rifampin for the Treatment of Latent TB Infection March 26, 2008 Alfred A. Lardizabal, MD Associate Professor of Medicine New Jersey Medical School Global Tuberculosis institute Treatment of
The Role of Rifampin for the Treatment of Latent TB Infection March 26, 2008 Alfred A. Lardizabal, MD Associate Professor of Medicine New Jersey Medical School Global Tuberculosis institute Treatment of
New TB Medications. National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention New TB Medications Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention New TB Medications Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers
PZA: A New Look Based on RNASeq, the Hollow Fiber System, and Patient Level Data. Tawanda Gumbo
 PZA: A New Look Based on RNASeq, the Hollow Fiber System, and Patient Level Data Tawanda Gumbo Office of Global Health University of Texas Southwestern Medical Center, Dallas, Texas The team: this work
PZA: A New Look Based on RNASeq, the Hollow Fiber System, and Patient Level Data Tawanda Gumbo Office of Global Health University of Texas Southwestern Medical Center, Dallas, Texas The team: this work
Treatment of Tuberculosis
 Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
TBTC research update: are we ready for 3 month treatment? 2009 TBTC Recompetition. NTCA presentation outline
 TBTC research update: are we ready for 3 month treatment? Stefan Goldberg, MD Project officer, TBTC Studies 27, 28, 29 Tuberculosis Trials Consortium (TBTC) CDC Division of TB Elimination NTCA breakout
TBTC research update: are we ready for 3 month treatment? Stefan Goldberg, MD Project officer, TBTC Studies 27, 28, 29 Tuberculosis Trials Consortium (TBTC) CDC Division of TB Elimination NTCA breakout
MDR-TB preventive treatment considerations. HS Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health Stellenbosch University
 MDR-TB preventive treatment considerations HS Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health Stellenbosch University Conflict of interest disclosure X I have no Conflict of Interest
MDR-TB preventive treatment considerations HS Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health Stellenbosch University Conflict of interest disclosure X I have no Conflict of Interest
TB ReFLECT Meta-Analysis of Fluoroquinolone-Containing Regimens for the Treatment of Drug-Susceptible TB
 TB ReFLECT Meta-Analysis of Fluoroquinolone-Containing Regimens for the Treatment of Drug-Susceptible TB Rada Savic, PhD Medical Consultant Meeting San Antonio, TX November 29-30, 2018 1 EXCELLENCE EXPERTISE
TB ReFLECT Meta-Analysis of Fluoroquinolone-Containing Regimens for the Treatment of Drug-Susceptible TB Rada Savic, PhD Medical Consultant Meeting San Antonio, TX November 29-30, 2018 1 EXCELLENCE EXPERTISE
Revised National Tuberculosis Control Programme
 Revised National Tuberculosis Control Programme 2015 C e n t r a l T B D i v i s i o n D i r e c t o r a t e G e n e r a l o f H e a l t h S e r v i c e s M i n i s t r y o f H e a l t h & F a m i l y
Revised National Tuberculosis Control Programme 2015 C e n t r a l T B D i v i s i o n D i r e c t o r a t e G e n e r a l o f H e a l t h S e r v i c e s M i n i s t r y o f H e a l t h & F a m i l y
Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation
 Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation Randall Reves, MD, MSc TB Consultant Professor of Medicine and
Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation Randall Reves, MD, MSc TB Consultant Professor of Medicine and
The Lancet Infectious Diseases
 Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study Susan E Dorman, Samuel G Schumacher, David Alland et al. 2017
Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study Susan E Dorman, Samuel G Schumacher, David Alland et al. 2017
Dosage and Administration
 SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
Annex 2. GRADE glossary and summary of evidence tables
 WHO/HTM/TB/2011.6b. GRADE glossary and summary of evidence tables GRADE glossary Absolute effect The absolute measure of intervention effects is the difference between the baseline risk of an outcome (for
WHO/HTM/TB/2011.6b. GRADE glossary and summary of evidence tables GRADE glossary Absolute effect The absolute measure of intervention effects is the difference between the baseline risk of an outcome (for
Pharmacokinetics (PK) and Pharmacodynamics (PD) in the Treatment of Tuberculosis
 and Pharmacodynamics (PD) in the Treatment of Tuberculosis") Pharmacokinetics (PK) and Pharmacodynamics (PD) in the Treatment of Tuberculosis Shaun E. Gleason, PharmD, MGS Associate Professor, Department of Clinical Pharmacy Director, Distance Degrees and Programs
Pharmacokinetics (PK) and Pharmacodynamics (PD) in the Treatment of Tuberculosis Shaun E. Gleason, PharmD, MGS Associate Professor, Department of Clinical Pharmacy Director, Distance Degrees and Programs
TB Prevention in PLHIV: Options Other Than Isoniazid. Johns Hopkins Center for Tuberculosis. Research. Richard E. Chaisson, MD
 TB Prevention in PLHIV: Options Other Than Isoniazid Johns Hopkins Center for Tuberculosis Richard E. Chaisson, MD Research Johns Hopkins University Center for Tuberculosis Research Consortium to Respond
TB Prevention in PLHIV: Options Other Than Isoniazid Johns Hopkins Center for Tuberculosis Richard E. Chaisson, MD Research Johns Hopkins University Center for Tuberculosis Research Consortium to Respond